Embed Size (px)
Citation preview
Welcome to the 6th Annual ACMA Kentucky / Tennessee Chapter
Case Management Conference
© 3M 2012. All rights reserved. Confidential and Proprietary.
3M Health Information Systems The ICD-10 Coding System & Impact on CM/SW/UM
ACMA KY/TN Chapter Education
Joyce Mosier, MBA, RN, CPHQ, ACM September 6, 2012
2
Objectives
Explain the premise of ICD-10-CM/PCS ICD-10 impact for Case Management, Social Work and Utilization
Management Assess ways Case Management, Utilization Management and Social
Work can benefit from this system
3M Health Information Systems 3M Health Information Systems
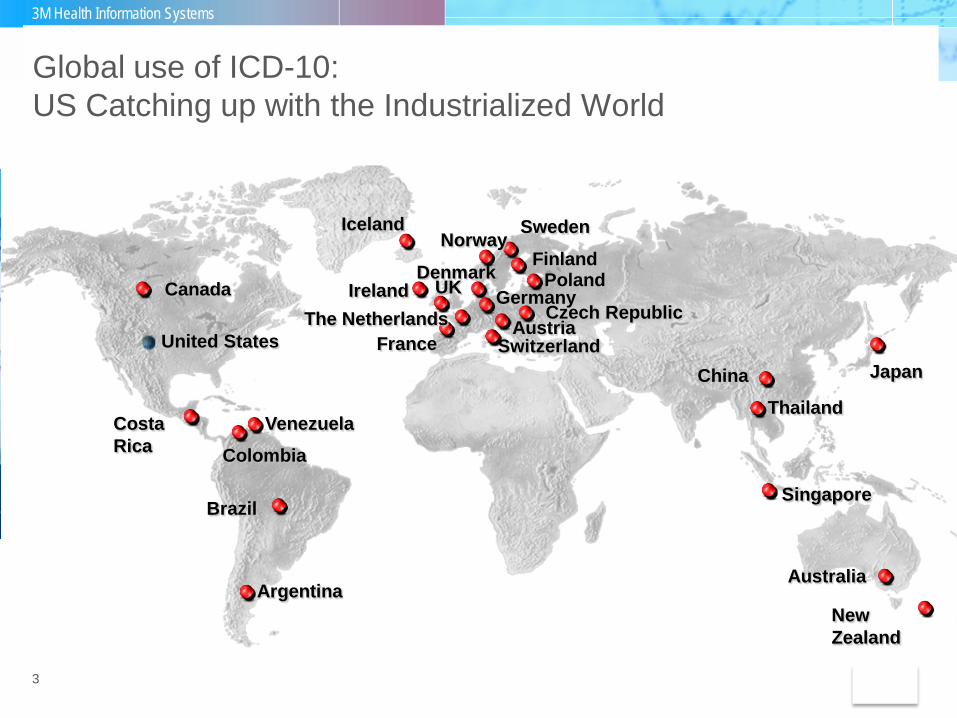
Global use of ICD-10: US Catching up with the Industrialized World
Poland
Thailand
United States
Iceland
Denmark
Brazil
New Zealand
Argentina
Austria
Norway
Australia
Finland
Singapore
Canada
Sweden
China Japan
Venezuela
Germany
Switzerland
Colombia
UK Ireland Czech Republic The Netherlands
France
Costa Rica
3
Overview
The United States has been using ICD-9-CM since 1979 and is the last industrialized nation to move to ICD-10.
On January 16, 2009, CMS published final rule CMS-0013-F mandating the
adoption of the ICD-10-CM and ICD-10-PCS code sets to replace ICD-9-CM under HIPAA.
The original compliance date for implementation was October 1, 2013,
however CMS has announced a delay for some entities--the date of implementation is pending.
The delay allows more time for hospitals and physicians to prepare for the
ICD-10 transition.
4
The Need for ICD-10
The ICD-9-CM code set is 30+ years old.
ICD-9 is no longer supported or maintained by the World Health Organization (ICD-10 was adopted by WHO in 1990).
Difficulty in assigning new codes Many chapters of ICD-9-CM are full Valuable new codes are not implemented due to insufficient space.
ICD-9 is not able to provide sufficient codes for healthcare encounters for
reasons other than disease (e.g. preventive care). Terminology often insufficient, obsolete and inconsistent with current medical practice and the medical technology being developed and in use today.
ICD-9-CM does not meet all HIPAA requirements for adopted standards.
5
Federal Register January 16, 2009
The Need for ICD-10
ICD-10 is needed to obtain full benefit for: Updated medical terminology more consistent with the 21st century Tracking of diseases/procedures/preventative care Better measuring of quality outcomes - Improved data allows for more
accurate severity of illness and risk of mortality data for profiling Data exchange Full use of HIT tools and technology (e.g. computer assisted coding ,
computer assisted coding for clinical documentation improvement, computer assisted coding for physician documentation)
Better specificity of medical necessity criteria Improved data allows for more accurate reimbursement for services
provided Procedure coding system allows for expansion and addition of new
technology
7
Requirements for ICD-10-CM and ICD-10 PCS
Use of ICD-10-CM and ICD-10-PCS applies to all covered entities (health care providers, health plans, and healthcare clearing houses) that transmit electronic data based on the Health Insurance Portability and Accountability Act (HIPAA) transaction standards.
ICD-10-PCS codes are only required to be used by hospitals to report
inpatient procedures.
CPT codes will continue to be used for outpatient and physician billing. However, some entities (hospitals, ambulatory surgery centers, etc) are choosing
to assign ICD-10- PCS codes in their ambulatory settings even though it is not mandated..
8
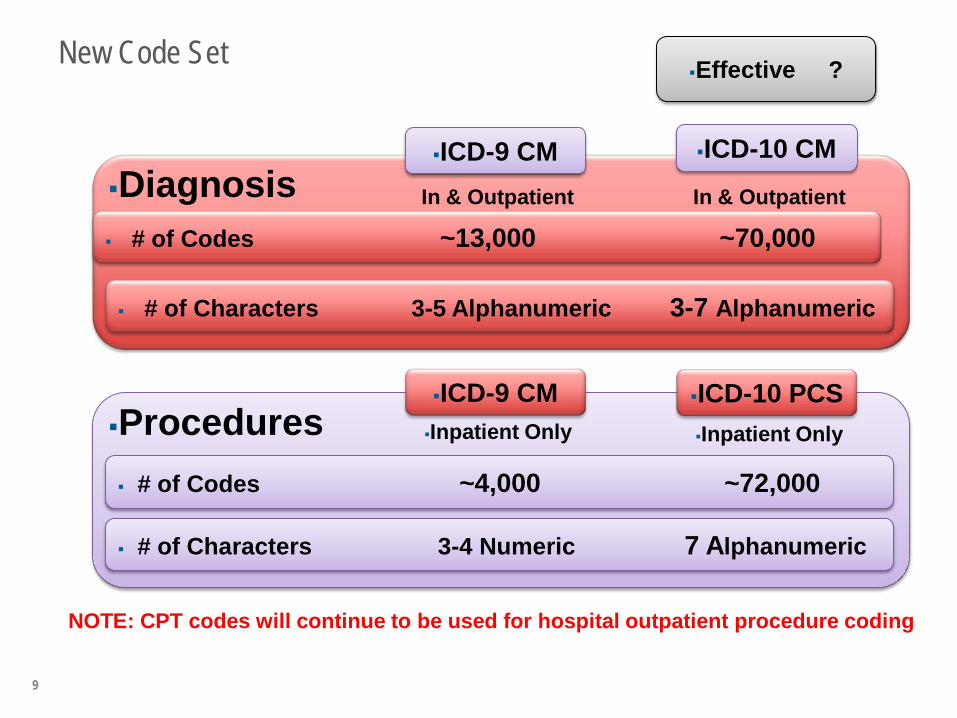
New Code Set
9
Diagnosis ICD-9 CM ICD-10 CM
In & Outpatient In & Outpatient
# of Codes ~13,000 ~70,000
# of Characters 3-5 Alphanumeric 3-7 Alphanumeric
Procedures ICD-9 CM ICD-10 PCS Inpatient Only Inpatient Only
# of Codes ~4,000 ~72,000
# of Characters 3-4 Numeric 7 Alphanumeric
NOTE: CPT codes will continue to be used for hospital outpatient procedure coding
Effective ?
