Embed Size (px)
DESCRIPTION
Â
Citation preview

LEADING MEDICINE YESTERDAY, TODAY AND TOMORROWAt Houston Methodist, we have a proud tradition of
revolutionizing medicine. Our past achievements
have built a legacy that spans multiple decades and
disciplines, and that same culture of excellence
inspires us to be the pioneers of tomorrow.
Houston Methodist Hospital
6565 Fannin St., Houston, TX 77030
713.441.5451
houstonmethodist.org/transplant
LEADING MEDICINE ADVANCED ORGAN FAILURE AND TRANSPLANT
2 0 1 4 - 2 0 1 5 Y E A R I N R E V I E W

Our commitment to advancing medicine with global impact
begins in Houston, Texas, where we pioneer a better tomorrow
through research, innovation and breakthroughs to rewrite the
future of health.
THAT’S THE DIFFERENCE BETWEEN PRACTICING MEDICINE AND LEADING IT.
Visit houstonmethodist.org/research to see all the ways we’re leading research.
©2015 Time Inc. FORTUNE and 100 Best Companies to Work For are registered trademarks of Time Inc. and are used under license. FORTUNE and Time Inc. are not affiliated with, and do not endorse products or services of Houston Methodist.
LEADERS IN RESEARCH At Houston Methodist, we are dedicated to defining the future of
medicine. We engineer discoveries in the lab to become clinically
useful products, channel the best innovations through early-stage
clinical trials, and actively transition those innovations to our
industry partners. Our commitment to the full cycle of discovery
and delivery sets us apart as leaders who provide patients from
around the world access to the latest health care advances.
34
26
10
32
CONTENTSLEADING MEDICINE: AN OVERVIEW 03
MAKING TRANSPLANT HISTORY:
SKULL/SCALP AND SOLID ORGANS 04
MYUNG H. PARK, MD: MULTIFACETED APPROACHES TO HEART FAILURE AND PULMONARY HYPERTENSION 06
ADAANI FROST, MD, CREATES A GLOBAL CENTER FOR
LUNG DISEASE AND TRANSPLANT 07
PHILANTHROPY TO FURTHER TRANSPLANT RESEARCH 08
REVOLUTIONIZING TREATMENTS TO DELIVER
BETTER OUTCOMES
HEART 10KIDNEY 12LIVER 14LUNG 20
EXPANDING COMPREHENSIVE, INTEGRATED CARE 24
PURSUING MEDICAL DISCOVERIES THROUGH RESEARCH 29
PIONEERING THE PATH IN TRANSPLANT EDUCATION 34
COVER PHOTO: R. Mark Ghobrial, MD, performs liver transplant surgery
MESSAGE FROM THE DIRECTORHouston Methodist J.C. Walter Jr. Transplant Center’s team of physicians, surgeons, scientists, nurses and other health care professionals are relentless in our pursuit of the very best therapies for patients facing end-stage organ failure. Our program continues to grow exponentially year over year, we push the envelope every day for patients with no other options, and we continue to directly translate our research into care at the bedside.
Last year, we participated in the world’s first multiple transplant of skull, scalp and solid organs — an historic transplant event. Surgical teams from Houston Methodist Hospital and The University of Texas MD Anderson Cancer Center came together to perform the scalp and skull transplant during the simultaneous transplant of a kidney and pancreas. The successful surgery ultimately required the skills of more than 50 health care professionals in an operation that lasted more than 15 hours.
Through our partnership with Houston Methodist Research Institute, as well as individual donors and foundations, we have advanced our areas of heart, kidney and lung transplant, device therapy and liver care. Our left ventricular assist device (LVAD) program is one of the largest in the country. In what has proven to be an excellent collaboration, physicians and surgeons from both the transplant center and Houston Methodist DeBakey Heart & Vascular Center work together to pursue the most advanced clinical trials in LVAD therapies. Our systematic approach to extracorporeal membrane oxygenation (ECMO) has provided increased benefit for respiratory patients who are awaiting transplant or who are in dire need of respiratory support.
Proficiency in liver transplants for even the sickest of patients has resulted in us maintaining the largest liver transplant waiting list of any facility in Texas. Additionally, in collaboration with MD Anderson, we are successfully treating previously inoperable patients with hepatocellular carcinoma and other liver cancers.
Moreover, we continue to be a national leader in clinical trials for the management of advanced organ failure and transplant. We are looking at the role of stem cells in immunosuppression, the roles of T and B cells, and a potentially landmark pharmacology trial that may provide agents to successfully treat hepatitis patients with chronic kidney disease.
We are making strides in bringing our innovations and newly made discoveries to others through publications, training and education. We offer informative conferences on advances in transplant and fellowships for transplant physicians in training. We are excited to now offer certified pancreas transplant training, providing physicians with a comprehensive fellowship in abdominal transplant — one of the few in the nation.
We invite you to browse through these pages and learn of our accomplishments and discoveries the last two years, all in the spirit of healing those with organ failure and growing the pool of viable organs that can save the lives of patients in need.
A. Osama Gaber, MD, FACSDirector, Houston Methodist J.C. Walter Jr. Transplant Center
02
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T

houstonmethodist.org/transplant
For more than 50 years, Houston Methodist J.C. Walter Jr. Transplant Center has been in the vanguard of the organ transplant field. Some of the world’s first transplants were performed here by legendary surgeons Michael E. DeBakey, MD, and George P. Noon, MD, in the 1960s, during the frontier days of transplant medicine.
Our present-day team of physicians, surgeons and researchers are equally committed to advancing the field, challenging the margins of current listing criteria, and continually looking for new and better ways to delay the need for transplant and to prolong graft life of transplanted organs. We are the largest and most comprehensive transplant center in the region, offering patients unparalleled care for end-stage organ failure, including heart, lung, liver, kidney, pancreas, islet, bone marrow and multiorgan.
The team performed its 5,000th transplant last year, with exponential growth taking place in the last decade. In 2005, transplants averaged less than 200 a year with the care of three dozen nurses, social workers and staff in a small clinic. In 2015, 421 patients underwent transplants as 150 employees prepared to move to a new outpatient clinic that occupies an entire floor.
From one inpatient unit a decade ago, Houston Methodist now has two fully dedicated transplant units and a specialized liver unit, with hundreds of health care providers fully committed to transplant patients. Likewise, research space that was once spread sporadically across the hospital campus has assembled into dedicated, contiguous space at Houston Methodist Research Institute, and has been integrated into many clinical areas.
Our world-class clinical expertise, cutting-edge technology and an integrated, multidisciplinary approach to treatment provide Houston Methodist the ability and agility to respond to needs within the transplant environment quickly and to achieve the best clinical outcomes. Our intense focus on research and innovation ensures endless advances in the therapies available to our patients.
Ranked No. 12nationally among transplant
centers based on total volume.*2014
*Source: UNOS
769total transplants
2014-2015
5,000thtransplant at Houston Methodist
performed in 2015
Ultimately, none of this would be possible without the selfless acts of organ donors and their families. This generosity drives our intrepid determination, and it is to them we dedicate this report.
LEADING MEDICINE: AN OVERVIEW J.C. WALTER JR. TRANSPLANT CENTER

PHOTO: Mayra Beltran/©Houston Chronicle. Used with permission.
04
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T

