Embed Size (px)
Citation preview

Re-visiting Hypersensitivity Reactions to Taxanes:A Comprehensive Review
Matthieu Picard & Mariana C. Castells
# Springer Science+Business Media New York 2014
Abstract Taxanes (a class of chemotherapeutic agents)are an important cause of hypersensitivity reactions(HSRs) in cancer patients. During the last decade, thedevelopment of rapid drug desensitization has been keyto allow patients with HSRs to taxanes to be safely re-treated although the mechanisms of these HSRs are notfully understood. Earlier studies suggested that solvents,such as Cremophor EL used to solubilize paclitaxel,were responsible for HSRs through complement activa-tion, but recent findings have raised the possibility thatsome of these HSRs are IgE-mediated. Taxane skintesting, which identifies patients with an IgE-mediatedsensitivity, appears as a promising diagnostic and riskstratification tool in the management of patients withHSRs to taxanes. The management of patients followinga HSR involves risk stratification and re-exposure couldbe performed either through rapid drug desensitizationor graded challenge based on the severity of the initialHSR and the skin test result. Rapid drug desensitizationhas been shown to be an effective and safe method tore-introduce taxanes in hundreds of patients, includingthose with life-threatening HSRs. Patients with non-severe delayed skin HSRs may benefit from rapid drugdesensitization since they may be at increased risk foran immediate HSR upon re-exposure. This review fo-cuses on the clinical presentation, diagnosis, and novelmechanisms of immediate HSRs to taxanes. A newmanagement strategy for HSRs to taxanes based on skintesting and rapid drug desensitization is proposed.
Keywords Taxane . Paclitaxel . Taxol . Docetaxel .
Taxotere . Nab-paclitaxel . Abraxane . Cabazitaxel .
Chemotherapy . Hypersensitivity . Allergy . Skin test .
Desensitization . Challenge . Diagnosis . Review . IgE .
Complement . Mechanism
Introduction
Hypersensitivity reactions (HSRs) to chemotherapy are in-creasingly common and represent an important impedimentto the care of cancer patients as they may entail seriousconsequences and prevent patients from being treated withthe most efficacious agent against their cancer [1]. During thelast decade, different groups have developed rapid drug de-sensitization (RDD) protocols that allow the safe re-introduction of a chemotherapeutic agent to which a patientis allergic, and their use have recently been endorsed by theNational Comprehensive Cancer Network (NCCN) [2].
Two classes of chemotherapeutic agents cause the vastmajority of chemotherapy-related HSRs: platins and taxanes[3]. Although it has now been well described that HSRs toplatins are IgE-mediated [4], the mechanism(s) of HSRs totaxanes remain to be established. This lack of a clear under-standing of what causes HSRs to taxanes has led in practice toa greater diversity of management strategies for taxanes com-pared with platins’ HSRs [5]. However, the possibility that anIgE-mediated mechanism might be implicated in some pa-tients with HSRs to taxanes has recently been raised, and skintesting has emerged as a new diagnostic and risk stratificationtool [6, 7]. Therefore, the need arose to re-visit the knowledgeacquired on HSRs to taxanes since the first use of the drug inthe late 1980s.
This review provides a general overview of the differenttaxanes currently used in practice as well as a presentation ofthe different types of HSRs encountered with these agents
M. Picard :M. C. Castells (*)Division of Rheumatology, Immunology and Allergy, Department ofMedicine, Brigham andWomen’s Hospital, HarvardMedical School,1 Jimmy Fund Way, Smith Building, Boston, MA 02115, USAe-mail: [email protected]
Clinic Rev Allerg ImmunolDOI 10.1007/s12016-014-8416-0

(with a focus on immediate HSRs). This is followed by adiscussion of the different mechanisms that could account forthese HSRs. Finally, the different strategies used in the man-agement of HSRs to taxanes (with an emphasis on rapid drugdesensitization) are reviewed.
Origins and Clinical Use of Taxanes
Paclitaxel
Paclitaxel (taxol) is a natural compound, originally isolatedfrom the bark of the Pacific yew tree (Taxus brevifolia) in the1960s, with potent anticancer properties [8]. It exerts itsantineoplastic effects by interfering with the dynamics ofmicrotubules (components of the cell cytoskeleton) therebycausing mitotic block and cell death [9, 10]. Taxol rarity innature (the extraction of a single therapeutic dose necessitatesthe sacrifice of a 100-year-old Pacific yew tree) and its insol-ubility in water significantly hindered its development as achemotherapeutic agent [11]. In the 1980s, a drug formulationsuitable for intravenous injection was devised usingCremophor EL (polyoxyethylated castor oil), a solubilizerand emulsifying agent, and ethanol allowing clinical trials toproceed [12]. Following demonstration of its efficacy againstnotably ovarian and breast cancer, the need arose for a moresustainable and efficient mean of production. Total (synthetic)synthesis of paclitaxel was accomplished in 1994, but itscomplexity made it not commercially viable [11, 13]. A firstsolution came from the presence of paclitaxel precursors (10-deacetylbaccatin III and baccatin III), which can be trans-formed via a semisynthetic process into paclitaxel, in theneedles of the European yew tree (Taxus baccata) (Fig. 1)[12]. European yew trees are more abundant than Pacific yewtrees, and the needles can be harvested without killing the tree[12]. In recent years, plant cell cultures isolated from differentTaxus species and grown in large bioreactors have become themethod of choice for paclitaxel production [12]. Paclitaxel isused for the treatment of ovarian, breast, non-small cell lungcancers, and AIDS-related Kaposi’s sarcoma. It is either in-fused weekly, typically over 1 h, or every 3 weeks, typicallyover 3 h [14].
Docetaxel
Docetaxel (taxotere) was discovered in 1986 in the search fora more soluble and easier to produce alternative to paclitaxel[12]. It was obtained from a semisynthetic process using thepaclitaxel precursor 10-deacetylbaccatin III extracted from theneedles of T. baccata [12]. Its structure is therefore highlysimilar to paclitaxel. Despite a higher solubility than paclitax-el, the molecule remains insoluble in water [12]. Docetaxel isformulated in polysorbate 80 (Tween 80), a solubilizer and
emulsifying agent, and further diluted in an ethanol/watersolution for intravenous administration [15]. It is used in thetreatment of breast, ovarian, prostate, head and neck, and non-small cell lung cancers and gastric adenocarcinoma [15].Docetaxel is usually administered as a 1-h infusion every3 weeks [15].
Nab-Paclitaxel
Nanoparticule albumin-bound paclitaxel (nab-paclitaxel;Abraxane) is a novel paclitaxel formulation, which does notcontain Cremophor EL [16, 17]. It uses human serum albuminto encapsulate hydrophobic paclitaxel molecules in particlesof around 130 nm [18]. In addition, albumin is thought toincrease paclitaxel tumor uptake by, among other mecha-nisms, binding to gp60 (albondin) receptor thereby enhancingthe transendothelial transport of the drug [18, 19]. Abraxanewas approved by the US FDA for the treatment of metastaticbreast cancer in 2005 and is now also approved for thetreatment of non-small cell lung cancer and adenocarcinomaof the pancreas [20, 21]. It is infused over 30 min and, in
Fig. 1 a Taxus baccata tree. b Taxus baccata needles and fruit. Picturestaken at Arnold Arboretum, Boston, MA
Clinic Rev Allerg Immunol

