Embed Size (px)
Citation preview

Maria Grazia Bongiorni,Direttore UOC Cardiologia 2
Azienda Ospedaliero –Universitaria - Pisa
Principali complessità cliniche e gestionali dell’estrazione di elettrocateteri
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
The need for lead extraction is rapidly increasing due to:
�New indication for device treatment
�Higher lead prevalence due to increased life expectancy
�CIED modes requiring more leads for patient
�Upgrading from device systems becoming more frequent
�Lead Recalls and malfunctions
�Lead Infections
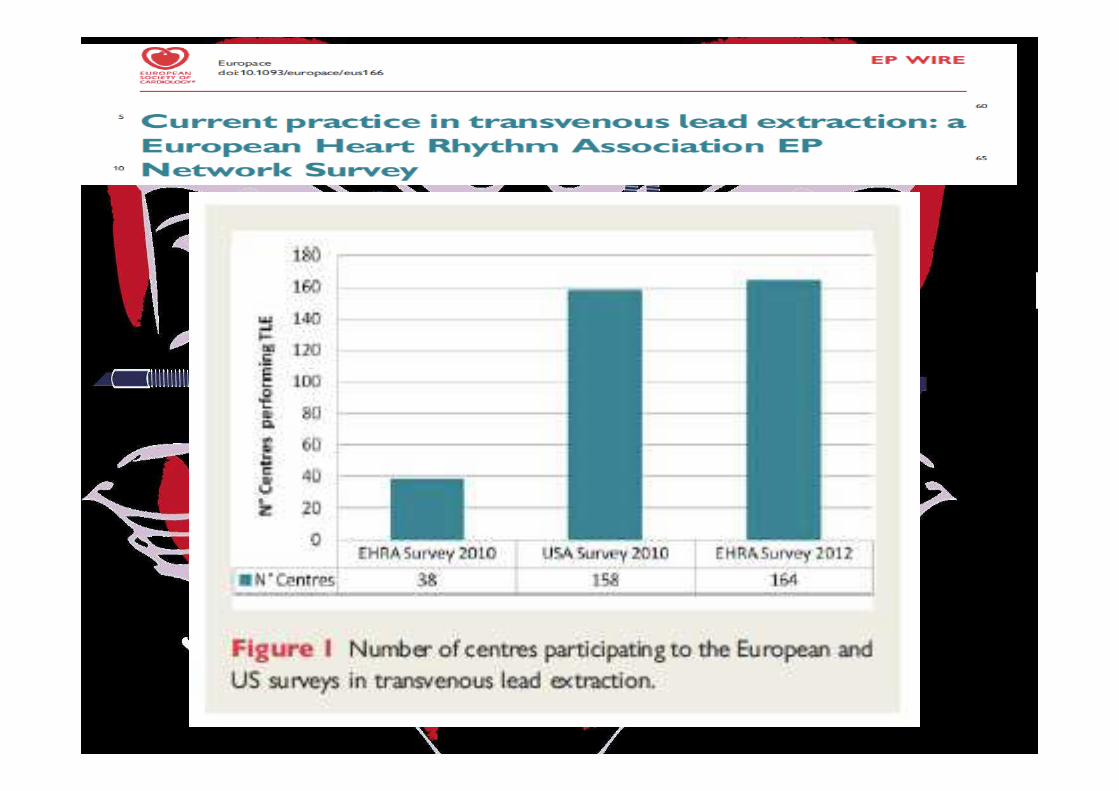
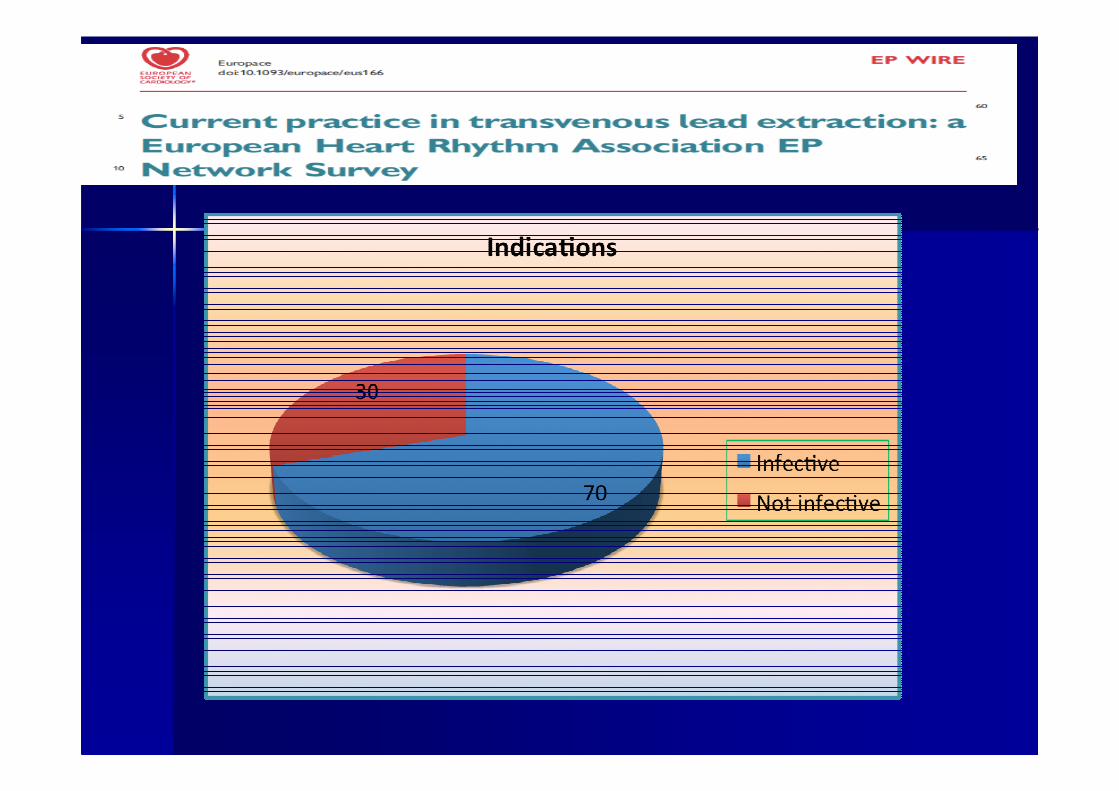
Indications for lead ExtractionIndications for lead Extraction
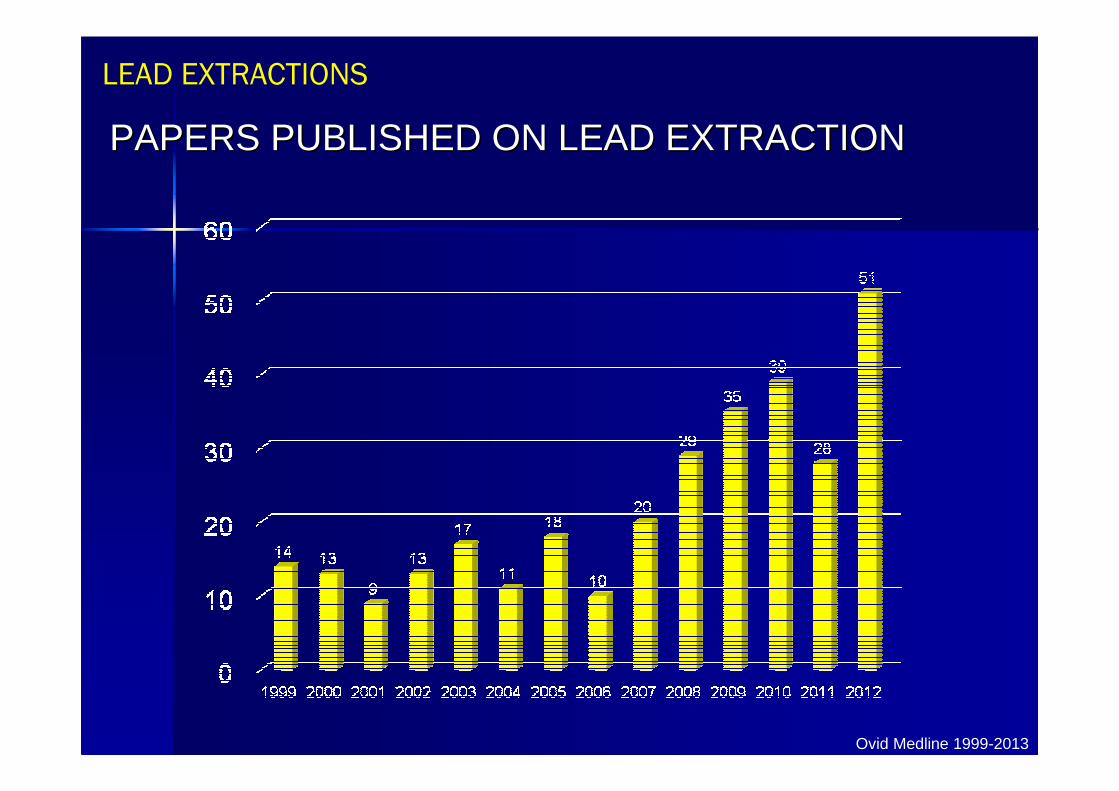
PAPERS PUBLISHED ON LEAD EXTRACTIONPAPERS PUBLISHED ON LEAD EXTRACTIONPAPERS PUBLISHED ON LEAD EXTRACTION
Ovid Medline 1999-2013
