Embed Size (px)
Citation preview

IN THE NAME OF GOD

Physiopathology of Allergic Diseases
by: Tooba MomenAssistant Professor of Asthma,
Allergy & Immunology

1. There has been a steady increase in the prevalence of
allergic diseases globally.
2. It is estimated that 30-40% of the world population is
now affected by one or more allergic conditions.
3. A high proportion of the increase in allergic disease is in
young people. In the near future, the burden of allergic
diseases is expected to greatly increase as these
patients become adults.
Why is allergy a major problem worldwide?

Allergy=Hypersensitivity– An exaggerated response by the immune system to a
foreign substance
Atopy
• Inherited tendency to produce increased amounts of IgE in response to small quantities of allergen, and to produce a clinical syndrome = Allergy + Clinical disease entity

Allergen
any antigen that causes allergy. The allergen is either inhaled or ingested and is then processed by the dendritic cell, an antigen-presenting cell. It can be complete protein antigens or low molecular weight proteins capable of eliciting an IgE response.
Allergic rhinitis, allergic athma, atopic dermatitis are the most common manifestation of atopy. These manifestation may coexist in the same patients at different times. → Atopic march

Hypersensitivity (hypersensitivity reaction) refers to undesirable immune reactions produced by the normal immune system.
Hypersensitivity reactions require a pre-sensitized (immune) state of the host.
Hypersensitivity

The Hypersensitivity Reactions
• Type I: Immediate→ IgE & IgG4
• Type II: Cytotoxic→ IgG & IgM
• Type III: Immune complex→ Ag, Ab complex
• Type IV: Delayed → T cell
Gell & Coombs

Hypersensitivity Reactions

• Type I hypersensitivity (immediate) • The primary cellular component in
this hypersensitivity is the mast cell or basophil. The reaction is amplified and/or modified by platelets, neutrophils and eosinophils
• The reaction may involve skin (urticaria and angioedema), eyes (conjunctivitis), nasopharynx (rhinorrhea, rhinitis), bronchopulmonary tissues (asthma) and gastrointestinal tract (gastroenteritis).

While first-time exposure may only produce a mild reaction, repeated exposures may lead to more serious reactions. Once a person is sensitized (has had a previous sensitivity reaction), even a very limited exposure to a very small amount of allergen can trigger a severe reaction.
Most occur within seconds or minutes after exposure to the allergen, but some can occur after several hours, particularly if the allergen causes a reaction after it is partially digested.
Mechanism

• The pathophysiology of allergic responses can be divided into two phases.
• Acute or early response that occurs immediately after exposure to an allergen.
• “late phase reaction” which can substantially prolong the symptoms of a response, and result in tissue damage.

The major mediators: Preformed mediators:
– Histamine is one well-known mediator. – Mediators have effects on local tissue and organs in addition to
activating more white blood cell defenders. It is these effects that cause the symptoms of the reaction.
– If the release of the mediators is sudden or extensive, the allergic reaction may also be sudden and severe.
– The actions of the mediators can cause variable clinical responses depending on which organ systems affected.
Histamine: This mediator acts on histamine 1 (H1) and histamine 2 (H2) receptors to cause: contraction of smooth muscles of the airway and GI tract, increased vasopermeability and vasodilation, nasal mucus production, airway mucus production, pruritus, cutaneous vasodilation, and gastric acid secretion.

Tryptase: Tryptase is a major protease released by mast cells; its exact role is uncertain, but it can cleave C3 and C3a. Tryptase is found in all human mast cells but in few other cells and thus is a good marker of mast cell activation.
Proteoglycans: Proteoglycans include heparin and chondroitin sulfate. The role is unknown; heparin seems to be important in storing the preformed proteases and may play a role in the production of alpha-tryptase.
Chemotactic factors: An eosinophilic chemotactic factor of anaphylaxiscauses eosinophil chemotaxis; an inflammatory factor of anaphylaxisresults in neutrophil chemotaxis. Eosinophils release major basicprotein and, together with the activity of neutrophils, cause significanttissue damage in the later phases of allergic reactions.