contrast to the other taxanes, does not require the use ofpremedication to prevent HSR [21]. Many other nanoparticuledelivery systems for paclitaxel are currently in development[20].
Cabazitaxel
Cabazitaxel (Jevtana) is a semisynthetic taxane derived fromthe precursor 10-deacetyl baccatin III contained in yew treeneedles that was developed to overcome tumor drug resistanceto paclitaxel and docetaxel [22]. Tumor cells can overexpressATP-dependant membrane transporter proteins, such as P-glycoprotein, that decrease intracellular drug concentrationsby pumping out of the cell drugs with affinity for the trans-porter [10]. Paclitaxel and docetaxel have a high affinity for P-glycoprotein whereas cabazitaxel has a poor affinity providingthe rationale for its use in certain taxane-resistant neoplasia[22]. Similarly to docetaxel, it is formulated in polysorbate 80and diluted in an ethanol/water solution before intravenousadministration [23]. In 2010, it was approved by the US FDAin combination with prednisone for the treatment of hormone-resistant metastatic prostate cancer in patients previously treat-ed with docetaxel [22]. It is usually infused every 3 weeksover 1 h [23].
Hypersensitivity Reactions to Taxanes
Incidence of Immediate Hypersensitivity Reactionsand Impact of Premedication
Paclitaxel
Early phase I clinical trials of paclitaxel were complicated by ahigh incidence of HSRs occurring during the drug infusion(immediate HSR) [24, 25]. Premedication with corticosteroids(oral dexamethasone 20 mg 12 and 6 h pretaxol) and antihis-tamines (histamine (H)-1 (dyphendydramine 50 mg or equiv-alents) and H2 (cimetidine 300 mg or ranitidine 50 mg) re-ceptor blockers) administered intravenously 30 to 60 minpretaxol allowed for a dramatic reduction in their incidence[14, 24, 26]. Immediate HSRs to paclitaxel occur in around10 % of premedicated patients and are severe in around 10 %of patients who react [27–38]. A simplified premedicationregimen consisting of a single intravenous or oral dexameth-asone dose (10 mg) given 30–60 min before paclitaxel hasbeen used with success by various groups without an obviousrise in immediate HSRs and has since gained wide acceptanceas a reasonable alternative to the two-dose dexamethasoneprotocol [27–30, 33, 36]. However, at least one retrospectivestudy reported a statistically significant lower rate of immedi-ate HSRs with the two-dose dexamethasone regimen com-pared to the simplified regimen (p=0.047); 7.5 % (0.9 %
severe) versus 17.3 % (7.3 % severe) [34]. Also, at least onedeath from a severe HSR has been reported in a patientpremedicated with the simplified regimen [39]. Inpremedicated patients, the duration of the paclitaxel infusion(3 versus 24 h) and the dose administered (175 versus 135mg/m2) do not influence the rate of HSRs [37, 40, 41]. Also, thereis no indication that weekly paclitaxel regimens, which con-tain lower doses and are administered as 1-h infusions, in-crease the rate of HSRs, and some groups have even success-fully withdrawn corticosteroid premedication in patients thathad not reacted during the initial cycles [42–46].
Docetaxel
Several unexpected adverse events were uncovered duringphase II trials of docetaxel. A majority of patients (>50 %)experienced immediate HSRs that were not prevented by theaddition of premedication with antihistamines or intravenouscorticosteroid 30 min prior to the infusion [47–50]. Fluidretention, which was later found to be caused by capillaryprotein leak induced by docetaxel [51], was an importantcause for treatment withdrawal in phase II studies and ap-peared to be related to the cumulative docetaxel dose [52].Finally, many patients experienced a variety of toxic skinreactions presenting as desquamative rash, hand-foot syn-drome, and plaque-l ike erythrodysesthesia [52].Premedication with oral dexamethasone 8 mg twice daily for3 days starting the day before the infusion was thereafteradopted as the standard premedication regimen and found togreatly reduce the prevalence of fluid retention and immediateHSRs to between 3.5–16.5 % and to around 5 %, respectively[53–55]. The impact of premedication on toxic skin reactionsis less clear as its prevalence has been found to vary greatlybetween different trials [56, 57]. In an effort to minimize theadverse effects of corticosteroids, different protocols havebeen used to reduce the duration of dexamethasone treatmentin patients receiving weekly docetaxel regimens without adeleterious impact on the rate of HSRs, fluid retention, andskin toxicity [58, 59].
Nab-Paclitaxel
Since nab-paclitaxel is devoid of Cremophor EL, thesuspected cause of taxol HSRs, it is administered withoutany premedication and as a 30-min infusion [21]. In a phaseIII trial, a direct comparison between nab-paclitaxel and taxol(administered with premedication) revealed that the rate ofHSRs was higher in the taxol arm;12 versus 4 %, severeHSRs; 4 versus 0 % [60, 61]. However, postmarketing sur-veillance has revealed cases of severe and even fatal HSRswith nab-paclitaxel [21]. Its use in patients with a history ofmild to severe HSR to taxol and/or docetaxel has been report-ed to be safe in a few case reports [62–65].
Clinic Rev Allerg Immunol

Cabazitaxel
Cabazitaxel has mostly been studied in patients with metasta-tic castration-resistant prostate cancer (mCRPC) previ-ously treated with docetaxel and in combination with adaily oral prednisone regimen [66]. Premedication withan intravenous corticosteroid (dexamethasone 8 mg) andH1 (dyphendydramine 25 mg) and H2 (ranitidine50 mg) blockers at least 30 min before the infusion isrecommended given its potential to cause HSRs [23].However, no HSR were reported in at least two trials cumu-lating 656 patients treated with cabazitaxel for mCRPC [67,68]. Interestingly, a large phase III trial in which 662 men withmCRPC were treated with docetaxel in combination withdaily prednisone also did not report any HSR [69]. In contrast,a phase II study of 71 patients with metastatic breast cancerresistant to taxanes (docetaxel and paclitaxael) found that 6 %of patients suffered a HSR to cabazitaxel [70]. Gender differ-ences and/or a higher and more prolonged intake of cortico-steroids in men with mCRPC could possibly account for thisdiscrepancy.
Non-Immediate Hypersensitivity Reactions to Taxanes
Although less common than immediate HSRs, a range ofdelayed, possibly immune-mediated, reactions have been de-scribed with taxanes. Importantly, delayed onset skin erup-tions (most commonly a benign maculopapular rash) can bethe prelude to an immediate HSR during the next infusion [7].In one case, a 37-year-old woman that had presented withurticaria, lip swelling, and fever 10 days after her first pacli-taxel infusion suffered a fatal anaphylactic reaction shortlyafter the start of the second infusion despite premedication[71]. Stevens-Johnson syndrome (SJS) and toxic epidermalnecrolysis (TEN) have also been described in case reports andpicked up in postmarketing surveillance with paclitaxel, do-cetaxel, and nab-paclitaxel [21, 72, 73]. Acute interstitialpneumonitis has been reported with paclitaxel, docetaxel,and more recently nab-paclitaxel and usually presents withfever, dry cough, dyspnea, bilateral interstitial lung infiltrates,and leukocytosis [74–77]. Around half of patients described incase reports required mechanical ventilation, and the mortalityrate was high [75]. Patients are usually treated with high-dosecorticosteroids for several weeks as the pneumonitis is thoughtto be T-cell mediated [78]. In a recent trial of nab-paclitaxeland gemcitabine in pancreatic cancer, 4 % of patients in thenab-paclitaxel/gemcitabine arm developed pneumonitiswhereas only 1 % did in the gemcitabine arm [77].Moreover, two patients in the nab-paclitaxel/gemcitabinearm died as a result [21]. Subacute cutaneous lupus erythe-matosus (SCLE), which presents as a photodistributed skineruption often accompanied by the presence of antiRo/SSAantibodies, has been associated with paclitaxel, docetaxel, and
nab-paclitaxel [79–81]. Drug discontinuation usually leads toa complete resolution [80].
Clinical Features of Immediate Hypersensitivity Reactionsto Taxanes
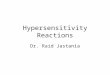
The majority of immediate HSRs to taxanes occurs during thefirst or second infusion of the drug and usually developswithin minutes of starting the infusion [26, 33, 82]. The signsand symptoms of these reactions are thought to be the result ofbasophil/mast cell degranulation (Fig. 2) and are similar inpremedicated and non-premedicated patients [3, 26, 33, 82].Patients commonly complain of localized or generalizedflushing, and a significant percentage report chest, back,and/or abdominal pain [3, 26, 82]. Respiratory and throatsymptoms (dyspnea, chest tightness, wheezing, throat tight-ness) can be prominent and associated with a significant dropin oxygen saturation [3, 26, 82]. Cardiovascular involvementrange from acute hypertension to hypotension, and patientsmay report a sense of impending doom [3, 26, 82]. Finally,gastrointestinal symptoms (nausea, vomiting, diarrhea) oftenaccompany these HSRs [3, 26, 82]. Following the discontin-uation of the infusion, rapid resolution is the norm althoughpatients with protracted courses (sometimes unresponsive toepinephrine) and biphasic reactions have been seen [26, 33,83, 84]. As of 2009, mortality from severe anaphylactic reac-tions had been reported in 54 % of 290 docetaxel cases and in29 % of 683 paclitaxel cases recorded by the US FDA [83].
Mechanisms of Immediate Hypersensitivity Reactionsto Taxanes
Three different mechanisms may account for immediateHSRs to taxanes: (1) complement activation induced byCremophor EL (compounded with paclitaxel) and poly-sorbate 80 (compounded with docetaxel) which generates
Fig. 2 Clinical features of immediate HSRs to taxanes. Created with datafrom J Allergy Clin Immunol. 2008;122:574–80 and Gynecol Oncol.2005;99:393–9
Clinic Rev Allerg Immunol

anaphylatoxins triggering basophil/mast cell activation [85,86]; (2) histamine release through a direct but undefined effectof paclitaxel on basophils [87]; (3) an IgE/IgG-mediatedmechanism directed against either the taxane moiety (pacli-taxel, docetaxel) or the solvent (Cremophor EL, polysorbate80) (Fig. 3) [6, 88–92].
Paclitaxel (compounded with Cremophor EL) has beenshown to cause a marked complement activation in vitro in4/10 healthy subjects and 5/10 cancer patients at a concentra-tion of 100 μg/ml, which translates into a Cremophor ELconcentration of 8.8 mg/ml [85]. In comparison, the maximalserum concentration of Cremophor EL reached with a 3-hpaclitaxel infusion at a dose of 175 mg/m2 averages 3 mg/ml[93]. Furthermore, Cremophor EL alone was found to triggercomplement activation to the same extent that paclitaxel/Cremophor EL did at equivalent concentrations suggestingthat Cremophor EL is solely responsible for this effect [85].Similarly, docetaxel (compounded with polysorbate 80) andpolysorbate 80 alone have been shown to cause complementactivation in vitro [86]. These findings support the role ofthese emulsifying agents in triggering complement activationin a high proportion of healthy subjects and thereby to causeimmediate HSRs through anaphylatoxin production.However, it remains to be demonstrated that complementactivation occurs in vivo in humans who react to taxanesand that this mechanism accounts for patients who reactdespite premedication and a slower infusion rate.
Essayan et al. reported the case of an ovarian cancer patientthat had suffered repeated immediate HSRs to paclitaxelstarting with the first infusion [87]. Premedication and asignificant reduction in the infusion rate did not prevent re-currences, and she received subsequent infusions through adesensitization protocol. Basophil activation tests on purifiedbasophils were performed on the patient and three healthycontrols with paclitaxel alone and Cremophor EL alone [87].They found that paclitaxel without Cremophor EL inducedhistamine release from basophils in the patient and the threehealthy controls at a concentration 10- to 100-fold higher thanthe expected paclitaxel serum concentration. In this study,Cremophor EL did not induce any histamine release, whichmight be explained by the fact that experiments were likelyconducted in a decomplemented medium [85]. Also, paclitax-el did not induce any histamine release from purified humanskin mast cells [87]. The authors therefore hypothesize thatpaclitaxel and not Cremophor EL might cause immediateHSRs by triggering basophil activation through a non-IgE-mediated mechanism. However, these findings also fail toidentify a mechanism that differentiates highly reactive pa-tients from healthy controls, which are likely to toleratetaxanes if given premedication.
More recently, Prieto-Garcia and Pineda de la Losa de-scribed a patient that had suffered a severe anaphylactic reac-tion within seconds of her second lifetime paclitaxel infusion[6]. The patient had a positive intradermal skin test (IDT) to
Fig. 3 Mechanisms of immediate HSRs to taxanes. The taxane moietymay cause mast cell and/or basophil activation through three differentmechanisms: (1) a direct but undefined action on basophils but not mastcells; (2) an IgE-mediated mechanism, or (3) an IgG-mediated mecha-nism that causes complement activation through immune complex for-mation leading to the production of anaphylatoxins (C3a and C5a) thatcan activate basophils and mast cells through their surface receptors.Solvents may cause mast cell and/or basophil activation through two
different mechanisms: (1) an IgE-mediated mechanism or (2) directcomplement activation that leads to the production of anaphylatoxins.Following activation, mast cells and basophils release a variety of medi-ators that can be measured (serum tryptase or 24-h urinarymethylhistamine), and the actions of which can be pharmaceuticallyblocked (histamine antihistamines; LTC4 montelukast; PGD2 aspirin).LTC4 leukotriene C4. PGD2 prostaglandin D2
Clinic Rev Allerg Immunol