houstonmethodist.org/transplant
In a momentous transplant event that received international media coverage, surgical teams from Houston Methodist J.C. Walter Jr. Transplant Center and The University of Texas MD Anderson Cancer Center teamed up to perform a first-of-its-kind scalp and skull transplant during the simultaneous transplant of a kidney and pancreas. More than 50 health care professionals took part in the historic 15-hour operation.
James Boysen, a 55-year old software developer from Austin, Texas, had a history of medical issues that required prior treatment:
• In 1992, Boysen received a double organ transplant of a kidney and pancreas due to comorbidities associated with diabetes.
• In 2006, Boysen was treated for leiomyosarcoma, an aggressive form of sarcoma. The successful treatment of the cancer left a deep wound on Boysen’s head, which included the scalp and full thickness of his skull down to his brain.
In 2015, after 23 years, Boysen’s kidneys and pancreas began to fail. A second organ transplant was not possible because the newly transplanted organs would require Boysen to take immunosuppression drugs. This, in turn, would compromise the head wound left by the leiomyosarcoma, causing it to be prone to infection.
“The patient came to us needing a kidney and pancreas transplant, and told us he was working with Dr. Selber at MD Anderson on a scalp transplant,” said A. Osama Gaber, MD, director of the transplant center. “We have done about 50 multiple organ transplants thus far. We clearly have the experience. We discussed the patient with Dr. Selber and we all decided it was highly feasible to do the skull/scalp transplant at the time of the kidney and pancreas transplant.”
All organs and tissues came from one generous donor, according to Jesse C. Selber, MD, director of clinical research and associate professor of plastic surgery at MD Anderson, who put together the team of surgeons from MD Anderson. “This was an ideal clinical situation, and James’ patience, courage and enthusiasm were vital,” he said.
MAKING TRANSPLANT HISTORY: A MULTIPLE TRANSPLANT OF SKULL/SCALP AND SOLID ORGANS
Michael Klebuc, MD, plastic surgeon at Houston Methodist, was instrumental in the aesthetic reconstructive portion of Boysen’s procedure. “It was a very complex surgery because we had to transplant the tissues using microsurgery,” he said.
Transplant surgery for composite tissue has never been done together with solid organ implants. “Because the patient was on immunosuppressive therapy for two life-giving organs already, his level of immunosuppression was high — higher than it would have been for the skull/scalp transplant alone,” Gaber said. “Research shows a reduction in rejection rates for multiple organ transplants compared to a single organ transplant. From our standpoint, this information was incredibly significant when it came to this situation.”
Boysen is doing quite well posttransplant. “This has been a long journey and I am grateful to all the doctors who performed my transplants,” Boysen said. “I’m amazed at how great I feel and am forever grateful that I have another chance to get back to doing the things I love and being with the people I love.”
PHOTO: Mayra Beltran/©Houston Chronicle. Used with permission.
Houston Methodist Hospital is pleased to welcome Myung H. Park, MD, in her new role as division chief of heart failure and transplant. Park is nationally and internationally known for her contributions in the fields of pulmonary hypertension, heart failure and cardiac transplant. Park’s professional path has taken her from a fellowship in advanced heart failure and transplant at the Cleveland Clinic Foundation to the Ochsner Clinic in New Orleans as director of heart failure and transplant, and, most recently, to the University of Maryland Medical Center in Baltimore, where she served as director of the pulmonary vascular diseases program and director of the cardiac care unit/cardiology inpatient services.
In her new role at Houston Methodist, Park sees an opportunity to create and oversee an optimal patient care model for individuals with advanced heart failure. “We have a dedicated team of advanced heart failure specialists with expertise in cutting-edge treatment modalities such as heart transplant and mechanical circulatory support devices. We treat the full spectrum of cardiomyopathies, including the uncommon forms like amyloidosis and chemotherapy-induced heart failure,” Park said. “Our mission is to create a network approach in heart failure care delivery. By partnering with our colleagues in the community, my goal is to establish patient care models that will expand the delivery of heart failure treatments into the areas where our patients live.”
Park is working closely with colleagues in the pulmonary division to build a multidisciplinary program for pulmonary hypertension. “Pulmonary hypertension is a condition with abnormalities in pathophysiology that involve both the heart and lungs. My goal is to integrate expertise from both cardiology and pulmonology, offering our patients a complete array of expertise that is so crucial in the management and care of this complex disease state,” Park said.
Park has initiated another ambitious endeavor that will foster a unique treatment program for patients with chronic thromboembolic pulmonary hypertension (CTEPH). “This is a complex condition that is under-recognized and often misdiagnosed,” she said. “When accurately diagnosed, the condition can be completely cured with a surgical procedure called thromboendarterectomy.”
Currently, there are no CTEPH centers in the southwest region. “With the collaboration of our cardiothoracic surgeons and anesthesiologists, pulmonary and critical care services, we will be able to create a lifesaving service,” she said. Park and Alan B. Lumsden, MD, medical director of Houston Methodist DeBakey Heart & Vascular Center, are planning a 2016 symposium that will address the management of acute and chronic pulmonary emboli.
Park said she also looks forward to working closely with Houston Methodist Institute for Technology, Innovation & Education (MITIESM) in continuing her studies in the mechanism and treatment of heart failure and pulmonary hypertension. “By focusing in both left- and right-sided heart failure, as well as the pulmonary vascular bed, we’re creating a one-stop shop for all forms of heart failure,” she said.
MYUNG H. PARK, MD: MULTIFACETED APPROACHES TO HEART FAILURE AND PULMONARY HYPERTENSION
06
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
houstonmethodist.org/transplant
Adaani Frost, MD, a recognized expert in pulmonary hypertension and pulmonary fibrosis, has rejoined Houston Methodist to oversee the establishment of a new lung center, with a goal of it becoming a comprehensive global leader in respiratory diseases. Frost originally came to Houston Methodist — which was then affiliated with Baylor College of Medicine — more than 25 years ago as director of one of the few lung transplant programs in the nation. Over time, Frost’s work in lung transplant led to a further interest in end-stage lung disease.
“To me, transplant has always been the final salvage pathway for people with immutable lung disease,” Frost said. “Coming back to Houston Methodist to work with the transplant doctors and develop a center with expertise in the management of lung disease, including end-stage lung disease, is very exciting. This center will serve as an umbrella institution for diagnosis and treatment of every type of lung disorder, from early detection of lung cancer and the promotion of lung cancer awareness, to research and new therapies for pulmonary hypertension and pulmonary fibrosis.
“It is a referral center as well. It’s not just a resource for patients, it’s a resource for their physicians. Physicians can send us a patient with the full knowledge that the patient is coming back to them with the information, expertise and direction required for their optimum care.”
In addition, Frost wants to build the lung center into a research hub. “All patients coming into the lung center ideally will contribute to data, information and scientific development in their own disease areas,” Frost said. ”At the end of two or three years, we may have information and biological samples on perhaps thousands of patients with asthma, COPD, pulmonary fibrosis and sarcoidosis. All of this anonymous patient information will be identified by diagnosis and outcome. This data then will be coupled with biological samples that our research colleagues can basically mine for new information about the contributors to disease, the genetic basis of disease, and the cellular and molecular markers of disease and disease progression.”
ADAANI FROST, MD, CREATES A GLOBAL CENTER FOR LUNG DISEASE AND TRANSPLANT
08
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
A GIVING LEGACY: THE FAMILY OF J.C. WALTER, JR.
Houston Methodist is home to one of the fastest growing transplant centers in the nation. Advancements in the program here have been made possible in large part from the generous commitment made in memory of Joseph C. Walter, Jr. Walter’s heart transplant in 1990 extended his life by seven years and allowed him additional time with family, including the birth of his grandchildren.
In appreciation, Walter’s children — J.C. “Rusty” Walter III and his sister, Carole Walter Looke — gave $10 million in support of the transplant facility. In 2010, the program was renamed Houston Methodist J.C. Walter Jr. Transplant Center in recognition of their father, who served on the Houston Methodist board for 30 years. Today, the center stands apart as the largest and most comprehensive transplant center in the region and one of the largest heart-lung transplant programs in the world.
PHILANTHROPY TO FURTHER TRANSPLANT RESEARCH
The field of transplantation is unique in that
no other area of medicine exists where the
concept of donation is so vital to its success —
from the selfless donation of viable organs to
funding for critical research.
The family of J.C. Walter, Jr. From left in back: Joseph C. “Rusty” Walter III, Paula Walter, Carole Walter Looke and C. James Looke III Seated in front: Elizabeth Walter

A GENEROUS DISPLAY OF GRATITUDE: SHERRIE AND ALAN CONOVER
After a successful liver transplant at Houston Methodist, Alan Conover and his wife Sherrie donated $6.5 million to the hospital’s liver program. The center was renamed Sherrie and Alan Conover Center for Liver Disease & Transplantation in June 2015.
The Conovers’ generous gift will help develop resources and support for family members and caregivers who are away from home tending to their loved one, as well as fund research. “This substantial and thoughtful gift will allow us to expand our clinical and research programs ever further,” said R. Mark Ghobrial, MD, PhD, director of the Conover Center. “We are currently researching new forms of immunosuppression strategies for reducing complications and new ways to fight postoperative infection. This gift gives us a better chance to reach those goals.”
MAGNANIMOUS SUPPORT FROM THE JLH FOUNDATION
Since its inception nearly 20 years ago, the JLH Foundation has generously supported Houston Methodist in advancing patient care and research at the transplant center, as well as assisting transplant patients with medication and other medical expenses. The foundation was established by the family of John L. Hern of Houston, who waited 252 days for a heart transplant at Houston Methodist Hospital in 1996.
Today, Houston Methodist J.C. Walter Jr. Transplant Center stands apart as the largest and most comprehensive transplant center in the region and one of the largest heart-lung transplant programs in the world.
From left: Sherrie and Alan Conover, R. Mark Ghobrial, MD, PhD, and Ed Jones, chief operating officer at Houston Methodist Research Institute

10
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
Jerry D. Estep, MD, medical director, heart and heart-lung transplant
The small wireless sensor is placed percutaneously into the patient’s pulmonary artery (PA) where it proactively measures PA pressure, an indirect measurement of fluid buildup in the heart. The monitor measures pressure in patients with either systolic or diastolic heart failure.
WIRELESSLY MONITORING THE FAILING HEARTHouston Methodist Hospital is one of the first hospitals in the country to adopt the CardioMEMS heart failure system to wirelessly monitor patients with compromised heart function. Use of the CardioMEMS monitor significantly reduces hospital admissions for patients with heart failure who continue to struggle with symptoms. In addition, research has documented a significant reduction in 30-day readmissions with the use of this device.

houstonmethodist.org/transplant
A heart failure exacerbation results when there is too much pressure (due to fluid buildup) in the lungs because the heart cannot pump efficiently. Such fluid buildup progresses over a period of several days and is frequently preceded by increased PA pressures in patients who are otherwise asymptomatic. The CardioMEMS system transmits PA pressure data to clinicians from the comfort of patients’ homes, allowing physicians to treat compromised heart function more quickly and reducing the need for hospitalization.
“If we see that the patient’s blood pressure is consistently high, we call in an alert,” said Arvind Bhimaraj, MD, MPH, heart failure cardiologist at Houston Methodist. “We explain to the patient that we see an irregularity and we adjust either medication or fluid intake.”
Studies show that one hospitalization for heart failure places that patient at a 35-percent risk of dying within a few years. Wireless monitoring will help clinicians and patients drastically lower this statistic.
The system doesn’t use batteries or power. Instead, the patient reclines on a pillow containing an antenna that translates the levels of blood flow and pressure into signals. With a press of a button, the antenna picks up the pressure and transmits it into the portal, which can be accessed on the Internet.
HEART TRANSPLANTS 2014
24 2015
38
116 TOTAL LVAD IMPLANTS2014-2015
10.1%9.5%
Houston Methodist HospitalNational SRTR Benchmark
2015 Waitlist Mortality Rate
Advanced heart failure team, from left: Arvind Bhimaraj, MD; Myung H. Park, MD; Barry Trachtenberg, MD; Ashrith Guha, MD; Guillermo Torre-Amione, MD

