Embed Size (px)
Citation preview

In The Name of God

ANAPHYLAXIS
Tooba Momen; MD; Allergy &Immunology

TERMINOLOGY
Traditionally, the term anaphylaxis has referred to a systemic, immediate hypersensitivity reaction caused by immunoglobulin E (IgE)-mediated immunologic release of mediators from mast cells and basophils. In the past, the term anaphylactoid reaction has been used to refer to a clinically similar event not mediated by IgE.
A change in terminology was suggested by the World Allergy Organization,
which proposed that anaphylaxis refer to a ‘severe, life threatening, generalized or systemic hypersensitivity reaction.’ They further suggested the
term : allergic anaphylaxis’ be used when this reaction ‘is mediated by an immunologic
mechanism, e.g., IgE, IgG, and immune-complex complement-related .non-allergic anaphylaxis.’ that anaphylaxis from a non-immunologic reaction.
Therefore, the term ‘anaphylactoid,’ according to this terminology, is being eliminated.

Visual schemata of change in terminology. (From Simons FER. Anaphylaxis, killer allergy: long-term management in the
community. J Allergy Clin Immunol 2006; 117:367–377.

Critical criteria for diagnosing anaphylaxis Anaphylaxis is highly likely when any one of the following
three criteria fulfilled
1. Acute onset of an illness (minutes to several hours) with involvement of the skin, mucosal tissues, or both (e.g., generalized hives, pruritus or flushing, swollen lips-tongue-uvula) AND AT LEAST ONE OF THE FOLLOWING:
a. Respiratory compromise (e.g., dyspnea, wheeze-bronchospasm, stridor, reduced PEF, hypoxemia)
b. Reduced BP or associated symptoms of end-organ dysfunction (e.g., hypotonia [collapse], syncope, incontinence)

2. Two or more of the following that occur rapidly after exposure to a likely allergen for that patient (minutes to several hours):
a. Involvement of the skin-mucosal tissue (e.g., generalized hives, itch-flush, swollen lips-tongue-uvula)
b. Respiratory compromise (e.g., dyspnea, wheeze-bronchospasm, stridor, reduced PEF, hypoxemia)
c. Reduced BP or associated symptoms of end-organ dysfunction (e.g., hypotonia [collapse], syncope, incontinence)
d. Persistent gastrointestinal symptoms (e.g., crampy abdominal pain, vomiting)

3. Reduced BP after exposure to known allergen for that patient (minutes to several hours) :
a. Infants and children: low systolic BP (age specific)
or greater than 30% decrease in systolic BP [ ]∗
b. Adults: systolic BP of less than 90 mmHg or greater than 30% decrease from their baseline∗
low systolic BP for children is defined as less than 70 mmHg from 1 month to 1 year, less than (70mmHg + [2 x age]) from 1 years to 10 years, and less than 90 mmHg from 11 to 17 years.

OVERALL INCIDENCE
>> No exact incidence can be established based on available data.
>> the incidence is approximately 50–2000 episodes per 100000 person-years with a possible ‘lifetime’ prevalence of 0.05–2% .
>> Most studies indicate a significant underreporting, and therefore the true incidence is probably significantly higher than formally reported.
>> In adults, based on series of episodes evaluated by allergy/immunology specialists,
events of unknown cause (idiopathic) account for as many as 60% of cases. In childhood anaphylaxis idiopathic events are rare.
>> Foods are probably the most frequent offenders with drugs closely behind. The
incidence of food allergy, especially to peanuts, appears to be increasing.
>> The most commonly incriminated drugs are non-steroidal antiinflammatory drugs
and antibiotics. Reactions to radiocontrast media appear to be diminishing in frequency
Beta-lactams are the most frequently incriminated agent, accounting for as many as 22% all
drug-related episodes
>> Perioperative episodes may be increasing, with muscle relaxants being the most common offenders in this setting.

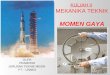
Causes of Anaphylaxis
www.emnet-usa.org

The overall incidence of anaphylactic reactions to latex increased markedly during the 1990s, but with the institution of non-powdered gloves and non-latex gloves in hospitals, the incidence may have stabilized
Radiocontrast media : Adverse reactions to ionic contrast media (hyperosmolar agents) occur with a frequency of 4–12% and to non-ionic (lower osmolar agents) with a frequency of 1–3%. Severe adverse reactions occur in 0.16% of ionic contrast administration and 0.03% with non-ionic media. Paradoxically, the death rate (1–3 per 100000 contrast administrations) appears to be similar for both ionic and non-ionic media.
Hymenoptera stings and bites : It is estimated that potentially life-threatening systemic reactions to insect stings occur in 0.4–0.8% of children and 3% of adults.
Food : As many as 6% of children and 3–4% of adults suffer from food allergy .Shellfish is probably the most common culprit in adults ,
peanuts the most common in children. It has also been reported that 1.1% of the US population may be allergic to tree nuts