paclitaxel at a concentration of 0.1 μg/ml (0.0001 mg/ml). Incontrast, 15 patients with adverse reactions to paclitaxel wereskin-test negative to paclitaxel up to a concentration of6 mg/ml (SPT) and 1 mg/ml (IDT) [6]. Furthermore, an IgEdot-blot assay performed with the patient’s serum waspositive to paclitaxel and negative to Cremophor EL [6].The assay performed with serum from a non-allergiccontrol was negative to paclitaxel and Cremophor EL[6]. Other groups have also reported positive skin testresults to paclitaxel and docetaxel performed at non-irritating concentrations [7, 88, 89]. Also, cases of IgE-mediated reactions to Cremophor EL and polysorbate 80(based on positive skin test results to these molecules andnot the active drug) have been reported upon the admin-istration of non-taxane drugs raising the possibility thatthis may also happen in some cases of immediate HSRs totaxanes [90–92]. Altogether, these findings strongly sup-port that at least in some patients, an IgE-mediated mech-anism may mediate immediate HSRs to taxanes.
It seems difficult to reconcile the fact that most patientsreact upon the first or second exposure (leaving a littleopportunity for sensitization) with an IgE-mediatedmechanism. This conundrum could potentially be ex-plained by the fact that sensitivity to taxanes can developwithout exposure to the drug, possibly via pollen expo-sure [94]. Paclitaxel and the precursors for docetaxel(baccatin III and 3-deacetylbaccatin III) have been isolat-ed from different species of yew trees and from differentparts of the plant including its pollen [94]. Interestingly,paclitaxel-specific IgG were found in the serum of 8.8 %of 63 healthy blood donors from Belgium (whereT. baccata is widespread) despite having never been ex-posed to the drug [94]. Among atopic blood donors (de-fined as sensitive to Betula species), this percentage in-creased to 21.4 %. In contrast, paclitaxel-specific IgGswere not detected in 50 healthy blood donors from thesouthern hemisphere (where yew trees do not grow) [94].There is evidence in some patients reactive to the heparinantidote, protamine, that drug-specific IgGs (in combina-tion with complement) can mediate immediate HSRs[95–97]. Although this mechanism has not been exploredin taxane HSRs, it may turn out to be relevant. Anotherpossibility is that paclitaxel-specific IgE are produced inpatients exposed to yew tree pollen. In this regard, theallergenic potential of yew tree pollen has been shown intwo different populations. In a study from Japan, 5/18patients with springtime allergic rhinitis showed sensitiv-ity to the Taxus cuspidata pollen as demonstrated by IgEimmunoblotting and, in a study from Italy, 27 % of 562patients allergic to the Cupressacea (cypress) pollen had apositive prick test to a T. baccata pollen extract [98, 99].The possibility that patients may develop IgE and/or IgGsensitivity to taxanes through pollen exposure and then
suffer an immediate HSR upon their first taxane exposurerequires further investigation. Nonetheless, it provides arationale for the use of taxane skin testing in the evalua-tion of patients with HSRs to taxanes.
Management of Hypersensitivity Reactions to Taxanes
As previously described, there are different types of HSRs totaxanes (immediate and non-immediate reactions), each ofwhich may vary in severity. These factors along with thebenefits expected from this treatment and the availability,effectiveness, and toxicity of alternative agents for a particularpatient will together influence the decision to discontinue orre-introduce the medication. As a general rule, severe non-immediate HSRs (SJS/TEN; pneumonitis) should lead to drugdiscontinuation however compelling the indication to pursuetreatment [100]. On the other hand, the management ofnon-severe delayed onset skin eruptions is less clearalthough data suggest that safe re-introduction can beachieved [7]. Importantly, since in some patients thesedelayed reactions can be the prelude to potentially se-vere immediate HSRs [71], precautions (such as the useof a rapid desensitization protocol) may be necessary incertain circumstances.
Since paclitaxel first clinical use in the 1980s, differentapproaches have been put forward to safely re-introducetaxanes in patients who suffered immediate HSRs and forwhich the causal agent was considered the best therapeu-tic option. In this section, we will review the datasupporting each approach as well as their potential short-comings before proposing a management strategy forimmediate and non-severe delayed HSRs based on thecurrently available evidence. The severity of immediateHSRs will be graded according to the classification pro-posed by Brown et al. (Table 1) [101].
Table 1 Severity grading system of immediate HSRs
Grade Severity Description
1 Mild Symptoms are limited to the skin (e.g., flushing)or involve a single organ/system and are mild(e.g., mild back pain).
2 Moderate Symptoms involve at least two organs/systems(e.g., flushing and dyspnea), but there is nosignificant drop in blood pressure or inoxygen saturation.
3 Severe Symptoms typically involve at least two organs/systems, and there is a significant drop inblood pressure (systolic ≤90 mmHg and/orsyncope) and/or oxygen saturation (≤92 %).
Adapted from Brown et al. [101]
Clinic Rev Allerg Immunol

Re-challenge
Weiss et al. reported the first cohort of patients with immediateHSRs to paclitaxel to undergo re-treatment with the drug [26].These patients were enrolled in different phase I trials ofpaclitaxel sponsored by the National Cancer Institute and werethus not premedicated. Among twenty-seven patients withdefinite immediate HSRs to paclitaxel (of which at least41 % had been severe), all underwent re-challenge withpremedication [26]. Eleven patients (41 %) had a recurrentHSR (one of which died as result), and seven of these patientsthat had reacted despite premedication tolerated subsequentpaclitaxel infusions without additional precautions [26]. In1993, Peereboom et al. described a re-challenge procedurefor patients with immediate HSRs despite premedication in acase series of eight patients [102]. Patients, which had expe-rienced grade 2 to 3 HSRs to paclitaxel, were re-challengedwithin 24 h of their initial HSR following additional doses ofdexamethasone and antihistamines, and the rate of the pacli-taxel infusion was progressively increased so that the infusionextended over 24 h. Three patients experienced minor symp-toms during the re-challenge procedure although, surprisingly,all seven tolerated a subsequent paclitaxel infusion despiteusing the same premedication regimen and infusion rate asduring the original infusion that had triggered the HSR [102].Other groups have also reported a high success rate using aprogressive 24-h paclitaxel infusion starting at 1–2 mg/h andslowly increasing the rate so as to complete the infusion over aperiod of 24 h [28, 31, 34]. Most groups administer anadditional dose of dexamethasone following the initial HSRand before the first re-infusion and perform subsequent pacli-taxel infusions using a standard premedication regimen and aprogressive 24-h infusion [28, 31, 34]. Whether this protocolis effective because it induces a certain degree of desensitiza-tion or because the maximal serum concentration of paclitaxeland/or Cremophor EL reached is below the threshold forbasophil/mast cell activation remains unknown. However,for practical reasons and because they carry a higher risk offebrile neutropenia, 24-h infusions are rarely performednowadays [40].
Markman et al. developed a slightly different strategy forre-treating patients with immediate HSRs to paclitaxel [33].Following an immediate HSR, the infusion was stopped andthe patient treated with intravenous corticosteroids and anti-histamines. Upon complete resolution (usually within30 min), the infusion was resumed at the previous rate.Subsequent infusions were given without any modificationof the premedication or the infusion rate. Among 44 patientswith mostly grades 1 and 2 HSRs, 43 agreed to the re-challenge procedure and one patient with a grade 3 reactionrefused. These 43 patients experienced a total of 70 HSRssince some patients reacted on subsequent infusions despitehaving tolerated the rapid re-challenge procedure. The rapid
re-challenge procedure allowed completing the paclitaxel in-fusion in 93 % of HSRs (65/70).
The experience with docetaxel is more limited. Schrijverset al. showed that premedication with corticosteroids starting12 h before the infusion along with antihistamines couldsuccessfully prevent grade 1 or 2 HSRs to docetaxel in 13/14 patients [47]. Markman et al. used a rapid re-challengeapproach (similar to the one described above for paclitaxel) in17 patients with HSRs to docetaxel [103]. All were able tocomplete every docetaxel infusion although one patient optedto discontinue treatment since she had reacted during each ofthe first three infusions. In contrast, a more recent studyshowed that 16/43 patients (34 %) re-challenged to docetaxelhad a recurrent HSR, and other groups have also reportedfailures of the rapid re-treatment strategy or of the progressive24-h infusions creating the need for alternative methods tosafely re-introduce taxanes in reactive patients [55, 104–106].
Changing to a Different Taxane
Paclitaxel and Docetaxel Cross-Reactivity
In 1998 and 2000, two case series described a total of sevenpatients with immediate HSRs to paclitaxel that did not reactwhen treated with docetaxel suggesting that cross-reactivitybetween taxanes was low or even non-existent [107, 108].However, one of the case series did not include any severeHSR to paclitaxel, [108] and in the other, the severity of thereactions was not described [107]. Dizon et al. reviewed allcases of severe HSRs to taxanes (defined as severe enough tojustify withdrawing the medication) at their institution over aperiod of 5 years [109]. They identified 16 patients with asevere HSR to paclitaxel of which 10 were treated withdocetaxel. Among those 10 patients, three had experienced agrade 3 HSR and seven a grade 2 HSR to paclitaxel. Upontheir first docetaxel infusion, 9/10 patients suffered a HSR(grade 2—8 and grade 1—1) indicating a 90 % cross-reactivity rate in their population. In this cohort, no patientthat had not had a prior HSR to paclitaxel had a severe HSR todocetaxel. More recently, Sanchez-Munoz et al. performed asimilar study and found that 3/8 patients switched from pac-litaxel to docetaxel and 4/9 patients switched from docetaxelto paclitaxel because of a severe HSR had a recurrent reaction[110]. It appears that the cross-reactivity rate between pacli-taxel and docetaxel varies among different populations andthat the severity of the initial HSR may influence this rate.
Paclitaxel, Docetaxel, and nab-Paclitaxel Cross-Reactivity
Fader et al. published a case series of five patients with grade 3HSRs to paclitaxel that all tolerated nab-paclitaxel [64]. Fourother patients with HSRs to paclitaxel and/or docetaxel (twoof which with grade 3 HSRs) have been reported to tolerate
Clinic Rev Allerg Immunol

