Embed Size (px)
Citation preview
Journal Club 2008.3.27
Clinical Review: Adrenocortical Carcinoma: Clinical Update
Bruno Allolio and Martin Fassnacht
Endocrinology and Diabetes Unit, Department of Medicine I, University Hospital Wuerzburg, 97080 Wuerzburg, Germany
The Journal of Clinical Endocrinology & Metabolism 2006 91(6): 2027-2037.

Epidemiology incidence adrenal tumor: at least 3%, over age of 50 yr adrenocortical carcinoma: 1-2 per 1 million age distribution: bimodal first peak childhood second peak forth and fifth decadeExceptionally high annual incidence in southern Brazil 3.4-4.2 per 1 million children vs. an estimated worldwide incidence of 0.3 per 1 million
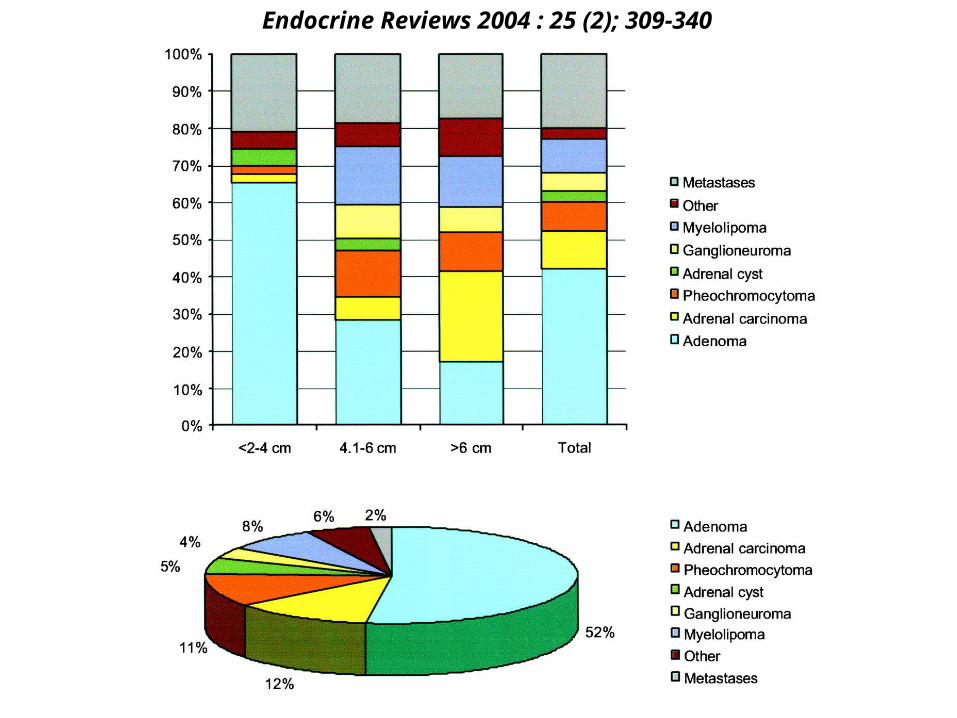
Endocrine Reviews 2004 : 25 (2); 309-340

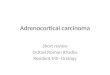
副腎偶発腫瘍、原因別頻度
51
11.7
4.3
0.2
0.6
8.7
3.8
4
3.6
1.4
2.3
1.6
ホルモン非産生腺腫コルチゾール産生腺腫アルドステロン産生腺腫アンドロゲン産生腺腫その他腺腫褐色細胞腫悪性腫瘍骨転移過形成骨髄脂肪腫癌のう胞神経節神経腫
厚生労働省「副腎ホルモン産生異常に関する研究班」
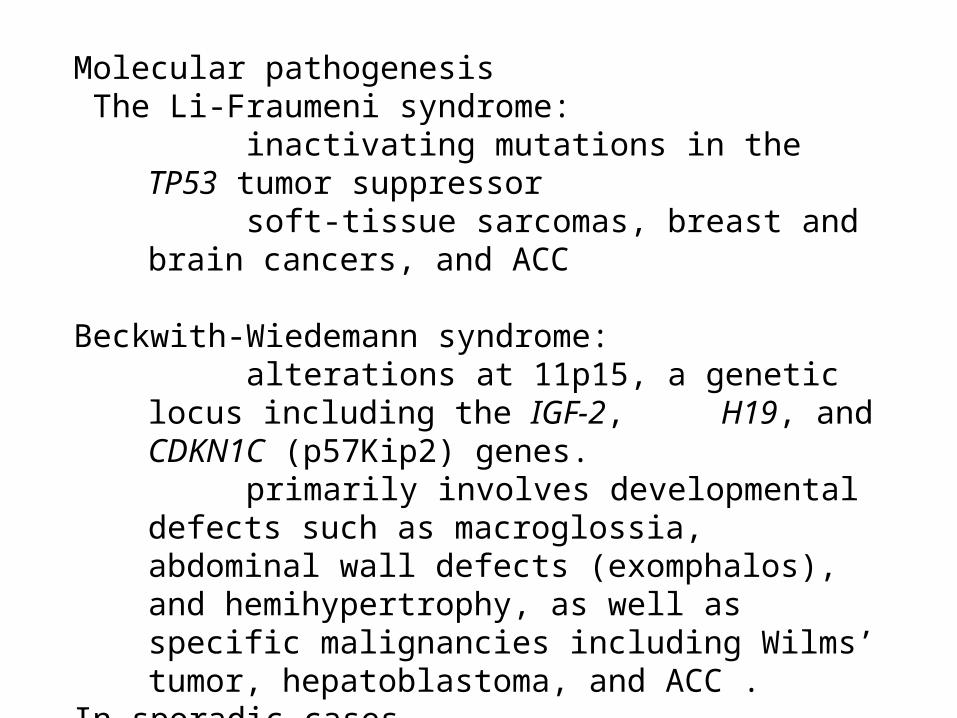
Molecular pathogenesis The Li-Fraumeni syndrome: inactivating mutations in the TP53 tumor suppressor soft-tissue sarcomas, breast and brain cancers, and ACC
Beckwith-Wiedemann syndrome: alterations at 11p15, a genetic locus including the IGF-2,
H19, and CDKN1C (p57Kip2) genes. primarily involves developmental defects such as
macroglossia, abdominal wall defects (exomphalos), and hemihypertrophy, as well as specific malignancies including Wilms’ tumor, hepatoblastoma, and ACC .
In sporadic cases loss of 17p and structural rearrangement of 11p15
(typically with resultant IGF-II overexpression) were both strongly associated with the malignant phenotype
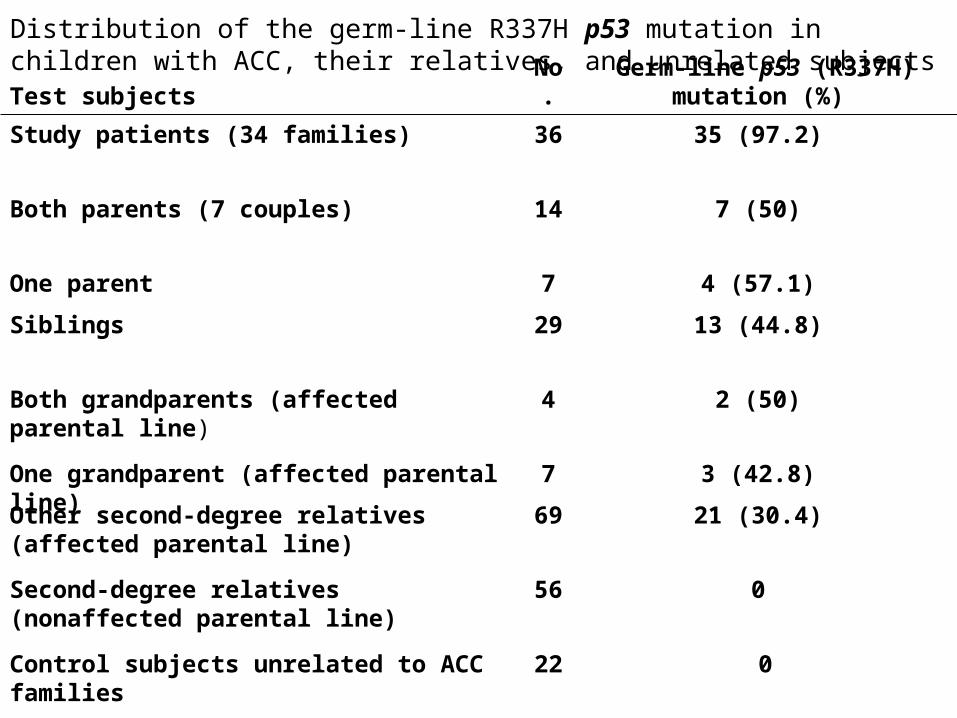
Test subjectsNo.