Non-steroidal antiinflammatory drugs : Incidence varies depending on whether or not asthmatic subjects are included. NSAIDs are probably the second most common medication offender next to antibiotics.
Antisera : At one time antisera were the most important cause of anaphylaxis. Now its importance has greatly diminished with the decreased use of antisera as therapeutic agents, but antiserum is still used to treat snake bites and for immunosuppression. Incidence in patients receiving antilymphocyte globulin may be as high as 2%, and the incidence to antivenom
ranges from 4.6 to 10% .
Reactions associated with hemodialysis : Incidence appears to be on the rise. Drug administration data shows severe hypersensitivity reactions 3.5 per 100000 hollow-fiber dialyzers sold. Twenty-one severe reactions including one fatality have been reported to occur in 260000 dialysis treatments.
Idiopathic anaphylaxis : The cause remains unidentified in as many as two-thirds of adults presenting to an allergist/immunologist for evaluation of anaphylaxis.

Factors affecting the incidence and/or severity of anaphylaxis
Age : More frequent in adults than children for some agents :radiocontrast media, plasma expanders, anesthetics – may be function of exposure frequency.
Socioeconomic status Higher socioeconomic status has been associated with an increased frequency of anaphylaxis based upon outpatient epinephrine dispensing rates.
Gender Reportedly more frequent in females for latex, aspirin, and muscle relaxants. In addition, appears to be more frequent overall for females in random
surveys .May be more frequent in males for Hymenoptera stings, perhaps a function of
exposure .An age-related effect has been shown with males affected more frequently under age 15 years, and females affected more frequently after age 15.
Route of administration Oral less likely to produce reaction and reaction usually less severe.
Constancy of administration Gaps in administration may predispose to reactions..

Time since last reaction The longer the interval, the less likely the recurrence for many allergens.
Atopy Risk factor for anaphylaxis as a result of ingested antigens, exercise anaphylaxis, idiopathic anaphylaxis, radiocontrast media reactions, latex reactions; probably not a risk factor for insulin, penicillin, and Hymenoptera reactions.
Geographic location In most instances, no known effect has been documented. However, in one study geographical location as well as a rural environment affected the incidence. Two investigations have now shown a clear north–south gradient in the Northern Hemisphere with reactions appearing to be more frequent in northern climes. The explanation for this is unclear at this time.
Race No known effect.
Chronobiology No known effect of time of day or lunar cycle

BASOPHIL AND MAST CELL DEGRANULATION SYNDROMES
Histamine and products of arachidonic acid metabolism
( leukotrienes, thromboxane, prostaglandins, and platelet-activating factor )
Smooth muscle spasm, mucus secretion, vasodilatation, increased vascular permeability, activation of nociceptive neurons, platelet adherence, eosinophil activation, eosinophil chemotaxis
Neutral proteases
Proteoglycans: heparin, chondroitin sulfate
Chemoattractants
Tumor necrosis factor alpha activates NF-κB

HISTAMINE The overall effect of histamine on the vascular bed is dilation .
flushing and a lowering of peripheral resistance, with fall in systolic pressureincrease in vascular permeability because of the exposure of the permeable basement membrane
secondary to separation of endothelial cells at the postcapillary venule level .Vasodilation is mediated by both H1 and H2 receptors.
Cardiac effects of histamine are mediated primarily through the H2 receptor, but the H1 receptor also plays a role .
increases both the rate and force of atrial and ventricular contraction H1 receptor stimulation also produces coronary artery vasospasm
extravascular smooth muscle .smooth muscle contraction in the bronchial tree .
H1 receptor stimulation also causes modest contraction of the human uterus, and H2 receptor stimulation can produce uterine relaxation .
gastrointestinal smooth muscle is contraction mediated via the H1 receptor.
Glandular secretion is mediated by both H1 and H2.
The H3 receptor on presynaptic terminals of sympathetic effector nerves innervating the heart and systemic
vasculature results in inhibition of norepinephrine release .Since norepinephrine is involved in the correction of hypotension in shock, blockade of H3 receptor
stimulation may have a beneficial effect in reversing hypotension .

