Embed Size (px)
Citation preview

Gut, 1976, 17, 81-91
Hypersensitivity reactions in the small intestine2 Effects of allograft rejection on mucosal architecture andlymphoid cell infiltrate
T. T. MAcDONALD' AND ANNE FERGUSON
From the Department of Bacteriology and Immunology, University of Glasgow, Glasgow, and GastrointestinalUnit, Western General Hospital and University of Edinburgh, Edinburgh
SUMMARY Small intestinal mucosa contains both thymus dependent and thymus independentlymphoid cells and thus has the capacity to act via humoral and cellular mechanisms as a site of localimmunity and local hypersensitivity. Allograft rejection of mouse small intestine is a model of alocal cell mediated reaction. The effects of this clearly defined, immunologically mediated damageon villi, crypts, enterocytes, and lymphoid cell infiltrate have been assessed by comparing themorphology of rejecting allografts with that of isografts and normal small intestine of the same age.In rejection there is infiltration of the lamina propria with lymphocytes, hyperplasia of the crypts ofLieberkuhn, and an eventual sloughing off of the mucosa. Usually, but not always, there is villousatrophy and increased numbers of intraepithelial lymphocytes. However, the morphology of indivi-dual enterocytes remains normal throughout rejection and neither plasma cells nor polymorpho-nuclear leucocytes infiltrate the lamina propria before mucosal ulceration. These results showunequivocally that a local T cell mediated immune response causes villous atrophy and crypt hyper-plasia in this animal model, and since there is no evidence of local enterocyte cytotoxicity, a lympho-kine may be the link between the activated T cell and the effects on mucosal architecture. We suggestthat a local CMI reaction may be the cause of villous atrophy, crypt hyperplasia, and malabsorptionin many clinical and experimental conditions, including coeliac disease, food allergy, and intestinalinfections.
The immune response to an antigen may have anentirely protective function, in the classical sense ofimmunity to infection. However, an immuneresponse may be the primary cause of disease andseveral types of these 'hypersensitivity' reactionscan be differentiated according to the immunemechanisms of tissue damage (Gell and Coombs,1969). Since animal experiments have shown thatthe small intestinal mucosa contains both thymusdependent and thymus independent lymphoid cells(Fichtelius et al., 1968; Sprent and Miller, 1972;Ferguson and Parrott, 1973a; Guy-Grand et al.,1974; Parrott and Ferguson, 1974) this tissue thushas the capacity to act via humoral and cellularmechanisms as the site of local immunity and localhypersensitivity.The functions of local T cell-mediated immune
'Address for correspondence: Mr T. T. MacDonald, University ofGlasgow, Department of Bacteriology and Immunology, Western In-firmary, Glasgow Gil 6NT, Scotland.Received for publication 14 November 1975
81
reactions in the intestinal mucosa are, as yet, un-defined. There is some evidence that local cell-mediated immunity (CMI) is important in immunityto helminth parasites (Jarrett and Urquhart, 1971;Dineen et al., 1973; Ogilvie and Jones, 1973; Ogilvieand Love, 1974) and in resistance to local tumourspread (Calman, 1974). We have proposed that localCMI may also have a pathological role, as the causeof villous atrophy and crypt hyperplasia (Ferguson,1974a, b; Ferguson and Jarrett, 1975). In a series ofexperiments in which thymus deprived rats wereinfected with the parasite Nippostrongylus brasiliensis,we found that not only were these rats immuno-deficient, with delayed elimination of the parasiteload, but also the worm associated partial villousatrophy failed to develop in 70% of experimentalanimals. This implied that the local enteropathyassociated with parasite infection was due to thethymus dependent immune reaction-that is, was alocal hypersensitivity reaction.
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

T. T. MacDonald and Anne Ferguson
Further support for the concept that local cell-mediated immune reactions may contribute to smallbowel damage and disease have come from investi-gations of intestinal allograft rejection and graftversus host disease (Reilly and Kirsner, 1965;Holmes et al., 1971; Ferguson, 1972; Ferguson andParrott, 1973b). These produce partial or sub-totalvillous atrophy in affected areas of the small intestineand, in the case of graft-versus-host disease, themorphological changes have been shown to beaccompanied by disaccharidase deficiency (Hedberget al., 1968), malabsorption (Palmer and Reilly,1971) and a protein losing enteropathy (Cornelius,1970).We have used allograft rejection of grafts of foetal
mouse small intestine (Ferguson and Parrott, 1973b)as a model of a cell-mediated immune reaction in thesmall intestinal mucosa. In the course of experimentswith thymectomised, irradiated, and bone marrowreconstituted mice, we demonstrated that rejectionof allografts in this system was a thymus dependentphenomenon (Ferguson and Parrott, 1973b) and,since rejection and the associated flat mucosa precedethe appearance of serum antibody by several days(Elves and Ferguson, 1975), we have confirmed thatthe response is mediated by lymphocytes. In addition,since the transplanted tissue is foetal and has neverbeen exposed to foods or micro-organisms, allpathological features observed can be attributeddirectly to the rejection process with no super-imposed local immune reactions to foods or bacteria.We have previously reported the histopathological
appearances of rejection in these grafts (Ferguson,1972; Ferguson and Parrott, 1972; Ferguson andParrott, 1973b; Ferguson and MacDonald, 1975)and the most interesting finding was that for a fewdays before complete rejection, many tissues had aflat luminal surface with long crypts of Lieberkuhn,so that the morphology was remarkably similar tothat of the small intestine in coeliac disease. Theobject of this work is to define more clearly the
effects of this thymus dependent, cell-mediatedrejection process on the villus and crypt architecture,the evolution of the changes observed, and also theeffect on the individual enterocytes and the intestinallymphoid cells. We report here the results of lightmicroscopic examination; scanning and trans-mission electron microscopy of rejection are des-cribed in a separate paper (Carr et al., 1976).
