Embed Size (px)
Citation preview
R U T H S H I M , M D , M P H
A S S I S T A N T P R O F E S S O R , D E P A R T M E N T O F P S Y C H I A T R Y A N D B E H A V I O R A L S C I E N C E S
A S S O C I A T E D I R E C T O R O F B E H A V I O R A L H E A L T H , N A T I O N A L C E N T E R F O R P R I M A R Y C A R E
Effective Treatment of Depression in Older African Americans:
Overcoming Barriers
Objectives
To review the epidemiology of late life depression
To discuss racial/ethnic disparities in late life depression
To describe the depression care process
To examine evidenced-based treatment of depression in older adults
Overview of Depression
The leading cause of disability worldwide
4th leading cause of total disease burden
16.2% lifetime prevalence in the United States (conservative estimate)
6.6% 12 month prevalence in the US
Late-Life Depression
Depression is the most prevalent psychiatric diagnosis among the elderly
Prevalence in adults aged 65 and older in 2004:
17% of women
11% of men
Depression in elderly leads to increased disability, morbidity, and risk of suicide, poor adherence with medical treatments, increased mortality from medical illnesses
Late-Life Depression by Setting
Prevalence of major depression in older Americans
Community Settings (1-3%)
Primary Care Settings (5-9%)
Institutional Settings (12-30%)
Depression is more prevalent among younger adults, but older adults are less likely to be identified and treated
Diagnosing Depression in Older Adults
Depression should not be considered just a normal part of aging
Depression in older adults may look different than in younger adults
More anxiety and anhedonia symptoms
More physical health problems
More ambivalence about life
“Sadless depression”
Depression can be confused with dementia
“Pseudodementia”

Challenges in Late-Life Depression
Depression can be confused with the effects of multiple illnesses and the medications used to treat older adults
Comorbidities are the rule, not the exception
Advancing age results in loss of support systems (death of spouse, siblings, retirement, relocation), which increase the risk for depression
Disparities in Treatment Engagement and Retention
Older adults seek mental health treatment less than any other age group
50% of adults over 65 are in need of mental health services, only 20% receive treatment
Older adults prefer psychotherapy to pharmacotherapy, but are rarely follow up when given a referral to therapy
Barriers for African Americans Older Adults with Depression
African American older adults are less likely to receive an accurate diagnosis of depression compared to White older adults
African American older adults are less likely to receive empirically supported treatments for depression compared to White older adults
Barriers for African Americans
African American older adults suffer more psychological distress due to racism, discrimination, poverty, violence, etc.
African American older adults often have fewer psychological, social, and financial resources for coping with stress than White older adults
Comorbidities in Older Adults
Late-Life Depression
Doubles the risk of cardiac diseases
Increases the risk of death from medical illness
Reduces the ability to rehab from medical illness
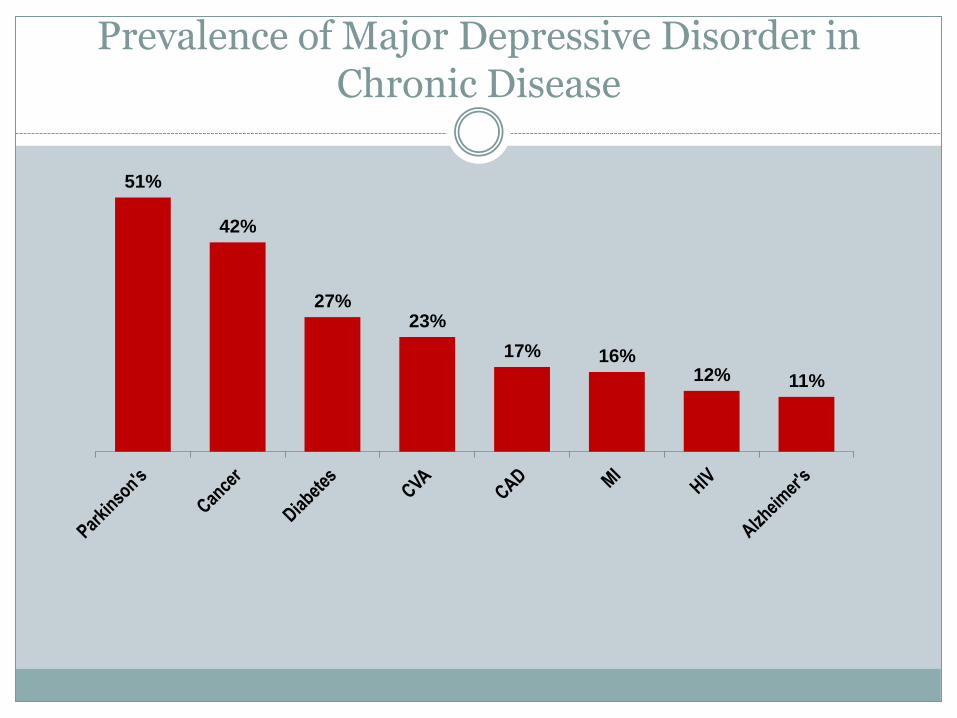
Prevalence of Major Depressive Disorder in Chronic Disease
51%
42%
27% 23%
17% 16% 12% 11%
Challenges in Elderly Underserved, Low Income Populations
Poor access to care
Disability
Mild Cognitive Impairment