12
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
88%
90%
92%
94%
96%
98%
100%
84%
86%
Jul 11 Jan 12 Jul 12 Jan 13 Jul 13 Jan 14 Jul 14 Fall 14
KIDNEY TRANSPLANT PROGRAM (2014)SRTR 3 Year Patient Survival Trending
National
HMH Observed
HMH Expected
90%
92%
94%
96%
98%
100%
88%
Jan 12 Jul 12 Jan 13 Jul 13 Jan 14 Jul 14 Fall 14 Spring 15 Fall 15 Spring 16
KIDNEY TRANSPLANT PROGRAM (2015)SRTR 1 Year Patient Survival Trending
National
HMH Observed
HMH Expected
In 2015, living donor transplants made up 54 percent of the 171 total kidney transplants performed at Houston Methodist J.C. Walter Jr. Transplant Center. This is made possible by an aggressive paired kidney donation program that significantly increases the availability of viable kidney donors nationally, locally and internally.
Paired kidney donation is benefited at the transplant center by state-of-the-art software that uses advanced matching and optimization algorithms to increase the number of available organs in the internal donation pool. Given the national shortage of available organs, paired kidney donation can significantly increase the availability of viable kidney donors, evaluating potential matches from two-way up to 12-way combinations within minutes, saving transplant centers months of work previously required to assess a smaller number of pairs.
Potential recipients for kidneys also may be helped by unknown donors. These altruistic — or nondirected — donors are individuals who choose to donate one of their kidneys, although they do not personally know someone who will directly benefit from their benevolent gesture.
INCREASING THE ODDS: LIVING KIDNEY DONORS“Our goal is to transplant people as soon as possible,” said Jennifer Hamilton, RN, CCTC, living donor and paired donation coordinator. “The less time they’re on dialysis, the better they’re going to do with their kidney transplant. We utilize many different systems to ensure we have the maximum number of donors matched with our patients.”
In addition, surgery has become far less traumatic for the donor. Kidney removal is now done less invasively. “Not only is it done laparoscopically, but we have gone from using multiple ports for donor surgery down to one port. This is a big deal,” said Lisa B. Yoder, BSN, RN, kidney and pancreas transplant manager, who has been working with the team on increasing the capabilities of the group to perform these kidney exchanges.
2014
652015
92
LIVING DONOR TRANSPLANTS
Obesity is no longer an immediate contraindication for patients with chronic kidney disease (CKD) at Houston Methodist J.C. Walter Jr. Transplant Center. Patients with a body mass index (BMI) greater than 35 who have been refused transplant surgery elsewhere may benefit from the excellent results achieved at Houston Methodist Hospital, where bariatric surgery is initially performed to obtain an optimal weight.
Historically, obesity has presented an increased risk of graft rejection and death in the transplant recipient. Rather than exclude obese patients, they are referred to Houston Methodist Weight Management Center for evaluation. “If the patient’s only hurdle for transplant qualification is losing weight, bariatric surgery could change his or her life. This person could get a transplant, stop dialysis, return to work, and be productive,” said Lisa B. Yoder, BSN, RN, kidney and pancreas transplant manager.
There is an increasing amount of research being performed on dialyzed patients with high BMIs and their potential for safe bariatric surgery. “We have enrolled a number of these patients who do not qualify for renal transplant but do qualify for bariatric surgery,” said Vadim Sherman, MD, medical director of the bariatric surgery program. “The goal is to reduce their BMI to an acceptable level for a workup and future transplant.”
Sherman and his team have found that patients typically lose significant weight within the first six months, which often helps them become eligible for transplant. “We’re finding that the outcomes for bariatric surgery in obese dialyzed patients are no different than for the general population,” he said. “We are accomplishing several positive outcomes with bariatric surgery in the CKD population. We’re
BARIATRIC SURGERY PREPARES MORE CANDIDATES FOR RENAL TRANSPLANT
assisting patients with weight loss, we’re improving and possibly resolving their obesity-related comorbidities such as diabetes and hypertension, and we’re helping them become candidates for renal transplant.”
According to Sherman, all of these positives are possible with a low risk of complications. These impressive outcomes have led Sherman and his team to begin similar studies in other obese end-stage organ failure patients, such as those requiring liver and heart transplants.
houstonmethodist.org/transplant
“ We’re finding that the outcomes for bariatric surgery in obese dialyzed patients are no different than for the general population.” VADIM SHERMAN, MD

14
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
Houston Methodist Hospital has the largest liver patient waiting list of any transplant center in Texas. At Sherrie and Alan Conover Center for Liver Disease & Transplantation at Houston Methodist J.C. Walter Jr. Transplant Center, physicians and transplant surgeons under the direction of R. Mark Ghobrial, MD, PhD, continue to explore the treatment boundaries of what is safely possible to help patients in dire need. Multidisciplinary teams have been specifically trained in all stages of liver transplant care. This unique combination of skills allows the team to extend the criteria of limitations that could disqualify extremely sick patients from the benefit of a liver transplant.
A summary of several research studies presented throughout 2014 and 2015 — referred to as “pushing the envelope” by Howard P. Monsour, Jr., MD, chief of hepatology — addressed how Houston Methodist successfully treats patients who would otherwise not be considered candidates for liver transplant. Monsour and his colleages, David Victor III, MD, transplant hepatologist and director of clinical research, and Maha Boktour, MD, MPH, epidemiologist, first presented at the International Liver Transplant Society 20th Annual International Congress in June 2014.
At the core is the need to evaluate patients individually, and not rely on a set of standard criteria. One primary area of focus was age. Many centers will not transplant patients over the age of 70. “Our group showed that if you highly select these patients — as we did in our septuagenarian study — they will actually have the same or better survival rate than in patients younger than 65,” Monsour said.
BREAKING DOWN THE BARRIERS TO LIVER TRANSPLANTMonsour contended that the same philosophy of treatment extends to patients with a high body mass index (BMI) as well. “We demonstrated that we were able to successfully transplant patients with a BMI greater than 40 with the same success and complication rates as patients with lower BMIs,” Monsour said.
Perhaps the most significant criterion for liver transplant viability is a patient’s Model for End-Stage Liver Disease (MELD) score. According to Monsour, throughout Europe and in many transplant centers around the United States, most patients are transplanted with MELD scores in the 20s. “At this time, we are transplanting patients with MELD scores greater than 40. So these are very sick patients,” Monsour said. “When we went back and looked at these high-MELD patients, we found that their survival was the same. Most importantly, their functionality at six months and one year was similar and not statistically different than patients with lower MELDs.”
Monsour believes successful liver transplantation in high-risk patients shows the intense resources that have been provided by Houston Methodist. “We are able to take these patients who were turned down at other centers and give them a good quality of life due to our surgical intensive care unit, the liver intensive care unit, the technical capabilities of our surgeons, and our postoperative care and management,” he said.
Monsour believes successful liver transplantation in high-risk patients shows the intense resources that have been provided by Houston Methodist.
houstonmethodist.org/transplant
75%
80%
85%
90%
95%
100%
70%
Jul 11 Jan 12 Jul 12 Jan 13 Jul 13 Jan 14 Jul 14 Fall 14
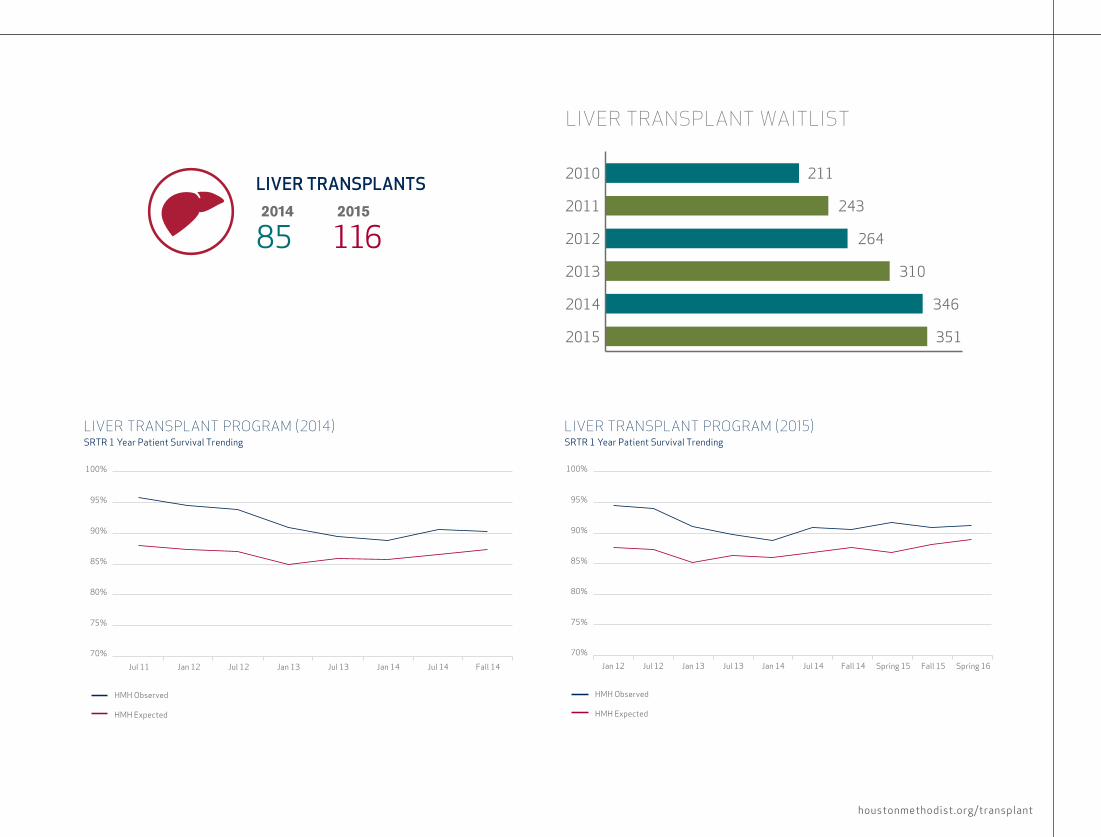
LIVER TRANSPLANT PROGRAM (2014)SRTR 1 Year Patient Survival Trending
HMH Observed
HMH Expected
75%
80%
85%
90%
95%
100%
LIVER TRANSPLANT PROGRAM (2015)SRTR 1 Year Patient Survival Trending
HMH Observed
HMH Expected
70%
Jan 12 Jul 12 Jan 13 Jul 13 Jan 14 Jul 14 Fall 14 Spring 15 Fall 15 Spring 16
LIVER TRANSPLANT WAITLIST
2010
2011
2012
2013
2014
2015
211
243
264
310
346
351
2014
85 2015
116
LIVER TRANSPLANTS