•Type II hypersensitivity is also known as cytotoxic hypersensitivity and may affect a variety of organs and tissues. e.g. Drug-induced hemolytic anemia, granulocytopenia and thrombocytopenia .
•Type II hypersensitivity is primarily mediated by antibodies of the IgM or IgG classes and complement. Phagocytes may also play a role (ADCC) .The lesion contains antibody, complement and neutrophils.

Type III Hypersensitivity
It is mediated by soluble immune complexes. They are mostly of the IgG class, although IgM may also be involved. •The antigen may be exogenous or endogenous (non-organ specific autoimmunity: e.g.,systemic lupus erythematosus, SLE). The antigen is soluble and not attached to the organ involved.
•Primary components are soluble immune complexes and complement (C3a, 4a and 5a). The damage is caused by platelets and neutrophils. The lesion contains primarily neutrophils and deposits of immune complexes and complement. Macrophages infiltrating in later stages may be involved in the healing process.

•Type IV hypersensitivity is also known as cell mediated or delayed type hypersensitivity. •e.g. Tuberculin reaction which peaks 48 hours after the injection of antigen (PPD) or (old tuberculin). The lesion is characterized by induration and erythema.
•Type IV hypersensitivity is involved in the pathogenesis of many autoimmune and infectious diseases (tuberculosis, leprosy, blastomycosis, histoplasmosis, toxoplasmosis, leishmaniasis, ……..) and granulomas due to infections and foreign antigens. Another form of delayed hypersensitivity is contact dermatitis (poison ivy , chemicals, heavy metals, etc.) in which the lesions are more papular.

Hygiene Hypothesis










Primary Allergic Conditions
Allergic rhinitis (AR) Seasonal allergic rhinitis (SAR) Perennial allergic rhinitis (PAR) Sinusitis Urticaria & Angioedema Atopic dermatitis (AD) Allergic asthma (AA)

Asthma

Definition -Defined by the Global Initiative on Asthma as follows:
a chronic inflammatory disorder of the airways in which many cells and cellular elements play a role. The chronic inflammation is associated with airway hyperresponsiveness that leads to recurrent episodes of wheezing, breathlessness, chest tightness and coughing, particularly at night or early in the morning. These episodes are usually associated with widespread, but variable, airflow obstruction within the lung that is often reversible either spontaneously or with treatment.’
In patients with suggestive symptoms the diagnosis of asthma requires the demonstration of the disease's main physiological characteristics, such as variable airway obstruction or hyperresponsiveness.


Asthma: Pathophysiology
• Inflammatory cell infiltrate consists of mainly of eosinophils and lymphocytes
• Denudation of airway epithelium• Mucus gland hyperplasia and
hypersecretion• Smooth muscle cell hyperplasia• Submucosal edema and vascular dilatation• Fibrin deposition/airway remodeling



NAEPP, EPR-3, pg. 15.
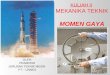
FACTORS LIMITING AIRFLOW IN ACUTE AND PERSISTENT ASTHMA

Epithelial damage
Airway smooth muscle
Inflammatory cell infiltration
Vascular dilatation
Mucous gland hypertrophy
Edema
Mucus
Thickening of basement membrane
Adapted from National Asthma Education and Prevention Program. Expert Panel Report: Guidelines for the diagnosis and management of asthma. NHLBI, NIH. 1991.
Pathologic airway changes induced in asthma

• Mast Cells
• Macrophages
• Eosinophils
• T-Lymphocytes
• Epithelial Cells
• Platelets
• Neutrophils
• Myofibroblasts
• Basophils
Multiple Mechanisms Contribute to Asthma: Inflammatory Mediators
HistamineLipid Mediators*
Peptides†
Cytokines‡
Growth Factors
MediatorSoup
Bronchoconstriction
Microvascular Leakage
Mucus Hypersecretion
AirwayHyperresponsiveness
*For example, prostaglandins and leukotrienes.†For example, bradykinin and tachykinin.‡For example, tumor necrosis factor (TNF).
Adapted with permission from Barnes PJ. In: Barnes PJ et al, eds. Asthma: Basic Mechanisms and Clinical Management. 3rd ed. Academic Press; 1998:487-506.

