Embed Size (px)
Citation preview

1

I principali markers di sepsi e la loro importanza nella fase
diagnostico-terapeutica Alessandro Russo
Department of Public Health and Infectious Diseases
“Sapienza” University of Rome

Effect of timing on survival
Crit Care Med 2006;34:1589-96
Time from hypotension onset (hours)
Frac
tion
of t
otal
pat
ient
s
Emergency
0
5
10
15
20
25
30
35
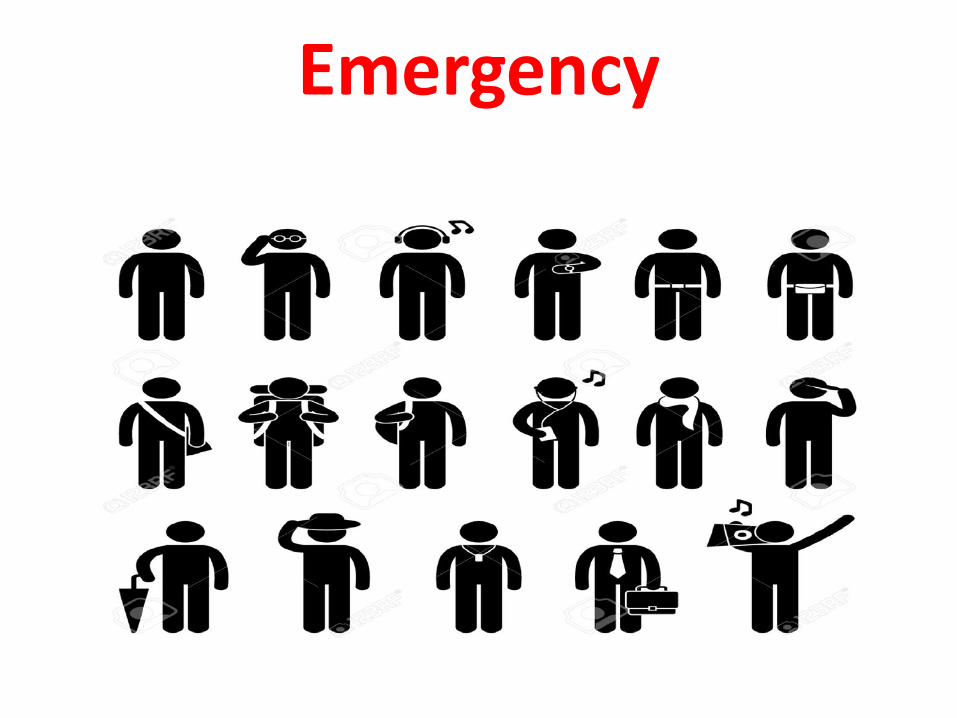
Possible sources of infection
Lung Intra- Genito- SSTI Bloodstream abdominal urinary
Crit Care Med. 2006;34:1589-96.

Positivity of blood cultures in different clinical syndromes
Endocarditis and bloodstream infections 85% - 95%
Bacteremic pneumonia 5% - 30%
Ascending Pyelonefritis 30% - 50%
Ematogenous osteomyelitis 30% - 50%
Bacterial Meningitis Variable
Intra-abdominal abscesses Variable
FUO Variable
Crit Care Med. 2006;34:1589-96.

Surviving sepsis campaign 3

10
Screening To identify patients at increased risk of adverse outcome to inform a prophylactic intervention or further diagnostic test Diagnosis To establish a diagnosis to inform a treatment decision and to do so more reliably, more rapidly, or more inexpensively than available methods Risk stratification To identify subgroups of patients within a particular diagnostic group who may experience greater benefit or harm with therapeutic intervention Monitoring To measure response to intervention to permit the titration of dose or duration of treatment Surrogate endpoint To provide a more sensitive measure of the consequences of treatment that can substitute for a direct measure of a patient-centered outcome
Uses of biomarkers

