Embed Size (px)
Citation preview

2 JOPA
Journal Mission The Journal of Orthopedics for Physician Assistants (JOPA) is an academic resource created to
deliver ongoing orthopedic education for physician
assistants. The journal is a unique forum to share
our knowledge and experiences with colleagues in
the profession. JOPA strives to publish timely and
practical articles covering all subspecialties. Each
article is peer reviewed to ensure accuracy, clinical
relevance, and readability.
Dagan Cloutier, PA-C, Editor in Chief
Ryan Ouellette, Webmaster, thejopa.org
Charles D. Frost, DHSc, PA-C Content Editor
Spectrum Marketing, Journal Design
Orthopedic Publishing Resources, LLC, Publisher
Journal of
Orthopedics for Physician Assistants
Contents 5 MAGEC (Magnetic Expansion
Control) Spinal Bracing and
Distraction System
7 Fluoroscopic Elbow Injections
9 Writing for JOPA Information for Authors
Monthly Image Quiz Follow-up 10 Lumbar Discitis
12 Medial epicondyle avulsion fracture
13 Spondylolysis
16 Quadriceps tendon autograft for ACL reconstruction: evidence for increased utilization
22 Perceptions and Expectations
26 AASPA Quiz Corner
Disclaimer: Statements and opinions expressed in articles
are those of the authors and do not necessarily re! ect those
of the publisher. The publisher disclaims any responsibility
or liability for any material published herein. Acceptance of
advertising does not imply the publisher guarantees,
warrants, or endorses any product or service.
Physician AssistantReview Board
Marlon AlexanderRosharon, TX
Corey AndersonHarrisburg, SD
Brian BarryPortsmouth, NH
David BeckPittsburgh, PA
Heidi BolgrenEdina, MN
Ryan BrainardSavannah, GA
Afton Branton Geneva, NY
Molly BuerkAurora, CO
Mark CarboAlexandria, LA
Ray CarlsonSan Diego, CA
Jeff ChambersAthens, Georgia
Larry CollinsTampa, FL
Michael CreminsHartford, CT
Greg DeConciliisBoston, MA
Charles DowellVancouver, WA
Caitlin EagenBoston, MA
Sophie EllisVancouver, WA
Marcie FitzgeraldErie, PA
Erich Fogg
York, ME
Charles D. FrostNorfolk, VA
Bruce GallioReno, NV
Angela GrochowskiHorsham, PA
Michael Hollopeter
Houston, TX
Jennifer HartmanPeoria, AZ
Michael HarveyFishers, IN
Sean HazzardBoston, MA
Matt HenryRapid City, SD
Tim HolmstromPullman, WA
Mike HouleHartford, CT
Alan Johnston Nashua, NH
Stuart JonesBrentwood, TN
Jason KatzPhiladelphia, PA
Jill KnightSeattle, WA
Stanley KotaraLubbock, TX
Kathleen Martinelli Durham, NC
Sean MetzBuffalo, VA
Ronald McCallSpring" eld, MO
Patrick McCarthyManchester, NH
Randall PapeUSAF Academy, CO
Keith PaulGreensboro, NC
Jason RandBoston, MA
Robert RoganPoughkeepsie, NY
Scott WaltonCaribou, ME
Todd RudyWellsboro, PA
Bradford SalzmannRoyalton, VT
John J. ShaffPhoenix, AZ
Jeffrey SommersMarietta, OH
Steve Steiner Manchester, NH
Wendi Martin StewartHouston, TX
Lori TappenDallas, TX
Timothy ThompsonNaples, FL
Mary VacalaSavannah, GA
Courtney Van ArsdaleBoston, MA
Marcos VargasFlushing, MI
JOPA has teamed up with The Clinical Advisor and
the America Association of Surgical Physician
Assistants (AASPA) to provide an orthopedic
focused educational resource to all Physician
Assistants and Nurse Practitioners.
This issue is presented to you by:

MINIMAL MAXIMUMDISRUPTION
OPTIMIZING BALANCE
FEATURING
CREO MCS™ + ALTERA™
The CREO MCS™ midline cortical stabilization system and ALTERA™ steerable expandable TLIF spacer combine
to maximize cortical bone fixation and optimize sagittal balance through an MIS approach.
STABILIZATION
Learn more at www.GlobusMedical.com/ALTERA
866.456.2871
Life moves us is a registered trademark of Globus Medical, Inc.
VISIT U
S AT
NASS
BOOTH #1119

4 JOPA
Subspeciality Sections
• Hand
• Spine
• Trauma
• Arthroplasty
• Sports
• Foot andAnkle
• Pediatrics
• Tumor
All articles submitted to JOPA are reviewed
by the Editor in Chief, who is responsible for
deciding whether an article is accepted, rejected,
or in need of revision before publication. JOPA
will be forming an editorial board by subspecialty.
Each subspecialty section will be represented
by a physician assistant or section editor whose
knowledge and experience lies within the chosen
subspecialty. Each section editor will review
submitted articles within their subspecialty prior
to publication and send articles to a group of peer
reviewers who share knowledge and experience in
the subspecialty. Once peer reviewed, authors will
have the opportunity to revise their article and
re-submit for publication. This will ensure that all
articles published in JOPA are accurate, clinically
relevant, and readable. Anyone interested in joining
the editorial board should email, Dagan Cloutier,
Editor in Chief, at [email protected].
Join the JOPA Editorial BoardSubspeciality Sections
• Hand
• Spine
• Trauma
• Arthroplasty
• Sports
• Foot andAnkle
• Pediatrics
• Tumor
866.225.8839
orthocaremedical.com
866.225.8839
orthocaremedical.com
Lowest Cost DME Provider
Best Patient Outcomes
100% Customer Loyalty!
You’re in good company whenyou partner with OrthoCare!
A DME partner that strives for the highest level of satisfaction.

JOPA 5
Marcie Fitzgerald, MPAS, PA-C, DFAAPAPatrick J. Cahill, MD
growth to minimize progression of the spinal deformity2. The rod contains a small internal magnet, which
allows the rod to be lengthened non-invasively with the ERC. When the ERC is placed over the patient’s
spine, where the magnet is located, and then activated, the magnet in the implanted rod rotates and will
either distract or retract the rod.
Periodic lengthening of the rod is performed in the outpatient setting. The distraction process takes
approximately � ve minutes. After the pre-lengthening x-ray is performed, the patient is placed prone on a
non-magnetic exam table. The MAGEC Wand Magnet Locator is held vertically by the distal end of the device
and moved until it naturally aligns itself parallel with the internal magnet. After a mark is made with a pen,
the External Remote Controller is placed on the patient and positioned so the implant locating window of
the ERC is over the magnet area that was previously marked. The “distract” button is pressed and held
MAGEC (Magnetic Expansion Control) Spinal bracing and Distraction System
The latest method in the treatment of
early onset scoliosis is truly MAGical. Ellipse
Technologies, Inc. has developed a new
system with an adjustable spinal growing rod
that is able to be lengthened non-invasively
with a magnet.
The device is indicated for skeletally
immature patients less than 10 years of age
with progressive spinal deformities, (Cobb
angle of 30 degrees or more and a thoracic
spine height less than 22 cm) and those at
risk for Thoracic Insuf� ciency Syndrome
(when the thorax is unable to support normal
respiration or lung growth1. Early onset
scoliosis is de� ned as scoliosis starting the
age of 5 years or less, regardless of etiology3.
These patients are at risk for rapid curve
progression and pulmonary insuf� ciency
because thoracic growth occurs most quickly
during this time of life. Contraindications for
this type of treatment include patients with
infections or pathologic conditions where
bone density would be decreased, metal
allergies and sensitivities, pacemakers or
other active electrical devices, those less
than two years of age, fewer than 25 pounds,
and those requiring MRI imaging during the
time period of device implantation.
The device is made up of one or
two sterile spinal rods that are surgically
implanted, a hand held non-invasive ERC
(External Remote Controller), the MAGEC
Manual Distractor and the MAGEC Wand
(Magnet Locator). The surgically implanted
spinal rod is used to brace the spine during
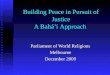
Figure 1. This is a PA spine � lm that shows the rod pre-
lengthening.