3M Health Information Systems
ICD-10-CM – Diagnosis Coding
10
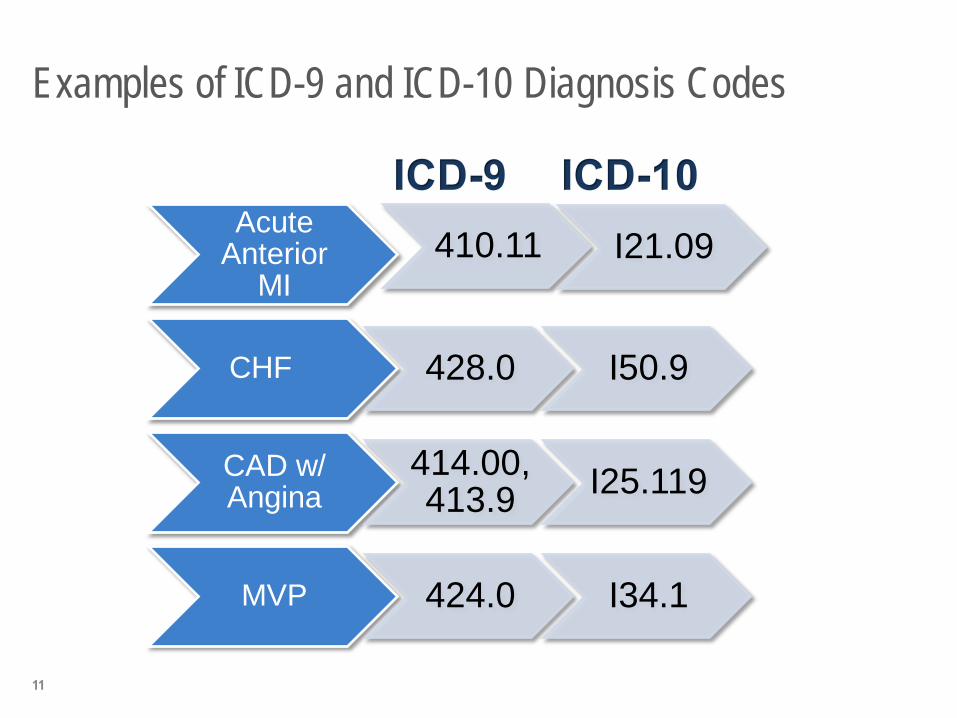
Examples of ICD-9 and ICD-10 Diagnosis Codes
Acute Anterior
MI 410.11 I21.09
CHF 428.0 I50.9
CAD w/ Angina
414.00, 413.9 I25.119
MVP 424.0 I34.1
11
Myocardial infarction Documentation will need to include:
• Type of infarction • STEMI • NSTEMI
• Age of infarction • If within 4 weeks coded as initial • If older than 4 weeks coded as “old”
• Specific site of myocardium involved • anterior wall • inferior wall
• Coronary artery involved • Information regarding treatment - initial or subsequent MI
Documentation for Cardiology/Cardiothoracic Diagnoses
12
13
Unique ICD-10-CM Guidelines Circulatory System
Acute Myocardial Infarctions (AMI) are identified by the site of the infarction along with the coronary artery involved.
The acute phase of the AMI is within 4 weeks of onset.
If a patient suffers a subsequent AMI within 4 weeks, a code for both
conditions is used, and sequencing depends on the reason for admission.
Note the change in the age of the MI. In ICD-9-CM it was 8 weeks. In ICD-
10-CM it is 4 weeks. • Think about past data comparing subsequent MI prevalence to current
episodes of subsequent MI occurrence. What impact might that have on data assessment of related outcomes?
A combination (single) code identifies both ASHD or CAD and angina.
14
Documentation Changes
Combination codes - In some cases a single code has been established to classify: 2 diagnoses A diagnosis with a manifestation or secondary process A diagnosis with a complication
Examples: Pathological compression fracture of the vertebrae due to osteoporosis, initial visit -
M80.08xA Type 2 DM with gastroparesis – E11.43 Stage III Pressure Ulcer R. Heel – L89.613 CAD with unstable angina – I25.110 Diverticulitis, large intestine with perforation, abscess and bleeding – K57.21
Documentation for Cardiology/Cardiothoracic Diagnoses
Hypertension HTN and chronic kidney disease are assumed to be a causal relationship;
however, it is important to document the stage of the CKD HTN and heart disease are not assumed to be linked and must be documented
when related. It is also important to state if heart failure is present. Examples include: Heart disease due to hypertension Hypertensive heart disease Hypertensive heart disease and CKD with heart failure and Stage 4 CKD
CHF
Specify acuity - acute , chronic or acute on chronic Specify type - systolic and/or diastolic heart failure Specify if CHF is a manifestation of another etiology (cardiomyopathy, HTN
heart disease, renal failure) The above documentation rules are the same in ICD-9- CM today; however this
remains an area of poor compliance
15
Renal Diseases
Chronic Kidney Failure is assigned by Stage in both ICD-9 and ICD-10. Stage I Stage II Stage III Stage IV Stage V ESRD
Acute Kidney Failure is reported based on cause in both ICD-9 and ICD-10 (eg. Acute Kidney Failure due to tubular necrosis)
16
Dementia Dementia is classified by type, or relationship to other disease processes: Alzheimer’s Dementia
Early or late onset Dementia with or without behavioral disturbances
Aggressive behavior Combative behavior Violent behavior Wandering off
Vascular or Multi-Infarct Dementia Alcohol or drug induced Dementia Dementia with Lewy Bodies or Parkinson’s Pick’s Disease with Dementia
17
Examples of Documentation Requirements
In ICD-10, respiratory failure no longer defaults to acute. Physician must specify if acute, chronic or acute on chronic
Respiratory Failure Specify acuity - acute, chronic or acute on chronic Document if respiratory failure is due to a specify etiology
Respiratory failure is assigned as a combination code that not only details the
severity of respiratory failure, but also association with hypoxia or hypercapnia. Hypoxia – insufficient oxygen reaching the tissue Hypercapnia – excess carbon dioxide in the blood
18
Examples of Documentation Requirements Asthma
Specify severity type as mild intermittent mild persistent moderate persistent or severe persistent
Specify status of asthma - uncomplicated, with acute exacerbation, or with status asthmaticus
Specify if the patient has any other diseases associated with asthma (COPD, bronchitis, etc.)
