Embed Size (px)
Citation preview

Patogenesi e terapia della GBS
IL RUOLO DELLE IMMUNOGLOBULINE
NELLA PATOLOGIA NEUROLOGICA
MILANO6 MARZO 2015
SALA Pirelli
Raffaella Fazio
Ospedale San Raffaele
DEFINIZIONE
Guillain-Barrè syndrome is a acute Guillain-Barrè syndrome is a acute inflammatory disorder of the peripheral nervous system thought to be due to autoimmunity for which immunotherapyis usually prescribed ( R.Hughes)
DEFINIZIONE
Guillain-Barrè syndrome is a acuteGuillain-Barrè syndrome is a acuteinflammatory disorder of the peripheral nervous system thought to be due to autoimmunity for which immunotherapyis usually prescribed ( R.Hughes)
DEFINIZIONE
Guillain-Barrè syndrome is a acute Guillain-Barrè syndrome is a acute inflammatory disorder of the peripheral nervous system thought to be due to autoimmunity for which immunotherapyis usually prescribed ( R.Hughes)
DEFINIZIONE
Guillain-Barrè syndrome is a acute Guillain-Barrè syndrome is a acute inflammatory disorder of the peripheral nervous system thought to be due to autoimmunity for which immunotherapyis usually prescribed ( R.Hughes)