6 JOPA
until the amount of distraction previously
programmed into the ERC is complete. Once
the lengthening procedure is performed,
the patient will be escorted to the radiology
department for post-lengthening � lms. A PA
spine � lm is used to measure and con� rm the
distraction length.
Prior to this technique, patients would
be required to go to the operating room
every few months for surgical lengthening
of the rods. Studies have demonstrated a
correlation between the number of surgical
procedures performed and the increased risk
of developing a complication3. Complications
can include skin infections, hardware
problems, and neurological abnormalities.
This highly innovative device allows for non-
invasive, outpatient spinal rod lengthening.
My supervising physician was the � rst
spine surgeon to perform this procedure in
the United States, following FDA approval
in February. As a PA, I am able to perform
the lengthening procedure in the outpatient
clinic. This is bene� cial to the patients, who
no longer need to go under general anesthesia
and have an incision in the operating room to
have the rod lengthened. It can now be done
with a just touch of a button.
References
1.Ellipse Technologies, Inc. Surgical Technique Guide MAGEC Remote Control Technology for the Treatment of Spine Deformities. 2012.
2. Campbell RM, Smith MD. Thoracic Insuf� ciency Syndrome and Exotic Scoliosis. J Bone Joint Surg. 2007: 108.
3. Bess, Shay, et al. Complications of Growing-Rod Treatment
for Early-Onset Scoliosis. J Bone Joint Surg. 2010: 2533-43.
Figure 2. This is a PA spine � lm that shows the rod post-
lengthening. This rod was lengthened 6.68 mm at the
cephalad end and 6.24 mm at the caudal end.

JOPA 7
Alan B. Johnston, PA-CNew Hampshire Orthopaedic Center, Nashua, NH
With the utilization of ! uoroscopic guidance, the accuracy of injections for both diagnostic and
therapeutic purposes can be dramatically increased. This is especially true in the case of the elbow. Some
common indications for intra-articular therapeutic elbow injections include osteoarthritis of the humeroulnar
and radiocapitellar joints, synovitis, and adhesive capsulitis. Fluoroscopically guided intra-articular injections
generally provide signi" cant relief for these conditions which may allow patients to delay or possibly even
avoid surgical intervention.
Fluoroscopic guidance can also con" rm accurate placement of contrast material during MRI
arthrography. Indications for MRI arthrography include intra-articular loose bodies, chondral and
osteochondral injuries, collateral ligament tears, and synovial and capsular abnormalities. Arthrography can
also help to determine the extent of the ligament tearing which may be dif" cult to visualize with the use of non-
contrast MRI. In particular, elbow arthrography is
commonly used to detect tears of the ulnar collateral
ligament.
Contraindications for the procedure include
allergies to contrast material, including both
iodine based contrast solution and Gadolinium,
injectable anesthetics, or corticosteroids. Relative
contraindications include use of anticoagulation
medications. Patients who are on aspirin therapy
may proceed with intra-articular injection treatment.
Patients taking other anticoagulants, including
Warfarin, Clopidogrel, Dabigatran, and the like,
should stop use of the anticoagulant " ve days before
the intra-articular injection procedure, if medically
appropriate. If diabetic patients are receiving a
corticosteroid injection, they should be cautioned
about possible elevation of their serum blood sugar
levels and are advised to adjust their diabetes
medications accordingly.
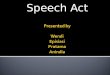
Procedure: The patient is seated in a chair facing the
front of a radiolucent table. The shoulder and elbow
are placed in a 90:90 position on the exam table.
(Figure 1) The radiocapitellar joint is palpated as the
soft spot in the middle of the “lateral triangle” formed
by the olecranon, radial head, and capitellum. The
image intensi" er is used to obtain a good, open clear
space of the humeroulnar joint. Elbow positioning can
be adjusted to achieve this if necessary. Following
this, the lateral aspect of the elbow is prepped with
Betadine and alcohol. A 25 gauge needle is placed on
the skin and utilizing the image intensi" er the point of
entry at the humeroulnar clear space is determined.
Procedures in Orthopedics:
Fluoroscopic Elbow Injections
FIGURE 2
FIGURE 1

8 JOPA
are also advised to limit unnecessary elbow motion
for 24-48 hours to avoid any undue discomfort. Ice
can be used at the injection site to reduce local
soreness. Diabetics are cautioned as outlined
above. If patients are having a MRI procedure,
they are taken to the scanner at this point for
completion of the examination. For patients
receiving a corticosteroid injection, they are seen
back in follow-up in approximately four to six weeks
for re-evaluation to determine their response to
the injection. If successful, the injection may be
repeated three to four times yearly so long as they
remain effective.
(Figure 2) A skin wheal is then raised at the entry
point with 1% plain Xylocaine and taken down in
to the subcutaneous tissues.
Once local anesthesia is obtained, a
25-gauge 1 ½ inch needle is introduced into the
elbow joint. The needle should be advanced
parallel to the x-ray beam and perpendicular to the
" oor. It is imperative to keep the needle as parallel
to the beam as possible to avoid losing orientation.
If done properly the needle should appear as a
small dot at the point of entry. (Figure 3) As the
needle advances through the capsule and into
the intra-articular space, less resistance should
be felt. To help con# rm intra-articular placement,
the needle may come in contact with the capitellar
surface indicating proper positioning, although
this should be kept to a minimum.
Once intra-articular position is suspected
on the image intensi# er, the needle is left in place
and extension tubing attached. Con# rmation is
then achieved by injection of contrast material (3
ml Isovue300 and 2 ml saline) while maintaining
needle position. A characteristic intra-articular
# lling pattern should be noted (Figure 4), and
only the amount of contrast material needed to
con# rm position is used. The contrast syringe is
removed and a syringe containing 3 ml 1% plain
Xylocaine and Methyprednisolone (40 mg or 80 mg
depending on practitioner preference) is injected
slowly into the elbow. For MRI arthrography, 0.1
ml of Gadolinium is injected in lieu of the steroid
followed by 2 ml of contrast material to insure no
contrast material remains in the tubing or needle.
The 25-gauge needle is then withdrawn and a
bandage is applied to the injection site after any
bleeding is controlled. For MRI arthrograms, the
patient is instructed to limit elbow movement
prior to the MRI so as to avoid extravasation of
the contrast material out of the elbow joint via the
injection tract.
Post injection instructions are given to
the patient prior to their departure from the
" uoroscopy suite. Patients are advised they may
experience some fullness or mild discomfort. They
Procedures in Orthopedics:
Fluoroscopic Elbow Injections
FIGURE 3
FIGURE 4

