Embed Size (px)
Citation preview

IB
Siw(saptfamcistas
D
A
1
mitators of Severe Pre-eclampsiaaha M. Sibai, MD
There are many obstetric, medial, and surgical disorders that share many of the clinical andlaboratory findings of patients with severe pre-eclampsia–eclampsia. Imitators of severepre-eclampsia–eclampsia are life-threatening emergencies that can develop during preg-nancy or in the postpartum period. These conditions are associated with high maternal andperinatal mortalities and morbidities, and survivors may face long-term sequelae. Thepathophysiologic abnormalities in many of these disorders include vasospasm, plateletactivation or destruction, microvascular thrombosis, endothelial cell dysfunction, andreduced tissue perfusion. Some of these disorders include acute fatty liver of pregnancy,thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, acute exacerbation ofsystemic lupus erythematosus, and disseminated herpes simplex and sepsis syndromes.Differential diagnosis may be difficult due to the overlap of several clinical and laboratoryfindings of these syndrome. It is important that the clinician make the accurate diagnosiswhen possible because the management and complications from these syndromes may bedifferent. Because of the rarity of these conditions during pregnancy and postpartum, theavailable literature includes only case reports and case series describing these syndromes.This review focuses on diagnosis, management, and counseling of women who developthese syndromes based on results of recent studies and my own clinical experience.Semin Perinatol 33:196-205 © 2009 Elsevier Inc. All rights reserved.
KEYWORDS severe pre-eclampsia, acute fatty liver, TTP, HUS
AAfdTptgwowotpsaaempa
j
everal microangiopathic disorders that are encounteredduring pregnancy provide physicians with a formidable,
f not impossible, diagnostic challenge. Severe pre-eclampsiaith hemolysis, elevated liver enzymes, and low platelets
HELLP) syndrome and many other obstetric and medical orurgical conditions produce similar clinical presentationsnd laboratory study results to pre-eclampsia.1 In addition,re-eclampsia is not infrequently superimposed upon one ofhese disorders, further confounding an already difficult dif-erential diagnosis. Because of the remarkably similar clinicalnd laboratory findings of these disease processes, even theost experienced physician will face a difficult diagnostic
hallenge.1 Therefore, an effort should be made to attempt todentify an accurate diagnosis given the fact that managementtrategies and outcome may differ among these conditions. Inhis review, I will describe the pathogenesis, differential di-gnosis, and management of the medical conditions de-cribed in the box below.
epartment of Obstetrics and Gynecology, University of Cincinnati, Collegeof Medicine, Cincinnati, OH.
ddress reprint requests to Baha M. Sibai, MD, Department of Obstetrics andGynecology, University of Cincinnati, 231 Albert Sabin Way, Cincinnati,
fiOH 45267. E-mail: [email protected]
96 0146-0005/09/$-see front matter © 2009 Elsevier Inc. All rights reserved.doi:10.1053/j.semperi.2009.02.004
cute Fatty Liver of Pregnancycute fatty liver of pregnancy (AFLP) is a rare but potentially
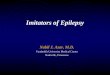
atal complication of the third trimester. The incidence of thisisorder ranges from 1 in 10,000 to 1 in 15,000 deliveries.he incidence is probably lower than that because the re-orted rates are usually from large referral centers, whichend to overestimate the true incidence.1-11 It has been sug-ested that AFLP is more common in nulliparous women asell as in those with multifetal gestation.1-7,9 The clinical onsetf symptoms ranges from 27 to 40 weeks, with an average of 36eeks’ gestation6; however, cases have been reported in the sec-nd trimester.11,2 In some cases, the first onset of signs/symp-oms may be in the postpartum period.2,9 The patient typicallyresents with a 1- to 2-week history of malaise, anorexia, nau-ea, vomiting, midepigastric or right upper quadrant pain, head-che, or jaundice. The urine will have a bright yellow appear-nce (Fig. 1). Rarely, the patient may present with hepaticncephalopathy.13 Symptoms of preterm labor or lack of fetalovement may be the presenting complaint in some of theseatients.2,3 In about 15-20%, the patient might not present withny of the above symptoms.2-5
Physical examination reveals an ill-appearing patient withaundice. Some patients will have a low-grade fever. Other
ndings may include hypertension and even proteinuria and
atpm
LTtivlla(aeenBapbetmt
isodCic
nlbss
isptu
dlRavt
MAic�bRwwipbyap
n55e((hPfot
pbIF
fi
T
●●●●●●●●
Imitators of severe pre-eclampsia 197
scites and bleeding from severe coagulopathy. Because ofhese findings, the diagnosis may be initially confused withre-eclampsia.1,2,6 Neurologic findings may range from nor-al to lethargy, agitation, confusion, and even coma.8,9,13,14
aboratory Findingshe complete blood count usually reveals hemoconcentra-
ion, elevated white blood count, and platelet count that isnitially normal but may be low.1-6 Coagulation findings re-eal low fibrinogen, prolonged prothrombin time (PT), andow levels of antithrombin.1-10 These abnormalities are re-ated to reduced production of these factors by the liver andre consistent with disseminated intravascular coagulopathyDIC). In contrast, the DIC seen in severe pre-eclampsia andbruptio placentae is due to abnormal consumption.15 Serumlectrolytes will reveal evidence of metabolic acidosis withlevated creatinine and uric acid values. Blood sugar may beormal but is usually low in the postpartum period.1-6,8,9,13
lood sugars may also be elevated in association with second-ry pancreatitis.1,8 Liver enzymes, such as AST, ALT, alkalinehosphatase, and bilirubin, will be elevated. The increase inilirubin is mainly of the conjugated form, with levels usuallyxceeding 5 mg/dL. Ammonia levels are also increased, par-icularly in late stage of the disease. Amylase and lipase valuesay be elevated in the presence of concomitant pancreati-
is.1,8 Hepatitis profile for A, B, and C will be negative.Ultrasonography of the liver may reveal the presence of
ncreased echogenicity in severe cases; however, it is lessensitive than computed tomography (CT) and magnetic res-nance imaging (MRI).16-20 In addition, quantitation of liverensity by ultrasound is subjective and operator-dependent.T scan of the liver may show decrease or diffuse attenuation
n the liver. However, none of these techniques are suffi-iently sensitive to exclude a diagnosis of AFLP.2,20
Liver biopsy is the gold standard for confirming the diag-osis of AFLP. Histopathologic findings in AFLP reveal swol-
en, pale hepatocytes with central nuclei.21 The diagnosis cane made only on a frozen section liver biopsy with specialtains for fat, such as oiled red (O).1,4 Plans to perform thistain should be made before the biopsy procedure because it
igure 1 Liver biopsy findings in herpes hepatitis. (Color version of
hgure is available online.)s not possible to be performed once the tissue has beenubmitted to routine paraffin blocks. Liver biopsy should beerformed only after correction of coagulopathy. However,his is rarely used in clinical practice, and the diagnosis issually made based on clinical and laboratory findings.1-9
In addition to the other conditions listed in Box I, theifferential diagnosis of AFLP should include idiopathic cho-
estasis of pregnancy, Budd-Chiari syndrome, adult-onseteye’s syndrome, and drug-induced hepatic toxicity (acet-minophen overdose, tetracycline-induced toxicity, anticon-ulsant drugs hypersensitivity, and methyldopa hepati-is).1,4,21
aternal and Perinatal ComplicationsFLP is associated with an increased risk of maternal mortal-
ty and morbidities. In the past, the rate of maternal death waslose to 70%; however, recent data indicate a mortality rate of10%, but maternal complications remain high. Table 1 descri-
es maternal complications in recent series of AFLP.1-11,14,22,23
ecently, Davidson and coworkers reported on three womenith triplet gestation who had AFLP proven by liver biopsyho survived. They suggested that women with triplets are at
ncreased risk for AFLP because of potential for increasedroduction of fatty acid metabolites by three fetuses. It haseen suggested that the improved maternal survival in recentears was related to the supportive care and aggressive man-gement of serious maternal complications by a multidisci-linary group of physicians from various specialties.2-9
Recently, Knight, and coworkers11 reported a prospectiveational study of AFLP in the UK. The participants included7 women with AFLP diagnosed mostly by clinical criteria;5 had abdominal ultrasound scan, but only 12 (27%) hadither ascites and/or abnormal liver findings. Forty-two74%) were diagnosed antepartum and 15 (26%) postpartumwithin 4 days of delivery). In general, most of these patientsad a biochemical diagnosis of AFLP (mild prolongation ofT, PTT, normal platelets), only 8 (16%) had acute renalailure, and 4 (7%) required ventilatory support. There wasnly 1 maternal death (1.8%) in a patient who received a liverransplant.14
Both perinatal mortality and morbidities are increased inatients of AFLP.2-9,20 The perinatal mortality among 160irths (142 pregnancies) in recent case series was 13.1%.9,22
n addition, neonatal morbidity remains high because of the
able 1 Imitators of Severe Pre-eclampsia/HELLP Syndrome
AFLPTTPHUSExacerbation of lupus erythematosusCatastrophic antiphospholipid syndromeSystemic viral sepsis (disseminated herpes)Systemic inflammatory response syndrome/septic shockOther conditions (cholestasis of pregnancy, necrotizingpancreatitis, etc.)