Germ-line p53 (R337H) mutation (%)
Study patients (34 families) 36 35 (97.2)
Both parents (7 couples) 14 7 (50)
One parent 7 4 (57.1)
Siblings 29 13 (44.8)
Both grandparents (affected parental line) 4 2 (50)
One grandparent (affected parental line) 7 3 (42.8)
Other second-degree relatives (affected parental line)
69 21 (30.4)
Second-degree relatives (nonaffected parental line)
56 0
Control subjects unrelated to ACC families 22 0
Distribution of the germ-line R337H p53 mutation in children with ACC, their relatives, and unrelated subjects
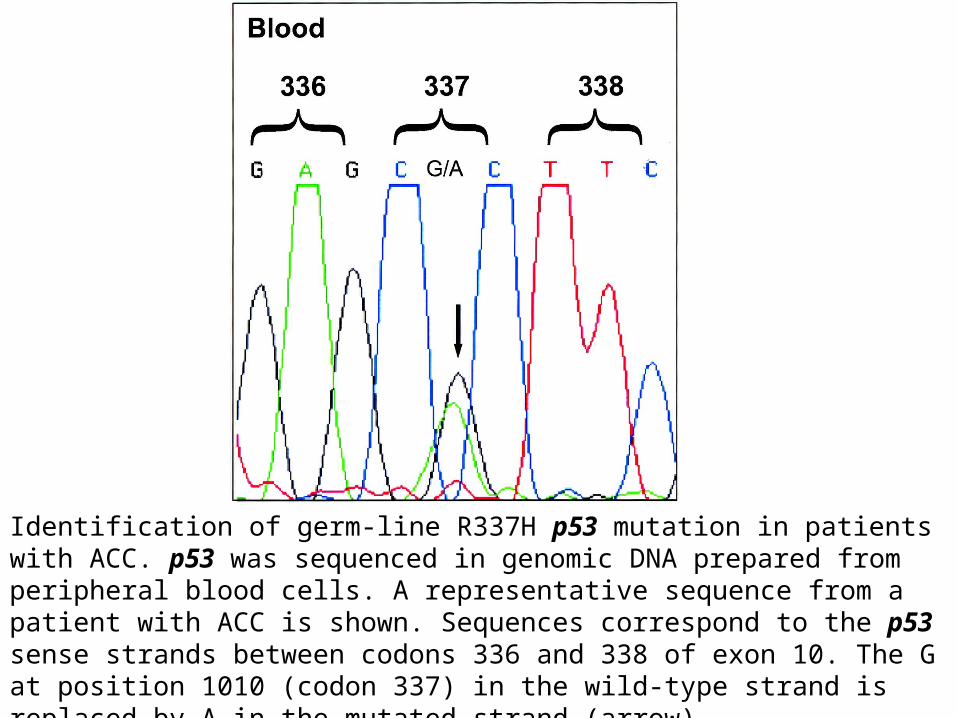
Identification of germ-line R337H p53 mutation in patients with ACC. p53 was sequenced in genomic DNA prepared from peripheral blood cells. A representative sequence from a patient with ACC is shown. Sequences correspond to the p53 sense strands between codons 336 and 338 of exon 10. The G at position 1010 (codon 337) in the wild-type strand is replaced by A in the mutated strand (arrow). PNAS | July 31, 2001 | vol. 98 | no. 16 | 9330-9335
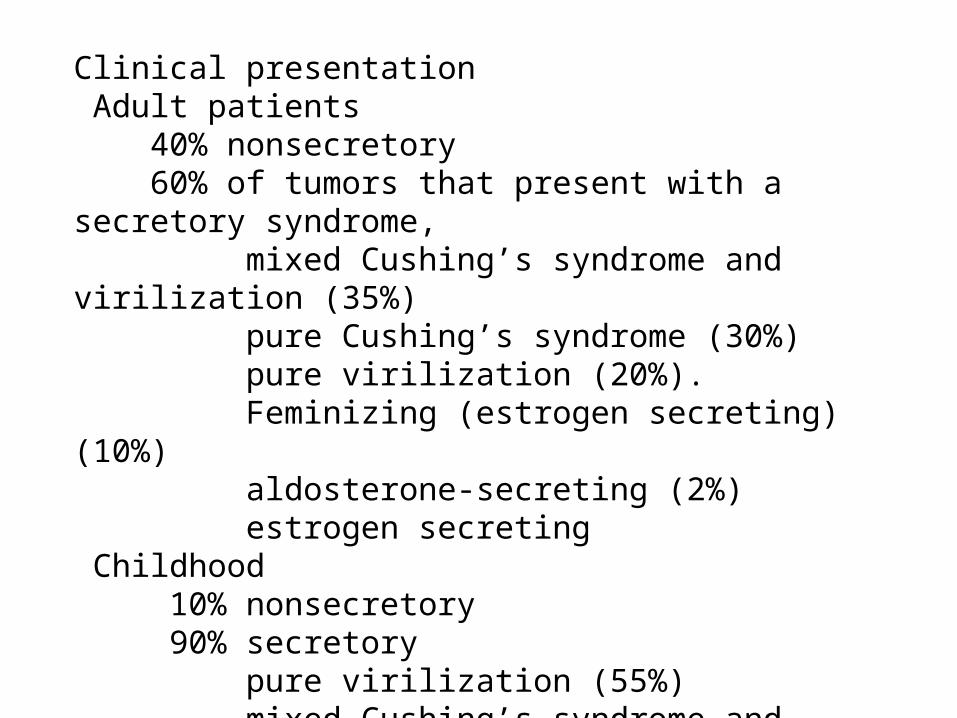
Clinical presentation Adult patients 40% nonsecretory 60% of tumors that present with a secretory syndrome, mixed Cushing’s syndrome and virilization (35%) pure Cushing’s syndrome (30%) pure virilization (20%). Feminizing (estrogen secreting) (10%) aldosterone-secreting (2%) estrogen secreting Childhood 10% nonsecretory 90% secretory pure virilization (55%) mixed Cushing’s syndrome and virilization (30%) Pure Cushing’s syndrome (fewer than 5%)
Diagnosis
Hormonal work-up
Imaging CT, MRI (chemical shift), scintigraphy,
FDG-PET, 11C-metomidate-PET
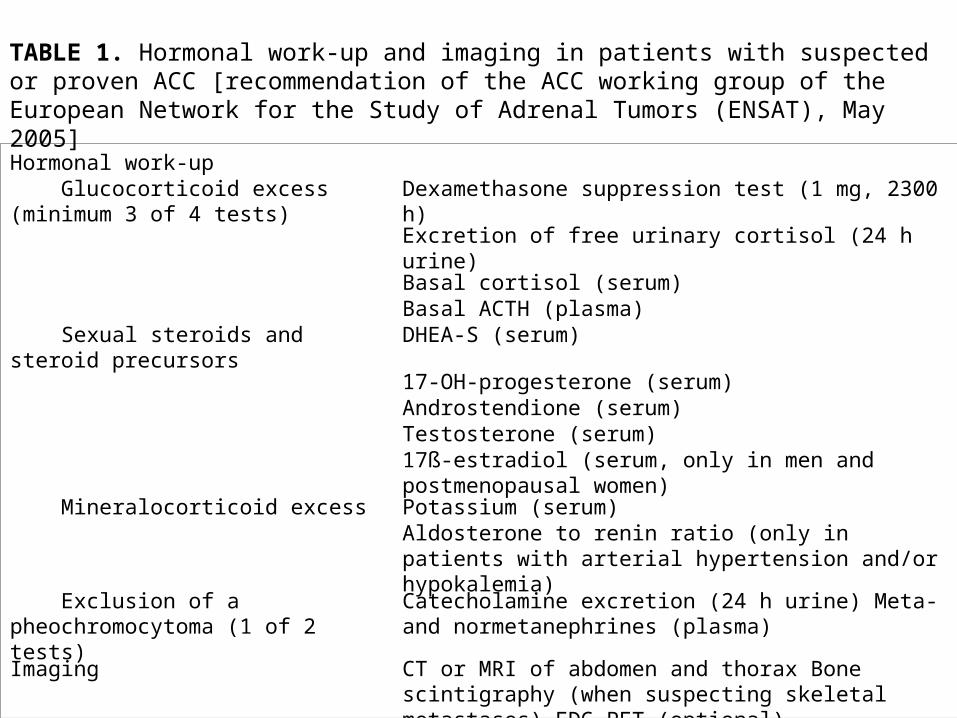
Hormonal work-up Glucocorticoid excess (minimum 3 of 4 tests)
Dexamethasone suppression test (1 mg, 2300 h)
Excretion of free urinary cortisol (24 h urine)
Basal cortisol (serum)Basal ACTH (plasma)
Sexual steroids and steroid precursors DHEA-S (serum)
17-OH-progesterone (serum)Androstendione (serum)Testosterone (serum)17ß-estradiol (serum, only in men and postmenopausal women)
Mineralocorticoid excess Potassium (serum)Aldosterone to renin ratio (only in patients with arterial hypertension and/or hypokalemia)