JOPA 9
The Journal of Orthopedics for Physician Assistants (JOPA) is a
peer-reviewed publication that delivers a broad range of orthopedic
content across all subspecialties. Authors can contribute any original
article that promotes an orthopedic education for physician assistants
(several examples are listed below). JOPA avoids publishing original
research articles, as well as articles previously published or being
considered for publication in other journals. Articles are peer reviewed
by a panel of orthopedic physicians and PAs to ensure accuracy, clinical
relevance, and readability.
References should be cited using the AMA Manual of Style, 10th edition. References should be recent and
predominately drawn from peer reviewed journals. Textbook and website references should be avoided if possible.
Article content, including the manuscript body and any tables, should be submitted in Microsoft Word format to
facilitate editing. Please use a standard font, such as Times New Roman, and a 12-point font size. Use appropriate
headings and subheadings in feature articles to organize paragraphs. JOPA reserves the right to edit content for space
and/or grammar issues. Any images that accompany an article must be sent as separate downloadable � les from the
manuscript text for publishing.
Featured Review Articles
Featured review articles should contain a comprehensive
review of literature on an orthopedic topic of choice.
These academic literature reviews should be heavily
referenced and may be co-authored. Subspecialists
should consider writing on topics in their � elds of
expertise. Featured review length should be 4-8 pages.
When considering the appropriate length, keep in mind
the clinical signi� cance and readability of content.
Review Articles
Review articles should be 3-4 pages on an orthopedic
topic of choice. Review articles should be selective and
include few references. Authors may review a clinical
condition, surgical procedure, or any other topic related
to orthopedics. Preceptors may consider co-authoring a
review article with a PA student interested in pursuing a
career in orthopedics.
Case Studies
Case studies choose a case and provide a complete
history of the clinical presentation, treatment, and
outcome. Radiographs and other imaging should
be included to follow the course of a diagnosis and
treatment. Several learning points should be included at
the end of the case study, with appropriate references.
Please remove all patient identi� cation information prior
to submission.
Case Reviews and Image Quizzes
Case reviews present a unique case with several images
and a brief description of the presentation, diagnosis,
and treatment. Image quizzes include an image for
readers to interpret. Answers should be provided, with
a brief explanation of the patient and correct diagnosis.
Do not include literature review or references for case
reviews or image quizzes.
Be Creative!
Consider submitting a description of how your practice
uses PAs or the relationship you have with your
supervising physicians. Consider writing on a patient’s
experience and how it could be of value to PA colleagues.
Write a detailed narrative of a typical day in your life as
a PA. Personal experiences can be some of the most
interesting and helpful articles for other PAs to read. If
you have any other submission ideas, please contact the
editor at [email protected].
Supervising Physicians and
Allied Health Professionals
Supervising physicians may submit articles on topics in
their subspecialty or issues related to the PA profession.
Physicians may also choose to write on a procedure or
service unique to their practice. Co-authoring an article
with a supervising physician is a great way to promote
the physician-PA relationship. Nurse Practitioners
practicing in orthopedics are encouraged to contribute,
and may receive a free copy of JOPA by contacting
the editor or subscribing online. Contributions from
other allied health professionals, such as physical
therapists and athletic trainers, give PAs an opportunity
to learn from those with whom we share patient care
responsibilities. Allied health professionals who wish
to contribute to JOPA can contact the editor, Dagan
Cloutier, at [email protected].
Writing for JOPA: Information for Authors

10 JOPA
September Image Quiz: Lumbar Discitis
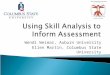
Hematogenous vertebral osteomyelitis and discitis are relatively uncommon causes of severe lower back pain in presenting patients. Vertebral osteomyelitis predominately occurs in adults over 50 years of age with two-thirds occurring in men. The elderly population is most commonly affected as prevalence increases with age. Over half of vertebral osteomyelitis infections occur in the lumbar region but may occur at any level of the spine. Hematogenous osteomyelitis can occur from several conditions that cause bacteremia which may include; urinary tract infections or genitourinary procedure, soft tissue infection, respiratory infection, and intravenous drug use. However 30-70% percent of hematogenous infections have no identi� able source. Infection by direct inoculation of bacteria into the spine can occur after any spinal procedure or penetrating trauma. Vertebral infection occurs when bacteria spreads to the vascular metaphyseal bone and into the
Figure 1 Figure 2
An 85-year old male presents to the ED with a three day history of severe lower back pain. He admits to having years of mild lower back pain from lumbar spine arthritis but the pain is much worse now. He denies any known injury and has been feeling feverish for the last few days. He denies any recent infection or genitourinary procedure. On exam the patient has point tenderness of the lumbar spine and paraspinous muscles but no neurological defects in the lower extremities. The patients white count is within normal limits but his CRP and ESR are mildly elevated. Blood cultures are obtained and results are pending. X-rays taken in the ED show severe lumbar degenerative arthritis but no acute abnormalities. An MRI with and without contrast is obtained due to a suspicion of vertebral osteomyelitis. Figure 1 is a STIR sagittal image of the lumbar spine showing ! uid between the L3-L4 disc space and edema noted within L3
and L4 vertebrae. Small ! uid collections are seen within the paraspinal soft tissues adjacent to the L3-
L4 disc interval (Figure 2). The ! uid collections within the paraspinous soft tissues show heterogeneous
enhancement after the administration of IV Gadolinium. These � ndings were reported as being consistent
with discitis and osteomyelitis at L3-L4. The patient underwent a CT-guided aspiration by radiology which
yielded one milliliter of “pus”. Initial gram stain shows no organisms but the � nal cultures are pending.
What is the most appropriate initial treatment option for this patient?
A. Urgent lumbar discectomy and inter-body fusion at L3-L4
B. Urgent open irrigation and debridement with bone grafting
C. Start Intravenous Vancomycin + Ceftriaxone
D. Observation and hold antibiotics until cultures are � nalized

JOPA 11
September Image Quiz: Lumbar Discitis
vertebral endplates. Because the disc has no direct blood supply, infection is spread from bone to the adjacent intervertebral discs. Staphylococcus aureus is the most common microorganism involved, followed by gram-negative organisms E. coli, Pseudomonas, and Proteus species. Gram-negative organisms are the most common causative agents in the presence of a genitourinary tract infection. In heroin users, Pseudomonas is the most common etiologic organism and predominately affects the cervical region. Presenting symptoms include fever, chills, and severe neck or lower back pain. A hip � exion
contracture may be present in patients with psoas
involvement. Vertebral infection may spread
to adjacent soft tissues causing a paraspinal
abscess. Progression of pain and neurological
de� cits indicates the infection may have spread
into the epidural space. Approximately 17%
percent of patients with vertebral osteomyelitis
and a disc space infection caused by contiguous
spread will develop an epidural abscess.
Less than half of patients with vertebral
osteomyelitis will have an elevated leukocyte
count but the CRP and ESR will likely be elevated;
one study found that the ESR was elevated in 92%
of presenting patients. Blood cultures are often
taken but are positive for the causative agent in
less than half of infected patients. Urine cultures
should also be done in all patients to rule out
urinary tract infections as a possible source.
Plain radiographs are often negative early
in the infection. Urgent MRI with and without
contrast should be performed when vertebral
osteomyelitis is suspected. Contrast, such as
gadolinium, helps enhance the extent of bone and
soft tissue involvement. MRI is very sensitive in
picking up the typical changes occurring within
the vertebral bodies, vertebral endplates, disc
space, and soft tissues. CT myelography and bone
scan may be used when MRI is contraindicated.
When vertebral osteomyelitis is present
on MRI an urgent guided biopsy is indicated
prior to the initiation of antibiotic therapy. CT-
guided biopsies can be an effective method to
determine the causative agent. However, if blood
cultures are positive for the suspected cause a
biopsy may not be necessary. Broad spectrum
antibiotics coverage including Vancomycin +
Ceftriaxone are commonly used until the biopsy
cultures are � nalized. Parental antibiotic therapy
is generally recommended for 6 weeks followed
by oral antibiotics until disease resolution. A
decline in ESR and CRP levels over the course
of treatment is valuable indicator of therapeutic
response. Lumbar bracing to immobilize the
spine in extension helps reduce pain and prevent
vertebral deformity during treatment. Once
antibiotic treatment is � nished and the discitis is
resolved the involved level will usually proceed to
auto-fusion.
Patients who present with an epidural
abscess or develop neurological de� cits may
require surgery. Neurological symptoms can
progress so timely action is necessary to avoid
permanent disability in these patients. Surgery
generally involves an anterior approach that
allows for an extensive debridement and bone
grafting. Posterior stabilization and fusion may be
performed in a later second stage procedure if the
initial debridement causes instability.
Figure 2. X-ray two months out showing autofusion at L3-L4. Final cultures came back with Peptostreptococcus. Prior to discharge from the hospital a PICC line was placed and he was prescribed 6 weeks of IV Ivanz. Weekly labs, including a CBC, ESR, and CRP were followed by the consulting infectious disease specialists. A follow-up MRI at 4 weeks showed resolving discitis. Infectious disease continued to watch the labs trend downward during treatment.
Patient follow-up