Methods
ANIMALSMice used were of the inbred strains CBA, C3H-Biand Balb/c (histocompatibility antigens H-2k, H-2kand H-2d respectively (Snell et al., 1964)) maintainedin the Department of Bacteriology and Immunology,University of Glasgow. The technique for graftingfoetal mouse intestine has been described in detailelsewhere (Ferguson and Parrott, 1972; Ferguson,1973) but is briefly as follows: pregnant mice werekilled on the 18th or 19th day of gestation, the foetalsmall intestine was dissected out and cut intosegments 5-10 mm in length, and pieces of smallintestine were then implanted under the kidneycapsules of adult recipient mice (two grafts permouse).Groups of recipient mice were killed by ether
overdosage at intervals from one to 20 days aftergraft implantation. The grafts were easily recog-nisable as white swellings under the kidney capsules.These were dissected out, with a little underlyingkidney tissue, and fixed in formol saline. Groups ofnormal CBA mice were killed by cervical dislocationat intervals from one to 20 days after birth and threepieces of small intestine were fixed in formol saline.Table 1 gives details of the number of specimensexamined, including normal small intestine, isograftsand allografts.
HISTOLOGYThe fixed tissues were paraffin embedded, 5,u thick
Experimental group Total number of Histologicalpreparations Age oftissue after implantation (days)grafts implanted suitablefor analysis
(no.) 0-5 6-10 11-15 16-20
Normal CBA small intestine 29 29 7 8 7 7Isografts ofsmall intestineCBA-CBA 35 27 4 6 4 13Balb/c-÷Balb/c 36 31 7 9 4 11
Allografts ofsmall intestineCBA-Balb/c 67 56 23 21 8 4Balb/c-CBA 79 63 28 34 1 -CBA C3H 35 35 9 10 8 8C3H CBA 22 22 3 1 6 12
Total number ofspecimens 303 263
Table 1 Details ofnumber and nature oftissues used to study the effect ofallograft rejection on mucosal morphology andymphoid cell infiltrate
82
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

Allograft rejection of mouse intestine
sections were cut at three levels and stained withhaematoxylin and eosin and with methyl greenpyronin. Sections were coded, mixed, and examinedon three occasions for morphological grading of thestage of rejection, for measurements of the lengthsof crypts and villi and of epithelial cell height, andfor lymphoid cell quantitation.
MORPHOLOGICAL GRADING OF REJECTIONThis was done by using the criteria described in ourearlier paper (Ferguson and Parrott, 1973b). Thegradings were as follows:Normal for age, with villi normal, crypts short, andvirtually no plasma cells or lymphocytes in thelamina propria.L+ lymphocyte infiltration of the lamina propria,with many lymphocytes and pyroninophilic blastcells in lymphatics.L+ +dense lymphocyte infiltration throughout thefull thickness of the graft, but villi still recognisable.Flat Villi very short or absent although epitheliumand crypts still present-that is, the appearance ofpartial or sub-total villous atrophy (Shiner andDoniach, 1960).Submucosa The epithelium and lamina propriadestroyed so that the graft consists of smooth muscleheavily infiltrated with lymphocytes and plasmacells.
MEASUREMENTS OF VILLI, CRYPTS, AND
EPITHELIAL CELLS
An eyepiece micrometer was used to measure thelengths of villi and crypts and epithelial cell height,in well-orientated sections. Where possible, 10measurements of enterocyte height/graft were madeand the mean value calculated. Villus height andcrypt depth were calculated as the mean of fivemeasurements per graft. In the smallest grafts (upto about 10 days after implantation), it was rarelypossible to make accurate measurements of thevilli, but measurements of crypts and enterocyteheight were possible in most specimens.
QUANTITATION OF LYMPHOID CELLSThe lymphocytes within the epithelium (intra-epithelial, IE, lymphocytes) and in the laminapropria were examined separately. IE lymphocyteswere investigated in two ways. In normal gut, inisografts and in the allografts between CBA andC3H mice it was possible to carry out differentialcounts of epithelial cells and IE lymphocytes aspreviously described (Ferguson and Murray, 1971)and thus to obtain counts of the number of lympho-cytes per 100 epithelial cells (a total of 500 cellscounted).
In the other strain combination between CBAand Balb/c mice, the presence or absence of IElymphocytes was noted (presence being defined asat least one lymphocyte per 200 epithelial cells).Lamina propria lymphoid cells were assessed as
absent, scanty infiltrate, or dense infiltrate. Plasmacells in the lamina propria were best observed in themethyl green pyronin stained sections.
