Embed Size (px)
Citation preview

Impact of Treatment Success on HealthService Use and Cost in DepressionLongitudinal Database Analysis
Sarah Byford,1 Barbara Barrett,1 Nicolas Despiegel2 and Alan Wade3
1 King’s College London, London, UK
2 Lundbeck SAS, Paris, France
3 CPS Clinical Research Centre, Glasgow, UK
Abstract Background: Research has consistently demonstrated a relationship between
depression and increased levels of health service use over the short term.
However, much less is known about how this relationship is influenced by the
success, or otherwise, of depression management strategies, and the economic
impact over the longer term.
Objective: To investigate the economic impact of non-remission on health
service use and costs over 12 months from the index episode in patients with
depression.
Methods:A naturalistic, longitudinal study was carried out using data from a
large primary care UK general practice research database between 2001 and
2006. The records of 88 935 patients aged ‡18 years, diagnosed with depres-
sion and in receipt of at least two antidepressant prescriptions (for amitripty-
line, citalopram, escitalopram, fluoxetine, paroxetine, sertraline or venlafaxine)
in the first 3 months after the index prescription were included. The main out-
come measures were health service use and cost over the 12-month study period,
by remission status, where remission is defined as patients not using anti-
depressants for at least 6 months after antidepressant treatment has ended.
Results: Sociodemographic and clinical characteristics were similar for par-
ticipants classified as in remission and those not in remission. Over 12 months
from the index prescription, patients classified as non-remitters spent longer,
on average, than patients classified as remitters on concomitant psychotropic
medication (204 days vs 93 days, respectively), and had more contact with
primary care services (17 vs 13GP visits), secondary care psychiatrists and other
specialists (47% vs 40%). Days in hospital, accident and emergency attendances
and psychological therapy contacts did not differ between the groups. Total
12-month costs per participant were significantly lower for remitters (mean d656
vs d937; mean difference d317; p< 0.0001). Total costs fell over time for both
groups, but at a faster rate for those in remission, and for those who remitted
earlier after the index prescription than for those who remitted later.
ORIGINAL RESEARCH ARTICLEPharmacoeconomics 2011; 29 (2): 157-170
1170-7690/11/0002-0157/$49.95/0
ª 2011 Adis Data Information BV. All rights reserved.

Conclusions: Successful cessation of antidepressant medication treatment in
adults with depression can result in significant cost savings to the health
service.
Background
Research has consistently demonstrated a re-lationship between depression and increased lev-els of health service use.[1,2] However, much lessis known about how this relationship is influ-enced by the success, or otherwise, of depressionmanagement strategies, and thus the economicimpact of depression treatment over the longerterm. Data from longitudinal studies suggest thatcosts are significantly lower for patients who ex-perience remission after the acute treatmentphase than for those with less favourable out-comes[3,4] and that full remission is associatedwith a significantly improved ability to work andthus reduced productivity losses resulting fromfewer sickness-related absences from work.[4]
However, the existing literature is limited in anumber of important ways. First, the findings arebased on relatively small samples,[1,3] principallyfrom randomized treatment trials,[3] althoughone study was naturalistic.[4] The association be-tween remission from depression and service useand cost has not been tested in a large, clinicallyrepresentative sample. Second, the duration overwhich study participants were followed-up waslimited in each case to 6 months. The impact onservice use beyond this point is not clear, al-though it has been hypothesized that the costsavings associated with remission would continueover time.[3] Finally, many of the studies testedfor remission at a point when a large proportionof participants would still be receiving antide-pressant medication. Patient surveys suggest thatindividuals do not like to continue long-termantidepressant treatment because of a preferencefor psychological treatment options[5] and be-cause of unwanted adverse effects.[6] Despite this,there is evidence to suggest that recent increasesin antidepressant prescribing in the UK can beexplained by changes in the proportion of patientsreceiving long-term treatment.[7] The relationship
between service costs and remission achieved afterantidepressant medication treatment has endedremains unclear.
Methods
Objective
The aimwas to quantify the economic impact ofnon-remission of depression on health service useand costs, over a 12-month period from the date offirst antidepressant prescription, in patients treatedin primary care settings in the UK, using a large,naturalistic sample representative of actual clinicalconditions.
Study Design
Data were extracted from the General PracticeResearch Database (GPRD),[8] one of the world’slargest databases of anonymous longitudinal med-ical records compiled from over 450 primary care-based general practices in the UK. The GPRDcontains full records for around 3.5 million cur-rently registered patients and over 10 million pa-tients in total, representing 39 million person-yearsand covering around 5% of the UK population.
Participants
Participants meeting the following criteriawere included in the study:� At least one prescription for a first-line anti-
depressant, including tricyclic antidepressants(amitriptyline), selective serotonin reuptakeinhibitors (citalopram, escitalopram, fluoxe-tine, paroxetine, sertraline) and serotonin andnoradrenaline reuptake inhibitors (venlafaxine),between 1 January 2001 and 30 June 2006. Thedate of the first prescription is referred to as theindex date.
� Age ‡18 years at the index date.� Data available for a minimum of 6 months
before the index date.
158 Byford et al.
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

� Data available for a minimum of 18 monthsafter the index date.
� Free of antidepressant use for a minimum of6 months before the index date.
� Diagnosis of depression in a –3-month windowsurrounding the index date, determined bysearching for the words ‘depression’ or ‘de-pressive’ in the READ/OXMIS (Oxford Med-ical Information System) coding framework,which is based on the International Classifica-tion of Diseases, Ninth Revision, ClinicalModification (ICD-9-CM) and is widely usedin British general practices to enter diagnoses.
� At least two antidepressant prescriptions inthe first 3 months after index date.
Definition of Remission
Since the GPRD database does not include theMontgomery-Asberg Depression Rating Scale[9]
commonly used for defining remission,[10] and givenour focus on the impact of remission achieved afterantidepressant treatment ended, alternative, proxycriteria for remission were defined, which focusedon the cessation of antidepressant treatment:� Remission included all patients not using anti-
depressants for at least 6 months after anti-depressant treatment ended, which correspondswith a successful cessation of treatment.
