-
7/31/2019 1 Hypersensitivity Reactions
1/55
HYPERSENSITIVITY
Kathrina S. Perez, MD, DPSP
-
7/31/2019 1 Hypersensitivity Reactions
2/55
Exposure to antigen
SENSITIZATION
Repeat exposure to same antigen
HYPERSENSITIVITYREACTION
-
7/31/2019 1 Hypersensitivity Reactions
3/55
Hypersensitivity reactions
May be elicited by exogenous or endogenousantigens
Endogenous Agautoimmune diseases
Minor trivial forms to fatal reactions
reflects an imbalance between the effectormechanisms of immune
responses and the
control mechanisms that serve to normally limitsuch
responses
-
7/31/2019 1 Hypersensitivity Reactions
4/55
Types of hypersensitivity reactions
Type I Immediate
Type II Antibody-mediated
Type III Immune complex-mediated Type IV - Cell-mediated
-
7/31/2019 1 Hypersensitivity Reactions
5/55
Immediate (type I) hypersensitivity
Rapid, occurs within minutes
mediated by IgE antibody-dependent activationof mast cells and
other leukocytes
Ag + Ab bound to mast cells in persons withprevious
sensitization to Ag
Reaction may be systemic (e.g. after injection ofAg) or local
(depending on portal of entry of
allergen) Examples: Skin allergy, conjunctivitis, rhinitis,
bronchial asthma, gastroenteritis
-
7/31/2019 1 Hypersensitivity Reactions
6/55
-
7/31/2019 1 Hypersensitivity Reactions
7/55
IMMEDIATE OR INITIAL REACTION
Vasodilation, vascular leakage, smooth muscle
spasm, glandular secretion
Seen 5-30 minutes after exposure
Subside in 60 minutes
LATE-PHASE REACTION
infiltration of tissues with eosinophils, neutrophils,
basophils, monocytes, CD4+ T cells
Tissue destruction (mucosal epithelial damage)
Seen in 2-24 hours without additional exposure to
allergen, may last for days
-
7/31/2019 1 Hypersensitivity Reactions
8/55
-
7/31/2019 1 Hypersensitivity Reactions
9/55
-
7/31/2019 1 Hypersensitivity Reactions
10/55
-
7/31/2019 1 Hypersensitivity Reactions
11/55
Mast cells
Widely distributed in tissues (bloodvessels, nerves,
subepithelium)
have cytoplasmic membrane-bound
granules that contain a variety ofbiologically active
mediators
activated by the cross-linking of high-
affinity IgE Fc receptors, complementcomponents C5a and
C3a(anaphylatoxins)
-
7/31/2019 1 Hypersensitivity Reactions
12/55
Mast cells
chemokines (e.g., IL-8), drugs such ascodeine and morphine,
adenosine, mellitin(in bee venom), and physical stimuli (e.g.,
heat, cold, sunlight)
Basophils- same as mast cells but are notnormally present in
tissues - circulate in
the blood in very small numbers
-
7/31/2019 1 Hypersensitivity Reactions
13/55
Immediate (type I) hypersensitivity
TH2 has a central role in the initiation andpropagation of
immediate hypersensitivity
reactions by stimulating IgE production and
promoting inflammation; they produce IL-4 switching of Ab class
to IgE
IL-5 - development and activation of eosinophils
IL-13 - enhances IgE production and acts onepithelial cells to
stimulate mucus secretion
-
7/31/2019 1 Hypersensitivity Reactions
14/55
Preformed mediators
Vasoactive amines Histamine smooth muscle contraction,
increased vascular permeability & mucussecretion
Enzymes neutral proteases (chymase, tryptase) and
several acid hydrolases Cause tissue damage
Proteoglycans Heparin, chondroitin sulfate Pack the amines into
granules
-
7/31/2019 1 Hypersensitivity Reactions
15/55
Lipid mediators
synthesized by sequential reactions in the mastcell membranes
that lead to activation ofphospholipase A2 yield arachidonic
acid
Leukotrienes
Prostaglandin D2 Platelet-activating factor
CytokinesPromote leukocyte recruitment, additional sourcesof
cytokines and of histamine-releasing factorsthat cause further mast
cell degranulation
-
7/31/2019 1 Hypersensitivity Reactions
16/55
Mast cell mediators.Upon activation, mast cells releasevarious
classes of mediators that areresponsible for the immediate
andlate-phase reactions.