Exclusion of a pheochromocytoma (1 of 2 tests)
Catecholamine excretion (24 h urine) Meta- and normetanephrines (plasma)
Imaging CT or MRI of abdomen and thorax Bone scintigraphy (when suspecting skeletal metastases) FDG-PET (optional)
TABLE 1. Hormonal work-up and imaging in patients with suspected or proven ACC [recommendation of the ACC working group of the European Network for the Study of Adrenal Tumors (ENSAT), May 2005]
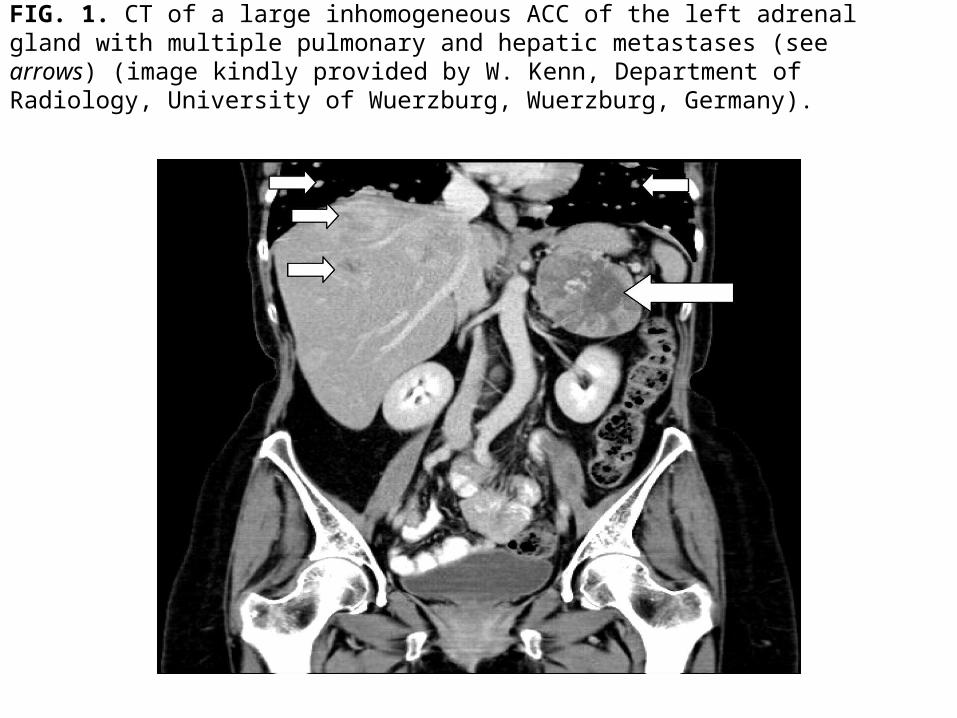
FIG. 1. CT of a large inhomogeneous ACC of the left adrenal gland with multiple pulmonary and hepatic metastases (see arrows) (image kindly provided by W. Kenn, Department of Radiology, University of Wuerzburg, Wuerzburg, Germany).

Radiological panel of an adrenal cortical adenoma. Findings in a 66-yr-old woman with a history of breast cancer. Panels A and B demonstrate the use of CT for calculation of the relative enhancement washout. A, The contrast-enhanced CT shows a left-sided 1.5-cm adrenal mass (arrow) with a mean attenuation of 32.9 HU. B, On the 12-min delayed image, the attenuation of the left adrenal (arrow) is 12.9 HU. The relative enhancement washout is calculated using the following equation: percentage of relative enhancement washout = (1 – delayed enhanced HU value/initial enhanced HU value) x 100. With a relative washout of (1 – 12.9 /32.9) x 100 = 61%, the delayed enhanced CT is indicative of an adrenal adenoma (196 215 ). Panels C and D depict the decrease in signal intensity in adrenal cortical adenoma using chemical-shift MRI. C, In the T1-weighted in-phase image, the signal intensity (SI) of the adrenal mass (arrow, SI = 131) is relatively isointense to the liver (L) and of slightly higher intensity than the spleen (S; SI = 93). D, The T1-weighted opposed-phase MRI shows a signal drop in the adrenal mass (arrow, SI = 39) relative to the spleen (S; SI = 110). The adrenal-spleen-ratio (ASR) is calculated by the following formula (Refs. 238 and 239 ): ASR = [(SI adrenal mass/SI spleen)opposed-phase/(SI adrenal mass /SI
spleen)in-phase] x 100. The diagnosis of an adenoma is confirmed by an ASR of [(39 /110)/(131 /93)] x 100 = 25.2.