nab-paclitaxel in the literature [62, 63, 65]. To our knowledge,some patients have reacted to nab-paclitaxel following a HSRto paclitaxel, and caution should be exercised if such a switchis desired. Finally, it should be mentioned that taxanes are notnecessarily equivalent to one another from an oncologic stand-point and regarding their general adverse effect profile[54, 60]. Therefore, the decision to change from onetaxane to another should not be based solely on the riskof cross-reactivity.
Desensitization Protocols
Essayan et al. performed the first desensitization to paclitaxelon a patient with a grade 3 HSR who had failed re-challengewith a progressive 24-h infusion [87]. The desensitizationprotocol was based on the one used in penicillin-allergicpatients and consisted of administering doubling doses ofpaclitaxel every 15 min starting with a 1-ml volume of asolution diluted 100, 000-fold compared with the final solu-tion. The protocol had 20 steps that preceded infusion of theundiluted final solution. The patient received three desensiti-zations and had minor symptoms that did not require anytreatment during each of them starting with a dose as low as2 ml of a 1,000-fold diluted solution. This report highlightedthe important role that desensitization could play in patientshighly reactive to paclitaxel and that had failed other methodsof drug re-introduction.
Markman et al. devised a desensitization protocol for pa-tients that failed their rapid re-challenge procedure mentionedabove [33]. Patients treated with this protocol were givendoses of dexamethasone starting 36 h before the procedureand received their paclitaxel infusion as follows: 2 mg/100 mlover 30 min followed by 10 mg/100 ml over 30 min and theremainder of the dose in 500 ml over 3 h. The first solution isapproximately a 30-fold dilution of the final concentrationtranslating into a 5-fold increase in concentration betweenbags. Nine patients were treated with this protocol, and eightdid not have any HSR. The patient that reacted was able tocomplete the infusion following the treatment of the HSR anda 30-min pause in the infusion. It should be noted that in thiscohort, most patients had a non-severe HSR to paclitaxel andthat one patient with a grade 3 HSR was not offered re-challenge and/or desensitization.
Robinson et al. proposed another desensitization protocolfor paclitaxel in which the total dose is diluted in a 1-l baginfused at an initial rate of 3–6 ml/h that is gradually increasedby 6 ml/h every 10–15 min until a final rate of 42 ml/h isreached [82]. The desensitization lasts around 24 h. Eightpatients were treated with this protocol (seven of which hadhad a severe HSR to paclitaxel) and four (50 %) had break-through reactions, one of which was severe and led to defin-itive paclitaxel discontinuation. The three other reactive pa-tients were able to receive the remainder of the paclitaxel dose
following the treatment of the reaction. In comparison, theprotocol used by Markman et al. administered a higher initialdose of paclitaxel, increased the dose more abruptly, andreached a much higher final rate than the protocol ofRobinson et al. and yet seemed more effective at preventingHSRs. Other small cohorts of ≤10 patients desensitized totaxanes have been described using a variety of protocols witha generally good success rate [55, 88, 89]. The diversity andsometimes-conflicting nature of the data show the need tovalidate desensitization protocols in a large number of patientsthat includes patients with severe HSRs and ideally in differ-ent populations to reliably establish their safety and efficacy.
Rapid Drug Desensitization
Safety and Efficacy In 2005, Feldweg et al. (from Brighamand Women’s Hospital/Dana-Farber Cancer Institute; BWH/DFCI) reported on the use of a 6- to 7-h rapid drug desensi-tization (RDD) protocol for patients with HSRs to paclitaxeland/or docetaxel [106]. Seventeen patients (eight with grade 3HSRs to paclitaxel and nine with grade 2 HSRs to paclitaxel,three of which also had a grade 2 HSR to docetaxel) weretreated with the RDD protocol described in detail below. Fivepatients had failed a re-challenge with a slower infusion rate,and one patient had failed a change from paclitaxel to doce-taxel prior to being referred to allergy for RDD. A total of 77desensitization procedures were performed, and four patients(24 %) had a breakthrough HSR most commonly during theirfirst desensitization. Three of them had a very minor HSR thatdid not recur on subsequent desensitizations following adjust-ments to the protocol that included reducing the final infusionrate. The other patient had minor flushing during the proce-dure, but 6 h after its completion, she had a severe HSR withhypotension that required epinephrine treatment. She decidednot to receive paclitaxel thereafter.
Two other studies have confirmed the safety and efficacy ofthe RDD protocol in patients reactive to paclitaxel and/ordocetaxel [3, 111]. Lee et al. reported on the outcome of 114desensitization procedures to paclitaxel in 22 patients [111].Breakthrough HSRs occurred in six patients (27 %) in a totalof nine procedures (8 %). Only one breakthrough HSR wassevere being associated with hypotension, but all desensi-tization procedures allowed the administration of thetotal dose. In addition, two desensitizations to docetaxelwere performed in one patient uneventfully. In a studyon 413 desensitizations to chemotherapy that mainlyinvolved platins and taxanes, 28 patients underwent140 intravenous and 12 intraperitoneal desensitizationprocedures to paclitaxel [3]. An important finding wasthat most breakthrough reactions occurred during thefirst desensitization and that their incidence dramaticallyreduced thereafter. These reactions were all less severethan the initial HSR, and only one required epinephrine
Clinic Rev Allerg Immunol

treatment. Importantly, all patients were able to safelyreceive their full treatment. Further evidence of thesafety and efficacy of this protocol has recently beenprovided among 62 patients that underwent 471 desen-sitization procedures of which 8 % were complicated bybreakthrough HSRs (none of them severe) [7].
Description of the Protocol The BWH/DFCI RDD protocol isas follows (Table 2): 1/10th and 1/100th of the total dose to beadministered are prepared in 250-ml bags (bags 1 and 2,respectively) [106]. Sometimes, an additional bag containing1/1000th the total dose in 250 ml is prepared if the patient hada very severe initial HSR or is thought to be very sensitive [5].The infusion of bag 1 is started at a rate of 2.5 ml/h, and therate is doubled every 15 min for three additional steps. Theinfusion then continues with the next bag, which has a 10-foldhigher concentration of the drug, and the rate is decreased 4-fold so that the dose administered during this step is approx-imately twice that of the previous one. The rationale fordoubling doses at each step to achieve desensitization is basedon in vitro data from mouse and human mast cells and on theexperience with penicillin desensitization protocols [100,112–114]. The final bag (usually bag 3 if bag 1 is a 1/100thdilution) contains the total dose to be administered (minus thedose given with bags 1 and 2) in 250 ml or a larger volume to
remain below the saturation point of the drug (e.g., 1.2 mg/mlfor paclitaxel). The final rate is usually 80 ml/h, which makesa 12-step/3-bag desensitization and a 16-step/4-bag lastaround 6 and 7 h, respectively. Figure 4 depicts schematicallyon a log scale the progressive increase in the cumulative doseinfused over time during a 12-step/3-bag desensitization andcompares it to a regular infusion. Interestingly, most break-through HSRs occur during step 12 of the protocol, whichmay be explained by the fact that the dose administered duringthis step would have been sufficient to trigger a HSR in allpatients, if they had not received it through desensitization upto this point [3].
Setting and Patient Preparation for RDD At BWH/DFCI,desensitization procedures are usually performed in the out-patient infusion unit with a one-to-one nurse/patient ratio. Thefirst desensitization might be performed in the intensive careunit if the initial HSR was severe (grade 3) and/or the patientpresents important co-morbidities (e.g., severe cardiovascularor respiratory disease) that would put her/him at a higher riskof having a severe or difficult to manage breakthrough HSR.As the risk of a breakthrough HSR steadily decreases witheach desensitization, subsequent procedures can be performedin the outpatient setting provided no severe HSR occurredduring the initial desensitization [3].
Table 2 Example of 12-step/3-bag desensitization protocol used at Brigham and Women’s Hospital and Dana-Farber Cancer Institute
Name of medication Paclitaxel
Target dose 300 mg (175 mg/m2; usually infused over 180 min)
Standard volume per bag 250 ml
Volume per bag Concentration (mg/ml) Total dose per bag (mg)
Solution 1 250 0.012 3
Solution 2 250 0.2 30
Solution 3 250 1.19 297.6300−2.3625 (cumulative dose received at step 8)
Step Solution Rate (ml/h) Time per step (min) Dose administeredper step (mg)
Cumulativedose (mg)
Fold increaseper step
1 1 2.5 15 0.0075 0.0075 –
2 1 5 15 0.015 0.0225 3
3 1 10 15 0.03 0.0525 2.3
4 1 20 15 0.06 0.1125 2.1
5 2 5 15 0.15 0.2625 2.3
6 2 10 15 0.3 0.5625 2.1
7 2 20 15 0.6 1.1625 2.1
8 2 40 15 1.2 2.3625 2.0
9 3 10 15 2.98 5.3375 2.3
10 3 20 15 5.95 11.288 2.1
11 3 40 15 11.9 23.188 2.1
12 3 80 174 276.8 300 ≤2.0Total time: 339 min=5.65 h
Clinic Rev Allerg Immunol