STATISTICSResults of the measurements and counts in the groupsof tissues were compared in two ways-by groupingspecimens according to age and also according tothe stage of rejection. Student's t test was used toassess the significance of differences between thevarious groups of measurements, with the exceptionof intraepithelial lymphocyte counts in the tissueswhere these were defined as being simply present orabsent. Yates's x2 test was used in analysis of theseresults.
Results
In these experiments the time course of rejection andthe morphological appearances of small intestinalallografts were as expected from our previous work,and tissues suitable for histological assessment wereobtained in 234 of 274 experiments. The effect ofstrain combination on the time course of rejection isillustrated by the results of morphological grading
Experimental group Grade ofrejection Number ofallografts at each grade, when examined at intervals aftertransplantation (days)
1-3 4-5 6-7 8-10 11-15 16-20
Allografts Normal 10 - - - - -CBA = Balb/c L+ 3 3 1 - _ _
L+ + 5 15 15 5 - -(H-2 incompatible) Flat 5 8 9 5 - -
Submucosa 1 1 9 13 7 4Allografts Normal 7 2 1 -
CBA=C3H L+ 2 4 2 -L++ 2 2 4 2
(H-2 compatible) Flat 1 3 6 13Submucosa - - 1 7
Table 2 Morphologicalgrading ofrejection in allografts ofmouse small intestine
83
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

T. T. MacDonald and Anne Ferguson
(a)
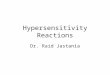
Fig. 1 (a) Isograft ofmouse small intestine, nine days afterimplantation ofafragment ofCBA foetal intestine under thekidney capsule ofan adult CBA mouse. Villi and cryptsappear normal, and there arefew lymphoid cells in thelamina propria and within the epithelium. HandE, x 120.(b) Allograft ofmouse small intestine, nine days afterimplantation ofafragment ofCBA foetal intestine underthe kidney capsule ofan adult Balblc mouse. The mucosaappearsflat, with villous atrophy, the crypts ofLieberkuhnare long and the laminapropria is extensively infiltratedwith lymphocytes. HandE, x 120.
of allografts, summarised in Table 2. The sequenceof events which leads to rejection is identical in allstrain combinations studied but rejection betweenthe H-2 identical strains CBA and C3H takes around20 days, whereas rejection of the allografts betweenthe unrelated strains CBA and Balb/c is completedby 10 days after transplantation. Figures la and lbillustrate the typical appearances of a normalisograft and a partly rejected allograft.
INFLUENCE OF REJECTION ON CRYPTS OFLIEBERKUHNIn newborn mice, the crypts are very short and mayoccasionally be impossible to define; however, theyincrease in length during the first week of life andby the age of 9 days have a mean length of 25-6 ,um(standard error, SE 4 6 Mm). Isograft crypts alsoenlarge during this period and have a mean lengthof 32 Mm (SE 2 6 Mm) by day 9 after implantation.This value is not significantly different from themean crypt length of normal mice of the same age.However, objective measurement ofwell-orientated
allograft crypts has shown that they are consistentlylonger than crypts of isografts and of normal smallintestine (Fig. 2). From the fourth day, the crypts ofrejecting grafts are always longer than those ofisografts and normal intestine of the same age, thisdifference being significant (p < 0001) in everycomparison made. This finding of abnormally longcrypts-crypt hyperplasia-has been the mostconsistent feature of rejection in these experiments,and forces us to modify previous subjective state-ments (Ferguson and Parrott, 1973a) about the'normal' appearance of some crypts in rejection.Although some variation in crypt length does occurduring rejection, our previous finding was probablydue to observation of crypts which were not properlyorientated.The relation between crypt depth and the general
morphological grading of rejection is shown in Fig.3. By using this type of analysis, the differences inthe time course of rejection between different strainsare circumvented, and it is clear that the effect ofrejection on crypt length is similar in slow and fastrejection. Significant lengthening of the crypts has
84
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

Allograft rejection ofmouse intestine
Length ofCrypts of Lieberkuhn
.( ImI
I-,,
)t
1-3 4-5 6-7Age of tissue (days)
8-9
Fig. 2 The influence ofallograft rejection on the lengthsofthe crypts ofLieberkuhn in mouse small intestine.Means ± SE ofcrypt length in groups ofspecimens ofnormal small intestine, isografts ofsmall intestine in CBAand Balblc mice, and allografts ofsmall intestine betweenthe strains CBA and Balblc. With this strain combinationrejection starts around the thirdday after graft implan-tation and is completed by 10 days. Specimens aregroupedaccording to tissue age-that is, days after birth orimplantation. At leastfive graftsperpointfor graftedintestine andfour miceperpointfor normally sitedintestine.
been found at grades L+ and L+ + in all of thegroups studied, and this occurs before the graftshave developed atrophy of the villi.
INFLUENCE OF REJECTION ON VILLI
For the first few days after implantation, grafts areextremely small and it is rarely possible to findenough suitably cut areas to allow measurement ofvillous height. Thus, we did not obtain meaningfulmeasurements of the villi during rejection of allo-grafts between the CBA and Balb/c strains. Theslower speed of rejection in the CBA-C3H com-bination allowed the grafts to grow to such a sizethat sequential measurements of villous heightcould be made and the results are illustrated inFig. 4. In normal small intestine and in isografts,villi slowly increase in height for three weeks after
0
I-,I .