1916- primi criteri diagnostici della
poliradicolonevrite acuta
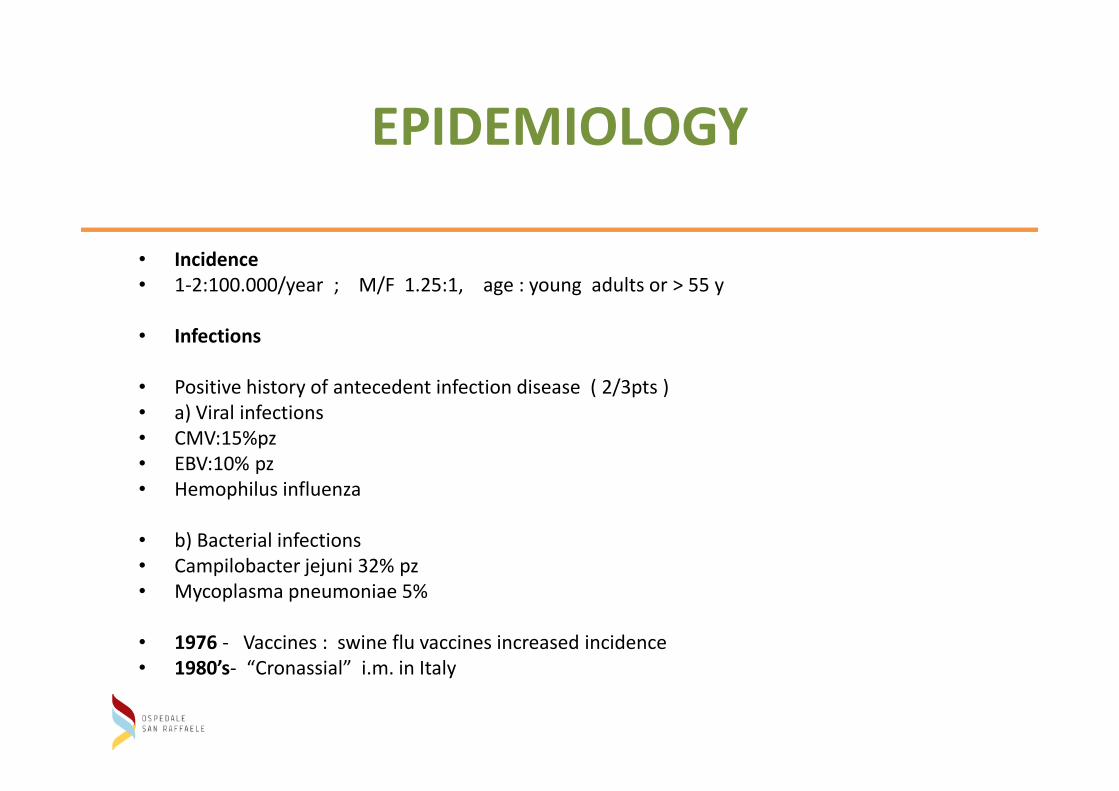
EPIDEMIOLOGY
• Incidence
• 1-2:100.000/year ; M/F 1.25:1, age : young adults or > 55 y
• Infections
• Positive history of antecedent infection disease ( 2/3pts )• Positive history of antecedent infection disease ( 2/3pts )
• a) Viral infections
• CMV:15%pz
• EBV:10% pz
• Hemophilus influenza
• b) Bacterial infections
• Campilobacter jejuni 32% pz
• Mycoplasma pneumoniae 5%
• 1976 - Vaccines : swine flu vaccines increased incidence
• 1980’s- “Cronassial” i.m. in Italy
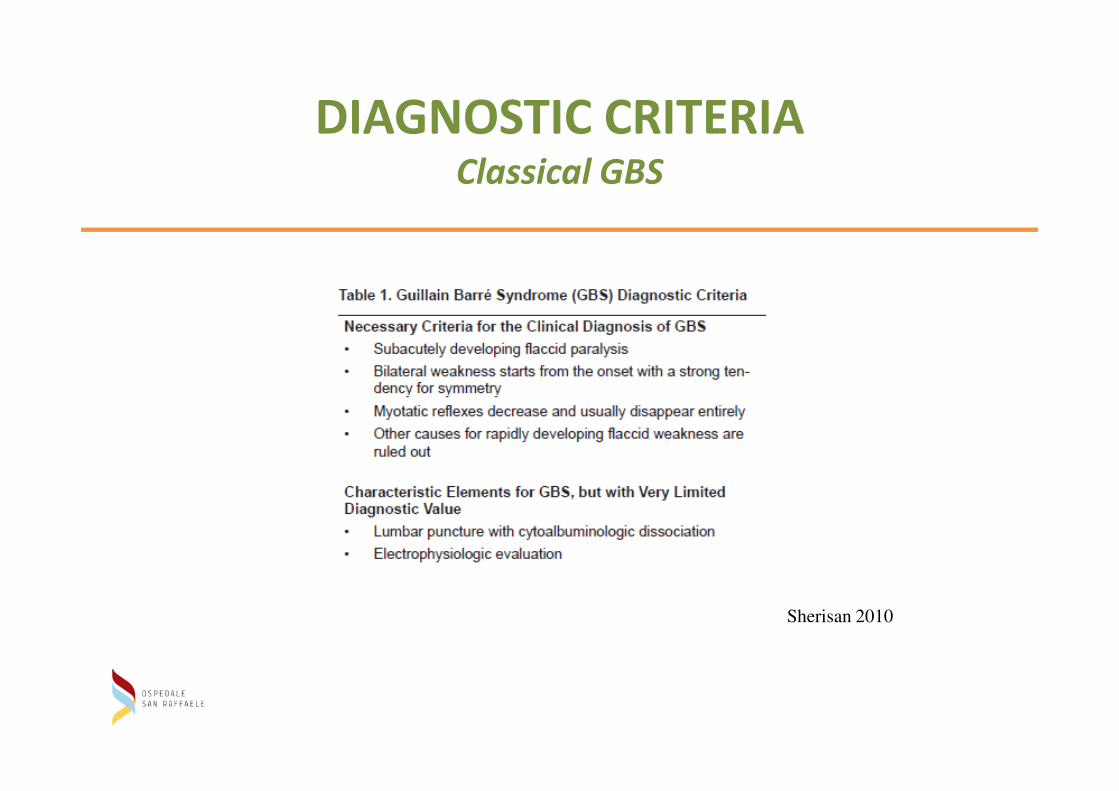
DIAGNOSTIC CRITERIAClassical GBS
Sherisan 2010
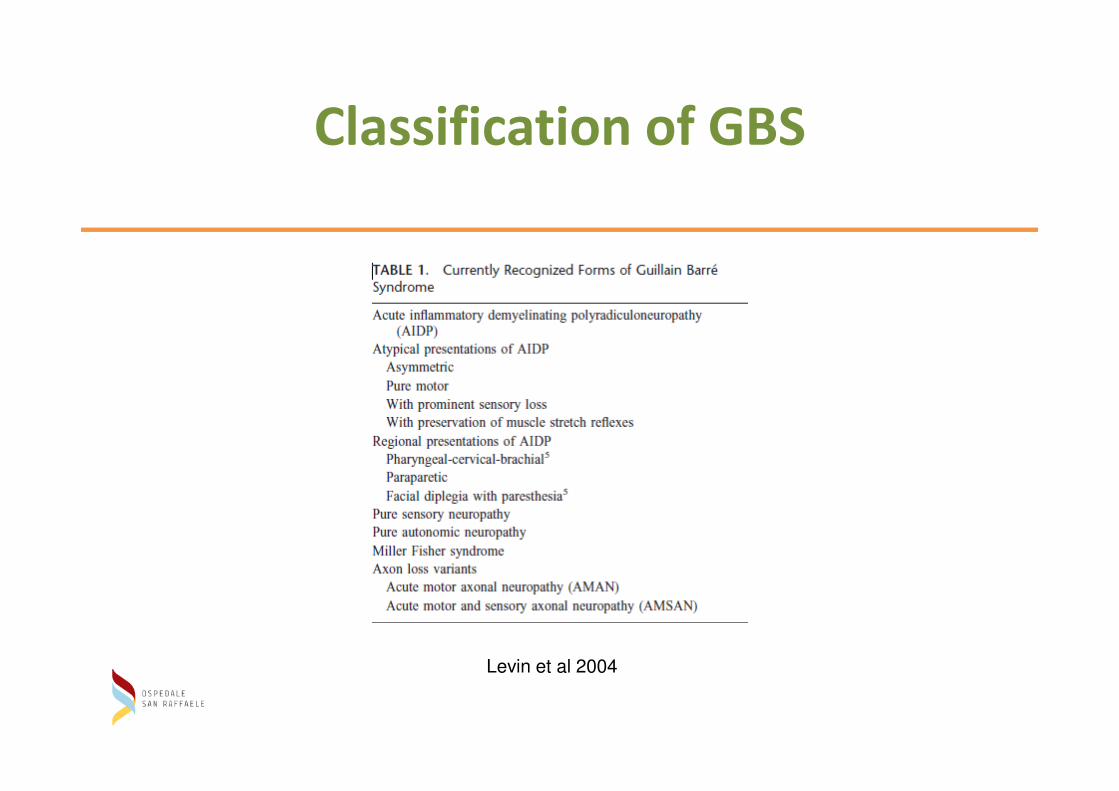
Classification of GBS
Levin et al 2004
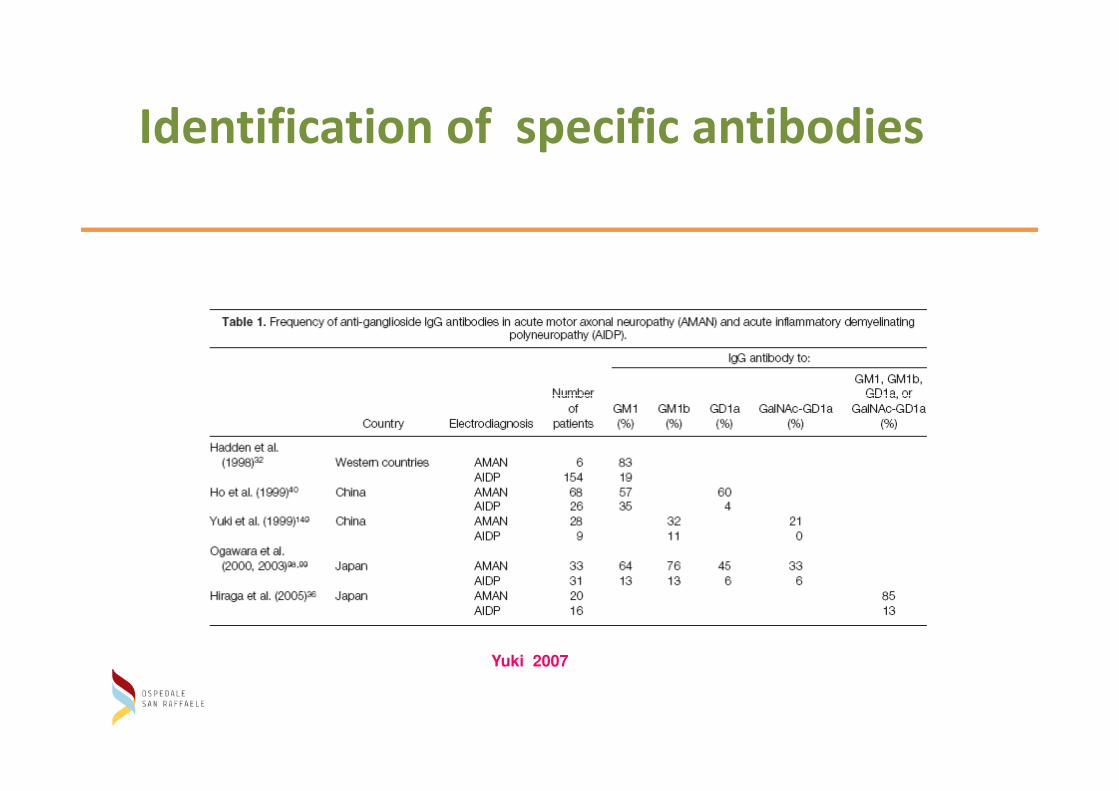
Identification of specific antibodies
Yuki 2007
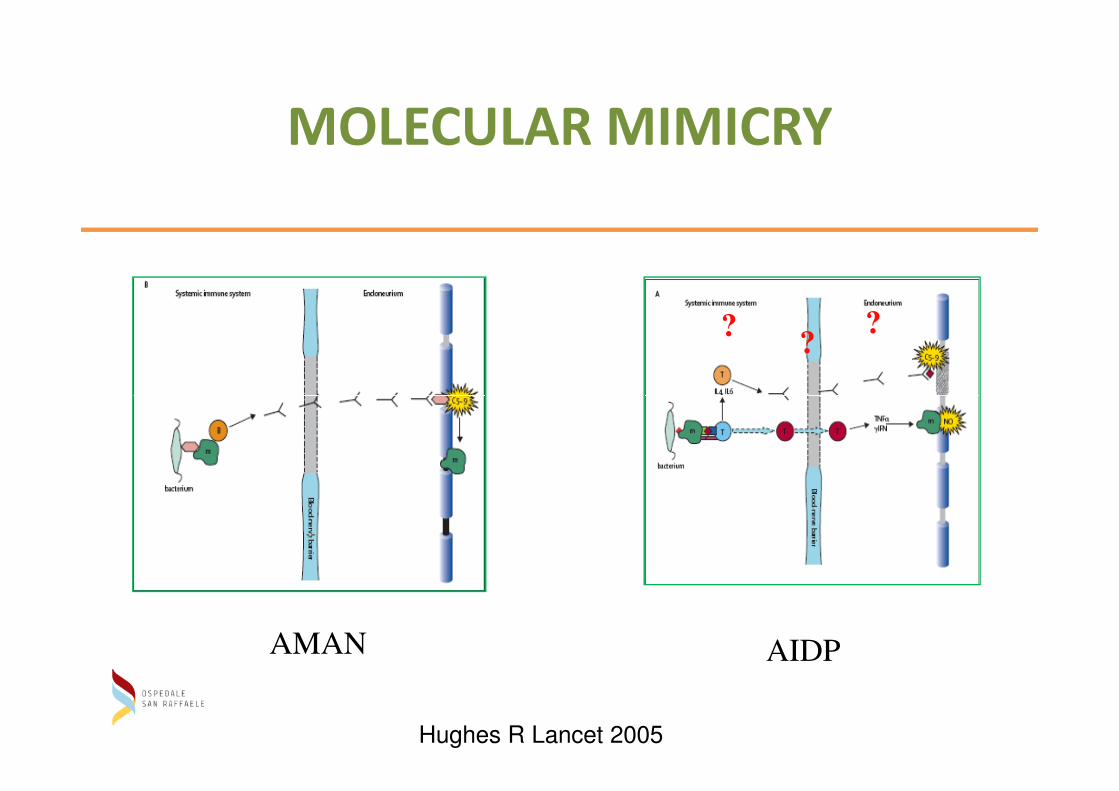
MOLECULAR MIMICRY
??
?