Beta-blockers should be withheld 24 h before the pro-cedure in all patients, unless extenuating circumstancesare present, as they might interfere with epinephrine,should it be required to treat a HSR [115]. Also, high-risk patients should also preferentially avoid angiotensin-converting enzyme inhibitors 24 h before desensitizationas they may increase the risk of prolonged hypotension inthe event of a HSR [116]. Patients are advised to reportany symptom they may experience during the proceduresince rapid discontinuation of the infusion and treatmentare keys to prevent severe HSRs. Following the end of theinfusion, patients are observed for 30 min and thendischarged home. They are advised to inform the desen-sitization team of any delayed reaction.
Patients receive the same standard premedication regi-men that they would for a regular infusion, which in-cludes dexamethasone as previously mentioned.However, additional doses of corticosteroids are rarelyused. Aspirin 325 mg (oral) and montelukast 10 mg(oral), which were shown to be more effective at mini-mizing breakthrough HSR compared with methylpredni-solone, are commonly given as a single dose 30–60 minbefore the procedure along with the other premedicationdrugs [117]. Aspirin acts by inhibiting the synthesis ofprostaglandins and montelukast by blocking the receptorfor cysteinyl leukotrienes; these are important mediatorssecreted by activated mast cells and basophils (Fig. 3)[117]. H1 (cetirizine 10 mg (oral) or diphenhydramine25–50 mg (IV) or hydroxyzine 25–50 mg (oral)) and H2(famotidine 20 mg (IV) or ranitidine 50 mg (IV)) blockers
are systematically given even if not part of the standardpremedication regimen. It is recommended that patientswith delayed HSRs following desensitization receive ashort-term (3–7 days) treatment with antihistamines, aspi-rin, montelukast, and, rarely, corticosteroids. Zileuton,which blocks the synthesis of leukotrienes through 5-lipooxygenase inhibition [118] and used as a single dose30–60 min before the procedure, may also be consideredin some patients with refractory breakthrough HSRs.
Management of Breakthrough HSRs During RDD If a HSRoccurs during a desensitization procedure, the infusion isimmediately paused; and depending on the severity ofsymptoms, treatment can vary from simple observationto epinephrine injection [3]. Once symptoms have subsi-ded, the procedure is resumed from the exact point whereit was stopped. The protocol may then be adjusted forsubsequent desensitizations to prevent recurrent break-through HSRs by either prolonging a step (from 15 to30 min), adding an extra step (with a rate at mid-pointbetween the rate of the previous and the next step), and/oradding premedication before the step where the HSR hasoccurred [3]. Also, patients who react early during thedesensitization process (bag 1) may benefit from a 16-step/4-bag protocol [5]. Together, these precautions andstrategies have contributed to make RDD a safe andeffective mean of re-introducing taxanes even in patientswith life-threatening HSRs.
Skin Testing
Taxane skin testing was initially performed on two patientswith severe HSRs to paclitaxel (administered withoutpremedication during phase I trials) and four paclitaxel-tolerant controls [26]. SPT and IDT were performed withdiluted and undiluted paclitaxel and were found to be negativein all patients. This somewhat limited experience (combinedwith the fact that most HSRs occurred with first exposure) ledto the assumption that taxane HSRs were not IgE-mediated.This long-held view was recently challenged by Prieto-Garciaand Pineda de la Losa who described a case of a patient with asevere paclitaxel HSR on her second lifetime exposure inwhom a positive IDT to paclitaxel was elicited at a concen-tration of 0.0001 mg/ml6. They also showed that a paclitaxelconcentration of 6 mg/ml (undiluted) in SPTand of 1mg/ml inIDT were non-irritant as they did not induce a positive re-sponse in 15 patients that had adverse reactions to paclitaxel.The experience with docetaxel skin testing is even morelimited. Messaad et al. skin tested to docetaxel (SPT10 mg/ml and IDT 1 mg/ml) a patient that had a severeimmediate HSR to docetaxel on first exposure [119]. Theresults were negative. To our knowledge, nab-paclitaxel andcabazitaxel skin testing have not been performed.
Fig. 4 Log scale of the cumulative dose of paclitaxel administered overtime during desensitization compared to a 3-h regular infusion of a 300-mgdose. The starting dose of a 12-step/3-bag protocol is around 40,000-foldless than the target dose and 3,000-fold less than the starting dose of aregular infusion. After 1 min of a regular infusion, around 1.7 mg ofpaclitaxel has already been administered. The desensitization protocol usesa very low starting dose to ensure that it is below the reaction threshold. Thedose is then increased by 2-fold increments every 15 min until a dosearound 10-fold less than the target dose is reached (step 11; 2.75 h). Thatdose is also roughly equivalent to the starting dose of a regular infusion,which is often sufficient to trigger a HSR if not administered throughdesensitization. The rate of step 12 is kept constant at 80 ml/h allowingthe remainder of the dose to be delivered at a slower pace (<2-fold increase)that is similar to the rate at which a regular infusion is delivered
Clinic Rev Allerg Immunol

Different groups have since adopted the practice of taxaneskin testing. Gastaminza et al. performed skin testing (SPT0.4 mg/ml and IDT 0.04 mg/ml) on three patients with HSRsto docetaxel and found one positive result [89]. All threepatients tolerated docetaxel re-administration through a desen-sitization protocol. In another study, 17 patients with immedi-ate HSRs to taxanes (14 with paclitaxel and three with doce-taxel) underwent skin testing [88]. Paclitaxel was used at up to6 mg/ml (SPTand IDT) and docetaxel at up to 10 mg/ml (SPTand IDT). Two patients had positive results although the drugand concentration to which they tested positive is not men-tioned. Among the 15 patients with negative skin tests, 12were challenged and eight reacted suggesting a poor negativepredictive value in this population. Skin-test and challenge-positive patients were subsequently desensitized to taxanes,and 5/10 (50 %) experienced a mild breakthrough HSR. Incontrast, paclitaxel skin testing (SPT 1 mg/ml; IDT0.001 mg/ml followed if negative by 0.01 mg/ml) was recent-ly performed on 64 patients with immediate and delayedHSRs to taxanes [7]. Forty-four out of 56 patients (79 %) witha paclitaxel HSR, 3/6 (50 %) with a docetaxel HSR, and 2/2(100 %) with HSRs to both drugs had a positive result.Patients were most commonly positive at the lowest IDTconcentration (0.001 mg/ml), and two patients exhibited apositive SPT. Patients with a negative skin test and either adelayed or grade 1 or 2 immediate HSR were considered forchallenge. All 11 patients that were challenged had no HSRand were able to resume regular infusions. Interestingly, oneof those subsequently developed a grade 3 HSR and, on re-evaluation, was found to have converted from a negative to apositive skin test. These preliminary data suggest thattaxane skin testing could be used as a risk stratificationtool in the decision to re-introduce taxane through achallenge or a desensitization procedure. However, experi-ence with taxane skin testing is still limited, and as shownby these studies, its value may vary between differentpopulations, highlighting the need for further research onthis promising new diagnostic and risk stratification toolfor taxane HSRs.
Proposed Management Strategy for HSRs to Taxanes
The management strategy proposed in this review aims toprovide a general approach to taxane HSRs based on theevidence currently available and our own experience. As theevidence on taxane skin testing is still fairly new and limited,this approach may be subject to change over the next fewyears as new data emerge. The proposedmanagement strategyfor HSRs to taxanes is summarized in Fig. 5.
There is a general agreement that patients with severedelayed type HSRs such as SJS/TEN or pneumonitis shouldnot be re-exposed to the inciting agent and probably topotentially cross-reacting drugs [100]. It should be
emphasized that desensitization protocols, despite theirefficacy at preventing life-threatening immediate HSRs,are not efficacious at preventing severe delayed reac-tions. On the other hand, patients with non-severe de-layed onset HSRs such as a benign maculopapular rashmay be safely re-exposed to taxanes although the meth-od of re-introduction will depend on skin testing results[7]. We have noticed that these delayed reactions recurin only a minority of patients and that when they do,they are rarely more severe than the initial reaction andthey tend to subside over repeated exposures. Anotherconcern is that such delayed reactions may be the pre-lude to an immediate HSR thus providing the rationalefor skin testing [7, 71].
Patients with immediate HSRs should undergo skin testingas the result can be used as a diagnostic and risk stratificationtool [7, 88]. Although the majority of immediate HSRs usu-ally occur within minutes of the start of the infusion, somereactions with features of immediate-type HSRs (e.g., flush-ing, pruritus, angioedema, urticaria, bronchospasm, and evenhypotension) may have a delayed onset of up to 24 h after theinfusion [106]. Such HSRs may represent a late-phase phe-nomenon of which the immediate phase would have beenblunted by the premedication given prior to the taxane infu-sion [115]. In patients with severe immediate HSRs, it may behelpful to measure mediators released by basophils/mast cellsupon activation (e.g., serum tryptase and 24-h urinarymethylhistamine) so as to document their role in the HSR[106] and to detect rare patients with mast cell activationdisorders, which may represent a particular challenge fordesensitization [120].
Skin testing should be performed at least 2 weeks afterthe event to minimize the possibility of a false-negativeresult due to the refractory period following a HSR [121].Drugs that may interfere with skin reactivity should alsobe withdrawn for the appropriate amount of time beforeskin testing [121]. Paclitaxel skin testing is performed at1 mg/ml (SPT); and if negative, 0.001 mg/ml (IDT); andif negative, 0.01 mg/ml (IDT) and docetaxel skin testingat 10 mg/ml (SPT); and if negative, 1 mg/ml (IDT).Systemic reactions, although very rare, may be inducedby skin testing, and emergency treatment should be avail-able to treat these reactions [121].
We recommend taxane re-introduction through a rapid drugdesensitization protocol in those with a positive skin test (evenif the initial reaction was consistent with a delayed onsetmaculopapular rash) since it indicates mast cell sensitivity totaxanes and possibly an underlying IgE-mediated mechanism[7, 88]. RDD also appears to be the safest approach fornegative skin-test patients with a severe initial HSR, especial-ly as the negative predictive value has not been established forthis test in this population [7]. It seems reasonable to proceedto a graded challenge in patients with grade 1 or delayed type
Clinic Rev Allerg Immunol