16
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
Howard P. Monsour, Jr., MD
Hepatocellular carcinoma is the most common form of liver cancer in the United States, with Texas heading the list as leader in incidence and mortality for this malignancy. Although hepatocellular carcinoma can be treated successfully when discovered early, most cases are first diagnosed at a late stage. Physicians at Houston Methodist seek to improve the survival rate from this form of liver cancer throughout Texas, with a large education campaign for both physicians and patients.
Howard P. Monsour, Jr., MD, chief of hepatology, was awarded a two-year, $150,000 grant from Amgen through the Texas Medical Association (TMA). The goal of the grant is to bring hepatocellular carcinoma into a broader focus in the Texas region. Monsour and TMA have formed a cancer committee of Texas-based, nationally recognized hepatologists and oncologists specializing in primary liver cancer to create a six-step plan that will increase physician and patient awareness, as well as stress the need for screening. Earlier detection would allow physicians and researchers to pursue curative measures.
EARLY DETECTION IS KEY TO TREATING HEPATOCELLULAR CARCINOMA
“We are designing CME conferences to be hosted at TMA meetings, a lecture series that will be given at various county medical society meetings across Texas, and a lead article that identifies the issues of hepatocellular carcinoma in Texas, which will be published in the TMA’s medical journal, Texas Medicine,” Monsour said. In addition, a patient-oriented blog, public service announcements in both English and Spanish (the rate of hepatocellular carcinoma is uniquely high in the Hispanic population), and informational ads are planned.
Earlier detection of hepatocellular carcinoma would allow physicians and researchers to pursue curative measures.