11

12 Ann Emerg Med. 2005; 45:524-28.

Algoritmo paziente infetto
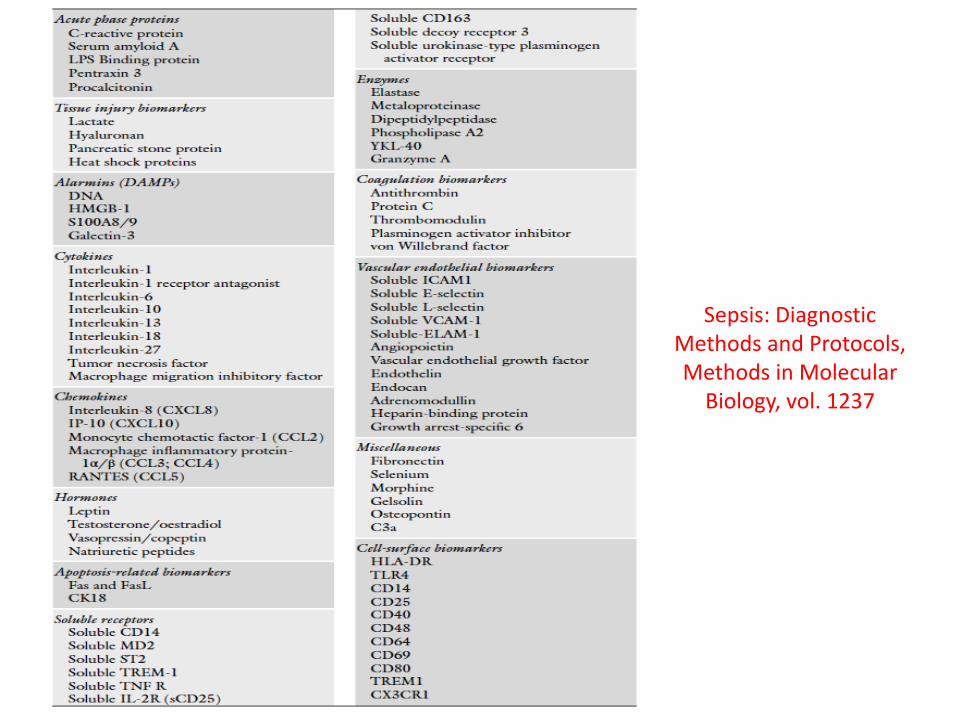
Sepsis: Diagnostic Methods and Protocols, Methods in Molecular
Biology, vol. 1237


16 Sepsis: Diagnostic Methods and Protocols, Methods in Molecular Biology, vol. 1237

17
• PCT levels accurately differentiate sepsis from noninfectious inflammation
Simon L. et al. Clin Infect Dis. 2004; 39:206-217.

SIGNIFICATO CLINICO DELLA PROCALCITONINA
BASSO RISCHIO DI PROGRESSIONE A SEPSI SEVERA E/O A SHOCK
SETTICO
POSSIBILE SEPSI
ELEVATO RISCHIO DI PROGRESSIONE A SEPSI SEVERA E/O A SHOCK
SETTICO

La cinetica della PCT mostra : 1.un aumento rispetto al valore basale dopo 3-6 ore dalla somministrazione di endotossina (o dell ’ invasione batterica)
2.un incremento significativo dopo circa 6 ore
3.il valore di picco viene raggiunto tre le 12 e le 48 ore
4.Ha un'emivita di 24 ore.
5.Cinetica migliore per descrivere l’evento infettivo rispetto alla PCR
CINETICA DELLA PROCALCITONINA