HSRs and a negative skin test, as their risk of recurrentreaction appears to be low [7]. Prior to challenge, the standardpremedication regimen for the taxane concerned should beadministered as for a regular infusion. To minimize the risk ofcausing a severe HSR, it is advised to start the infusion at arelatively low rate (e.g., 2 mL/h) that can then be increased by10-fold increments so as to reach the rate of a regular infusionin around three steps [100]. If no HSR occurs with the gradedchallenge procedure, the patient can safely resume regularinfusions; whereas in the event of an immediate HSR, RDDis recommended for future infusions [7]. The management ofskin-test negative grade 2 reactors is less clear as fewer ofthose patients have been challenged [7]. The decision toproceed with either a graded challenge or desensitization willthus depend on the level of comfort of the allergist thatsupervises the procedure and of the patient who undergoes itas well as on the severity of the initial HSR. Therefore, anallergist experienced in drug allergy may feel comfortable toperform a graded challenge in a patient with a moderate grade2 HSR (e.g., flushing, dyspnea, and back pain) without sig-nificant co-morbidities and who wishes to resume regularinfusions whereas he may opt for RDD in patient with a more
severe grade 2 HSR (e.g., flushing, dyspnea, throat tightness,back pain, and sense of impending doomwithout any changesin vital signs).
Conclusions
The field of HSRs to chemotherapy is rapidly evolving, andimportant achievements have been made over the yearsallowing many patients allergic to their chemotherapy toreceive it safely. As highlighted in this review, the manage-ment strategies for taxane HSRs are being progressively re-fined and will likely continue to evolve, especially as more isdiscovered on the underlying mechanisms of those reactions.Further research is thus needed on the mechanisms of HSRs totaxanes and on those of rapid drug desensitization as well ason the clinical approach to patients suffering from HSRs totaxanes.
Conflicts of Interest Matthieu Picard and Mariana C. Castells declarethat they have no conflict of interest.
Fig. 5 Algorithm for the management of HSRs to taxanes. See text fordetails. Asterisk denotes that some patients may experience HSR that areconsistent with basophil/mast cell activation up to 24 h following an
infusion. These reactions should be classified as immediate as they mayrepresent a late-phase reaction of which the immediate phase could havebeen blunted by premedication
Clinic Rev Allerg Immunol

References
1. Limsuwan T, Castells MC (2010) Outcomes and safety of rapiddesensitization for chemotherapy hypersensitivity. Expert OpinDrug Saf 9:39–53
2. Morgan RJ, Alvarez RD, Armstrong DK et al (2012) Ovariancancer, version 3.2012. J Natl Compr Canc Netw 10:1339–49
3. Castells MC, Tennant NM, Sloane DE et al (2008) Hypersensitivityreactions to chemotherapy: outcomes and safety of rapid desensiti-zation in 413 cases. J Allergy Clin Immunol 122:574–80
4. Caiado J, Venemalm L, Pereira-Santos M, Costa L, Barbosa M,Castells M (2013) Carboplatin-, oxaliplatin-, and cisplatin–specificIgE: cross-reactivity and value in the diagnosis of carboplatin andoxaliplatin allergy. J Allergy Clin Immunol Pract 1:494–500
5. Mezzano V, Giavina-Bianchi P, Picard M, Caiado J, Castells M(2013) Drug desensitization in the management of hypersensitivityreactions to monoclonal antibodies and chemotherapy. BioDrugs28:133–44
6. Prieto Garcia A, Pineda de la Losa F (2010) Immunoglobulin E-mediated severe anaphylaxis to paclitaxel. J Investig Allergol ClinImmunol 20:170–1
7. PicardM, Pur L, Caiado J, Galvao V, Giavina-Bianchi P, Castells M(2014) Added value of skin testing in hypersensitivity reactions totaxanes [Abstract]. J Allergy Clin Immunol 133:AB152
8. Wani MC, Taylor HL, Wall ME, Coggon P, McPhail AT (1971)Plant antitumor agents. VI. The isolation and structure of taxol, anovel antileukemic and antitumor agent from Taxus brevifolia. J AmChem Soc 93:2325–7
9. Schiff PB, Fant J, Horwitz SB (1979) Promotion of microtubuleassembly in vitro by taxol. Nature 277:665–7
10. JordanMA,Wilson L (2004) Microtubules as a target for anticancerdrugs. Nat Rev Cancer 4:253–65
11. Horwitz SB (1994) How to make taxol from scratch. Nature 367:593–4
12. Exposito O, Bonfill M, Moyano E et al (2009) Biotechnologicalproduction of taxol and related taxoids: current state and prospects.Anticancer Agents Med Chem 9:109–21
13. Nicolaou KC, Yang Z, Liu JJ et al (1994) Total synthesis of taxol.Nature 367:630–4
14. Taxol Prescribing Information (2014) (Accessed January 13, 2014,at http://packageinserts.bms.com/pi/pi_taxol.pdf.)
15. Taxotere Prescribing Information (2013) (Accessed December 24,2013, at http://products.sanofi.us/Taxotere/taxotere.html.)
16. Stinchcombe TE (2007) Nanoparticle albumin-bound paclitaxel: anovel Cremphor-EL-free formulation of paclitaxel. Nanomedicine(Lond) 2:415–23
17. Cucinotto I, Fiorillo L, Gualtieri S et al (2013) Nanoparticle albuminbound paclitaxel in the treatment of human cancer: nanodeliveryreaches prime-time? J Drug Deliv 2013:905091
18. Kratz F (2008) Albumin as a drug carrier: design of prodrugs, drugconjugates and nanoparticles. J Control Release 132:171–83
19. Desai N, Trieu V, Yao Z et al (2006) Increased antitumor activity,intratumor paclitaxel concentrations, and endothelial cell trans-port of Cremophor-free, albumin-bound paclitaxel, ABI-007,compared with cremophor-based paclitaxel. Clin Cancer Res12:1317–24
20. Ma P, Mumper RJ (2013) Paclitaxel nano-delivery systems: acomprehensive review. J Nanomed Nanotechnol 4:1000164
21. Abraxane Prescribing Information (2014) (Accessed January 3, 2014,at http://abraxane.com/downloads/Abraxane_PrescribingInformation.pdf.)
22. GalskyMD, Dritselis A, Kirkpatrick P, OhWK (2010) Cabazitaxel.Nat Rev Drug Discov 9:677–8
23. Cabazitaxel Prescribing Information (2014) (Accessed January 12,2014, at http://products.sanofi.us/jevtana/jevtana.html.)
24. Wiernik PH, Schwartz EL, Strauman JJ, Dutcher JP, Lipton RB,Paietta E (1987) Phase I clinical and pharmacokinetic study of taxol.Cancer Res 47:2486–93
25. Kris MG, O'Connell JP, Gralla RJ et al (1986) Phase I trialof taxol given as a 3-hour infusion every 21 days. CancerTreat Rep 70:605–7
26. Weiss RB, Donehower RC, Wiernik PH et al (1990)Hypersensitivity reactions from taxol. J Clin Oncol 8:1263–8
27. Gennari A, Salvadori B, Tognoni A, Conte PF (1996) Rapid intra-venous premedication with dexamethasone prevents hypersensitiv-ity reactions to paclitaxel. Ann Oncol 7:978–9
28. BookmanMA,Kloth DD, Kover PE, Smolinski S, Ozols RF (1997)Short-course intravenous prophylaxis for paclitaxel-related hyper-sensitivity reactions. Ann Oncol 8:611–4
29. MarkmanM, KennedyA,Webster K, Peterson G, Kulp B, BelinsonJ (1997) Simplified regimen for the prevention of paclitaxel-associated hypersensitivity reactions. J Clin Oncol 15:3517
30. Micha JP, Rettenmaier MA, Dillman R, Fraser P, Birk C, Brown JV(1998) Single-dose dexamethasone paclitaxel premedication.Gynecol Oncol 69:122–4
31. Olson JK, Sood AK, Sorosky JI, Anderson B, Buller RE (1998)Taxol hypersensitivity: rapid retreatment is safe and cost effective.Gynecol Oncol 68:25–8
32. Cormio G, Di Vagno G, Melilli GA et al (1999) Hypersensitivityreactions in ovarian cancer patients receiving paclitaxel. JChemother 11:407–9
33. MarkmanM, KennedyA,Webster K, Kulp B, Peterson G, BelinsonJ (2000) Paclitaxel-associated hypersensitivity reactions: experienceof the gynecologic oncology program of the Cleveland ClinicCancer Center. J Clin Oncol 18:102–5
34. Kwon JS, Elit L, Finn M et al (2002) A comparison of twoprophylactic regimens for hypersensitivity reactions to paclitaxel.Gynecol Oncol 84:420–5
35. Henry A, Charpiat B, Perol M, Vial T, de Saint Hilaire PJ, DescotesJ (2006) Paclitaxel hypersensitivity reactions: assessment of theutility of a test-dose program. Cancer J 12:237–45
36. Kosmas C, Tsavaris N (2006) A simplified premedication protocolfor one-hour paclitaxel infusion in various combinations. Med SciMonit 12:CR462–6
37. Eisenhauer EA, ten Bokkel Huinink WW, Swenerton KD et al(1994) European-Canadian randomized trial of paclitaxel in re-lapsed ovarian cancer: high-dose versus low-dose and long versusshort infusion. J Clin Oncol 12:2654–66
38. Sendo T, Sakai N, Itoh Yet al (2005) Incidence and risk factors forpaclitaxel hypersensitivity during ovarian cancer chemotherapy.Cancer Chemother Pharmacol 56:91–6
39. Kloover JS, den Bakker MA, Gelderblom H, van Meerbeeck JP(2004) Fatal outcome of a hypersensitivity reaction to paclitaxel: acritical review of premedication regimens. Br J Cancer 90:304–5
40. Williams C, Bryant A (2011) Short versus long duration infusions ofpaclitaxel for any advanced adenocarcinoma. Cochrane DatabaseSyst Rev 11:CD003911
41. Smith RE, BrownAM,Mamounas EP et al (1999) Randomized trialof 3-hour versus 24-hour infusion of high-dose paclitaxel in patientswith metastatic or locally advanced breast cancer: National SurgicalAdjuvant Breast and Bowel Project Protocol B-26. J Clin Oncol 17:3403–11
42. Kelly CM, Green MC, Broglio K et al (2012) Phase III trialevaluating weekly paclitaxel versus docetaxel in combinationwith capecitabine in operable breast cancer. J Clin Oncol 30:930–5
43. Mannel RS, Brady MF, Kohn EC et al (2011) A randomized phaseIII trial of IV carboplatin and paclitaxel ×3 courses followed byobservation versus weekly maintenance low-dose paclitaxel in pa-tients with early-stage ovarian carcinoma: a Gynecologic OncologyGroup Study. Gynecol Oncol 122:89–94
Clinic Rev Allerg Immunol

