Embed Size (px)
Citation preview
![Page 1: [IEEE NAFIPS 2005 - 2005 Annual Meeting of the North American Fuzzy Information Processing Society - Detroit, MI, USA (26-28 June 2005)] NAFIPS 2005 - 2005 Annual Meeting of the North](https://reader036.pdfslide.us/reader036/viewer/2022092702/5750a6151a28abcf0cb6d833/html5/thumbnails/1.jpg)
NAFIPS 2005 - 2005 Annual Meeting of the North American Fuzzy Information Processing Society
Fuzzy Analysis of Internment Factors for PediatricBurned
J. T. WestphalMinisterio PuTblico Federal
Procuradoria da RepuTblica em Santa CatarinaFlorian'polis, Santa Catarina, Brazil
julian(prsc.mpf.gov.br
Abstract -The decision between hospital internment or clinicaltreatment of pediatric burned represents a delicate andcomplex task for medical experts that are unprovided ofcomputational tools to help in this decision process. The socialcontext of child family, the available hospital structure, andmainly the clinical picture of the burned child are importantfactors to be evaluated in this decision context. Importantcriteria such as: Extent, Depth, Location of the Burn, Child'sAge, and Social Aspects must be weighted by the expert toreach a decision. The uncertainty derived from impreciselinguistic terms such as Moderate Injury or Great Extension arethe natural reasoning mechanism in this area. There are noprecise boundaries separating these linguistic values. Themedical reasoning based on these imprecise values leads to theconclusion about the injury classification (the diagnostic) andabout the correct decision to be made: interning the child orprescribing an ambulatory treatment. An Expert System thattranslates the -uncertain medical knowledge in a set of fuzzyrules is the proposal of this research. The model was designedas an interactive and flexible tool that allows therepresentation of distinct scenarios through modifications ofparameters such as weights of interment factors and type orparameters of membership functions.
I. INTRODUCTION
Computers has been used as an essential tool in allfields of human activities. Initially used as sophisticatedcalculator machines, the computers are now used aspowerful tools to help in the decision making process.Excepting the well-known calculation power of thesemachines, the objective of AI (Artificial Intelligence)researches is to provide new models and mechanisms toincrease the potential and applicability of computersthrough the simulation of intelligence. Among theobjectives of new researches in the AI field is the treatmentof more complex problems, mainly problems that involvesophisticated reasoning mechanisms to be solved. In thiscontext are the decision making problems that are in thescope of the present work.
An important result of the researches in Al was thedevelopment of Expert Systems (ES) [1,2]. These systemsare designed to act as the human expert in a specific field.And to perform this task, an ES must be composed of deepknowledge related to the area where it will be applied. Anarea of vast application for ES has been the medicine.Medicine is the Science where the power of Al was earlyrecognized, in the middle of 70's, when the most ofcomputers applications were constructed to treat the
G. F. RoyesMinisterio Pu'blico Federal
Procuradoria da RepuTblica em Santa CatarinaFlorian'polis, Santa Catarina, Brazil
uncertainty in the diagnostic of diseases. In this domain, theES can help in several stages of the clinical proceedings,such as: diagnosis analysis, assessment of internmentcriteria, and therapeutic indication.
The main initial objective of the present work is toconstruct an ES that can help the decision maker in theprocess of evaluating the internment (or ambulatorytreatment) of pediatric burned, through the assessment ofsome important criteria.
The decision about patient's internment, according tothe clinical condition, represents a specialized medicalactivity. After the diagnostic emission, a careful medicalanalysis indicates if a patient must be interned to makepossible a more intensive care or if a simple ambulatorytreatment is enough. An ES in this area can deal with theinitial diagnosis obtained by another system or by medicalprofessionals, analyzing the patient's health situation andthen indicating the necessity of internment using somecriteria applied by medical experts.
