Embed Size (px)
Citation preview

World Health Organization 17 September, 2008
1
How to protect yourself against malariaHow to protect yourself against malaria
Mine Action Technology Workshop 2008
co-hosted by the United Nations Mine Action Service (UNMAS)
and the Geneva International Centre for Humanitarian Demining
Presented by Dr Andrea Bosman
Global Malaria Programme
Geneva, 10 September 2008
Mine Action Technology Workshop | 10 September 20082 |GLOBAL
MALARIA PROGRAMME
THE GLOBAL BURDEN OF MALARIA:
EVERY DAY MALARIA KILLS IN NUMBERS EQUIVALENT TO "9/11" TRAGEDY OF THE NEW YORK TWIN TOWERS

World Health Organization 17 September, 2008
2
Mine Action Technology Workshop | 10 September 20083 |GLOBAL
MALARIA PROGRAMME
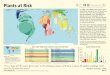
If malaria burden was proportional
to country surface areas …
If malaria If malaria burdenburden waswas proportionalproportional
to country surface areas to country surface areas ……
Dorling D Worldmapper. PLoS Med 4 (1), 2007
Mine Action Technology Workshop | 10 September 20084 |GLOBAL
MALARIA PROGRAMME
Global malaria burdenGlobal malaria burden
� 4 species of malaria parasites infect people
– Plasmodium falciparum, P. vivax, P. malariae, P. ovale
� 247 million malaria patients per year
� Nearly 1 million deaths due to malaria per year
� 90% of deaths and 60% of cases occur in Africa south of the Sahara
� 109 malaria endemic countries/territories
– 15 countries with no P.falciparum transmission, only P.vivax
– 7 countries with recently no more locally transmitted cases

World Health Organization 17 September, 2008
3
Poor access to health care in the
Amazonas
MDRfalciparummalaria
Resurgence in Central Asia & Eastern Europe
Childhood dealths in
sub-Saharan Africa
Vast burden of morbidity & economic loss
The Global Malaria PictureThe Global Malaria Picture
EMRO INTERCOUNTRY MEETING, 1-4 June 20086 |GLOBAL
MALARIA PROGRAMME
Evolution of global malaria distribution
Mid 19th centuryMid 19th century 19451945
19771977 20072007
37 countries
freed from malaria
37 countries
freed from malaria
Sweden and parts of North America
freed from malaria
Sweden and parts of North America
freed from malaria
Tunisia, Maldives and UAE
freed from malaria
Tunisia, Maldives and UAE
freed from malaria

World Health Organization 17 September, 2008
4
Mine Action Technology Workshop | 10 September 20087 |GLOBAL
MALARIA PROGRAMME
199419941994
196619661966
194619461946
mid 19th centurymidmid 1919thth centurycentury
Lower malaria vectorial capacity
in temperate and sub-tropical areasLowerLower malaria malaria vectorialvectorial capacitycapacity
in in temperatetemperate and suband sub--tropical areastropical areas
Mine Action Technology Workshop | 10 September 20088 |GLOBAL
MALARIA PROGRAMME

World Health Organization 17 September, 2008
5
SporozoitesSporozoitesSporozoitesSporozoitesHepatic phaseHepatic phaseHepatic phaseHepatic phaseInvading Invading Invading Invading ring stagering stagering stagering stageTrophozoiteTrophozoiteTrophozoiteTrophozoite
Sexual phaseSexual phaseSexual phaseSexual phaseGametocytesGametocytesGametocytesGametocytes
AsexualAsexualAsexualAsexualErythrocyticErythrocyticErythrocyticErythrocyticcyclecyclecyclecycleThe life cycle of the
malaria parasite,
Plasmodium
Non-Infected
Infected Disease Severe Death
Effective interventions are availableEffective interventions are available
Resolved Cured Cured
• Vector control
• Intermittent Preventive Therapy in pregnancy
• Chemoprophylaxis
• Early Diagnosis
• Appropriate Treatment
• Referral
• Hospital-based management