COPD
Specify if acute component such as exacerbation, bronchitis or lower respiratory infection
Specify if oxygen dependent Specify if in chronic respiratory failure
If Asthma and COPD are reported together, they are coded separately in ICD-10.
19
Pneumonia – Core Measure Diagnosis Pneumonia is classified by type and linked to the organism in both ICD-9 and
ICD-10. Types of pneumonia: Lobar pneumonia Aspiration pneumonia Pneumonia with influenza Pneumonia due to bacteria Viral pneumonia Organizing pneumonia Hypostatic pneumonia Bronchopneumonia
In ICD-10-CM is there no specific code for ‘isolation’ or for flu shots. If running data related to number of patients over certain age or with specific diagnoses to see if they had a flu shot, proactively assigning an indicator may be needed.
20
Anemia
Anemia in both ICD-9 and ICD-10 can be classified by specific type or cause Anemia due to malignancy – anemia is principal diagnosis in ICD-9-CM. In
ICD-10-CM it is secondary and the malignancy is principal. Take this into consideration if running data for quality or readmission
reports.
21
3M Health Information Systems
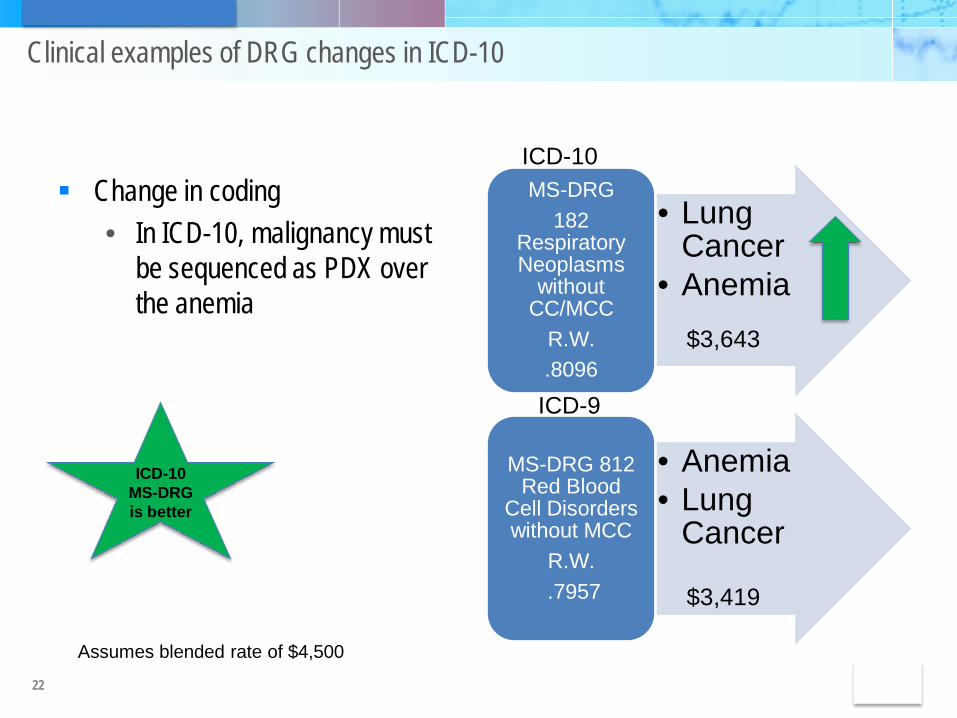
Clinical examples of DRG changes in ICD-10
Change in coding • In ICD-10, malignancy must
be sequenced as PDX over the anemia
• Lung Cancer
• Anemia
MS-DRG 182
Respiratory Neoplasms
without CC/MCC
R.W. .8096
• Anemia • Lung
Cancer
MS-DRG 812 Red Blood
Cell Disorders without MCC
R.W. .7957
22
ICD-10
ICD-9
ICD-10 MS-DRG is better
Assumes blended rate of $4,500
$3,643
$3,419
Unique ICD-10-CM Guidelines
Dominant/Nondominant Hemiplegia and monoplegia codes have a digit to identify dominant versus
nondominant side. If unspecified, the default code is dominant.
Glasgow coma scale In a Traumatic Brain Injury or sequela of a CVA, the Glasgow coma scale
can be coded along with the condition to more accurately reflect the patient’s condition
Musculoskeletal Conditions in the musculoskeletal system involving bone, joint or muscle
are reported by type and cause and have specific designations for site and laterality
23
Injuries, Poisoning, Adverse Effects, Underdosing and Toxic Effects Injuries and poisonings, adverse effects, underdosing and toxic effects – For many of
the codes related to these diagnoses there is a character within the code to denote the episode of care for which the condition is being treated – the encounters with their associated characters are: A = initial encounter D = subsequent encounter S = sequela
In ICD-9 levels of the spinal cord were grouped while in ICD-10 there is specificity for levels.
Example: Each cervical level is identified. Thoracic levels have T1 separate and others grouped: T2 – T6, T7 – T10, T11 –
T12. Fractures have a unique 7th character extension which indicates open or closed
fracture, initial or subsequent encounter with delayed healing, malunion or nonunion.
24
Injuries, Poisoning, Adverse Effects, Underdosing and Toxic Effects continued
Underdosing is new in ICD-10-CM Codes for taking less of a drug, medicament or biological substance have
been added to the Table of Drugs and Chemicals Specificity exists for intentional or unintentional.
No funds? No access to medications? Taking less than prescribed?
25
3M Health Information Systems
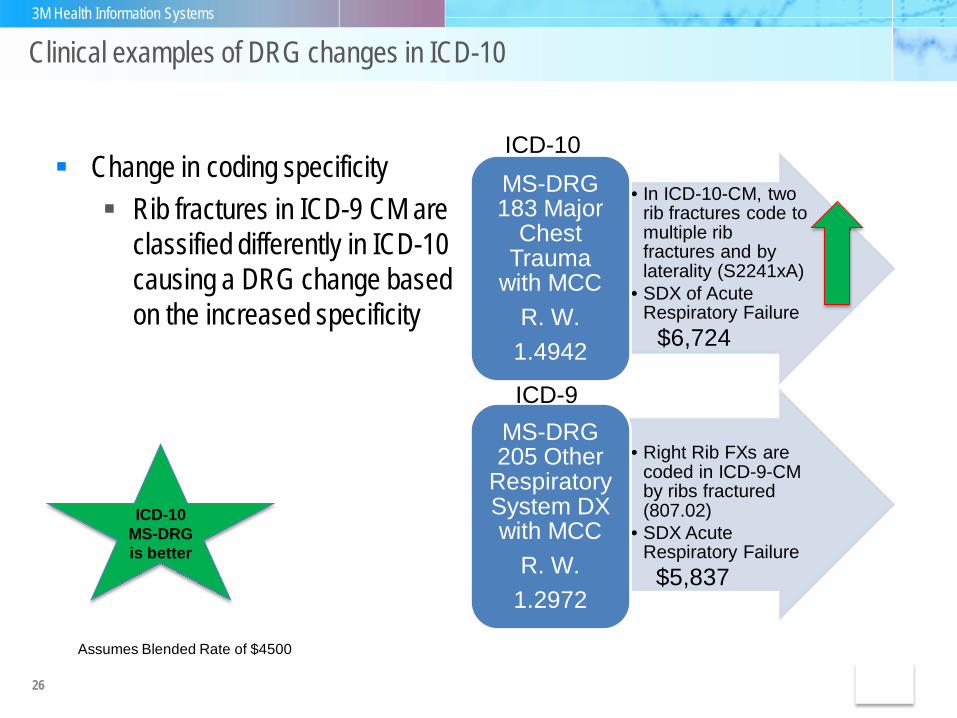
Clinical examples of DRG changes in ICD-10
• In ICD-10-CM, two rib fractures code to multiple rib fractures and by laterality (S2241xA)
• SDX of Acute Respiratory Failure
MS-DRG 183 Major
Chest Trauma
with MCC R. W.