LEAD EXTRACTIONSLEAD EXTRACTIONS
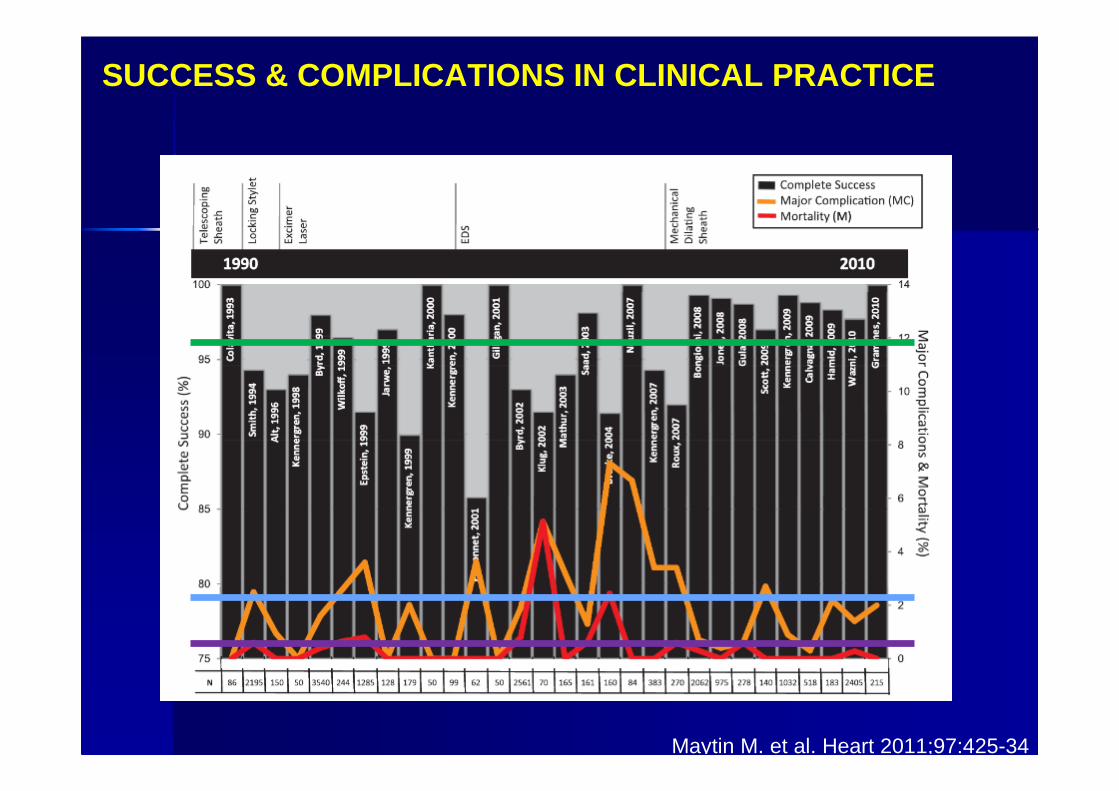
SUCCESS & COMPLICATIONS IN CLINICAL PRACTICESUCCESS & COMPLICATIONS IN CLINICAL PRACTICE
Maytin M. et al. Heart 2011;97:425-34
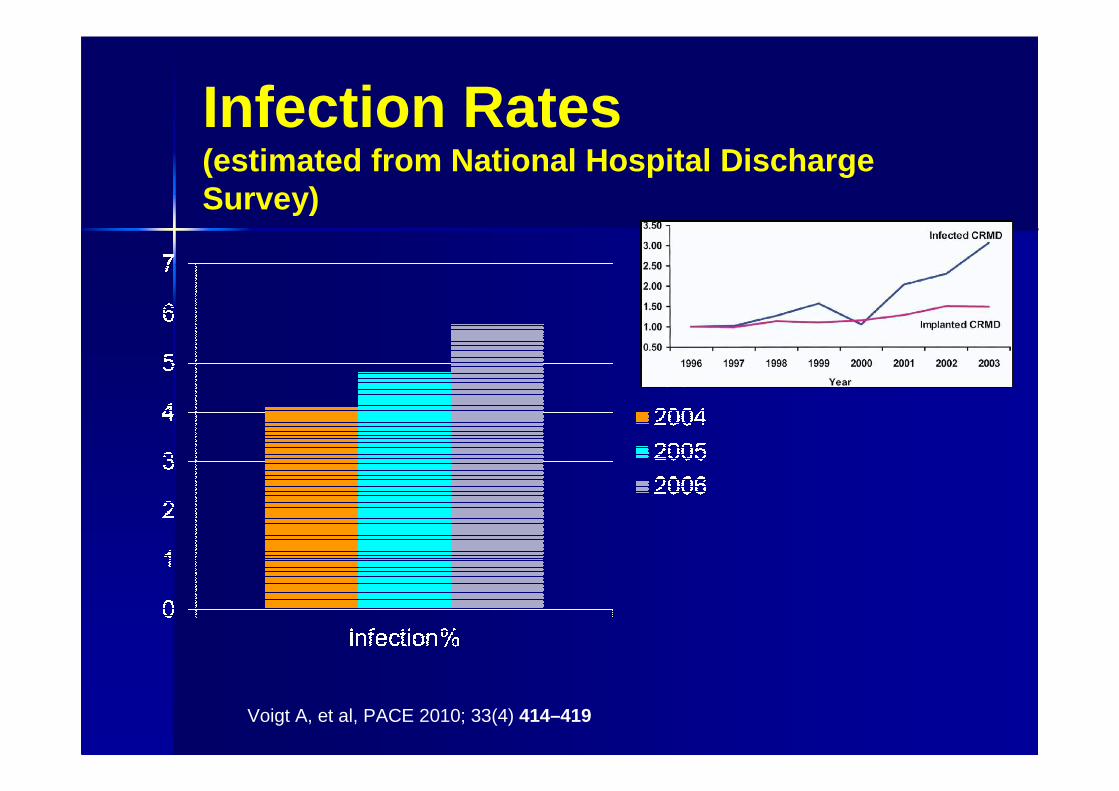
Infection Rates(estimated from National Hospital Discharge Survey)
Voigt A, et al, PACE 2010; 33(4) 414–419
Why?
� Patients with more co-morbidities– “Sicker Patients”
� Larger Devices– More ICDs
� Longer implant time– Less experienced implanters
– More complex devices
� “Cathlab sterile technique”
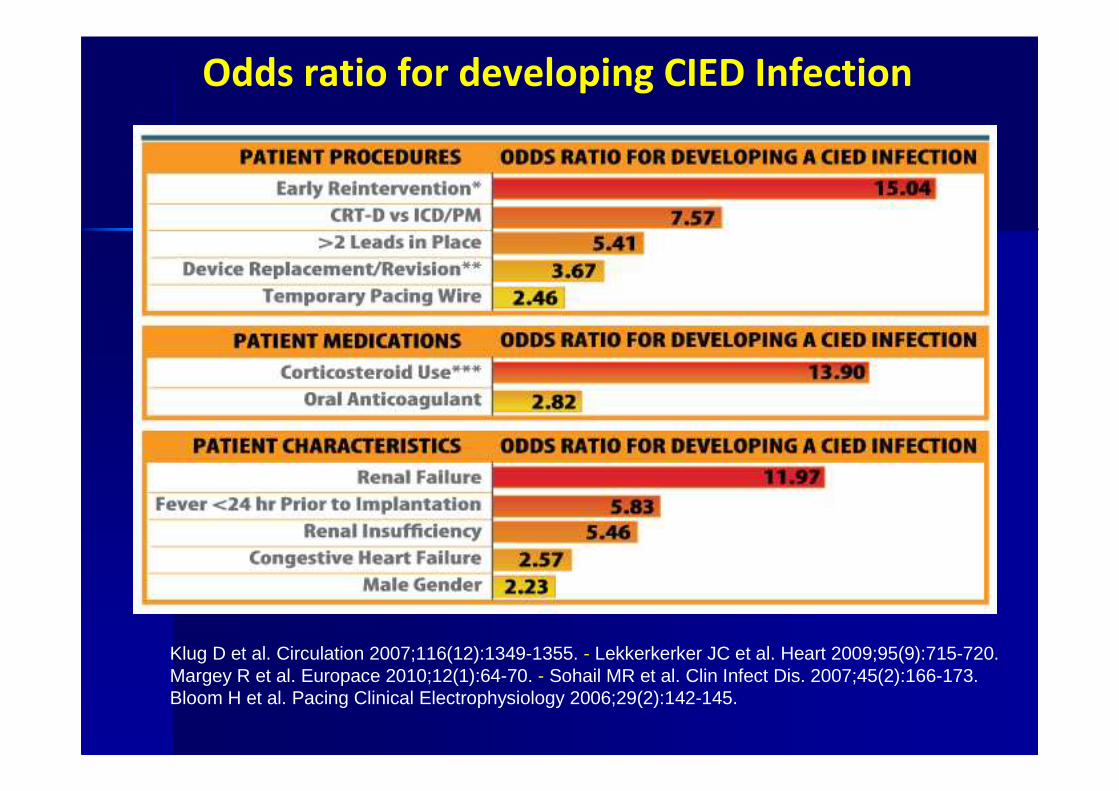
Odds ratio for developing CIED Infection
Klug D et al. Circulation 2007;116(12):1349-1355. - Lekkerkerker JC et al. Heart 2009;95(9):715-720.Margey R et al. Europace 2010;12(1):64-70. - Sohail MR et al. Clin Infect Dis. 2007;45(2):166-173.Bloom H et al. Pacing Clinical Electrophysiology 2006;29(2):142-145.