12 JOPA
October Image Quiz: Medial epicondyle avulsion fracture
Figure 1
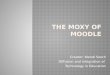
A 6-year old boy presents to the orthopedic urgent care complaining of severe left elbow pain after a fall from the monkey bars earlier in the day. His mother did not witness the fall and says he has not been able to use the arm since. On exam the boy has swelling and tenderness over the medial elbow. Motor and sensation is intact throughout. X-rays taken at the local urgent care of� ce are shown to the left.
What is the best treatment option for this patient? a. Closed reduction with percutaneous pinning b. Open reduction internal � xation with one cannulated screw c. Long arm cast for 4 weeks d. Normal x-rays, no treatment necessary
The above x-rays show a displaced medial epicondyle avulsion fracture or a medial epicondylar apophyseal avulsion. Soft tissue swelling medial to the fracture is also noted. Medial epicondyle fractures can occur as a result of a direct blow, avulsion type mechanism, or with an elbow dislocation. Avulsion of the medial apophysis generally occurs with a valgus loading with the arm in extension. Avulsion fractures generally involve the apophysis only. Attachments to the medial epicondyle include the ulnar collateral ligament and common wrist ! exors. These
soft tissue attachments exert a pulling force distally which
typically causes fracture displacement in this direction.
Isolated avulsions can occur in adolescent throwing athletes
as a result of a sudden contracture of the forearm ! exors.
Treatment of these fractures is controversial and
typically depends on neurovascular function and degree of
displacement. Incarceration of the fracture fragment into the
joint space or complete ulnar nerve dysfunction generally
requires open reduction and internal � xation. Otherwise,
non-operative management of medial epicondyle fractures is
generally preferred as results have shown a high rate of union
and good results seen with a � brous union. Non operative
treatment involves 3-4 weeks of immobilization with a sling
or long arm cast. Early motion is then encouraged to prevent
elbow stiffness commonly seen with pediatric elbow injuries.
Surgical � xation can be dif� cult in this patient’s age group
as the medial epicondyle is mostly cartilaginous. The ulnar
nerve runs behind the medial epicondyle and can be injured
during surgical � xation. Surgery generally includes closed
reduction with K-wire � xation or single cannulated screw
� xation.
Figure 2. Above is an AP x-ray 4 weeks out from the fracture. The long arm cast was removed and the patient was allowed to resume activities as tolerated at 5 weeks. Interestingly, the x-rays at 4 weeks show less displacement.

JOPA 13
November Image Quiz: Spondylolysis
Figure 1
A 16-year-old male presents to your of� ce with a three week history of lower back pain that he believes started after playing a basketball game. He denies any prior history of lower back pain, recent fall, or known injury. He denies numbness or weakness of lower extremities. He has tried anti-in� ammatories, ice, and rest but continues to experience lower back pain with athletic activities. On exam he has no palpable tenderness over the lumbar spine. Motor, sensation, and deep tendon re� exes are intact in the lower extremities. Range of motion of the hip, knee, and ankle are within normal limits. X-rays obtained, including AP, lateral, and oblique view show a possible right sided L5 spondylolysis. Lateral and right sided oblique � lms are shown above.
What is the next best step in treating this patient? A. Recommend lumbar corset bracing and activity modi� cation for 3 months B. Order an MRI of the lumbar spineC. Resume activities as tolerated, obtain follow-up x-rays in 3 monthsD. Order � exion-extension lateral lumbar � lms
The most common cause of back pain in adolescent athletes is idiopathic; 75% of presenting patients have no identi� able cause of the pain. The most common identi� able cause by x-ray or MRI of back pain in this age group is due to spondylolysis. Pain associated with spondylolysis is usually activity related and exacerbated with spinal extension. The majority of athletes do not recall a precipitating event; only 40% of patients with spondylolysis recall a known injury. On exam, unilateral back pain that worsens in extension is common. Neurological de� cits are rarely seen. Initial work-up should include AP, lateral, and oblique x-rays. Oblique x-rays should clearly see the “scotty dog” view which includes the nose as the transverse process, the eye as the pedicle, the neck as the pars interarticularis, the ear as the superior facet, the front leg as the inferior facet, and the body as the lamina. A fracture through the neck of “scotty dog” or the pars
Figure 2

November Image Quiz: Spondylolysis
Figure 3. The patient’s MRI shows a stress reaction of the pedicle up into the pars on the right side. No fracture line was seen. He was placed in a brace for two months and returned to sports when pain had subsided in three months.
interarticularis indicates spondylolysis. The majority of x-rays will not show a fracture or stress reaction early in presentation. Spondylolysis rarely causes associated spondylolisthesis in adolescents and therefore obtaining routine � exion- extension x-rays is unnecessary.
MRI is sensitive in picking up an early stress reaction
and is the study of choice in the presence of any
neurological de� cits. MRI also helps rule out other
conditions in the differential diagnosis including
commonly seen annular tears, disc herniations, facet
disease as well as other boney and soft tissue pathology.
A bone scan may help � nd an early stress reaction if
x-rays and MRI are negative. CT scan is the best study
to see an occult fracture line or evidence of healing. CT
is also helpful in chronic spondylolysis to determine
whether the fracture is healed or a stable nonunion
is present. Potentially harmful radiation exposure
associated with bone scans and CT scans should be
considered when choosing the initial study of choice in
adolescents.
If MRI or bone scan is negative than conservative
care with a course of physical therapy and NSAIDS is
recommended. No activity restrictions or bracing is
necessary and patients may resume sports to tolerance.
Asymptomatic chronic spondylolysis may be picked up incidentally and should be treated
conservatively as well.
Treatment of symptomatic acute spondyloysis (evident by a fracture line or boney edema)
should include activity modi� cation for 6-12 weeks to prevent progression of the fracture and
to promote healing. Bracing with a lumbar corset type (LSO) brace to reduce lumbar lordosis
is recommended. Immobilizing the spine helps the pars defect heal. The brace is typically
recommended for the 3 months of sports restrictions and another three months with activities to
tolerance. Sports that require signi� cant extension type forces like football and gymnastics may
restrict participation for up 6 months depending on symptoms.
In rare instances, spondylolysis may also cause instability resulting in the vertabrae
shifting forward causing spondylolisthesis. Spondylolysis is the most common cause of isthmic
spondylolisthesis. Adolescents with spondylolisthesis should be followed with serial x-rays
every 6 months until skeletal maturity to monitor potential slip progression. Surgery should be
considered in patients with spondylolysis and progressive spondylolisthesis, with any associated
neurological de� cits, and with persistent pain despite 6-months of conservative treatment.
The most common location for spondylolysis with slip in athletes is at L5 vertabrae on the S1
vertabrae. This location absorbs the greatest spinal stress forces during sporting activities.
For a L5 spondylolisthesis, an L5-S1 in situ fusion is the recommended in the presence of pain,
progressive slip, and neurological de� cits. In adolescents and young adults a repair of the pars
is recommended at the L4 vertebrae and above. Loss of motion proximal to L4 is more relevant
clinically than with fusions distally; this makes motion preservation preferable at the proximal
levels.
Patient follow-up