The decision for internment results in a series ofconsequences involving costs, risks, and a possiblyunnecessary wearing for pediatric patients. The internmentof pediatric patients must be a careful decision since thehospital environment is usually propitious to contaminationand the separation of the familiar support must be alsoconsidered. However, the omission of an adequateimmediate treatment can prejudice the suitable patientrecovery, making difficult the scaring process and, at theworst, this omission can cost the patient's life [3].
The presence of the uncertainty is a constant in thisdomain where the medical reasoning must be modeled. Theuncertainty is derived from different sources such as: theindividual differences between patients, absence of enoughclinical data, classification of injuries, extent and location ofthe injured area, and the distinct analysis produced bydifferent professionals for the same clinical picture. Hence,some relevant variables were considered after the detailedanalysis of the internment conduct: Injury Extent, Thicknessof Burn Injury, Age Group, Location of the Bum, CausativeAgents of Burns, and Social-economical Conditions.
The assessment of the degree of fulfillment of eachcriterion is the great difficulty in the internment decision.For instance, patients with 10% or more of the Total BurnedSurface Area (TBSA) configure a typical case of internment(in this case these patients are considered Medium Burned),however, since the exact burned surface is difficult toestimate, as well as the singularities of each specific case, it
0-7803-9187-X/05/$20.00 ©2005 IEEE. 442
![Page 2: [IEEE NAFIPS 2005 - 2005 Annual Meeting of the North American Fuzzy Information Processing Society - Detroit, MI, USA (26-28 June 2005)] NAFIPS 2005 - 2005 Annual Meeting of the North](https://reader036.pdfslide.us/reader036/viewer/2022092702/5750a6151a28abcf0cb6d833/html5/thumbnails/2.jpg)
is not desirable that patients with 9% of TBSA have thedecision of internment completely dismissed. Using a fuzzyreasoning model, the decision is based on degrees ofmembership to frizzy sets (in this case the internment fuizzyset) that are much more accurate and suitable to representthe decision process in this context than a crisp solution.
In the present research, the concept of fuzzy sets [4] andfuzzy logic [5] was applied in an ES to deal with the kind ofuncertainty present in the medical reasoning used to analyzethe internment criteria of pediatric burned. The choice forfuzzy was made by the kind of uncertainty [6] that thisapproach can handle. The subjectivity, vagueness andimprecision of the medical reasoning (linguistic terms arenaturally used) is justly the kind of uncertainty that can besimulated using fuzzy.
The Fuzzy ES was constructed with the direct help ofexperts in the domain of pediatric burned in the onlyinstitution specialized in the treatment of burned children inthe whole State of Santa Catarina (located in Florianopolis -Brazil), the Joana de Gusmao Hospital. The criteria, fuzzysets and fuzzy rules are defined with the assistance of theseexperts.
The next sections are organized as follows: Section IIshows the motivations for the ES construction, Section IIIpresents the main objectives of the present research, SectionIV presents some aspects of the application domain, SectionV details all the ES structure, and, finally, the last section isdedicated to the conclusions and future extensions of thiswork.
II. MOTIVATION
This research was motivated by two years ofcooperative work developed with an important expert in thefield of pediatric burned. One of the main lacks identifiedby this expert was the absence of a computationalmechanism to help in the decision about the internment ofpediatric patients (possibly by the subjective decision natureof this field). With an analysis tool, the decision process canbe systematized and more secure decisions can be madebased on experimented knowledge. The existence ofsubjective internment criteria and the vagueness of themedical reasoning lead to a decision based on theprofessional skill only. The lack of specialized professionalsin this area, the absence of computational intelligentmechanisms that could help in this complex internmentdecision, and the impact that a bad decision can representfor the patient are some of the motivation factors of thisresearch.
The inadequate conditions of hospital institutions forthe treatment of burned patients represents a great lack ofthe public health system and another motivation for thiswork. The Joana de Gusmao Hospital (JGH), in the State ofSanta Catarina - Brazil, was used as the base of experimentsfor the present research. The JGH is located in Florian'polis(the capital of Santa Catarina State) and it has the only unitofburned children in the whole State. Only this institution isqualified to assist a great population in a wide area, assistedby a restricted staff of qualified professionals.