� Non-remission included (i) patients for whomantidepressant treatment did not end; and(ii) patients for whom antidepressant treatmentended but who resumed antidepressant treat-ment within 6 months of the treatment ending.This proxy measure of remission is supported
by recent evidence from a Spanish retrospectivedatabase study[11] that evaluated the concordancebetween remission as defined by antidepressantcessation for at least 6 months and remission de-termined by clinical criteria from a review of med-ical records. Themeasurement of remission definedaccording to antidepressant cessation from com-puterized records was shown to be valid andreliable when compared with remission definedaccording to clinical criteria, and the level of con-cordance between the two approaches was con-sidered acceptable[11] (Cronbach’s alpha 90.6%,95% CI 85.6, 95.6).
Observation Period
For each individual, the observation periodstarted on the date of the first dispensing of anantidepressant of interest (the index date), between1 January 2001 and 30 June 2006, and continued for18 months after this index date. The first 12 monthsof follow-up is denoted as the study period and isthat period over which study data were collectedand analysed. The additional 6-month period offollow-up was included to ensure adequate timeto assess whether remission had been achieved,given our definition of remission noted above. Theremission period (ceasing antidepressant treatment)could begin at any point during the 12-monthstudy period, but a participant was only classifiedas ‘in remission’ if they remained off antidepres-sants for a minimum of 6 months (i.e. for the pur-pose of this study all patients could have amaximumof 12 months’ treatment from the index date).Hence, a maximum follow-up of 18 months wasneeded to accurately classify remission in allparticipants.
Economic Methods
Service use data contained in the GPRDincludes only health services provided by theUK NHS. Thus, the perspective of the currentanalysis was limited to that of the NHS. Serviceuse components extracted from the GPRD(and summarized in table I) included GP con-tacts, general practice phone calls for med-ication renewals, referrals to psychiatrists andother secondary care specialists for any reason,inpatient stays for all reasons, psychologicalinterventions and accident and emergency at-tendances. Medication data extracted includedantidepressant prescriptions and psychiatric-related concomitant medication, including an-xiolytics, mood stabilizers, antipsychotics andhypnotics.
Nationally applicable UK unit costs for thefinancial year 2005–6 were applied to the serviceuse data[12-14] and are reported in table I. The2005–6 financial year was selected as the most re-cent year during which service use data were col-lected. Mean duration for all face-to-face contacts,
Impact of Treatment Success on Cost in Depression 159
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

phone contacts and hospitalizations were assumedto be constant and based on national estimates.[12]
Mean duration of hospitalizations were taken fromhospital episode statistics for England.[15] Formedication, defined daily dose was estimated fromtheWHOCollaborating Centre for Drug StatisticsMethodology[16] and an average cost for each cat-egory of drug applied.
Statistical Analyses
Service use items were summarized by remis-sion status, using mean percentage of patientswith at least one unit of service use and meannumber of service contacts, prescriptions or daysin hospital, as appropriate. Antidepressant treat-ments were described using number of prescrip-tions, cumulative duration of treatment (equalto the sum of the duration of all antidepressantprescriptions, whether given consecutively or atthe same time) and actual time on treatment (totalperiod of time between first and last prescription,excluding periods when antidepressant use hadceased) and other medications were summarizedusing the number of prescriptions and cumulativeduration of treatment.
Costs were summarized by remission statusand explored in the full population of partici-pants and a subgroup of patients diagnosed at theindex date with severe depression. Severity was
defined using the work by Martinez et al.,[17]
which describes a classification assigned by anexpert panel to READ and OXMIS medicalterms for depression included in the GPRD. Thelatter analysis was to determine the influenceof the severity of depression on the findings fromthe full sample, to ensure that we were not com-paring biased samples. The non-remission groupwas also split in two: patients who remainedon treatment during the 12-month period andpatients who attempted to stop antidepressanttreatment in the year after the index date butwho resumed in the 6-month period after stop-ping. In addition, total costs were explored overtime by remission status and for participantsachieving very early remission (onset of remissionwithin 4 months of index antidepressant prescrip-tion date), early remission (onset of remission5–8 months after index antidepressant prescrip-tion date) and late remission (onset of remission9–12 months after index antidepressant prescrip-tion date).
Total costs per participant for the full sam-ple were compared between remitters and non-remitters using a multivariable generalized linearmodel (GLM) regression with log link and gammavariance function.[18] Adjustment factors werefirst selected using a univariate model, and thosesignificant at the 5% level were included as po-tential predictors in the final model. A backwardselection process was then applied to obtain thefinal model, again using a 5% level of significance.Adjustment factors included were sex, age (con-tinuous variable), NHS region (Eastern, London,Northern Ireland, North West, Northern andYorkshire, Scotland, South East, South West,Trent,Wales,WestMidlands), index severity (mild,moderate, severe, as defined using the work byMartinez et al.[17]), index treatment (escitalopram,fluoxetine, paroxetine, venlafaxine, none), combi-nation of antidepressants at index date (yes/no),history of psychiatric diagnoses in the 6 monthsprior to index date (depression, bipolar, substanceabuse and dependence, schizophrenia), history ofuse of psychiatricmedication in the 6months priorto index date (anxiolytics, benzodiazepine hypno-tics, other hypnotics, typical neuroleptics, atypicalneuroleptics, lithium, antiepileptic mood stabilizers),
Table I. Services included and unit costs applied (£, year 2005–6
values)
Service Unit cost
GP visits 25.00 per surgery consultation[12]
GP phone contact 12.70 per phone call[12]
Psychological therapy 66.00 per contact[12]
Referral to psychiatrist 155.00 per contact[12]
Referral to other specialist 107.00 per contact[13]
Hospitalizations 1887.60 per admission[12]
Accident and emergency 105.00 per attendance[12]
Medications[14]
antidepressants 0.43 per day
anxiolytics 0.19 per day
mood stabilizers 0.44 per day
antipsychotics 1.64 per day
hypnotics 0.12 per day
160 Byford et al.
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

history of health service use in the 6 months priorto index date (GP visits, GP phone contacts, refer-rals to psychiatrist, referrals to any other secondarycare specialists, accident and emergency attendance)and total healthcare costs in the 6 months prior toindex date (continuous variable). The estimationswere adjusted to account for over-dispersionusing Pearson’s chi-squared.