igh rate of preterm delivery (74%) among reported cases.

T2
tn
MTimAdowbNapti
dscafcsdccgthcaipbsd
gqassl
voataofh
cmbtidaot
aiozTob
2iastptpl
CScsewcclwsieecaaramc
TTloT
198 B.M. Sibai
he average gestational age at delivery was 34 weeks (range,5-42 weeks).2-9,22
In the study by Knight and coworkers,11 the perinatal mor-ality was 10.4% among 67 infants (6 stillbirths and 1 neo-atal death).
anagement of AFLPhe clinical course of women with AFLP is usually character-
zed by progressive and sometimes sudden deterioration inaternal and fetal conditions.9 Therefore, patients in whomFLP is considered require hospitalization in a labor andelivery unit. Fetal heart rate monitoring and/or performingf a biophysical profile should be performed concurrentlyith maternal evaluation. Evidence of fetal compromise maye present even in those with stable maternal conditions.onreassuring fetal testing may be secondary to maternal
cidosis and/or reduced uteroplacental blood flow.1-6 Theresence of maternal acidosis may be reflected in reduced-o-absent fetal movement, absent fetal breathing, or tone dur-ng biophysical profile testing.1
The next step in management is to confirm or exclude theiagnosis of AFLP according to the clinical findings and re-ults of blood tests.1,23 The presence of bleeding and/or severeoagulopathy requires transfusion with fresh frozen plasmand other blood products as needed. The ultimate treatmentor this condition is maternal stabilization and delivery be-ause there are no reports of women recovering from AFLPpontaneously. The presence of AFLP is not an indication forelivery by cesarean section because of the risks of bleedingomplications in the presence of coagulopathy.2-6,10 The de-ision to perform cesarean delivery should be based on fetalestational age, fetal condition, and presence of labor. Induc-ion of labor with an attempt for vaginal delivery within 24ours is a reasonable approach. Because of the associatedoagulopathy, most anesthesiologists will avoid epidural an-lgesia. Maternal analgesia during labor can be provided byntermittent use of small doses of systemic opioids. The use ofudendal block should be avoided because of the risk ofleeding and hematoma formation into this area. Cautionhould be exercised to avoid vaginal trauma and lacerationsuring vaginal delivery.1
In case of cesarean delivery, the patient should receiveeneral anesthesia. It is advisable to avoid incisions that re-uire extensive dissection, such as the Pfannenstiel incision,nd meticulous attention should be given to secure hemosta-is. It is advisable to perform a midline incision, to use aubfascial drain, and to keep the skin incision open for ateast 48 hours to avoid hematoma formation.1,23
In the postpartum period, the patient should be monitoredery closely with careful evaluation of vital signs, intake–utput, and bleeding. Some of these patients may developcute refractory hypotensive shock in the immediate postpar-um period. Serial measurements of hematologic, hepatic,nd renal function should be performed and recorded in anrganized fashion. Blood sugars should be monitored everyew hours with a bedside glucometer because of the risk of
ypoglycemia in the postpartum period. Glucose infusions ran be used to maintain blood sugars above 60 mg/dL. Ane-ia and DIC should be treated as needed by a packed red
lood cells, platelets, and fresh frozen plasma. It is importanto aggressively treat maternal hypotension to avoid furthernjury to the liver, kidneys, and other organs. Invasive hemo-ynamic monitoring may be necessary in some patients tossess fully the intravascular volumes and maintain cardiacutput, and in patients who develop acute respiratory dis-ress syndrome (ARDS).
Pancreatitis is a potentially lethal complication of AFLP,nd thus all patients with AFLP should undergo serial screen-ng of serum lipase and amylase for several days after thenset of hepatic dysfunction.1,8 Abnormalities in these en-ymes typically appear after hepatic and renal dysfunction.he development of pseudocysts with secondary infectionsr hemorrhagic pancreatitis with resultant retroperitonealleeding increases the risk for maternal death.8
In general, most patients with AFLP will start to improve-3 days after delivery. In some cases, however, deterioration
n liver function tests, renal function, mental status, and co-gulopathy may continue for about 1 week. In such cases,ome authors suggest using plasmapheresis to improve ma-ernal outcome. This method of treatment was recently re-orted in six such cases with no maternal death. However,he value of such therapy remains unclear. In rare cases, aatient will progress into fulminant hepatic failure, requiring
iver transplantation.21
ounseling of Women with AFLPeveral case reports and case series22-26 have noted an asso-iation between the development of AFLP and/or HELLPyndrome and a deficiency of long-chain 3-hydroxyacyl-co-nzyme A dehydrogenase (LCHAD) in infants born toomen with the above complications. This disorder of mito-
hondrial fatty acid oxidation might lead to significant in-rease in maternal fatty acid levels that are highly toxic to theiver. Based on these findings, some authors suggest thatomen with AFLP as well as their partners and children
hould undergo molecular testing for Glu 474 Gln mutationn the LCHAD.22,24 Screening for this mutation would allowarly diagnosis and treatment in newborns of affected moth-rs and would allow counseling about subsequent pregnan-ies.22,25 The risk of recurrence is increased in women whore carriers for this mutation, particularly if the fetus is alsoffected during a subsequent pregnancy. There are few caseeports describing recurrent AFLP in women without thebove mutation2,4; however, the risk of this recurrence re-ains unknown because of the limited number of pregnan-
ies reported following AFLP in these women.