Zeni et al. Clin Intens Care 1994; 5: 2
I livelli di PCT sono progressivamente maggiori a seconda della severità della sepsi
I livelli di PCT correlano con il grado di insufficienza dorgano nei pazienti settici, valutato con il SOFA-score
Luzzani et al. Crit Care Med 2001; Vol.31 No.6
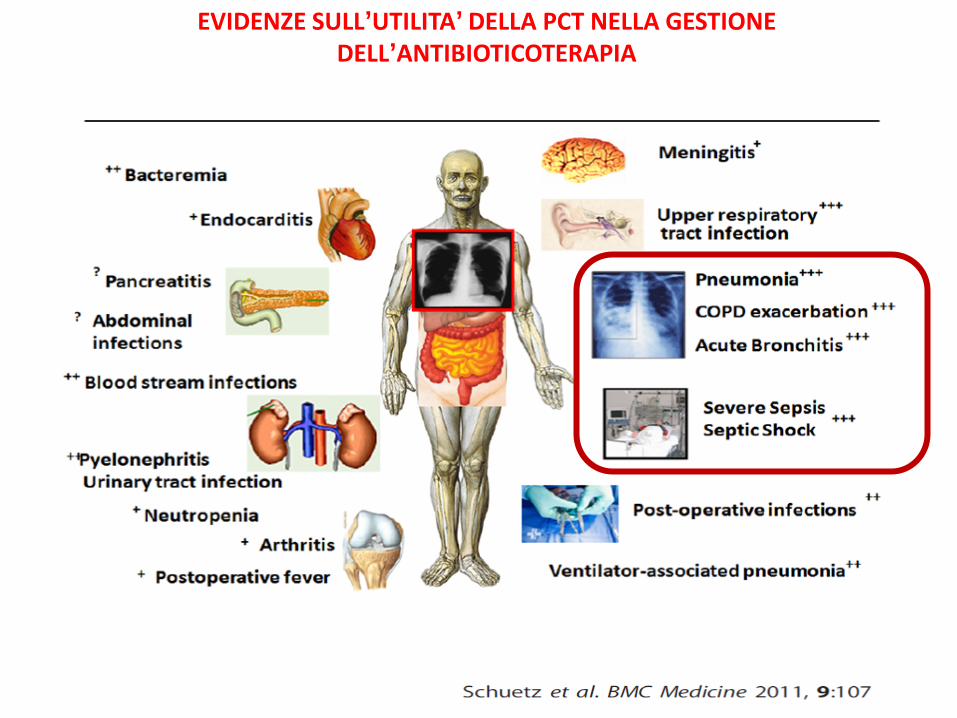
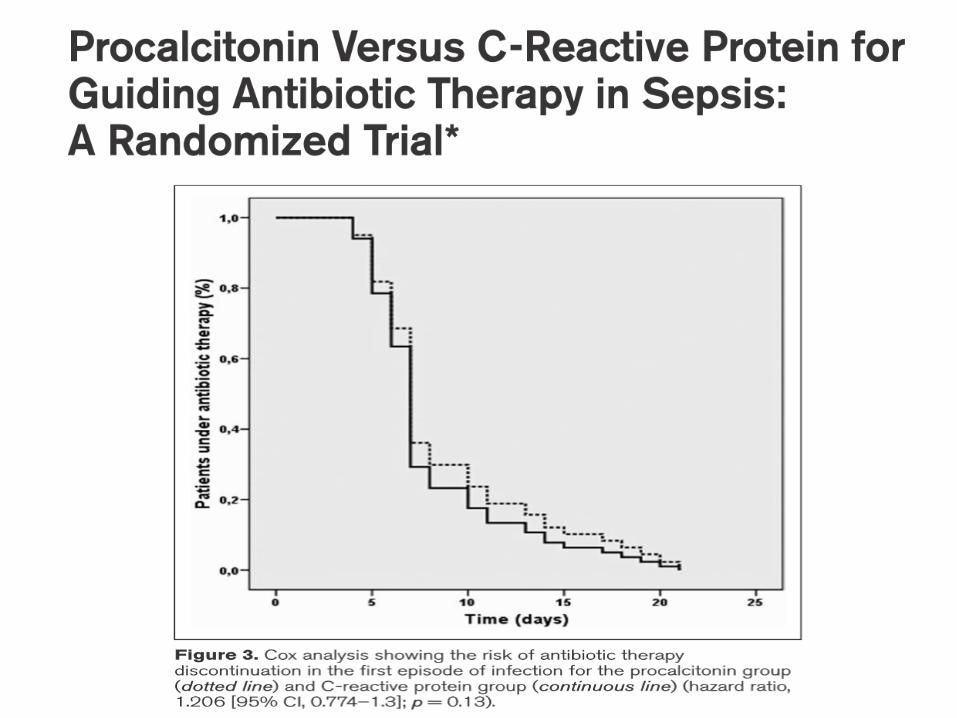
EVIDENZE SULL’UTILITA’ DELLA PCT NELLA GESTIONE DELL’ANTIBIOTICOTERAPIA