The same factors were used to explore pre-dictors of remission status using a multivariablelogistic regression. As in the previous model,potential predictors were first selected using uni-variate tests and those significant at the 5% levelwere included in the final model. A backwardselection process was then applied to obtain thefinal model, using a 5% level of significance. Thediscriminative power of the logistic regressionwas then evaluated with the C-statistic.
Results
Participants
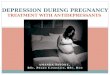
Details of the patient-selection process are re-ported in figure 1. A total of 88 935 individualsin the GPRD met the inclusion criteria for the
study, 53 654 (60%) of whom achieved remissionduring the course of the study period. Of the35 281 patients who did not meet the criteria forremission, 60% (n = 21 082) were patients forwhom antidepressant treatment ended at somepoint over the 12-month study period but re-sumed within 6 months of antidepressant cessa-tion and 40% (n = 14 199) were patients for whomantidepressant treatment did not end over the12-month study period.
Patient sociodemographic and clinical charac-teristics by remission status are described in table II.Although the very large sample size generatedevidence of statistically significant differences, thetwo groups were in fact similar on all availablesociodemographic indicators. In terms of clinicalcharacteristics, a lower percentage of patients withsevere depression achieved remission than thosewith mild to moderate depression (54.6% of severepatients vs 60.9% of non-severe; p< 0.0001) and agreater proportion of those with a history of de-pression achieved remission than those with nohistory of depression (65.5% vs 56.5%; p< 0.0001).Health service costs were higher on average in thenon-remission group than the remission group inthe 6 months prior to the index date (d298.17 vsd246.60; mean difference d51.57; p< 0.0001).
Service Use over the 12-Month Study Period
Health services used by remitting and non-remitting patients are reported in table III. Patientswho did not cease antidepressant treatment for aminimum of 6 months over the 18-month follow-up period (non-remitters), were on average morelikely to be using concomitant psychotropic med-ication and spent longer receiving each cate-gory of concomitant psychotropic medicationthan patients classified as achieving remissionover the 12-month study period. Non-remitterswere also more likely to have at least one contactwith primary and secondary healthcare services,and the mean number of contacts was higher onaverage for GP visits and phone calls and contactswith psychiatrists and other secondary care spe-cialists. Days in hospital, accident and emergencyattendances and psychological therapy contactsdid not differ by remission status.
Prescription of antidepressant between 1 January 2001 and 30 June 2006414 508 patients; 3 476 244 potential index dates
Aged 18 years or older with at least 6 months' databefore and 18 months' data after index date320 997 patients; 2 252 261 potential index dates
Diagnosis of depression from 3 months before and3 months after index date143 049 patients; 650 072 potential index dates
No antidepressant prescription in the 6 monthsbefore the index date118 368 patients; 129 723 potential index dates
At least two antidepressant prescriptions in the first3 months after the index date88 935 patients and index dates
Most recent index date118 368 patients and index dates
Fig. 1. Patient selection flowchart.
Impact of Treatment Success on Cost in Depression 161
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

Costs over the 12-Month Study Period
Total costs per participant over the 12-monthstudy period are reported in table IV. General
practice contacts accounted for >50% of totalcosts in the total population, and medicationscontributed around 18%. Hospitalizations ac-counted for around 20% of total costs. Costs in
Table II. Sociodemographic and clinical characteristics by remission status
Characteristic Remission
(n= 53654)Non-remission
(n= 35 281)p-Valuea
Age [mean (SD)] 42.2 (17.0) 46.5 (16.5) <0.0001Sex [n (%)] <0.0001male 17 918 (33.4) 10 737 (30.4)
female 35 735 (66.6) 24 544 (69.6)
Region [n (%)] <0.0001East 5732 (10.7) 3810 (10.8)
London 5050 (9.4) 3080 (8.7)
Northern Ireland 1641 (3.1) 1323 (3.7)
North West 6934 (12.9) 4676 (13.3)
Northern and Yorkshire 3634 (6.8) 2438 (6.9)
Scotland 3351 (6.2) 2403 (6.8)
South East 10 984 (20.5) 7245 (20.5)
South West 4898 (9.1) 2871 (8.1)
Trent 3287 (6.1) 2199 (6.2)
Wales 2031 (3.8) 1292 (3.7)
West Midlands 6112 (11.4) 3944 (11.2)
Severity of depression [n (%)] <0.0001
mild 27 458 (51.2) 17 421 (49.4)
moderate 21 773 (40.6) 14 177 (40.2)
severe 4423 (8.2) 3683 (10.4)
Initial antidepressant [n (%)]
escitalopram 2902 (5.4) 1885 (5.3) 0.6929
citalopram 13773 (25.7) 9622 (27.3) <0.0001
fluoxetine 20 333 (37.9) 12 023 (34.1) <0.0001
paroxetine 5869 (10.9) 4395 (12.5) <0.0001
sertraline 4791 (8.9) 3394 (9.6) 0.0004
venlafaxine 2631 (4.9) 2265 (6.4) <0.0001
duloxetine 2 (0.0) 1 (0.0) 0.8230
tricyclic antidepressant 3144 (5.9) 1527 (4.3) <0.0001
combination 209 (0.4) 169 (0.5) 0.0448
Psychiatric history [n (%)]
depression 24 711 (46.1) 13 023 (36.9) <0.0001
anxiety 5582 (10.4) 3611 (10.2) 0.4188
bipolar disorder 15 (0.0) 28 (0.1) 0.0006
obsessive compulsive disorder 31 (0.1) 27 (0.1) 0.2839
eating disorders 33 (0.1) 16 (0.0) 0.3152
substance abuse and dependence 274 (0.5) 159 (0.5) 0.2084
schizophrenia 18 (0.0) 24 (0.1) 0.0206
Total 6-month costs prior to index date [mean (SD)] 246.60 (504.54) 298.17 (538.54) <0.0001a Chi-squared test was used for categorical variables and t-test for continuous variables.