1.4942
• Right Rib FXs are
coded in ICD-9-CM by ribs fractured (807.02)
• SDX Acute Respiratory Failure
MS-DRG 205 Other
Respiratory System DX with MCC
R. W. 1.2972
Change in coding specificity Rib fractures in ICD-9 CM are
classified differently in ICD-10 causing a DRG change based on the increased specificity
26
ICD-10
ICD-9
ICD-10 MS-DRG is better
$6,724
Assumes Blended Rate of $4500
$5,837
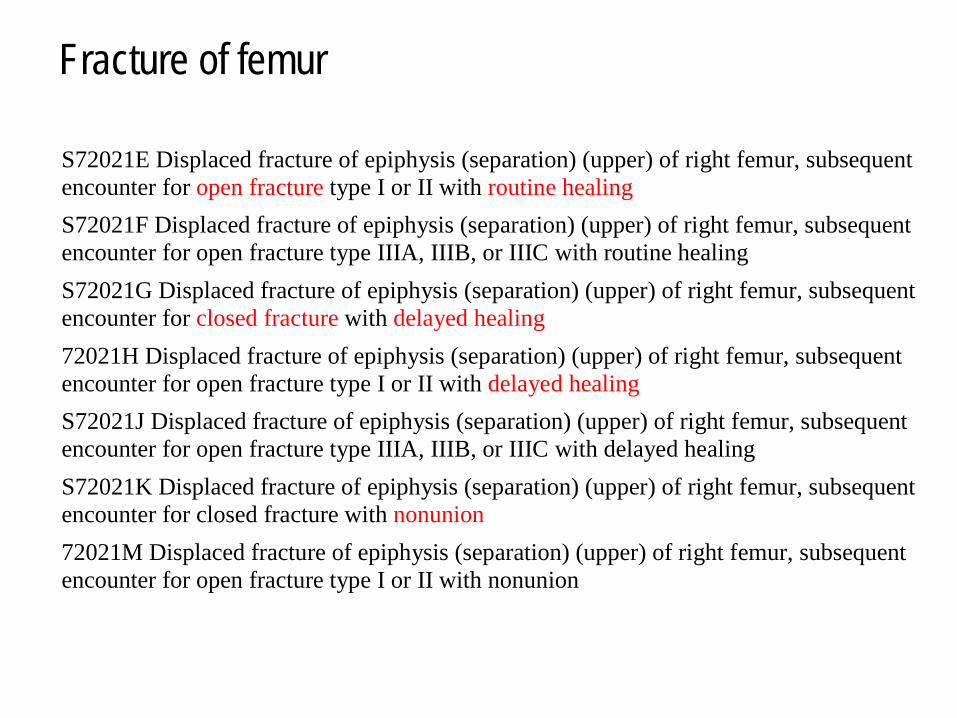
Fracture of femur
S72021E Displaced fracture of epiphysis (separation) (upper) of right femur, subsequent encounter for open fracture type I or II with routine healing S72021F Displaced fracture of epiphysis (separation) (upper) of right femur, subsequent encounter for open fracture type IIIA, IIIB, or IIIC with routine healing S72021G Displaced fracture of epiphysis (separation) (upper) of right femur, subsequent encounter for closed fracture with delayed healing 72021H Displaced fracture of epiphysis (separation) (upper) of right femur, subsequent encounter for open fracture type I or II with delayed healing S72021J Displaced fracture of epiphysis (separation) (upper) of right femur, subsequent encounter for open fracture type IIIA, IIIB, or IIIC with delayed healing S72021K Displaced fracture of epiphysis (separation) (upper) of right femur, subsequent encounter for closed fracture with nonunion 72021M Displaced fracture of epiphysis (separation) (upper) of right femur, subsequent encounter for open fracture type I or II with nonunion
28
Unique ICD-10-CM Guidelines
Diabetes (E08 – E13) A combination code identifies the type of diabetes, the associated
complication or manifestation and the body system involved. Inadequately controlled, out of control and poorly controlled
are coded to Diabetes, by type, with hyperglycemia. If the type of diabetes is indicated as secondary to another disease
process or a drug, then that diabetic code is listed as secondary to the underlying cause
Most frequent MCC/CC changes within ICD-10
Diagnoses that are no longer MCC/CCs in ICD-10 MS-DRGs Esophageal Hemorrhage (no longer a MCC) Type II Diabetic Ketoacidosis (no longer a MCC) Malignant HTN (no longer a CC) Non-healing surgical wound (no longer a CC) Schizoaffective Disorders, Specified types (no longer a CC) Major Depression, NOS (no longer a CC) Code 403.00, Mal HTN w/ CKD (no longer a CC) Hemorrhage into bladder wall (596.7) is a CC in I-9 (no longer
a CC)
29
Most frequent MCC/CC changes within ICD-10
Diagnoses that are CCs in ICD-10 MS-DRGs but are not in ICD-9: • Bi-fasicular Block(s)—Example: 426.52 (RBB/LAFB) is not a CC in
ICD-9, but I452 is a CC in ICD-10. • Concussion, Unspecified and Unspecified Duration of LOC is a CC
in ICD-10. • 344.61 Cauda Equina is not a CC in ICD-9 but G834 is a CC in
ICD-10. • Code 136.1 Behcet Syndrome (type of vasculitis) is not a CC in
ICD-9 but is a CC in ICD-10 (M352).