18
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T In collaboration with oncologists from The University of Texas MD Anderson Cancer Center, physicans at Houston Methodist are challenging current medical theory and proving it is possible to successfully transplant livers in patients with large liver cancers. Historically, it has been thought that large hepatocellular carcinomas and intrahepatic cholangiocarcinomas represent a poor indication for transplant due to a narrow disease-free window and low overall survival rates in those who do not undergo surgery. However, the team at Sherrie and Alan Conover Center for Liver Disease & Transplantation at Houston Methodist J.C. Walter Jr. Transplat Center continues to observe excellent outcomes in patients with both cancers — patients who were deemed to be outside the standard criteria elsewhere.
A group of physicians from Houston Methodist — R. Mark Ghobrial, MD, PhD, director of the Conover Center; Howard P. Monsour, Jr., MD, chief of hepatology; and Kirk Heyne, MD, oncologist — have developed a strong collaboration with MD Anderson
WHERE ONCOLOGY MEETS TRANSPLANT: SUCCESS FOR PATIENTS WITH LIVER CANCER
oncologists Ahmed Kaseb, MD, and Milind Javle, MD, which allows for successful liver transplants in patients with these advanced primary liver cancers. At the 20th Congress of the International Liver Transplantation Society held in June 2014 in London, results were presented that demonstrated equal four-year survival in patients with large, out-of-criteria cancers when compared to patients with smaller, in-criteria hepatocellular carcinomas. The team has performed five successful transplants in these patients to date. “We’re transplanting cholangiocarcinoma patients who have responded to chemotherapy and remained stable and well on treatment after six months,” Monsour said.
The partnership with MD Anderson has helped expand and accelerate the liver transplant program at Houston Methodist. “We’re looking at how we can transplant larger tumors,” Monsour said. “We’re working together with MD Anderson to do research and molecular profiling on the tumors. It has been an excellent collaborative program where both centers have benefited.”
Kirk Heyne, MD, and Howard P. Monsour, Jr., MD
houstonmethodist.org/transplant
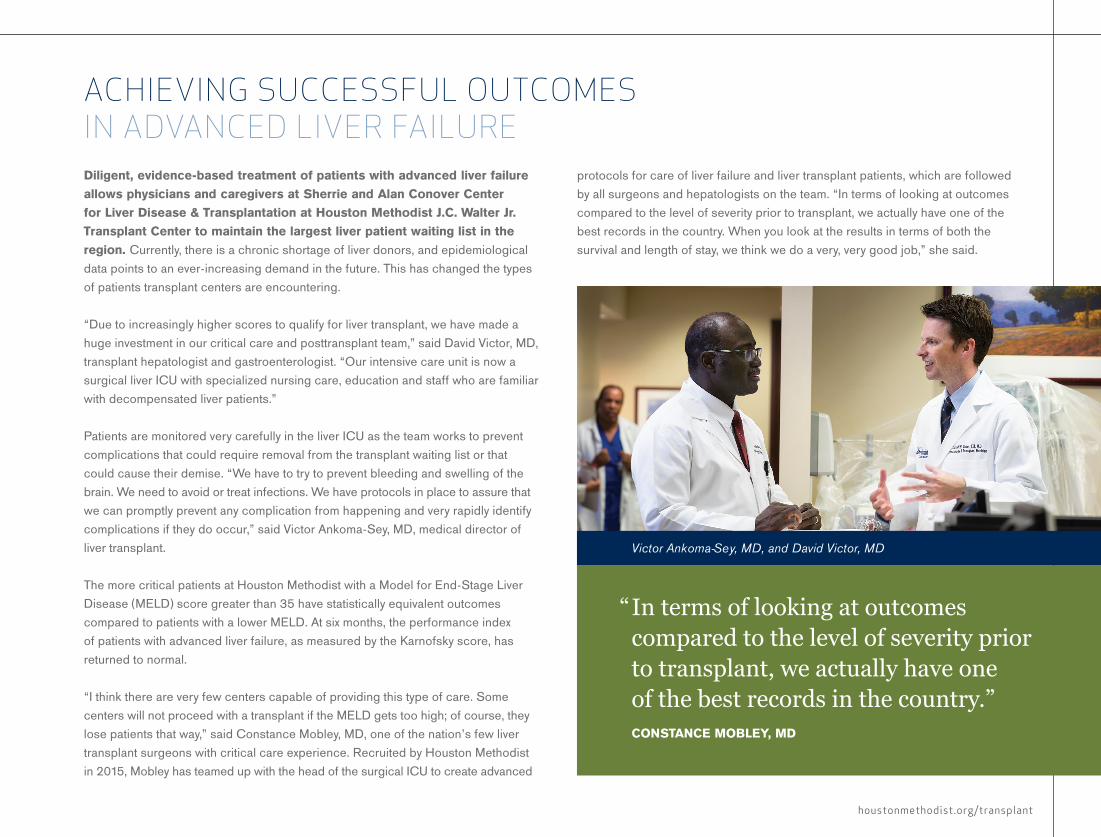
Diligent, evidence-based treatment of patients with advanced liver failure allows physicians and caregivers at Sherrie and Alan Conover Center for Liver Disease & Transplantation at Houston Methodist J.C. Walter Jr. Transplant Center to maintain the largest liver patient waiting list in the region. Currently, there is a chronic shortage of liver donors, and epidemiological data points to an ever-increasing demand in the future. This has changed the types of patients transplant centers are encountering.
“Due to increasingly higher scores to qualify for liver transplant, we have made a huge investment in our critical care and posttransplant team,” said David Victor, MD, transplant hepatologist and gastroenterologist. “Our intensive care unit is now a surgical liver ICU with specialized nursing care, education and staff who are familiar with decompensated liver patients.”
Patients are monitored very carefully in the liver ICU as the team works to prevent complications that could require removal from the transplant waiting list or that could cause their demise. “We have to try to prevent bleeding and swelling of the brain. We need to avoid or treat infections. We have protocols in place to assure that we can promptly prevent any complication from happening and very rapidly identify complications if they do occur,” said Victor Ankoma-Sey, MD, medical director of liver transplant.
The more critical patients at Houston Methodist with a Model for End-Stage Liver Disease (MELD) score greater than 35 have statistically equivalent outcomes compared to patients with a lower MELD. At six months, the performance index of patients with advanced liver failure, as measured by the Karnofsky score, has returned to normal.
“I think there are very few centers capable of providing this type of care. Some centers will not proceed with a transplant if the MELD gets too high; of course, they lose patients that way,” said Constance Mobley, MD, one of the nation’s few liver transplant surgeons with critical care experience. Recruited by Houston Methodist in 2015, Mobley has teamed up with the head of the surgical ICU to create advanced
ACHIEVING SUCCESSFUL OUTCOMES IN ADVANCED LIVER FAILURE
protocols for care of liver failure and liver transplant patients, which are followed by all surgeons and hepatologists on the team. “In terms of looking at outcomes compared to the level of severity prior to transplant, we actually have one of the best records in the country. When you look at the results in terms of both the survival and length of stay, we think we do a very, very good job,” she said.
“ In terms of looking at outcomes compared to the level of severity prior to transplant, we actually have one of the best records in the country.” CONSTANCE MOBLEY, MD
Victor Ankoma-Sey, MD, and David Victor, MD
20
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
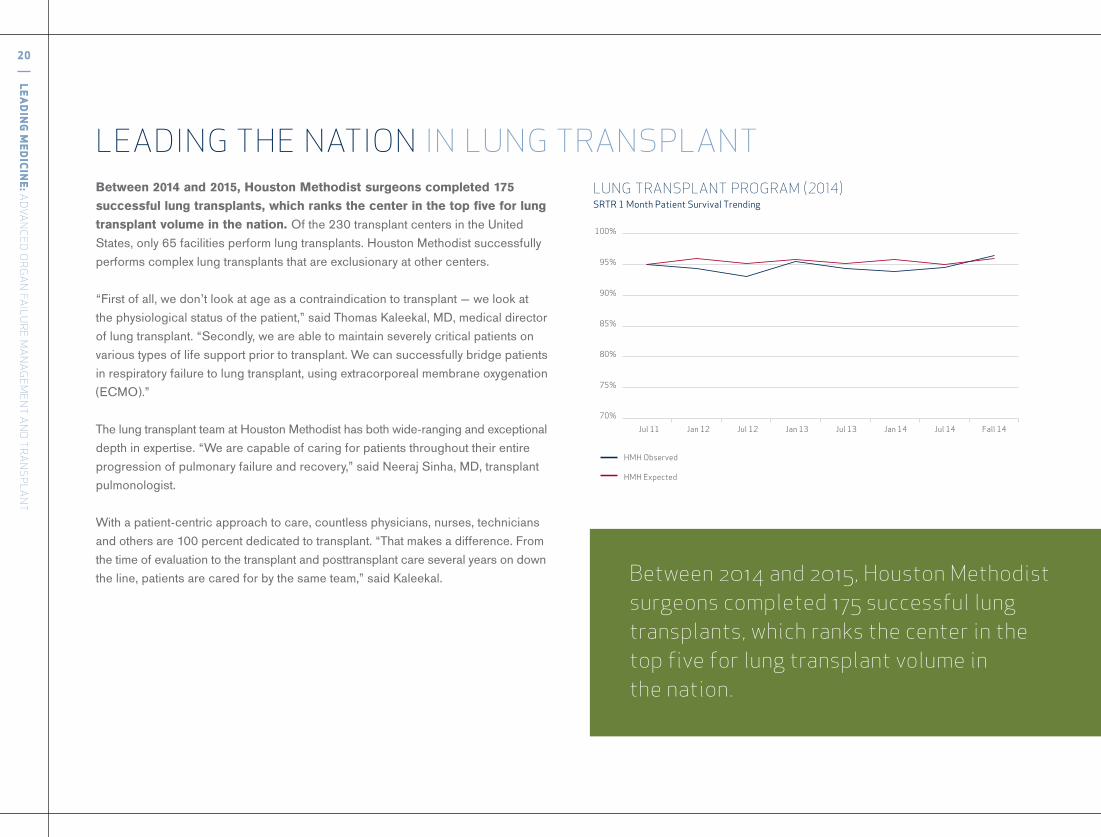
LEADING THE NATION IN LUNG TRANSPLANTBetween 2014 and 2015, Houston Methodist surgeons completed 175 successful lung transplants, which ranks the center in the top five for lung transplant volume in the nation. Of the 230 transplant centers in the United States, only 65 facilities perform lung transplants. Houston Methodist successfully performs complex lung transplants that are exclusionary at other centers.
“First of all, we don’t look at age as a contraindication to transplant — we look at the physiological status of the patient,” said Thomas Kaleekal, MD, medical director of lung transplant. “Secondly, we are able to maintain severely critical patients on various types of life support prior to transplant. We can successfully bridge patients in respiratory failure to lung transplant, using extracorporeal membrane oxygenation (ECMO).”
The lung transplant team at Houston Methodist has both wide-ranging and exceptional depth in expertise. “We are capable of caring for patients throughout their entire progression of pulmonary failure and recovery,” said Neeraj Sinha, MD, transplant pulmonologist.
With a patient-centric approach to care, countless physicians, nurses, technicians and others are 100 percent dedicated to transplant. “That makes a difference. From the time of evaluation to the transplant and posttransplant care several years on down the line, patients are cared for by the same team,” said Kaleekal. Between 2014 and 2015, Houston Methodist
surgeons completed 175 successful lung transplants, which ranks the center in the top five for lung transplant volume in the nation.
75%
80%
85%
90%
95%
100%
70%
Jul 11 Jan 12 Jul 12 Jan 13 Jul 13 Jan 14 Jul 14 Fall 14
LUNG TRANSPLANT PROGRAM (2014)SRTR 1 Month Patient Survival Trending
HMH Observed
HMH Expected
houstonmethodist.org/transplant
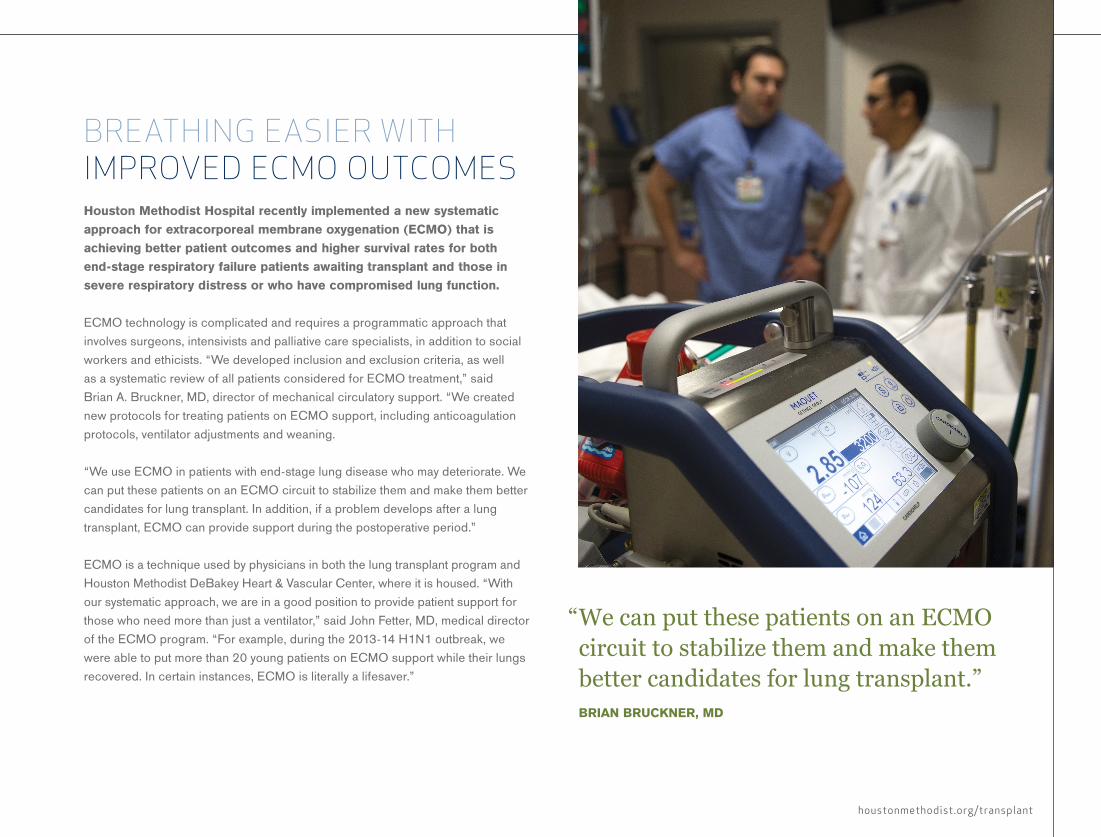
Houston Methodist Hospital recently implemented a new systematic approach for extracorporeal membrane oxygenation (ECMO) that is achieving better patient outcomes and higher survival rates for both end-stage respiratory failure patients awaiting transplant and those in severe respiratory distress or who have compromised lung function.
ECMO technology is complicated and requires a programmatic approach that involves surgeons, intensivists and palliative care specialists, in addition to social workers and ethicists. “We developed inclusion and exclusion criteria, as well as a systematic review of all patients considered for ECMO treatment,” said Brian A. Bruckner, MD, director of mechanical circulatory support. “We created new protocols for treating patients on ECMO support, including anticoagulation protocols, ventilator adjustments and weaning.
“We use ECMO in patients with end-stage lung disease who may deteriorate. We can put these patients on an ECMO circuit to stabilize them and make them better candidates for lung transplant. In addition, if a problem develops after a lung transplant, ECMO can provide support during the postoperative period.”
ECMO is a technique used by physicians in both the lung transplant program and Houston Methodist DeBakey Heart & Vascular Center, where it is housed. “With our systematic approach, we are in a good position to provide patient support for those who need more than just a ventilator,” said John Fetter, MD, medical director of the ECMO program. “For example, during the 2013-14 H1N1 outbreak, we were able to put more than 20 young patients on ECMO support while their lungs recovered. In certain instances, ECMO is literally a lifesaver.”
BREATHING EASIER WITH IMPROVED ECMO OUTCOMES
“ We can put these patients on an ECMO circuit to stabilize them and make them better candidates for lung transplant.” BRIAN BRUCKNER, MD