.1
A CBA-+Balb/cA Balb/c-÷CBAX CBA--C3H0 C3H-÷CBA
NORMAL L+ L++ FLAT
Histological grade of graft
Fig. 3 Correlation between histologicalgrade ofrejectionand the length ofthe crypts ofLieberkuhn in allografts offoetal mouse small intestine(four strain combinations).Means ± SEofallgroups ofspecimens classified accordingto histologicalgrade, irrespective oftissue age. At leastsixgraftsperpoint.
birth. However, the villi are shorter in isografts. Thisdifference from normal intestine is real, and not dueto fixation or orientation artefacts. Possible reasonsfor the shorter villi in isografts are presently underinvestigation. However, in allografts undergoingrejection, villi are consistently shorter than inisografts of the same age (p < 0-01 for all groupsafter day 6). This difference is at maximum inspecimens examined between 16 and 20 days afterimplantation; the mean villous height for normalintestine of this age is 390 ,um; for isografts the meanvillous height is 217 um; and for allografts betweenCBA and C3H strains the mean villous height is only12 ,um.
INFLUENCE OF REJECTION ON EPITHELIAL
CELL HEIGHTMeasurement of enterocyte height did not reveal any
Length ofCrypts of Lieberkuhn
(km)100-
80-
60-
20-
0 9F l~~~~~~~~~~~~~~~~~~~~~ 85
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

T. T. MacDonald and Anne Ferguson
Length of villiI lguM)
Epithelial cellheight ( Lm)
20-
16-
12-
1-5 6-10 11-15 16-20Age of tissue (days)
Fig. 4 Influence ofallograft rejection on the length ofvilliin mouse small intestine. Means ± SE of villus lengthin groups ofspecimens ofnormal small intestine, isograftsofsmall intestine in CBA and Balblc strains, and allograftsofsmall intestine between strains CBA and C3H. Withthis strain combination rejection starts aboutfive daysafter implantation and in most grafts is completed by25 days. At least six grafts or normally sited smallintestineperpoint.
significant differences between normal intestine,isografts and allografts (Fig. 5). Enterocyte heightwas in the range 13-18 ,um in all groups studied.The enterocytes appeared to have essentially normalmorphology as assessed by light microscopy.However, electron microscopic studies have shownsome changes in the brush border and these findingsare discussed in another paper (Carr et al., 1976).
INFLUENCE OF REJECTION ON LYMPHOID
CELLS OF LAMINA PROPRIA
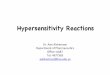
Lamina propria lymphoid cells are not present inneonatal mouse intestinal mucosa (Ferguson andParrott, 1973a; Mattioli and Tomasi, 1973) and byour definition the earliest sign of rejection is theappearance of mucosal lymphocytes. These are atfirst confined to the draining lymphatics wherepyroninophilic blast cells are obvious. As rejectionproceeds, the lymphocytes infiltrate the laminapropria and in established rejection there is denselymphocyte infiltration of the mucosa and sub-mucosa with the lymphatic vessels packed withlymphocytes (Fig. 6). Plasma cells are not found inthe mucosa in early rejection but at the 'submucosa'
8
A
x0
CBA-+Balb/cBalb/c-+CBACBA-+C3HCH3-+CBH
NORMAL L+ L++ FLATHistological grade of graft
Fig. 5 Lack ofinfluence ofallograft rejection on theheight ofsmall intestinal villous epithelial cells. Means ±SE ofepithelial cell height in allografts ofmouse smallintestine (four strain combinations). Specimens aregroupedaccording to histologicalgrade ofrejection. At leastfivegraftsperpoint.
stage-that is, when the mucosa has been destroyed,they are present and infiltrate the residual musclelayers.
INFLUENCE OF REJECTION ON IE LYMPHO-CYTESIntraepithelial lymphocyte counts have been carriedout in normal intestine, in isografts, and in allograftsbetween the strains CBA and C3H. The results ofthese counts are summarised in Fig. 7. Whereas IElymphocytes are infrequent or absent in neonatalmouse intestine and in isografts, many are presentin the allografts from day 6 (p < 0-01 for all com-parisons); and the numbers of IE lymphocytesincrease progressively with time after implantation.Figures 8a and 8b highlight the absence and presenceof IE lymphocytes within the epithelium of anisograft and an allograft.Only a limited assessment of IE lymphocyte
infiltration of grafts between CBA and Balb/c hasbeen possible and Table 3 illustrates the numbers ofgrafts in these combinations in which IE lympho-cytes were assessed to be present or absent (they wereconsidered absent if no lymphocytes were foundamong 200 epithelial cells examined). As in slowrejection, this semiquantitative assessment of IElymphocyte levels in acute rejection shows that asrejection proceeds there is an influx of lymphocytesinto the epithelium.
I I
86
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

Allograft rejection ofmouse intestine
Intraepithelial lymphocytecount ( per 100 epithelial cells)
t o *0 %. - VW" ...