MULTIMEDIATOR RECRUITMENT OCCURRING DURING ANAPHYLAXIS
- Coagulation pathway Decreased factor V
Decreased factor VIII Decreased fibrinogen
- Complement cascade Decreased C4
Decreased C3 Formation of C3a
- Contact system (kinin formation) Decreased high-molecular-weight kininogen
Formation of kallikrein–C1-inhibitor complexes and factor XIIa–C1-inhibitor complexes
-Platelet activation - NITRIC OXIDE
Potentially detrimental Vasodilation (peripheral vascular bed)
Increased vascular permeability
Potentially beneficial Bronchodilation
Vasodilation (coronary arteries) Decreased mast cell degranulation

MECHANISMS INVOLVED IN THE PRODUCTION OF ANAPHYLACTIC SHOCK
Increased vascular permeability can produce a rapid and dramatic loss of intravascular volume. Fluid shifted to the extravascular space can result in a loss of 50% of vascular volume within 10 minutes.
This loss of blood volume leads to compensatory mechanisms that involve the secretion of catecholamines, such as norepinephrine and epinephrine;[activation of the angiotensin system with production of angiotensin I and angiotensin II;[and the production of endothelin-1, a potent vasoconstrictor peptide that is elevated in patients with heart failure, strokes, and hypotension.
These internal compensatory vasopressor responses can produce variable results. In some patients with anaphylaxis the peripheral resistance is abnormally elevated (indicating maximal vasoconstriction) because of this response. In others, despite elevation of catecholamines, systemic vascular resistance falls.
It has been suggested that failure to mobilize these compensatory mechanisms may predispose patients to anaphylaxis.[
.Angioedema may be related to the appearance of activation products of the contact (kinin-kallikrein) system

Dynamics of cardiovascular abnormalities in anaphylactic shock
At onset of reaction Early stage (minutes)with no treatment Prolonged shock Blood
pressure ↓ ↓↓ ↓↓↓ Pulse
↑↑ ↑ ↑
Cardiac output ↑ ↓ ↓↓
Peripheral vascular resistance ↓↓→ ↑↓→
Intravascular volume ↓ → ↓ ↓↓↓

FREQUENCY OF OCCURRENCE OF SIGNS AND SYMPTOMS OF ANAPHYLAXIS
Signs and symptoms Percentage of cases -Cutaneous >90
Urticaria and angioedema 85–90 Flush 45–55
Pruritus without rash 2–5 Respiratory 40–60 -
Dyspnea, wheeze 45–50 Upper airway angioedema 50–60
Rhinitis 15–20- Dizziness, syncope, hypotension 30–35
-Abdominal Nausea, vomiting, diarrhea, cramping pain 25–30 -Miscellaneous
Headache 5–8 Substernal pain 4–6 Seizure 1–2
∗Based on a compilation of 1784 patients


cardiovascular collapse with shock can occur immediately without any cutaneous manirestation
→data were recorded only from signs observed after the arrival of emergency personnel .
→profound hypotension with loss of blood volume into the third space and therefore inability to manifest cutaneous symptoms such as urticaria
The signs and symptoms of anaphylaxis that occur during anesthesia may be different .
Cardiovascular collapse appears to occur more commonly in operative events than those occurring outside of the operating room .
Overall, IgE-mediated events during surgery are more severe than those
caused by non-IgE-mediated mechanisms. There are no clear explanations for these observations .
.-

Symptoms usually begin within 5 to 30 minutes when antigen has been administered by injection; however, there can be a delay of an hour or more.
When antigen has been ingested, symptoms usually occur within the first 2 hours after ingestion but can be delayed for several hours.
It should be noted, however, that the onset of symptoms can occur immediately after ingestion, and such rapidly occurring events can be fatal.
There is believed to be a direct correlation between the immediacy of onset of symptoms and the severity of a given attack: the more rapid the onset, the more severe the episode

biphasic anaphylaxis. →1-20%
Protracted anaphylaxis, persisting for several days, and can be characterized by multiple recurrences interrupted by asymptomatic periods lasting hours
A delay in the administration of epinephrine and underdosing with epinephrine have been incriminated as predisposing factors for a late-phase response .
There is no clear evidence that the recurrent response can be suppressed by the administration of corticosteroids.
Most biphasic reactions occur within the first 8 hours after resolution of the primary phase. However, recurrent events have been described as late as 72 hours after the initial event. Such events are more common when antigen has been ingested rather than injected. The mechanism of production of the biphasic event is not known.
-Tachycardia
-Bradycardia → Bezold-Jarisch reflex
Myocardial depression with decreased cardiac output as a result of contractile depression can
occur and can persist for several days. This is thought to be due to hypoxemia.
Coronary artery vasospasm has been documented with coronary angiography and can be severe
enough to result in myocardial infarction (Kounis syndrome).[