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
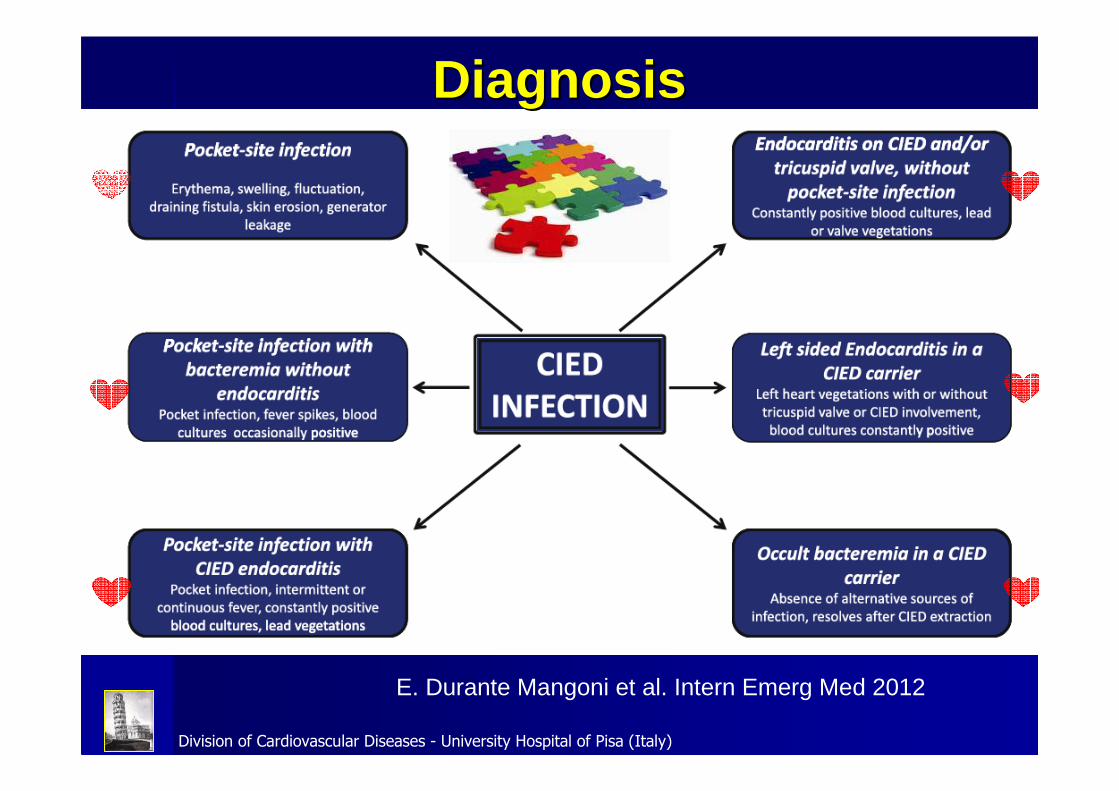
E. Durante Mangoni et al. Intern Emerg Med 2012
Diagnosis Diagnosis
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
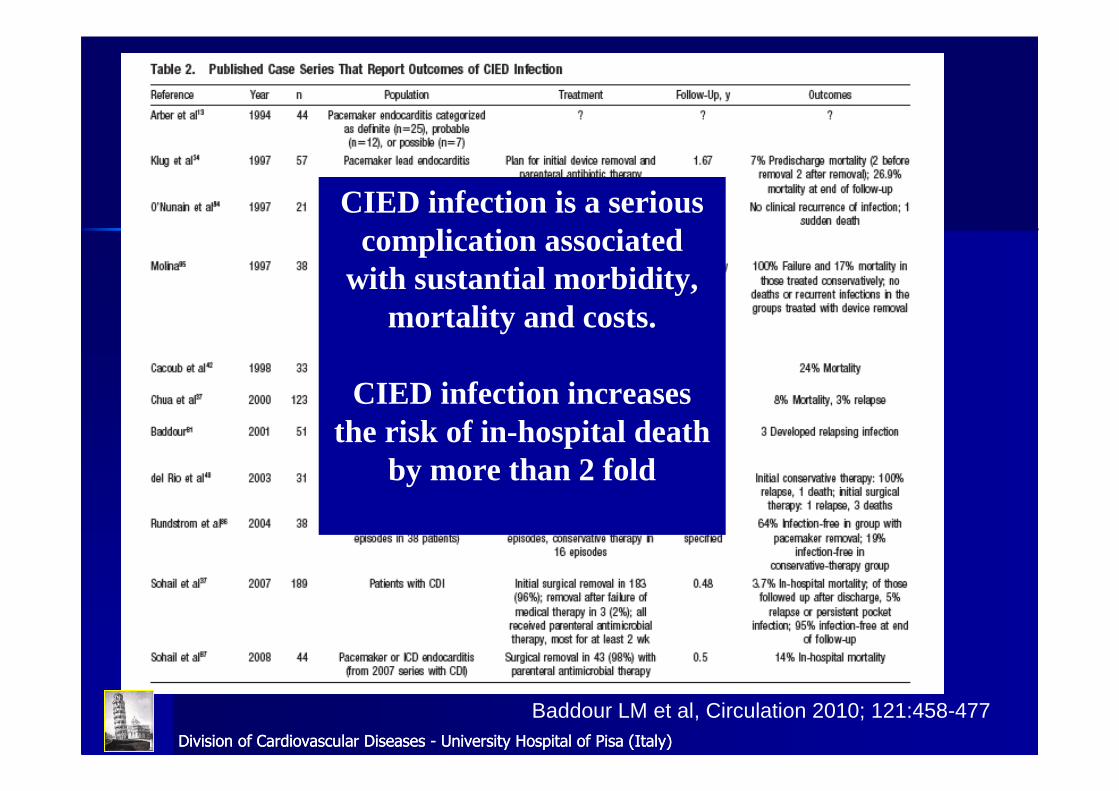
CIED infection is a serious complication associated
with sustantial morbidity, mortality and costs.
CIED infection increases the risk of in-hospital death
by more than 2 fold
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
Baddour LM et al, Circulation 2010; 121:458-477
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
THERAPYTHERAPY
Transvenous Lead Extraction
Although clinical presentation might be different, the management of both pocket infection or systemic infection is very similar and involves complete
system removal and antibiotic therapy. The type of infection might affect the duration of antibiotic therapy and the
decision for timing and type of reimplant.
Antibiotic Therapy
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
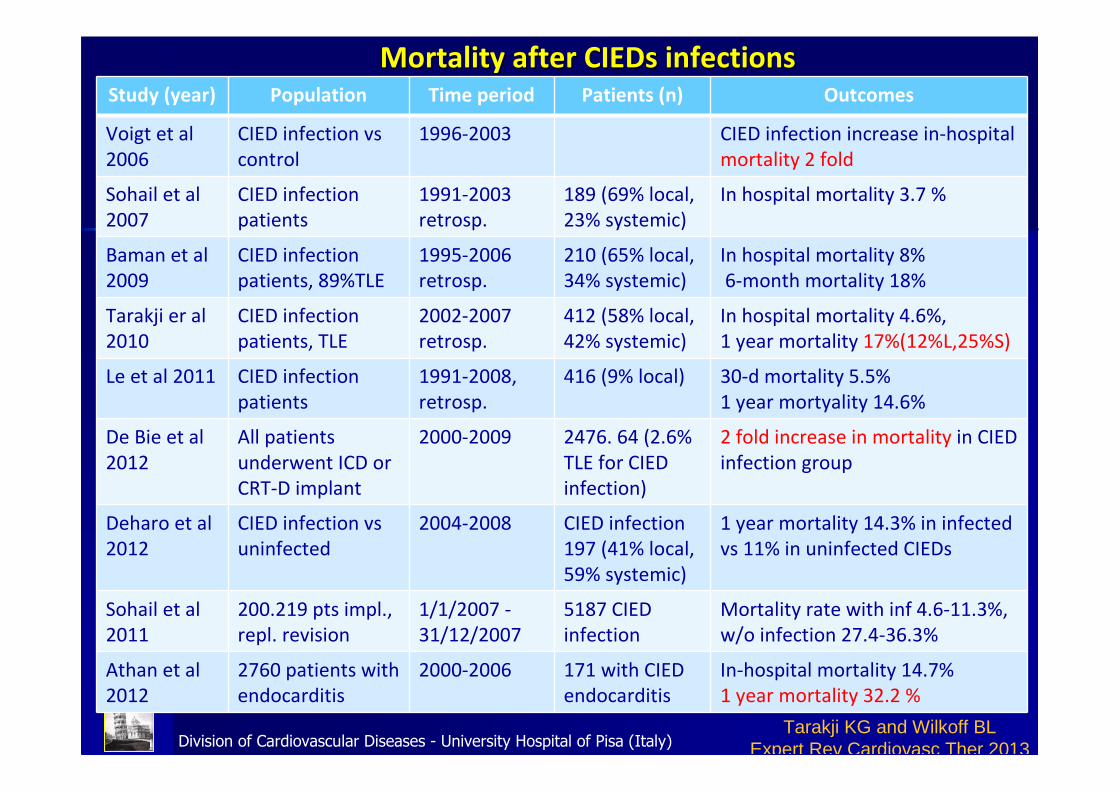
Mortality after CIEDs infectionsMortality after CIEDs infectionsStudy (year) Population Time period Patients (n) Outcomes
Voigt et al
2006
CIED infection vs
control
1996-2003 CIED infection increase in-hospital
mortality 2 fold
Sohail et al
2007
CIED infection
patients
1991-2003
retrosp.
189 (69% local,
23% systemic)
In hospital mortality 3.7 %
Baman et al
2009
CIED infection
patients, 89%TLE
1995-2006
retrosp.
210 (65% local,
34% systemic)
In hospital mortality 8%
6-month mortality 18%
Tarakji er al
2010
CIED infection
patients, TLE
2002-2007
retrosp.
412 (58% local,
42% systemic)
In hospital mortality 4.6%,
1 year mortality 17%(12%L,25%S)
Le et al 2011 CIED infection
patients
1991-2008,
retrosp.
416 (9% local) 30-d mortality 5.5%
1 year mortyality 14.6%
De Bie et al
2012
All patients
underwent ICD or
CRT-D implant
2000-2009 2476. 64 (2.6%
TLE for CIED
infection)
2 fold increase in mortality in CIED
infection group
Deharo et al
2012
CIED infection vs
uninfected
2004-2008 CIED infection
197 (41% local,
59% systemic)
1 year mortality 14.3% in infected
vs 11% in uninfected CIEDs
Sohail et al
2011
200.219 pts impl.,
repl. revision
1/1/2007 -
31/12/2007
5187 CIED
infection
Mortality rate with inf 4.6-11.3%,
w/o infection 27.4-36.3%
Athan et al
2012
2760 patients with
endocarditis