hrombotic Microangiopathieshrombotic thrombocytopenic purpura (TTP) and hemo-
ytic uremic syndrome (HUS) are two microangiopathic dis-rders that are extremely rare during pregnancy/postpartum.hey are usually reported as case reports or small case se-
ies.1,26-35 Thus, their expected development during preg-
nntdpwolmvtTa
elp(imfTovsmt
msaHhwfHiv(arwfiaH
tntbA
ncdsai
upccysoee
c(tegecu
iIhhafipuotamlimn
MM
Fa
Imitators of severe pre-eclampsia 199
ancy or postpartum is probably �1 case in 100,000 preg-ancies. Because of that, they are even infrequent in referralertiary perinatal centers.26-35 The underlying pathologicalisturbance involves systemic or intrarenal aggregation oflatelets within the arterioles and capillaries in associationith endothelial cell injury. In patients with TTP, high levelsf endothelial membrane protein thrombomodulin as well asarge multimers of von Willebrand factor (VWF) are found in
aternal serum.36,37 These abnormal molecules cause micro-ascular platelet aggregates in various organs with resultanthrombocytopenia and mechanical injury to erythrocytes.his latter process results in microangiopathic hemolyticnemia.36-38
Most multimers of VWF in the plasma originate from thendothelial cells, but they also can be produced by plate-ets.36 A VWF-cleaving metalloprotease (ADAMTS13) inlasma normally prevents the entrance into the circulationor persistence) of unusually large multimers.36 This enzymes produced mainly by hepatocytes, and it degrades these
ultimers by cleavage to peptide bonds directly on the sur-ace of endothelial cells.36 In most patients with acquiredTP, plasma ADAMTS13 activity is markedly reduced (�5%f normal).39 This reduction of activity of ADAMTS13 pre-ents timely cleavage of large multimers of VWF as they areecreted by endothelial cells. Consequently, the uncleavedultimers induce adhesion and aggregation of platelets in
he microcirculation.36-39
Unlike the findings in TTP, the levels of ultralarge VWFultimers are generally not elevated in patients with HELLP
yndrome.40,41 However, one study found that the amount ofctive VWF was significantly increased in patients withELLP syndrome compared with the amount measured inealthy pregnant women and in those with pre-eclampsiaithout HELLP syndrome.42 In the same study, the authors
ound that ADAMTS 13 activity was lower in patients withELLP syndrome (74 � 21%) as compared with the values
n patients with normal pregnancies (10.5 � 15%), but thealues in HELLP syndrome were within the normal range61-142%).42 In addition, two other studies found that thectivity of ADAMTS 13 was reduced, but within normalange, and inactivating autoantibodies against ADAMTS 13ere absent in patients with HELLP syndrome.41,43 Thesendings suggest that measurements of ADAMTS 13 activitynd/or of inactivity autoantibodies can distinguish betweenELLP syndrome and TTP.40-43
The classic clinical pentad of TTP consists of thrombocy-openia, microangiopathic hemolytic anemia, neurologic ab-ormalities, fever, and renal dysfunction. The complete pen-ad is rarely seen in patients with documented cases of TTP39,ut 50-75% will have the first three clinical findings.27-39
nemia and thrombocytopenia are frequently severe.36-39
The presenting symptoms may include abdominal pain,ausea, vomiting, gastrointestinal bleeding, epistaxis, pete-hiae, or purpura.37-39 Neurologic abnormalities are oftenifficult to diagnose and may include transient and recurrentymptoms, such as headache, visual changes, confusion,phasia, transient paresis, weakness, and seizures.28-39 Fever
s present in about 30-40% of cases, and when present, it is nsually �101°F. Renal involvement manifests as hematuria,roteinuria, and renal insufficiency. The urine is usually tea-olored, similar to that in patients with HELLP syndrome. Inontrast, the urine color in AFLP patients is usually brightellow (Fig. 2). Hypertension may be present or absent. Inevere cases, the pathological lesion of TTP may involve otherrgans, such as liver, pancreas, heart, and lungs.37,38 Thextent of involvement of different systems will lead to differ-nt and specific clinical manifestations.
Laboratory findings will reveal thrombocytopenia (plateletount �100,000/mm3, usually �20,000), severe anemiahematocrit �25%), marked elevation in serum levels of lac-ate dehydrogenase (LDH), and the presence of fragmentedrythrocytes (schistocytes, helmet cells).36-39 It has been sug-ested that elevated LDH levels are largely derived from isch-mic or necrotic tissue cells as well as ruptured red bloodells.36 Liver enzymes may be normal or elevated, and coag-lation studies are frequently normal.29-39
HUS is mostly seen in children in association with entericnfections with Escherichia coli that produce Shiga toxin.36,37
t is extremely rare during pregnancy, and almost all casesave been described in the postpartum period (within 48ours to 10 weeks).1,29,44-48 The microvascular injury mainlyffects the kidneys and results from glomerular and arteriolarbrin thrombi. Patients with HUS present with edema, hy-ertension, bleeding manifestations, or severe renal fail-re.1,26,29,30,44-48 Renal involvement is more severe than inther thrombotic microangiopathies.36-38 Microscopic hema-uria and proteinuria are always present. Acute renal failure isn important feature in the clinical course of the disease, andost patients with HUS in pregnancy or postpartum will be
eft with some form of residual renal deficit. Laboratory find-ngs are similar to those found in TTP, but they are of less
agnitude. However, renal function is always markedly ab-ormal.1,29,30,44-48
aternal Outcomes in TTP-HUSaternal mortality and morbidity are usually high in preg-
igure 2 Urine of a patient with AFLP. (Color version of figure isvailable online.)
ancies complicated by TTP or HUS. Maternal mortality rates

wpyaavhiepth
lhccampidp
PIecamuvp
MPwstpanhttPssttte
Aptbbrfusc
TP
DDHAEASPPD
T
HEEDCVDSST
*†
200 B.M. Sibai
ere as high as 60% before the use of plasma infusions andlasma exchange. In the cases reviewed by Weiner for theears 1966-1987, the maternal mortality for TTP was 44%,nd for HUS it was 55%.48 However, recent case series reportmaternal mortality rate of 0-10%.31-34 This improved sur-
ival in recent studies is attributable to early detection (prioristory of TTP or HUS), inclusion of minor forms of TTP,
nclusion of women with probable HELLP syndrome orclampsia, and to improved therapeutic measures, such aslasma infusion, plasma exchange, or immune suppressiveherapy.26,33,34 However, maternal morbidities continue to beigh (Table 2).27-35
In general, maternal outcome is usually favorable with veryow maternal mortality and morbidities in those known toave TTP/HUS before pregnancy, because these patients re-eive close observation with serial plasmapheresis or ex-hange as needed.1,26-29,33,34 In contrast, maternal mortalitynd morbidities are usually high in those who develop theanifestations for the first time during pregnancy and/orostpartum.1,26,29,35 In such cases, there is a delay in confirm-
ng the diagnosis because of confusion with HELLP syn-rome and other medical conditions. As a result, plasma-heresis is usually initiated late in the disease process.26,35
able 2 Maternal Complications in Recent Series of 150regnancies with AFLP
Complication %
eath 0-20IC 50-100ypoglycemia 50-100TN 50-100ncephalopathy 20-67scites 30-50epsis 30-50ulmonary edema/ARDS 15-30ancreatitis 0-40iabetes insipidus ?
able 3 Maternal/Perinatal Outcome in TTP/HUS
AuthorsNo. ofWomen
No. ofPregnancies Death
ayward, et al.27 9 9 1zra, et al.28† 5 8 1german, et al.29 11 11 2ashe, et al.30 11 13 3astella, et al.31* 9 9 1esely, et al.32† 5 7 0ulcoy-Bouthars34 5 6 0hamseddine33 4 4 1tella, et al.35 12 14 3otal 71 81 12/71 (17%
CNS, central nervous system.