Procalcitonin in septic shock
Muller and Trampuz. Int J Antimicrob Agents 2007; 30 Suppl 1: S16-23

IL SETTING CLINICO INFLUISCE SUI “VALORI NORMALI” DELLA PCT
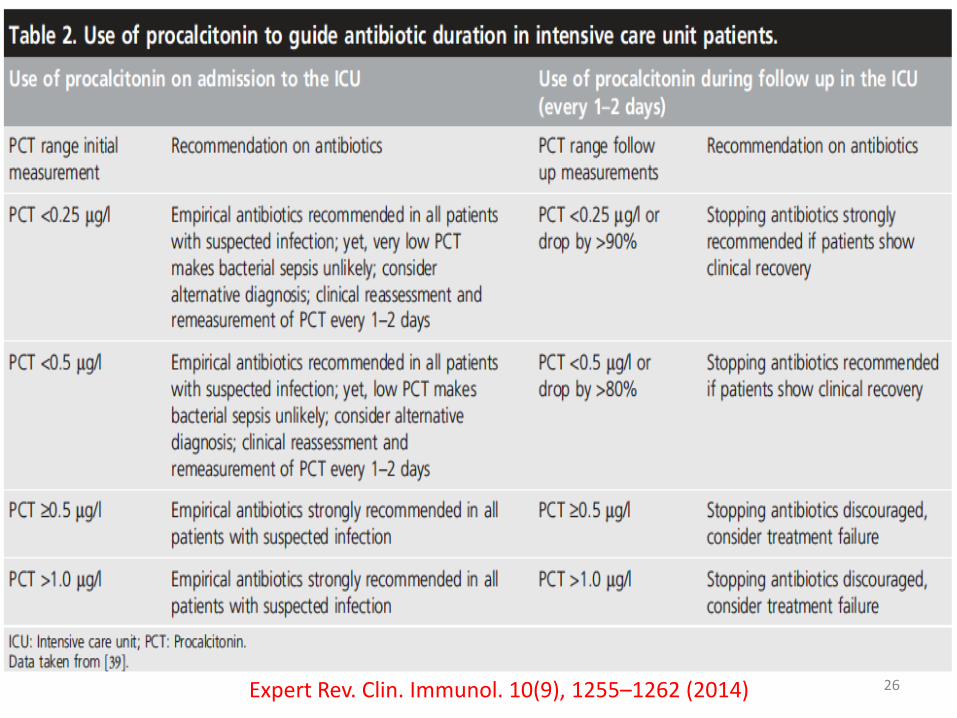
26 Expert Rev. Clin. Immunol. 10(9), 1255–1262 (2014)