-Electrocardiographic abnormalities include S-T segment elevation, flattening of T waves, inversion of T waves, and arrhythmias including those resulting from heart block. Cardiac enzyme elevations also occur.
-Arterial blood gas abnormalities usually consist of a fall in PO2 and PCO2 early in the course. If severe respiratory difficulty supervenes, the hypoxia worsens and an elevation of PCO2 may occur, along with a fall in pH that is probably due to a combination of carbon dioxide retention and metabolic acidosis.
-Syncope without other manifestations can occur and has been reported in episodes due to fire ant sting and from mastocytosis.
-In toddlers and infants who present with anaphylactic episodes, the major manifestation may mimic foreign body aspiration. Vomiting without aspiration minutes after the ingestion of an allergenic food is also a common initial presentation in this age group.
adrenal hemorrhage.-
DIC

DIFFERENTIAL DIAGNOSIS OF ANAPHYLAXIS
Vasodepressor reactions
Flush syndromes
Carcinoid Menopause Chlorpropamide– alcohol
Medullary carcinoma thyroid Autonomic epilepsy
‘Restaurant syndromes’
Monosodium glutamate (MSG) Sulfites Scrombroidosis
Other forms of shock Hemorrhagic Cardiogenic Endotoxic

Excess endogenous production of histamine syndromes Systemic mastocytosis Basophilic leukemia Acute promyelocytic leukemia (tretinoin treatment) Hydatid cyst Non-organic disease
Panic attacks
Munchausen stridor
Vocal cord dysfunction syndrome
Undifferentiated somatoform anaphylaxis Miscellaneous
Hereditary angioedema
Urticarial vasculitis
Pheochromocytoma
Neurologic (seizure, stroke)
Pseudoanaphylaxis
Red man syndrome (vancomycin)

Laboratory tests in the diagnosis of anaphylaxis
0 30 60 90 120 150 180 210 240 270 300 330
Plasma histamine
Serum tryptase
24-hr Urinary histamine metabolite

-If a patient is seen shortly after the onset of anaphylaxis, plasma and urinary histamine (or histamine metabolites) and serum
tryptase determinations may be helpful .
-Plasma histamine levels begin to rise within 5 to 10 minutes and remain elevated for 30 to 60 minutes. Therefore, they are of little help if the patient is seen even 1 hour after the onset of the event. However, urinary histamine metabolites are elevated for
a longer period of time and therefore may be useful .
-Serum tryptase levels peak 60 to 90 minutes after the onset of anaphylaxis and persist longer than plasma histamine levels do. Elevated tryptase concentrations are not uncommonly seen as
long as 5 hours after the onset of symptoms and rarely can.

TreatmentImmediate action
Assessment Check airway and secure if needed Rapid assessment of level of consciousness Vital signs
Treatment Epinephrine
Supine position, legs elevated Oxygen Tourniquet proximal to injection site
Dependent on evaluation Start peripheral intravenous fluids
H1 and H2 antihistamines Vasopressors Corticosteroids Aminophylline Glucagon Atropine Electrocardiographic monitoring Transfer to hospital
Hospital management Medical antishock trousers
Continued therapy with above-noted agents and management of complications

Epinephrine
-1:1000 0.3–0.5 mL I.M, lateral thigh (adult);
-1:1000 0.01 mg/kg or 0.1–0.3 mL I.M, lateral thigh (child)
0.1–1.0 mL (0.1–1.0 mg) of 1:1000 aqueous epinephrine diluted in 10 mL normaL saline i.v
in 5-10 (100 μg at a rate of 10–20 g/min)μ
-Alternatively, an epinephrine infusion can be prepared by adding 1 mg (1 mL) of 1:1000
dilution of epinephrine to 250 mL of D5W to yield a concentration of 4 g/mL. This solution is μinfused at a rate of 1–4 g/min (15–60 drops per minute with a microdrip apparatus) [60 drops μper minute = 1 mL = 60 mL/h]), increasing to a maximum of 10 g/minμ.
- Initial drug of choice for all episodes; should be given immediately; may repeat q 5–15 minute
-If intravenous access cannot be obtained, sublingual (rather than subcutaneous or intramuscular) injection has been suggested as an alternative route because of the rich vascularity of this area.( 40 mg sublingually (was roughly equivalent to 0.3 mg intramuscularly
If the patient has an endotracheal tube in place, the intravenous dose can be administered via a long catheter through the endotracheal tube into the area underneath the carina. It is rapidly absorbed from this area and dispersed within 5 to 10 breaths.