Hughes R Lancet 2005
AMAN AIDP
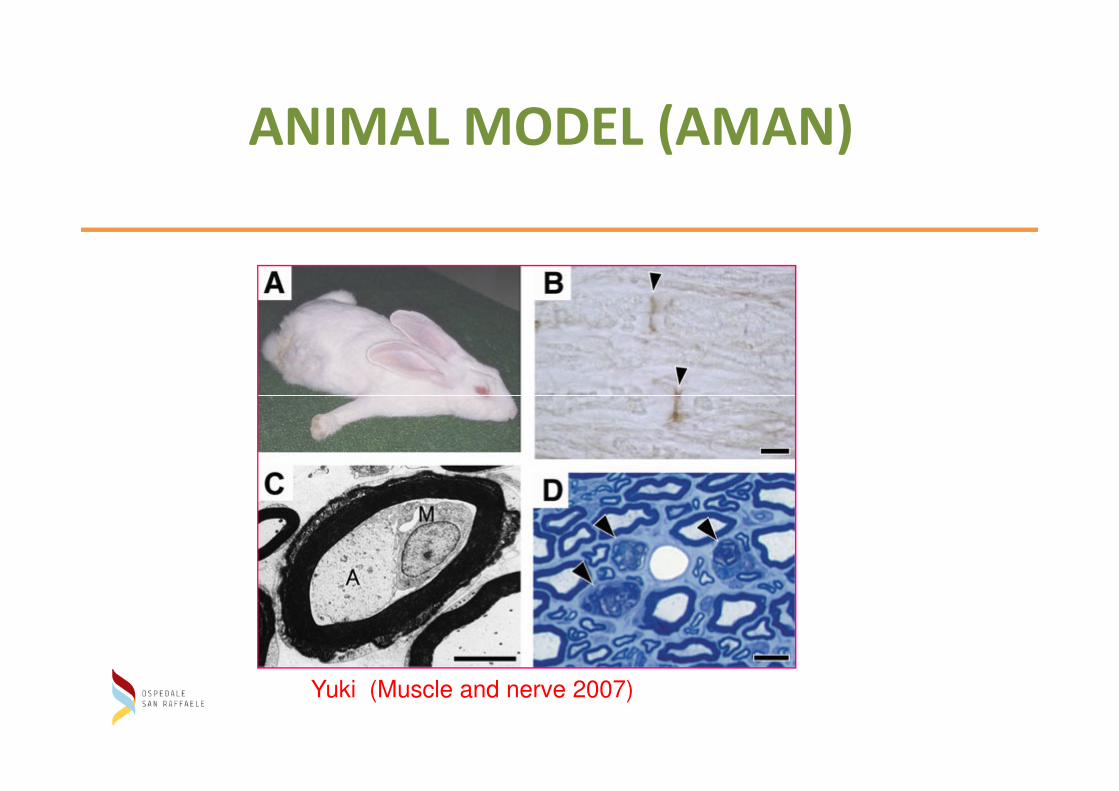
ANIMAL MODEL (AMAN)
Yuki (Muscle and nerve 2007)
PATHOGENICITY OF Ab ANTIGAGLIOSIDES
• Higher titer of anti GM1 is present at the AMAN onset and
then decreased
• Treatment with anti GD2 Ab induced peripheral s m
neuropathyneuropathy
• C.J has lipogangliosides on its surface mimiking GM1 etc
• Monoclonal anti GD1A + complement block nerve conduction
and disrupt motor nerve
• Anti GM1 Ab deceased Na+ current in nerve fiber preparation
in presence of active complement
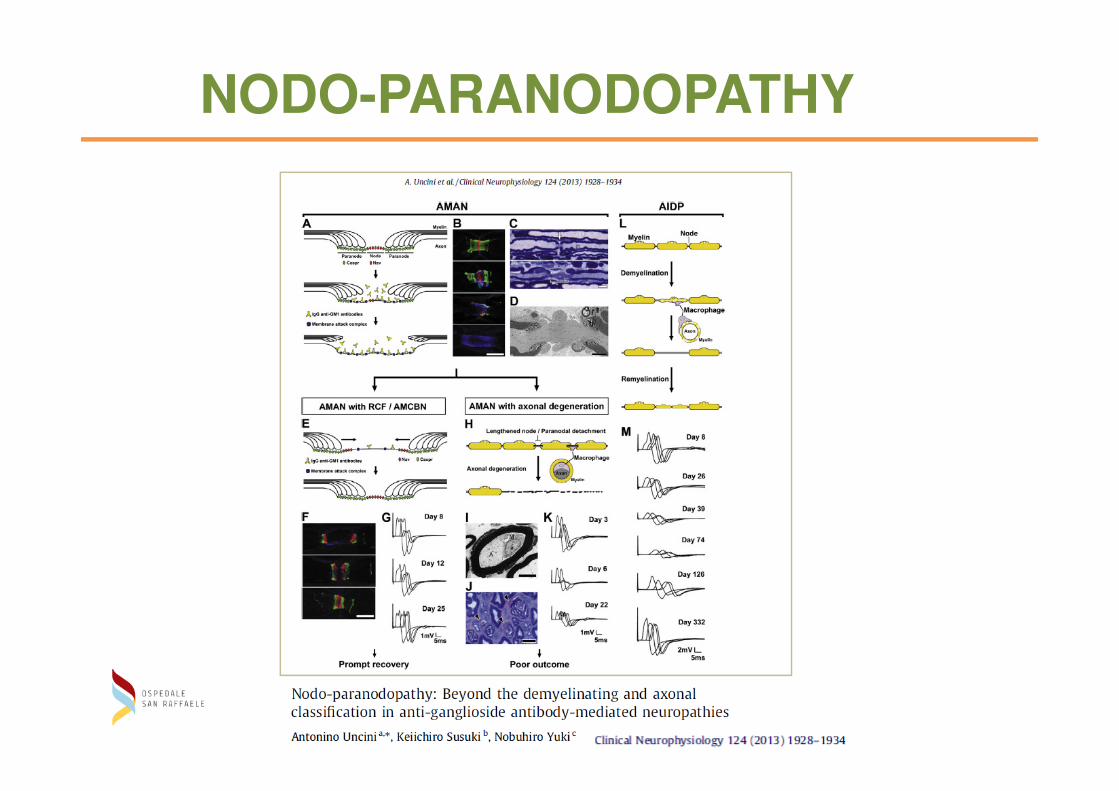
NODO-PARANODOPATHY
clinically:
MILLER FISHER SYNDROME
• Ophthalmoplegia
• Ataxia
• Areflexia
MILLER FISHER SYNDROME
Epidemiology 0.09/100.000 population Spring
-Taiwan 7-18% GBS