III. MAIN OBJECTIVES
The main objective of this research is supporting themedical decision about internment or ambulatory treatment,that is usually made by an unique isolated expert, throughthe application of an intelligent mechanism that will beconstantly improved by the expert staff. Some otherimportant objectives can be pointed out:* Present a model to deal with the imprecise information
existent in the internment decision without suppress thenatural uncertainty present in the process.
* Minimize errors of internment conduct by the constantuse and improvement of the proposed model.
* Offer a robust tool for training of inexperienced medicalstaff in hospitals and also as a mechanism for simulationof cases.
IV. APPLICATION DOMAIN
A. Skin Anatomy and Physiology [7]The skin is the largest organ of the body composed of
specialized epithelial and connective tissue cells. Besidesthe covering tissue, it consists of mucous membranes, nails,and hair. Among the vital functions of skin can be pointedout: protection, immunity, body temperature regulation,fluid balance, and metabolism. In a vertical perspective, theskin can be divided in three distinct layers: the epidermis(forms the external surface of the skin with distinct depthsfrom 0.05mm in the eyelids to 1.0mm in the foot plantarregion), the dermis (the intermediate layer, ten times thickerthan the epidermis), and hypodermis or subcutis (the deeperlayer - serves to attach the dermis to its underlying tissues).
The epidermis is the more external surface of the bodyand it is mainly composed by keratinocytes (epithelialcells), Langerhans cells, basal cells, and melanocytes. Incontact with the external environment the epidermissupports different kinds of aggressions such as impacts,burns, and contact with harmful substances. In consequence,the skin is completely renovated in cycles of 28 days frombasal cells. The main characteristics of epidermis are thepower, flexibility, elasticity, and resistance.
After the epidermis, the dermis is the next layer. Itsmain function is the protection against harmful agents thathave surpassed the protection of epidermis. The dermis canbe subdivided in two parts: the papillary dermis (the mostsuperficial composed of collagen fibers and weak elasticfibers) and the reticular dermis (the deeper layer thatreaches the adipose layer - composed of elastic fibers and atick bundle of collagen). The nails, sebaceous glands, hairs,and sudoriparous glands (the cutaneous appendices) areoriginated from the dermis.
The deeper potion of skin is the hypodermis layer (orsubcutaneos tissue). Its composition is based on bundles ofconjunctive tissue covering the adipocytes (fat cells). Themain functions of hypodermis are: protect the body againstphysical traumas and provide a store of calories.
The structure of skin in layers is shown in Fig. 1.
B. Burns [8]Burn is a kind of injury caused by different agents
443
![Page 3: [IEEE NAFIPS 2005 - 2005 Annual Meeting of the North American Fuzzy Information Processing Society - Detroit, MI, USA (26-28 June 2005)] NAFIPS 2005 - 2005 Annual Meeting of the North](https://reader036.pdfslide.us/reader036/viewer/2022092702/5750a6151a28abcf0cb6d833/html5/thumbnails/3.jpg)
(thermal, electrical, chemical, or radioactive) that affects thecovering tissues. The bum injury may cause total or partialdestruction of skin and cutaneous appendices, includingdeeper layers of subcutaneos tissues, tendons, and bones.Bum is one of the most critical categories of injury not onlyby the risk of death but also by the physical andpsychological sequels and important repercussions in themetabolism.
With regard to age, the most severe bums happen withchildren. The corporal surface in relation to weight is threetimes higher in children compared to adults. Moreover, thechild's skin is thin and subject to deeper injuries and to amajor loss of body fluids. The limited pulmonary reserveand an immature immunology system cause a higherphysiological impact ofbum in children than in adults.
The main causative agents ofbums are classified in twogroups: physical agents and chemical agents. The kinds ofagents are detailed below:* Physical Agents can be thermal (caused by fire, steam,
hot objects, or hot liquids), electrical (whose lesion canaggravate in the first days after the accident), andradiation bums (caused by the sun). These agents are themain cause ofbums.