22
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
Scott Scheinin, MD

Houston Methodist is the world’s first institution to have a dedicated bloodless lung transplant program. The concept of bloodless surgery arose from a need to operate on Jehovah’s Witness patients who do not accept transfusions, believing that Scripture forbids the transfusion of blood.
Surgeons and their teams at Houston Methodist J.C. Walter Jr. Transplant Center tackled the challenge of bloodless surgery with cardiac operations initially, and achieved good outcomes. As a result of this success, the principles and techniques of bloodless surgery were carefully integrated into lung transplant three years ago.
Scott Scheinin, MD, surgical director of thoracic transplant, attributes the success to the multidisciplinary care team. “It’s not easy doing a bloodless lung transplant. You can follow the guidelines to a T, but if your operative execution is not perfect, then the outcome will be bad,” he said. “The reason this has been a success is because we have a dedicated group of surgeons, anesthesiologists and care professionals afterwards — the nurses on the floor. Everyone is involved.”
The transplant team takes a stringent, multipronged approach to bloodless surgery, which begins with the initial patient evaluation and treatment of any form of anemia. Perioperatively, a variety of techniques are used.
FIRST IN THE WORLD TO PERFORM BLOODLESS LUNG TRANSPLANTS
Thus far, 16 patients have received bloodless lung transplants — approximately 10 patients from Houston and six referred from out of state. “I think it is important to note that we have not lost a single patient in the early transplant period. No one has had a complication related to the fact that the individual didn’t accept blood transfusions,” Scheinin said.
From left: Dewei Ren, MD; Erik Suarez, MD; Ahmad Goodarzi, MD; Neeraj Sinha, MD; Jihad Youssef, MD
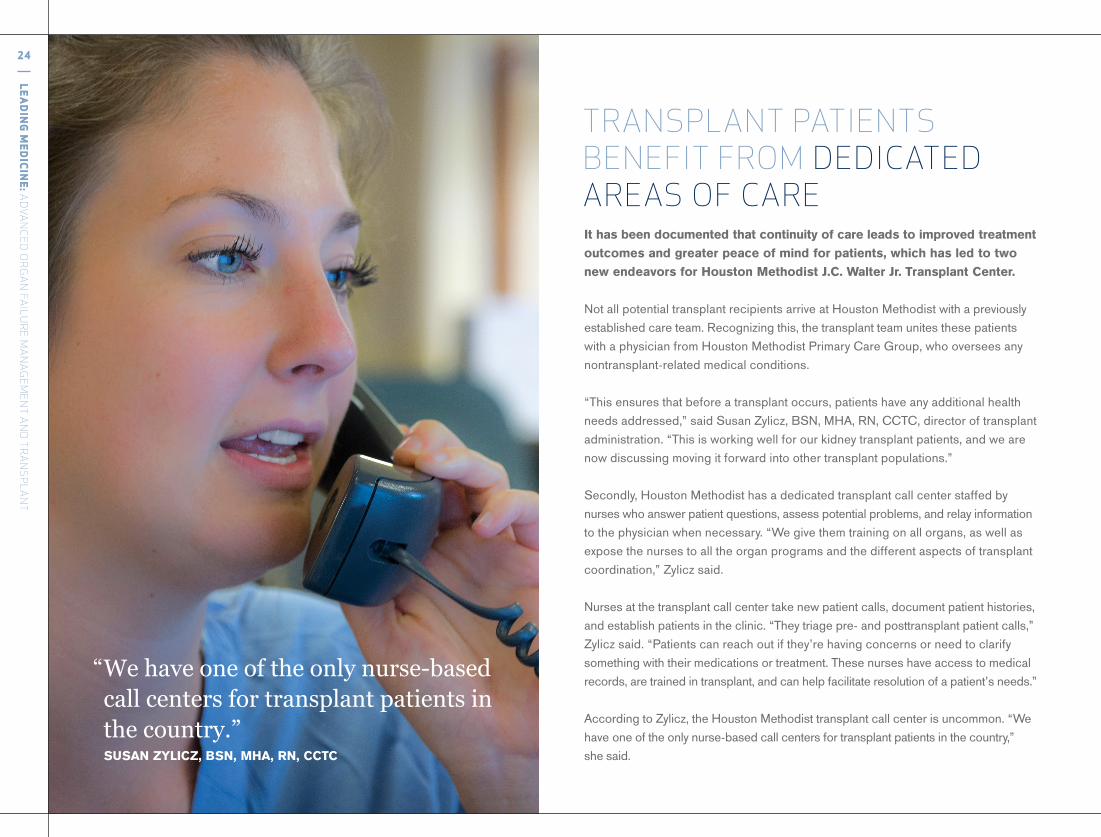
It has been documented that continuity of care leads to improved treatment outcomes and greater peace of mind for patients, which has led to two new endeavors for Houston Methodist J.C. Walter Jr. Transplant Center.
Not all potential transplant recipients arrive at Houston Methodist with a previously established care team. Recognizing this, the transplant team unites these patients with a physician from Houston Methodist Primary Care Group, who oversees any nontransplant-related medical conditions.
“This ensures that before a transplant occurs, patients have any additional health needs addressed,” said Susan Zylicz, BSN, MHA, RN, CCTC, director of transplant administration. “This is working well for our kidney transplant patients, and we are now discussing moving it forward into other transplant populations.”
Secondly, Houston Methodist has a dedicated transplant call center staffed by nurses who answer patient questions, assess potential problems, and relay information to the physician when necessary. “We give them training on all organs, as well as expose the nurses to all the organ programs and the different aspects of transplant coordination,” Zylicz said.
Nurses at the transplant call center take new patient calls, document patient histories, and establish patients in the clinic. “They triage pre- and posttransplant patient calls,” Zylicz said. “Patients can reach out if they’re having concerns or need to clarify something with their medications or treatment. These nurses have access to medical records, are trained in transplant, and can help facilitate resolution of a patient’s needs.”
According to Zylicz, the Houston Methodist transplant call center is uncommon. “We have one of the only nurse-based call centers for transplant patients in the country,” she said.
TRANSPLANT PATIENTS BENEFIT FROM DEDICATED AREAS OF CARE
“ We have one of the only nurse-based call centers for transplant patients in the country.” SUSAN ZYLICZ, BSN, MHA, RN, CCTC
24
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T

houstonmethodist.org/transplant
Caregivers at Houston Methodist J.C. Walter Jr. Transplant Center recognize the problem that distance can create for potential transplant patients in a state as large as Texas. To ease this burden, Houston Methodist has opened a transplant clinic in Lubbock to help assess and care for potential liver, kidney and pancreas transplant patients in the West Texas/eastern New Mexico region.
Richard J. Knight, MD, director of pancreas and kidney-pancreas transplant, oversees kidney and pancreas patients. “The idea is that we can do the majority of their pretransplant workup in Lubbock rather than bringing them all the way to Houston, because the workup process is very lengthy,” Knight said. “If a patient in Lubbock is a candidate for a living donor kidney transplant, his or her only trip to Houston would be for the actual transplant. Everything else can be done in Lubbock.”
Timing is crucial when patients must travel to Houston for their transplant. “If we call them on a Thursday night and say we’ve got a kidney for you and we’re going to do the transplant in the morning, we have to figure out a way to get them to Houston,” Knight said. “If they have the stamina, they will drive. They fly if they can afford to. Alternatively, there’s a type of air ambulance service in Lubbock that will bring patients to Houston.”
Tinsay Woreta, MD, MPH, is a Lubbock hepatologist affiliated with Houston Methodist who cares for patients in need of a liver transplant and posttransplant patients. “Once a month, we have a liver transplant clinic where patients can be referred from anywhere in this West Texas/eastern New Mexico area to be seen and
BROADENING OUR REACH: TAKING TRANSPLANT PROGRAMS TO WEST TEXAS
evaluated for liver transplant,” Woreta said. “Inpatients who are too sick to be discharged from the hospital due to complications of end-stage liver disease can be transferred directly to Houston Methodist to undergo inpatient transplant workup and listing. In the past eight months, I have sent five very ill patients to Houston Methodist, four who received a liver transplant and are doing well, and one who is currently listed.”
Without the Houston Methodist outreach program in Lubbock, potential transplant patients would have to travel to Dallas, San Antonio or Houston for all appointments. “We’re just trying to make it a little bit easier for the patient by going out there to perform as much of the workup and follow-up care as we can,” Knight said.
“ We can do the majority of their pretransplant workup in Lubbock rather than bringing them all the way to Houston.” RICHARD J. KNIGHT, MD

Nora’s Home is a unique, independent hospitality home that provides affordable lodging for the more than 700 patients and families who stay there each year after traveling to the Texas Medical Center for a transplant. No other facility in Houston offers specialized lodging for transplant patients.
“We are happy to become a member of the Texas Medical Center,” said Kayla Lehmann, executive director of Nora’s Home. “This reflects the depth of our commitment to transplant patients across the entire medical center.”
As the number of individuals who require transplant increases annually, the staff at Nora’s Home must turn away three patients and their families for every family they accept.
“Because of the capacity issue, Nora’s Life Gift Foundation is expanding Nora’s Home to triple the space so no one has to be turned away.” said A. Osama Gaber, MD, director of the transplant center and president of the board of directors for Nora’s Life Gift Foundation. “Houston Methodist donated the land and has always been a major supporter of Nora’s Home. The physicians, nurses and administrators are generous contributors.”
Nora’s Home has become a major hub for volunteers — employees from Houston Methodist and other hospitals — who want to further support transplant patients and their families. This year, a major art project is underway at Nora’s Home that encourages patients to paint tiles depicting their transplant experience.
“It is developed by one of our high school volunteers, Claire McCarthy. We already have a wall of these beautiful tiles, with everybody describing their journey through transplantation,” Gaber said. “It’s amazing what people create when given the chance to express themselves.”
Nora’s Home honors the memory of Gaber’s daughter. To learn more, visit the Nora’s Home website at norashome.org.
NORA’S HOME OFFERS A HOME AWAY FROM HOME
“ Houston Methodist is helping expand Nora’s Home to triple the space so no one has to be turned away.” A. OSAMA GABER, MD
26
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T

houstonmethodist.org/transplant
At Houston Methodist J.C. Walter Jr. Transplant Center, nurse dialysis liaisons improve the communication between dialysis centers and the transplant center. Dialysis liaisons are clinical nurses who work closely with dialysis centers to keep patients updated on their transplant status. Houston Methodist is one of the first hospitals in the country where nurse liaisons have addressed the communication gap between these two entities.
Confusion can easily develop in the dialysis/transplant data trail. There is no central dialysis center that serves as a hub for all patients on the transplant list. Instead, clinical information and personal data are scattered across numerous dialysis centers — information that is critical to the patient and must be maintained by the transplant center. When a patient’s health status worsens or a patient switches dialysis centers, the liaison must document the changes and communicate it back to the transplant center. To maintain excellence of care, there cannot be any gaps in this process.
“We have a standard frequency of updating the dialysis center electronically on our patients,” said Lisa B. Yoder, BSN, RN, kidney and pancreas transplant manager. “When the liaisons are at the dialysis units, they review these updates with individuals who have been referred for transplant or review the status with patients on the list.”
The liaison also performs chairside patient assessments at the dialysis centers and asks about changes in health status, addresses concerns about transplant, and discusses any questions the patient may have. In this way, the nurse dialysis liaison can help the patient adjust to the idea of transplant, calm anxieties, and educate the patient in what to expect posttransplant.
“We created the dialysis liaison role to improve communication between dialysis centers and transplant centers,” said Charlotte Roach, BSN, RN, CCTC, Houston Methodist’s first dialysis liaison and a former heart and kidney transplant coordinator. “This will allow everyone on the team and within the center to function as partners and provide the best possible care to our patients.”
NURSE DIALYSIS LIAISONS CLOSE A CRITICAL CARE GAP FOR TRANSPLANT PATIENTS
Houston Methodist is one of the first hospitals in the country where nurse liaisons have addressed the communication gap between dialysis centers and the transplant center.
Charlotte Roach, BSN, RN, CCTC