2000-2006 171 with CIED
endocarditis
In-hospital mortality 14.7%
1 year mortality 32.2 %
Tarakji KG and Wilkoff BL Expert Rev Cardiovasc Ther 2013
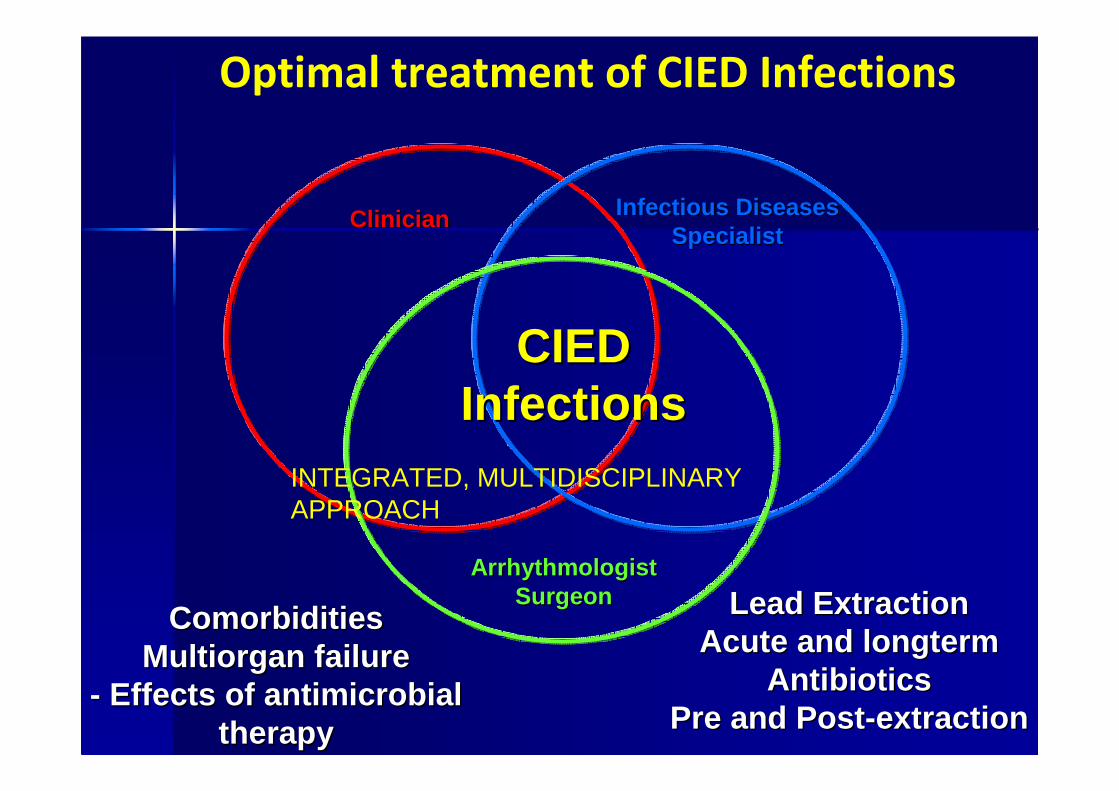
Optimal treatment of CIED Infections
ClinicianClinician Infectious DiseasesInfectious DiseasesSpecialistSpecialist
ArrhythmologistArrhythmologistSurgeonSurgeon
CIEDCIEDInfectionsInfections
ComorbiditiesComorbiditiesMultiorgan failureMultiorgan failure
-- Effects of antimicrobial Effects of antimicrobial therapytherapy
Lead ExtractionLead ExtractionAcute and longtermAcute and longterm
AntibioticsAntibioticsPre and PostPre and Post --extractionextraction
INTEGRATED, MULTIDISCIPLINARY APPROACH
Lead extractionLead extraction
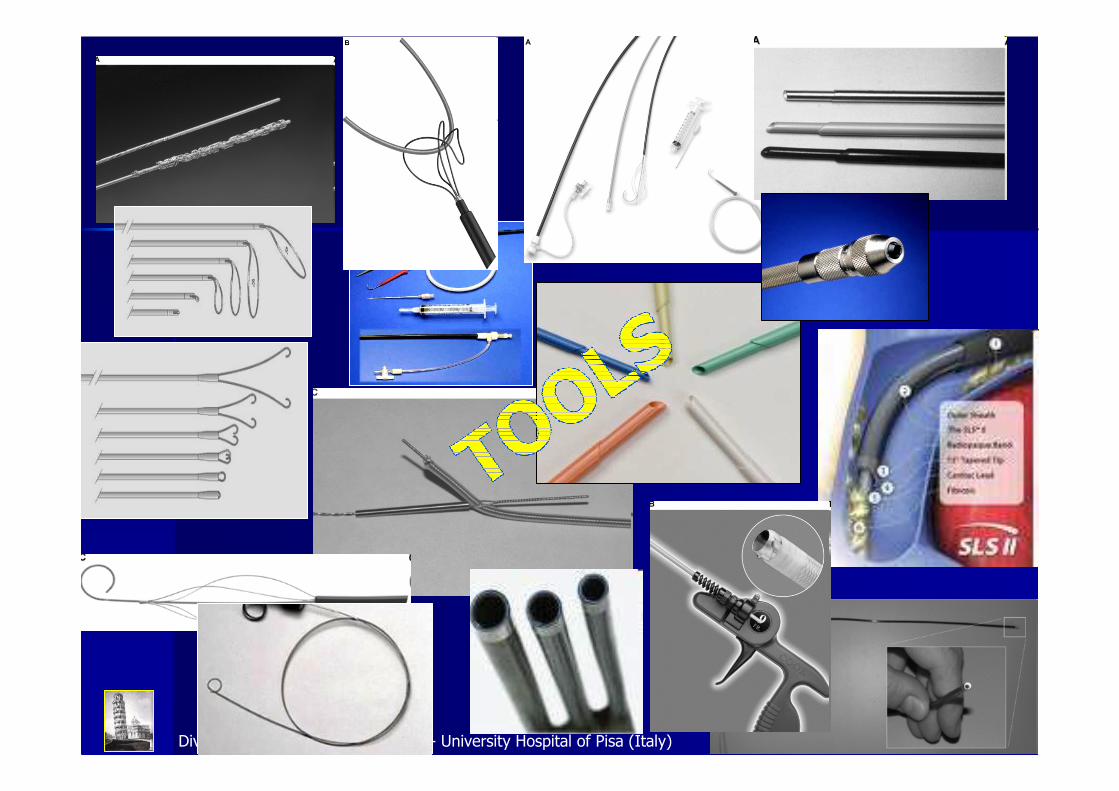
TOOLS TOOLS
TECHNIQUES TECHNIQUES
VENOUS APPROACHESVENOUS APPROACHES
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
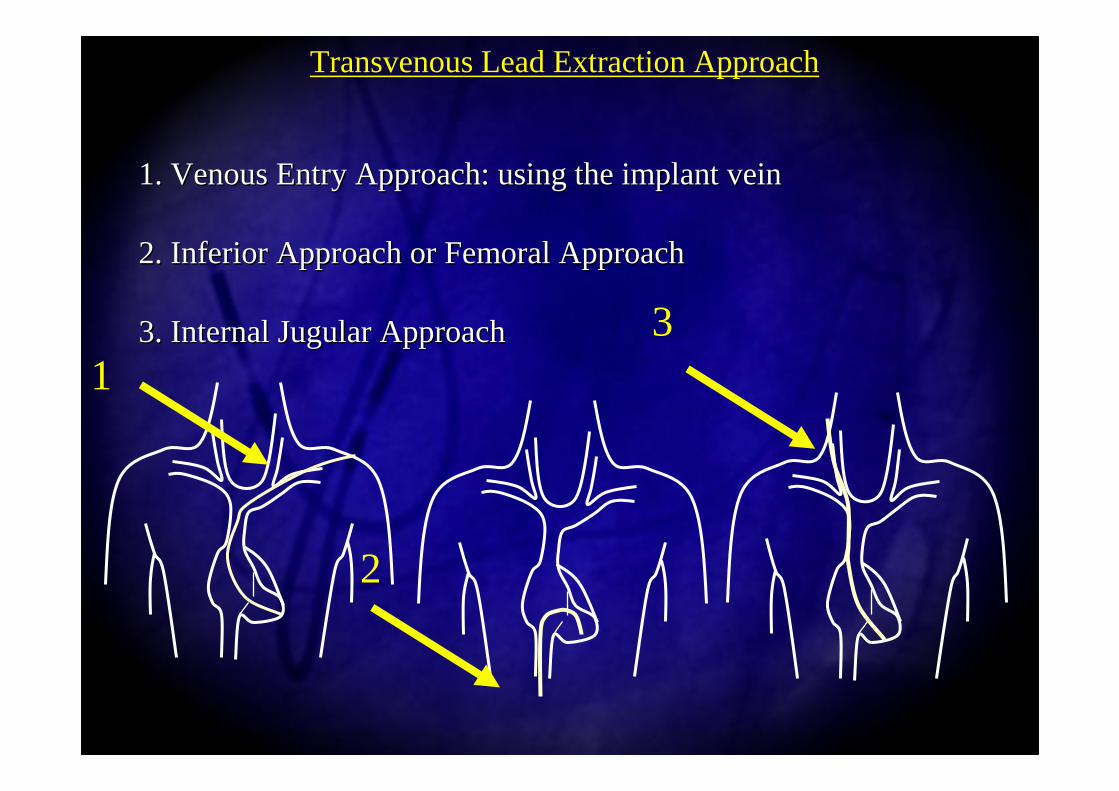
1. Venous Entry Approach: using the implant vein1. Venous Entry Approach: using the implant vein
2. Inferior Approach or Femoral Approach2. Inferior Approach or Femoral Approach
3. Internal Jugular Approach 3. Internal Jugular Approach
Transvenous Lead Extraction Approach
13
2
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
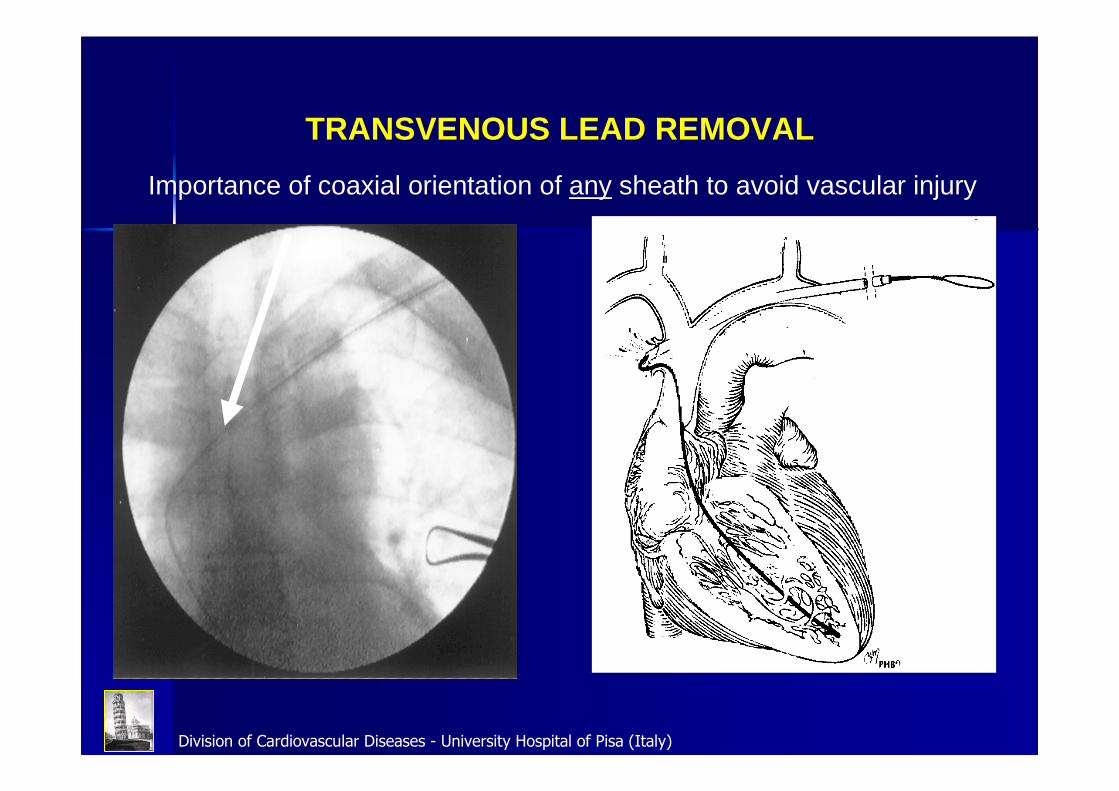
Importance of coaxial orientation of any sheath to avoid vascular injury
TRANSVENOUS LEAD REMOVAL
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
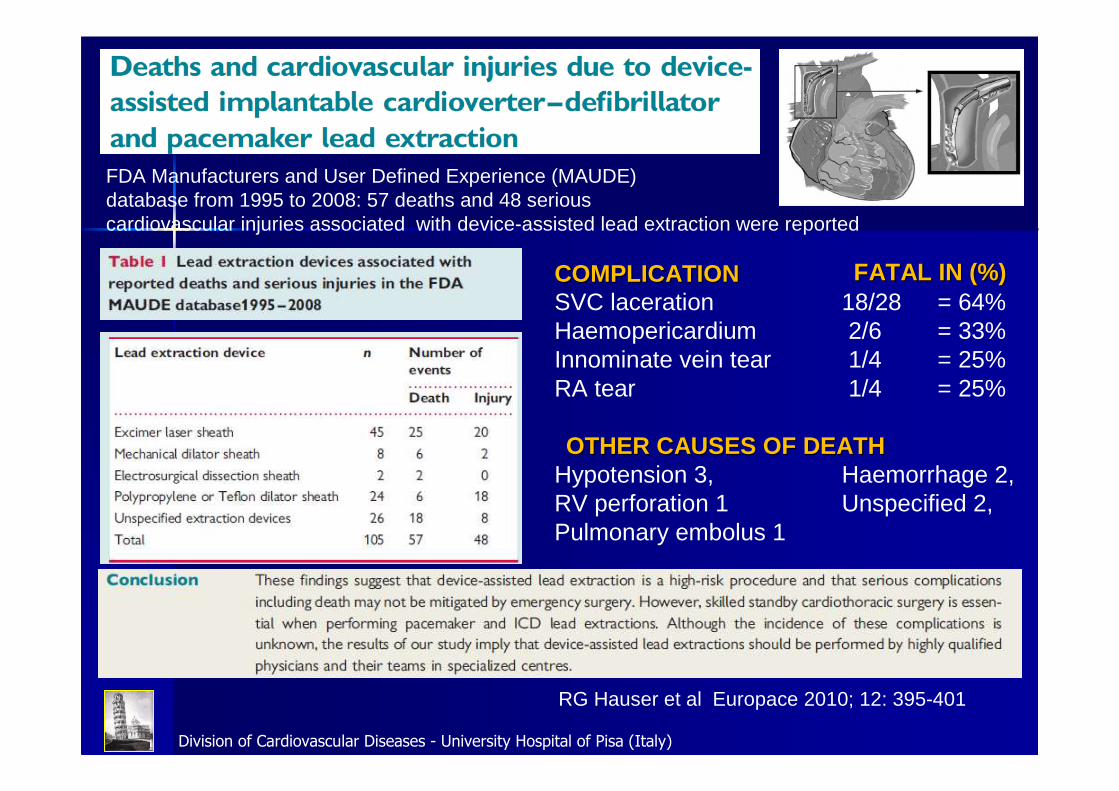
RG Hauser et al Europace 2010; 12: 395-401
SVC laceration 18/28 = 64%Haemopericardium 2/6 = 33%Innominate vein tear 1/4 = 25%RA tear 1/4 = 25%
Hypotension 3, Haemorrhage 2, RV perforation 1 Unspecified 2,Pulmonary embolus 1
FATAL IN (%)FATAL IN (%)COMPLICATIONCOMPLICATION
OTHER CAUSES OF DEATHOTHER CAUSES OF DEATH
FDA Manufacturers and User Defined Experience (MAUDE)database from 1995 to 2008: 57 deaths and 48 serious cardiovascular injuries associated with device-assisted lead extraction were reported
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
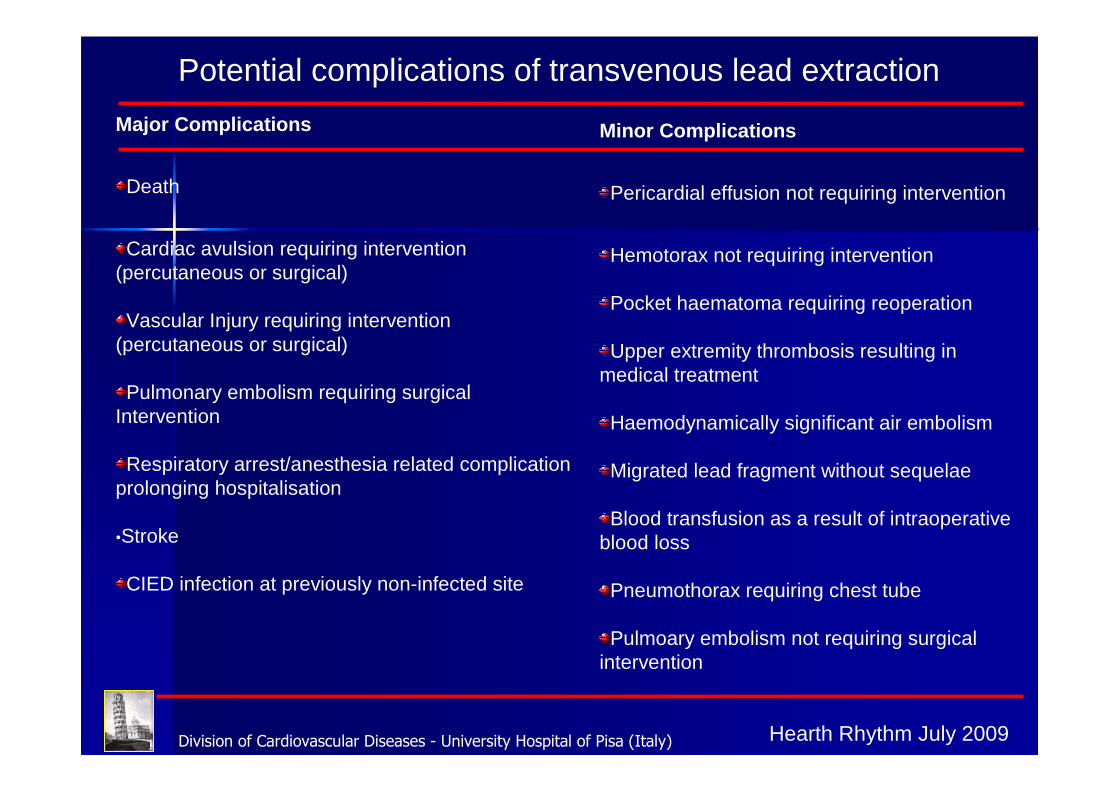
Major Complications
Death
Cardiac avulsion requiring intervention(percutaneous or surgical)
Vascular Injury requiring intervention(percutaneous or surgical)
Pulmonary embolism requiring surgicalIntervention
Respiratory arrest/anesthesia related complicationprolonging hospitalisation