-Italy ( Lombardy) 3% GBS
Antecendent respiratory symtoms 76%
Gastrointestinal symptoms 4%
Within 8 days
IgG Anti GQ1b 89%
Prognosis good no death reported
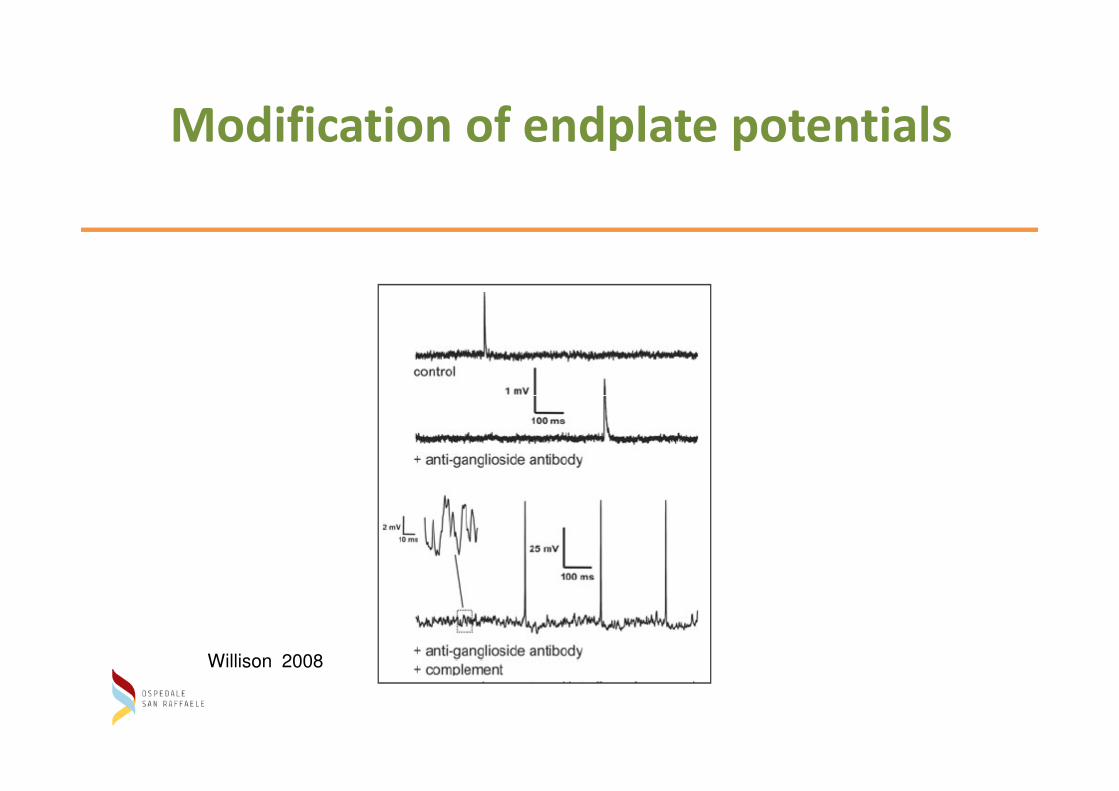
Modification of endplate potentials
Willison 2008
IMMUNOTERAPIA NELLA GBS
1) Corticosteroidi
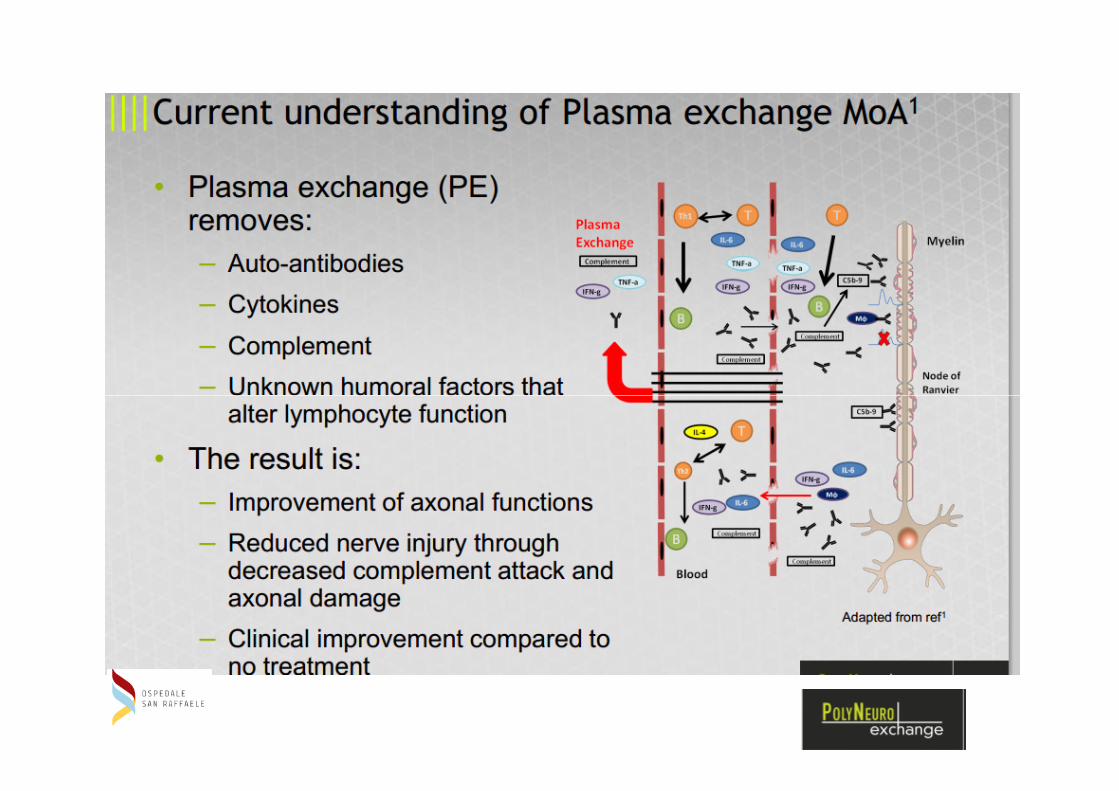
2) Plasmaexchange2) Plasmaexchange
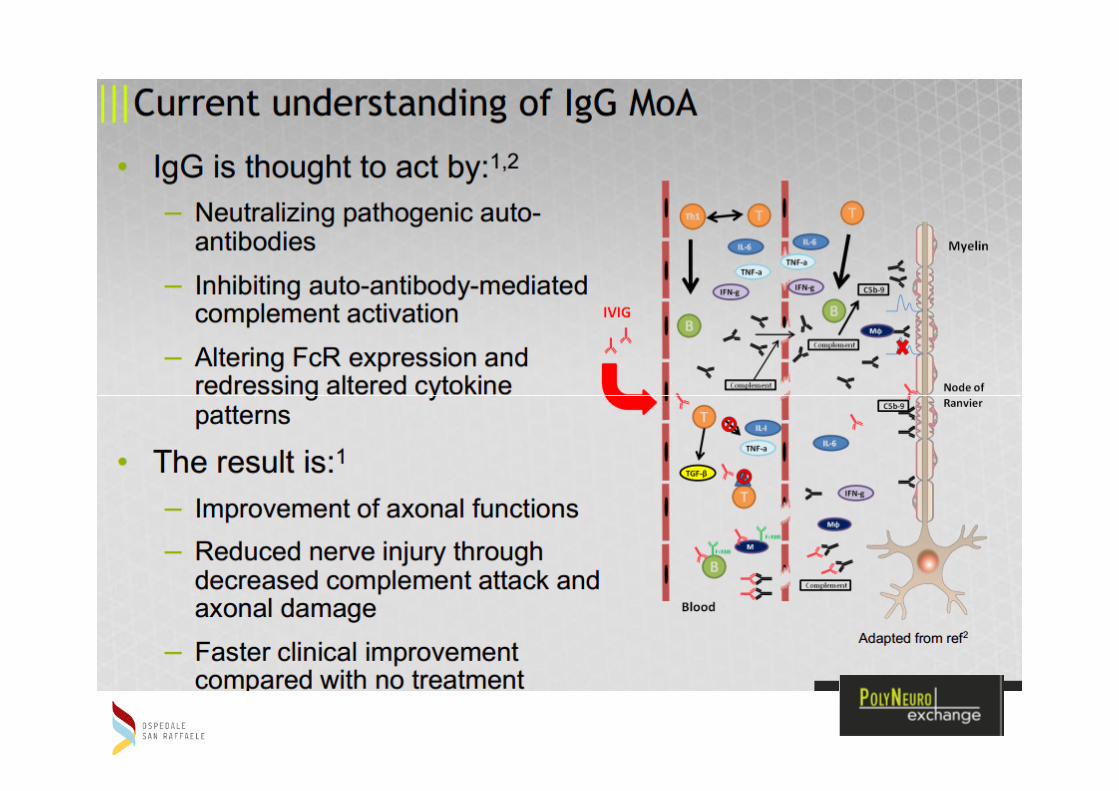
3) Igev ad alte dosi
4) Combinazione costicosteroidi e Igev
5) Altre immunoterapie
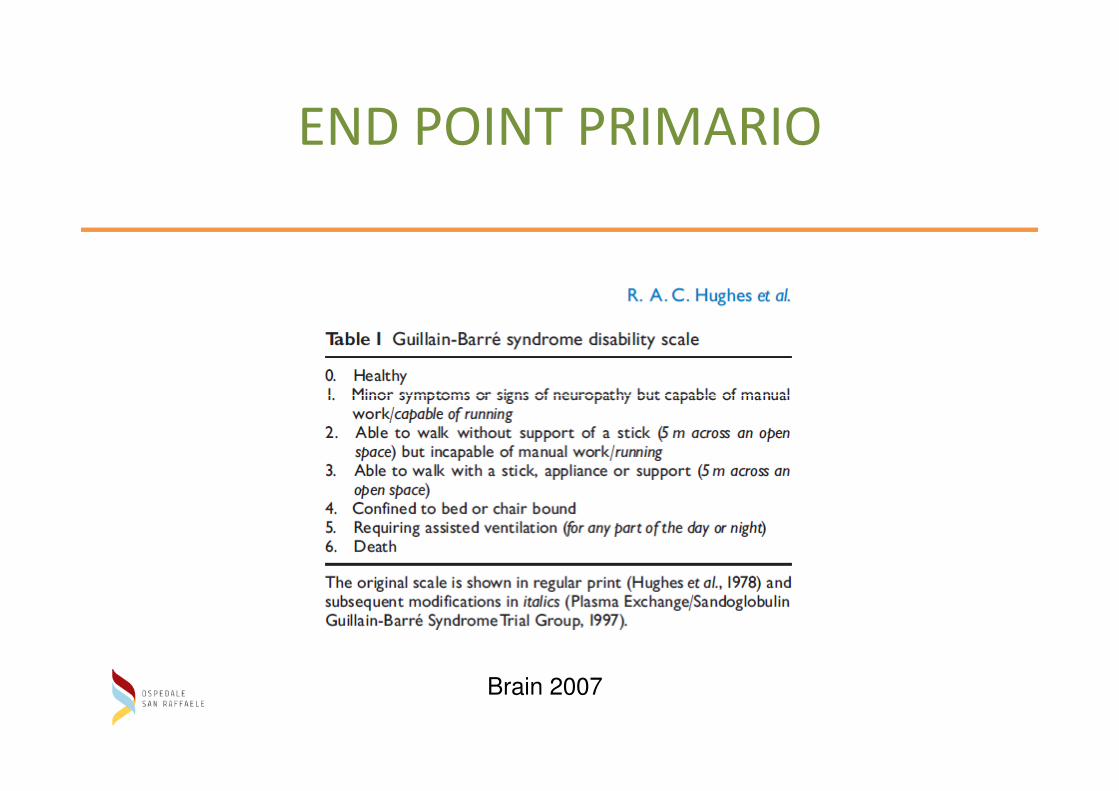
END POINT PRIMARIO
Brain 2007
Linee guida per terapia della GBS
AAN Quality standards Subcommitee
Hughes et al Neurology 2003
1: Corticosteroidi
Dosi : 500 mg ev per 5 giorni, 40-60 mg per os, ACTH 100 UI per
10 giorni.