Dealing with Social Adversity
Depression in the Elderly and Suicide
Increased risk of suicide in elderly
Suicide rate in people ages 80 to 84 is twice that of the general population
Suicide in people age 65 and older is a major public health problem
Myths about Treating Late Life Depression
Mental health treatment is not effective
There is no cure for depression
Antidepressants are addictive and like street drugs
There are too many side effects with antidepressant medications
African American Older Adults
More likely to deal with depression through:
Informal support networks
Church
Primary care physicians
Depression in African Americans is less likely to be detected in primary care than it is in whites
Cultural Coping Strategies
Self-reliance
Keeping busy
Staying active in the community
Cooking and cleaning
Self-medicating – alcohol and nicotine
Pushing through the depression
Denial
Relying upon God
Racial/Ethnic Disparities Among Older Adults
African Americans seek treatment at half the rate of Whites
Attend fewer sessions when they do seek treatment
Tend to terminate treatment prematurely
Limited research shows African American older adults with depression are less likely:
To be in treatment
To intend to seek treatment in the future
To have ever sought mental health treatment for depression

Barriers to Treatment
Ageism
Shame/Stigma
Cultural Barriers
Fear/Distrust of the Treatment System
Lack of Knowledge
Lack of Insurance/Financial Barriers
Transportation
African Americans have greater negative attitudes toward seeking treatment (in some studies)
Depression Care Process
Step 1: recognition and diagnosis
Step 2: patient education
Step 3: treatment
Step 4: monitoring
Step 1: Recognition and Diagnosis
The clinician suspects that a patient may be depressed
Patient may self-identify
Patient may present with somatic complaints
Clinician may use screening tools
Formal assessment must be done to confirm the diagnosis
Step 2: Patient Education
Clinician and staff education patient about depression and the care process
Engage the patient
Determine patient preference for treatment
Patient Education
EXTREMELY IMPORTANT
Stigma and lack of education will lead many people to avoid treatment
Information about what depression is (and is not)
Steps involved in treatment
How antidepressants work – common questions and answers
What to expect from psychological counseling
Step 3: Treatment
Clinician and patient select the appropriate management approach
Three Phases of Treatment
Acute – aims to minimize depressive symptoms and achieve remission
Continuation – tries to prevent return of symptoms during current episode
Maintenance – focus is to prevent lifetime return of new episodes
Treatment for Depression in Elderly
Medication
Psychotherapy
Electroconvulsive therapy (ECT)
Antidepressant Medications
Medications are equally effective in older adults
SSRIs are well tolerated
May take longer to start working
May need to start at lower doses in elderly
Tricyclic antidpressants
Orthostatic hypotension – increased risk of falls
Urinary retention
Less well tolerated at effective doses
Anticholinergic effects
Cardiac side effects
Antidepressant Medications
SSRIs Fluoxetine
Sertraline
Paroxetine
Citalopram/Escitalopram
SNRIs Venlafaxine/Desvenlafaxine
Duloxetine
Other Antidepressants Mirtazapine
Bupropion

Psychotherapy
In general, many African Americans prefer psychotherapy (in theory) to medication
Referral and follow through is often difficult