Epithelial Damage in Asthma
AsthmaticNormal

Lumen
Epithelium
Subepithelial Collagen Deposition
Consequences of Persistent Asthma:Subepithelial Collagen Deposition
Reprinted with permission from Holloway L et al. In: Busse WW, Holgate ST, eds. Asthma and Rhinitis. Blackwell Scientific Publications; 1995:109-118.

Consequences of Persistent Asthma: Smooth Muscle Hyperplasia
Reprinted with permission from Solway J et al. CG. N Engl J Med. 2007;356:1367-1369.
Normal Airway Asthmatic Airway

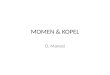
FEV 1 %
Pre
dict
ed
Duration of Asthma (years)
80
40
120
10 20 5040300
r = -0.47n = 89
P<.001
60
20
100
Consequences of Persistent Asthma: Progressive Decline in FEV1
FEV1 = forced expiratory volume in 1 second.
Adapted with permission from Brown PJ et al. Thorax. 1984;39:131-136.

• Most likely a complex interaction between– Host Factors/Predisposition– Environmental Challenges
Etiology Asthma?


Environmental Risk Factors for Development of asthma
• Indoor allergens• Outdoor allergens• Occupational
sensitizers• Tobacco smoke• Air Pollution• Respiratory Infections

Asthma Symptoms
Symptoms may include:
Coughing
Wheezing
Chest tightness
Shortness of breath
Excessive fatigue

Key symptom indicators for considering a diagnosis of asthma
Wheezing
History of any following Cough Recurrent wheeze Recurrent difficulty breathing Recurrent chest tightness
Symptoms occur or worsen in presence of trigger
Symptom occur or worsen at night, waking the patient

Features isn't favor of asthma
Symptom starting at or shortly after birth
FTT
Complete failure to respond to anti asthmatic medication
Continuous wheezing
No association with typical trigger

DIAGNOSIS OF ASTHMA
• History and patterns of symptoms
• Physical examination
• Measurements of lung function

Physical Examination
During routine clinic visits, commonly present without abnormal signs, which stresses the importance of the medical history in diagnosing asthma.
Some may exhibit a dry, persistent cough.
The chest examination is often normal. Deeper breaths can sometimes elicit otherwise undetectable wheezing.
In clinic, quick resolution (within 10 min) or convincing improvement in symptoms and signs of asthma with administration of a short-acting inhaled beta-agonist (SABA [albuterol]) is supportive of the diagnosis of asthma.

Physical Examination
During asthma exacerbation Expiratory wheezing and a prolonged expiratory phase can
usually be appreciated by auscultation.
Crackles (or rales) and rhonchi can sometimes be heard, resulting from excess mucus production and inflammatory exudate in the airways.
The combination of segmental crackles and poor breath sounds can indicate lung segmental atelectasis that is difficult to distinguish from bronchial pneumonia and can complicate acute asthma management.

In severe exacerbations
-inspiratory and expiratory wheezing,
-increased prolongation of exhalation,
-poor air entry, suprasternal and intercostal retractions,
-nasal flaring, and accessory respiratory muscle use.
-In extremis, airflow may be so limited that wheezing cannot be heard.

Allergic Rhinitis

Background
• Rhinitis is defined as inflammation of the nasal membranes and is characterized by a symptom complex that consists of any combination of the following:
• sneezing, nasal congestion, nasal itching, and rhinorrhea.
• Allergic rhinitis is the most common cause of rhinitis.

Pathophysiology
• Type I immediate hypersensitivity reaction mediated by IgE antibodies, which trigger the
mast cells and basophils to release pharmacologically active agents.