=sk%vi_ a. ,i. w3~~~~~L .A.....
Fig. 6 Lymphocyte infiltration ofthe laminapropria in anallograft ofCBA foetal small intestine 17 days afterimplantation in a C3H host mouse. HandE, x 300.
Table 4 illustrates intraepithelial lymphocyte levelsand villus/crypt ratio during rejection (obtained bydividing the mean villus height by the mean cryptdepth at each time interval). During rejection, villusheight diminishes and crypt length increases, thusproducing as rejection progresses a decrease in thevalue of the v/c ratio. At the same time there is astriking increase in the intraepithelial lymphocytelevels. In isografts, however, villus height is main-tained during the time studied, the v/c ratio remainshigh, and there is only a slight increase in IE lympho-cyte levels.The association between the morphological
changes accompanying rejection or the laminapropria lymphocyte infiltration and the presence ofintraepithelial lymphocytes is, however, not com-plete, as is illustrated by Table 5. It can be seen that,even in late rejection, in all of the strain combinationscombined, almost one quarter of the grafts with a'flat' appearance, and thus a low v/c ratio and denselamina propria lymphocyte infiltrate, have no IElymphocytes present.
1-5 6-10 11-15Age of tissue (days)
* CBA-oC3H
I
C3H*CBA
I_/
I NORMAL S.I
,ISOGRAFTS
-2016-20
Fig. 7 Influence ofallograft rejection on the intra-epithelial lymphocytes ofthe small intestine. Means i SEofIE lymphocyte counts(per 100 epithelial cells) in normalsmall intestine, isograft ofsmall intestine in CBA andBalblc mice, andallografts between CBA and C3Hstrains.Specimens aregrouped according to tissue age. At leastfive grafts or normally sited intestinesperpoint.
Experimental Days after Grafts Grafts with IEgroup implantation examined lymphocytes
ofgraft (no.) present (at least Ilymphocyte per 200epithelial cells(no.)
Isografts 1-3 7 04-5 2 1
CBA-CBA 6-7 2 2Balb/c -* Balb/c 8-9 4 0
Allografts 1-3 20 4CBA Balb/c 4-5 27 18
6-7 25 238-9 9 7
Table 3 Presence or absence ofintraepitheliallymphocytes in isografts and allografts ofmouse smallintestine during acute rejection
Discussion
Allograft rejection of small intestine is a cell-mediated reaction directed against histocompatibility
87
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

T. T. MacDonald and Anne Ferguson
(a)Fig. 8 Isograft ofsmall intestine in a CBA mouse 18 days Table 5 Presence or absence ofintraepithelialafter implantation. Note the absence ofintraepithelial lymphocytes in allografts ofmouse small intestine atlymphocytes. HandE, x 315. (b) Allograft ofCBA small different grades of rejectionintestine implanted in a C3H host 17 dayspreviously. Notethe presence ofbasally situated intraepithelial lymphocytesbetween columnar enterocytes. HandE, x 315.
Age oftissue Isografts Ailografts(days) CBA -- CBA CBA C3H
Balblc - Balblc
v/c JE lymph/.100 v/c IE lymph/100ratio epithelial cells ratio epithelial cells
1- 5 - 02 51 056-10 47 02 1 8 1 711-15 32 02 1-7 2516-20 35 14 02 83
Table 4 Villus/crypt ratio (v/c) andIE lymphocytenumbers at different times during slow rejectioncompared with isografts ofsame age
antigens which differ in the cells in the small intestinalmucosa of the different strains of mice used (Fer-guson and Parrott, 1973b; Elves and Ferguson,1975). We have now shown that constant morpho-logical features of this reaction are infiltration ofthe lamina propria with lymphocytes, hyperplasia ofthe crypts of Lieberkuhn, and ulceration of the
mucosa. Usually, but not always, there is alsovillous atrophy and increased numbers of intra-epithelial lymphocytes. The morphology of in-dividual enterocytes seems to remain normalthroughout rejection, these cells being columnar,with basal nuclei and an easily distinguishable brushborder even when the general architecture of thespecimen is of sub-total villous atrophy. Plasmacells have not been found in the lamina propriaduring early rejection. These infiltrate the debrisof the allografts which remains after ulceration ofthe mucosa. Polymorphonuclear leucocytes haverarely been found in rejecting allografts in ourexperiments.The striking changes which occur in villus-crypt
architecture in the absence of morphological damageto individual enterocytes are important and inter-esting. Indeed, we have previously reported thatsheets of apparently normal enterocytes are extrudedinto the lumen of rejecting grafts (Ferguson andParrott, 1973b). This exfoliation of the epitheliumcannot be attributed entirely to a cytotoxic effect ofthe infiltrating intraepithelial lymphocytes, for,
88
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

Allograft rejection ofmouse intestine
although these cells are in intimate contact with theenterocytes and are usually present during rejection,this is not always the case. A more constant obser-vation has been the presence of many lymphocytesin the lamina propria below the basement membrane.It seems possible that the local immune responsemay influence adhesion of enterocytes to the under-lying connective tissue rather than have a directlycytotoxic effect on these epithelial cells. Enterocyteadhesion could be impaired by an effect of the localcell-mediated immune reaction on local blood flowor on the connective tissue of the basement mem-brane; alternatively, the effect could be produced bydirect damage to the cell membranes which wouldthen influence the adhesion of the enterocytes to thebasement membrane and to one another.