World Health Organization 17 September, 2008
6
Non-Infected
Infected Disease Severe Death
Need for new tools and technologies Need for new tools and technologies
Resolved Cured Cured
••New combination therapiesNew combination therapies
••Better rapid diagnostic testsBetter rapid diagnostic tests
••Better drug formulations Better drug formulations
••ITN:ITN: new long lasting new long lasting
••Insecticides: Insecticides: Safer & Safer &
longer residual effect longer residual effect
••Intermittent Rx: Intermittent Rx:
safer drugs in pregnancysafer drugs in pregnancy
••VaccinesVaccines
Current WHO recommendations for risk areas in malaria endemic countries
Green Green no prevention needed
BlueBlue type I prevention (anti-mosquito)
YellowYellow type II prevention (CQ)
OrangeOrange type III prevention (CQ+P)
RedRed type IV prevention (M, D or A-P)
Plus mosquitoPlus mosquito
bite preventionbite prevention

World Health Organization 17 September, 2008
7
Personal
protection
Insecticide treated
mosquito nets &
curtains
Now insecticides
are incorporated
into the synthesis of
the netting material
itself - LLNs
Can you see any problem? Can you see any problem?

World Health Organization 17 September, 2008
8
Mine Action Technology Workshop | 10 September 200815 |GLOBAL
MALARIA PROGRAMME
Chemoprophylaxis for areas with high
falciparum transmission or high resistance
Chemoprophylaxis for areas with high Chemoprophylaxis for areas with high
falciparum transmission or high resistancefalciparum transmission or high resistance
WHO Recommended regimens
� Mefloquine 5mg/kg weekly
� Doxycycline 1.5 mg/kg daily
� Atovaquone proguanil *- 11-20 kg: One pediatric tab daily
- 21-30 kg: Two pediatric tabs daily
- 31-40 kg: Three paediatric tabs daily
- > 40 kg: One adult tablet daily
* start 1 day before departure and continue for 7 days after return
Additional regimen
� Primaquine off-label use
� 30 mg base daily has protective
efficacy above 85% against
P.falciparum and primary
infections with P.vivax
� Needs G6PD screening
JAMA 2007; 297: 2251-2263
Similar protective efficacy and effective against all Plasmodium species
Current WHO recommendations when to start & when to stop taking chemoprophylaxis
International Travel and Health (WHO, 2008)
mefloquine
chloroquineweekly
doxycycline
proguanil
chloroquine
When interruptedatovaquone-
proguanil
daily
exceptionally
4 weeks upon return
4 weeks
upon return
1 week
upon return
day
before arrival
1 week
before arrival
preferably 2-3 weeks
before departure
Chemo-
prophylaxisregimen
stopstart

World Health Organization 17 September, 2008
9
current guidelines & WHO recommendations
long-term travellers
no increased risks if tolerated in the short term, no accumulationmefloquine
risks lowproguanil
limited data > 12 months use, but reassuringdoxycycline
risks low, except retinal toxicity at cumulative dose of 100 g (3-5 yrs)chloroquine
In European countries use of limited duration (5 weeks, 3 months, 6 months, "many months", 1 year), in USA
unlimited duration
atovaquone-proguanil
long term use > 6 months
In sum: "Anything tolerated in the short term can most probably also be taken long-term"
Adherence -- Tolerability
Mine Action Technology Workshop | 10 September 200818 |GLOBAL
MALARIA PROGRAMME
High risk group: pregnant womenHigh risk group: pregnant womenHigh risk group: pregnant women
In areas with low or unstable transmission
Acquired Immunity = Low
Clinical Illness
Severe Disease
Risk to Mother Risk to Fetus
• All pregnancies at risk
• Up to 60% fetal loss and 10% maternal deaths
• 50% maternal mortality with severe disease