Distinguish Yourself as a PA in Orthopaedic Surgery.
Earn a CAQ. You are building your reputa�on as a clinician, and
you want to set yourself apart.
You’ve honed your skills. You’ve gained knowledge
and exper�se. You’ve done everything to be an
accomplished orthopaedic surgery PA.
The Cer�ficate of Added Qualifica�ons (CAQ) in
Orthopaedic Surgery is your chance to prove it.
The CAQ is offered by NCCPA—the only cer�fying
organiza�on for PAs in the U.S. Already trusted
by health care employers, NCCPA helps you
document your advanced qualifica�ons.
You already have what it takes.
Visit www.nccpa.net/orthopaedicsurgery
or call 678-417-8100, and start earning your
CAQ in Orthopaedic Surgery today.
Register Now!
Sign in to your record
to register for the
CAQ program.
www.nccpa.net/PALogin

16 JOPA
Quadriceps tendon autograft for ACL reconstruction: Evidence for increased utilization
Sean Hazzard, PA-CMassachusetts General Hospital Sports Medicine Service
ABSTRACT
Purpose: To review the current literature of quadriceps tendon (QT) autograft tissue for ACL reconstruction and assess it’s evidence to become a more mainstream graft option
Methods: A database review of clinical studies involving quadriceps tendon autograft tissue for ACL reconstruction was compared to results of ACL reconstructions using BTB and hamstring autograft tissue.
Results: 20 articles were noted totaling 1,686 reconstructions including 6 studies which compared QT to either hamstring or BTB grafts. Quadriceps tendon grafts reported signi! cantly
less anterior knee pain (3.8%) compared to BTB
(17.4%) and hamstring (11.5%) while providing
clinical stability, adequate amount of graft
tissue, and subjective outcomes comparable to
traditional BTB and HS autograft options.
Conclusions: Quadriceps tendon autograft is a
strong and clinically proven alternative to BTB
and hamstring autografts while decreasing graft
site morbidity and should be considered a ! rst
line ACL graft option.
Introduction
Anterior cruciate ligament (ACL)
rupture is a common musculoskeletal injury
with an increasing amount of reconstructions
being performed annually38. Since the early
2000’s, various techniques and methods have
been described and researched focusing on a
more anatomic placement of the ACL graft to
restore native kinematics. As this ‘anatomic
reconstruction’ ideology has become an
accepted and established technique, surgeons
are becoming more open to utilizing various graft
options as prior use of certain grafts with non-
anatomic techniques may not have produced
optimal results. Autologous bone patella tendon
bone (BTB) and hamstring (HS) grafts are the
most common autograft tissues utilized for
ACL reconstruction14. BTB grafts have a known
potential complication of donor site morbidity
(speci! cally anterior knee pain) while hamstring
autograft has the risk of a higher risk of re-
rupture, higher infection rate, and insuf! cient
size (potentially requiring the need for allograft
augmentation)8,34. 39, 40. This paper describes
the additional quadriceps tendon autograft as
an option that can provide the strength, size
and success of the BTB graft with substantially
less donor site morbidity. Additionally, it can
potentially avoid the higher risk of re-rupture and
infection that can be associated with hamstring
autograft34,39,40.
Harvest of the graft typically involves
making a 5cm longitudinal incision from the
superior pole of the patella going proximal. Skin
" aps are developed to allow for appropriate
exposure of the tendon. The central ! bers of the
quadriceps tendon are identi! ed to an area 6 to
7cm proximal to the patella. A 10mm wide section
of tendon is incised. Careful attention should be
made to not violate the suprapatellar pouch. If
this is incised, the defect should be closed to
avoid " uid escape during arthroscopy. If a #10
blade is used, this is typically 7mm wide which
is average thickness of the quadriceps tendon.
The fat stripe intersecting the rectus femoris
and the vastus intermedius is also a landmark
to use to identify that the blade is approaching
the pouch. A Kelly clamp can be used to create
a plane between the graft and the suprapatellar
pouch. Once the soft tissue aspect of the graft is
harvested, a determination can be made (usually
dependent on length) to either harvest a 20mm
bone plug or to cut the distal graft at the patella
insertion. The tendon defect is then closed with
the knee in 90 degrees of " exion.
Materials and Methods
A search of PUBMED (through March 2014)
was performed using keywords “anterior cruciate
Quadriceps tendon autograft for ACL reconstruction:
Evidence for increased utilization
Sean Hazzard, PA-C
Massachusetts General Hospital Sports Medicine Service

JOPA 17
ligament reconstruction”, “ACL technique”, and “ACL reconstruction with quadriceps tendon autograft”. References from primary and review articles were cross referenced to identify any additional information and/or papers not included in the PUBMED results. Papers with outcomes were a minimum of 12 month follow-up.
Results
The initial search identi! ed 20 studies
involving quadriceps tendon autograft for ACL
reconstruction totaling 1,686 grafts performed in
humans 9,16-33, 35, 36. Of these 20 studies, 6 of them
compared QT grafts directly to BTB and/or HS
grafts18, 22, 24, 28, 32, 36. Not all of these papers provided
outcomes, speci! cally, re-rupture. Various studies
were also identi! ed discussing the anatomy and
morphology of the quadriceps tendon as well as
donor site morbidity. The primary outcomes that
were investigated were anterior knee pain and
instability.
Anterior knee pain after quadriceps tendon
autograft harvest was noted in fourteen articles
and reported to be 3.8% (30/805 patients)13,32,33.
Comparatively, anterior knee pain after BTB
autograft harvest is reported to be 17.4% (1,348
patients) and anterior knee pain after hamstring
autograft is 11.5% (628 patients)8.
Instability was measured using various
methods including KT-1000, Lachman exam, and
pivot shift exam. Traditional normal Lachman
and pivot shift exams for BTB grafts are 76-
100% and 81-100% of the time respectively.
Lachman and pivot shift exams for HS grafts are
traditionally normal 64-100% and 72-100% of the
time respectively15. Review of current literature
for quadriceps tendon autograft shows 81-95%
patients had a normal Lachman and 80-95% a
normal pivot shift exam. The six comparative
studies showed that BTB, HS, and quadriceps
tendon autograft had no signi! cant laxity
difference between the groups 18, 22, 24, 28, 32.
Discussion
Bone-tendon-bone and hamstring autograft
tissues are a well established as suitable grafts for
ACL reconstruction. The advantage of BTB is that
it provides a strong graft and secure ‘bone-to-bone
! xation’ with a very low failure rate8 however
are associated anterior knee pain 17-26% of the
time, crepitus, loss of extension in conjunction
with possible patellar tendon shortening and
infrapatellar contracture6. Hamstring autograft
has gained more popularity, possibly due to less
graft site morbidity, and have been shown to
have similar functional outcomes compared to
BTB7. The disadvantage with hamstring autograft
is increased clinical laxity (5.2% more compared
to BTB) and higher failure/re-rupture rate (4.9%
compared to 1.9% with BTB)8. Several recent
publications (including two ACL registries)
totaling 22,460 ACL reconstructions comparing
BTB vs Hamstring autograft showed that
hamstring grafts were 2.26-2.3 more times likely
to re-rupture compared to BTB grafts39,40. Recent
evidence also suggests that hamstring autograft
can have an infection rate up to 8.2 times more
that of BTB autograft34.
Quadriceps tendon autograft has been
an option for ACL reconstruction for nearly
30 years but remains less commonly used and
therefore not as commonly studied30. Quadriceps
tendon autograft has been shown to have a larger
cross sectional area than the native ACL, patella
tendon, and quadrupled hamstring autograft
with a tensile load higher than that of the native
ACL1-5. It is versatile in that it can be used with or
without a bone plug, is suitable for double bundle
reconstruction, and consistently provides enough
length and width to avoid allograft augmentation.
Several studies obtained showed that quad graft
harvest resulted in less of a decrease in strength
of the extensor mechanism than harvest of the
patella tendon graft36,37.
Graft site morbidity (particularly anterior
knee pain) is a common concern for both
orthopedic surgeons and patients. Quadriceps
tendon appears to produce a cumulative 3.8%
chance of anterior knee pain compared to 17-
26% with BTB graft and 11% with hamstring
autograft6,8,13,32,33. Post-operative quadriceps
weakness is very comparable at 11% compared
to BTB (10-18%) and hamstring (10%)9,10. The
risk of patella fracture is also similar (when
applicable) to BTB harvest (1.2% vs 0.2-
1.8)9,11,12. Review of literature showed that
knees that had quadriceps tendon autograft
harvested obtained a normal range of motion 97%
of the time13.
Patient satisfaction scores using
the Lysholm system were comparable with
quadriceps tendon (91 points), BTB (91-93
points), and hamstring (80-94 points) grafts15.
These studies showed no difference in the
functional scores of patients with each type of
autograft.