STATE-OF-THE-ART FACILITY FOR ORGAN FAILURE AND TRANSPLANT CARETransplant patients are a unique patient group who often require comprehensive care and specialized services that do not translate well into either an acute care unit or a skilled nursing facility. This gap in medical resources is a significant concern for transplant teams who recognize the need for consistency of care on an extended, albeit temporary, basis. At Houston Methodist, this medical quandary has been addressed by the recent acquisition of its first long-term acute care hospital (LTACH).
Along with other patient groups, Houston Methodist St. Catherine Hospital bridges the need for intermediate care for transplant patients. The specialized multidisciplinary team at the hospital is distinguished by servicing patients with a fairly specific group of medical disorders. For transplant patients, the interim medical care offered at the hospital benefits individuals with multiorgan or multisystem failure, those who require inpatient dialysis, ventilator-dependent patients, and patients with posttransplant complications. Many LTACH patients simply need daily care from a dedicated medical team for a longer period (typically 25 days or more) before they are well enough to return home.
GROWING TO SERVEIn October 2015, the first patient walked through the doors of a new-and-improved transplant clinic at Houston Methodist. Located on the top floor of the 26-story Houston Methodist Outpatient Center, the expanded location encompasses 36,000 square feet of open, naturally lit space that overlooks the city.
Dedicated patient clinic rooms have been specifically created for liver, lung, heart, kidney and pancreas patients, who are cared for by more than 150 employees before and after their transplants.
“The transplant clinic houses a workup center providing specialty services that the patient can immediately access, including vascular and diagnostic ultrasound, phlebotomy services and routine diagnostic tests. We are fortunate that all of these services are made available for our patients, and the entire floor is dedicated to transplant services,” said Michael Garcia, JD, RN, senior vice president. “The center was uniquely designed with the transplant patient in mind for ease of the evaluation and pre- and postoperative clinic visits. This is all available in one cohesive unit, tailor-made for the transplant patient.”
28
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T

With more than 30 years of research into kidney disease, Wadi N. Suki, MD, director of the kidney transplant program at Houston Methodist and past president of the American Society of Nephrology, continues to aggressively seek ways to improve kidney health.
In a report recently published in the American Journal of Clinical Nutrition, Suki collaborated with Linda Moore, RD, director of clinical research programs for Houston Methodist Department of Surgery, to examine the impact of dietary phosphates on survival.
“Phosphates are commonly found additives,” said Moore, lead author of the research. “This paper is a landmark contribution to understanding the impact of phosphates on survival and kidney disease.”
Phosphates are used as preservatives in soft drinks, snacks and many foods. “They actually give meat in the supermarket its intense red color,” she said.
Suki and Moore gathered patient data from 2003 to 2006 to determine what foods people were eating and how these foods affected blood phosphorus levels. Foods were rated and phosphate content quantified based on Academy of Nutrition and Dietetics guidelines. Blood phosphate levels were determined from lab tests performed within 24 hours of the first recorded meal. Kidney function was estimated from blood creatinine levels.
“We correlated phosphate intake to survival using the National Health and Nutrition Examination Survey database,” Suki said. “Restricting phosphates turns out to be good for health and raises the issue of whether they should be regulated as food additives.”
In a separate study, Suki and a large group of researchers are working on testing the potential for kidney injury in hospitalized patients.
RESEARCHING THE KIDNEY: A LIFELONG ENDEAVOR
Wadi N. Suki, MD
houstonmethodist.org/transplant
Alcohol-related liver disease should not preclude a liver transplant nor should the patient be viewed with discrimination when placed on the liver transplant list. This is the philosophy and medical position of Joseph Galati, MD, medical director of Sherrie and Alan Conover Center for Liver Disease & Transplantation at Houston Methodist J.C. Walter Jr. Transplant Center.
First, according to Galati, the standard transplant criterion that requires a six-month period of sobriety in alcohol-related liver disease is arbitrary. “The six-month rule is not rooted in any research,” said Galati. “Many patients do not have six months to live and demonstrate sobriety. And there is no research to show that the length of time people were abstinent — whether it was three months, six months or a year — would in any way predict whether or not they would drink again after the transplant.”
To ensure the best possible outcomes for alcoholic liver patients, Galati and his team perform a careful evaluation. “We have a multidisciplinary team that incorporates social workers, dedicated transplant psychiatrists and board-certified addictionologists, and we work very closely with them to render the absolute best opinion with regard to who is high risk, medium risk or low risk for alcohol use after treatment,” Galati said.
Ethicists also consult to provide clarity to the value of a medical procedure that continues to be viewed with a fair amount of bias. “The ethicist says that if the outcome of the alcoholic liver transplant is at least as good as livers transplanted for hepatitis C and fatty liver, then it is unethical not to approve the alcoholic patient for treatment,” Galati said.
Researchers have documented that people with alcoholic liver disease have the best possible outcomes when compared to other liver transplant patients. A benchmark for determining outcomes is the manifestation of recurrent disease. In the nonalcoholic liver patient, recurrent disease refers to a return of liver disease. In the alcoholic liver patient, recurrent disease means a return to alcohol abuse.
A RE-EVALUATION OF BIAS IN ALCOHOL-RELATED LIVER DISEASE
“We know about 25 percent of patients with fatty liver disease will have a recurrence at one year. At three years, it’s 70 percent. Patients with a genetic cause of liver failure have a 30- to 50-percent recurrence rate at five years. Significant, heavy alcohol drinking is somewhere around 10 percent. So if you look at recurrent disease, alcohol is one of the lowest,” Galati said.
To spread awareness and encourage meaningful conversation, Galati hosts an annual alcohol and transplantation conference. The two-day program in 2015 was entitled, Medical and Ethical Management of Alcohol-Related Disease: Where Will We Be in 2020?
30
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
Joseph S. Galati, MD
houstonmethodist.org/transplant
At Houston Methodist J.C. Walter Jr. Transplant Center, researchers aggressively study both the beneficial and destructive function of immune cells in the realm of transplant medicine. Xian C. Li, MD, PhD, scientific director of Houston Methodist Immunobiology Research Center and director of the transplant immunology program, and his team work to decipher the mechanism of T-cell development and differentiation.
T lymphocytes play a protective role against pathogens, although their destructive actions in chronic tissue rejection is well documented. Activation of aggressive lymphocytes in the immune system is guided by a number of surface molecules and cytokine receptors that collectively control the survival and assault of activated lymphocytes. Li and his team seek to identify essential molecular targets at key stages in lymphocyte activities. Their objective is to develop therapeutic antibodies that will manipulate these checkpoints to either repress or stimulate molecular pathways. Modulation of these checkpoints would allow physicians to regulate immune responses and boost desired outcomes in transplant patients.
“When I started, I thought the best way to contain T cells was to drive them to death by apoptosis; if they die, the transplant will be fine,” Li said. “We now know that’s only part of the story. There are broadly two types of T lymphocytes — protective and disruptive — and it is the balance of these two populations that maintains homeostasis.”
In addition, scientists investigate transplant-related issues, such as the mechanisms of graft injury and repair, B cells and antibodies, immunosuppression, transplant tolerance, and diagnostic and prognostic biomarkers for rejection or acceptance.
“Our team aspires to develop new protocols to ensure survival of lifesaving transplants without lifelong immunosuppression. This would markedly enhance quality of life for transplant patients,” Li said.
IMPROVING TRANSPLANT OUTCOMES THROUGH T-CELL MANIPULATION
Hematologists at Houston Methodist are broadening the treatment armamentarium for both virus-associated diseases posttransplant and for use as targeted cancer therapy.
Research in posttransplant immunotherapy studies the characteristics that promote the healthy persistence of transferred antigen-specific cytotoxic T lymphocytes (CTLs) in an immunocompromised setting. Ongoing investigations demonstrate that CTLs can ameliorate viral disease in a posttransplant microenvironment threatened by such opportunistic infections as cytomegalovirus, Epstein-Barr virus, adenovirus and BK virus.
“Drugs used in standard therapies can be toxic to the kidney or bone marrow in immunocompromised patients,” said George Carrum, MD, hematologist and director of the bone marrow transplant program. “We are able to expand T cells and outfit them with the required immunologic properties. When transplanted, these cells enable the immunocompromised patient to combat the disease naturally, without the use of potentially harmful antiviral agents.”
In the realm of cancer treatment, Helen Heslop, MD, specialist in hematology and oncology, works with her team to target malignancies such as certain leukemias, lymphomas and myelomas. Cells are removed from the patient’s blood, modified in the laboratory with specific proteins unique to the tumor cells, and infused back into the patient. The goal of therapy is to instigate a therapeutic immune response from the manufactured CTLs that will successfully attack the cancer through an autologous cellular mechanism.
Houston Methodist hematologists are also actively studying multivirus CTLs and third party, off-the-shelf cells. “Our laboratory has been collecting cell samples from donors who have been exposed to these viruses. We have developed a number of T cells that are stored in frozen aliquots,” said Carrum. “These are ready-made cells that we can take off the shelf and provide to the patient on an as-needed basis. Thus far, our results with this third-party application are encouraging.”
REVOLUTIONIZING TREATMENTS IN BONE MARROW TRANSPLANT