ECF, eosinophil chemotactic factor;NCF, neutrophil chemotactic
factor(neither of these is biochemicallydefined);PAF,
platelet-activating factor
-
7/31/2019 1 Hypersensitivity Reactions
17/55
dependent on the coordinated actions of avariety of chemotactic,
vasoactive, andspasmogenic compounds
Activated eosinophils and other WBCs alsoproduce mediators which
directly activate mastcells to degranulate -- recruited cells
amplify
and sustain the inflammatory response withoutadditional exposure
to the triggering antigen
Immediate (type I) hypersensitivity
-
7/31/2019 1 Hypersensitivity Reactions
18/55
Immediate (type I) hypersensitivity
Atopy
predisposition to develop localized immediatehypersensitivity
reactions to a variety of inhaled
and ingested allergens higher serum IgE levels, and more
IL-4-producing TH2 cells
positive family history of allergy found in 50% of
atopic individuals
-
7/31/2019 1 Hypersensitivity Reactions
19/55
Immediate (type I) hypersensitivity
Non-atopic allergy
triggered by temperature extremes and exercise,and do not
involve TH2 cells or IgE
mast cells are abnormally sensitive to activationby various
non-immune stimuli
-
7/31/2019 1 Hypersensitivity Reactions
20/55
Systemic anaphylaxis
vascular shock, widespread edema,difficulty in breathing
Triggers:
foreign proteins (e.g., antisera), hormones,enzymes,
polysaccharides, and drugs(e.g. penicillin)
food allergens (e.g. peanuts, shellfish)
insect toxins (e.g. bee venom)
-
7/31/2019 1 Hypersensitivity Reactions
21/55
Systemic anaphylaxis
itching, hives, and skin erythema appear withinminutes, followed
shortly thereafter by a strikingcontraction of respiratory
bronchioles and
respiratory distress Laryngeal edema hoarseness, dyspnea
Vomiting, abdominal cramps, diarrhea
patient may go into shock and even die withinthe hour!
-
7/31/2019 1 Hypersensitivity Reactions
22/55
Local Immediate Hypersensitivity Reactions
urticaria, angioedema, allergic rhinitis (hayfever), and
bronchial asthma
Seen in 10-20% of the population
-
7/31/2019 1 Hypersensitivity Reactions
23/55
Immediate (type I) hypersensitivity
Summary:
complex disorder resulting from an IgE-mediated triggering of
mast cells andsubsequent accumulation of inflammatorycells at sites
of antigen deposition
-
7/31/2019 1 Hypersensitivity Reactions
24/55
Immediate (type I) hypersensitivity
regulated mainly by the induction of TH2 helperT cells that
stimulate production of IgE (whichpromotes mast cell activation),
cause
accumulation of inflammatory cells (particularlyeosinophils),
and trigger secretion of mucus
clinical features result from release of mast cell
mediators as well as the eosinophil-richinflammation
-
7/31/2019 1 Hypersensitivity Reactions
25/55
Antibody-mediated (type II)hypersensitivity
caused by antibodies that react withantigens present on cell
surfaces or in theextracellular matrix
Intrinsic Ags Extrinsic Ags adsorbed on cell
surface/matrix
Resultant injury due to inflammation,complement- & Fc
receptor-dependentreactions
-
7/31/2019 1 Hypersensitivity Reactions
26/55
-
7/31/2019 1 Hypersensitivity Reactions
27/55
Antibody-mediated (type II)hypersensitivity
Occur in the following settings:
1) Transfusion reactions
cells from incompatible donor react with and are
opsonized by preformed antibody in the host
2) Hemolytic disease of the newborn(erythroblastosis
fetalis)
Maternal IgG Abs cross placenta & destroy fetalred cells
-
7/31/2019 1 Hypersensitivity Reactions
28/55
Antibody-mediated (type II)hypersensitivity
3) Autoimmune hemolytic anemia, agranulocytosis&
thrombocytopenia
Person with Abs against his own blood cells
4) Certain drug reactions
drug acts as a "hapten" by attaching to surfacemolecules of red
cells Abs are produced
against the drug-membrane protein complex
-
7/31/2019 1 Hypersensitivity Reactions
29/55
Antibody-mediated (type II)diseases
Autoimmune hemolytic anemia Autoimmune thrombocytopenic purpura