•Stroke
CIED infection at previously non-infected site
Minor Complications
Pericardial effusion not requiring intervention
Hemotorax not requiring intervention
Pocket haematoma requiring reoperation
Upper extremity thrombosis resulting inmedical treatment
Haemodynamically significant air embolism
Migrated lead fragment without sequelae
Blood transfusion as a result of intraoperativeblood loss
Pneumothorax requiring chest tube
Pulmoary embolism not requiring surgicalintervention
Potential complications of transvenous lead extraction
Hearth Rhythm July 2009
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
Factors affecting outcomeFactors affecting outcome
PATIENT-RELATED- Gender, Age, BMI
- Comorbidities
- Infections
- Diabetes
- Renal Failure
LEAD-RELATED- Type , Number and position
- Dwelling time
- Lead damage
TEAM-RELATED- Experience and Volume
- Staff training
- Surgical back-up
TOOLS-TECHNIQUES AND APPROACHES RELATED- Tools
- Techniques
- Venous Approaches

Division of Cardiovascular Diseases - University Hospital of Pisa (Italy) EHRA position paper 2012
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
EXTRACTION - REQUIREMENTSEXTRACTION - REQUIREMENTS
PERSONNELPERSONNELPERSONNEL
HRS Expert Consensus 2009, EHRA position paper 2012
1. PRIMARY OPERATOR
2. CARDIOSURGEON (IF NOT A PRIMARY OPERATOR), TRAINED TO FIX ACUTE COMPLICATIONS
3. ANESTESIOLOGIST
4. „SCRUBBED” ASSISTANT
5. „NON-SCRUBBED” ASSISTANT
6. TECHNICIAN – FLUOROSCOPIC EQUIPMENT
7. ECHOCARDIOGRAPHER
1. PRIMARY OPERATOR
2. CARDIOSURGEON (IF NOT A PRIMARY OPERATOR), TRAINED TO FIX ACUTE COMPLICATIONS
3. ANESTESIOLOGIST
4. „SCRUBBED” ASSISTANT
5. „NON-SCRUBBED” ASSISTANT
6. TECHNICIAN – FLUOROSCOPIC EQUIPMENT
7. ECHOCARDIOGRAPHER
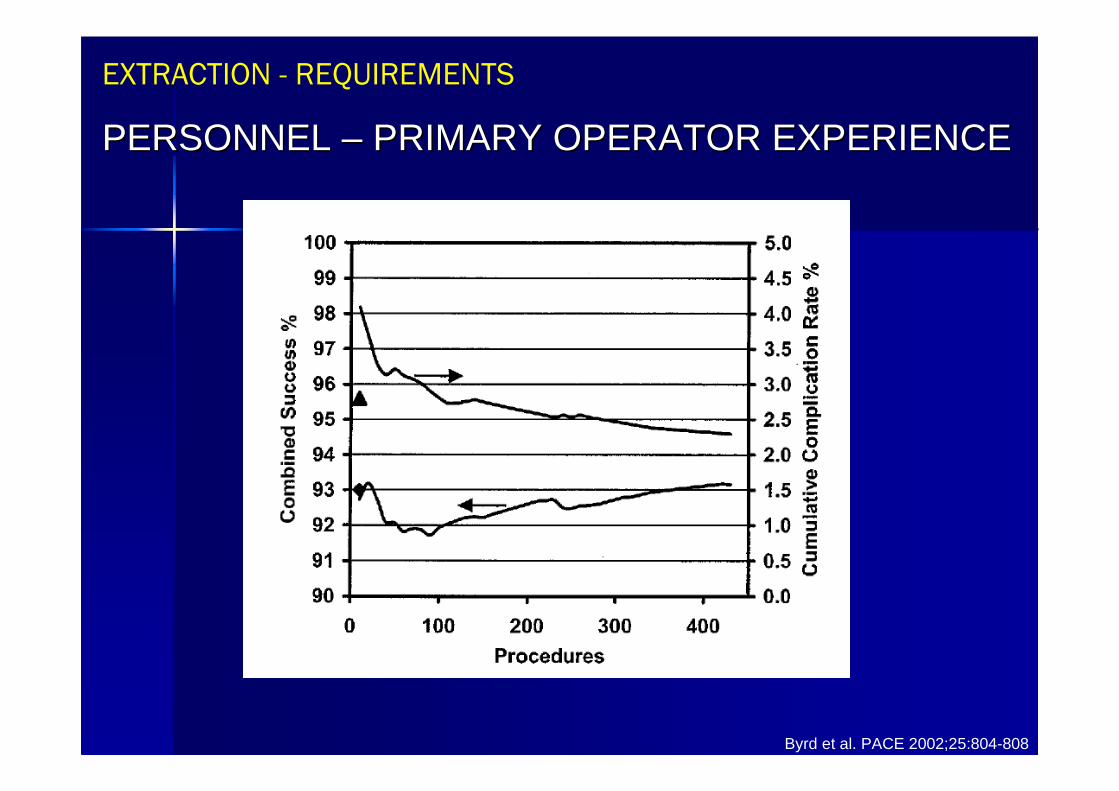
Byrd et al. PACE 2002;25:804-808
EXTRACTION - REQUIREMENTSEXTRACTION - REQUIREMENTS
PERSONNEL – PRIMARY OPERATOR EXPERIENCEPERSONNEL PERSONNEL –– PRIMARY OPERATOR EXPERIENCEPRIMARY OPERATOR EXPERIENCE
HRS Expert Consensus 2009, EHRA position paper 2012
CARDIOTHORACIC SURGEON:
• IMMEDIATELY AVAILABLE
• IS AWARE OF PROCEDURE
• ABLE TO MANAGE LIFE-THREATENING COMPLICATIONS
CARDIOTHORACIC SURGEON:
• IMMEDIATELY AVAILABLE
• IS AWARE OF PROCEDURE
• ABLE TO MANAGE LIFE-THREATENING COMPLICATIONS
EXTRACTION - REQUIREMENTSEXTRACTION - REQUIREMENTS
PERSONNELPERSONNELPERSONNEL