162 Byford et al.
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

all categories were lower for patients achievingremission than for non-remitters. The mean costof antidepressant treatment was 57% lower forremitters than non-remitters (mean d67 vs d154;mean difference d88). Total 12-month costs perparticipant were approximately 33% lower forremitters than non-remitters when all costs wereincluded (mean d656 vs d973; mean differenced317) and 25% lower excluding the cost of med-ications (mean d562 vs d754; mean differenced192), which are by definition lower for remittersthan non-remitters. Remission status was signif-icantly associated with lower total cost per par-ticipant in multivariable analysis, adjusting forsociodemographic and baseline clinical character-istics (p< 0.0001). Among non-remitters, patientswho remained on treatment during the 12 monthswere found to be slightly more expensive thanthose who withdrew and relapsed (mean d1026 vsd938, mean difference d88). The former group was
substantially more expensive than patients dem-onstrating successful withdrawal (mean d1026vs d656, mean difference d370).
In this multivariablemodel, most of the initiallyconsidered predictors remained in the model: re-mission status, age, region, depression severity,initial treatment, psychiatric history (depression,bipolar disorder, schizophrenia, substance abuseand dependency), use of other psychotropic med-ications before index date, use of healthcare ser-vices before index date (GP visits, phone contacts,referrals, acute and emergency), total costs withinthe year prior to index date (see table V).
Exploration of total costs by remission statusfor the subgroup of participants with severe de-pression replicates the findings from the fullsample to a large extent (see table VI). With theexception of hospitalizations, all categories of costwere lower on average in the remission group, andtotal cost per participant was significantly lower
Table III. Service use over the 12-month study period by remission status
Remission (n= 53654) Non-remission (n= 35281)
% using mean (SD) % using mean (SD)
Antidepressant use
Number of prescriptions 100 4.76 (3.19) 100 11.07 (5.65)
Cumulative duration (days) 155.21 (101.53) 358.74 (158.36)
Time on treatment (days) 129.81 (73.71) 283.91 (63.78)
Concomitant medication duration (days)
Anxiolytics – BZD 8.2 32.41 (241.70) 12.6 69.48 (458.46)
Anxiolytics – other 0.7 0.76 (15.03) 1.1 1.61 (23.70)
Hypnotics – BZD 11.4 39.76 (258.73) 16.9 84.05 (552.11)
Hypnotics – Z drugs 9.2 7.54 (44.43) 12.9 16.39 (71.62)
Hypnotics – other 0.5 0.80 (22.13) 0.6 1.52 (30.28)
Mood stabilizers – lithium 1.2 6.02 (47.91) 3.1 12.71 (90.20)
Mood stabilizers – antiepileptic 4.7 2.16 (31.54) 6.2 8.48 (72.40)
Neuroleptics – typical 0.2 0.37 (11.17) 0.5 1.40 (25.88)
Neuroleptics – atypical 0.7 3.02 (54.70) 1.1 8.33 (120.02)
Service use
GP visits 100 12.88 (8.92) 100 17.34 (10.44)
GP phone calls 55.2 2.48 (4.26) 86.7 5.41 (6.05)
Psychological therapy contacts 0.2 0.00 (0.06) 0.2 0.00 (0.10)
Psychiatrist contacts 2.9 0.04 (0.28) 5.0 0.07 (0.42)
Other specialist contacts 38.6 0.62 (1.08) 44.9 0.77 (1.24)
Inpatient days 5.2 0.07 (0.36) 5.7 0.08 (0.42)
Accident and emergency attendances 3.1 0.04 (0.29) 3.3 0.05 (0.29)
BZD = benzodiazepines; Z = zopiclone, zolpidem and zaleplon.
Impact of Treatment Success on Cost in Depression 163
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

(mean d749 vs d1037; mean difference d288),amounting to a 28% reduction in costs overall forthose in the remission group.
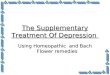
Exploration of total costs over time by remis-sion status is illustrated in figure 2a. Total costsfall over time for both remitters and non-remitters, although at a faster rate for remitters.Of those achieving remission (n = 53 654), 44%(n = 23 794) ceased antidepressant medicationwithin the first 4 months of the index prescription(very early remission), 35% (n= 18546) ceased anti-depressant medication in months 5–8 (early remis-sion) and the remaining 21% (n= 11 314) ceased inmonths 9–12. Figure 2b demonstrates that costsfall at a faster rate the earlier the remission begins.
Predictors of Remission
Sociodemographic and clinical characteristicsfound to be significantly and independently as-sociated with remission status over the 12-monthfollow-up period are reported in table VII. TheC-statistic was 0.619. This value is rather low,indicating that some important factors were notincluded in the model. The likelihood of achievingremission was found to be higher for patientswho were older, male, those with mild or mod-erate depression (vs severe) and those with a his-tory of depression. Patients less likely to achieveremission included those who were younger, fe-male, those with severe depression, those with ahistory of bipolar disorder, those with a historyof psychotropic medication use (in particular, the
use of neuroleptics [odds ratio {OR} = 0.69] andantiepileptics [OR = 0.68]), those with previouscontact with psychological therapists (OR= 0.21),psychiatrists and other secondary care specialists,frequent GP contacts and those who started de-pression treatment with venlafaxine, citalopram orparoxetine.
Discussion
Exploration of a large, naturalistic populationof patients with depression found a consistentrelationship between successful withdrawal fromantidepressant treatment and health service useand costs. Successful remission (cessation of anti-depressant use for a minimum of 6 months) wasassociated with lower or similar health service usein all service categories and significantly lowercosts than non-remission. Total costs fell overtime for both groups, but at a faster rate for thosein remission.