30
3M Health Information Systems
ICD-10-PCS - Procedure Coding System
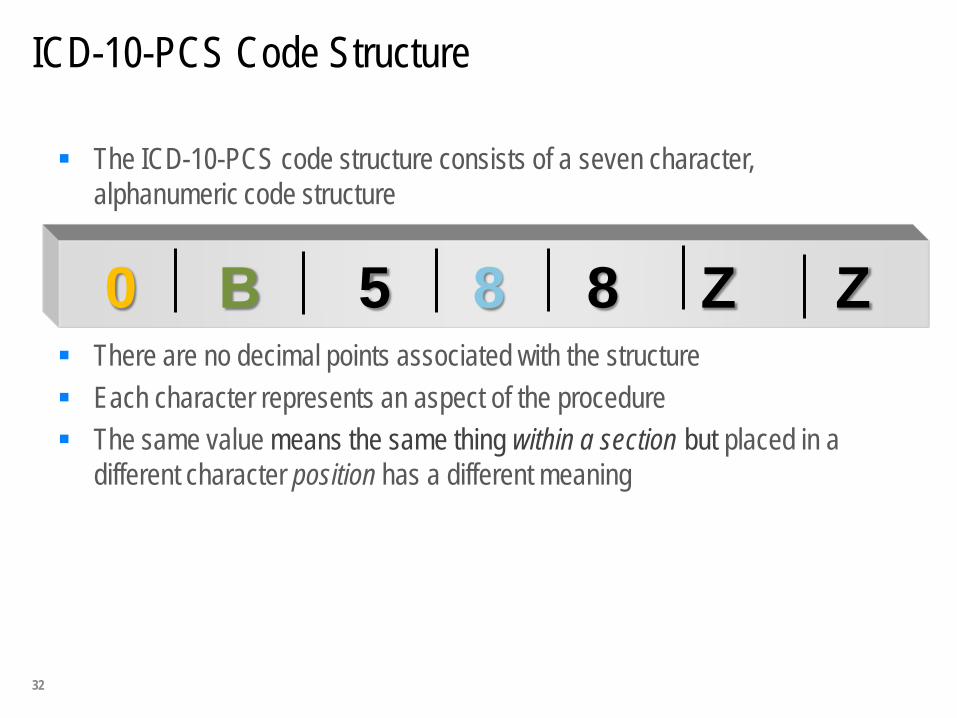
ICD-10-PCS Code Structure
The ICD-10-PCS code structure consists of a seven character, alphanumeric code structure
Letters O and I are not used to in order to avoid confusion with the numbers 0 and 1
There are no decimal points associated with the structure Each character represents an aspect of the procedure The same value means the same thing within a section but placed in a
different character position has a different meaning
0 B 5 8 8 Z Z
32
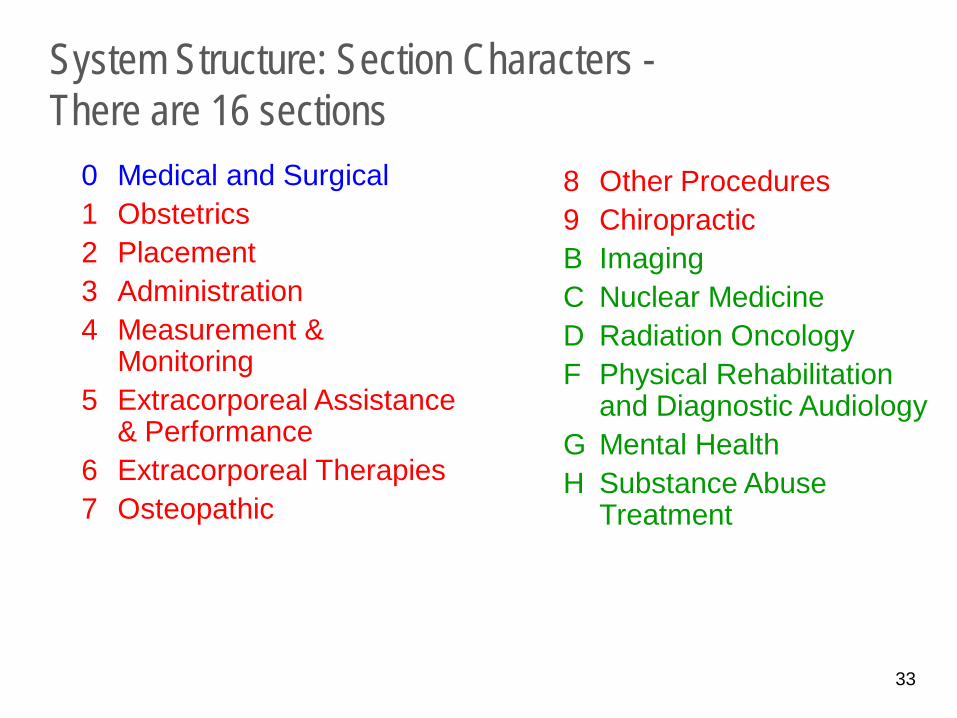
System Structure: Section Characters - There are 16 sections
0 Medical and Surgical 1 Obstetrics 2 Placement 3 Administration 4 Measurement &
Monitoring 5 Extracorporeal Assistance
& Performance 6 Extracorporeal Therapies 7 Osteopathic
8 Other Procedures 9 Chiropractic B Imaging C Nuclear Medicine D Radiation Oncology F Physical Rehabilitation
and Diagnostic Audiology G Mental Health H Substance Abuse
Treatment
33
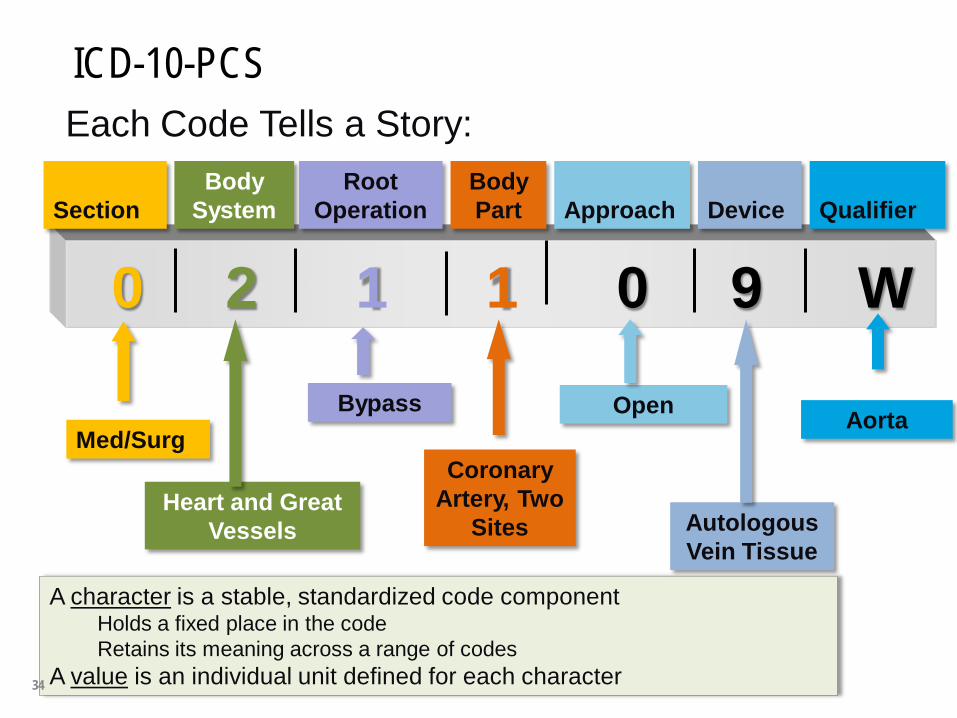
A character is a stable, standardized code component Holds a fixed place in the code Retains its meaning across a range of codes
A value is an individual unit defined for each character
0 2 1 1 0 9 W
Med/Surg
Heart and Great Vessels
Bypass
Coronary Artery, Two
Sites
Open
Autologous Vein Tissue
Aorta
Each Code Tells a Story: Section
Body System
Root Operation
Body Part
Approach
Device
Qualifier
ICD-10-PCS
34
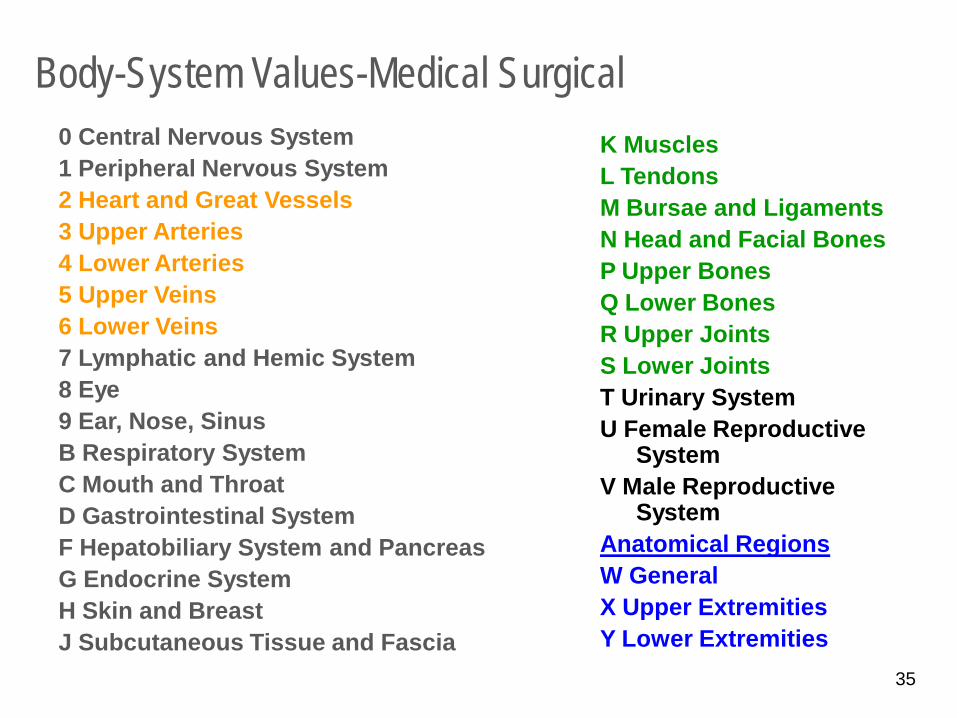
Body-System Values-Medical Surgical 0 Central Nervous System 1 Peripheral Nervous System 2 Heart and Great Vessels 3 Upper Arteries 4 Lower Arteries 5 Upper Veins 6 Lower Veins 7 Lymphatic and Hemic System 8 Eye 9 Ear, Nose, Sinus B Respiratory System C Mouth and Throat D Gastrointestinal System F Hepatobiliary System and Pancreas G Endocrine System H Skin and Breast J Subcutaneous Tissue and Fascia
K Muscles L Tendons M Bursae and Ligaments N Head and Facial Bones P Upper Bones Q Lower Bones R Upper Joints S Lower Joints T Urinary System U Female Reproductive
System V Male Reproductive
System Anatomical Regions W General X Upper Extremities Y Lower Extremities 35
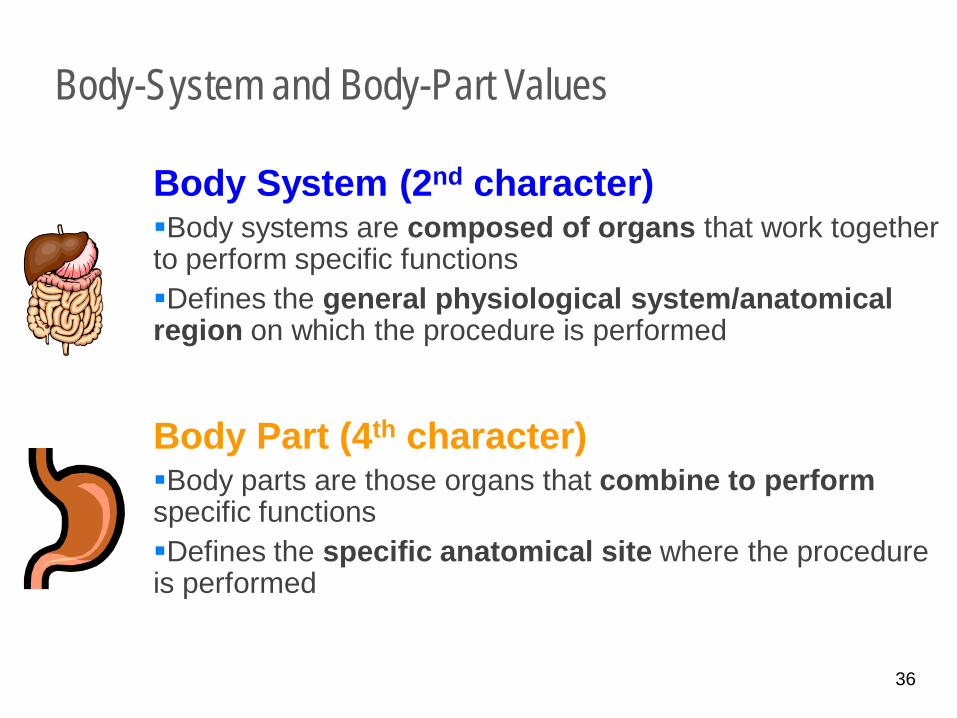
Body-System and Body-Part Values