18 JOPA
This paper provides a summary of existing literature regarding the use of quadriceps tendon autograft for use in anterior cruciate ligament reconstruction including direct comparison to the most commonly used grafts today (patella tendon and hamstring). 1,686 total quadriceps tendon grafted ACL reconstructions were evaluated and show a potential decrease in the chance of anterior knee pain development by up to 22% (compared to other autografts) while providing adequate strength, larger overall graft thickness, and comparable satisfaction scores.
Conclusion
Quadriceps tendon autograft is a proven option for the use in anterior cruciate ligament reconstruction and should be considered as a mainstream graft choice in addition to BTB and hamstring autografts.
References
1. Harris N.L., Smith D.A., Lamoreaux L., et al: Central quadriceps tendon for anterior cruciate ligament reconstruction. Part I: morphometric and biomechanical evaluation. Am J Sports Med 25. (1): 23-28.19972. Staubli H.U., Schatzmann L., Brunner P., et al: Mechanical tensile properties of the quadriceps tendon and patellar ligament in young adults. Am J Sports Med 27. (1): 27-34.19993. Noyes F.R., Butler D.L., Grood E.S., et al: Biomechanical analysis of human ligament grafts used in knee-ligament repairs and reconstructions. J Bone Joint Surg Am 66. (3): 344-352.1984 4. Hamner D.L., Brown , Jr. , Jr.C.H., Steiner M.E., et al: Hamstring tendon grafts for reconstruction of the anterior cruciate ligament: biomechanical evaluation of the use of multiple strands and tensioning techniques. J Bone Joint Surg Am 81. (4): 549-557.19995. Woo S.L., Hollis J.M., Adams D.J., et al: Tensile properties of the human femur-anterior cruciate ligament-tibia complex. The effects of specimen age and orientation. Am J Sports Med 19. (3): 217-225.19916. Geib T.M., Shelton W.R., Phelps R.A., et al: Anterior cruciate ligament reconstruction using quadriceps tendon autograft: intermediate-term outcome. Arthroscopy 25. (12): 1408-1414.2009 7.Feller J, Webster K (2003) A randomized comparison of patellartendon and hamstring tendon anterior cruciate ligament reconstruction.Am J Sports Med 31:564–5738. Freedman K.B., D’Amato M.J., Nedeff D.D., et al: Arthroscopic anterior cruciate ligament reconstruction: a metaanalysis comparing patellar tendon and hamstring tendon autografts. Am J Sports Med 31. (1): 2-11.20039. Lee S., Seong S.C., Jo H., et al: Outcome of anterior cruciate ligament reconstruction using quadriceps tendon autograft. Arthroscopy 20. (8): 795-802.200410. Nakamura N., Horibe S., Sasaki S., et al: Evaluation of active knee ! exion and hamstring strength after anterior cruciate ligament reconstruction using hamstring tendons. Arthroscopy 18. (6): 598-602.200211. Christen B., Jakob R.P.: Fractures associated with patellar ligament grafts in cruciate ligament surgery. J Bone Joint Surg Br 74. (4): 617-619.199212. Viola R., Vianello R.: Three cases of patella fracture in 1,320 anterior cruciate ligament reconstructions with bone-patellar tendon-bone autograft. Arthroscopy 15. (1): 93-97.199913. Mulford J.,Hutchinson S.,Hang J.: Outcomes for primary ACL reconstruction with quadriceps autograft: a systemic review, Knee Surg Sports Traumatol Arthrosc 21 (8) 1882-1888. 201314. Johnson RJ, Beynnon BD, Nichols CE: The treatment of injuries of the anterior cruciate ligament [current concepts review]. J Bone Joint Surg 74A:140 –151,199215. Magnussen RA, Carey JL, Spindler KP: Does autograft choice determine intermediate-term outcome of ACL reconstruction?, Knee Surg Sports Traumatol Arthrosc 19:462–472. 2010
16. Chen CH, Chou SW, Chen WJ, Shih CH, Ueng WN Arthroscopic anterior cruciate ligament reconstruction with quadriceps tendon autograft–minimal 4-year follow-up (SS-14). Arthroscopy 20:e7. 200617. Chen CH, Chen WJ, Shih CH Arthroscopic anterior cruciate ligament reconstruction with quadriceps tendon-patellar bone autograft. J Trauma 46:678–682. 199918. Chen CH, Chuang TY, Chen LH, Chen WJ, Chen CH Comparison of quadruple hamstring graft and quadriceps (SS-05). Arthroscopy 19:SS-05. 200319. DeAngelis JP, Fulkerson JP, Quadriceps tendon–a reliable alternative for reconstruction of the anterior cruciate ligament. Clin Sports Med 26:587–596. 200720. Geib T, Shelton WR, Arthroscopic Anterior cruciate ligament reconstruction utilizing quadriceps tendon autograft: intermediate results (SS-32). Arthroscopy 24:e17–e18. 200821. Gorschewsky O, Stapf R, Geiser L, Geitner U, Neumann W. Clinical comparison of " xation methods for patellar bone quadriceps tendon autografts in anterior cruciate ligament reconstruction: absorbable cross-pins versus absorbable screws. Am J Sports Med 35:2118–2125. 200722. Han HS, Seong SC, Lee S, Lee MC.Anterior cruciate ligament reconstruction: quadriceps versus patellar autograft. Clin Orthop Relat Res 466:198–204. 200823. Kim SJ, Jo SB, Kumar P, Oh KS. Comparison of single- and double-bundle anterior cruciate ligament reconstruction using quadriceps tendon-bone autografts. Arthroscopy 25:70–77. 200924. Kim SJ, Kumar P, Oh KS. Anterior cruciate ligament reconstruction: autogenous quadriceps tendon-bone compared with bone-patellar tendon-bone grafts at 2-year follow-up. Arthroscopy 25:137–144. 200925. Lee S, Seong SC, Jo CH, Han HS, An JH, Lee MC. Anterior cruciate ligament reconstruction with use of autologous quadriceps tendon graft. J Bone Joint Surg Am 89(Suppl 3):116–126. 200726. Leitman EH, Morgan CD, Grawl DM. Quadriceps tendon anterior cruciate ligament reconstruction using the all-inside technique. Op Tech Sports Med 7:179–188. 199927. Noronha JC. Reconstruction of the anterior cruciate ligament with quadriceps tendon. Arthroscopy 18:E37p1–E37p5, 200228. Sarrafan N, Mehdinasab SA. Anterior cruciate ligament reconstruction using the patella tendon and quadriceps tendon: a comparative study. Pak J Med Sci 24:416–419. 200829. Shelton WR, Holt S. Quadriceps tendon anterior cruciate ligament reconstruction (SS-15). Arthroscopy 20:e7. 200430. Stanish WD, Kirkpatrick J, Rubinovich RM. Reconstruction of the anterior cruciate ligament with a quadricep patellar tendon graft. Preliminary results. Can J Appl Sport Sci 9:21–24. 198431. Theut PC, Fulkerson JP, Armour EF, Joseph M. Anterior cruciate ligament reconstruction utilizing central quadriceps free tendon. Orthop Clin North Am 34:31–39. 200332. Lund B, Nielsen T, Fauno P, et al. Is quadriceps tendon a better graft choice than patellar tendon? A prospective randomized study, Arthroscopy Vol 30 (ePub ahead of print) 2014 33. Schulz AP, Lange V, Gille J, et al. Anterior cruciate ligament reconstruction using bone plug-free quadriceps tendon autograft: intermediate-term clinical outcome after 24-36 months, Open Access Sports Med 4: 243-249, 201334. Maletis G, Inacio M, Reynolds S., et al. Incidence of post-operative anterior cruciate ligament reconstruction infections: Graft choice makes a difference, Am J Sports Med 41, 1780-1785. 201335. Rabuck S, Musahl V, Fu F, West, R., Anatomic anterior cruciate ligament reconstruction with quadriceps tendon autograft, Clin Sports Med 32, 155-164. 201336. Adams D.J., Mazzocca A.D., Fulkerson J.P.: Residual strength of the quadriceps versus patellar tendon after harvesting a central free tendon graft. Arthroscopy 22. (1): 76-79.200637. Shoemaker S.C., Adams D., Daniel D.M., et al: Quadriceps/anterior cruciate graft interaction. An in vitro study of joint kinematics and anterior cruciate ligament graft tension. Clin Orthop 294. 379-390.199338. Gianotti S, Marshall S, Hume P, Bunt L, Incidence of anterior cruciate ligament injury and other knee ligament injuries: a national
population based study, J Sci Med Sport 12: 622-627. 2009
39. Persson A, Fjeldsgaard K, Gjertsen, J, et al, Increased risk of
revision with hamstring tendon grafts compared with patellar tendon
grafts after anterior cruciate ligament reconstruction; a study of
12,643 patients from the Norweigian cruciate ligament registry, 2004-
2012, Am J Sports Med 42; 285-291. 2013
40. Maletis G, Inacio M, Desmond J, Funahashi T, Reconstruction
of the anterior cruciate ligament; association of graft choice with
increased risk of early revision, The Bone & Joint Journal 95-B 623-
628. 2013


