Embed Size (px)
DESCRIPTION
kuliah syok cardiogenik
Citation preview

ShockShock

DefinitionDefinition
SHOCK: inadequate organ SHOCK: inadequate organ perfusion to meet the tissue’s perfusion to meet the tissue’s
oxygenation demand.oxygenation demand.

Three major types of shockThree major types of shock Hypovolemic shockHypovolemic shock
» Decreased intravascular volume resulting Decreased intravascular volume resulting form loss of blood, plasma, or fluids and form loss of blood, plasma, or fluids and electrolytes electrolytes
Cardiogenic shockCardiogenic shock» Pump failure due to myocardial damage Pump failure due to myocardial damage
or massive obstruction of outflow tractsor massive obstruction of outflow tracts Distributive shockDistributive shock
» Reduction of vascular resistance formReduction of vascular resistance form SepsisSepsis AnaphylaxisAnaphylaxis Systemic inflammatory response Systemic inflammatory response
syndrome (SIRS)syndrome (SIRS)


Cardiogenic ShockCardiogenic Shock

Cardiogenic ShockCardiogenic Shock
Diminished cardiac output Diminished cardiac output leading to impaired tissue leading to impaired tissue
perfusionperfusion
Most extreme form of pump Most extreme form of pump failurefailure

Cardiogenic ShockCardiogenic Shock
Occurs in about 15% of acute MI Occurs in about 15% of acute MI patientspatients
Usually occurs when 40% or Usually occurs when 40% or more of the left ventricular more of the left ventricular muscle mass infarctsmuscle mass infarcts
Mortality is 85% or more Mortality is 85% or more with with treatmenttreatment

EtiologiesEtiologies Acute myocardial Acute myocardial
infarction/ischemia infarction/ischemia LV failure LV failure Papillary Papillary
muscle/chordal muscle/chordal rupture- severe MRrupture- severe MR
Ventricular free wall Ventricular free wall rupture with rupture with subacute subacute tamponade tamponade
Other conditions complicating large Other conditions complicating large MIs MIs
» HemorrhageHemorrhage» Infection Infection » Excess negative inotropic or Excess negative inotropic or
vasodilator medications vasodilator medications » Prior valvular heart disease Prior valvular heart disease » Hyperglycemia/ketoacidosisHyperglycemia/ketoacidosis» Post-cardiac arrestPost-cardiac arrest» Post-cardiotomyPost-cardiotomy» Refractory sustained Refractory sustained
tachyarrhythmiastachyarrhythmias» Acute fulminant myocarditisAcute fulminant myocarditis» End-stage End-stage
cardiomyopathyHypertrophic cardiomyopathyHypertrophic cardiomyopathy with severe cardiomyopathy with severe outflow obstructionoutflow obstruction
» Aortic dissection with aortic Aortic dissection with aortic insufficiency or tamponadeinsufficiency or tamponade
» Pulmonary emboluPulmonary embolu» Severe valvular heart disease -Severe valvular heart disease -
Critical aortic or mitral stenosis, Critical aortic or mitral stenosis, Acute severe aortic or MRAcute severe aortic or MR

PathophysiologyPathophysiology

Characteristics of Cardiogenic Shock Characteristics of Cardiogenic Shock Low cardiac outputLow cardiac output
Peripheral vasoconstrictionPeripheral vasoconstriction
Left sided heart failure leads to Left sided heart failure leads to pulmonary venous congestion and pulmonary venous congestion and pulmonary edemapulmonary edema
Right sided heart failure leads to Right sided heart failure leads to systemic venous congestion and systemic venous congestion and peripheral edemaperipheral edema

It is essential to distinguish a cardiogenic from a hypovolemic shock!Both forms are associated with reduced cardiac out put, and increased peripheral vascular resistance, however:
Cardiogenic shock: jugular venous distention (high CVP)
Hypovolemic shock: collapsed capacitance veins (low CVP)

Signs/SymptomsSigns/SymptomsConfusion, restlessness, Confusion, restlessness,
anxiety, stupor, comaanxiety, stupor, comaCool, clammy skinCool, clammy skinPallorPallorWeak or absent extremity Weak or absent extremity
pulsespulsesTachycardiaTachycardiaSlow or absent capillary refillSlow or absent capillary refill