Body System (2nd character) Body systems are composed of organs that work together to perform specific functions Defines the general physiological system/anatomical region on which the procedure is performed Body Part (4th character) Body parts are those organs that combine to perform specific functions Defines the specific anatomical site where the procedure is performed
36
Uniqueness of ICD-10 PCS
Procedures: Anatomically Driven
ICD-10 –PCS is more anatomically specific than ICD-9 CM procedures codes
Device characteristics (examples) Autologous vein or artery tissue Synthetic substitute Nonautologous tissue substitute Drug eluting intraluminal device Intraluminal device Zooplastic Tissue Implantable heart assist system External heart assist system
37
Uniqueness of ICD-10 PCS Procedures require: Laterality of site
Specificity of approach Open Percutaneous Percutaneous endoscopic Via natural or artificial opening Via natural or artificial opening endoscopic Open with percutaneous endoscopic assistance External
38
Root operations Coders are required to know the root operation definitions and apply them
accurately. Physicians are not required to know the root operation definitions and should
not be queried. Example root operations in Medical / Surgical section: Control – Stopping, or attempting to stop, postprocedural bleeding. Destruction – Physical eradication of all or a portion of a body part by the
direct use of energy, force, or a destructive agent. Detachment – Cutting off all or part of the upper or lower extremities Drainage – Taking or letting out fluids and/or gases from a body part. The qualifier ‘diagnostic’ is used to identify drainage procedures that are
diagnostic.
39
Root Operation Examples continued
Extirpation – Taking or cutting out solid matter from a body part. Example: Thrombectomy.
Excision – Cutting out or off, without replacement, a portion of a body part. The qualifier ‘diagnostic’ is used to identify excision procedures that are
diagnostic. Resection – Cutting out or off, without replacement, all of a body part. Repair – Restoring, to the extent possible, a body part to its normal anatomic
structure and function. Reposition – Moving to its normal location or other suitable location all or a
portion of a body part. Example: fracture reduction. Removal – Taking out or off a device from a body part. Replacement – Putting in or on a biological or synthetic material that
physically takes the place and/or function of all or a portion of a body part. Example: Total hip replacement.