Pemphigus vulgaris Vasculitis caused by ANCA Goodpasture syndrome
Acute rheumatic fever Myasthenia gravis (Ab impairs receptor
function)
Graves disease (hyperthyroidism) (Ab stimulatesreceptor
function) Insulin-resistant diabetes Pernicious anemia
-
7/31/2019 1 Hypersensitivity Reactions
30/55
Immune complex-mediated (type III)hypersensitivity
Results from antigen-antibody complexesproducing tissue damage
by elicitinginflammation at the sites of deposition
ICs typically deposited in vessel walls
Some ICs in extravascular sites where Ag mayhave been "planted"
previously (in situ immunecomplexes)
Ags may be exogenous or endogenous Diseases may be systemic or
localized
-
7/31/2019 1 Hypersensitivity Reactions
31/55
Systemic immune complex disease
Prototype: Acute Serum Sickness
sequela to the administration of largeamounts of foreign serum
(e.g., serumfrom immunized horses used for protectionagainst
diphtheria)
-
7/31/2019 1 Hypersensitivity Reactions
32/55
Introduction of protein Ag
Formation of Abs after 1 week
Abs secreted into blood
1st phase: Abs react with Ag still present in blood, forming
Ag-Abcomplexes
2nd phase: circulating antigen-antibody complexes deposited in
various
tissues
3rd phase: Immune complexes initiate acute inflammatory reaction
(10 daysafter)
-
7/31/2019 1 Hypersensitivity Reactions
33/55
-
7/31/2019 1 Hypersensitivity Reactions
34/55
Systemic immune complex disease
Complexes of medium size are most pathogenic(slight Ag
excess)
Organs where blood is filtered at high pressureto form other
fluids, like urine and synovial fluid,are favored (glomeruli,
joints)
3
rd
phase: fever, urticaria, joint pains(arthralgias), lymph node
enlargement, andproteinuria appear
-
7/31/2019 1 Hypersensitivity Reactions
35/55
Systemic immune complex disease
complement-fixing Abs (i.e., IgG and IgM) andAbs that bind to
leukocyte Fc receptors (somesubclasses of IgG) involved
Consumption of complement in active phase ofdiseasedrop in serum
C3 level can be usedfor monitoring
Single exposure to Ag lesions resolve Prolonged exposure to Ag
results in chronic formof serum sickness (e.g. SLE)
-
7/31/2019 1 Hypersensitivity Reactions
36/55
Local immune complex disease (ArthusReaction)
localized area of tissue necrosis resulting fromacute immune
complex vasculitis, usuallyelicited in the skin
Injection of Ag in sensitized animal with circulating Abs vs the
Ag
Ag diffuses thru vascular wall, binds with Ab & forms immune
complexes
Complexes precipitate in vessel walls
Fibrinoid necrosis, thrombosis, ischemic injury
-
7/31/2019 1 Hypersensitivity Reactions
37/55
Immune complex vasculitis. The necrotic vessel wall is replaced
by smudgy, pink" "
-
7/31/2019 1 Hypersensitivity Reactions
38/55
Immune complex-mediated (type III)hypersensitivity
SLE nuclear antigens
PSGN - streptococcal cell wall antigen(s); may be "planted" in
glomerularbasement membrane
Polyarteritis nodosa HBV Ag in some cases Reactive arthritis
bacterial Ag (e.g. yersinia)
Serum sickness various proteins (e.g. foreign serum protein)
Arthus reaction - various proteins
-
7/31/2019 1 Hypersensitivity Reactions
39/55
T-Cell mediated (type IV)hypersensitivity
initiated by antigen-activated (sensitized) Tlymphocytes,
including CD4+ and CD8+ T cells
Adaptive immune system plays a vital role
(immune inflammation) Reactions by CD4+ T cells initially
called
delayed-type hypersensitivity (DTH)
Responsible for chronic reactions vs self-tissues
-
7/31/2019 1 Hypersensitivity Reactions
40/55
T-Cell mediated (type IV)hypersensitivity
phases:
Proliferation & differentiation of CD4+ T cells
Responses of Differentiated Effector T Cells
-
7/31/2019 1 Hypersensitivity Reactions
41/55
Proliferation & differentiation of CD4+ Tcells
Peptides displayed bydendritic cells, APCs
Nave CD4+ T cells
Secrete IL-2, proliferation ofAg-responsive forms
APCs produce cytokines
TH1 subsetmacrophage-mediated
reactions
TH2 subset-PMN-mediated