RCTs: 6 con 195 pz e 187 controlli con placeboRCTs: 6 con 195 pz e 187 controlli con placebo
Outcome 1°: miglioramento a 4 settimane:
Risultato: Nessuna efficacia
Evidenza classe I- Raccomandazione livello A
Outcomes II°: raggiungimento di marcia autonoma, sospensione
della ventilazione assistita, mortalità e morbilità ad un anno
Risultato: Nessuna differenza Evidenza classe I
Raccomandazione livello A
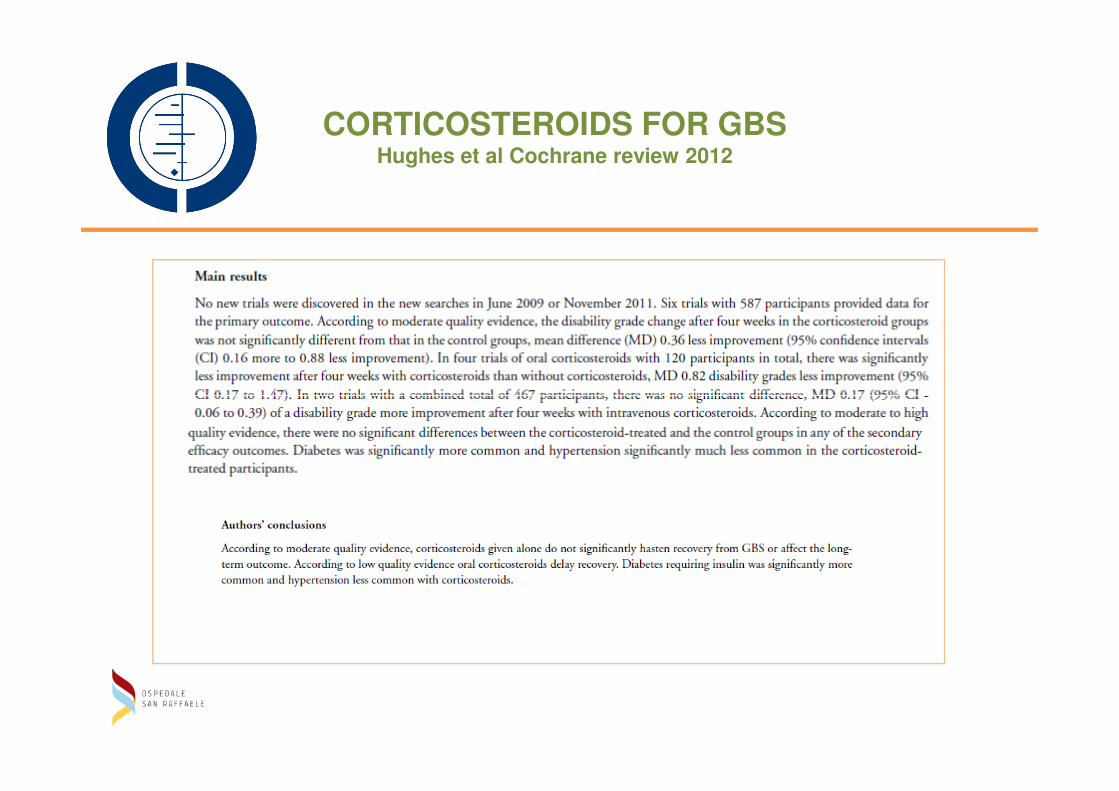
CORTICOSTEROIDS FOR GBSHughes et al Cochrane review 2012
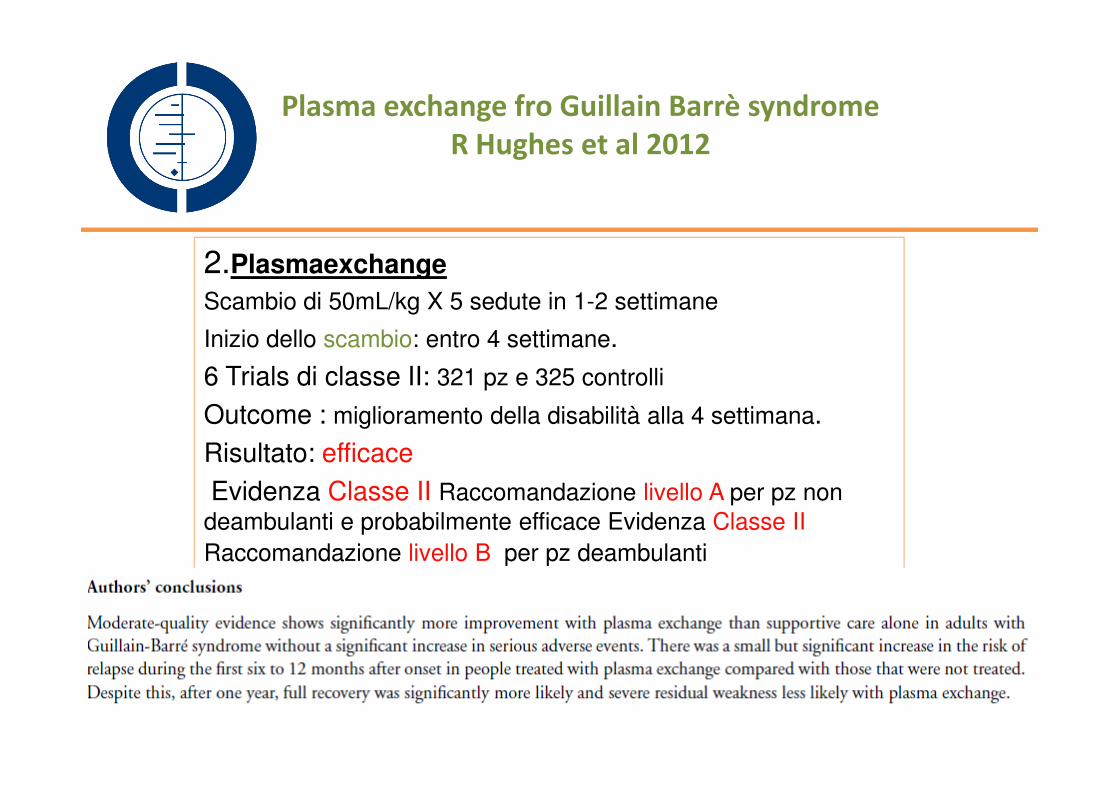
2.Plasmaexchange
Scambio di 50mL/kg X 5 sedute in 1-2 settimane
Inizio dello scambio: entro 4 settimane.