Access to effective therapy is limited in underserved populations
Limited providers
Insurance limitations
Psychotherapy Preference
Although preferred, few older African Americans use this option
50% copayment for outpatient psychotherapy under Medicare
Less practical – weekly appointments
Electroconvulsive Therapy
Extremely effective in older adults
Barriers include access/availability
Effective when medications are contraindicated, or when there has been limited response to medication
Stigma regarding ECT limits availability of this therapy
Step 4: Monitoring
The clinician and support staff monitor compliance with the plan and improvement in symptoms/function
Modify treatment as appropriate
Goal is remission
Stepped-Care
Aims to provide the most effective but least intrusive treatment appropriate to an individual's needs
Assumes that the course of the disorder is monitored and referral to the appropriate level of care is made depending on the person’s difficulties
Each step introduces additional interventions
Higher steps normally assume interventions in previous steps have been offered and/or attempted
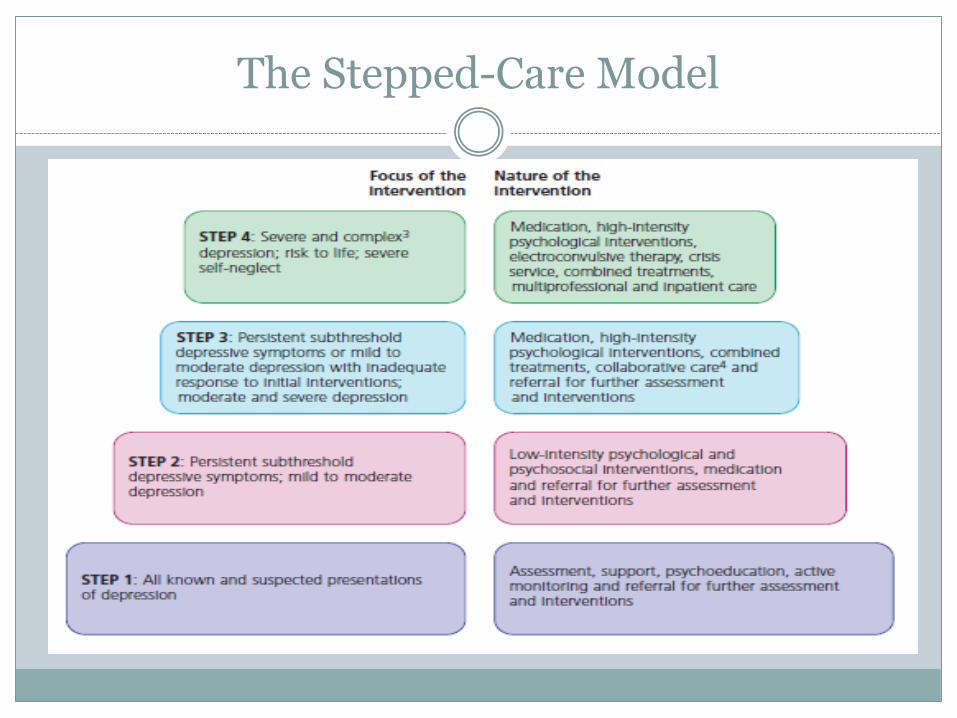
The Stepped-Care Model
Conclusions
Late life depression is a major public health problem that must be addressed
Racial/ethnic disparities exist in the diagnosis and treatment of late life depression
Late-life depression is treatable and recovery is possible
Specific treatment of depression should be tailored to fit the unique needs of African American older adults
References
1. Alston, M.H., S.H. Rankin, and C.A. Harris, Suicide in African American Elderly. Journal of Black Studies, 1995. 26(1): p. 31-35.
2. Blazer, D.G. and C.F. Hybels, Origins of depression in later life. Psychological medicine, 2005. 35(09): p. 1241-1252.
3. Comer, R.J., Abnormal psychology. 2009: Worth Pub. 4. Conner, K.O., et al., Mental health treatment seeking among older adults with depression: the impact of
stigma and race. American Journal of Geriatric Psych, 2010. 18(6): p. 531. 5. Conner, K.O., et al., Barriers to treatment and culturally endorsed coping strategies among depressed
African-American older adults. Aging & mental health, 2010. 14(8): p. 971-983. 6. Conner, K.O., et al., Attitudes and beliefs about mental health among African American older adults
suffering from depression. Journal of Aging Studies, 2010. 24(4): p. 266-277. 7. Cooper, L.A., et al., The acceptability of treatment for depression among African-American, Hispanic,
and white primary care patients. Medical Care, 2003. 41(4): p. 479. 8. Gallo, J.J., L. Cooper-Patrick, and S. Lesikar, Depressive symptoms of whites and African Americans
aged 60 years and older. The Journals of Gerontology Series B: Psychological Sciences and Social Sciences, 1998. 53(5): p. P277.
9. Gum, A.M., et al., Depression treatment preferences in older primary care patients. The Gerontologist, 2006. 46(1): p. 14.
10. Unützer, J., et al., Depression treatment in a sample of 1,801 depressed older adults in primary care. Journal of the American Geriatrics Society, 2003. 51(4): p. 505-514.
11. Wang, P.S., P. Berglund, and R.C. Kessler, Recent care of common mental disorders in the United States. Journal of General Internal Medicine, 2000. 15(5): p. 284-292.
12. Young, A.S., et al., The quality of care for depressive and anxiety disorders in the United States. Archives of General Psychiatry, 2001. 58(1): p. 55.
T H A N K Y O U !
R S H I M @ M S M . E D U
Questions/Comments