If the cell height is a valid measurement of injuryto mucosal cells, the absence of any decrease incell height during rejection would seem to indicatethat it is the stroma of the transplanted tissue whichis bearing the brunt of the reaction rather than theepithelial cell itself. The link between the histologicalpicture of villous atrophy and crypt hyperplasia andthe local cell mediated immune response may be byone or more humoral factors produced as a resultof the interaction between sensitized lymphocytesand the histocompatibility antigens of the allograft.Lymphokines have been shown to be mitogenic andcytotoxic for other cell types (Remold, 1972) andwe have suggested that such an enteropathiclymphokine may cause enterocyte exfoliation, whichwould cause villous atrophy and compensatorycrypt hyperplasia, not only in allograft rejection butalso in other situations where a local CMI reactiontakes place in the vicinity of the small intestinalmucosa (Ferguson, 1974b; Ferguson and Jarrett,1975; Ferguson and MacDonald, 1975; Fergusonet al., 1975). A humoral factor which causes migrationinhibition of human peripheral leucocytes has beenobserved after gluten challenge of intestinal biopsiesfrom patients with coeliac disease (Ferguson et al.,1975) and a factor which inhibits the migration ofmouse peritoneal macrophages has recently beenfound to be produced during allograft rejection offoetal intestine, but not in isografts of the same age(MacDonald and Russell, 1976). Further investi-gations into the role of lymphokines in rejection areat present being carried out.
Hyperplasia of the crypts of ILieberkuhn occursearly in rejection (at four to five days) and this maybe due to a direct effect of the rejection process onthe crypt cells or a compensatory hyperplasia afteran increased rate of enterocyte loss. An early inter-action between sensitised lymphocytes and thetissue antigens might produce a mitogenic lyinpho-kine which would cause increased cell division in the
crypts; however, the same interaction might producean enteropathic lymphokine which would causeincreased cell loss and compensatory hyperplasia.But, as crypt hyperplasia is occurring without anydemonstrable loss of villus height, we favour theconcept of a direct mitogenic effect of rejection uponthe crypt cells themselves. In late rejection, however,when villus height dramatically drops, compensatorycrypt hyperplasia should occur.The homing of lymphoid cells to the mucosa of
rejecting allografts differs from the usual homing ofimmunoblasts to the small intestine (Delorme et al.,1969 in at least two respects. In rejection, theinfiltrating cells are mainly lymphocytes, whereas innormal intestine there is a mixture of lymphocytesand plasma cells; furthermore, lymphocytes appearin the mucosa of allografts up to two weeks earlierthan these cells infiltrate the intestine of normalmice. In this context, it is important to emphasizeagain that, in the small intestine of normal mice,within the age range used for these experiments,lymphocytes and plasma cells are almost neverpresent outside the Peyer's patches (Ferguson andParrott, 1973a; Mattioli and Tomasi, 1973). Aspecific homing of immunoblasts to the smallintestine of the mouse begins in the third week oflife and experiments in both mice and rats have shownthat homing of plasma cell precursors to grafts ofsmall intestine will occur in the complete absence ofintraluminal antigens (Moore and Hall, 1972;Ferguson and Parrott, 1973a; Guy-Grande et al.,1974; Parrott and Ferguson, 1974). In our work onthe induction of antibodies to grafts of intestine, wefound that the stimulus for production of thehumoral response to an allograft was probably thedebris produced by an early cell-mediated immuneresponse (Elves and Ferguson, 1975). For thisreason, the humoral antibody response to anallograft occurred several days after rejection wascompletely established. The late infiltration ofgrafts with plasma cells is in keeping with the timecourse of humoral antibody production and islikely, therefore, to be associated with the specifichumoral immune response to an allograft ratherthan to a gut-directed homing mechanism. Furtherexperiments on the traffic of lymphoid cells toallografts of small intestine will be required toconfirm this.There are scattered reports in the literature of the
effects of experimental hypersensitivity reactions inthe small intestinal mucosa, although these haveusually been observed in the course of experimentsdesigned for different purposes. For example, underappropriate conditions a local reaginic (type 1)immune response can produce oedema of the villiwith exfoliation of the epithelium (Barth et al., 1966).