6 Trials di classe II: 321 pz e 325 controlli
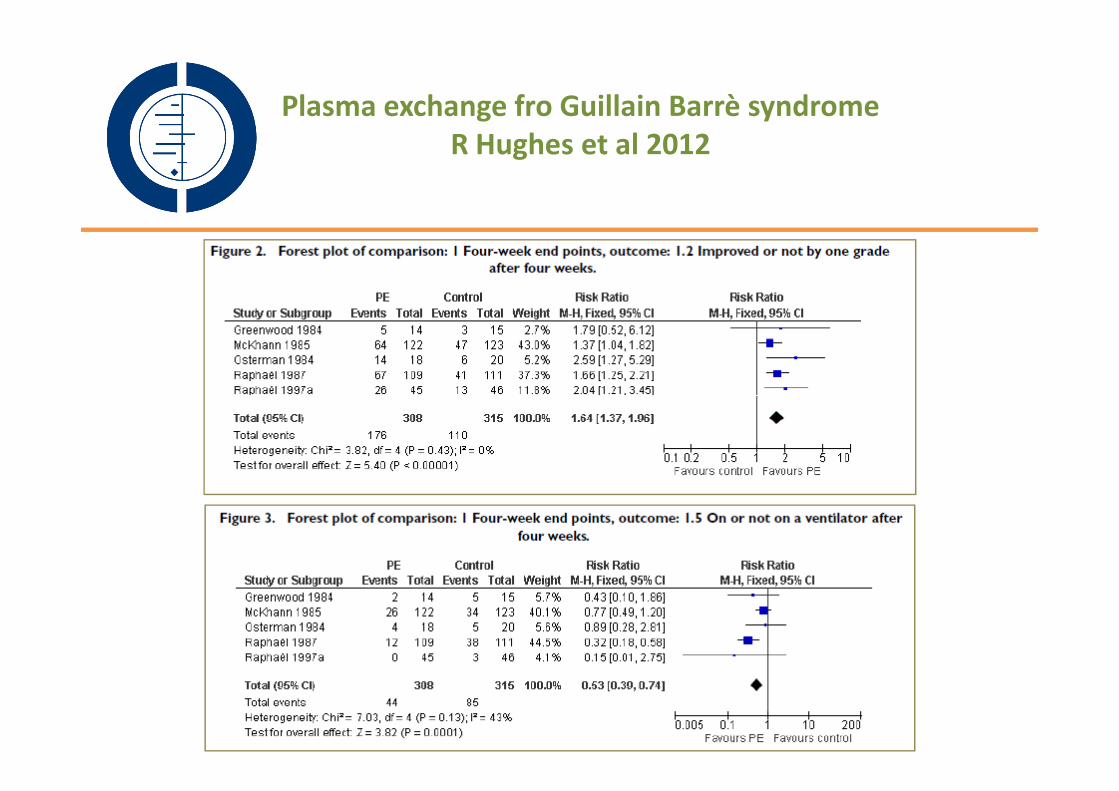
Plasma exchange fro Guillain Barrè syndrome
R Hughes et al 2012
Outcome : miglioramento della disabilità alla 4 settimana.
Risultato: efficace
Evidenza Classe II Raccomandazione livello A per pz non
deambulanti e probabilmente efficace Evidenza Classe II
Raccomandazione livello B per pz deambulanti
Plasma exchange fro Guillain Barrè syndrome
R Hughes et al 2012
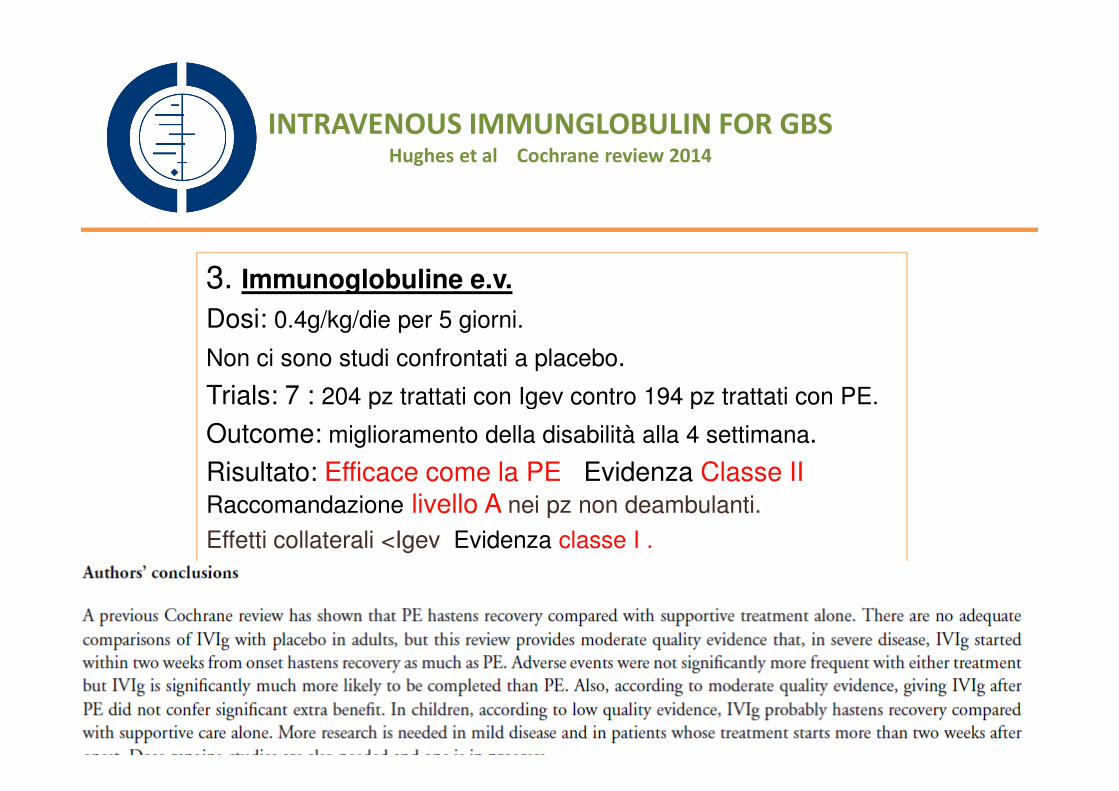
3. Immunoglobuline e.v.
Dosi: 0.4g/kg/die per 5 giorni.
Non ci sono studi confrontati a placebo.
Trials: 7 : 204 pz trattati con Igev contro 194 pz trattati con PE.
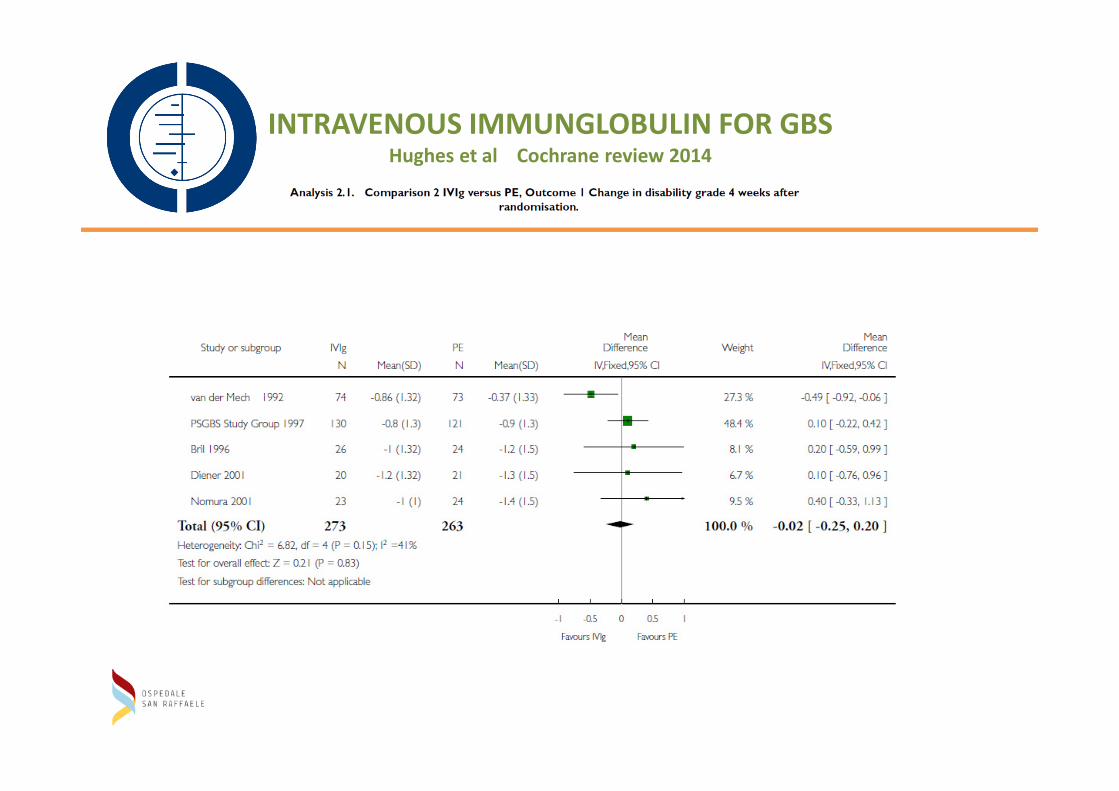
INTRAVENOUS IMMUNGLOBULIN FOR GBSHughes et al Cochrane review 2014
Trials: 7 : 204 pz trattati con Igev contro 194 pz trattati con PE.