Signs/SymptomsSigns/Symptoms
BP < 90 systolic or BP < 90 systolic or >> 30mmHg below normal30mmHg below normal»BP is BP is NOTNOT the same as the same as perfusionperfusion
»Shock can be present with a Shock can be present with a “normal” BP“normal” BP
»Evaluate signs of peripheral Evaluate signs of peripheral perfusion in addition to BPperfusion in addition to BP

Cardiogenic ShockCardiogenic Shock
Treatment Priorities:Treatment Priorities:»RateRate»RhythmRhythm»BP (Volume, Pump/Vascular BP (Volume, Pump/Vascular tone)tone)
Correct major disorders of Correct major disorders of rate, rhythm rate, rhythm beforebefore directly directly treating BPtreating BP

Goals of ManagementGoals of Management
Improve oxygenation and Improve oxygenation and peripheral perfusionperipheral perfusion
Avoid increasing cardiac Avoid increasing cardiac workloadworkload»myocardial oxygen demandmyocardial oxygen demand

ManagementManagement
Primary assessment & Primary assessment & Focused HxFocused Hx
Identify source of problemIdentify source of problem»Acute pulmonary edemaAcute pulmonary edema»Volume problemVolume problem»Pump problemPump problem»Rate problemRate problem

Acute Pulmonary EdemaAcute Pulmonary EdemaFirst line interventionsFirst line interventions
»IV/O2/ECG MonitorIV/O2/ECG Monitor»If BP > 90-100 mm Hg:If BP > 90-100 mm Hg:
furosemide 0.5 – 1.0 mg/kg slow furosemide 0.5 – 1.0 mg/kg slow IV (or twice patient’s single daily IV (or twice patient’s single daily dose up to 120 mg)dose up to 120 mg)
Morphine 2 – 10 mg slow IVMorphine 2 – 10 mg slow IV Nitroglycerin 0.4 mg SLNitroglycerin 0.4 mg SL
»If BP < 90 mm Hg:If BP < 90 mm Hg: Vasopressors based on SBPVasopressors based on SBP

Volume ProblemVolume Problem IV/O2/ECG MonitorIV/O2/ECG MonitorFluid challenge until rales or Fluid challenge until rales or
if evidence of anterior wall if evidence of anterior wall AMIAMI
Vasopressors based on SBPVasopressors based on SBP

Pump ProblemPump Problem IV/O2/ECG MonitorIV/O2/ECG MonitorSBP <70 mmHg:SBP <70 mmHg:
»norepinephrine 0.5 – 30 mcg/min norepinephrine 0.5 – 30 mcg/min IV infIV inf
SBP 70 – 100 mm Hg & shockSBP 70 – 100 mm Hg & shock»dopamine 5 – 15 mcg/kg/min IV infdopamine 5 – 15 mcg/kg/min IV inf
SBP > 100 mm Hg w/o shockSBP > 100 mm Hg w/o shock»dobutamine 2 – 20 mcg/kg/min IV dobutamine 2 – 20 mcg/kg/min IV infinf

ManagementManagement If rate/rhythm adequate, If rate/rhythm adequate,
treat BPtreat BP»Consider fluid challenge of Consider fluid challenge of 250cc LR over 10-15 minutes if 250cc LR over 10-15 minutes if relative or absolute relative or absolute hypovolemia possible, hypovolemia possible, including RVF and NO including RVF and NO pulmonary edemapulmonary edema
»Avoid use of vasopressors until Avoid use of vasopressors until volume deficits corrected or volume deficits corrected or pulmonary edema presentspulmonary edema presents

BP Treatment ReviewBP Treatment Review
If rate, rhythm, volume If rate, rhythm, volume adequate, treat BP with adequate, treat BP with vasopressors:vasopressors:»Norepinephrine, orNorepinephrine, or»DopamineDopamine