89
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

90 T. T. McDonald and Anne Fergusoir
A local Arthus (type III) reaction, with depositionof immune complexes within the mucosa, maycause local polymorph infiltration without obvioustissue damage (Bellamy and Nielsen, 1974). Themorphological and functional changes associatedwith the initiation of, and recovery from, thesehypersensitivity reactions have not been describedso it remains to be defined whether or how an anti-body mediated local immune reaction can influencethe villus-crypt architecture, lymphoid cell infiltrate,and absorption. However, in the experiments onrejection described above, we have definitely shownthat a local delayed hypersensitivity reaction affectsvilli, crypts, and the lymphoid cells of the intestine.If these changes are produced by lymphokines, theyshould occur in any situation where a cell-mediatedimmune response occurs in the vicinity of theintestinal mucosa, and not merely when the responseis directed against the tissue itself. Indeed, there is aprecedent for this concept of local tissue damageas an unavoidable effect of a protective immunereaction, for this is the case in the lesions of leprosy(Turk and Bryceson, 1971). A local cell-mediatedimmune response may be the common factor whichcauses villous atrophy, crypt hyperplasia, andmucosal ulceration in food allergy, coeliac disease,local parasitic infections, and gastroenteritis. Whensuch a reaction occurs in an intestine alreadycolonised by commensal flora and exposed daily tofood, the ulceration, and perhaps also adjuvanteffects mediated by lymphokines (Krejci et al., 1973)could allow ingress of immunogenic food andmicrobial antigens, with immune reactions to theseintestinal constituents superimposed upon andultimately masking the primary disease processwhich is mainly cell mediated.
Nevertheless, local cell-mediated immunity cannotbe considered in isolation. In the Nippostrongylusbrasiliensis infection referred to in the introduction,there is evidence of IgE, IgG, mast cell, eosinophiland lymphocyte involvement in the local lesion(Jarrett and Urquhart, 1971; Dineen et al., 1973;Ogilvie and Jones, 1973; Ogilvie and Love, 1974).When patients with coeliac disease are challengedwith oral gluten, IgM, IgA, IgG and IgE are involvedin the subsequent local immune reaction (Shiner,1973; Lancaster-Smith et al., 1974; Lancet, 1974).Recently, we have also reported evidence of a localcell-mediated immune response to gluten in coeliacdisease (Ferguson et al., 1975). Clearly, greatcaution must be exercised in attributing enteropathyand malabsorption to any one type of local hyper-sensitivity reaction. Nevertheless, by using a clearlydefined experimental model such as allograftrejection, in which the extent and type of the localimmune reaction can be controlled, interactions
between local immunity, local hypersensitivity, the.absorptive and the endocrine functions of the smallintestine can now be thoroughly investigated.
This work has been supported by a grant from theNational Fund for Research into Crippling Diseases,and by research facilities supplied by E. Merck Ltd.We gratefully acknowledge the excellent technicalhelp of Mr H. Cairns of the Department of Bac-teriology and Immunology.
References
Barth, E. E. E., Jarrett, W. F. H., and Urquhart, G. M.(1966). Studies on the mechanism of the self-cure reactionin rats infected with Nippostrongylus brasiliensis. Immuno-logy, 10, 459-464.
Bellamy, J. E. C., and Nielsen, N. 0. (1974). Immune-mediatedemigration of neutrophils into the lumen of the smallintestine. Infection and Immunity, 9, 615-619.
Calman, K. C. (1974). Why are small bowel tumours rare?An experimental model. Gut, 15, 552-554.
Carr, K. E., MacDonald, T. T., and Ferguson, A. (1976).Influence of allograft rejection on small intestinal mucosalarchitecture, assessed by scanning and transmissionelectron microscopy. (In preparation).
Cornelius, E. A. (1970). Protein-losing enteropathy in thegraft-versus-host reaction. Transplantation, 9, 247-252.
Delorme, E. J., Hodgett, H. J., Hall, J. G., and Alexander, P.(1969). The cellular immune response to primary sarcomatain rats: 1. The significance of large basophilic cells in thethoracic duct lymph following antigenic challenge. Pro-ceedings of the Royal Society of London (Biology), 174,229-236.
Dineen, J. K., Ogilvie, B. M., and Kelly, J. D. (1973).Expulsion of Nippostrongylus brasiliensis from the intestineof rats: collaboration between humoral and cellularcomponents of the immune response. Immunology, 24,467-475.
Elves, M. W., and Ferguson, A. (1975). The humoral immuneresponse to allografts of foetal small intestine in mice.British Journal of Experimental Pathology. 56, 454-458.
Ferguson, A. (1972). Immunological roles of the gastro-intestinal tract. Scottish Medical Journal, 17, 111-118.
Ferguson, A. (1973). Implantation of tissue under the kidneycapsule. In Handbook of Experimental Immunology.p.A312-A313, Blackwell: Oxford.
Ferguson, A. (1974a). Lymphocytes in coeliac disease. InCoeliac Disease, pp. 265-276. Edited by W. T. J. M.Hekkens and A. S. Pena. Stenfert Kroese: Leiden.
Ferguson, A. (1974b). Thymus dependence of experimentalvillous atrophy. In Coeliac Disease, pp. 286-287. Edited byW. T. J. M. Hekkens and A. S. Pena. Stenfert Kroese:Leiden.
Ferguson, A., and Jarrett, E. E. E. (1975). Hypersensitivityreactions in the small intestine. 1. Thymus dependence ofexperimental 'partial villous atrophy'. Gut, 16, 114-117.
Ferguson, A., and MacDonald, T. T. (1975). Effects of localhypersensitivity reactions on small intestinal morphology.Behring Institute Research Communications, 57, 118-121.
Ferguson, A., and Murray, D. (1971). Quantitation of intra-epithelial lymphocytes in human jejunum. Gut, 12, 988-994.