40
PCS Section for Bypass
Bypass – Altering the route of passage of the contents a tubular body part. Cardiology bypass – body part is the number of distinct sites bypassed
“to” rather than the name of the vessel. The qualifier captures the origin “from” of the bypass
Example: Two vessel CABG using the right internal mammary artery.
Other bypasses – body part is the origin “from” of the bypass. The qualifier captures the body part bypassed “to”.
Examples: Transverse colon to cutaneous (colostomy to skin) Right femoral artery to right popliteal artery Tracheostomy is trachea to cutaneous Stomach to jejunum
41
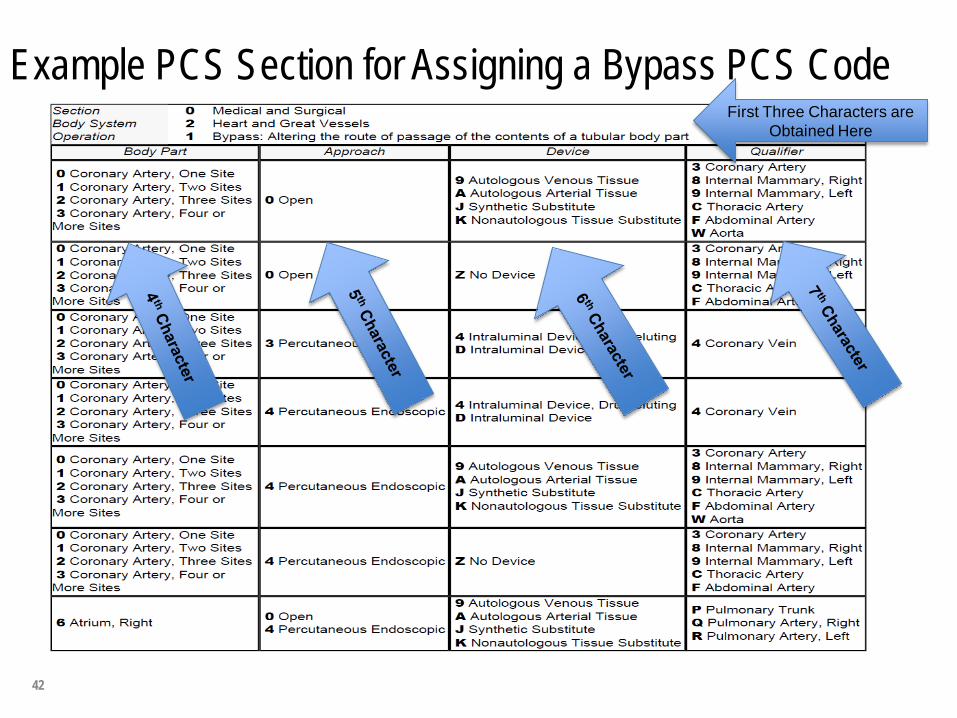
Example PCS Section for Assigning a Bypass PCS Code First Three Characters are
Obtained Here
42
Coronary Bypass Coding Guideline B3.6b Coronary arteries are classified by number of distinct sites treated, rather than number
of coronary arteries or anatomic name of a coronary artery (e.g., left anterior descending). Coronary artery bypass procedures are coded differently than other bypass procedures as described in the previous guideline. Rather than identifying the body part bypassed from, the body part identifies the number of coronary artery sites bypassed to, and the qualifier specifies the vessel bypassed from. Example: Aortocoronary artery bypass of one site on the left anterior descending
coronary artery and one site on the obtuse marginal coronary artery is classified in the body part axis of classification as two coronary artery sites and the qualifier specifies the aorta as the body part bypassed from.
B3.6c If multiple coronary artery sites are bypassed, a separate procedure is coded for each
coronary artery site that uses a different device and/or qualifier. Example: Aortocoronary artery bypass and internal mammary coronary artery
bypass are coded separately.
43
3M Health Information Systems
44
45
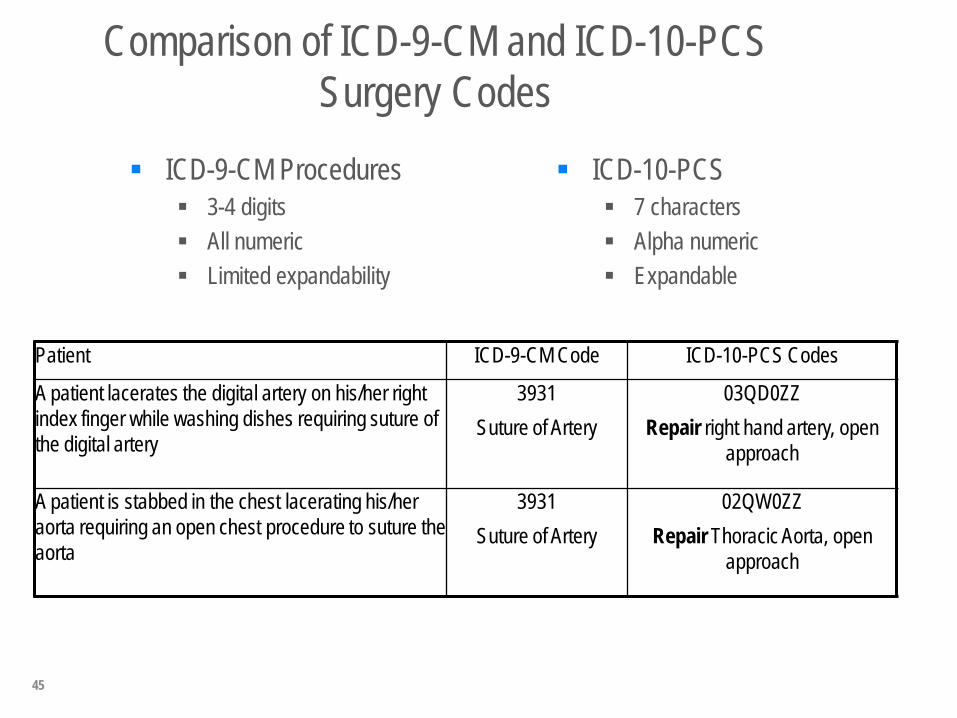
Comparison of ICD-9-CM and ICD-10-PCS Surgery Codes
ICD-9-CM Procedures 3-4 digits All numeric Limited expandability
ICD-10-PCS 7 characters Alpha numeric Expandable
Patient ICD-9-CM Code ICD-10-PCS Codes
A patient lacerates the digital artery on his/her right index finger while washing dishes requiring suture of the digital artery
3931 Suture of Artery
03QD0ZZ Repair right hand artery, open
approach
A patient is stabbed in the chest lacerating his/her aorta requiring an open chest procedure to suture the aorta
3931 Suture of Artery
02QW0ZZ Repair Thoracic Aorta, open
approach
46
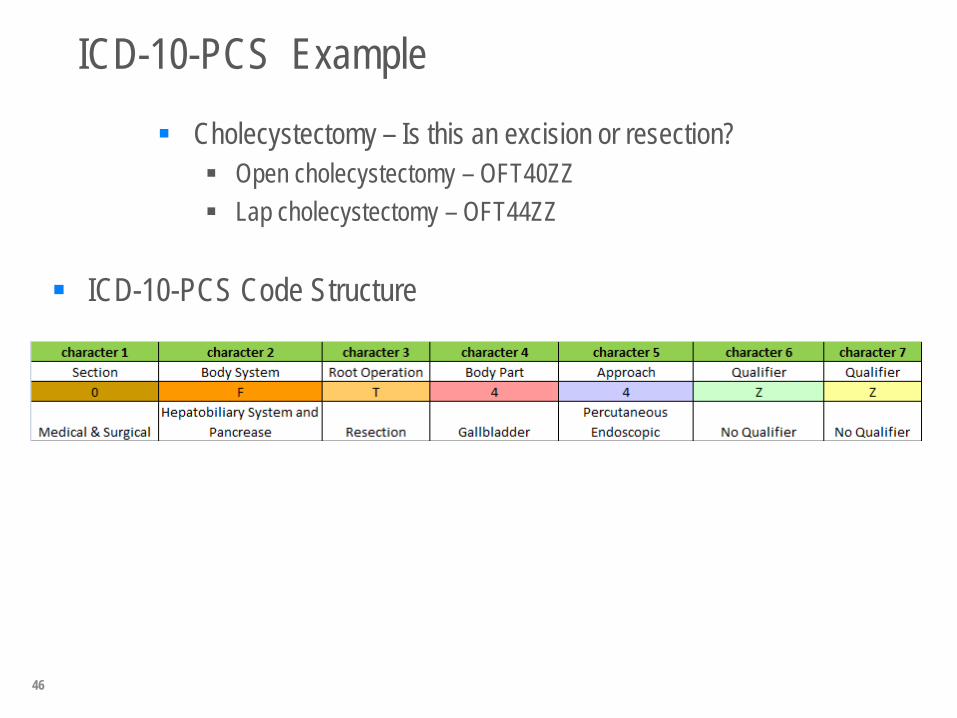
ICD-10-PCS Example
Cholecystectomy – Is this an excision or resection? Open cholecystectomy – OFT40ZZ Lap cholecystectomy – OFT44ZZ
ICD-10-PCS Code Structure
Node biopsy If an ultrasound guided fine needle biopsy of a lymph node is done, the root
operation is drainage – taking or letting out fluids and/or gases from a body part. The qualifier diagnostic is used to identify drainage procedures that are biopsies.