ONE by DesignDelivering the most HA per milliliter to provide knee OA pain relief
MONOVISC® High Molecular Weight HyaluronanChoose the product with the highest concentration of HA available in a single injection
Gel-ONE®
SYNVISC-ONE®
MONOVISC
30 mg/3 mL = 10 mg/mL
48 mg/6 mL = 8 mg/mL
88 mg/4 mL = 22 mg/mL
Drawn to Scale
Manufacturer’s full prescribing information
for Gel-One, Synvisc-One and MONOVISC.

DePuy Mitek, Inc.325 Paramount DriveRaynham, MA 02767-0350USA
T.+1 (800) 382-4682
www.depuysynthes.com
The MONOVISC Difference
• MONOVISC High Molecular Weight Hyaluronan can deliver up to 6 months of efficacy4
• Only non-avian HA single injection available on the market
Efficacy of MONOVISC compared with other single injection HA products
*SYNVISC-ONE® data based on WOMAC Likert scale, adjusted to correlate with MONOVISC and GEL-ONE® VAS 100mm scale response.
References:
1. Data on file. Anika Therapeutics, Inc. Bedford, MA.
2. SYNVISC-ONE data from: Chevalier et al. Single, intra-articular treatment with 6 ml hylan G-F 20 in patients with symptomatic primary osteoarthritis of the knee:
a romdomized, multicenter, double-blind, placebo controlled trial. Ann Rheum Dis. 2010:69(1):113-119. Synvisc-One manufacturer’s full prescribing information.
3. GEL-ONE data from: Strand et al. A multicenter, randomized controlled trial comparing a single intra-articular injection of Gel-200, a new cross-linked formulation of
hyaluronic acid, to phosphate buffered saline for treatment of osteoarthritis of the knee. Osteoarthritis Cartilage 2012:20:350-356. Gel-One manufacturer’s full prescribing
information.
4. MONOVISC manufacturer’s full prescribing information.
Information from package inserts.
MONOVISC® is a registered trademark of and is manufactured by Anika Therapeutics. MONOVISC, SYNVISC-ONE®, and GEL-ONE® are all indicated for knee osteoarthritis.
The third party trademarks used herein are the trademarks of their respective owners.
Important Safety Information
MONOVISC High Molecular Weight Hyaluronan is indicated in the treatment of pain in osteoarthritis (OA) of the knee in patients who have failed to respond adequately to
conservative nonpharmacologic therapy and to simple analgesics, e.g., acetaminophen. In clinical studies, the most commonly reported adverse events were arthralgia,
joint swelling and injection site pain. MONOVISC is contraindicated in patients with known hypersensitivity to hyaluronate formulations or known hypersensitivity (allergy)
to gram positive bacterial proteins. MONOVISC should not be injected in patients with infections or skin diseases in the area of the injection site or joint. MONOVISC
should not be administered to patients with known bleeding disorders.
WOMAC pain reduction from baseline (%)1-3
Week
-10%
0%
-20%
-30%
-40%
-50%
-60%
0 4 8 12 16 20 24 28
MONOVISC
SYNVISC-ONE
GEL-ONE
*
© DePuy Synthes Mitek Sports Medicine, a division of DOI 2014. All rights reserved. DSUS/MTK/0714/0231 09/14

22 JOPA
PERCEPTIONS AND EXPECTATIONS
Reza Ghadimi, PA
Albuquerque, NM
A few years ago, on a cold January morning, a man walked unto the L’Enfant Plaza subway platform in Washington DC, carrying a violin case. He opened the case and placed it on the ground in front of him, took a violin out and started playing. Hundreds of people passed by. Some glanced over at him, some listened while waiting for their train. A few dropped coins and money into the open case without even looking at him. He played for about forty � ve minutes and then left. He had collected about 30 dollars in coins. Three nights previous to that morning, the same man had played the same exact piece of music on the same exact violin to a sold out audience at Boston’s Stately Symphony Hall. Admission tickets were at an average of $150.00 Many years ago, when serving in the United States Air Force, the hospital I worked in required all doctors and medical personnel working in specialty clinics to cover the ER on rotation in the evenings and weekends. Dr. V. was a recently arrived physician of African American race and was pulling his � rst ER shift. The ER was quiet and everyone watching TV in the back room. Outside a civilian janitor was buf� ng the � oor of the waiting area. Our doctor was restless. Suddenly he got up, took his white coat off and went outside and asked the janitor to let him buff the � oor - to burn some of his excess energy. The janitor gladly obliged. A few minutes later a Caucasian lady - wife of an of� cer - arrived, seeking medical care. Not seeing anyone at the desk, asked our doctor/ janitor as to where everyone was. Dr. V. called for someone to come and get her checked in. The corpsman on duty took her back to the exam room, got her H & P, vital signs, gave her a gown and informed her that the doctor would be with her shortly. Outside, he told our doctor that she was ready and went back to watching TV. Our doctor passed the buffer back to the real janitor, put his white coat on and went to see the patient. Well you guessed it, moments later the patient exited the room yelling and screaming that her husband was a Major and that she was going to
have everyone court marshaled for playing games with her. About a few months after the above incident - as a member of the United State Air Force’s Air Transportable Hospital (ATH - Air Force equivalent of the Army’s MASH unit) - we were sent to Jordan following the Jordanian Civil War of 1970, to care for the injured (we were sent as Red Cross Volunteers - our military did not want to be directly involved in another country’s civil war). For the � rst three weeks, I was the only member of the team with orthopaedic surgical experience who also spoke a little Arabic. There was an OB-GYN doctor (our CO), two family practice docs, an Ophthalmologist, and one general surgeon on our team. Prior to this deployment, we never went anywhere so I guess the Air Force didn’t see any reason to have ER and trauma personnel on ATH. It being war, many of the injured required orthopaedic surgical intervention. So we sent an urgent request for an orthopaedic surgeon and in the meanwhile I assisted on all surgical cases of orthopaedic nature. To the non-English speaking patient population and Jordanian medical personnel helping us, I became known as Doctor Reza. Though I repeatedly informed everyone that I was not a doctor, since I was being consulted on all orthopaedic problems and scrubbing on their surgical procedures, their perception was otherwise. And though I was an enlisted person, my teammates felt that if it eased the injured’s mental health, let it be. After a while, Gary C, an orthopaedic surgeon from my own out� t back in Lakenheath � nally arrived. By then however, the native population expected my presence on all orthopaedic cases. Although even our newly arrived surgeon found the situation humorous, it did create problems as patients demanded that I do the surgery. We solved the problem by me showing up on most cases till the patient was put to sleep. Then I left and attended to my own work. By the way that particular assignment earned me the Air Force’s Commendation Medal.