Over 40% of participants who successfullyceased antidepressant treatment ceased within4 months of the index prescription and almost80% ceased within 8 months. Such durations areshorter than would be expected given the currentNational Institute for Health and Clinical Ex-cellence (NICE) guidelines for depression[19] andindeed earlier consensus guidelines.[20] The NICEguidelines, for example, recommend that anti-depressants should be continued for at least6 months after remission of symptoms to reducethe risk of relapse, and for 2 years in patients who
Table IV. Healthcare costs by category and total costs (£, year 2005–6 values) over the 12-month study period by remission status, all
participants
Healthcare cost category Remission
(n= 53654) [mean (SD)]
Non-remission
(n= 35281) [mean (SD)]
Remission vs non-remission
[difference (adjusted p-valuea)]
Antidepressant medication 66.74 (43.66) 154.26 (68.09) -87.52 (<0.0001)
Concomitant medication 26.99 (136.33) 64.77 (271.96) -37.78 (<0.0001)
GP contacts 353.42 (243.41) 502.20 (279.92) -148.78 (<0.0001)
Psychological therapies 0.13 (3.64) 0.23 (6.33) -0.10 (<0.0001)
Secondary care contacts 72.24 (125.22) 93.31 (149.29) -21.07 (<0.0001)
Hospitalizations 132.17 (686.75) 153.76 (796.13) -21.59 (0.0260)
Accident and emergency 4.51 (30.11) 4.74 (30.32) -0.23 (0.4700)
Total 656.20 (846.92) 973.28 (1015.38) -317.07 (<0.0001)a Generalized linear model of each cost category and total costs with log link and gamma variance function, adjusting for significant
predictors amongst sociodemographic and baseline clinical characteristics.
164 Byford et al.
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

Table V. Multivariable analysis of total costs over the 12-month study period
Co-variate Class Reference
class
RR (95% CI) p-Value
Intercept <0.0001
Remission Yes No 0.7243 (0.7145, 0.7343) <0.0001
Age 1.0016 (1.0012, 1.0020) <0.0001
Region East West Midlands 0.9611 (0.9344, 0.9885) 0.0056
London West Midlands 1.0553 (1.0248, 1.0868) 0.0003
Northern Ireland West Midlands 1.3105 (1.2573, 1.3659) <0.0001
North West West Midlands 1.0630 (1.0348, 1.0919) <0.0001
Northern and Yorkshire West Midlands 1.1728 (1.1359, 1.2111) <0.0001
Scotland West Midlands 1.0047 (0.9726, 1.0380) 0.7769
South East West Midlands 1.0032 (0.9790, 1.0281) 0.7953
South West West Midlands 1.0527 (1.0219, 1.0845) 0.0007
Trent West Midlands 1.0693 (1.0346, 1.1053) <0.0001
Wales West Midlands 1.2044 (1.1579, 1.2528) <0.0001
Index depression severity Mild Severe 0.9002 (0.8791, 0.9220) <0.0001
Moderate Severe 0.8843 (0.8630, 0.9060) <0.0001
Index treatment
escitalopram Yes No 1.0672 (0.9660, 0.9090) <0.0001
fluoxetine Yes No 0.9519 (0.9375, 0.9665) <0.0001
paroxetine Yes No 0.9649 (0.9439, 0.9864) 0.0015
venlafaxine Yes No 1.0824 (1.0506, 1.1153) <0.0001
non-SRI, non-TCA Yes No 1.3777 (1.0874, 1.7456) 0.0080
combination of AD Yes No 1.2350 (1.0994, 1.3872) 0.0004
Psychiatric history
depression Yes No 1.5250 (1.4826, 1.5685) <0.0001
bipolar Yes No 0.4828 (0.2528, 0.9221) 0.0274
abuse and dependency Yes No 0.8891 (0.8772, 0.9011) <0.0001
schizophrenia Yes No 0.7156 (0.5266, 0.9725) 0.0325
Past medication use
anxiolytics – BZD Yes No 1.0877 (1.0446, 1.1327) <0.0001
hypnotics – BZD Yes No 1.0729 (1.0358, 1.1113) <0.0001
hypnotics – Z drugs Yes No 1.0460 (1.0110, 1.0823) 0.0098
neuroleptic – typical Yes No 1.1342 (1.0911, 1.1789) <0.0001
neuroleptic – atypical Yes No 1.3055 (1.1943, 1.4270) <0.0001
mood stabilizers – lithium Yes No 1.3490 (1.1152, 1.6320) 0.0021
mood stabilizers – antiepileptic Yes No 1.3047 (1.1934, 1.4265) <0.0001
Past service use
number of GP visits 1.0290 (1.0274, 1.0307) <0.0001
GP phone calls Yes No 1.1391 (1.1199, 1.1586) <0.0001
psychiatrist Yes No 1.1354 (1.0502, 1.2274) 0.0014
other specialist Yes No 1.0232 (1.0051, 1.0414) 0.0115
acute and emergency Yes No 1.1097 (1.0516, 1.1709) 0.0001
Past total costs
total baseline costs 1.0003 (1.0003, 1.0003) <0.0001AD= antidepressant; BZD = benzodiazepines; RR = relative risk; SRI = serotonin reuptake inhibitor; TCA = tricyclic antidepressant;
Z = zopiclone, zolpidem and zaleplon.
Impact of Treatment Success on Cost in Depression 165
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

have had two or more depressive episodes in therecent past and who have experienced significantfunctional impairment during the episodes.[19]
This difference may reflect either patient pref-erence, given evidence to suggest that patients donot like to continue long-term antidepressanttreatment,[5,6] and/or practitioner prescribing pref-erences. Costs over the 12-month study periodfell faster for those patients who remitted earlythan for those who remitted later or who did notachieve remission, suggesting that for some pa-tients, early cessation of antidepressants is likely
to be cost saving to the NHS and may be costeffective if successful cessation of antidepressanttreatment for a minimum of 6 months is asso-ciated with a good outcome.