NorepinephrineNorepinephrine 0.5 - 30 mcg/min0.5 - 30 mcg/min Inotropic and vasoconstrictive Inotropic and vasoconstrictive
propertiesproperties Can be used if systolic BP < 70Can be used if systolic BP < 70 If systolic BP > 70, use dopamine If systolic BP > 70, use dopamine
insteadinstead DO NOTDO NOT use until hypovolemia use until hypovolemia
correctedcorrected DO NOTDO NOT allow infiltration allow infiltration

DopamineDopamine 2 - 20 mcg/kg/min2 - 20 mcg/kg/min
» Place 200 mg/250cc of DPlace 200 mg/250cc of D55WW» Begin at 5 mcg/kg/minBegin at 5 mcg/kg/min» In 2 - 10 mcg/kg/min range, In 2 - 10 mcg/kg/min range, effects effects
dominatedominate» > 20 mcg/kg/min > 20 mcg/kg/min effects dominate effects dominate» Use lowest dose that produces good Use lowest dose that produces good
perfusionperfusion Use as initial vasopressor if BP 70-Use as initial vasopressor if BP 70-
100 systolic100 systolic» If dopamine infusion rate is > 20 If dopamine infusion rate is > 20
mcg/kg/min use norepinephrinemcg/kg/min use norepinephrine

DopamineDopamine
May cause tachycardia, May cause tachycardia, ectopy, nauseaectopy, nausea
DO NOTDO NOT use until hypovolemia use until hypovolemia is correctedis corrected

Distributive Distributive ShockShock

Distributive ShockDistributive Shock
Reduced peripheral vascular Reduced peripheral vascular tone leads to pooling of blood in tone leads to pooling of blood in extremities extremities poor venous poor venous returnreturn
Physical exam depends on stagePhysical exam depends on stage»Early: Warm extremities, wide Early: Warm extremities, wide pulse pressure, low diastolic pulse pressure, low diastolic pressurepressure
»Late: perfusion pressure falls and Late: perfusion pressure falls and acidosis developsacidosis develops

Distributive ShockDistributive Shock
SepsisSepsis» Due to gram negative or gram positive Due to gram negative or gram positive
bacteriabacteria Anaphylaxis Anaphylaxis
» Due to previous sensitization to an Due to previous sensitization to an allergenallergen
NeurogenicNeurogenic» Due to traumatic spinal cord injuryDue to traumatic spinal cord injury» Effects of epidural or spinal Effects of epidural or spinal
anestheticsanesthetics» Reflex parasymapthetic stimulationReflex parasymapthetic stimulation

Bacteremia, SIRS, SepsisBacteremia, SIRS, Sepsis
BacteremiaBacteremia: an identifiable organism : an identifiable organism cultured from the bloodcultured from the blood
Systemic Inflammatory Response Systemic Inflammatory Response Syndrome (SIRS)Syndrome (SIRS): sepsis without : sepsis without organism identified. Meet at least 2 of organism identified. Meet at least 2 of criteria:criteria:» Hypo or hyperthermiaHypo or hyperthermia» Tachycardia or bradycardiaTachycardia or bradycardia» Tachypnea Tachypnea » Leukocytosis or leukopeniaLeukocytosis or leukopenia
SepsisSepsis: SIRS from a systemic illness : SIRS from a systemic illness (bacterial, viral, protozoal)(bacterial, viral, protozoal)

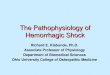
Pathogenesis of Septic Shock(vasodilatory shock)
Pathogenesis of Septic Shock(vasodilatory shock)
Sepsis is defined as a systemic inflammatory Sepsis is defined as a systemic inflammatory response to a bacterial infection with response to a bacterial infection with bacteriemia (though blood cultures can be bacteriemia (though blood cultures can be negative)negative)
Severe sepsis is defined by additional end-Severe sepsis is defined by additional end-organ dysfunction (mortality rate: 25-30%)organ dysfunction (mortality rate: 25-30%)
Septic shock is defined as sepsis with Septic shock is defined as sepsis with hypotension despite fluid resuscitation and hypotension despite fluid resuscitation and evidence of inadequate tissue perfusion (40-evidence of inadequate tissue perfusion (40-70%)70%)