JOPA 23
FIGURE 1. Reza Ghadimi helping the appli-cation of anesthesia to young girl who lost her right leg in the war.
I pride myself in always dressing professionally when I see patients. I wear a tie, white coat and try to present myself accordingly. I sincerely believe that I am not only presenting myself to my patients but representing the entire medical profession. As a PA, I feel that I need to try even harder in order to show the true professionalism of our relatively new profession. I am proud to say that most of my PA colleagues too, are professionally attired and well groomed.Since I am telling war and PA stories, one day, while working at an urgent-care, the physician working with me was a particularly egotistical obese female with manners of ... well not becoming a professional. She wore a cheap dress without a white coat. An elderly female patient was being taken to the exam room by the nurse. As she past us, she gave us all a piercing evaluating look. She seemed particularly ill and thus our doctor went in to see her. Soon however, the doctor returned, upset and cursing. “Reza, she wants to see a real doctor. I told her that I was the only real doctor working here. But she insists that I am lying to her and that the doctor was the man outside in the white coat with a tie” - me. As a PA, we deal with many levels of people in our profession. Both in our patient population and our work environment. Some of the biggest resentments, I have faced as a PA, have been from other PAs and medical personnel.
FIGURE 2. Dr C. (Lt) and Reza building a prostheses for the young girl using plaster and a broom stick.
FIGURE 3. Dr C. (Lt) and Reza (Rt), helping the young girl with her new prostheses.

24 JOPA
When one of them seeks medical care, often they ask to see an MD and not a PA. In the patient population, the most resistance comes from patients from the lower class of our society and from those of foreign origin. The problem here, as I see it is our name. ‘Assistant’ by de� nition requires someone for us to assist. Thus giving us a second class status, even before we enter the exam room. Many times, I have � nished with a patient - done my exam, started the treatment and even given them a prescription and expecting them to leave and they just sit there. “Is there anything else, you need?” I ask.“Well when is the doctor going to come and see me?” Is a standard question.
Patients who have been treated by PAs however, usually appreciate the experience well. In busy practices many patients feel that they get better attention from PAs and I have to say Nurse Practitioners as well. Back in the eighties, I was the sole provider at a small clinic in the resort town of Red River, NM. It is a ski resort with an average population of 500 year round, back then. But during the winter and summer, the population explodes to many thousands. My orthopaedic experience got me the job, since my practice was more like an urgent-care or ER, as 99% of my patients returned to their respective towns after receiving their initial care. They took with them a positive experience and that gained me a reputation at the clinics these people went to for follow up. So it was that when a friend of mine at an orthopaedic clinic in a busy metropolitan city needed some time off, he asked me to go cover for him. There was a secondary reason for this invitation however. My reputation had raised the curiosity of the physicians in that clinic so they wanted to check me out and perhaps recruit me to join their practice. Since it was during off season for me, I gladly accepted it. Once there however, the very busy practice and the rushed way of patient care became a turn off for me very quickly. A particular incident killed the deal for good. One clinic rule was that all new PAs were to present new injuries and fractures to the on-call physician before casting and discharging the patient (no problem there.) On one very busy morning I saw a young patient with a non-displaced distal radius fracture. I informed the family that I was new and thus had to get my doctor’s OK before proceeding. They understood and after I informed the doc I was working with, we waited. The attending for that morning (a
relatively young doctor who didn’t know anything about me) had arrived late and was very busy seeing his own patients and so took a long time to get to me. But � nally after repeated requests, he dashed into my room, walked to the viewing box, took a quick look at the x-rays, walked to the patient and made a cursory exam of the wrist and told me, “put him in a short arm cast and let me see him back in 6 weeks.” and without talking to the patient or the family left the room. Now my routine is to re-check the cast in two weeks and change it since once the swelling subsides, many casts loosen and also in the heat of that southwestern city, many children’s cast become rancid with sweat and dirt. So I ran after him and asked whether we should re-check the cast in two weeks? He gave me an annoying look over his shoulder and snapped back that six weeks would be � ne and that if he (the patient) had any problems he could just return and be seen in the walk-in clinic, and again rushed away from me. So I cried after him; “the family lives too far and the patient is a girl not a boy!”
A great football player - whose name I
have unfortunately forgotten, was once asked;
“why do you always play with such zeal, passion,
and enthusiasm?” Pointing to the thousands of
people in the stands, he replied; “Football is THE
great American game. These people have paid
a lot of money to see a great game. But more
importantly, there may be just one person in this
entire crowd who is here for the � rst time and
expects to see a great American game. I play for
that person and want to make sure that that one
person sees the game he or she expects.”
In our profession, we see thousands of
ill and injured people. They expect us to be
professional and caring people. Among the many
we see daily, there maybe - by chance - a patient
who is seeing a healthcare provider for the � rst
time. He or she expects full attention from us -
regardless whether the problem is a hangnail or
cardiac arrest - and we must give that person our
full attention. Anything less not only degrades
us individually but the profession as a whole.
In today’s computerized healthcare system,
personal care is being all but forgotten. We are
expected to see patients in rapid succession and
generate a good revenue for the bean counters.
Yet it is our reputation that is on the line. If we
get sued, it is us who face the judge and jury.
The hospital administrator is not going to court
with us. So it behooves us to be vigilant in
providing care to our patients and to assure that

JOPA 25
their perceptions and expectations are answered and met. It’s what makes a PA or NP even more valuable to a particular practice. I hope I am not being pedantic, but I have done this for a very long time and still have most of my original teeth in my head. As my mentor and long time friend of more than forty years; doctor George E. Omer (chief orthopaedic and professor emirate at UNM HSC) use to say; “Listen to me, I have done this for more than � fty years and I have never been sued.” Oh yes, the man who played the violin in the story at the beginning of this article was Joshua Bell, one of the world’s renown violinists of our time and the violin he played on was a three and half million dollar Stradivarius, handmade in 1713. His performance at the subway station in DC was part of a study arranged by The Washington Post. By the way, the DC people never let him forget that inattention, so on September 30 of this year, he returned to DC in the main hall of Union Station. This time he played for a large and engaged audience. Bell says he performs best when all the pressure is on. “When hundreds of people are paying hundreds of dollars to hear him play music that is hundreds of years old. It warrants perfection.” That is what I feel about performing
medicine. The person trusting you with his medical problem needs to see the hundred years of accumulated knowledge of medicine passed on to you by your educators to play magic in treating him or her. That happens by you showing a little concern about his or her problem. When you rush in and rush out without even noticing whether the patient is male or female, … well you can see how that could vex people!

26 JOPA
QUIZ - TRAUMA -
-
- -
-
QUIZQUIZQUIZ CORNER CORNER CORNER --- TRAUMATRAUMATRAUMA
-
-
-
-
Quiz corner is brought to you in partnership by the American
Association of Surgical Physician Assistants (AASPA)
www.AASPA.com

JOPA 27
-
-
-
QUIZQUIZQUIZ CORNER CORNER CORNER --- TRAUMATRAUMATRAUMA
'