World Health Organization 17 September, 2008
10
current guidelines & WHO recommendations
chemoprophylaxis use in special groups
proguanil
< 5 kg ??mefloquine
< 8 yrsdoxycycline
chloroquine
<11 kg
atovaquone-
proguanil
young children
breast feeding
2nd & 3rd
trimester pregnancy
1st
trimester pregnancy
Chemo-prophylaxis
= contra-indicated
= not recommended for lack of data
= safe
International Travel and Health (WHO, 2008)
Mine Action Technology Workshop | 10 September 200820 |GLOBAL
MALARIA PROGRAMME
Chemoprophylaxis during pregnancy
and breastfeeding periodChemoprophylaxis during pregnancy Chemoprophylaxis during pregnancy
and breastfeeding periodand breastfeeding period
� Areas with P.vivax or CQ sensitive P.falciparum- Chloroquine weekly chemoprophylaxis
� Areas with P.vivax and P.falciparum and emerging CQ
resistance- Chloroquine + proguanil daily chemoprophylaxis
� Areas with high P.falciparum transmission or high levels
of resistance– Mefloquine weekly chemoprophylaxis (limited safety information in first
trimester)

World Health Organization 17 September, 2008
11
The clinical
presentation
of malaria
The clinical
presentation
of malaria
Fever (uncomplicated malaria)
Severe malaria
ANTIMALARIAL
TREATMENT
Cu
mu
lati
ve
Pro
ba
bil
ity
of
a
fata
l o
utc
om
e
t (hours)
Foundations of the Case Management Strategy
The earlier the treatment, the lower the probability of fatal outcome

World Health Organization 17 September, 2008
12
Plasmodium falciparumPlasmodium falciparum
Plasmoodium vivax
Malaria mortalityMalaria mortality
Malaria Rapid Diagnostic Tests (RDTs)
contact e-mail for
specific questions:

World Health Organization 17 September, 2008
13
Rapidly increasing
range of malaria RDT
products
Manufacturer Product
Access Bio Carestart Malaria
ACON laboratories Malaria Rapid Test Device
Alldiag Palutop
Ameritek dBest Malaria Rapid Test
Amgenix OnSight Malaria
Binax NOW-ICT
r-Biopharm MalaQuick (~NOW-ICT)
Bio-Quant Inc. One Step malaria Rapid Test
Biotech Trading Partners Malaria Pf-only Rapid Test
Cellabs Rapimal
Brittney Immu-Sure Malaria
Bio-Analytics C.A. Malaria Test
Core Diagnostics Core Malaria
Cortez Malaria P.f. RapiCard InstaTest CTK CTK Onsite
Diamed AG OptiMal
Fortress Diagnostics Malaria Test
Genelabs Assure Malaria
GlobaleMed Smart Check Malaria
Guangzhou Wondfo One Step Malaria
Human Gmbh Hexagon Malaria
Inbios
International Immunodiagnostics Malaria Test Card
J Mitra Advantage Malaria
KAT Medical KatQuick
Makro Medical MakroMAL
Merlin Labs Malaria Pf test
Omega Diagnostics Visitect malaria
Orchid Biomedical Systems Paracheck
Premier Medical Corporation First Response Malaria Antigen Test
R&R Marketing ICT Malaria
SDHO
Span Diagnostics ParaHIT
Standard Diagnostics SD Bioline Malaria
Syntillent ADI Malaria
Tashima
Trinity Biotech Uni-Gold Malaria
Unimed FirstSign / Paraview Malaria
Vision Biotech Malaria Pf
Zephyr Biomedical Systems Falcivax
~50 manufacturers with named products known to WHO
>50 million tests procured in 2007
Most endemic countries have no / weak regulations
Vulnerabilities of RDTs in the field
Cautions:
• Detect antigen, not parasites.
• (-) May reflect recent, not current,
parasitaemia.
• Degraded by excessive heat.
• Limited shelf life.
• Accuracy is dependent on technique used.

World Health Organization 17 September, 2008
14
Variation in results in published trials… e.g. ICT Malaria, ‘OptiMAL’: Sensitivity >90% in multiple trials, but…...
Sensitivity (% ) for P. falciparum (vs. microscopy)
ICT M alaria Pf, Pf/Pv 82-95 Iqbal et al 2001
82.6 Huong et al 2002
80.8 Stow et al 1999
74-90 W ongsrichanalai 1999
89 Gaye et al 1998
86.2 M ason et al 2002
66.1 Rubio et al 2001
84 Leke 1999
Sensitivity (% ) for P. falciparum (vs. microscopy)
'O ptiM AL' 80% Hernandez et al 2001
88.5 Jelinek et al. 1999
70.7 M ankhambo et al 2002
83 R icci et al 2000
49.7 Huong et al 2002
42.6 M ason et al 2002
81.3 Rubio et al 2001
Field trials…
All had poor sensitivity below 100 parasites per microlitre.
eg.
Mine Action Technology Workshop | 10 September 200828 |GLOBAL
MALARIA PROGRAMME
Malaria diagnosisMalaria diagnosis
�Quality-assured confirmation of diagnosis with
microscopy before treatment
Exception:
– Patients with suspected severe malaria when blood slide
examination is not immediately possible