Only definite cases developing during pregnancy are included.erinatal Outcome in TTP-HUSn the review by Weiner,48 the fetal loss rate was 80%. How-ver, recent case series reported a fetal loss rate of 20%. Mostases of TTP develop antepartum with average gestational aget diagnosis of 26 weeks. Therefore, preterm delivery is com-on. These pregnancies are also associated with reducedteroplacental blood flow secondary to maternal hypoxia orascular lesions in the placenta.43,49 Perinatal outcome re-orted in recent series is summarized in Table 3.27-35
anagement of TTP/HUSatients with TTP/HUS should be managed in consultationith a hematologist and/or a nephrologist. Plasma transfu-
ions and exchanges have revolutionized the treatment ofhese syndromes. Fresh frozen plasma (platelet-poor), cryo-recipitate-poor plasma (cryosupernatant), and plasma tre-ted with a mixture of solvent and detergent all contain theeeded deficient metalloprotease.41-43 Plasma exchange willelp remove unusually large multimers of VWF and autoan-ibodies against the metalloprotease (ADAMTS13).41-43 Thisherapy is usually effective in approximately 90% of cases.lasma infusion alone has a response rate of 64%. Treatmenthould be initiated soon after the diagnosis is made. A re-ponse manifested by an increase in platelet count and reduc-ion in LDH levels is expected within a few days of initiatingherapy. Plasma exchanges should be performed daily untilhe platelet count becomes normal and hemolysis resolves, asvident by decrease in LDH levels.42,43
Some patients with TTP and high antibody titers againstDAMTS may not respond to plasma exchange alone. Theseatients require immunosuppressive therapy and/or splenec-omy.37,41,42 Platelet transfusions should be avoided if possi-le, given the potential for increased microvascular throm-osis. Because severe hemorrhage can occur with TTP, it iseasonable to transfuse platelets when there is the potentialor life-threatening bleeding.37 Red cell transfusion should besed according to clinical need.38,39 Furthermore, immuno-uppressive agents with steroids, cyclophosphamide, vin-ristine, or rituximab may be needed in patients who
ternal OutcomesPerinatal OutcomesNS*
njuryRenalInjury Death Preterm
2 2 1 4/90 0 4 4/81 4 2 5/110 5 1 3/130 0 2 4/90 1 3 4/70 0 1 2/50 0 3/5 4/50 1 4/16 —
(3%) 13 (18%) 21/73 (29%) 30/67 (45%)
Ma
CI
) 3

ds
tp
dirtcmrbiao
CWorteTsr
SSocpoatblsautmhs
filcfldtptTw
ipeibtHtsltess
�amoiifit
MPwdcanitirrfvroeaMc
MMtiossrml
Imitators of severe pre-eclampsia 201
evelop exacerbations or relapse after plasma exchange istopped.37,41,42
The treatment of HUS is similar to that of TTP. However,he response to plasma infusions is not as favorable, and mostatients will require dialysis.Delivery is the only cure for patients with HELLP syn-
rome or AFLP. In contrast, pregnancy should be continuedn patients with TTP or HUS who develop the conditionemote from term in the absence of fetal compromise and inhose who respond to plasma infusions and/or plasma ex-hange. In rare cases, plasmapheresis results in improve-ents in fetal heart rate tracing.50 However, theses patients
equire close observation of laboratory and clinical findingsecause of the risk of relapse. Some of the managements used
n such patients have included corticosteroids, antiplateletgents, weekly plasma infusions, and serial plasma exchanger dialysis.1,26,33-35
ounseling of Women with TTPomen who develop TTP during pregnancy should be aware
f the potential of relapse after delivery as well as of risk ofelapse in subsequent pregnancies.28,30,32,34,35,38 Therefore,hese women should be instructed about the symptoms ofarly relapse and to report these symptoms immediately.here are few case reports describing recurrent TTP/HUS inubsequent pregnancies28,32,34,35,38; however, the risk of thisecurrence remains unknown because of limited data.
ystemic Lupus Erythematosusystemic lupus erythematosus (SLE) is an autoimmune dis-rder that is characterized by deposits of antigen–antibodyomplexes in capillaries and various visceral structures. Mostatients are female and of reproductive age (26-40 yearsld).51 The clinical findings may be mild or severe amd mayffect multiple organ systems, including the kidneys (nephri-is), lungs (pleuritis or pneumonitis), liver (hepatitis), andrain.51-59 In patients with lupus nephritis, the clinical and
aboratory findings are similar to those of severe pre-eclamp-ia.51-57 Such patients will have hypertension, proteinuria,nd microscopic hematuria. In some of these women, partic-larly during an acute exacerbation, patients will havehrombocytopenia. The thrombocytopenia is usually mild tooderate (�50,000/mm3).51-59 Most patients with lupusave skin lesions (typical discoid or malar rash), and jointymptoms and fever are very common during an acute flare.
During the active phase of SLE exacerbation, laboratoryndings will show pancytopenia, thrombocytopenia, hemo-
ytic anemia, and an increase in anti-DNA antibodies. Serumomplement levels may be normal or depressed. Severe lupusares occur in 25-30%, and it may develop for the first timeuring pregnancy or in the postpartum period.51,55 In pa-ients with lupus nephritis who develop active flare duringregnancy, the clinical and laboratory findings are similar tohose with severe pre-eclampsia and HELLP syndrome.53-56,58
he exact diagnosis may be difficult, particularly in those
ith associated antiphospholipid antibodies (APAs).58-63 aAPAs (lupus anticoagulant and/or anticardiolipin antibod-es) are present in 30-40% of patients with systemic lu-us.59-61 These patients are at increased risk for thromboticvents. Patients with lupus and APA are at risk for tissueschemia secondary to thromboembolic events and throm-otic microangiopathy, resulting in a clinical picture similaro that seen in HELLP syndrome, eclampsia, TTP, andUS.61-67 Thrombocytopenia is seen in about 40-50% of
hese cases and hemolytic anemia in 14-23%.61 Cerebral le-ions and symptoms will develop because of cerebral vascu-itis and/or cerebral vaso-occlusive disease. In such patients,he clinical and laboratory findings are similar to those withclampsia.61 In patients with renal involvement, hyperten-ion and proteinuria are the rule with findings identical toevere pre-eclampsia.