Outcome: miglioramento della disabilità alla 4 settimana.
Risultato: Efficace come la PE Evidenza Classe II Raccomandazione livello A nei pz non deambulanti.
Effetti collaterali <Igev Evidenza classe I .
INTRAVENOUS IMMUNGLOBULIN FOR GBSHughes et al Cochrane review 2014
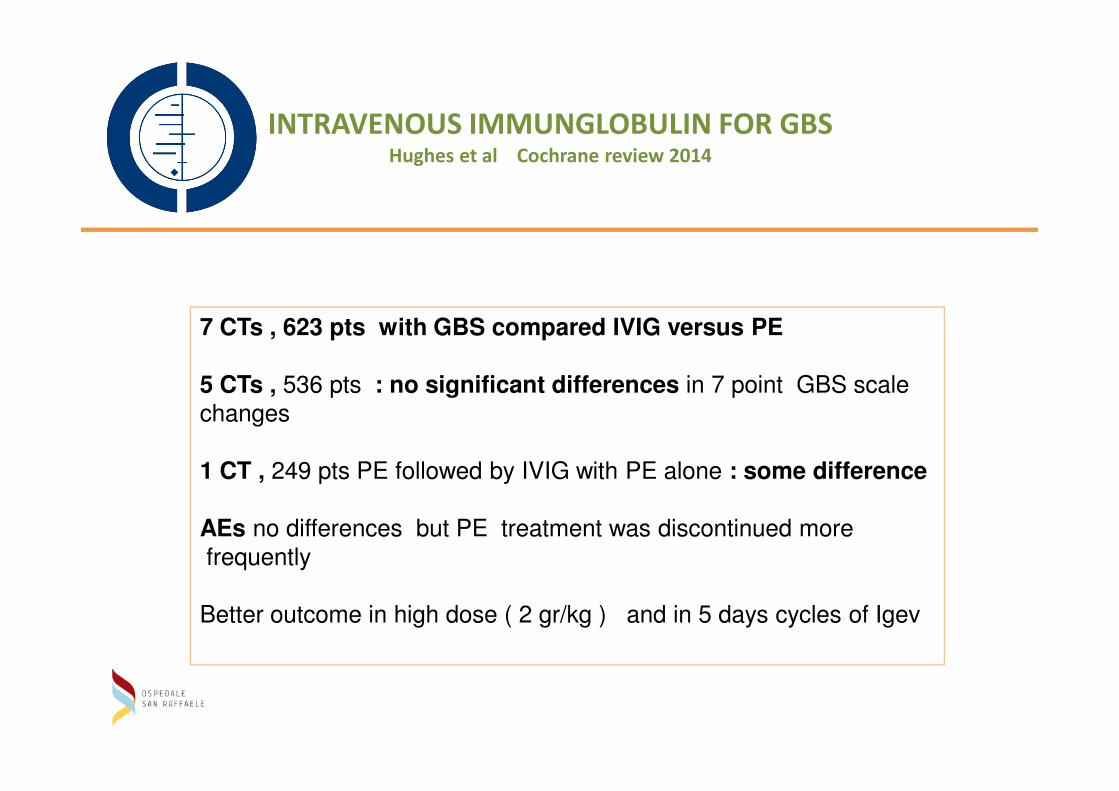
7 CTs , 623 pts with GBS compared IVIG versus PE
5 CTs , 536 pts : no significant differences in 7 point GBS scale5 CTs , 536 pts : no significant differences in 7 point GBS scale
changes
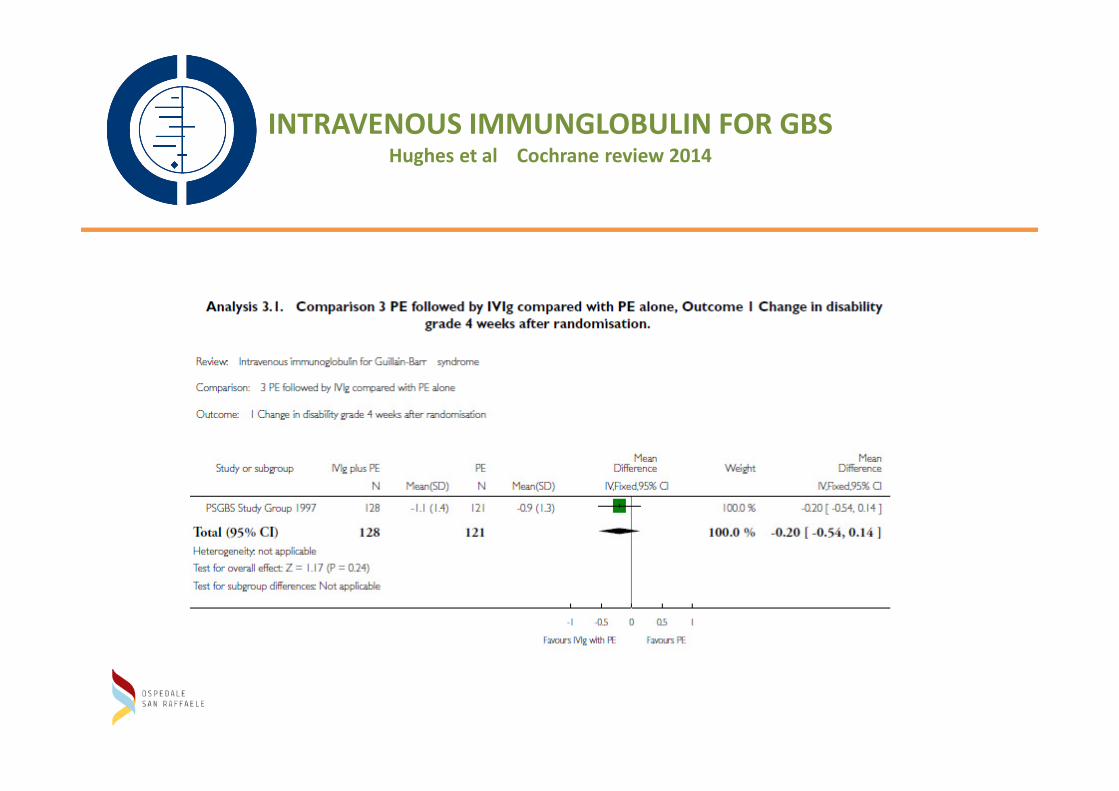
1 CT , 249 pts PE followed by IVIG with PE alone : some difference
AEs no differences but PE treatment was discontinued more
frequently
Better outcome in high dose ( 2 gr/kg ) and in 5 days cycles of Igev
INTRAVENOUS IMMUNGLOBULIN FOR GBSHughes et al Cochrane review 2014
Confronto tra IVIG e PE:
Nessuna differenza: su decessi, fluttuazione della malattia
INTRAVENOUS IMMUNGLOBULIN FOR GBSHughes et al Cochrane review 2014
Nessuna differenza: su decessi, fluttuazione della malattia
A favore delle Igvena : discontinuazione terapia, complicazioni sistemiche,
effetti collaterali