* Chemical Agents are usually acids (sulfuric or nitric)and alkali (caustic soda or ammonia). The injury causedby these agents usually evolve after the accident still thata suitable asepsis have been made.The age of patients more reached by accidents involving
bums is until five years old - children that are in the phaseof "discovering". The low social-economical level and theomission of parents are factors that more contribute to thehigh level of accidents with children.
TS\\\ \ bHairThe Skin\\ \\ /Sebaceous Gland
,Sensoy Nave Ending
_ -EpidermisI Nerve
Dennis
Subcutaneous risrue
=Bo~~~- -I Arterioie7 Musc~le \Sweat Gland Fat, Collagen, Fibroblasts
Fig. I Skin Structure
C. Burns Classification [9]The diagnostic of the bum's extension is normally
characterized by the uncertainty and by the necessity of adeep knowledge by the expert. In some cases, the realextension of bum cannot be correctly evaluated in the firstdays.
Until recently, the criterion for classification of bumswas the deep of tissue destruction. The injuries weredistinguished in different degrees: first degree, seconddegree superficial, second degree deep, third degree, andfourth degree.
The first degree bums are characterized by theepidermis destruction, hence, considered superficial. Anedema may occur with local pain, but without blistering.The cause of this kind of bum is usually sun exposure andusually heals in seven days approximately.
In second degree bums the damage extends through theepidermis and involves portions of dermis. They areconsidered superficial when the damage involves only thesuperior portions of dermis. They are very painful andpresent blistering. The reepithelization process takes twoweeks approximately with minimal scars. This kind of bumis usually caused by excessive sun exposure or by hotliquids. Deep second degree bums are characterized by thedestruction of great part of dermis with a few epithelialsurviving elements. Due to the depth and almost absence ofepithelial surviving elements the reepithelization isuncertain and several weeks can be necessary to appear afine and unstable epithelium.
Third degree bums destroy all the thickness of the skinand adjacent tissue without possibility of a spontaneousregeneration oftissues, excepting small lesions. This kind ofbum is caused by exposure to radiation of high density,direct fire, chemical substances, electricity, or a longexposure to a heat source.
Fourth degree bums are characterized by very deepinjuries reaching muscles, tendons, and bones. Theamputation of the injured area is usually necessary.
A more recent classification of bums observes thecapacity of tissue reepithelization after the injury. The newclassification distinguishes the lesions in total or partialthickness.
The bums of partial thickness are subdivided in twocategories: superficial and deep, according to the naturalcapacity of tissue regeneration from the preserved epithelialelements.
The bums of undefined thickness between the partialand total thickness representing an area of uncertaintydiagnostic.
In bums of total thickness, the destruction of skin andcutaneous appendices is complete, making impossible thetissue regeneration (the treatment is usually based ongrafts).
In recent therapies, an important focus is on the lesiondeep, since this characteristic is used to define the patient'streatment. The residual tissue that does not presentpossibility of spontaneous regeneration is removed andsurgeries with graft implant are realized [10].
D. Estimation ofthe Extension ofthe Total Burned SurfaceArea (TBSA) [11]
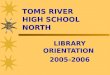
The different proportions of body regions must beconsidered to verify the extension of the bumed surface andconsequently the classification of the injury. Theseproportions change according to the patient's age (Fig. 2shows how these proportions change according to the groupage). This characteristic is essential to evaluate the TotalBumed Surface Area (TBSA) in patients of different ages.
444
![Page 4: [IEEE NAFIPS 2005 - 2005 Annual Meeting of the North American Fuzzy Information Processing Society - Detroit, MI, USA (26-28 June 2005)] NAFIPS 2005 - 2005 Annual Meeting of the North](https://reader036.pdfslide.us/reader036/viewer/2022092702/5750a6151a28abcf0cb6d833/html5/thumbnails/4.jpg)
4A
stSuckling
Fig. 2 Distinct body proportions according to the age group [11]
V. EXPERT SYSTEM FOR THE EVALUATION OF INTERNMENTFACTORS IN PEDiATRIC BURNED (ESEIF - PB)
The expert system here specified is the practical resultof the detailed analysis of the reasoning mechanism appliedby the medical experts. The sequence of this sectionpresents the main characteristics of the proposed system.