CLINICAL
• "Allergic shiners" • "Nasal crease" (allergic
salute).• Nasal
examination :swollen (boggy), pale, blue-gray mucosa

Diagnosis of Allergic Rhinitis
1. History & symptoms of recurrent or persistent rhinitis and/or associated health effects
2. Signs of atopy and recurrent or persistent rhinitis3. Demonstration of IgE allergy4. Exclusion of other causes of rhinitis

Co-morbid conditions• Patients with allergic rhinitis may have other atopic conditions such as
asthma or atopic dermatitis.• Look for conditions that can occur as complications of allergic rhinitis.
Sinusitis occurs quite frequently• Other possible complications include otitis media, sleep disturbance or
apnea, dental problems (overbite), and palatal abnormalities.• Nasal polyps occur in association with allergic rhinitis, although whether
allergic rhinitis actually causes polyps remains unclear. • Investigate past medical history, including other current medical
conditions. Diseases such as hypothyroidism or sarcoidosis can cause nonallergic rhinitis.



Management of allergic rhinitis
The management of allergic rhinitis involves the followingcomponents:• Allergen avoidance• Pharmacotherapy.• Allergen immunotherapy. Of note, immunotherapy helps
prevent the development of asthma in children with allergic rhinitis, and thus should be given special consideration in the pediatric population.

sneezing rhinorrhea nasal nasal eyeobstruction itch symptoms
H1-antihistaminesoral +++ +++ 0 to + +++ ++intranasal ++ +++ + ++ 0intraocular 0 0 0 0 +++
Corticosteroids +++ +++ ++ ++ +Cromones
intranasal + + + + 0intraocular 0 0 0 0 ++
Decongestantsintranasal 0 0 ++ 0 0oral 0 0 + 0 0
Anti-cholinergics 0 +++ 0 0 0Anti-leukotrienes 0 + ++ 0 ++
Medications for Allergic Rhinitis - ARIA

Atopic Dermatitis

• atopic eczema is a very common skin disease.
• It affects around 10% of all infants and children.
• The exact cause is not known, but AD results from a combination of family heredity and a variety of conditions in everyday life that triggers the red, itchy rash.

• This type of eczema usually begins during the first year of life and almost always within the first five years.
• It’s seldom present at birth, but it often comes on during the first six weeks. AD tends to persist. It may wax and wane, but it keeps coming back


• Diagnostic criteria for atopic dermatitis (AD) have been proposed by Hanifin and Rajka (1980) and largely adopted by the American Academy of Allergy, Asthma, and Immunology
• Major characteristics : -Pruritus -Typical morphology and distribution (ie, flexural lichenification and linearity in adults, facial and extensor involvement in infants and young children) -Chronic or chronically relapsing dermatitis -Personal or family history of atopy (eg, asthma, allergic rhinoconjunctivitis, atopic dermatitis)

Minor Criteria• Xerosis (dry skin)• Ichthyosis, palmar
hyperlinearity, keratosis pilaris
• Hand dermatitis, foot dermatitis
• Nipple eczema• Susceptibility to cutaneous
infection (eg, with Staphylococcus aureus, herpes simplex virus [HSV], other viruses, warts, molluscum, dermatophytes)
• Pityriasis alba
• Infraorbital fold (eg, Dennie pleat, Morgan fold)
• Keratoconus• Anterior subcapsular
cataracts• Sensitivity to emotional
factors• White dermographism• Immediate type I skin test
response





• The pathogenesis is multifactorial and involves a complex immunologic cascade, including disruption of the epidermal barrier, IgE dysregulation, defects in the cutaneous cell-mediated immune response, and genetic factors.

• The major elements in immune dysregulation are Langerhans' cells, inflammatory dendritic epidermal cells, monocytes, macrophages, lymphocytes, mast cells, and keratinocytes, all of which interact through an intricate cascade of cytokines leading to a predominance of Th2 cells over (Th1 cells).
• The Th2 cytokines, interleukin (IL)-4, IL-5, IL-10, and IL-13, are increased in the skin, and there is a corresponding decrease in Th1 cytokines, mainly interferon-γ and IL-2.

