Embed Size (px)
DESCRIPTION
Depression Treatment
Citation preview

Depression Depression TreatmentsTreatmentsDrugs
Tricyclic Antidepressants (TCAs) • Some of the first antidepressants• Three-ring antihistaminic chemical structure• Tofranil (1958), Elavil, Norpramin, Pamelor•Affect Norepinephrine and Serotonin• Prior to TCAs severely depressed patients would have only 2 options: Amphetamines or Electroshock Therapy• Side effects & Dietary restrictions can be severe. These aren’t prescribed unless newer safer treatments have failed• About 70% of patients responded to tricyclics
Monoamine Oxidase Inhibitors (MAOIs)• Among the earliest depression treatments• Nardil, Parnate, Marplan• Blocks monoamine oxidase which breaks down NE, 5-HT, and DA• MAO is also responsible for breaking down Tyramine, a molecule affecting blood pressure.• Interacts with certain foods containing tyramine (aged cheese, wines, chocolate, bananas, chicken liver)• A rise In Tyramine may cause death by brain hemorrhages• Usually prescribed as a last resort to patients with severe treatment resistant depression
Kevin Yetman

Drugs
Serotonin and Norepinephrine Reuptake Inhibitors (SNRIs)• Newer• Effexor, Pristiq, Cymbalta• Similar to SSRI’s but affect both 5-HT (influencing mood), and NE (believed to be more involved with alertness and energy) attacking 2 aspects of depression• This dual action offers an advantage (over SSRIs) in certain patients
Aminoketones• Wellbutrin• Mechanism is not known for sure, but it is understood to be a relatively weak inhibitor of the neuronal uptake of Norepinephrine, Serotonin, and Dopamine• Ideal for patients who do not respond to, or who experience unacceptable side effects with other anti- depressants• Side effects are generally milder and include less chance of sexual side effects
Selective Serotonin Reuptake Inhibitors (SSRIs)• Introduced mid to late 1980’s, today’s most common antidepressant• Celexa, Lexapro, Luvox, Paxil, Prozac, Zoloft• Blocks reuptake of Serotonin (prolongs response)• Side effects less severe (stomach upset, sexual problems, fatigue, dizziness, weight change, and headaches.)• Approximately 60-80% success rate

PsychotherapyCognitive-Behavioral Therapy (CBT)
• Many approaches to CBT: Rational Emotive Behavior Therapy, Rational Behavior Therapy, Rational Living Therapy, Cognitive Therapy, Dialectic Behavior Therapy • Based on the idea that thoughts cause feelings and behaviors (not external things such as people, situations, and events)• Therefore we can change the way we think to affect the way we feel and act• Inductive Method: Rational thinking = based on fact
Encourages clients to look at thoughts as hypotheses which can be questioned
and tested. When negative thoughts are found to be incorrect, the client can change their thinking to reflect this revelation• Socratic Method: Therapist asks questions, and encourage clients to ask questions of themselves For example: “How do I really know that those people are laughing at me?" "Could they be laughing about something else?"• Average of 16 sessions (one of the most rapid forms of psychotherapy)• CBT is highly structured, therapists have a specific agenda for each session • Therapists help their clients come up with goals, then show them ways to think and behave in order to obtain those goals• Homework is integral: Techniques learned in therapy are practiced and reading is sometimes assigned
Cognitive Model of Emotional Response

PsychotherapyInterpersonal therapy• Focus on practical issues and relationships. Emphasis on recognizing and changing unhealthy behaviorsPsychodynamic therapy• Get to roots of depression (possibly explore childhood traumas)Family counseling• Focuses on family aspect of depression• Not only treats the individual, but educates and helps all involved deal with stress of emotional illness.
Group counseling• Allow for sharing and relating of feelings• “Give and take” aspect of group sessions can change the way patients view their illness and improve coping abilityAll Therapy•Helps to form coping strategies & Increases adherence to medication •A 2004 review published in the Archives of General Psychiatry concluded that therapy combined with antidepressants was better than medication alone, and that therapy encourages compliance to drug treatments.

Electroconvulsive Therapy (ECT)• aka Electroshock therapy• Treats severe depression• Patient is given a muscle relaxant and is put to sleep with general anesthesia• Electric current is briefly applied through the scalp to the brain• This pulse produces a seizure by exciting the brain cells & causing them to fire in unison• Performed up to 3 times a week for 2-4 weeks (6-12 treatments) - Average is 9 treatments
• Only used in severe cases (after not responding to other treatments) or when patient requires immediate help (poses threat to self /others)
• Major side effects: Short term confusion following procedure, memory loss- (a) difficulty in retaining new memories, and (b) gaps in events from the past. Both are often temporary, but in some cases permanent gaps in memory may occur.
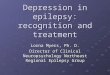
Right Unilateral Electrode Placement

Electroconvulsive Therapy (ECT)
Right Unilateral Electrode Placement
Bilateral Electrode Placement
• It is not specifically known the exact reason for the positive results of ECT• A few theories include:
- The seizure itself causes an alteration of neurotransmitters
- ECT may adjust stress hormone regulation in the brain (affecting energy, sleep, appetite, and mood)• Right Unilateral Treatment: - Somewhat slower response compared to those receiving bilateral treatment (generally only 1 – 2 treatments) - Typically fewer memory side effects• Bilateral Treatment: - Indicated for severe mental illness (including those who do not respond to right unilateral treatment) - May be associated with more memory side effects
EEG Seizure Activity
EEG Seizure Termination
• According to WebMD, 80-90% of patients who receive ECT see improvement• According to a Mayo Medical School survey, 91% of respondents had positive attitudes about the ECT treatment they received