The catastrophic antiphospholipid syndrome occurs in1% of patients with APA syndrome.60 It is characterized by
cute thrombotic microangiopathy affecting small vessels ofultiple organs (at least three). The most common affected
rgans are the kidneys and central nervous system.60,61 Livernvolvement will result in cellular necrosis and infarcts, lead-ng to elevated liver enzymes.64-66 The clinical and laboratoryndings may also be similar to other microvascular angiopa-hies.60-67
aternal–Perinatal Outcomeregnancy outcome is usually favorable in patients with SLEho were in remission before pregnancy and who do notevelop a flare during pregnancy.51,57 In addition, the out-ome is favorable in those without lupus nephritis and/orbsent antiphospholipid antibodies.52,55-57 However, mater-al morbidities and perinatal mortality and morbidity are
ncreased in those with lupus nephritis central nervous sys-em disease and in those with antiphospholipid antibod-es.51-55,59-62 These latter pregnancies are associated with highates of miscarriage, fetal death (4-19%), intrauterine growthestriction, and preterm delivery (38-54%). This high rate ofetal loss and perinatal complications is related to decidualascular thrombosis and placental infarctions and hemor-hage.59-62 Maternal complications include a high rate of earlynset pre-eclampsia and complications related to thrombo-mbolism and microangiopathy.57-61 Maternal morbiditiesre substantially increased in those with APA syndrome.58-67
aternal mortality is almost 50% in patients who develop theatastrophic APA syndrome.61
anagementanagement of SLE flare during pregnancy will depend on
he presence of the organ systems involved, laboratory find-ngs (thrombocytopenia, APAs), and the presence or absencef nephritis. Treatment usually includes the use of cortico-teroids, low-dose aspirin, hydroxychloroquine immuno-uppressive drugs, and heparin.51-68 The usual dose of ste-oids is 40-80 mg/day of prednisone, and for aspirin it is 81g/day. Prednisone therapy is usually used in patients with
upus nephritis, whereas combined regimens of prednisone
nd low-dose aspirin are recommended in patients with
Ahtmdtqpfp
aot(dopt
SDp
neaptsfissmutupiss(ip
tau
T
HPFJNAC
*†‡ syndro
T
THADHVAILEEE
*
†
202 B.M. Sibai
PAs.59-61,68 Alternative regimens have included the use ofeparin plus low-dose aspirin. For patients with severehrombocytopenia that does not respond to the above regi-ens, intravenous � globulin may be beneficial.61 Recentata also suggested that the use of other agents, such as aza-hioprine, cyclosporin, and hydroxychloroquine, may be re-uired in management of some of these patients.54,59,68 Inatients with catastrophic APA syndrome, treatment includesull anticoagulation with heparin, steroids, plus plasma-heresis.60,61,66
In summary, the clinical presentations of AFLP, TTP, HUS,nd exacerbation of SLE can be easily confused with thosef severe pre-eclampsia–eclampsia HELLP syndrome. Al-hough these conditions share a range of signs and symptomsTable 4) and laboratory tests (Table 5) with HELLP syn-rome, each has some distinguishing clinical findings or lab-ratory results. Making the right diagnosis is extremely im-ortant regarding decisions about need for delivery as well asreatment and complications.
ystemic Viral Sepsisisseminated herpes simplex is a rare complication duringregnancy. It is usually seen in immunocompromised preg-
able 4 Frequency of Various Signs and Symptoms Among Im
Signs and SymptomsHELLP
Syndrome AFLP
ypertension 85% 50%roteinuria 90-95% 30-50%ever Absent 25-32%aundice 5-10% 40-90%ausea/vomiting 40% 50-80%bdominal pain 60-80% 35-50%entral nervous system 40-60% 30-40%
?, values not reported.Common, reported as the most common presentation.APA, antiphospholipid antibodies � catastrophic antiphospholipid
able 5 Frequency and Severity of Laboratory Findings Amon
Laboratory FindingsHELLP
Syndrome AF
hrombocytopenia (<100,000/mm3) >20,000 >50emolysis 50-100% 15-2nemia <50% AbsIC <20% 7ypoglycemia Absent 6W factor multimers Absent AbsDAMTS 13% < 5% Absent Abs
mpaired renal function 50% 90-1DH (IU/L) >600 Varlevated ammonia Rare 5levated bilirubin 50-60% 10levated transaminases 100% 10
Abbreviations: APA, antiphospholipid antibodies; DIC, Disseminaterythematosus; LDH, lactic dehydrogenase.
Levels < 100 IU/L.
ant women. The onset is usually in the third trimester (av-rage onset of 30 weeks) with clinical presentation of fever,bdominal pain, and upper respiratory symptoms.69-72 Someatients will have hepatitis without jaundice and encephali-is.69,71,72 Hepatitis is a common finding in fulminant sep-is.70,72 Hypertension and proteinuria are absent. Laboratoryndings will reveal leukopenia, thrombocytopenia, hemoly-is, DIC, markedly elevated levels of AST (�2000 IU/L), andevere elevations in LDH levels. In fulminant cases, the am-onia levels may be elevated; however, bilirubin values aresually normal or slightly elevated, which is different fromhe usual finding in patients with AFLP. The diagnosis issually made in the presence of vesicular lesions in the skin,erineum, or the cervix. Liver biopsy will show the typical
ntranuclear inclusions (Cowdry type A inclusions) with as-ociation with cell necrosis and hemorrhage (Fig. 2). The CTcan may show the typical mottled appearance in the livermultiple low-density areas that do not enhance with contrastnjection), which is different from the CT scan findings inatients with HELLP syndrome, AFLP, or liver infarction.1
Disseminated herpes infection is associated with high ma-ernal and perinatal mortality if not treated promptly.69-72 Inreview of 24 cases of herpes simplex hepatitis in pregnancyp to the year 1998, Kanga and Graves70 found an overall
s of Pre-eclampsia–Eclampsia
TTP HUS Exacerbation of SLE
20-75% 80-90% 80% w/APA/nephritisith hematuria 80-90% 100% w/nephritis
20-50% ?* Common during flareare Rare Absentommon† Common Only w/APA‡ommon Common Only w/APA
60-70% ? 50% w/APA
me.