SUCCESS & COMPLICATIONS IN CLINICAL PRACTICESUCCESS & COMPLICATIONS IN CLINICAL PRACTICE
Hauser R.G. et al. Europace 2010;12:395-401
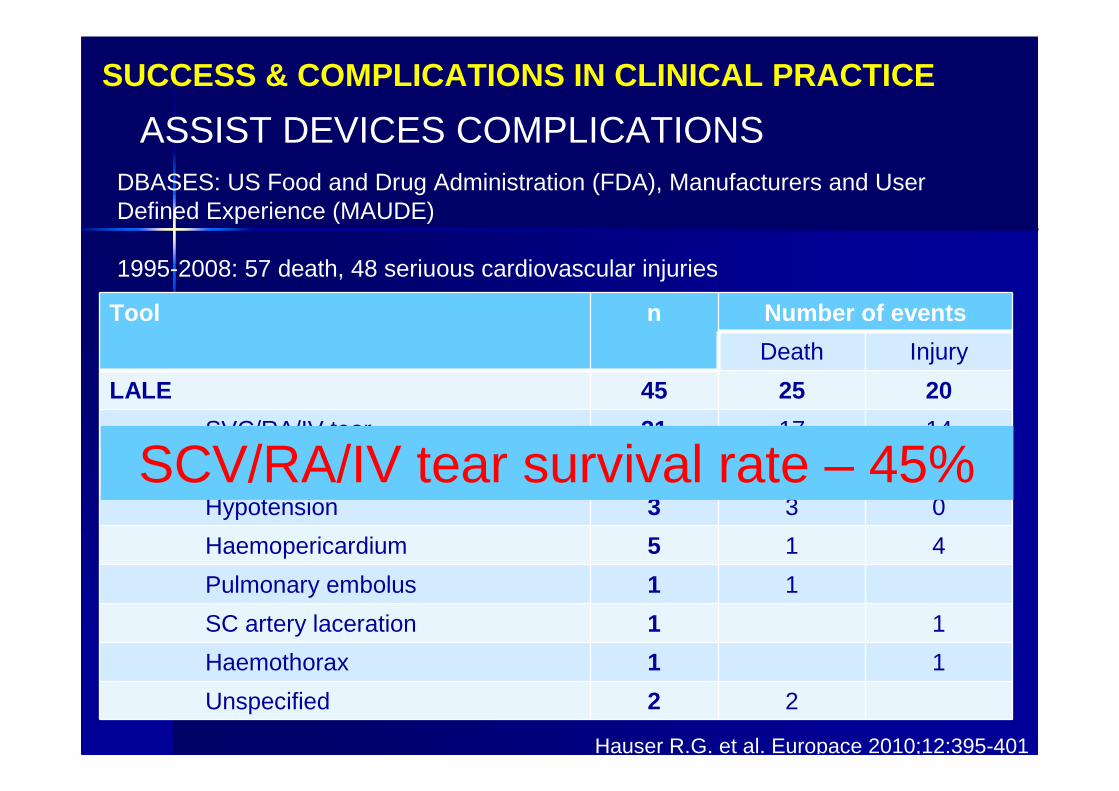
ASSIST DEVICES COMPLICATIONSASSIST DEVICES COMPLICATIONSDBASES: US Food and Drug Administration (FDA), Manufacturers and User Defined Experience (MAUDE)
1995-2008: 57 death, 48 seriuous cardiovascular injuries
Tool n Number of events
Death Injury
LALE 45 25 20
SVC/RA/IV tear 31 17 14
RV perforation 1 1 0
Hypotension 3 3 0
Haemopericardium 5 1 4
Pulmonary embolus 1 1
SC artery laceration 1 1
Haemothorax 1 1
Unspecified 2 2
SCV/RA/IV tear survival rate – 45%
HRS Expert Consensus 2009, EHRA position paper 2012
IT IS RECOGNIZED THAT IN CASE OF SVC IS TORN OR PERFORATED, DELAYS OVER 5-10 MINUTES TO HAVING OPEN ACCESS TO THE HEART IS OFTEN ASSOCIATED WITH FATAL OUTCOME
IT IS RECOGNIZED THAT IN CASE OF SVC IS TORN OR PERFORATED, DELAYS OVER 5-10 MINUTES TO HAVING OPEN ACCESS TO THE HEART IS OFTEN ASSOCIATED WITH FATAL OUTCOME
EXTRACTION - REQUIREMENTSEXTRACTION - REQUIREMENTS
PERSONNEL – PRIMARY OPERATORPERSONNEL PERSONNEL –– PRIMARY OPERATORPRIMARY OPERATOR
EHRA position paper 2012
REQUIREMENTS - GENERAL:
• HOSPITAL WITH CARDIOTHORACIC SURGERY, ANGIOGRAPHY AND PACEMAKER LABORATORY
• FULL RANGE OF EXTRACTION (AND OTHER) TOOLS
REQUIREMENTS - GENERAL:
• HOSPITAL WITH CARDIOTHORACIC SURGERY, ANGIOGRAPHY AND PACEMAKER LABORATORY
• FULL RANGE OF EXTRACTION (AND OTHER) TOOLS
LEAD EXTRACTION ENVIRONMENTLEAD EXTRACTION ENVIRONMENT
LEAD EXTRACTION CENTERLEAD EXTRACTION CENTERLEAD EXTRACTION CENTER
PATIENTPATIENT LEADLEAD
TIMETIME
TEAMTEAM
(Facilities,(Facilities,
Experience)Experience)
Lead Extraction: The Devil’s Triangle
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
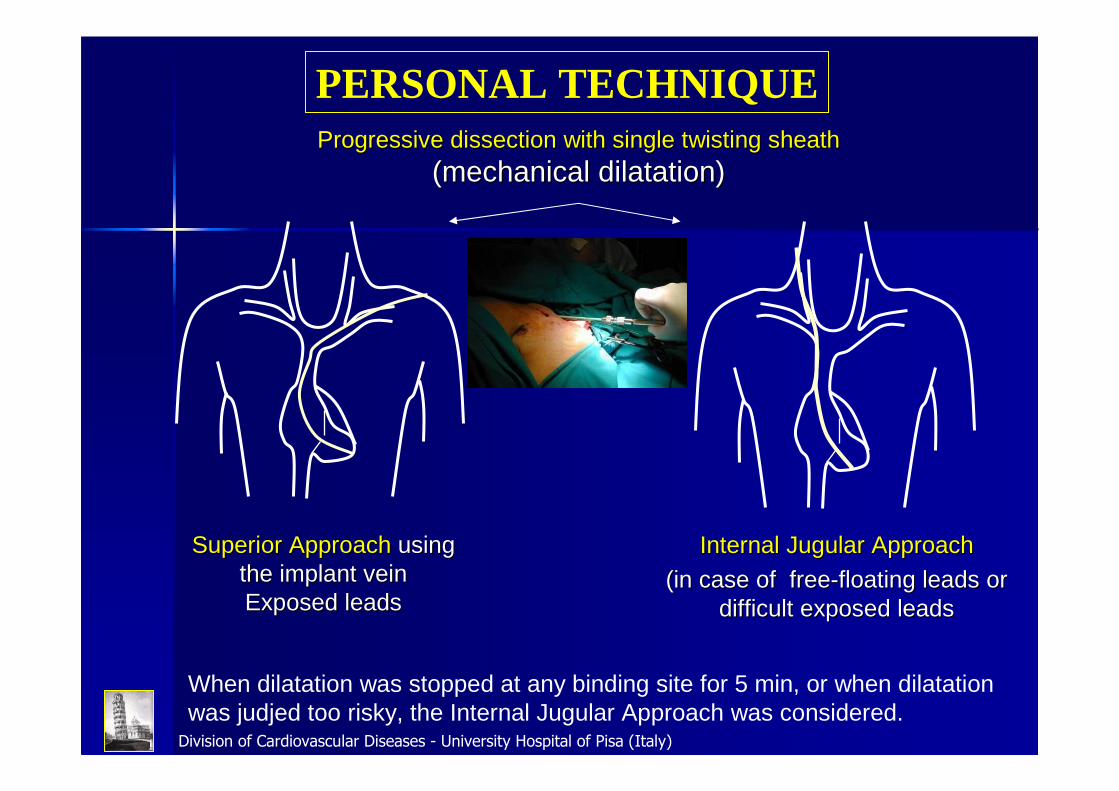
Superior ApproachSuperior Approach using using the implant veinthe implant veinExposed leadsExposed leads
Internal Jugular ApproachInternal Jugular Approach
(in case of free(in case of free--floating leads or floating leads or difficult exposed leadsdifficult exposed leads
Progressive dissection with single twisting sheath Progressive dissection with single twisting sheath
(mechanical dilatation)(mechanical dilatation)
When dilatation was stopped at any binding site for 5 min, or when dilatation was judjed too risky, the Internal Jugular Approach was considered.