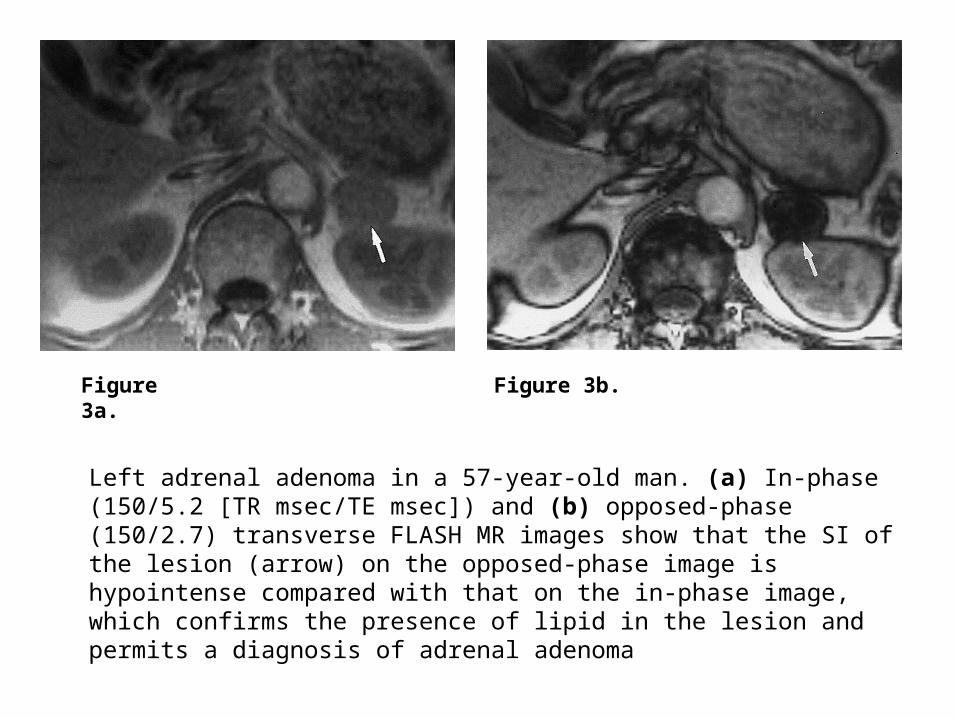
Left adrenal adenoma in a 57-year-old man. (a) In-phase (150/5.2 [TR msec/TE msec]) and (b) opposed-phase (150/2.7) transverse FLASH MR images show that the SI of the lesion (arrow) on the opposed-phase image is hypointense compared with that on the in-phase image, which confirms the presence of lipid in the lesion and permits a diagnosis of adrenal adenoma
Figure 3a. Figure 3b.
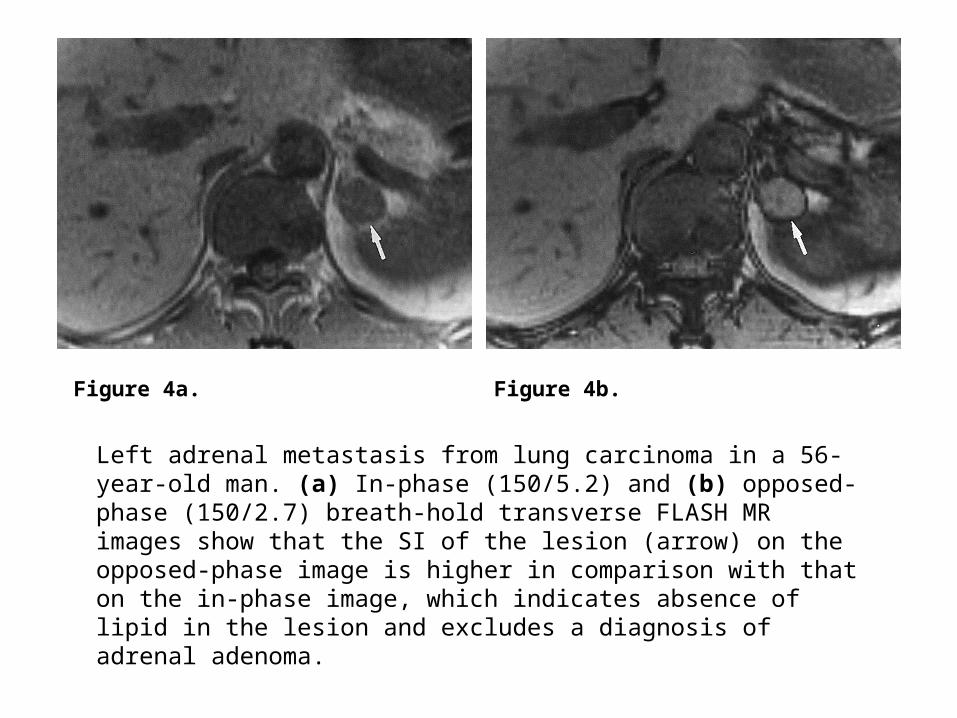
Left adrenal metastasis from lung carcinoma in a 56-year-old man. (a) In-phase (150/5.2) and (b) opposed-phase (150/2.7) breath-hold transverse FLASH MR images show that the SI of the lesion (arrow) on the opposed-phase image is higher in comparison with that on the in-phase image, which indicates absence of lipid in the lesion and excludes a diagnosis of adrenal adenoma.
Figure 4a. Figure 4b.
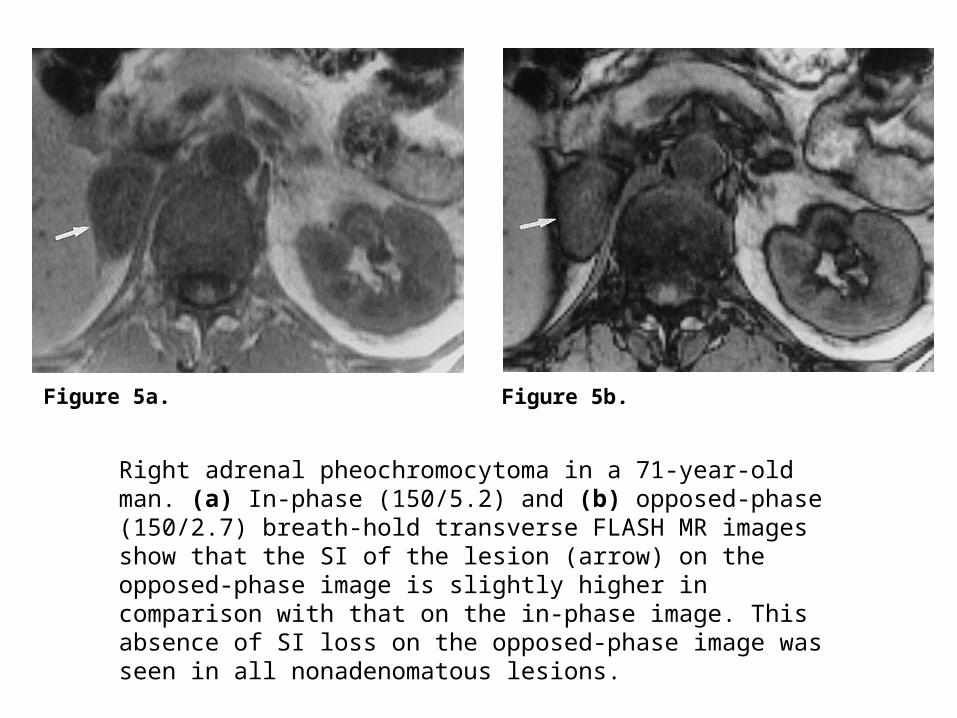
Right adrenal pheochromocytoma in a 71-year-old man. (a) In-phase (150/5.2) and (b) opposed-phase (150/2.7) breath-hold transverse FLASH MR images show that the SI of the lesion (arrow) on the opposed-phase image is slightly higher in comparison with that on the in-phase image. This absence of SI loss on the opposed-phase image was seen in all nonadenomatous lesions.
Figure 5a. Figure 5b.