ators of Pre-eclampsia–Eclampsia
TTP HUSExacerbation of
SLE
<20,000 >20,000 >20,000100% 100% 14-23% w/APA*100% 100% 14-23% w/APA
Rare Rare RareAbsent Absent Absent
80-90% 80% <10%33-100% Rare Rare
30% 100% 40-80%>1000 >1000 with APA
Absent Absent Absent100% <10%
Usually mild† Usually mild† with APA
vascular coagulopathy; VW, von Willebrand; SLE, systemic lupus
itator
w
RCC
g Imit
LP
,0000%ent3%1%entent00%
iable0%0%0%
ed intra

mMawttbatihsn
SISSgpbsmtoacsbmonb
piiaisesro
hH1csdbp
It
pnstatttetloao
MOManw3ath(wepw
MTima
itotcoau(cbptoitet
Imitators of severe pre-eclampsia 203
aternal mortality of 39% and perinatal mortality of 39%.aternal mortality was 0% among 13 women treated with
cyclovir and 20% among 4 women treated with vidarabine,hereas it was 67% among 15 women receiving no antiviral
herapy.70 In addition, the perinatal mortality was 18% inhose receiving acyclovir, 67% among those receiving vidara-ine, and 44% among those receiving no therapy. Therefore,ccurate and urgent diagnosis is important because earlyherapy with acyclovir improves survival. The usual dose ofntravenous acyclovir is 10-15 mg/kg of body weight every 8ours to be continued for at least 10 days.69-72 These patientshould be managed in an intensive care facility. There is noeed for early delivery in the absence of fetal indications.70
ystemicnflammatory Responseyndrome (SIRS)/Septic Shock
IRS describes a systemic inflammatory process that can beenerated by infection or by noninfectious causes, such asancreatitis, burns, and major trauma.73-78 It is characterizedy a hyperdynamic state, endothelial cell injury, leukocyto-is, neutrophil activation, and tissue hypoperfusion withultiorgan dysfunction.71,73-78 Sepsis is SIRS due to infection
hat is associated with hypoperfusion or hypotension withrgan dysfunction. Septic shock is a subset of sepsis defineds sepsis-induced hypotension despite adequate fluid resus-itation along with the presence of perfusion abnormalities,uch as lactic acidosis, renal dysfunction (oliguria, acute tu-ular necrosis), hepatic dysfunction, and acute changes inental status.73-78 Laboratory findings include leukocytosis
r leukopenia (white blood count �4000), thrombocytope-ia, hemolysis, DIC, elevated liver enzymes, and elevatedilirubin.Some authors suggested that the maternal syndrome of
re-eclampsia share many of the clinical and laboratory find-ngs of patients with SIRS.79,80 Both syndromes are character-zed by systemic inflammation, neutrophilia, and neutrophilctivation. Indeed, many of the clinical and laboratory find-ngs of women with HELLP syndrome, such as hemoly-is, hepatocellular necrosis, renal dysfunction, pulmonarydema, ARDS, and thrombocytopenia, are similar to thoseeen in patients with severe sepsis and septic shock.79,80 Aecent report by Afessa and coworkers74 found that 59% ofbstetric patients admitted to ICU developed SIRS.In general, patients with severe sepsis or septic shock will
ave fever, but hypertension and proteinuria are absent.owever, hypertension or proteinuria may be absent in 10-5% of patients with HELLP syndrome. In addition, leuko-ytosis and fever may be present in women with pre-eclamp-ia because of endomyometritis, particularly after cesareanelivery. Table 1 compares clinical and laboratory findingsetween those with disseminated herpes and SIRS/sepsis inregnancy.Septic shock is rare during pregnancy or postpartum.73-76
t should be considered in the differential diagnosis of pa-
ients with fever, microangiopathic hemolysis, thrombocyto- aenia, renal insufficiency, altered mental status, and pulmo-ary insufficiency. The clinical picture can mimic HELLPyndrome, AFLP, TTP and HUS, and an SLE flare. It can behe primary cause or it can be a complication of any one of thebove syndromes. The clinical findings include a tempera-ure �38°C or �36°C, tachycardia (pulse �100 bpm),achypnea (respiratory rate �24/min), and hypotension (sys-olic blood pressure �90 mm Hg). Cardiac output is initiallylevated, systemic vascular resistance is low, and venous re-urn is reduced. With reduced tissue perfusion, oxygen de-ivery is impaired, resulting in increased lactate levels sec-ndary to anerobic cellular metabolism. Both hypotensionnd poor tissue perfusion will ultimately lead to multiplergan failure.73-78
aternal and Perinatalutcome in Septic Shockabie and coworkers73 reported the etiology, management,
nd outcome in 18 patients with septic shock during preg-ancy. The etiology of shock were pyelonephritis in 6omen, chorioamnionitis in 3, postpartum endometritis in, toxic shock syndrome in 2, and 1 each of septic abortion,ppendicitis, ovarian abscess, necrotizing fasciitis, and bac-erial endocarditis. Five women (28%) died, and 15 (82%)ad multiorgan dysfunction. The perinatal survival was 50%10 of 20, one set of triplets). Five of the 10 losses were �20eeks’ gestation, and 5 were stillbirths.73 Afessa and cowork-
rs74 reported on 44 obstetric patients who developed SIRS; 2atients had septic shock and 18 had severe sepsis. Twoomen (4.5%) died, and 36 (82%) had multiorgan failure.
anagement of Septic Shockreatment of septic shock consists of resuscitation with flu-
ds, vasopressors, antibiotics, hemodynamic monitoring, re-oval of source of infection (surgery or percutaneous drain-
ge of abscesses), and modifying of inflammatory mediators.Patients with SIRS or septic shock require admission to an
ntensive care unit to monitor volume replacement with crys-alloids or blood components, to monitor vital signs, urineutput, oxygenation, and mental status.73-78 Fluid resuscita-ion will include 3-4 L of crystalloid over 60 minutes, toorrect hypotension and to achieve a central venous pressuref 8-12 mm Hg. If hypotension persists, then vasoactivegents are used. The first drug of choice is dopamine, titratedp to 20 mg/kg/min to achieve a MAP of at least 65 mm HgMAP needed to keep adequate tissue perfusion, particularlyerebral perfusion).73-78 Other vasoactive drugs, such as do-utamine or norepinephrine, can be used as needed. If theatient does not show good response to broad spectrum an-ibiotic therapy, attention should be given to identify a sourcef infection (retained products of conception, microabscessesn uterine wall, pelvic abscess, etc.) that require surgical in-ervention.71,73-76 In general, delivery is required if there isvidence of an infected fetus, amniotic fluid, or placentalissues. On the other hand, delivery is not indicated in the
bsence of infection in the uterine cavity. A detailed descrip-
td
CSidtcdCafeoafm
BP
R
1
1
1
1
1
1
1
1
1
1
2
2
2
2
2
2
2
2
2
2
3
3
3
3
3
3
204 B.M. Sibai
ion of pathophysiology and management of sepsis has beenescribed.76-80
onclusionseveral microangiopathic disorders can occur any time dur-ng pregnancy or during the postpartum period. The inci-ence of these disorders is extremely low; however, the ma-ernal and perinatal complications are extremely high. Thelinical presentation and laboratory findings in these disor-ers can mimic those seen in pre-eclampsia and eclampsia.onsequently, there is the potential for delay in diagnosisnd treatment during management of these women. There-ore, it is important that managing physicians be aware of thetiology, diagnostic findings, and management of such dis-rders. Finally, a rapid diagnosis and close consultation withn interdisciplinary team of physicians, such as maternal–etal medicine, nephrologist, hematologist, critical care, etc.,
ay result in optimal outcome for the mother and fetus.12
ox I Imitators of Severere-eclampsia/Hellp Syndrome● AFLP● TTP● HUS● Exacerbation of lupus erythematosus● Catastrophic antiphospholipid syndrome● Systemic viral sepsis (disseminated herpes)● SIRS/septic shock● Other conditions (cholestasis of pregnancy, necrotizing
pancreatitis, etc.)