Deep Brain Stimulation• Developed in France in 1987
• Evolved out of ablative or lesioning surgeries where doctors would permanently damage regions of the brain with a heat probe
• Originally treated Parkinson’s disease
• Today used for treatment of Parkinson’s, Depression, OCD, Epilepsy, Chronic pain, Tourette’s, among others…
• Most invasive form of brain stimulation treatment for depression.
• The limbic structures that regulate mood feed into the frontal cortex, striatum, thalamus, hypothalamus and brain stem. Constantly communicating
• A problem with part of this circuit may lead to abnormalities in thinking, mood, attention, and behavior

Deep Brain Stimulation
• Electrodes pump steady pulses of electricity
• Over five years, no adverse side effects have been observed in patients treated for depression with deep brain stimulation in Brodmann Area 25
• Unit can be programmed up to 60,000 different ways, fine tuning is required
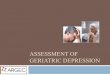
• Brodmann area 25 (part of the subgenual cingulate region) has been found to be unusually overactive in depressed patients
• This region has strong connections with nucleus accumbens, amygdala, hypothalamus, and orbitofrontal cortex
• Electrodes 1mm thick are implanted in this area then wires are run under the skin to the chest where a power pack is implanted.
• Positron emission tomography (PET) scan of Brodmann area 25• Top image shows over activity (red)• Bottom image shows reduced activity (blue) after 6 months of DBS treatment

Repetitive Transcranial Magnetic Stimulation (rTMS)• NeuroStar TMS device
• Experimental in US, approved/available in Canada
• Used to treat milder treatment resistant Depression (where one to two meds have failed), Schizophrenia, Mania, OCD, and neurological conditions like stroke, Parkinson’s Disease, Migraine, Multiple Sclerosis, Autism,
• Magnetic field is applied to left dorsolateral prefrontal cortex (DLPFC) which is a few inches above the temple and beneath the skull. • DLPFC is highly interconnect w/limbic structures which play dominant role in mood modulation and major depression.
• Individuals suffering from depression often portray insufficient levels of glucose metabolism, and lower blood flow in the DLPFC and increased activity in the Limbic system

• The magnetic current that is created in DLPFC regulates the interaction between neurons to increase or decreases activity in the proper regions to relieve symptoms • Some research suggests that rTMS regulates beta adreno receptors and increases Dopamine and Serotonin levels.
• Can alter activity in more remote brain areas also thought to affect depression through focal cortical stimulation
• Indirect stimulation occurs via trans-synaptic effects (the directly stimulated area (DLPFC) indirectly stimulates less accessible areas)
• Different frequencies may be applied (10 Hz = moderately fast)
• No seizure, no loss of consciousness, no sedation
• Treated 4-5 times per week for 4 weeks.
• During trials active rTMS had better rates of response than sham rTMS
Repetitive Transcranial Magnetic Stimulation (rTMS)

ReferencesNazario, Brunilda MD. “Depression Medicines.” WebMD. 7 July 2009 <http://www.webmd.com/depression/guide/optimizing-depression-medicines>
Croft, Harry MD. “List of Antidepressants.” Healthy Place. 12 Feb. 2009<http://www.healthyplace.com/depression/antidepressants/list-of-antidepressants/menu-id-68/>
“Cognitive-Behavioral Therapy.” National Association of Cognitive-Behavioral Therapists.<http://www.nacbt.org/whatiscbt.htm>
Nazario, Brunilda MD. “Psychotherapy for Depression.” WebMD. 30 Oct. 2009<http://www.webmd.com/depression/guide/treatment-resistant-depression-psychotherapy>
Hoffman, Matthew MD. “Electroconvulsive and Other Depression Therapies.” WebMD. 3 May 2008 <http://www.webmd.com/depression/guide/electroconvulsive-therapy>
“[ECT] Side Effects and Risks.” The University Hospital. <http://www.theuniversityhospital.com/ect/effects.htm>
“How Does ECT Work?” Electroconvulsive Therapy Program, University of Michigan Psychiatry. <http://www.psych.med.umich.edu/ECT/how-does-ECT-work.asp>
Song, Sora. “How Deep-Brain Stimulation Works.” Time. 16 Jul. 2006. <http://www.time.com/time/magazine/article/0,9171,1214939,00.html>

Bubnoff, Andreas von. “With deep brain stimulation, experts want to tread carefully.” Los Angeles Times. 1 June 2009. <http://www.latimes.com/features/health/la-he-deep-brain-risks1-2009jun01,0,4634809.story>
Talan, Jamie. “Deep Brain Stimulation Offers Hope in Depression.” The DANA Foundation. 31 Mar. 2008. <http://www.dana.org/news/cerebrum/detail.aspx?id=12622>
“What is Repetitive Transcranial Magnetic Stimulation?” Yale University Dept. of Psychiatry. 11 Mar. 2009. <http://www.med.yale.edu/psych/clinics/rTMS.html>
Dubovsky, Steven MD. “rTMS for Refractory Depression?” Journal Watch Psychiatry. 8 Mar. 2006. <http://psychiatry.jwatch.org/cgi/content/full/2006/308/1>
“Depression.” Mindcare Centers. 2007. <http://www.mindcarecentres.com/diseasestates/depression.aspx>
Johanson-Berg H. “Anatomical connectivity of the subgenual cingulate region targeted with deep brain stimulation for treatment-resistant depression.” University of Oxford. 18 Jun. 2008 <http://www.ncbi.nlm.nih.gov/pubmed/17928332>
Goodman, JA. “Patient satisfaction with electroconvulsive therapy.” Mayo Medical School. Oct. 1999. <http://www.ncbi.nlm.nih.gov/pubmed/10918861?dopt=Abstract>
References continued