A. General CharacteristicsThe system has an interactive interface through which
the main patient's features and injury's features are
informed. A child picture in both dorsal and ventral planesis showed (see Fig. 3). The system user paint thecorrespondent burned areas, with distinct colors accordingto the injury thickness. The Total Bumed Surface Area(TBSA) to each kind of injury is calculated, observing allthe variations of body proportions according to the patient'sage group (Fig. 3).
Injury. The system reasoning mechanism is composed oftwo main steps:* First, the crisp values relative to the three input variables
(Patient's Age Group, Injury Thickness, and InjuryExtent) are informed through the system interface. Thesevalues are fuzzified through the membership functionsand the activated rules generate alfa-cuts levels in thesets of the output variable Injury Classification. Thesegenerated sets determined by the cuts are thenaggregated to obtain the fuzzy result for the outputvariable Injury Classification. Finally, a crisp valuerepresenting this fuzzy result is calculated by adefuzzification method [13];
* Second, the defuzzified crisp value relative to the InjuryClassification is used to calculate the resulting degree ofmembership for the sets of the output linguistic variableIntetmment Conduct (Intermment or AmbulatoryTreatment) - a new fuzzification process isaccomplished (see Fig. 4).
Besides the fuzzy reasoning represented by the fuzzyrules (considering the uncertainties in the medicalreasoning), the proposed system has also a set of crisp rulesthat are used to compare the new fuzzy model with thetraditional methodology suggested by the Brazilian HealthMinistry. This traditional method classifies the patient asSmall Bumed, Medium Bumed, or Great Bumed. Thepatient who is classified in one of the two last sets (Mediumor Great) is directly conducted to intermment [ 12]. Using thefuzzy reasoning, the partial membership to the sets isconsidered and the conclusion about the IntemmentConduct is more accurate, according to the experts.
RHO r,IfHRflDtdOHWOl 011R. 3. 0 *0t84*1*11018,I 8 180844m
Rd. 1I t(SMIF 1 I S -.-1. 35[ L2 I 1a-8-
I i =4! 56 7C i
Fig. 4 Rules Evaluation
Fig. 3 The ESEIF-PB interactive interface
A set of rules is evaluated and gives as the first resultthe injury classification according to its seriousnessrepresented by the fuzzy sets: Soft, Moderate, or Hard
B. System Fuzzy Variables (Internment Criteria) andRules
The fuzzy variables (only the more important criteriafor the intemment decision were selected) showed in Table Iwere defined based on the detailed analysis of theinternment conduct problem and with the direct help ofmedical experts. Table I shows the system fuzzy variableswith their respective fuzzy sets.
445
RM- i;iv11td ,,l
![Page 5: [IEEE NAFIPS 2005 - 2005 Annual Meeting of the North American Fuzzy Information Processing Society - Detroit, MI, USA (26-28 June 2005)] NAFIPS 2005 - 2005 Annual Meeting of the North](https://reader036.pdfslide.us/reader036/viewer/2022092702/5750a6151a28abcf0cb6d833/html5/thumbnails/5.jpg)
TABLE ISystem Fuzzy Variables and Fuzzy Sets
Injury Extent Small, Medium, Greatlatient's Age Group Suckling, Child, Adultnjury Thickness Partial, Undefined, TotalInjury Classification - Soft, Moderate, HardInterment Conduct - Ambulatory, Internment
The base of rules has both fuzzy rules (see the ES fuzzyrules in Table II), that can be partially activated according tothe degree of membership obtained for the fuzzy sets of therule antecedents, and crisp rules (see the ES crisp rules inTable III) that are simply activated or not activated. Theserules represent special cases in which the InjuryClassification is directly assessed, such as in the case of faceburning, where all the other criteria are dismissed and theinjury is assessed as critical.