A favore della PE: migliore outcome in pz con diarrea e più veloce recupero
nei pz ventilati
INTRAVENOUS IMMUNGLOBULIN FOR GBSHughes et al Cochrane review 2014
• In GB patients:
1. La bassa glicosilazione del FC delle IgG1 e 2 predispone alla GB1. La bassa glicosilazione del FC delle IgG1 e 2 predispone alla GB
le Igev aumentano la % di IgG glicosilate nella maggior parte dei pz
se la glicosilazione rimane bassa : outcome povero
2. La dose di 0,4g/kg / die per 3 rispetto a 6 giorni non modifica l’outcome (39 pz)
ma la modifica se pz ventilato
3. La stessa dose data in 2 giorni anziché 5 ( nei bambini) non modifcia l’outcome
ma più facile la relapse
4. Il Delta IgG level dopo 15 giorni dall’infusione è indice di buona risposta
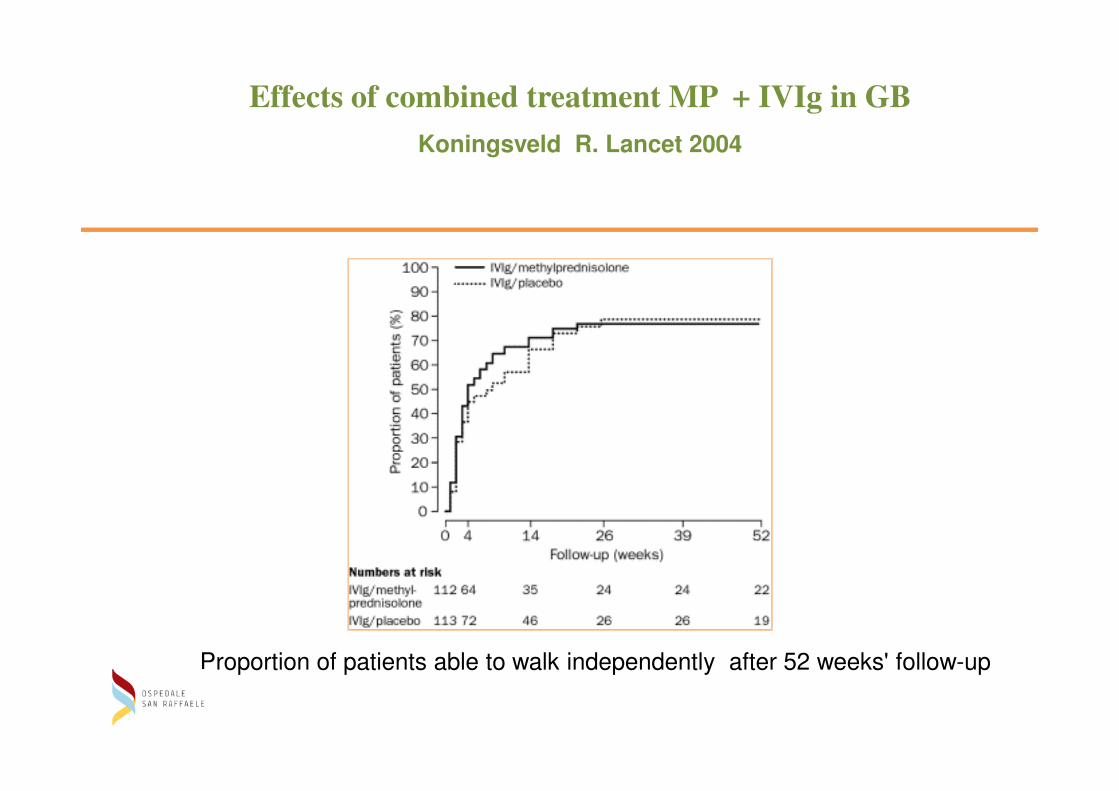
Effects of combined treatment MP + IVIg in GB
Koningsveld R. Lancet 2004
Proportion of patients able to walk independently after 52 weeks' follow-up
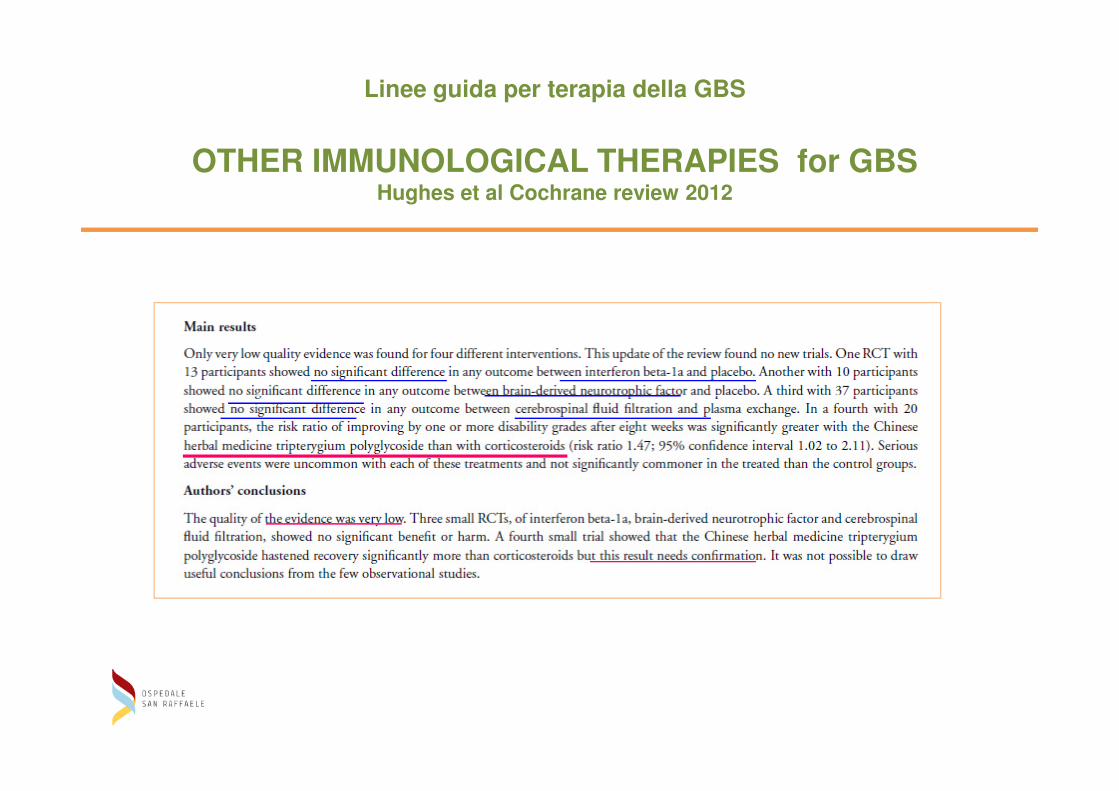
Linee guida per terapia della GBS
OTHER IMMUNOLOGICAL THERAPIES for GBSHughes et al Cochrane review 2012
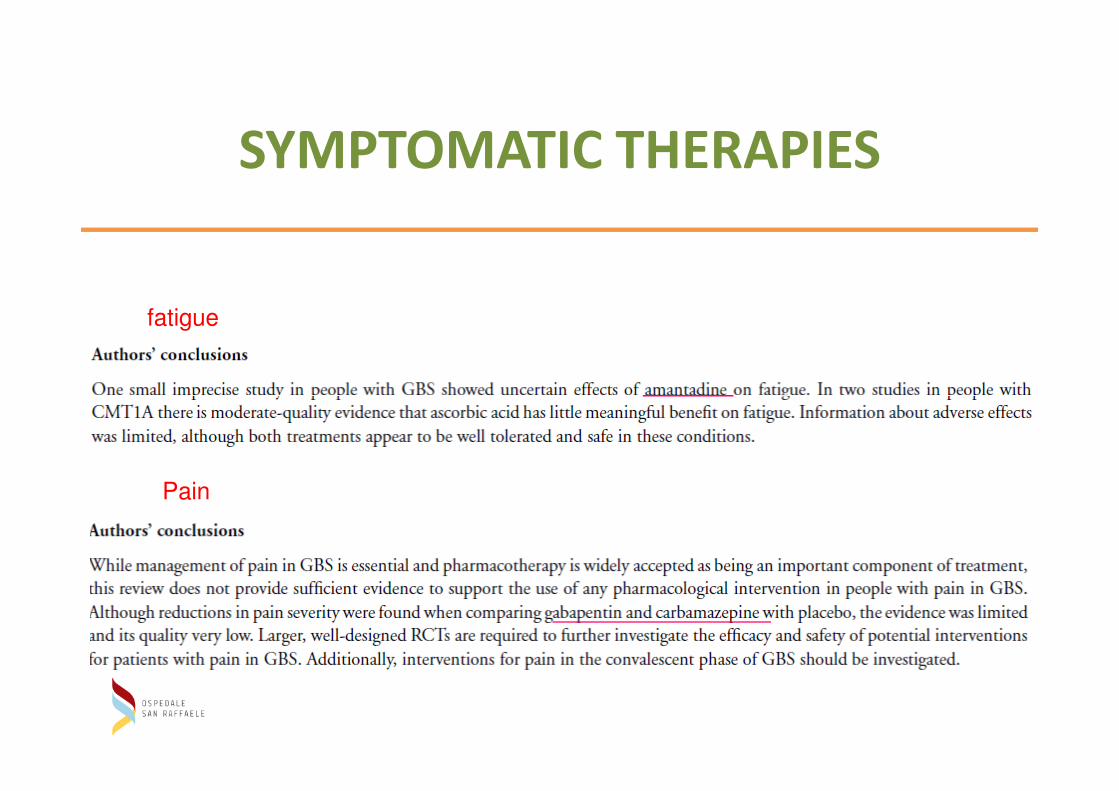
SYMPTOMATIC THERAPIES
fatigue
Pain
NEW STRATEGY
Grazie per l’ attenzione