PERSONAL TECHNIQUE
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
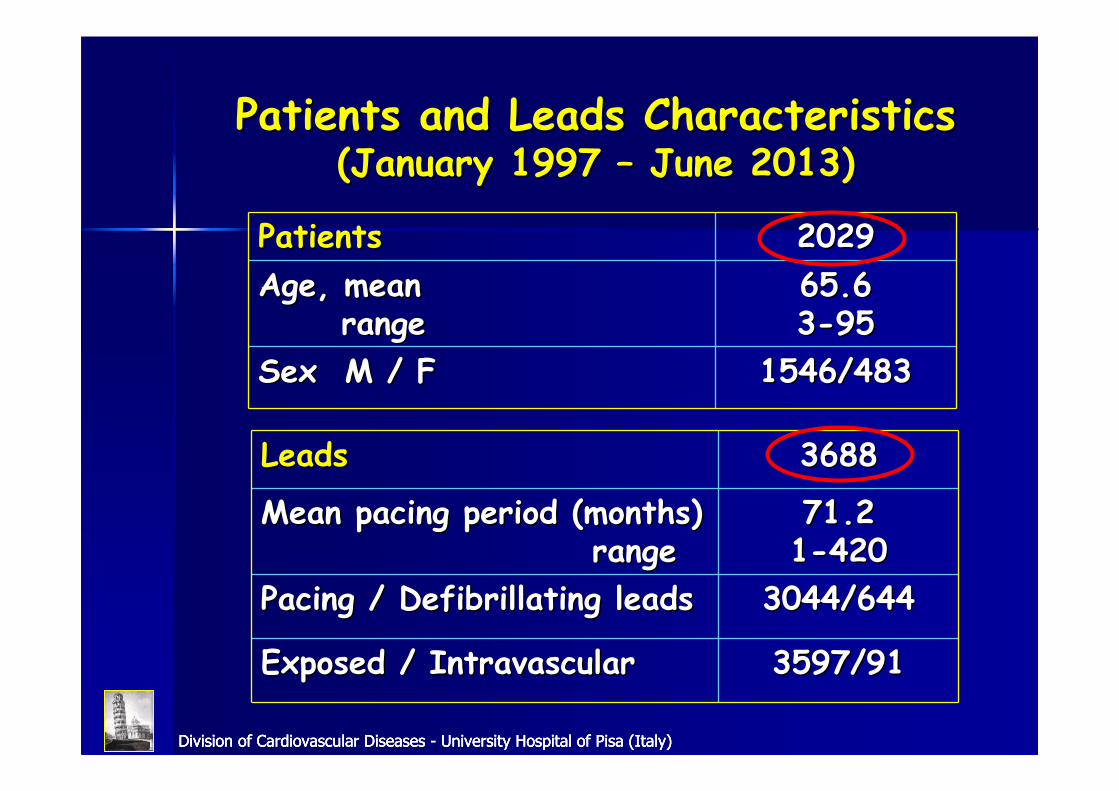
PatientsPatients 20292029
Age, meanAge, meanrangerange
65.665.633--9595
Sex M / FSex M / F 1546/4831546/483
LeadsLeads 36883688
Mean pacing period (months)Mean pacing period (months)rangerange
71.2 71.2 11--420420
Pacing / Defibrillating leadsPacing / Defibrillating leads 3044/6443044/644
Exposed / IntravascularExposed / Intravascular 3597/913597/91
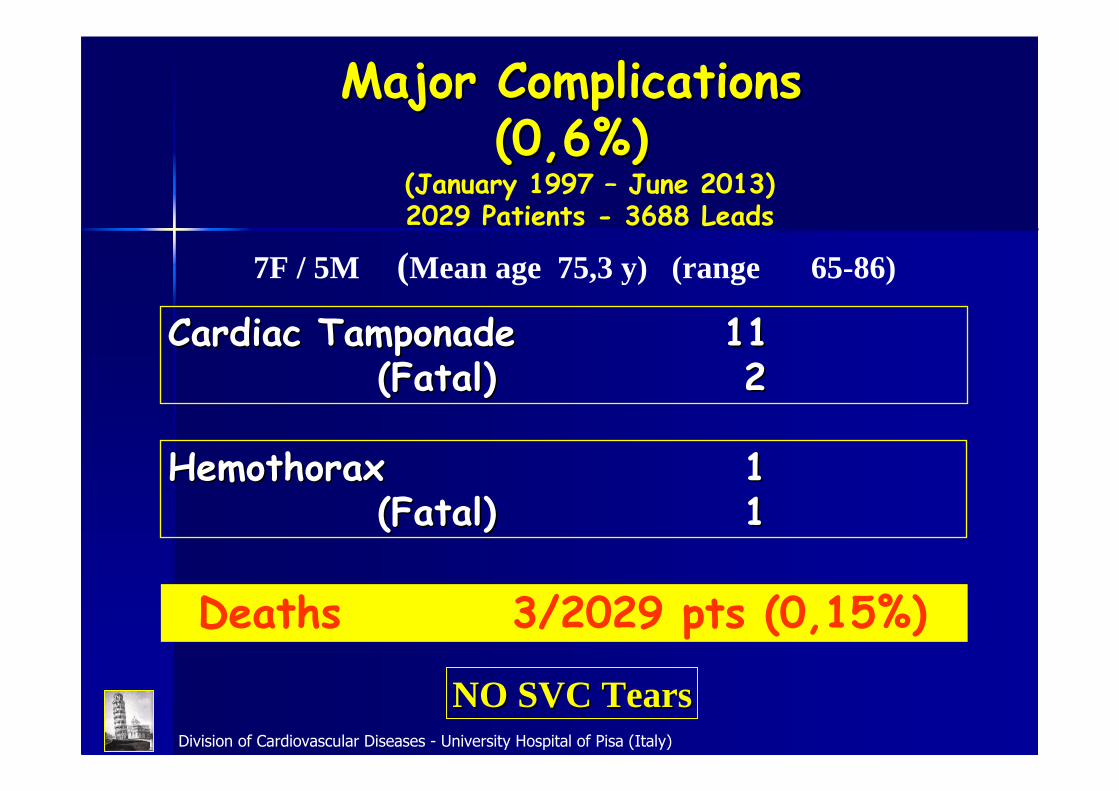
Patients and Leads CharacteristicsPatients and Leads Characteristics(January 1997 (January 1997 –– June 2013)June 2013)
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
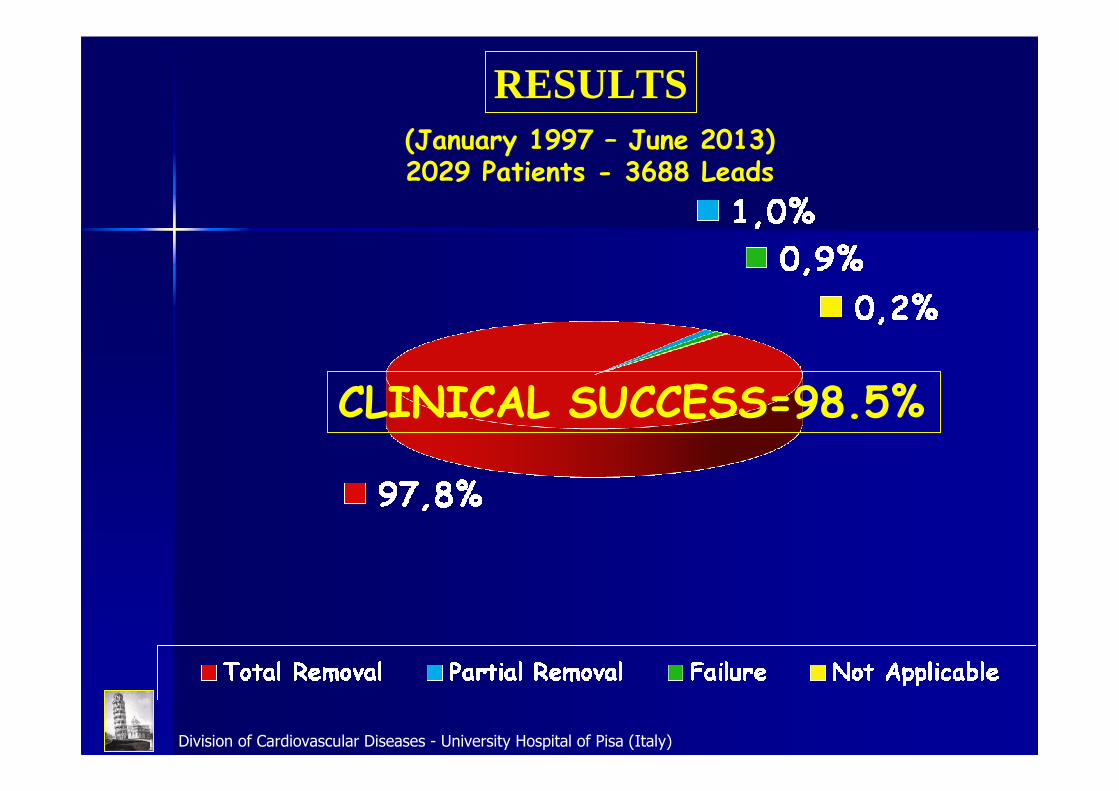
RESULTS
CLINICAL SUCCESS=98.5%
(January 1997 – June 2013)2029 Patients - 3688 Leads
Division of Cardiovascular Diseases - University Hospital of Pisa (Italy)
Cardiac Tamponade Cardiac Tamponade 1111(Fatal)(Fatal) 22
Major ComplicationsMajor Complications(0,6%)(0,6%)
Deaths 3/2029 pts (0,15%)
HemothoraxHemothorax 1 1 (Fatal)(Fatal) 11
7F / 5M (Mean age 75,3 y) (range 65-86)
NO SVC TearsNO SVC Tears
(January 1997 – June 2013)2029 Patients - 3688 Leads
REQUIREMENTS TO PERFORM LEAD EXTRACTIONSREQUIREMENTS TO PERFORM LEAD EXTRACTIONS
SURVEY
REGISTRY
SURVEYSURVEY
REGISTRYREGISTRY
HRS Expert Consensus 2009, EHRA position paper 2012
Study design and method
This is the first large prospective, multicentre, European Controlled Registry of
consecutive patients undergoing TLE procedures in European Countries.