Ferguson, A., MacDonald, T. T., McClure, J. P., andHolden, R. J. (1975). Cell-mediated immunity to gliadinwithin the small-intestinal mucosa in coeliac disease.Lancet, 1, 895-897.
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from

Allograft rejection of mouse injection 91
Ferguson, A., and Parrott, D. M. V. (1972). Growth anddevelopment of 'antigen-free' grafts of foetal mouseintestine. Journal of Pathology, 106, 95-101.
Ferguson, A., and Parrott, D. M. V. (1973a). The effect ofantigen deprivation on thymus-dependent and thymus-independent lymphocytes in the small intestine of themouse. Clinical and Experimental Imnmunology, 12, 477-488.
Ferguson, A., and Parrott, D. M. V. (1973b). Histopathologyand time course of rejection of allografts of mouse smallintestine. Transplantation, 15, 546-554.
Fichtelius, K. E., Yunis, E. J., and Good, R. A. (1968).Occurrence of lymphocytes within the gut epithelium ofnormal and neonatally thymectomized mice. Proceedingsof the Society for Experimental Biology and Medicine, 128,185-188.
Gell, P. G. H., and Coombs, R. R. A. (eds) (1969). ClinicalAspects of Immunology, pp. 575-596. Blackwell: Oxford.
-Guy-Grand, D., Griscelli, C., and Vassalli, P. (1974). Thegut-associated lymphoid system: nature and properties ofthe large dividing cells. European Journal of Immunology,4, 435-443.
Hedberg, C. A., Reiser, S., and Reilly, R. W. (1968). Intestinalphase of the runting syndrome in mice. 2. Observations onnutrient absorption and certain disaccharidase abnor-malities. Transplantation, 6, 104-1 10.
Holmes, J. T., Klein, M. S., Winawer, S. J., and Fortner,J. G. (1971). Morphological studies of rejection in caninejejunal allografts. Gastroenterology, 61, 693-706.
Jarrett, E. E. E., and Urquhart, G. M. (1971). The immuneresponse to nematode infections. International Review ofTropical Medicine, 4, 53-96.
Krejci, J., Pekarek, J., Svejcar, J., and Johanovsky, J. (1973).The effect of lymphokines on the development of delayedhypersensitivity to an unrelated antigen. Immunology, 25,875-879.
Lancaster-Smith, M., Kumar, P. J., and Clark, M.L. (1974).Immunological phenomena following gluten challenge inthe jejunum of patients with adult coeliac disease anddermatitis herpetiformis. In Coeliac Disease, pp. 173-174.Edited by W. T. J. M. Hekkens and A. S. Pena. StenfertKroese: Leiden.
Lancet (1974). The coeliac philosophy. (Editorial). Lancet,2,501-502.
MacDonald, T. T., and Russell, R. J. (1976). The detectionof lymphokines in rejecting allografts of foetal mouseintestine. (In preparation.)
Mattioli, C. A., and Tomasi, T. B. (1976). The lifespan ofIgA plasma cells from the mouse intestine. Journal ofExperimental Medicine, 138, 452-460.
Moore, A. R., and Hall, J. G. (1972). Evidence for a primaryassociation between immunoblasts and small gut. Nature,239, 161-162.
Ogilvie, B. M., and Jones, V. E. (1973). Immunity in theparasitic relationship between helminths and hosts.Progress in Allergy, 17, 93-144.
Ogilvie, B. M., and Love, R. J. (1974). Co-operation betweenantibodies and cells in immunity to a nematode parasite.Transplantation Reviews, 19, 147-168.
Palmer, R. H., and Reilly, R. W. (1971). Bile salt depletionin the runting syndrome. Transplantation, 12, 479-483.
Parrott, D. M. V., and Ferguson, A. (1974). Selectivemigration of lymphocytes within the mouse small intestine.Immnunology, 26, 571-588.
Reilly, R. W., and Kirsner, J. B. (1965). Runt intestinaldisease. Laboratory Investigation, 14, 102-107.
Remold, H. G. (1972). Purification and characterization oflymphocyte mediators in cellular immunity. Transplanta-tion Reviews, 10, 152-176.
Shiner, M. (1973). Ultrastructural changes suggestive ofimmune reactions in the jejunal mucosa of coeliac childrenfollowing gluten challenge. Gut, 14, 1-12.
Shiner, M., and Doniach, I. (1960). Histopathologic studiesin steatorrhoea. Gastroenterology, 38, 419-440.
Snell, G. D., Hoecker, G., Amos, D. B. and Stimpfling, J. H.(1964). A revised nomenclature for the histocompatibility-2locus of the mouse. Transplantation, 2, 777-784.
Sprent, J., and Miller, J. F. A. P. (1972). Interaction ofthymus lymphocytes with histoincompatible cells. II. Re-circulating lymphocytes derived from antigen-activatedthymus cells. Cell Immunology, 3, 385-404.
Turk, J. L., and Bryceson, A. D. M. (1971). Immunologicalphenomena in leprosy and related diseases. Advances inImmunology, 13, 209-266.
on October 7, 2021 by guest. P
rotected by copyright.http://gut.bm
j.com/
Gut: first published as 10.1136/gut.17.2.81 on 1 F
ebruary 1976. Dow
nloaded from