reactions
-
7/31/2019 1 Hypersensitivity Reactions
42/55
Responses of DifferentiatedEffector T Cells
Repeat exposure to antigen
Previously activated T cells respond to Ag presented by APCs
TH1 cells secrete IFN-
Macrophages activated,augmented power, secrete
more cytokines to amplify TH1response
Ag eliminated
TH17 secrete cytokines
Neutrophils & monocytesrecruited to the reaction
Promoted inflammation
-
7/31/2019 1 Hypersensitivity Reactions
43/55
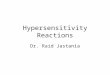
A, In delayed-type hypersensitivity reactions, CD4+ TH1 cells
(and sometimes CD8+ T cells, not shown) respond to tissue
antigensby secreting cytokines that stimulate inflammation and
activate phagocytes, leading to tissue injury. CD4+ TH17 cells
contribute to
inflammation by recruiting neutrophils (and, to a lesser extent,
monocytes).B, In some diseases, CD8+ cytotoxic T lymphocytes (CTLs)
directly kill tissue cells
C
-
7/31/2019 1 Hypersensitivity Reactions
44/55
T-Cell mediated (type IV)hypersensitivity
CD8+ CTLs kill antigen-bearing target cells
CTLs vs cell surface MHC Ags graft rejection
Kill virus-infected cells responsible for tissue
damage seen in infections (e.g. viral hepatitis) Involved in
tumor rejection
Killing mechanism involves perforins&
granzymes Cytokines also involved, notably IFN-
T C ll di d ( IV)
-
7/31/2019 1 Hypersensitivity Reactions
45/55
T-Cell mediated (type IV)hypersensitivity
Associated medical conditions
Type I diabetes mellitus -Antigens of pancreatic islet
cells(insulin, glutamic acid decarboxylase, others)
Crohn disease - Unknown antigen; role for commensal bacteria
Rheumatoid arthritis - Unknown antigen in joint synovium
Multiple sclerosis - Protein antigens in CNS myelin
Peripheral neuropathy, Guillain-Barr syndrome
- Protein antigens of peripheral nerve myelin Contact dermatitis
- Various environmental antigens (e.g., poison ivy)
T C ll di d ( IV)
-
7/31/2019 1 Hypersensitivity Reactions
46/55
T-Cell mediated (type IV)hypersensitivity
Tuberculin reaction
Injection of PPD/tuberculin
reddening and induration of the site appear in 8-
12 hours, peak in 24-72 hours, and thereafterslowly subside
accumulation of mononuclear cells, mainlyCD4+ T cells and
macrophages, aroundvenules, producing perivascular "cuffing"
-
7/31/2019 1 Hypersensitivity Reactions
47/55
intradermal injection of exactly one tenth of a milliliter (mL)
of PPD tuberculin
-
7/31/2019 1 Hypersensitivity Reactions
48/55
size of induration is measured 4872 hours later; erythema
(redness) should not bemeasured
-
7/31/2019 1 Hypersensitivity Reactions
49/55
-
7/31/2019 1 Hypersensitivity Reactions
50/55
A, Perivascular infiltration by T cells and mononuclear
phagocytes.
B, Immunoperoxidase staining reveals a predominantly
perivascular cellular infiltrate that markspositively with
antibodies specific to CD4.
T C ll di t d (t IV)
-
7/31/2019 1 Hypersensitivity Reactions
51/55
T-Cell mediated (type IV)hypersensitivity
Granulomatous inflammation
With persistent nondegradable Ag (e.g. TB)
Activated macrophagesepithelioid cells
associated with strong T-cell activation withcytokine
production
an also be caused by foreign bodies thatactivate macrophages
without eliciting an
adaptive immune response
-
7/31/2019 1 Hypersensitivity Reactions
52/55
A section of a lymph node shows several granulomas, each made up
of an aggregate of
epithelioid cells and surrounded by lymphocytes. The granuloma
in the center showsseveral multinucleate iant cells.
T C ll di t d (t IV)
-
7/31/2019 1 Hypersensitivity Reactions
53/55
T-Cell mediated (type IV)hypersensitivity
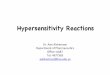
Contact dermatitis
may be evoked by contact with urushiol (Agcomponent of poison
ivy or poison oak)
vesicular dermatitis
-
7/31/2019 1 Hypersensitivity Reactions
54/55
-
7/31/2019 1 Hypersensitivity Reactions
55/55
Contact dermatitis. The lesion shows an epidermal blister
(vesicle) with