44. Quock J, Dea G, Tanaka M, Gandara D, Lara P, Lau D (2002)Premedication strategy for weekly paclitaxel. Cancer Invest 20:666–72
45. MarkmanM, Blessing J, Rubin SC, Connor J, Hanjani P, WaggonerS (2006) Phase II trial of weekly paclitaxel (80 mg/m2) in platinumand paclitaxel-resistant ovarian and primary peritoneal cancers: aGynecologic Oncology Group study. Gynecol Oncol 101:436–40
46. Braverman AS, Rao S, Salvatti ME, Adamson B, McManus M,Pierre S (2005) Tapering and discontinuation of glucocorticoidprophylaxis during prolonged weekly to biweekly paclitaxeladministration. Chemotherapy 51:116–9
47. Schrijvers D, Wanders J, Dirix L et al (1993) Coping with toxicitiesof docetaxel (Taxotere). Ann Oncol 4:610–1
48. Mertens WC, Eisenhauer EA, Jolivet J, Ernst S, Moore M, MuldalA (1994) Docetaxel in advanced renal carcinoma. A phase II trial ofthe National Cancer Institute of Canada Clinical Trials Group. AnnOncol 5:185–7
49. Pazdur R, Lassere Y, Soh LT et al (1994) Phase II trial of docetaxel(Taxotere) in metastatic colorectal carcinoma. Ann Oncol 5:468–70
50. Francis PA, Rigas JR, Kris MG et al (1994) Phase II trial ofdocetaxel in patients with stage III and IV non-small-cell lungcancer. J Clin Oncol 12:1232–7
51. Semb KA, Aamdal S, Oian P (1998) Capillary protein leak syn-drome appears to explain fluid retention in cancer patients whoreceive docetaxel treatment. J Clin Oncol 16:3426–32
52. Piccart MJ, Gore M, Ten Bokkel HW et al (1995) Docetaxel: anactive new drug for treatment of advanced epithelial ovarian cancer.J Natl Cancer Inst 87:676–81
53. Cortes JE, Pazdur R (1995) Docetaxel. J Clin Oncol 13:2643–5554. Vasey PA, Jayson GC, Gordon A et al (2004) Phase III randomized
trial of docetaxel-carboplatin versus paclitaxel-carboplatin as first-line chemotherapy for ovarian carcinoma. J Natl Cancer Inst 96:1682–91
55. Syrigou E, Dannos I, Kotteas E et al (2011) Hypersensitivity reac-tions to docetaxel: retrospective evaluation and development of adesensitization protocol. Int Arch Allergy Immunol 156:320–4
56. Poi MJ, Berger M, Lustberg M et al (2013) Docetaxel-induced skintoxicities in breast cancer patients subsequent to paclitaxelshortage: a case series and literature review. Support CareCancer 21:2679–86
57. Piccart MJ, Klijn J, Paridaens R et al (1997) Corticosteroids signif-icantly delay the onset of docetaxel-induced fluid retention: finalresults of a randomized study of the European Organization forResearch and Treatment of Cancer Investigational Drug Branchfor Breast Cancer. J Clin Oncol 15:3149–55
58. Schwartz JR (2012) Dexamethasone premedication for prophylaxisof taxane toxicities: can the doses be reduced when paclitaxel ordocetaxel are given weekly? J Oncol Pharm Pract 18:250–6
59. Sparano JA, Wang M, Martino S et al (2008) Weekly pac-litaxel in the adjuvant treatment of breast cancer. N Engl JMed 358:1663–71
60. Gradishar WJ, Tjulandin S, Davidson N et al (2005) Phase III trialof nanoparticle albumin-bound paclitaxel compared withpolyethylated castor oil-based paclitaxel in women with breastcancer. J Clin Oncol 23:7794–803
61. Yamamoto Y, Kawano I, Iwase H (2011) Nab-paclitaxel for thetreatment of breast cancer: efficacy, safety, and approval. OncoTargets Ther 4:123–36
62. de LeonMC, Bolla S, Greene B, Hutchinson L, Del Priore G (2013)Successful treatment with nab-paclitaxel after hypersensitivity reac-tion to paclitaxel and docetaxel. Gynecol Oncol Case Rep 5:70–1
63. Kimura K, Tanaka S, IwamotoM et al (2013) Safety of nanoparticlealbumin-bound paclitaxel administered to breast cancer patientswith clinical contraindications to paclitaxel or docetaxel: Four casereports. Oncol Lett 6:881–4
64. Fader AN, Rose PG (2009) Abraxane for the treatment of gyneco-logic cancer patients with severe hypersensitivity reactions to pac-litaxel. Int J Gynecol Cancer 19:1281–3
65. Micha JP, Goldstein BH, Birk CL, Rettenmaier MA, Brown JV 3rd(2006) Abraxane in the treatment of ovarian cancer: the absence ofhypersensitivity reactions. Gynecol Oncol 100:437–8
66. Fernandez O, Afonso J, Vazquez S, et al (2014) Metastaticcastration-resistant prostate cancer: changing landscape withcabazitaxel. Anticancer Drugs 25(3):237–43
67. de Bono JS, Oudard S, Ozguroglu M et al (2010) Prednisone pluscabazitaxel or mitoxantrone for metastatic castration-resistant pros-tate cancer progressing after docetaxel treatment: a randomisedopen-label trial. Lancet 376:1147–54
68. Bracarda S, Gernone A, Gasparro D, et al (2013) Real-worldcabazitaxel safety: the Italian early-access program in metastaticcastration-resistant prostate cancer. Future Oncol. doi:10.2217/fon.13.256
69. Tannock IF, de Wit R, Berry WR et al (2004) Docetaxel plusprednisone or mitoxantrone plus prednisone for advanced prostatecancer. N Engl J Med 351:1502–12
70. Pivot X, Koralewski P, Hidalgo JL et al (2008) A multicenter phaseII study of XRP6258 administered as a 1-h i.v. infusion every3 weeks in taxane-resistant metastatic breast cancer patients. AnnOncol 19:1547–52
71. Anonymous (2011) A fatal anaphylactic reaction to paclitaxel isdescribed, which was preceded by a possible delayed reaction to theinitial infusion. Allergy Asthma Proc 32:79
72. Hiraki A, Aoe K, Murakami T, Maeda T, Eda R, Takeyama H(2004) Stevens-Johnson syndrome induced by paclitaxel in a patientwith squamous cell carcinoma of the lung: a case report. AnticancerRes 24:1135–7
73. Sawada Y, Sugita K, Kabashima R, Nakamura M, Tokura Y (2009)Docetaxel-induced Stevens-Johnson syndrome with regeneratingepidermis composed of atypical keratinocytes. J Eur AcadDermatol Venereol 23:1333–5
74. Taj A (2013) Docetaxel-induced hypersensitivity pneumonitismimicking lymphangitic carcinomatosis in a patient withmetastatic adenocarcinoma of the lung. Hematol OncolStem Cell Ther 6:117–9
75. Nagata S, Ueda N, Yoshida Y, Matsuda H, Maehara Y (2010)Severe interstitial pneumonitis associated with the administrationof taxanes. J Infect Chemother 16:340–4
76. Read WL, Mortimer JE, Picus J (2002) Severe interstitial pneumo-nitis associated with docetaxel administration. Cancer 94:847–53
77. Von Hoff DD, Ervin T, Arena FP et al (2013) Increased survival inpancreatic cancer with nab-paclitaxel plus gemcitabine. N Engl JMed 369:1691–703
78. Fujimori K, Yokoyama A, Kurita Y, Uno K, Saijo N (1998)Paclitaxel-induced cell-mediated hypersensitivity pneumonitis.Diagnosis using leukocyte migration test, bronchoalveolar lavageand transbronchial lung biopsy. Oncology 55:340–4
79. Chen M, Crowson AN, Woofter M, Luca MB, Magro CM (2004)Docetaxel (taxotere) induced subacute cutaneous lupus erythema-tosus: report of 4 cases. J Rheumatol 31:818–20
80. Marchetti MA, Noland MM, Dillon PM, Greer KE (2013) Taxaneassociated subacute cutaneous lupus erythematosus. DermatolOnline J 19:19259
81. LamondNW,Younis T, PurdyK, DorreenMS (2013) Drug-inducedsubacute cutaneous lupus erythematosus associated with nab-paclitaxel therapy. Curr Oncol 20:e484–7
82. Robinson JB, Singh D, Bodurka-Bevers DC, Wharton JT,Gershenson DM, Wolf JK (2001) Hypersensitivity reactionsand the utility of oral and intravenous desensitization inpatients with gynecologic malignancies. Gynecol Oncol 82:550–8
Clinic Rev Allerg Immunol