TABLE IIFuzzy Rules (ESEIF-PB)
Medium Partial ModerateUndefined ModerateTotal Hard
Great Partial HardUndefined HardTotal Hard
Child Small Partial SoftUndefined ModerateTotal Moderate
Medium Partial SoftUndefined ModerateTotal Hard
Great Partial ModerateUndefined HardTotal Hard
All the system rules that are activated in each case forthe conclusion of the internment conduct are presented forthe decision maker (the system user), aiming at the learningof the decision process for inexperienced professionals andas a explaining mechanism of the obtained conclusion (seeFig. 4).
TABLE mCrisp Rules (ESEIF-PB)
lectrical Agents Hardands Bums Moderateeet Burns Moderateace Burns HardSteam Inhalation HardUnfavorable Social-economical HardConditionsPerineum Bums ModerateGenitals Burns Moderate
C. Adjust ofSystem ParametersIn ESEIF-PB, several parameters initially supplied by
the medical specialists could be changed by the decisionmaker in order to observe and simulate different behaviors,to make the knowledge updating, or to represent adaptationsto new realities. It is possible to create several distinctconfigurations that can be saved and used alternately, inspite of a standard configuration defined by experts isinitially provided. The medical expert (the decision maker)can adapt the model parameters according to the hospitalstructure and social conditions. The universe of discourse,the function format (bell, type S, Z, L, gamma, trapezoidal,or triangular functions) and function parameters of themembership functions of the fuzzy sets of system variablescan also be changed.
For instance, when the number of available beds isreduced in a hospital, some adaptations must be performedin the system reasoning structure to adapt it to the newscenario. In this specific case, the weights of the fuzzy setsof variable Injury Classification must be adapted to reflect amore flexible internment conduct.
D. System Validation and Practical ResultsIn order to perform a system validation, it was utilized
clinical cases provided by medical experts. The parameterswere adjusted, in order to get the expected conduct. Thequalitative evaluation was made with cases like theexamples showed in Table IV.
Table IV shows the initial crisp patient's information,the fuzzified values for the input variables (Patient's AgeGroup, Injury Thickness, and Injury Extent), the degree ofmembership for each one of the fuzzy sets of the outputvariables (Injury Classification andInternment Conduct).
It is necessary to emphasize that, in the system result,the degree of membership for the two possible actions(Ambulatory Treatment or Internment) is detached, leavingto the decision maker (the doctor) the final choice. TheTable IV shows, in the last column, the system resultsindicating the ambulatory treatment for the first case and theinternment for the last two cases.
446
![Page 6: [IEEE NAFIPS 2005 - 2005 Annual Meeting of the North American Fuzzy Information Processing Society - Detroit, MI, USA (26-28 June 2005)] NAFIPS 2005 - 2005 Annual Meeting of the North](https://reader036.pdfslide.us/reader036/viewer/2022092702/5750a6151a28abcf0cb6d833/html5/thumbnails/6.jpg)
Soft = I Ambulatory =Moderate = 0,38 Internment =
Hard = 0
8 years Old, Suclding = I Undefined Soft = 0 Ambulatory = 0,13TSBA = 8,5 %, Medium= 0,894 Moderate = 0,894 Internment = 0,825Undefined thickness Great = 0,004 Hard = 0,0046 month Old, Suckling = I Total Soft = 0,75 Ambulatory = 0TSBA = 20,5 % Small = I Moderate = I Internment = 0,975Undefined , Partial and Partial Hard = 0Total thickness Small = 0,74
Medium = 0,04UndefinedSmall = 0,59Medium = 0,06
* Total Burned Surface Area
VI. FuTuRE WoRKs AND CONCLUSIONS
As a suggestion of future works is proposed theconstruction of an intelligent integrated platform to help inseveral stages of the care of pediatric burned, which willcombine different.activities related with this clinical area.Some main modules of this platform are described below:* Indication of bums treatment, recommending the correct