Patients who were more likely to cease anti-depressant use and to remain off antidepressantsfor a minimum of 6 months included those whowere male, older, with mild or moderate depres-sion (vs severe) and with a history of depression.Those patients less likely to remit included thosewith a history of bipolar disorder, a history of con-comitant psychotropic medication use, a history of
Table VI. Healthcare costs by category and total costs (£, year 2005–6 values) over the 12-month study period by remission status, severe
depression only
Healthcare cost category Remission
(n= 3683) [mean (SD)]
Non-remission
(n =4423) [mean (SD)]
Remission vs non-remission
(difference [adjusted p-valuea])
Antidepressant medication 67.98 (44.09) 157.98 (73.59) -90.00 (<0.0001)
Concomitant medication 46.25 (188.43) 101.08 (309.46) -54.83 (<0.0001)
GP contacts 363.42 (252.57) 515.83 (283.02) -152.41 (<0.0001)
Psychological therapies 0.12 (2.80) 0.39 (6.69) -0.27 (<0.0001)
Secondary care contacts 74.09 (117.28) 92.57 (137.30) -18.48 (<0.0001)
Hospitalizations 191.19 (841.40) 162.98 (764.86) 28.21 (0.0360)
Accident and emergency 6.08 (35.21) 6.53 (34.81) -0.45 (0.7600)
Total 749.13 (1029.90) 1037.35 (1017.04) -288.22 (<0.0001)a Generalized linear model of each cost category and total costs with log link and gamma variance function, adjusting for significant
predictors among sociodemographic and baseline clinical characteristics.
0
50
100
150
200
250
300
350a b
1−3 4−6 7−9 10−12
Months
Tot
al c
ost (
£)
1−3 4−6 7−9 10−12
Months
Non-remissionLate remissionEarly remissionVery early remissionRemission
Fig. 2. Total costs (year 2005–6 values) over the 12-month study period by trimester; (a) remission versus non-remission; (b) very early(1–4 months after onset), early (5–8 months) and late (9–12 months) remission.
166 Byford et al.
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

previous contact with various health services andthose starting treatment on certain antidepressants.The findings relating to a history of depression(more likely to remit) and a history of past healthservice use (less likely to remit) appear at odds withone another. The former relationship may reflectgreater patient experience, resulting in a greater
understanding of antidepressant medication and amore informed capacity to exercise patient choice.However, the history of depression variable corre-sponds to recent depression only (in the 6 monthsbefore index date), which was, by definition, nottreated with antidepressants, since included patientswere free of antidepressant use for a minimum of
Table VII. Multivariable logistic analysis of remission status over the 12-month study perioda
Co-variate Class Reference class OR (95% CI) p-Value
Intercept <0.0001
Age 1.0116 (1.0107, 1.0126) <0.0001
Sex Female Male 0.8525 (0.8275, 0.8783) <0.0001
Region East West Midlands 1.0675 (1.0068, 1.1318) 0.0287
London West Midlands 0.9757 (0.9177, 1.0374) 0.4317
Northern Ireland West Midlands 1.2766 (1.1727, 1.3897) <0.0001
North West West Midlands 1.0393 (0.9829, 1.0988) 0.1759
Northern and Yorkshire West Midlands 0.9861 (0.9226, 1.0539) 0.6791
Scotland West Midlands 1.0967 (1.0252, 1.1732) 0.0073
South East West Midlands 1.0302 (0.9792, 1.0839) 0.2500
South West West Midlands 0.9489 (0.8915, 1.0098) 0.0987
Trent West Midlands 1.0766 (1.0051, 1.1532) 0.0353
Wales West Midlands 1.0160 (0.9358,1.1031) 0.7049
Index depression severity Mild Severe 1.3310 (1.2676, 1.3977) <0.0001
Moderate Severe 1.2463 (1.1857, 1.3100) <0.0001
Index treatment
citalopram Yes No 0.8950 (0.8664, 0.9246) <0.0001
paroxetine Yes No 0.8009 (0.7664, 0.8369) <0.0001
venlafaxine Yes No 0.7148 (0.6732, 0.7591) <0.0001
Psychiatric history
depression Yes No 1.5250 (1.4826, 1.5685) <0.0001
bipolar Yes No 0.4828 (0.2528, 0.9221) 0.0274
Past medication use
anxiolytics – BZD Yes No 0.8598 (0.8086, 0.9143) <0.0001
anxiolytics – other Yes No 0.7256 (0.5849, 0.9000) 0.0035
hypnotics – Z drugs Yes No 0.9041 (0.8429, 0.9697) 0.0048
neuroleptic – typical Yes No 0.9013 (0.8330, 0.9752) 0.0098
neuroleptic – atypical Yes No 0.6931 (0.5769, 0.8327) <0.0001
mood stabilizers – antiepileptic Yes No 0.6813 (0.5676, 0.8179) <0.0001
Past service use
number of GP visits 0.9916 (0.9888, 0.9945) <0.0001
GP phone calls Yes No 0.7402 (0.7151, 0.7662) <0.0001
psychiatrist Yes No 0.8202 (0.6982, 0.9636) 0.0159
other specialist Yes No 0.9548 (0.9207, 0.9900) 0.0124
psychological therapy Yes No 0.2086 (0.0883, 0.4928) 0.0004
a C-statistic =0.619.
BZD = benzodiazepines; OR =odds ratio; Z = zopiclone, zolpidem and zaleplon.
Impact of Treatment Success on Cost in Depression 167
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

6 months before the date of index prescription. Thisdefinition raises the possibility that patients with arecent history of depression were not severely illenough at that time to warrant an antidepressantprescription or that the patients preferred not totake antidepressant medication. Thus, the higherrates of remission in this groupmay indicate that thecurrent depression episode was amenable to anti-depressant treatment or a less favourable attitudetowards antidepressant medication. History of de-pression in the more distant past was not available.