Antihistamines: Diphenhydramine 25–50 mg i.m. or i.v. (adult);
12.5–25 mg p.o., i.m., or i.v. (child) Ranitidine 1mg/kg i.v
Cimetidine 4mg/kg i.v. - Route of administration depends on severity of episode -Cimetidine should be administered slowly because rapid administration has been associated with hypotension; doses shown are for adults; dose in children less well established
Corticosteroids Hydrocortisone 100 mg–1 g i.v. or i.m. (adult), 10–100 mg i.v. (child)Exact dose not established; other preparations such as methylprednisolone can be used as well; for milder episodes, prednisone 30–60 mg may be given

Drugs for resistant bronchospasm - Aerosolized beta-agonist (albuterol, metaproterenol) Dose as for asthma (0.25–0.5 mL in
1.5–2 mL saline q4h, p.r.n.) →Useful for bronchospasm not responding to epinephrine
- Aminophylline Dose as for asthma→Rarely indicated for recalcitrant bronchospasm
-beta-agonist is drug of choice
Volume expanders - Crystalloids (normal saline or Ringer's lactate)
1000–2000 mL rapidly in adults; 30 mL/kg in first hour in children.-Colloids (hydroxyethyl starch)
500 mL rapidly followed by slow infusion in adults -Rate of administration titrated against blood pressure response for i.v. volume expander;
after initial infusion, further administration requires tertiary care monitoring; in patients who are beta-blocked, larger amounts may be needed
Vasopressors Dopamine 400 mg in 500 mL; dextrose 5% in water as i.v. infusion; 2–20 g/kg/minμ
-Dopamine probably the drug of choice; the rate of infusion should be titered against the blood pressure response; continued infusion requires intensive care monitoring

Drugs employed in patients who are beta-blocked
- Atropine sulfate 0.3–0.5 mg i.v.; may repeat every 10
minutes to a maximum of 2 mg in adults Glucagon Initial dose of 1–5 mg i.v. followed by infusion of 5–15 g/minute titrated against blood pressureμ
-Glucagon is probably the drug of choice with atropine useful only for treatment of bradycardia
-If resistant bronchospasm, and not shock, is the problem, then aminophylline, in doses used for the treatment of asthma, becomes the drug of choice. However, aminophylline must be used with caution if hypotension is present

INDICATIONS FOR PROLONGED OBSERVATION (8–24 HOURS AFTER RESOLUTION OF SYMPTOMS)
>> Moderate to severe reaction >> Episode in asthmatic with wheezing >> Ingested antigen with the possibility of continued absorption >> Previous history of a biphasic response

prevention of AnaphylaxisEducation
Obtain thorough history for drug allergy.
Avoid drugs that have immunologic or biochemical cross-reactivity with any agents to which the patient is sensitive.
Administer drugs orally rather than parenterally when possible.
Check all drugs for proper labeling.
Keep patients in the office 20 to 30 minutes after injections.
Allergen avoidance
Written emergency action plan
Prescription for self-injectable epinephrine
Have patient wear and carry warning identification tags.
Discontinue beta-adrenergic blocking agents, angiotensin-converting enzyme (ACE) inhibitors, ACE blockers, monoamine oxidase inhibitors, and certain tricyclic antidepressants when possible.
Use preventive techniques when patients are required to undergo a procedure or take an agent that places them at risk. Such techniques include pretreatment, provocative challenge, and desensitization.
Referral to an allergy specialist

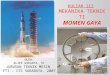
How To Use An Epi-PenRemove safety cap
when ready to use.Place black tip on
thigh at right angle to leg. You do not need
to remove the clothing.
Press hard, through the clothing, into the thigh until you hear a
click.Hold for 10 seconds
against thigh.

PROGNOSIS FOR RECURRENCE
The prognosis for recurrent anaphylactic episodes in a given patient is reasonably good.
It is better, of course, when the allergen is known versus when events are
idiopathic in nature .
However, even in idiopathic cases the episodes usually diminish in frequency over time and resolution is the rule.
Neither the presence of asthma nor atopy was a risk factor for recurrence .
The best predictor of a serious recurrence was the presence of serious symptoms at the time of the initial event.
Peanuts and tree nuts were the most common original causes and the most common triggers for recurrence.

FATALITIES-Anaphylactic deaths are relatively rare but many are
preventable, and a significant percentage are iatrogenic; therefore, it is important to consider the characteristics that place a patient at risk for death, and learn what might be done to prevent fatal
episodes .
-Airways obstruction and cardiovascular collapse were the most common causes of death. Disseminated intravascular coagulation was the cause in several instances.
-The most common foods to cause fatalities were nuts.

T H A N
Y O U
K