eferences1. Sibai BM: Imitators of severe preeclampsia. Obstet Gynecol 109:956-
966, 20072. Usta IM, Barton JR, Amon EA, et al: Acute fatty liver of pregnancy: An
experience in the diagnosis and management of fourteen cases. Am JObstet Gynecol 171:1342-1347, 1994
3. Castro MA, Fassett MJ, Reynolds TB, et al: Reversible peripartum liverfailure: A new perspective on the diagnosis, treatment, and cause ofacute fatty liver of pregnancy based on 28 consecutive cases. Am JObstet Gynecol 181:389-395, 1999
4. Reyes H: Acute fatty liver of pregnancy. Clin Liver Dis 3:69-81, 19995. Pereira S, O’Donohue J, Wendon J, Williams R: Maternal and perinatal
outcome in severe pregnancy related liver disease. J Hepatol 26:1258-1262, 1997
6. Vigil-DeGracia P, Lavergue JA: Acute fatty liver of pregnancy. Int JGynecol Obstet 72:193-195, 2001
7. Davidson KM, Simpson LL, Knox TA, et al: Acute fatty liver in tripletgestation. Obstet Gynecol 91:806-808, 1998
8. Moldenhauer JS, O’Brien JM, Barton JR, et al: Acute fatty liver of preg-nancy associated with pancreatitis: A life-threatening complication.Am J Obstet Gynecol 190:502-506, 2004
9. Fesenmeier MF, Coppage KH, Lambers DS, et al: Acute fatty liver ofpregnancy in 3 tertiary care centers. Am J Obstet Gynecol 192:1416-1419, 2005
0. Castro MA, Goodwin TM, Shaw KJ, et al: Disseminated intravascularcoagulation and antithrombin III depression in acute fatty liver of preg-nancy. Am J Obstet Gynecol 174:211-216, 1996
1. Knight M, Nelson-Piercy C, Kurinczuk JJ: And on behalf of UK obstet-
ric surveillance system (UKOSS). A prospective national study of acutefatty liver of pregnancy in the UK. Gut 57:951-956, 2008
2. Suzuki S, Watanalie S, Araki T: Acute fatty liver of pregnancy at 23weeks of gestation. Br J Obstet Gynaecol 108:223-224, 2001
3. de Nagy J, Strittmatter CA, Lee RV: Acute fatty liver of pregnancypresenting as hepatic encephalopathy at 28 weeks’ gestation. J ObstetGynaecol 28:100-102, 2008
4. Martin JN Jr, Briery CM, Rose CH, et al: Postpartum plasma exchangesadjunctive therapy for severe acute fatty liver of pregnancy. J ClinApher 23:138-143, 2008
5. Sibai BM: Diagnosis, controversies, and management of HELLP syn-drome. Obstet Gynecol 103:981-991, 2004
6. Mabie W, Dacus J, Sibai BM, et al: Computed tomography in acute fattyliver of pregnancy. Am J Obstet Gynecol 158:142-145, 1988
7. Van Le L, Podrasky A: Computed tomographic and ultrasonographicfindings in women with acute fatty liver of pregnancy. J Reprod Med35:815-817, 1990
8. Farine D, Newhouse J, Owen J, et al: Magnetic resonance imaging andcomputed tomography scan for the diagnosis of acute fatty liver ofpregnancy. Am J Perinatol 7:316-318, 1990
9. Clements D, Young W, Thornton J, et al: Imaging in acute fatty liver ofpregnancy. Br J Obstet Gynaecol 97:631-633, 1990
0. Castro M, Ouzounian JG, Colletti PM, et al: Radiologic studies in acutefatty liver of pregnancy. A review of the literature and 19 new cases. JReprod Med 41:839-843, 1996
1. Knox TA, Olans LB: Liver disease in pregnancy. Review article. N EnglJ Med 335:569-576, 1996
2. Zang Z, Yamada J, Zhao Y, et al: Prospective screening for pediatricmitochondrial trifunctional protein defects in pregnancies complicatedby liver disease. JAMA 288:2163-2166, 2002
3. Rajasri AG, Sretha R, Mitchell J: Acute fatty liver of pregnancy (AFLP):An overview. J Obstet Gynaecol 27:237-240, 2007
4. Tyni T, Ekholm E, Pihko H: Pregnancy complications are frequent inlong-chain 3-hydroxyacyl-coenzyme A dehydrogenase deficiency.Am J Obstet Gynecol 178:603-608, 1998
5. Ibdah JA, Bennett MJ, Rinaldo P, et al: A fetal fatty-acid oxidationdisorder as a cause of liver disease in pregnant women. N Engl J Med340:1723-1731, 1999
6. Martin JN Jr, Bailey AP, Rehberg JF, et al: Thrombotic thrombocytope-nic purpura in 166 pregnancies, 1955-2006. Am J Obstet Gynecol199:98-104, 2008
7. Hayward CPM, Sutton DMC, Carter WH Jr, et al: Treatment outcomesin patients with adult thrombotic thrombocytopenic purpura/hemo-lytic uremic syndrome. Arch Intern Med 154:982-987, 1994
8. Ezra Y, Rose M, Elder A: Therapy and prevention of thrombotic throm-bocytopenic purpura during pregnancy: A clinical study of 16 preg-nancies. Am J Hematol 51:1-6, 1996
9. Egerman SS, Witlin AG, Friedman SA, et al: Thrombotic thrombocy-topenic purpura/hemolytic uremic syndrome in pregnancy: Review of11 cases. Am J Obstet Gynecol 175:950-956, 1996
0. Dashe JS, Ramin SM, Cunningham FG: The long-term consequences ofthrombotic microangiopathy (thrombotic thrombocytopenic purpuraand hemolytic uremic syndrome) in pregnancy. Obstet Gynecol 91:662-668, 1998
1. Castella M, Rujol M, Julia A, et al: Thrombotic thrombocytopenic pur-pura and pregnancy: A review of ten cases. Vox Sang 87:287-290, 2004
2. Vesely SK, Li X, McMinn JR, et al: Pregnancy outcomes after recoveryfrom thrombotic thrombocytopenic purpura-hemolytic uremic syn-drome. Transfusion 44:1149-1158, 2004
3. Shamseddine A, Chehal A, Usta I, et al: Thrombotic thrombocytopenicpurpura and pregnancy report of four cases and literature review. J ClinApher 19:5-10, 2004
4. Dulcoy-Bouthars AS, Caron C, Sulitil D, et al: Thrombotic thrombocy-topenic purpura: Medical and biological monitoring of six pregnancies.Eur J Obstet Gynecol Reprod Biol 111:146-152, 2003
5. Stella CA, Dacus J, Guzman E, et al: The diagnostic dilemma of throm-botic thrombocytopenic purpura/hemolytic uremic syndrome in theobstetric triage and emergency department. Lessons from 4 tertiary
hospitals. Am J Obstet Gynecol Epub: doi:10.1016/j.acog.2008.10.037
3
3
3
3
4
4
4
4
4
4
4
4
4
4
5
5
5
5
5
5
5
5
5
5
6
6
6
6
6
6
6
6
6
6
7
7
7
7
7
7
7
7
77
8
Imitators of severe pre-eclampsia 205
6. Moake JL: Thrombotic microangiopathies. N Engl J Med 347:589-600,2002
7. Allford SL, Hunt BJ, Rose P, et al: Guideline-guidelines on the diagnosisand management of the thrombotic microangiopathic haemolytic ane-mias. Br J Haematol 120:556-573, 2003
8. George JN: Thrombotic thrombocytopenic purpura. N Engl J Med354:1927-1935, 2006
9. George JN, Terrell DR, Swisher KK, et al: Lessons learned from theOklahoma thrombotic thrombocytopenic purpura-hemolytic uremicsyndrome registry. J Clin Apher 23:129-137, 2008
0. Thorp JM, White GD, Moake JL, et al: Willebrand factor multimericlevels and patterns in patients with severe preeclampsia. Obstet Gy-necol 75:163-167, 1990