In contrast, a history of health service use(again in the 6 months prior to index date) sug-gests greater severity of illness, long-standinglow-grade mental health symptoms and/or theexistence of co-morbid psychiatric and physicalconditions than for those without such a history.This is supported by the negative relationshipbetween remission and both bipolar disorder andconcomitant psychotropic medication use andthe fact that the history of health service usevariable includes all national health services, notjust mental health services. This is in line withstandard economic practice, which suggests thata gold standard economic evaluation shouldmeasure all costs of all participants regardless ofwhy the costs were incurred.[21] Mental healthproblems are known to be associated with a rangeof physical co-morbidities,[22] so it would be in-appropriate to assume that non-mental healthservice use is irrelevant to an economic evalua-tion in the area of mental health.
The work presented here benefits from a large,naturalistic and thus clinically representativesample but it is also limited in a number of im-portant ways. First, it was not possible to test forremission in terms of symptom severity. Instead,our definition of remission was determined bycessation of antidepressant use, which involvesan implicit assumption that cessation of anti-depressant treatment is associated with positiveoutcomes, or at least is positive in the sense that itis an outcome preferred by patients.[5,6] The in-clusion of patients who cease all antidepressanttreatment because of adverse effects or lack ofefficacy is unavoidable, but is kept to a minimumby the exclusion of patients who received onlyone prescription for antidepressants in the first
3 months after the index date. Moreover, the factthat remitters remained off antidepressant med-ication for a minimum of 6 months supports thebelief that this group are in some sense doingbetter than the group of non-remitters, 60% ofwhom had attempted withdrawal but relapsedwithin 6 months of antidepressant cessation. Thesituation is less clear for the remaining 40% ofnon-remitters who were prescribed antidepres-sant medication for the full 12-month studyperiod, since this may reflect NICE recommend-ations for duration of treatment,[19] rather thannon-remission of the symptoms of depression.However, exploration of the total cost of thisgroup found them to be slightly more expensivethan those who withdrew and relapsed and sub-stantially more expensive than those demon-strating successful withdrawal, a difference thatcannot be explained by the cost of medicationalone. This finding does not support the hypo-thesis that those prescribed antidepressants con-tinuously over the 12-month study period werebeing maintained on antidepressants whilst inremission of symptoms. Further support for thevalidity of our definition of remission is providedby recent evidence from a Spanish retrospectivedatabase study that found the measurement ofremission defined according to antidepressantcessation from computerized records to be validand reliable when compared with remission de-fined according to clinical criteria.[11]
Second, there was some evidence to suggestthat those who remitted were less severely de-pressed at the time of first antidepressant pre-scription and were less costly in the 6-monthperiod prior to the index prescription date thanthose who did not remit, although adjusted ana-lyses, including clinical indicators of severity andbaseline costs, did not alter the statistical signif-icance of the cost differences reported. In order toexplore this concern further, a subgroup analysiswas performed for the population of patients di-agnosed with severe depression. For total costs,the findings of this analysis replicated the find-ings for the population as a whole, with thosein remission being associated with significantlylower total cost on average than those not achiev-ing remission. A multivariable analysis was also
168 Byford et al.
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

conducted to account for the effect of potentialconfounders. However, as some factors (such asethnicity, marital status or co-morbidity) werenot considered in the model, the possibility ofbias in the estimation of the effect of remission onthe use of healthcare services cannot be excluded.The exclusion of these variables may also explainthe modest predictive power of the model used topredict remission.
Third, the perspective taken was limited tohealth services and excluded productivity losses,for example, known to constitute a substantialproportion of the total costs of depression.[23]
Whilst this means that total costs to society areunderestimated, evidence suggests that remissionfrom depression is associated with a significantlyimproved ability to work and thus the inclusionof productivity losses is unlikely to alter thefindings presented here and is more likely to in-crease the strength of the relationships reported.
Within the health service perspective, informa-tion regarding length of stay in hospital was notavailable from the GPRD, so a mean cost peradmission was applied, assuming a constant lengthof stay, rather than a cost per day. It is possiblethat this hides differences between remitters andnon-remitters, and thus conclusions regardingthe cost of hospitalizations should be drawn withcaution. Costs reported here are somewhat lowerthan those reported in recent UK randomized con-trolled trials, such as the THREAD (THREsholdfor AntiDepressant response) study,[24] particularlyin relation to hospitalization costs. This is mostlikely to reflect differences in data collection meth-ods, with trials generally capturing a broader rangeof health services through the use of patient serviceuse questionnaires, rather than relying on generalpractice databases. This is in line with evidence tosuggest that, whilst general practice records providemore accurate data than patient report on the useof general practice-based contacts, they provide lessreliable information on contacts with other healthservices, with patients consistently reporting highernumbers of contacts than GP records.[25]
Finally, the point at which remission began(cessation of antidepressant treatment) couldoccur at any time during the 12-month study pe-riod from date of index antidepressant prescrip-
tion, that period over which service use data werecollected. Thus, the data reported include serviceuse that occurs before, during and after remission.The impact of this is an inability to determinewhether the cost savings associated with remissionare subsequent to the remission or begin prior tothe remission. To minimize the impact of thislimitation and maximize the service use and costdata that fall after the start of remission, an ana-lysis was performed on a subgroup of patients whoremitted early (onset of remission within 8 monthsof index antidepressant prescription) comparedwith those who remitted later (onset of remission9–12 months after index antidepressant prescrip-tion). The findings replicated the results in thepopulation as a whole. Similarly, it is not possibleto determine whether the additional costs asso-ciated with non-remission are borne whilst parti-cipants are still on medication, which may suggestthat their medication is not working effectively, orafter cessation of medication in those who attemptwithdrawal but relapse within 6 months, whichmay suggest inappropriately early withdrawal,perhaps due to adverse effects or lack of effec-tiveness. It is likely to be a combination of both,with non-remitters receiving more services whilston medication and after a relapse following anattempt to cease antidepressant medication.