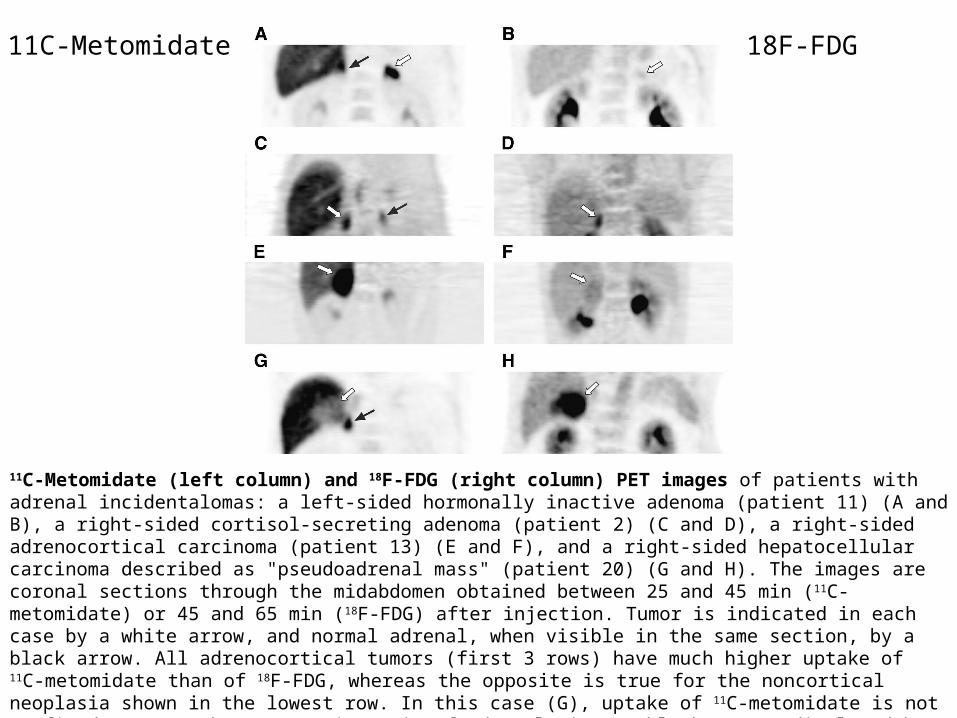
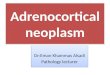
11C-Metomidate (left column) and 18F-FDG (right column) PET images of patients with adrenal incidentalomas: a left-sided hormonally inactive adenoma (patient 11) (A and B), a right-sided cortisol-secreting adenoma (patient 2) (C and D), a right-sided adrenocortical carcinoma (patient 13) (E and F), and a right-sided hepatocellular carcinoma described as "pseudoadrenal mass" (patient 20) (G and H). The images are coronal sections through the midabdomen obtained between 25 and 45 min (11C-metomidate) or 45 and 65 min (18F-FDG) after injection. Tumor is indicated in each case by a white arrow, and normal adrenal, when visible in the same section, by a black arrow. All adrenocortical tumors (first 3 rows) have much higher uptake of 11C-metomidate than of 18F-FDG, whereas the opposite is true for the noncortical neoplasia shown in the lowest row. In this case (G), uptake of 11C-metomidate is not confined to tumor but occurs in a rim of adrenal tissue (black arrow) displaced by the mass. Initially, the high 18F-FDG uptake of the adenoma in 1 d was misjudged as metastasis, with an average SUV of 3.9 (maximum, 6). Liver has invariably high uptake of 11C-metomidate, and tracer excreted in the urinary tract presents the highest radioactivity in 18F-FDG images.
18F-FDG11C-Metomidate
Pathological Assessment
Weiss score nuclear atypia atypical and frequent mitosis ( more than five of 50 high-
power fields) vascular and capsular invasion necrosis
Normal (n = 38) ACC (n = 38) P No. %
Negative< .001
.09
< .001
< .001
.54
NA
NA
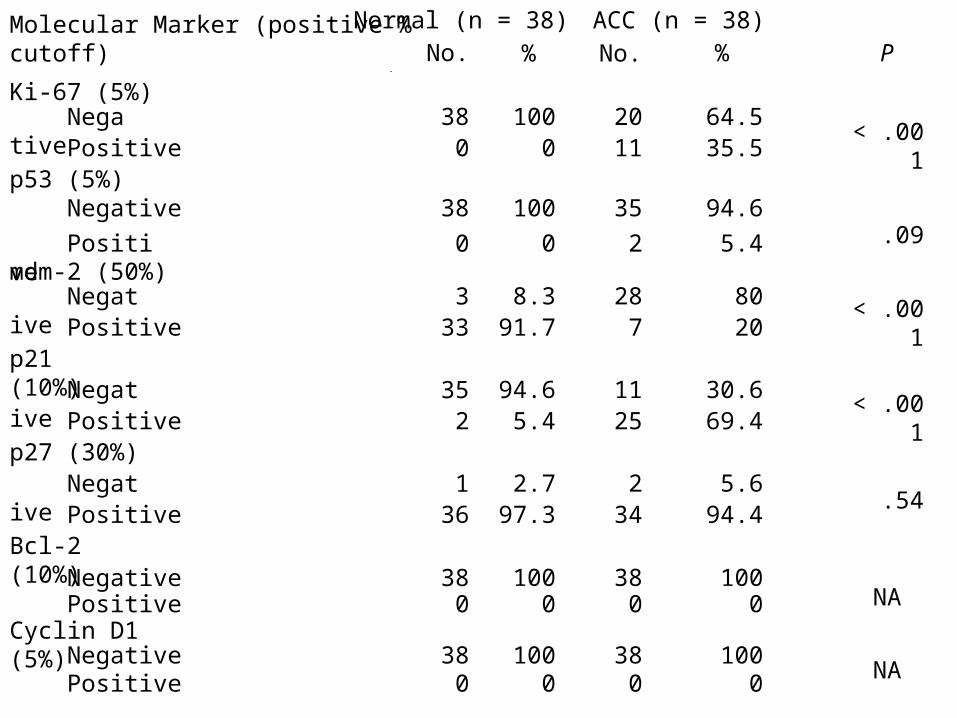
Molecular Marker (positive % cutoff)
Ki-67 (5%)
Positivep53 (5%) Negative
Positivemdm-2 (50%) Negative Positivep21 (10%) Negative Positivep27 (30%) Negative PositiveBcl-2 (10%) Negative PositiveCyclin D1 (5%) Negative Positive
No.