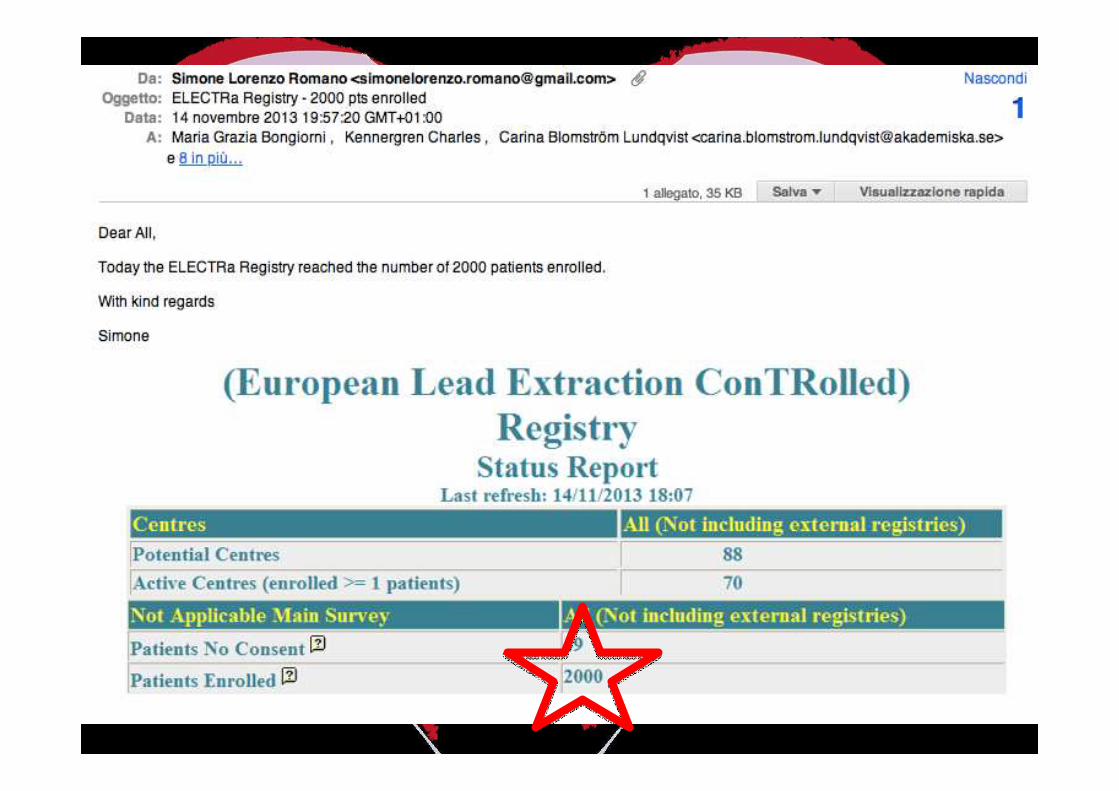
(EuropeanLead Extraction ConTRolled Registry)
ELECTRa Registry
• About 100 centres were invited to participate in the registry from 25 countries.
• Each centre will register consecutive patients for a total of 3500 patients.
• Every patient will be enrolled the day before the procedure.
• All consecutive patients will be followed up to 1 year.
• Indications to perform procedures will be left to the decision of participating physicians.
• No specific protocol or recommendations for the procedure, materials, techniques of lead
extractions, or treatment after the procedure will be mandated during this observational
study.

First large Prospective, multicentre, European Controlled Registry of
consecutive patients undergoing TLE procedures
in European Countries
Prospective
Controlled
ELECTRa Registry(EuropeanLead Extraction ConTRolled Registry)
Executive Committee
Maria Grazia Bongiorni (Chair)
Charles Kennergren (Co-chair)
Christian Butter
Jean-Claude Deharo
Andrzej Kutarski
Aldo Rinaldi
Aldo Maggioni (EORP)
Carina Blomström-Lundqvist (Chair-SIC)
Angelo Auricchio (EHRA President)
ELECTRa RegELECTRa Registryistry
EURObservational Research Programme
Thierry Ferreira - Head of department EORP
Gérard Gracia Data MonitorViviane Missiamenou Data MonitorMarème Konte Data MonitorMaryna Andarala Data MonitorCécile Laroche StatisticianCharles Taylor IT Specialist
Patti-Ann McNeill AssistantMyriam Glemot AssistantEmanuela Fiorucci AssistantMyriam Lafay Assistant
Simone Romano Fellow
•
Regional Coordinators
Maria Grazia Bongiorni
Charles Kennergren
Christian Butter
Jean-Claude Deharo
Andrzej Kutarski
Aldo Rinaldi 41
Primary Objective
The primary objective is:
� To evaluate the acute and Long-Term safety of TLE
Measures:
� Major procedure-related complications
(including death) in acute and Long-Term follow-up
ELECTRa Registry
Secondary Objectives
• To describe demographic, clinical, and biological characteristics of patients undergoing TLE procedure in a representative setting of European cardiology Centres.
• To describe the characteristics of leads undergoing extraction.
• To evaluate indications for TLE procedures.
• To describe the diagnostic and therapeutic approaches employed in the routine practice of physicians performing TLE procedures.
• To assess the acute and chronic outcomes of TLE procedures.
ELECTRa Registry
ELECTRa Registry
44

ELECTRa Registry
ELECTRa Registry
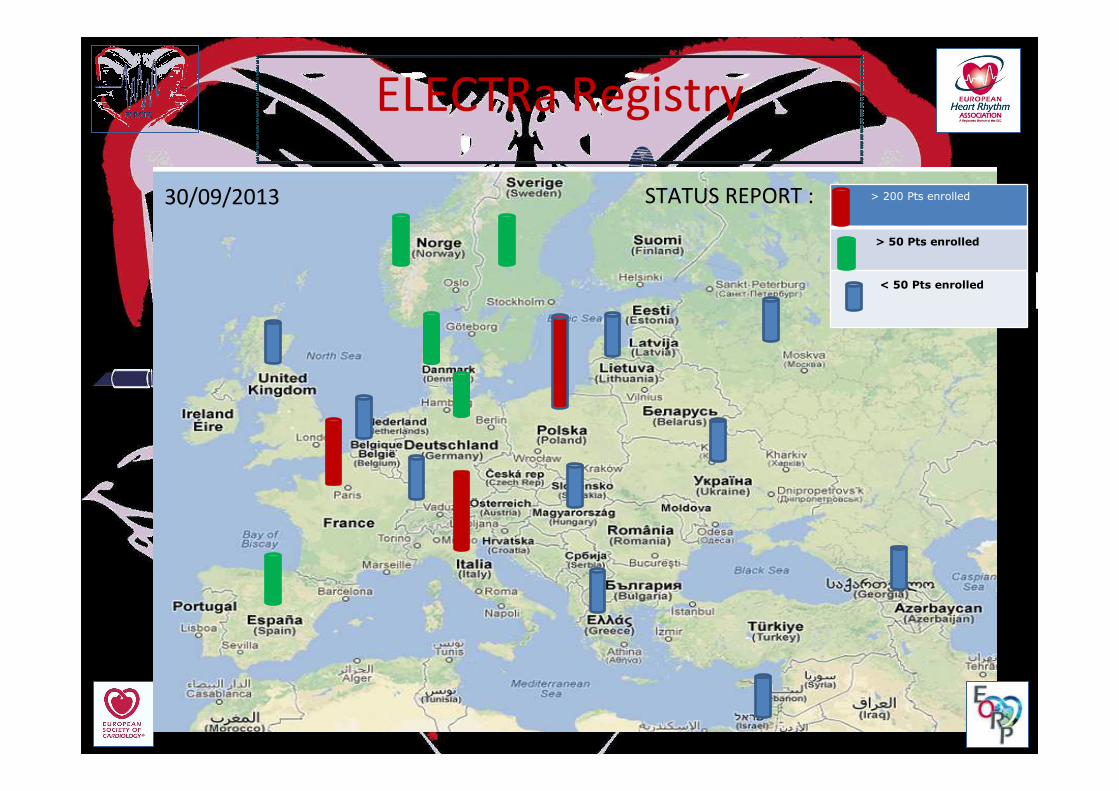
> 200 Pts enrolled
> 50 Pts enrolled
< 50 Pts enrolled
30/09/2013 STATUS REPORT :
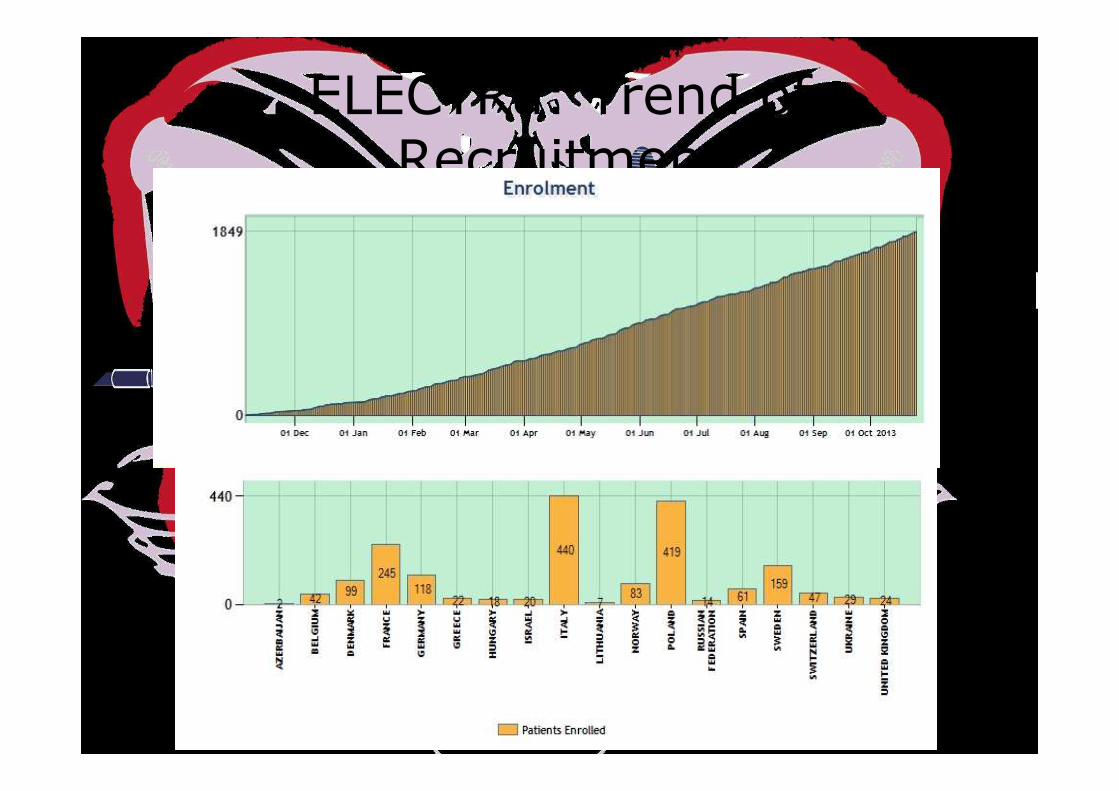
ELECTRa: Trend of
Recruitment
Approaching lead extractionApproaching lead extraction
Grazie per lGrazie per l’’ attenzioneattenzione







![[PPT]Apparato circolatorio - marino's space | Just another ... · Web viewApparato circolatorio nomi di arterie e vene principali Apparato circolatorio nomi di arterie e vene principali](https://img.pdfslide.us/doc/110x75/5c71a41e09d3f2b92e8b462a/pptapparato-circolatorio-marinos-space-just-another-web-viewapparato.jpg)