NEJM 2004, Vol. 351;2 pp 159-169

The syndrome of septic shock is characterized by
The syndrome of septic shock is characterized by
Systemic vasodilation (hypotension)Systemic vasodilation (hypotension)
Diminished myocardial contractilityDiminished myocardial contractility
Widespread endothelial injury and Widespread endothelial injury and activation leading to fluid leakage activation leading to fluid leakage (capillary leak) resulting in acute (capillary leak) resulting in acute respiratory distress syndrome (ARDS)respiratory distress syndrome (ARDS)
Activation of the coagulation cascade Activation of the coagulation cascade (DIC)(DIC)

Septic ShockSeptic Shock Early “Warm Early “Warm
Shock”Shock” ↑ ↑ CO and ↓ SVR CO and ↓ SVR
and wide pulse and wide pulse pressurepressure
Signs: warm Signs: warm extremities, extremities, flushing, bounding flushing, bounding pulses, ↑ HR, pulses, ↑ HR, confusionconfusion
Hypocarbia, Hypocarbia, elevated lactate, elevated lactate, hyperglycemiahyperglycemia
Late “Cold Shock”Late “Cold Shock” Uncompensated Uncompensated
shock with drop in shock with drop in COCO
Signs: cyanosis, Signs: cyanosis, cold, clammy skin, cold, clammy skin, thready pulse, thready pulse, shallow respirationshallow respiration
Metabolic acidosis, Metabolic acidosis, hypoxia, hypoxia, coagulopathy, coagulopathy, hypoglycemiahypoglycemia

S/S of Septic ShockS/S of Septic Shock
Increased to low blood Increased to low blood pressurepressure
High fever, no fever, High fever, no fever, hypothermichypothermic
Skin flushed, Pale, CyanoticSkin flushed, Pale, CyanoticDifficulty breathing and Difficulty breathing and
altered lung soundsaltered lung sounds

TX of Septic ShockTX of Septic Shock
Airway controlAirway controlAdminister oxygenAdminister oxygen IV of crystalloid solutionIV of crystalloid solutionDopamine for blood pressure Dopamine for blood pressure
supportsupportMonitor other vitalsMonitor other vitals

Anaphylatic ShockAnaphylatic ShockSevere immune response to Severe immune response to
foreign substanceforeign substanceS/S most often occur within S/S most often occur within
minutes but can take up to minutes but can take up to hours to occurhours to occur
The faster the reaction develops The faster the reaction develops the more severe it is likely to bethe more severe it is likely to be
Death will occur if not treated Death will occur if not treated promptlypromptly

S/S of Anaphylactic ShockS/S of Anaphylactic Shock
SkinSkin
- Flushing- Flushing
- Itching- Itching
- Hives- Hives
-Swelling-Swelling
-Cyanosis-Cyanosis

S/S of Anaphylactic ShockS/S of Anaphylactic Shock
Respiratory SystemRespiratory System
- Breathing difficulty- Breathing difficulty
- Sneezing, Coughing- Sneezing, Coughing
- Wheezing, Stridor- Wheezing, Stridor
- Laryngeal edema- Laryngeal edema
- Laryngospasm- Laryngospasm

S/S of Anaphylactic ShockS/S of Anaphylactic Shock
Cardiovascular SystemCardiovascular System
- Vasodilation- Vasodilation
- Increased heart rate- Increased heart rate
- Decreased blood pressure- Decreased blood pressure

S/S of Anaphylactic ShockS/S of Anaphylactic Shock
Gastrointestinal SystemGastrointestinal System
- Nausea, vomiting- Nausea, vomiting
- Abdominal cramping- Abdominal cramping
- Diarrhea- Diarrhea

TX for Anaphylactic ShockTX for Anaphylactic Shock
Airway protection which may include Airway protection which may include Endotracheal IntubationEndotracheal Intubation
Establish IV with crystalloid solutionEstablish IV with crystalloid solution Pharmacological interventions: Pharmacological interventions:
Epinephrine, Antihistamines(Benadryl), Epinephrine, Antihistamines(Benadryl), Corticosteroids(dexamethasone), Corticosteroids(dexamethasone), Vasopressors(dopamine, Epinephrine), Vasopressors(dopamine, Epinephrine), and inhaled beta agonist(albuterol)and inhaled beta agonist(albuterol)