World Health Organization 17 September, 2008
15
Mine Action Technology Workshop | 10 September 200829 |GLOBAL
MALARIA PROGRAMME
Treatment of uncomplicated
falciparum malaria
Treatment of uncomplicated
falciparum malaria
� Artemisinin-based combination therapies (ACT) are treatments of choice for all cases of uncomplicated falciparum malaria including:
– infants,
– people living with HIV/AIDS
– for home-based management of malaria
– pregnant women in the 2nd and 3rd trimesters
Exception:
• 1st trimester of pregnancy*
* use ACTs only if no alternative effective antimalarials
Mine Action Technology Workshop | 10 September 200830 |GLOBAL
MALARIA PROGRAMME
� The following ACTs are recommended by WHO:– artemether-lumefantrine
– artesunate + amodiaquine
– artesunate + mefloquine
– artesunate + sulfadoxine-pyrimethamine
� 1st-line treatment based on therapeutic efficacy studies
in the country
� Response to treatment of travellers depends on the
origin of infection
Treatment of uncomplicated
falciparum malaria
Treatment of uncomplicated
falciparum malaria
95% cure rates in most studies
95% cure rates 95% cure rates
in in mostmost studiesstudies

World Health Organization 17 September, 2008
16
Mine Action Technology Workshop | 10 September 200831 |GLOBAL
MALARIA PROGRAMME
Anti-relapse therapy in vivax malariaAntiAnti--relapse therapy in relapse therapy in vivaxvivax malariamalaria
� To achieve radical cure, relapses must be prevented by giving
primaquine.
� In low-transmission areas the benefits of deploying primaquine
are considered to exceed the risks.
� Primaquine in 0.25 mg/kg daily doses (adult daily dose of 15 mg)
should be given for 14 days - no evidence that shorter courses
are effective.
� P. vivax infections acquired in Indonesia and Oceania require
higher dose of primaquine for radical cure, i.e. 0.50 mg/kg
per day for 14 days
Mine Action Technology Workshop | 10 September 200832 |GLOBAL
MALARIA PROGRAMME
Key points to rememberKey points to remember
1. No protective malaria "immunity" even after living many years without clinical attacks in endemic areas – be aware of the risk
2. Travel to endemic areas with insecticide-treated mosquito nets, preferably long-lasting
3. Start appropriate chemophrophylaxis as for short-term travellers, and continue for all the duration of exposure
4. Evaluate possibilities for access to early malaria diagnosis andprompt treatment at destination
5. Procure highly effective artemisinin-based combination therapy for stand-by emergency treatment of uncomplicated malaria
6. If febrile, report exposure to malaria risk to the treating clinician

World Health Organization 17 September, 2008
17
Mine Action Technology Workshop | 10 September 200833 |GLOBAL
MALARIA PROGRAMME
Acknowledgements
David Bell, WHO
Western Pacific Region
Kamini Mendis, WHO
Global Malaria Programme
Aafje Rietveld , WHO
Global Malaria Programme
Contact email
to ask more specific
malaria questions:
Contact email
to ask more specific
malaria questions:
Many thanks for your kind attentionMany thanks for your kind attention





![Antagonistic effects of Plasmodium-helminth co-infections ...¼rlimann-PLoS Negl Trop Dis-2019.pdfable to parasitic diseases, such as malaria and helminth infections [1]. Yet, the](https://img.pdfslide.us/doc/110x75/5f6fbfb25562bc6e7a14e80d/antagonistic-effects-of-plasmodium-helminth-co-infections-rlimann-plos-negl.jpg)