Conclusions
Evidence from a large general practice researchdatabase suggests that the successful cessation ofantidepressant treatment (cessation for a mini-mum of 6 months) in adults with depression isassociated with lower health service use and coststhan non-remission. Given evidence to support thevalidity and reliability of cessation of antidepres-sant treatment as a measure of clinical success,these results suggest there may be a substantialeconomic burden associated with ineffective de-pression management, compared with successfullytreated depression. Future research should rep-licate this analysis to explore the impact of the2004 NICE guidelines for depression,[19] whichrecommend longer periods of antidepressant usethan is demonstrated in the current cohort.
Impact of Treatment Success on Cost in Depression 169
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)

Acknowledgements
This work was funded by H. Lundbeck A/S. The fundingorganization were involved in the design of the study, pro-vided statistical support to collect and analyse the data(Nicolas Despiegel), commented on drafts of the documentand approved the final version.
Sarah Byford and Barbara Barrett received funding fromH. Lundbeck A/S to undertake the work. Nicolas Despiegel isa full-time employee of H. Lundbeck A/S.
Alan Wade has acted as a consultant to and has receivedlecture fees and research grants from H. Lundbeck A/S.He received no direct funding for his contribution to thismanuscript.
References1. Simon G, Ormel J, VonKorff M, et al. Health care costs
associated with depressive and anxiety disorders in primarycare. Am J Psychiatry 1995; 152 (3): 352-7
2. Katon WJ. Clinical and health services relationships be-tween major depression, depressive symptoms, and generalmedical illness. Biol Psychiatry 2003; 54 (3): 216-26
3. Simon GE, Khandker RK, Ichikawa L, et al. Recovery fromdepression predicts lower health services costs. J Clin Psy-chiatry 2006; 67 (8): 1226-31
4. Sobocki P, Ekman M, Agren H, et al. The mission is re-mission: health economic consequences of achieving fullremission with antidepressant treatment for depression.Int J Clin Pract 2006; 60 (7): 791-8
5. van Schaik DJF, Klijn AFJ, van Hout HPJ, et al. Patients’preferences in the treatment of depressive disorder in pri-mary care. Gen Hosp Psychiatry 2004; 26: 184-9
6. Cooper C, Bebbington P, King M, et al. Why people do nottake their psychotropic drugs as prescribed: results fromthe 2000 National Psychiatric Morbidity Survey. ActaPsychiatr Scand 2007; 116: 47-53
7. Moore M, Yuen HM, Dunn N, et al. Explaining the rise inantidepressant prescribing: a descriptive study using thegeneral practice research database. BMJ 2009; 339: b3999
8. The General Practice Research Database (GPRD) [online].Available from URL: http://www.gprd.com [Accessed2008 Sep 5]
9. Montgomery SA, AsbergM. A new depression scale designedto be sensitive to change. Br J Psychiatry 1979; 134: 382-9
10. Hawley CJ, Gale TM, Sivakumaran T. Defining remissionby cut off score on the MADRS: selecting the optimalvalue. J Affective Disord 2002; 72 (2): 177-84
11. Sicras-Mainar A, Blanca-Tamayo M, Navarro-Artieda R,et al. Clinical validity of remission in patients with majordepression in population databases [abstract no. PMH50].Value Health 2009; 12 (7): A360
12. Curtis L, Netten A. Unit costs of health and social care2006. Canterbury: Personal Social Services Research Unit,2006
13. Department of Health. NHS reference costs 2006. London:Department of Health, 2006
14. British Medical Association, Royal Pharmaceutical Society.British national formulary. London: British Medical As-sociation, 2006
15. Hospital Episode Statistics (HESonline�) [online]. Avail-able from URL: http://www.HESonline.nhs.uk [Accessed2008 Sep 5]
16. WHO Collaborating Centre for Drug Statistics Methodol-ogy. ATC/DDD index 2010 [online]. Available from URL:http://www.whocc.no/atcddd [Accessed 2008 Sep 5]
17. Martinez C, Rietbrock S, Wise L, et al. Antidepressanttreatment and the risk of fatal and non-fatal self harm infirst episode depression: nested case-control study. BMJ2005; 330: 389-93
18. McCullagh P, Nelder J. Generalized linear models. London:Chapman and Hall, 1989
19. National Institute for Health and Clinical Excellence.Depression: management of depression in primary andsecondary care. Clinical guideline 23. London: NICE, 2004
20. Paykel ES, Priest RG. Recognition and management of de-pression in general practice: consensus statement. BMJ1992; 305: 1198-202
21. Glick HA, Briggs AH, Polsky D. Quantifying stochasticuncertainty and presenting results of cost-effectiveness anal-yses. Exp Rev Pharmacoeconomics Outcomes Res 2001;1 (1): 25-36
22. Rodin G, Voshart K. Depression in the medically ill: anoverview. Am J Psychiatry 1986; 143: 696-705
23. Thomas CM, Morris S. Cost of depression among adults inEngland in 2000. Br J Psychiatry 2003; 183: 514-9
24. Kendrick T, Chatwin J, Dowrick C, et al. Randomisedcontrolled trial to determine the clinical effectiveness andcost-effectiveness of selective serotonin reuptake inhibitorsplus supportive care, versus supportive care alone, for mildto moderate depression with somatic symptoms in primarycare: the THREAD (THREshold for AntiDepressant re-sponse) study. Health Technol Assess 2009 Apr; 13 (22):iii-iv, ix-xi, 1-159
25. Byford S, Leese M, Knapp M, et al. Comparison of alter-native methods of collection of service use data for theeconomic evaluation of health care interventions. HealthEcon 2007; 16: 531-6
Correspondence: Dr Sarah Byford, King’s College London,Centre for the Economics of Mental Health, P024, Instituteof Psychiatry, De Crespigny Park, London SE5 8AF, UK.E-mail: [email protected]
170 Byford et al.
ª 2011 Adis Data Information BV. All rights reserved. Pharmacoeconomics 2011; 29 (2)