83. Raisch DW, Campbell W, Garg V et al (2011) Description ofanaphylactic reactions to paclitaxel and docetaxel reported to theFDA, with a focus on the role of premedication. Expert Opin DrugSaf 10:521–8
84. Bennett CL, Adegboro OS, Calhoun EA, Raisch D (2010) Beyondthe black box: drug- and device-associated hypersensitivity events.Drug Healthc Patient Saf 2:1–5
85. Szebeni J, Muggia FM, Alving CR (1998) Complement activationby Cremophor EL as a possible contributor to hypersensitivity topaclitaxel: an in vitro study. J Natl Cancer Inst 90:300–6
86. Weiszhar Z, Czucz J, Revesz C, Rosivall L, Szebeni J, Rozsnyay Z(2012) Complement activation by polyethoxylated pharmaceuticalsurfactants: Cremophor-EL, Tween-80 and Tween-20. Eur J PharmSci 45:492–8
87. Essayan DM, Kagey-Sobotka A, Colarusso PJ, Lichtenstein LM,Ozols RF, King ED (1996) Successful parenteral desensitization topaclitaxel. J Allergy Clin Immunol 97:42–6
88. Madrigal-Burgaleta R, Berges-Gimeno MP, Angel-Pereira D et al(2013) Hypersensitivity and desensitization to antineoplastic agents:outcomes of 189 procedures with a new short protocol and noveldiagnostic tools assessment. Allergy 68:853–61
89. Gastaminza G, de la Borbolla JM, Goikoetxea MJ et al (2011) Anew rapid desensitization protocol for chemotherapy agents. JInvestig Allergol Clin Immunol 21:108–12
90. Ebo DG, Piel GC, Conraads V, Stevens WJ (2001) IgE-mediatedanaphylaxis after first intravenous infusion of cyclosporine. AnnAllergy Asthma Immunol 87:243–5
91. Perez-Perez L, Garcia-Gavin J, Pineiro B, Zulaica A (2011)Biologic-induced urticaria due to polysorbate 80: usefulness ofprick test. Br J Dermatol 164:1119–20
92. Limaye S, Steele RH, Quin J, Cleland B (2002) An allergic reactionto erythropoietin secondary to polysorbate hypersensitivity. JAllergy Clin Immunol 110:530
93. van Zuylen L, Gianni L, Verweij J et al (2000) Inter-relationships ofpaclitaxel disposition, infusion duration and Cremophor EL kineticsin cancer patients. Anticancer Drugs 11:331–7
94. Vanhaelen M, Duchateau J, Vanhaelen-Fastre R, Jaziri M (2002)Taxanes in Taxus baccata pollen: cardiotoxicity and/or allergenici-ty? Planta Med 68:36–40
95. Lakin JD, Blocker TJ, StrongDM, YocumMW (1978)Anaphylaxisto protamine sulfate mediated by a complement-dependent IgGantibody. J Allergy Clin Immunol 61:102–7
96. Weiss ME, Adkinson NF Jr (1991) Allergy to protamine. Clin RevAllergy 9:339–55
97. Dykewicz MS, Kim HW, Orfan N, Yoo TJ, Lieberman P (1994)Immunologic analysis of anaphylaxis to protamine component inneutral protamineHagedorn human insulin. J Allergy Clin Immunol93:117–25
98. Maguchi S, Fukuda S (2001) Taxus cuspidata (Japanese yew)pollen nasal allergy. Auris Nasus Larynx 28(Suppl):S43–7
99. Italian Association of Aerobiology (2002) An epidemiological sur-vey of Cupressaceae pollenosis in Italy. J Investig Allergol ClinImmunol 12:287–92
100. Joint Task Force on Practice Parameters; American Academy ofAllergy, Asthma and Immunology; American College of Allergy,Asthma and Immunology; Joint Council of Allergy, Asthma andImmunology (2010) Drug allergy: an updated practice parameter.Ann Allergy Asthma Immunol 105:259–73
101. Brown SG (2004) Clinical features and severity grading of anaphy-laxis. J Allergy Clin Immunol 114:371–6
102. Peereboom DM, Donehower RC, Eisenhauer EA et al (1993)Successful re-treatment with taxol after major hypersensitiv-ity reactions. J Clin Oncol 11:885–90
103. MarkmanM, Kennedy A,Webster K, Peterson G, Kulp B, BelinsonJ (2001) Combination chemotherapywith carboplatin and docetaxelin the treatment of cancers of the ovary and fallopian tube andprimary carcinoma of the peritoneum. J Clin Oncol 19:1901–5
104. Laskin MS, Lucchesi KJ, Morgan M (1993) Paclitaxel rechallengefailure after a major hypersensitivity reaction. J Clin Oncol 11:2456–7
105. Del Priore G, Smith P, Warshal DP, Dubeshter B, Angel C (1995)Paclitaxel-associated hypersensitivity reaction despite high-dosesteroids and prolonged infusions. Gynecol Oncol 56:316–8
106. Feldweg AM, Lee CW, Matulonis UA, Castells M (2005) Rapiddesensitization for hypersensitivity reactions to paclitaxel and do-cetaxel: a new standard protocol used in 77 successful treatments.Gynecol Oncol 96:824–9
107. Lokich J, AndersonN (1998) Paclitaxel hypersensitivity reactions: arole for docetaxel substitution. Ann Oncol 9:573
108. Moon C, Verschraegen CF, Bevers M, Freedman R, Kudelka AP,Kavanagh JJ (2000) Use of docetaxel (Taxotere) in patients withpaclitaxel (Taxol) hypersensitivity. Anticancer Drugs 11:565–8
109. Dizon DS, Schwartz J, Rojan A et al (2006) Cross-sensitivitybetween paclitaxel and docetaxel in a women's cancers program.Gynecol Oncol 100:149–51
110. Sanchez-Munoz A, Jimenez B, Garcia-Tapiador A et al (2011)Cross-sensitivity between taxanes in patients with breast cancer.Clin Transl Oncol 13:904–6
111. Lee CW, Matulonis UA, Castells MC (2005) Rapid inpatient/outpatient desensitization for chemotherapy hypersensitivity: stan-dard protocol effective in 57 patients for 255 courses. GynecolOncol 99:393–9
112. Sancho-Serra Mdel C, Simarro M, Castells M (2011) Rapid IgEdesensitization is antigen specific and impairs early and late mastcell responses targeting FcepsilonRI internalization. Eur J Immunol41:1004–13
113. Zhao W, Gomez G, Macey M, Kepley CL, Schwartz LB (2012) Invitro desensitization of human skin mast cells. J Clin Immunol 32:150–60
114. Oka T, Rios EJ, Tsai M, Kalesnikoff J, Galli SJ (2013) Rapiddesensitization induces internalization of antigen-specific IgE onmouse mast cells. J Allergy Clin Immunol 132:922–32 e1-16
115. Sampson HA, Munoz-Furlong A, Campbell RL et al (2006) Secondsymposium on the definition and management of anaphylaxis:summary report—Second National Institute of Allergy andInfectious Disease/Food Allergy and Anaphylaxis Network sympo-sium. J Allergy Clin Immunol 117:391–7
116. Rueff F, Przybilla B, Bilo MB et al (2009) Predictors of severesystemic anaphylactic reactions in patients with Hymenoptera ven-om allergy: importance of baseline serum tryptase—a study of theEuropean Academy of Allergology and Clinical ImmunologyInterest Group on Insect Venom Hypersensitivity. J Allergy ClinImmunol 124:1047–54
117. Breslow RG, Caiado J, Castells MC (2009) Acetylsalicylic acid andmontelukast block mast cell mediator-related symptoms duringrapid desensitization. Ann Allergy Asthma Immunol 102:155–60
118. Fanning LB, Boyce JA (2013) Lipidmediators and allergic diseases.Ann Allergy Asthma Immunol 111:155–62
119. Messaad D, Sablayrolles P, Pujol JL, Demoly P (2003) Successfuldocetaxel tolerance induction. Allergy 58:1320–1
120. Picard M, Giavina-Bianchi P, Mezzano V, Castells M (2013)Expanding spectrum of mast cell activation disorders: monoclonaland idiopathic mast cell activation syndromes. Clin Ther 35:548–62
121. Brockow K, Romano A, Blanca M, Ring J, Pichler W, Demoly P(2002) General considerations for skin test procedures in the diag-nosis of drug hypersensitivity. Allergy 57:45–51
Clinic Rev Allerg Immunol