380
38
0
333
352
136
380
380
%
1000
100
0
8.391.7
94.65.4
2.797.3
1000
1000
2011
35
2
287
1125
234
380
380
64.535.5
94.6
5.4
8020
30.669.4
5.694.4
1000
1000
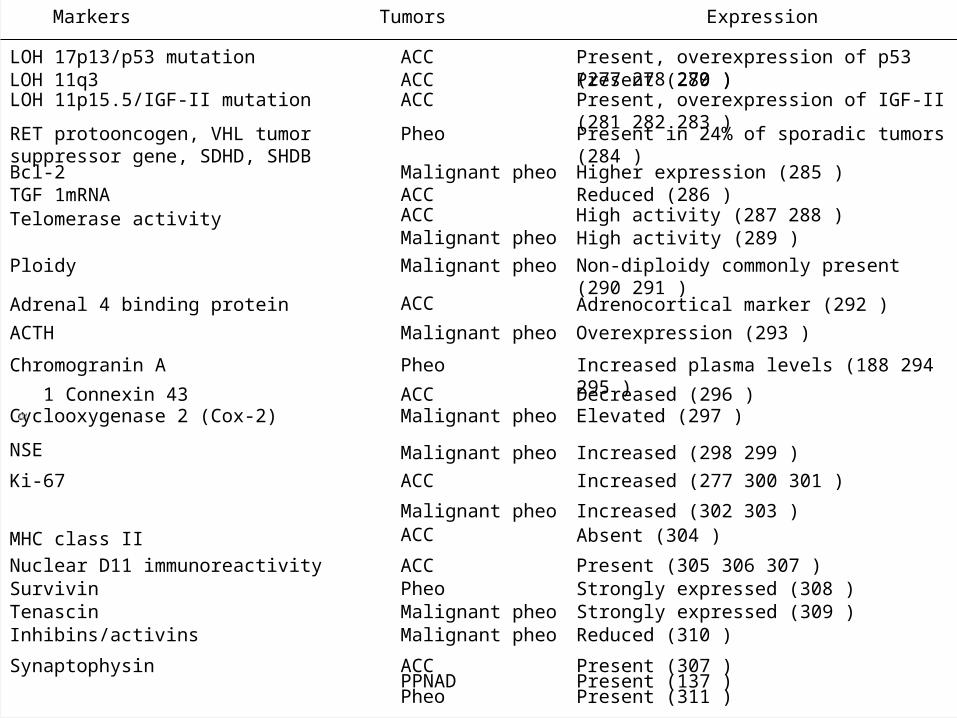
Tumors ExpressionMarkers
LOH 17p13/p53 mutation ACC Present, overexpression of p53 (277 278 279 )LOH 11q3 ACC Present (280 )LOH 11p15.5/IGF-II mutation ACC Present, overexpression of IGF-II (281 282 283 )
RET protooncogen, VHL tumor suppressor gene, SDHD, SHDB
Pheo Present in 24% of sporadic tumors (284 )
Bcl-2 Malignant pheo Higher expression (285 )TGF 1mRNA ACC Reduced (286 )Telomerase activity ACC High activity (287 288 )
Malignant pheo High activity (289 )
Ploidy Malignant pheo Non-diploidy commonly present (290 291 )
Adrenal 4 binding protein ACC Adrenocortical marker (292 )
ACTH Malignant pheo Overexpression (293 )
Chromogranin A Pheo Increased plasma levels (188 294 295 )
1 Connexin 43 ACC Decreased (296 )Cyclooxygenase 2 (Cox-2) Malignant pheo Elevated (297 )
NSE Malignant pheo Increased (298 299 )
Ki-67 ACC Increased (277 300 301 )
Malignant pheo Increased (302 303 )
MHC class II ACC Absent (304 )
Nuclear D11 immunoreactivity ACC Present (305 306 307 )Survivin Pheo Strongly expressed (308 )Tenascin Malignant pheo Strongly expressed (309 )Inhibins/activins Malignant pheo Reduced (310 )
Synaptophysin ACCPPNADPheo
Present (307 )Present (137 )Present (311 )

Staging
The new Union International Cotre Cancer (UICC) staging system
Stage Ⅰ: ≦5cmStage : >5cmⅡStage : local invasion or regional lymph node metastasisⅢStage : invading adjacent organs or distant metastasisⅣ
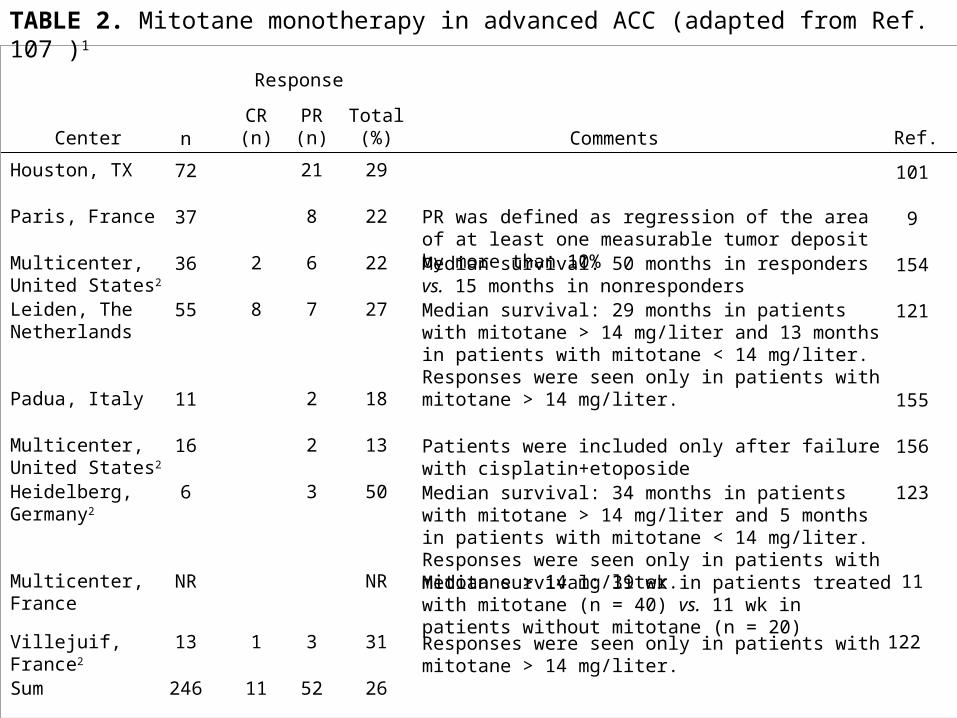
Response
Ref.CR (n)
PR (n)
Total (%)
Houston, TX 21 29
8 22
2 6 22
8 7 27
2 18
2 13
3 50
NR
1 3 31
Comments
PR was defined as regression of the area of at least one measurable tumor deposit by more than 10%Median survival: 50 months in responders vs. 15 months in nonrespondersMedian survival: 29 months in patients with mitotane > 14 mg/liter and 13 months in patients with mitotane < 14 mg/liter. Responses were seen only in patients with mitotane > 14 mg/liter.
Patients were included only after failure with cisplatin+etoposideMedian survival: 34 months in patients with mitotane > 14 mg/liter and 5 months in patients with mitotane < 14 mg/liter. Responses were seen only in patients with mitotane > 14 mg/liter.Median survival: 39 wk in patients treated with mitotane (n = 40) vs. 11 wk in patients without mitotane (n = 20)
Responses were seen only in patients with mitotane > 14 mg/liter.
101
9
154
121
155
156
123
11
122
Center
Paris, France
Multicenter, United States2
Leiden, The Netherlands
Padua, Italy
Multicenter, United States2
Heidelberg, Germany2
Multicenter, France
Villejuif, France2
Sum
n
72
37
36
55
11
16
6
NR
13
246 11 52 26
TABLE 2. Mitotane monotherapy in advanced ACC (adapted from Ref. 107 )1
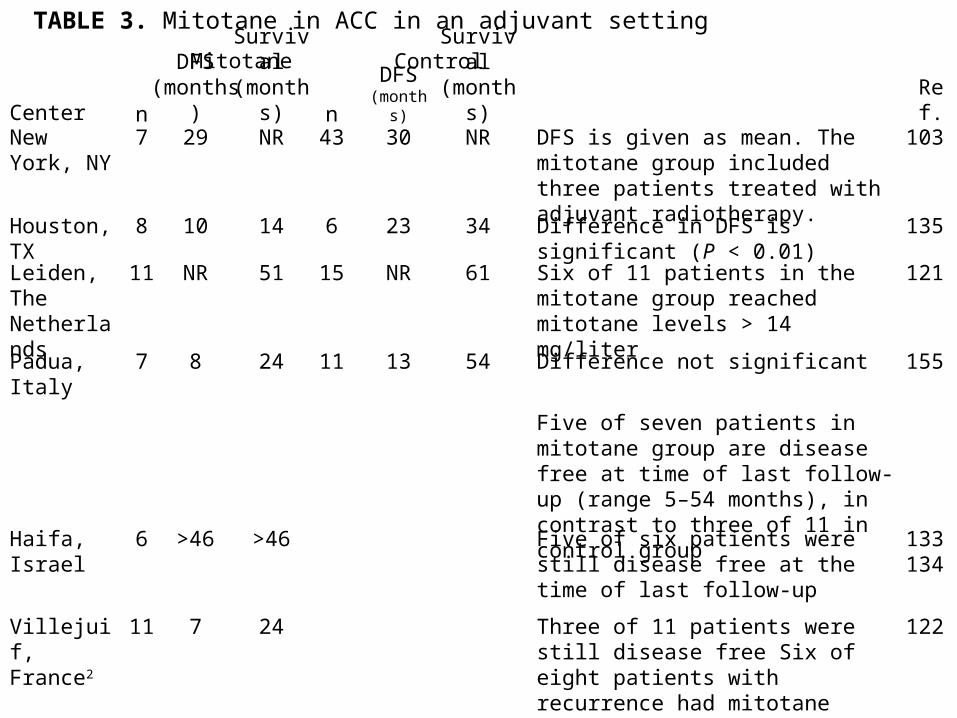
n43
6
15
11
DFS (months)
30
23
NR
13
Survival (months)
NR
34
61
54
CenterNew York, NY
Houston, TX
Leiden, The Netherlands
Padua, Italy
Haifa, Israel
Villejuif, France2
n7
8
11
7
6
11
DFS (months)
29
10
NR
8
>46
7
Survival (months)
NR
14
51
24
>46
24
Mitotane Control
DFS is given as mean. The mitotane group included three patients treated with adjuvant radiotherapy.