1. Lattuada A, Rossi E, Calzarossa C, et al: Mild to moderate reduction ofa von Willebrand factor cleaving protease (ADAMTs-13) in pregnantwomen with HELLP microangiopathic syndrome. Haematologica 88:1029-1034, 2003
2. Hulstim JJJ, van Rumard Heimel PJ, Fraux A, et al: Acute activation ofthe endothelium results in increased levels of active von Willebrandfactor in hemolysis, elevated liver enzymes and low platelets (HELLP)syndrome. J Thromb Haemost 4:2569-2575, 2006
3. Bartz C, Brandenburg V, Rath W: Is von-Willebrand-cleaving protease(ADAMTs-13) useful in differentiating HELLP from TTP. HypertensPregnancy 23(Suppl 1): abstract no. 69, 2004
4. Hebisch G, Bernasconi MT, Ganuer J, et al: Pregnancy-associated re-current hemolytic uremic syndrome with fetal thrombotic vasculopa-thy in the placenta. Am J Obstet Gynecol 185:1265-1266, 2001
5. Pajor A, Hintalan A, Bakos L, et al: Postpartum hemolytic uremic syn-drome following placental abruption. Eur J Obstet Gynecol Reprod Biol49:201-204, 1993
6. Martinez-Roman S, Gratacos E, Torne A, et al: Successful pregnancy ina patient with hemolytic-uremic syndrome during the second trimesterof pregnancy. J Reprod Med 41:211-214, 1996
7. Rosen M, Brauer KI, Alperin JB, et al: Postpartum hemorrhagic shockresulting in thrombotic thrombocytopenic purpura-hemolytic uremicsyndrome. J Matern Fetal Neonatal Med 13:208-210, 2003
8. Weiner CP: Thrombotic microangiopathy in pregnancy and the post-partum period. Semin Hematol 24:119-129, 1987
9. Jamshed S, Kouides P, Sham R, et al: Pathology of thrombotic throm-bocytopenic purpura in the placenta, with emphasis on the “snowmansign.” Pediatr Dev Pathol 10:455-462, 2007
0. Strasser SM, Kwee A, Fijnheer R, et al: Transient severe fetal heart rateabnormalities in pregnancy complicated by thrombotic thrombocyto-penic purpura. Obstet Gynecol 111:517-521, 2008
1. Cortes-Hernandez J, Ordi-Ros J, Paredes F, et al: Clinical predictors offetal and maternal outcome in systemic lupus erythematosus: A pro-spective study of 103 pregnancies. Rheumatology 41:643-650, 2002
2. Clark CA, Spitzer KA, Nadler JN, et al: Preterm deliveries in womenwith systemic lupus erythematosus. J Rheumatol 30:2127-2132, 2003
3. Tandon A, Ibanez D, Gladman DD, et al: The effect of pregnancy onlupus nephritis. Arthritis Rheum 50:3941-3946, 2004
4. Clowse MEB, Magder L, Petri M: Cyclophosphamide for lupus duringpregnancy. Lupus 14:593-597, 2005
5. Chakravarty EF, Colon I, Langen ES, et al: Factors that predict prema-turity and preeclampsia in pregnancies that are complicated by sys-temic lupus erythematosus. Am J Obstet Gynecol 192:1897-1904,2005
6. Egerman RS, Ramsey RD, Kao LW, et al: Hypertensive disease in preg-nancies complicate by systemic lupus erythematosus. Am J Obstet Gy-
necol 193:1676-1679, 20057. Dahr JP, Essenmacher LM, Ager JW, et al: Pregnancy outcome beforeand after diagnosis of systemic lupus erythematosus. Am J Obstet Gy-necol 193:1444-1455, 2005
8. Hilbrand P, Eignmann C, Gugger M, et al: Pre-eclampsia with acuteheart failure postpartum as primary manifestation of systemic lupuserythematosus. Eur J Heart Fail 7:1057-1058, 2005
9. Ticani A, Bompane D, Danieli E, et al: Pregnancy, lupus and antiphos-pholipid syndrome (Hughes Syndrome). Lupus 15:15761160, 2006
0. Hanly JG: Antiphospholipid syndrome: An overview. CMAJ 168:1675-1682, 2003
1. Levine JS, Branch DW, Rauch D: The antiphospholipid syndrome.N Engl J Med 346:752-763, 2002
2. Kupferminc MJ, Lee MJ, Green D, et al: Severe postpartum pulmonary,cardiac, and renal syndrome associated with antiphospholipid antibod-ies. Obstet Gynecol 83:806-807, 1994
3. Kniaz D, Eisenberg GM, Ebrad H, et al: Postpartum hemolytic uremicsyndrome associated with antiphospholipid antibodies: A case reportand review of the literature. Am J Nephrol 12:126-133, 1992
4. Amant F, Spitz B, Arnout J, et al: Hepatic necrosis and hemorrhage inpregnant patients with antiphospholipid antibodies. Lupus 6:552-555,1997
5. Fehr T, Cathomas G, Weber C, et al: Foetal loss, liver necrosis and acutelupus erythematosus in a patient with antiphospholipid antibody syn-drome. Lupus 10:576-579, 2001
6. Roberts G, Gordon MM, Porter D, et al: Acute renal failure complicatingHELLP syndrome, SLE, and antiphospholipid syndrome: Successfuloutcome using plasma exchange therapy. Lupus 12:251-257, 2003
7. Sakhel K, Usta IM, Hannoun A, et al: Liver infarction in a woman withlupus nephritis and antiphospholipid syndrome. Scand J Rheumatol35:405-408, 2006
8. Lockshin MD, Erkan D: Treatment of antiphospholipid syndrome.N Engl J Med 349:1177-1179, 2003
9. Klein NA, Mabie WC, Shaver DC, et al: Herpes simplex virus hepatitisin pregnancy. Two patients successfully treated with acyclovir. Gastro-enterology 100:239-244, 1991
0. Kang AH, Graves CR: Herpes simplex hepatitis in pregnancy: A casereport and review of the literature. Obstet Gynecol 54:463-468, 1999
1. Maupin RT: Obstetric infectious disease emergencies. Clin Obstet Gy-necol 45:393-404, 2002
2. Allen RH, Tuomala RE: Herpes simplex virus hepatitis causing acuteliver dysfunction and thrombocytopenia in pregnancy. Obstet Gynecol106:1187-1189, 2005
3. Mabie WC, Barton JR, Sibai BM: Septic shock in pregnancy. ObstetGynecol 90:553-561, 1997
4. Afessa B, Green B, Delke I, et al: Systemic inflammatory response syn-drome, organ failure, and outcome in critically ill obstetric patientstreated in an ICU. Chest 120:1271-1277, 2001
5. KanKuri E, Kurki T, Carlson P, et al: Incidence, treatment and outcomeof peripartum sepsis. Acta Obstet Gynecol Scand 82:730-735, 2003
6. Fernandez-Perez ER, Salam S, Pendem S, et al: Sepsis during preg-nancy. Crit Care Med 33:S286-S293, 2005
7. Sheffield JS: Sepsis and septic shock in pregnancy. Crit Care Clin 20:651-660, 2004
8. Russell JA: Management of sepsis. N Engl J Med 355:1699-1713, 20069. Von Dadelszen P, Magee LA, Marshall JC, et al: The maternal syndrome
of preeclampsia: A forme fruste of the systemic inflammatory responsesyndrome. Sepsis 4:43-47, 2000
0. VonDadelszen P, Magee LA, Lee SK, et al: Activated protein C in normalhuman pregnancy and pregnancies complicated by severe preeclamp-
sia: A therapeutic opportunity? Crit Care Med 30:1883-1892, 2002