• Patients with atopic dermatitis often have dry, sensitive skin due to changes in the epidermis, which serves as a barrier to the environment by maintaining the water balance of the skin.
• Essential fatty acids (EFAs), such as linoleic and linolenic acid, are important components of the epidermal barrier
• Defects in the epidermal barrier also lead to increased susceptibility to allergens (atopic allergens such as house dust mites, grass, or pollen). When such allergens contact atopic skin, they stimulate Th2 lymphocytes to produce cytokines such as IL-4, IL-5, and IL-13, which in turn promote an increase in IgE synthesis.
• atopic dermatitis patients often have high levels of IgE antibodies to house dust mites and other allergens

• Defective cell-mediated immunity leads to increased susceptibility to many bacterial, viral, and fungal infections of the skin.
• Children with atopic dermatitis are particularly susceptible to severe, widespread herpes simplex virus infection (eczema herpeticum), a systemic and potentially fatal infection affecting primarily areas of active eczema
• More than 90% of patients with atopic dermatitis have S. aureus colonization of lesional skin, and more than 75% have colonization of uninvolved skin.


Urticaria & Angioedema

• Urticaria (hives) is a vascular reaction of the skin marked by the transient appearance of smooth, slightly elevated patches (wheals) that are erythematous and that are often attended by severe pruritus.

Urticaria
hives or wheals may occur and cause significant purities; individual wheals resolve after minutes to hours, but new wheals can continue to form. • Acute urticaria: (lasting <6 wk) can be caused by foods, drugs, or contact
allergens. • Chronic urticaria: lasts longer than 6 weeks.

Urticaria • Common problem!
– Affects up to 20% of the population
1. Pruritic (itch!)2. Blanche with pressure3. -No scarring
Weal &Flare

Angioedema
• Angioedema is localized tissue swelling that can occur in soft tissues throughout the body., which may account for a substantial volume of fluid loss from the intravascular compartment. Patients may report pain at the site of swelling instead of pruritus, which occurs with urticaria.
• Angioedema of the laryngopharynx can obstruct the airway, and patients may
report difficulty breathing. Stridor or hoarseness may be present. It can be life threatening.

Angioedema (Swelling)
• Edema of the deep layers of the dermis and subcutaneous tissue.
1. Non-pitting edema 2. Skin is not hot3. Non-dependent areas
It is not: “pre-tibial pitting edema”

Acute Urticaria
Definition: Hives lasting less than 6 weeks
Common triggers:– Foods *Shellfish, peanut, wheat, egg, fresh fruits, milk
– Infections More common in children
– Animal dander– Pollens– Drugs
Aspirin, NSAIDS, antibiotics
– Occupational– Stinging Insects
Kaplan, A. P. N Engl J Med 2002;346:175-179

Pathophysiology
• Urticaria results from the release of histamine, bradykinin, leukotriene C4, prostaglandin D2, and other vasoactive substances from mast cells and basophils in the dermis.
• These substances cause extravasation of plasma into the dermis, leading to the urticarial lesion. The intense pruritus of urticaria is a result of histamine released into the dermis.

Anaphylaxis

TERMINOLOGYTraditionally, the term anaphylaxis has referred to a systemic, immediate hypersensitivity reaction
caused by immunoglobulin E (IgE)-mediated immunologic release of mediators from mast cells and
basophils. In the past, the term anaphylactoid reaction has been used to refer to a clinically similar
event not mediated by IgE.
A change in terminology was suggested by the World Allergy Organization, which proposed that
anaphylaxis refer to a ‘severe, life threatening, generalized or systemic hypersensitivity reaction.’
They further suggested the term:
allergic anaphylaxis’ be used when this reaction ‘is mediated by an immunologic mechanism, e.g., IgE,
IgG, and immune-complex complement-related.
non-allergic anaphylaxis.’ that anaphylaxis from a non-immunologic reaction .
Therefore, the term ‘anaphylactoid,’ according to this terminology, is being eliminated.

BASOPHIL AND MAST CELL DEGRANULATION SYNDROMES
Histamine and products of arachidonic acid metabolism (leukotrienes, thromboxane, prostaglandins, and platelet-activating factor) Smooth muscle spasm, mucus secretion, vasodilatation, increased vascular
permeability, activation of nociceptive neurons, platelet adherence, eosinophil activation, eosinophil chemotaxis
Neutral proteases
Proteoglycans: heparin, chondroitin sulfate
Chemoattractants
Tumor necrosis factor alpha activates NF-κB