Difference in DFS is significant (P < 0.01)Six of 11 patients in the mitotane group reached mitotane levels > 14 mg/liter
Difference not significant
Five of seven patients in mitotane group are disease free at time of last follow-up (range 5–54 months), in contrast to three of 11 in control group
Five of six patients were still disease free at the time of last follow-up
Three of 11 patients were still disease free Six of eight patients with recurrence had mitotane levels > 14 mg/liter
Ref.
103
135
121
155
133 134
122
TABLE 3. Mitotane in ACC in an adjuvant setting

Adverse effect Frequency
Gastrointestinal: nausea, vomiting, diarrhea, anorexia, mucositis Very common
CNS: lethargy, somnolence, vertigo, ataxia confusion, depression, dizziness, decreased memory, polyneuropathy
Very common, common
Adrenal insufficiency Very commonPrimary hypogonadism in men CommonGynecomastia CommonSkin rash CommonAutoimmune hepatitis RareCardiovascular: hypertension Very rareOcular: blurred vision, double vision, toxic retinopathy, cataract, macular edema Very rare
Hemorrhagic cystitis Very rareIncrease of hepatic enzymes (in particular γ-GT) Very commonIncrease in hormone binding globulins (CBG, SHBG, TBG, vitamin D binding protein)
Very common
Disturbance of thyroid parameters (interference with binding of T4 to TBG, total
T4 ↓ )
Very common
Hypercholesterolemia, hypertriglyceridemia Very commonProlonged bleeding timeLeucopenia CommonThrombocytopenia, anemia RareHematuria, albuminuria Very rareHepatic microsomal enzyme induction with increased metabolism of glucocorticoids and other steroids and barbiturates, phenytoin, warfarin
Very common, common
TABLE 4. Adverse effects during mitotane treatment1
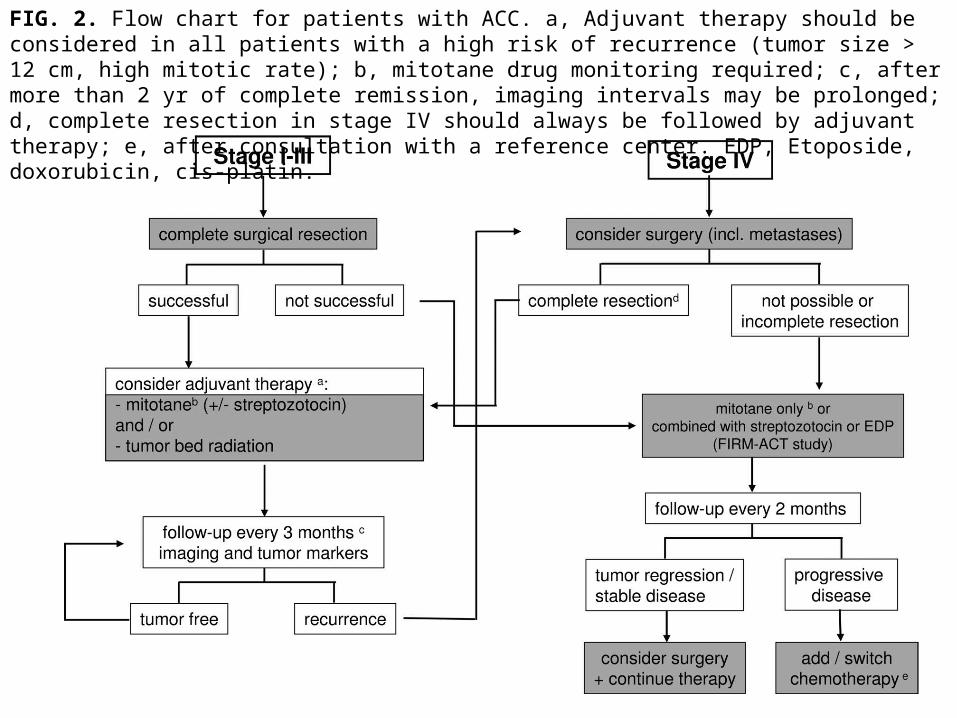
FIG. 2. Flow chart for patients with ACC. a, Adjuvant therapy should be considered in all patients with a high risk of recurrence (tumor size > 12 cm, high mitotic rate); b, mitotane drug monitoring required; c, after more than 2 yr of complete remission, imaging intervals may be prolonged; d, complete resection in stage IV should always be followed by adjuvant therapy; e, after consultation with a reference center. EDP, Etoposide, doxorubicin, cis-platin.