Lancet Infect Dis 2016; 16:819-27

Conditions causing elevation of C-reactive protein
• Bacterial infections • Hypersensitivity complications of infections • Inflammatory diseases • Transplantation • Cancer • Necrosis • Trauma • Burns • Fractures
29
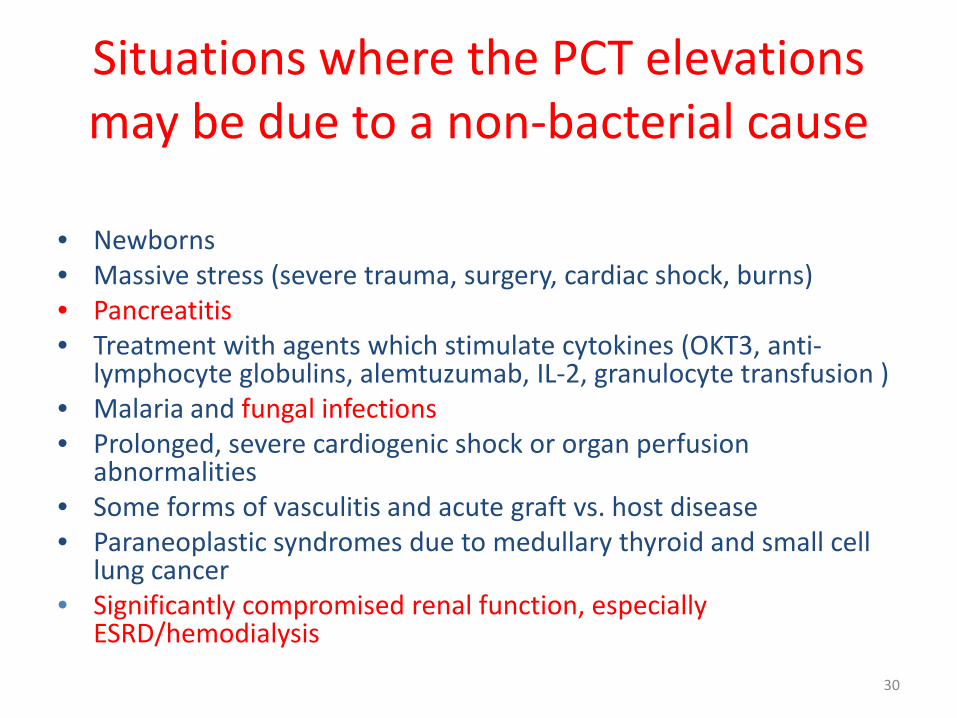
Situations where the PCT elevations may be due to a non-bacterial cause
• Newborns • Massive stress (severe trauma, surgery, cardiac shock, burns) • Pancreatitis • Treatment with agents which stimulate cytokines (OKT3, anti-
lymphocyte globulins, alemtuzumab, IL-2, granulocyte transfusion ) • Malaria and fungal infections • Prolonged, severe cardiogenic shock or organ perfusion
abnormalities • Some forms of vasculitis and acute graft vs. host disease • Paraneoplastic syndromes due to medullary thyroid and small cell
lung cancer • Significantly compromised renal function, especially
ESRD/hemodialysis
30

Serum procalcitonin measurement contribution to the early diagnosis of candidemia in critically ill patients
Charles E et al Intensive Care Med (2006) 32:1577–1583

Early diagnosis of candidemia in ICU patients with sepsis: a prospective comparison of (1®3)-b-D-glucan assay, Candida score, and colonization index
Posteraro B, Antonelli M, Tumbarello M, ..& Sanguinetti M Crit Care Med, 2012
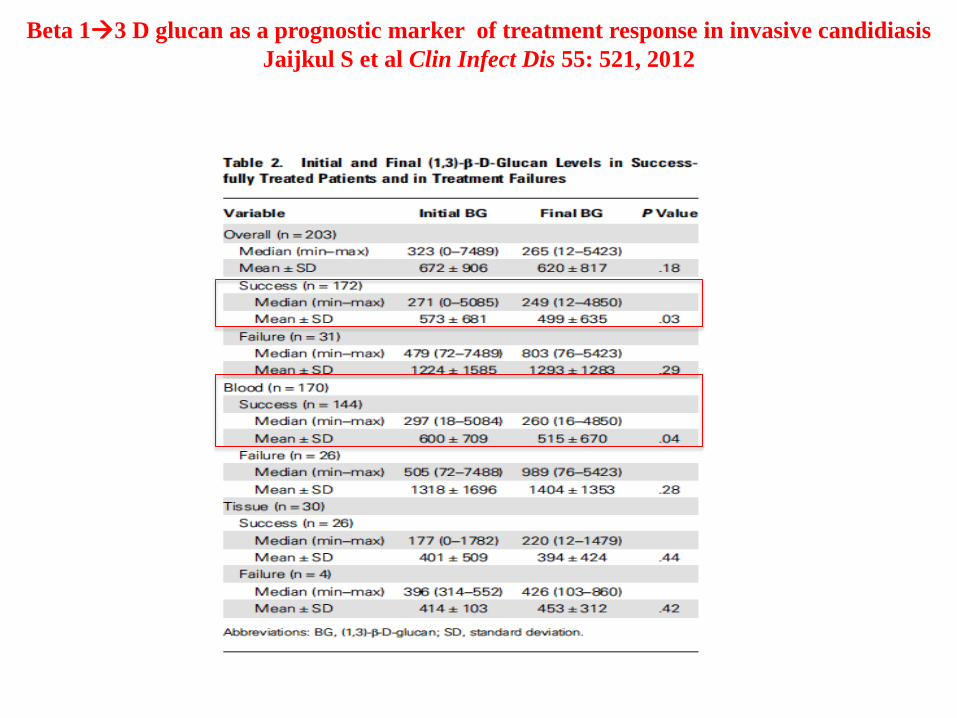
Beta 13 D glucan as a prognostic marker of treatment response in invasive candidiasis Jaijkul S et al Clin Infect Dis 55: 521, 2012