dosage of medicaments and hydration formulas. Thismodule would work with the uncertainties handled in theinternment diagnostic. A hybrid mechanism with Fuzzyand Case Based Reasoning (CBR) [14] can be utilized torecover past similar cases that can be adapted to offer anindication of treatment (surgery, graft, hydration, etc.)for a new patient. The success of past treatments (thekind of hydration and medicament dosage used) insimilar cases can be used as an indicative of goodpractices in a new situation. The acquisition of newrelevant cases will improve the capacity of a correctdiagnostic indication and of a suitable treatmentindication;
* Surgery indication to skin graft. This module willrecommend how many graft surgeries will be done, withthe respective graft extensions, to minimize thecommitment of skin breath, which is an important factorto the success of the surgery process. A mechanismbased on Fuzzy Sets and Case Based Reasoning willanalyze several past cases for matching, and suggest, foreach surgery done, the next step indicated, according tothe patient's treatment response;
* A base of past cases with the expert conduct can also beused as a learning mechanism to allow the adaptation ofthe system parameters according to these experimentedcases. This mechanism would be useful since parameterssuch as limits and function formats of each fuzzy set aredifficult to define.The main criteria for the decision about the internment
of pediatric burned were modeled in an Expert System with
the objective of helping in the complex decision about thecorrect conduct: internment or ambulatory treatment. TheES was also constructed to act as a learning tool forinexperienced doctors.
At this moment, the system is in a practical evaluationprocess in the Joana de Gusmao Hospital, using the initialconfigurations proposed by the medical experts. The initialresults concerning to the internment conduct have beenpositive according to the expectancy of the experts. Thesuggestions of the experts involved in this project will beused to improve the mechanism and, in a second step, with aconsolidated model, the Expert System will be implementedin other public hospitals that deal with pediatric burned.
REFERENCES
[1] N. Kasabov, Foundations of Neural Networks, Fuzzy Systems, andKnowledge Engineering, Boston: Kluwer Academic, 1996.
[2] P. Jackson, Introduction to Expert Systems, 3rd ed., Harlow, England:Addison Wesley Longman, 1999.
[3] L. Rylah, Critical Care of the Burned Patient, London: CambridgeUniversity Press, 1992.
[4] L. Zadeh, "Fuzzy sets," Information and Control, vol. 8, 1965, pp.
338-359.[5] L. Zadeh, "The role of fuzzy logic in the management of uncertainty
in expert systems," Fuzzy Sets and Systems, vol. 11, 1983, pp. 199-227.
[6] G. Klir and B. Yuan, Fuzzy Sets and Fuzzy Logic: Theory andApplications, USA: Prentice Hall, 1995.
[7] D. L. Bisset, Anatomy and Biochemistry of the skin, in TransdermalDelivery of Drugs, vol.. 1, Kydonieus A. F. Eds. Boca Raton: CRCPress, 1987, pp. 29-42.
[8] J. A. Latarjet, "Simple Guide to Bum Treatment," Bums, vol. 21, no.3, 1995, pp. 221-225.
[9] E. D. Morgan et al., "Ambulatory management of bums," AmericanFamily Physician, vol. 62, no. 9, 2000.
[10] K. F. Muiri. and T. L. Barclay, Burns and their treatment, London:Lloyd Luke, 1974.
[11] D. N. Herndon, R. Rutan, "Management of the pediatric patient withbums," Journal ofBurn Care & Rehabilitation, vol. 14, 1993.
[12] J. A. Souza, "Analise de 573 Criancas com Queimaduras Internadasno Hospital Infantil Joana de Gusmao," Revista Brasileira deQueimaduras, 2001 (in Portuguese).
[13] R. R. Yager and D. P. Filev, Essentials of Fuzzy Modeling andControl, New York: John Wiley & Sons, 1994.
[14] D. B. Leake, Case-Based Reasoning: Experiences, Lessons, andFuture Directions, USA: AAAI Press, 1996.
447
TABLE IVCase Example
6 years Old,TSBA= 14,5 %Undefined and Partialthickness
Suclding = 0,38Child = I
PartialSmall = I
UndefinedSmall = 0,9Medium = 0.01