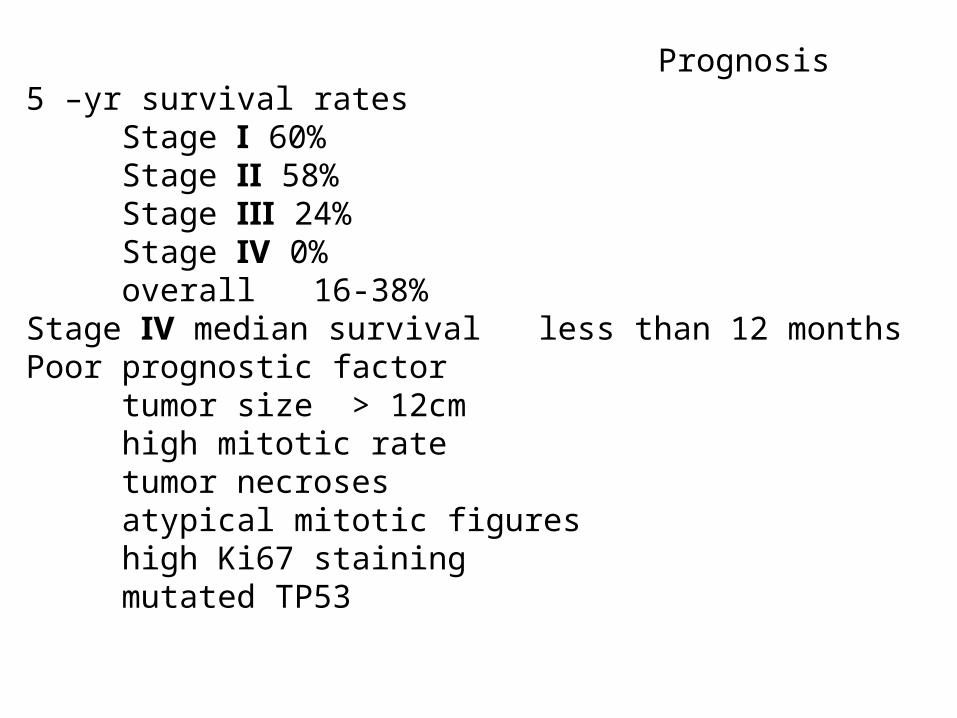
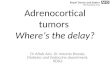
Prognosis5 –yr survival rates Stage Ⅰ 60% Stage Ⅱ 58% Stage Ⅲ 24% Stage Ⅳ 0% overall 16-38%Stage Ⅳ median survival less than 12 monthsPoor prognostic factor tumor size > 12cm high mitotic rate tumor necroses atypical mitotic figures high Ki67 staining mutated TP53
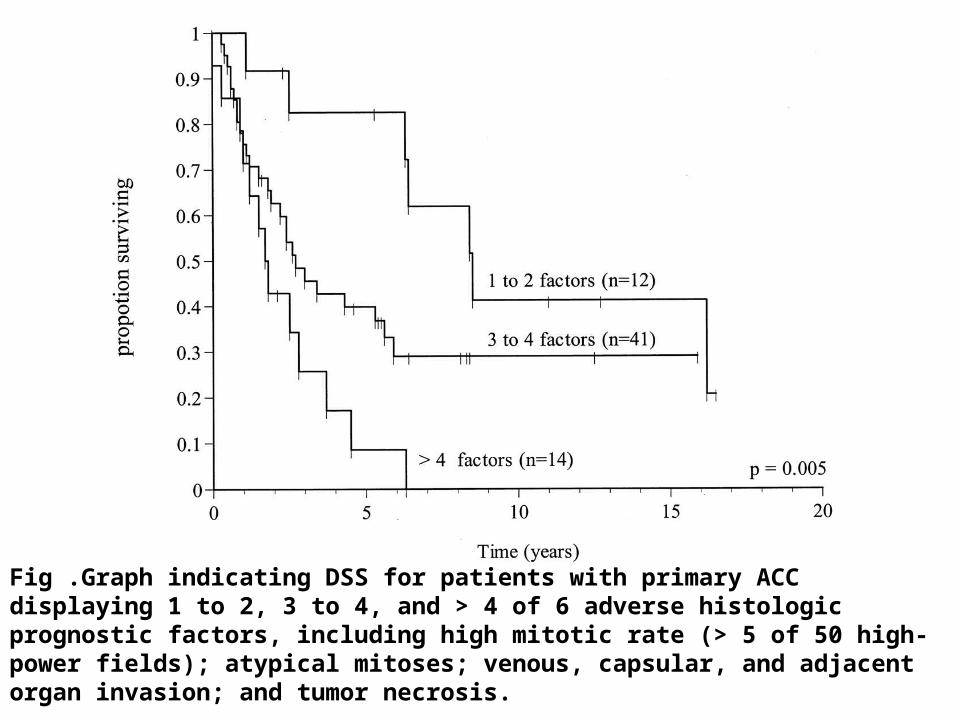
Fig .Graph indicating DSS for patients with primary ACC displaying 1 to 2, 3 to 4, and > 4 of 6 adverse histologic prognostic factors, including high mitotic rate (> 5 of 50 high-power fields); atypical mitoses; venous, capsular, and adjacent organ invasion; and tumor necrosis.

Trial ID Agent Rationale Contact/location
NCT00094497 (FIRM-ACT)
EDP/M vs. SO chemotherapy (Phase III)
Establish best chemotherapeutic regimen
www.firm-act.org
International sites
NCT00071058
Chemotherapy with mitotane and tariquidar (Phase II)
Inhibit multidrug resistance to chemotherapy
Dr. Tito Fojo, National Institutes of Health, Bethesda, MD ([email protected])
DMS 0327
Iressa (Gefitinib) (Phase II)
Inhibit EGFR signaling
Dr. Vivek Samnotra, Norris Cotton Cancer Center, Lebanon, NH ([email protected])
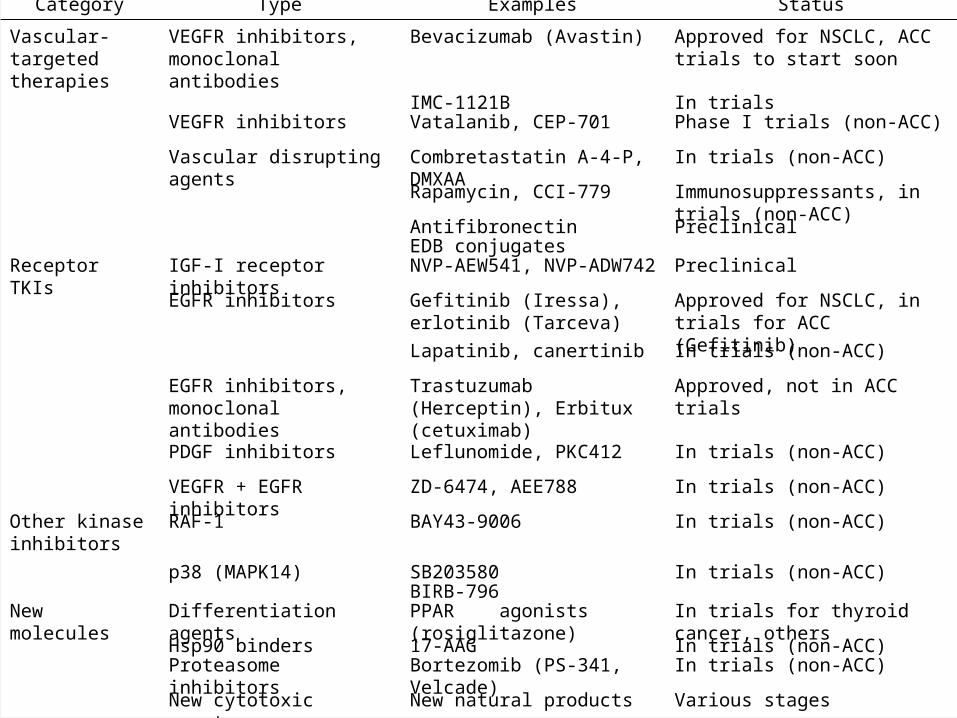
Category Type Examples Status
Vascular-targeted therapies
VEGFR inhibitors, monoclonal antibodies
Bevacizumab (Avastin) Approved for NSCLC, ACC trials to start soon
IMC-1121B In trialsVEGFR inhibitors Vatalanib, CEP-701 Phase I trials (non-ACC)
Vascular disrupting agents Combretastatin A-4-P, DMXAA In trials (non-ACC)
Rapamycin, CCI-779 Immunosuppressants, in trials (non-ACC)
Antifibronectin PreclinicalEDB conjugates
Receptor TKIs IGF-I receptor inhibitors NVP-AEW541, NVP-ADW742 Preclinical
EGFR inhibitors Gefitinib (Iressa), erlotinib (Tarceva)
Approved for NSCLC, in trials for ACC (Gefitinib)
Lapatinib, canertinib In trials (non-ACC)
EGFR inhibitors, monoclonal antibodies
Trastuzumab (Herceptin), Erbitux (cetuximab)
Approved, not in ACC trials
PDGF inhibitors Leflunomide, PKC412 In trials (non-ACC)
VEGFR + EGFR inhibitors ZD-6474, AEE788 In trials (non-ACC)
Other kinase inhibitors
RAF-1 BAY43-9006 In trials (non-ACC)
p38 (MAPK14) SB203580 In trials (non-ACC)BIRB-796
New molecules Differentiation agents PPAR agonists (rosiglitazone) In trials for thyroid cancer, others
Hsp90 binders 17-AAG In trials (non-ACC)Proteasome inhibitors Bortezomib (PS-341, Velcade) In trials (non-ACC)
New cytotoxic agents New natural products Various stages