Un possibile approccio pre-emptive nel paziente critico
• BDG>250 pg/uL inizia echinocandina
• BDG <200 - >80 pg/uL Candida score>=3 inizia echinocandina

BioMed Research International Volume 2014, Article ID 985813, 10 pages

Platelet Activation Is Associated With Myocardial Infarction in Patients With Pneumonia
Cangemi, R., et al., J Am Coll Cardiol. 2014; 64(18):1917–25.
Potential Mechanisms for Platelet Activation During Severe Pneumonia

37 Expert Rev. Clin. Immunol. 10(9), 1255–1262 (2014)

PRESEPSIN AS A POTENTIAL USEFUL MARKER TO PREDICT A BACTERIAL INFECTION RELAPSE IN CRITICAL CARE UNIT PATIENTS. PRELIMINARY STUDY
Sargentini V, Ceccarelli G, Morelli A, Venditti M & Bachettoni A et Clin Chem Lab Med. 2014
38
Clinical course of Presepsin and Procalcitonin in a septic patient
39
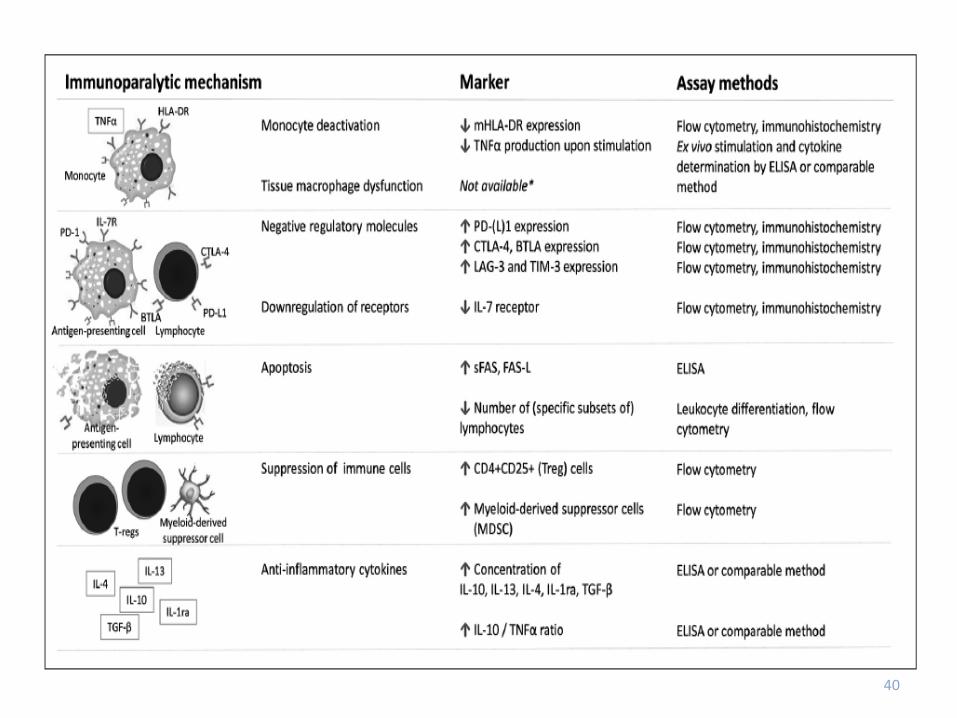
40