If one or more lymph nodes are removed but less than the entire chain, the root operation is excision – cutting out or off, without replacement, a portion of a body part. The qualifier diagnostic is used to identify drainage procedures that are biopsies. Example: 07B53ZX Excision right axillary lymphatic percutaneous approach
diagnostic
If the entire chain is removed the root operation is resection – cutting out or off, without replacement, all of a body part. No qualifier for diagnostic is used. Example: 07T60ZZ – Resection left axillary lymphatic via open approach
Documentation detail on forms
Administration of blood products Specificity is required for
Site – peripheral vein, central vein, peripheral artery or central artery Donor type – as autologous or non-autologous
Ventilator assistance - are forms clear with start time and end time, when
weaning is in progress? ICD-10-CM/PCS delineates time as <24 consecutive hours, 24-96
consecutive hours and > 96 consecutive hours. The chart must be clear with the start and end times.
Where are the gaps today?
Largest gaps identified from readiness assessment roadmaps: • Budgetary needs • IT remediation • Lack of physician documentation • Impact to coding/CDI productivity Plans to dual code prior to October 2014
• Training and education of coding/CDI staff and physicians • Need for assistance in translating ICD-9 codes into
ICD-10 codes
49
Common Question- What is the Impact to Reimbursement??
Here is what we know today: The ICD-10 version of MS-DRGs posted on the CMS website replicates the ICD-9
version of the MS-DRGs (subject to change between now and implementation date) The posted version of ICD-10 version MS-DRGs is unlikely to cause a
significant redistribution of payments across hospitals Once sufficient data code in ICD-10-CM/PCS becomes available, CMS will
likely use the increased specificity of ICD-10-CM/PCS to enhance the MS-DRGs
If hospitals are losing money in current MS-DRG’s with ICD-9-CM coding and the lack of higher specificity/documentation they will continue to lose money under ICD-10-CM/PCS
Payers have not stated they will remain budget neutral Payer market is very active and ahead of provider market in preparing for ICD-
10-CM/PCS
50
Impact on Hospitals
Hospitals and Physicians will be required to undertake significant planning efforts for ICD-10 implementation, budgeting for capital and anticipated operational expenses, a complete systems inventory and development of educational activities to prepare staff.
The implementation of ICD-10 will impact every:
Paper and software system Information system Functional department
Scheduling – preauthorization & medical necessity Admission Physician/Clinical Care Case Management Lab, Radiology and other Ancillary areas Transcription Performance management HIM Department & HIM system Billing and Accounting Contract management Payer relationships Data warehouse
51
Impact on Clinical Providers
Clinical provider documentation is the foundation of ICD-10 specificity; incomplete documentation will impede ability to code accurately.
Physicians and other Clinicians will need to undergo training to learn about the
detailed documentation that ICD-10 requires of them. Training will need to be general awareness as well as specialty-based.
Clinical providers will need to collaborate closely with the HIM Coding and the Clinical Documentation Improvement teams.
Changes may need to be made to existing systems and processes such as clinical documentation, practice management systems, electronic billing systems, and encounter forms/superbills.
52
Impact to Clinical Documentation Improvement Team
If your hospital has a Clinical Documentation Improvement Team, the CDI specialists (CDIS) will need to be trained on the detailed documentation requirements for ICD-10.
A CDI team can be instrumental in working with clinicians/physicians to ensure
the specificity and level of detail needed to support ICD-10 is captured in the clinicians’ medical record documentation.
Existing CDI program may only touch Medicare; ICD-10 is across all payers.
53
Impact on Coding Staff
Coding Staff will need to be extensively trained to become fully proficient in ICD-10 coding. Educational requirements will differ based on the coder’s responsibility.
Coding Staff will need to have a deeper knowledge of the biomedical sciences than was required under ICD-9-CM. Specifically in the areas of: anatomy and physiology pathophysiology pharmacology medical terminology
In addition, staff need better comprehension of operative and procedure reports.
Contrast for radiology or cardiology services Some ICD-10-PCS code descriptions for imaging procedures include the type of
contrast utilized. Example: Arteriogram of left vertebral artery
54
Summary
Physician offices and ambulatory care will continue to use CPT for procedural codes.
Hospitals will team with physicians to query when more documentation is
needed. Physician engagement and responsiveness to queries will assist in
capturing the most accurate coding of the patient’s acuity and outcomes.
ICD-10 will require further documentation of specificity of diseases by all entities (inpatient, extended care facilities, physician offices or clinics). Physician offices will be impacted most in the area of medical necessity
and need to provide specified diagnoses, diagnostics, and care.
55
Summary continued
Case Management, Social Services and Utilization Management will be impacted in the area of medical necessity and the process to authorize/precert services, (OR case boarded with use of CPT code or ICD10-PCS?) obtaining readmission data, tracking avoidable day data, facilitating transfer to post discharge care providers, evaluating patients for transfer to another facility with awareness of reimbursement impacted by transfer, and tracking quality indicators.
CM/SW/UM can benefit from more specific data to establish screening priority
for discharge planning, assess outlier trends, quality issues, readmission drivers, medical necessity roadblocks.
56
Questions?
Queries?
Confabulation?
Wishful thinking?
Hopeful outcomes?
57