41

42 Trends Mol Med. 2009 March ; 15(3): 129
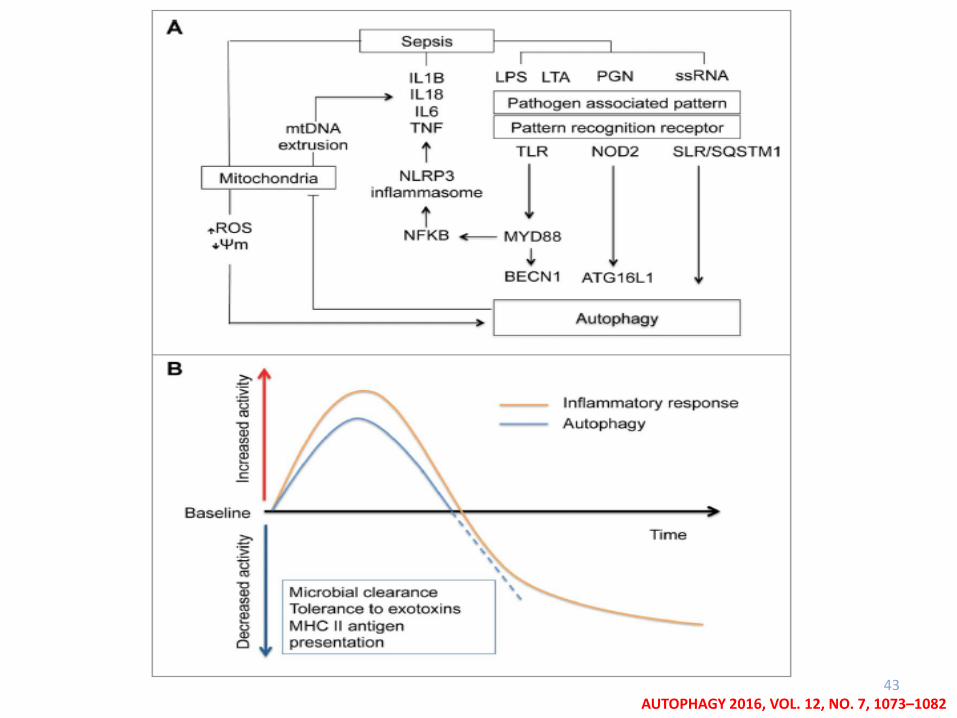
43 AUTOPHAGY 2016, VOL. 12, NO. 7, 1073–1082

44
How to manage septic shock? • Every medical therapy has potential adverse effects, and selection of patients most likely to
benefit is crucial, making more personalized approaches necessary.
• Immune biomarkers measured on admission and during follow-up can guide/support the clinician’s early recognition of sepsis, severity assessment and therapeutic decisions in individual patients.
• Biomarkers may allow transition from generalizing sepsis care bundles to a more tailored management in individual patients thereby reducing the risk for adverse treatment outcomes in patients who – based on their biomarker levels – do not likely benefit from therapy.
• Lactate improves initial risk stratification and prompts early fluid resuscitation. Lactate clearance may be used for assessing a patient’s response to fluids.
• Procalcitonin facilitates assessment of bacterial infection risk. Procalcitonin algorithms for guiding therapeutic decisions about initiation and duration of antimicrobial therapy have shown strong effects in regard to lower antibiotic consumption and appear to be safe regarding the results from interventional trials.
• Proadrenomedullin is an inflammatory prognostic immune marker that improves early mortality prediction and might improve site-of care decisions in patients with respiratory infections.
• Autophagy and “precisione medicine” are the new frontiers?