Houston Methodist’s left ventricular assist device (LVAD) program has distinction as one of the largest in the country. Under the wide umbrella of cardiovascular and transplant medicine, physicians and surgeons from both Houston Methodist J.C. Walter Jr. Transplant Center and Houston Methodist DeBakey Heart & Vascular Center work together to pursue the most current and advanced clinical trials in LVAD therapy.
“We offer cutting-edge trials for several ventricular assist devices, such as HeartWare’s ENDURANCE Supplemental Trial,” said Brian Bruckner, MD, director of mechanical circulatory support at Houston Methodist. “We’re also doing the ReliantHeart’s HeartAssist device, a prospective, randomized, multicenter, clinical trial to evaluate
NATIONAL LEADERS IN LVAD RESEARCHthe safety and efficacy of 96 patients implanted with the ReliantHeart HeartAssist5® VAD system compared to 96 patients implanted with either a Thoratec HeartMate II® LVAD or HeartWare HVAD® for left ventricular support while awaiting cardiac transplantation.”
Houston Methodist is participating in Thoratec’s MOMENTUM 3 clinical trial, which will enroll more than 1,000 participants in up to 60 centers across the nation to evaluate the HeartMate 3 for use as long-term support for individuals who are not candidates for heart transplantation (known as destination therapy). The device will also be evaluated for short-term use in patients awaiting transplantation. “Houston Methodist is the first center in Texas to implant the HeartMate 3 device, which is the newest assist device out in trial,” Bruckner said.
Recently, Houston Methodist was the largest enroller in Thoratec’s pivotal ROADMAP (Risk Assessment and Comparative Effectiveness of Left Ventricular Assist Device and Medical Management in Ambulatory Heart Failure Patients) trial. Led by Jerry Estep, MD, medical director of the heart transplant and LVAD program, the trial included 200 patients and compared the HeartMate II LVAD therapy with optimal medical management in ambulatory heart failure patients who were not dependent on intravenous inotropic support but met the FDA-approved indication for destination therapy. The primary endpoint measurement was a composite of survival with improvement in the Six Minute Walk Test distance from a baseline of ≥ 75 meters at 12 months. “This study gives us, for the first time, data that carefully allows us to weigh the benefits and risks of using current LVAD therapy in this patient population. This clarity of projected benefit versus risk allows us to tailor our treatment decision more accurately and appropriately,” Estep said. The study findings were published in the October 2015 issue of the Journal of the American College of Cardiology and Estep was the first author of the paper. The two-year follow-up study of patients is currently in progress.
The VAD program at Houston Methodist has a rich history. The first assist device was implanted by Michael E. DeBakey, MD, in the 1960s. DeBakey continued to develop assist devices with George P. Noon, MD, also at Houston Methodist, and together they designed the first continuous flow pump, called the DeBakey VAD.
32
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
Hany Samir, MD, center, Brian Bruckner, MD, right
Houston Methodist was a recent participant in what will most likely be a landmark multinational study that tested the once-daily combination of two oral hepatitis C drugs in patients with chronic kidney disease (CKD). Known as the C-SURFER study, the trial found that the combination of elbasvir and grazoprevir cured both cirrhotic and noncirrhotic hepatitis C in 99 percent of patients with advanced CKD on hemodialysis. The study offers hope to a subset of patients with hepatitis C who cannot benefit from recent pharmacological advances due to complications of previous antiviral treatment.
Kidney disease progresses more rapidly in individuals with hepatitis C and frequently requires dialysis and transplantation sooner than CKD patients without the virus. In a cruel twist of biology, people with hepatitis C have a higher risk of graft failure and poor survival when transplanted.
LANDMARK STUDY FOR HEPATITIS C IN CKD PATIENTS
LEADING THE WAY IN CLINICAL TRIALSThe physicians, surgeons and scientists of Houston Methodist J.C. Walter Jr. Transplant Center continue to champion the progress of cutting-edge pharmacology, technology and procedural techniques. They accomplish this through numerous clinical trials, a few of which are highlighted below.
C-PULSE® SYSTEM: A HEART ASSIST DEVICE CLINICAL STUDY (COUNTER HF)
Jerry D. Estep, MD, leads a study to determine whether the use of Sunshine Heart’s C-Pulse Heart Assist System as a treatment for patients in moderate to severe heart failure has demonstrated safety and efficacy, such that the C-Pulse System merits FDA approval to market the device in the United States. The C-Pulse System is an implantable heart assist device that provides cardiac assistance through an extra-aortic balloon cuff and electrocardiogram (ECG) sense lead connected by a percutaneous interface lead (PIL) to an external pneumatic driver. The system provides a different approach to augment the heart’s function, not replace it. It can be implanted using a minimally invasive approach and is designed to treat clinical symptoms associated with moderate to severe heart failure.
Howard P. Monsour, Jr., MD, chief of hepatology, discussed the initial results of C-SURFER at the European Association for the Study of the Liver 50th International Liver Conference in April 2015.
“It is a huge breakthrough because the other new drugs out there have not been approved for dialysis patients,” Monsour said. “The findings are also important since most hemodialysis patients are minorities who historically have been undertreated.”
The two drugs, elbasvir and grazoprevir, are made by Merck Sharp & Dohme Corp., which also funded the study. “This is a highly significant development for the treatment of hepatitis C in CKD patients,” Monsour said.
MYFORTIC, PROGRAF AND CORTICOSTEROIDS IN DE NOVO LIVER TRANSPLANT
R. Mark Ghobrial, MD, PhD, has completed a Novartis-sponsored study that gathered information on the use of three immunosuppressive drugs — Myfortic, Prograf and corticosteroids — in new liver transplant recipients. The information obtained in this study relates to the body’s absorption, distribution, breakdown and elimination of Myfortic when used in combination with Prograf and corticosteroids in patients undergoing de novo liver transplant.
STEM CELL TREATMENT AND KIDNEY TRANSPLANT
A. Osama Gaber, MD, is the principal investigator in a phase I study that will look at the use of autologous bone marrow production of stem cells to aid in immunosuppression after a kidney transplant. Stem cells will be harvested from the patient’s bone marrow prior to transplant, incubated, and then reinfused at the time of transplant, as well as at a designated time posttransplant. The ultimate goal of this study is to determine effective dose ranging for stem cell treatment.

Houston Methodist J.C. Walter Jr. Transplant Center embodies the principles, knowledge and ethics that characterize transplant medicine. We have a commitment to educate and share this realm of medical excellence with the next generation’s best and brightest transplant physicians.
The transplant center offers fellowships for surgeons who would like to pursue thoracic transplantation. Erik Suarez, MD, is a testament of the program’s success, recently graduating and joining the Houston Methodist thoracic transplant team.
“The training was integral in my development as a cardiothoracic transplant surgeon,” said Suarez. “It made me feel comfortable with even the most complex of cases.”
In addition, Houston Methodist has recently inaugurated an abdominal transplant program. The first fellow to matriculate is Stephanie Yi, MD. Yi earned her undergraduate degree at University of California, Berkeley, and completed her medical training at the University of Buffalo.
“I really enjoy working with this patient population,” Yi said. “I feel as though I can make a difference, especially in those who suffer from chronic diseases that warrant transplantation. There is a sense of hope these patients feel when they are given this ‘second chance,’ and I want to be a part of that.”
As the largest transplant center in Texas, program director Sherilyn Gordon Burroughs, MD, said it only stands to reason that Houston Methodist would be poised to train future transplant surgeons.
“The scope and the knowledge necessary for the transplant surgeon has expanded and is much broader than in past years, so the challenge of the transplant training program is more complex,” she said. “We are required to educate the fellows not just in surgical technique, but also in the tenants of immunology and perioperative care specialized to this unique population. Techniques in minimally invasive surgery have made this specialized training even more important.”
To help embolden the aspirations of young physicians, A. Osama Gaber, MD, director of the transplant center, is attempting to secure an integrated pathway for the transplant fellowship. “There are very few transplant fellowships across the country that offer this,” he said. “We could be the first. It will allow physicians who are committed to transplant to gain access to the fellowship earlier on in their surgical training.”
PERPETUATING THE BEST AND BRIGHTEST: TRAINING THE NEXT GENERATION OF PHYSICIANS AND SURGEONS
34
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
Stephanie Yi, MD, and Sherilyn Gordon Burroughs, MD

houstonmethodist.org/transplant
ASTS-CERTIFIED PANCREAS PROGRAM ADDS DISTINCTION TO ABDOMINAL FELLOWSHIPHouston Methodist J.C. Walter Jr. Transplant Center recently expanded its abdominal fellowship program to include American Society of Transplant Surgeons (ASTS)-accredited pancreas transplant training. Only a handful of major medical centers can provide an abdominal fellowship that offers certification in pancreas transplant.
“To qualify to be a member of the fellowship training program for pancreas, you have to perform more than 20 pancreas transplants a year, on average, for three years in a row. So that would obviously be a very small number of programs,” said Richard J. Knight, MD, director of pancreas and kidney-pancreas transplant. “I think there are 12 pancreas programs out of about 70 abdominal fellowships around the country.”
The transplant center’s addition of a pancreas program to the abdominal fellowship program of liver and kidney transplant will increase its attraction to potential candidates.
“The pancreas program separates Houston Methodist from other teaching hospitals,” Knight said. “If you’re going into transplant, you would want to get certified for all three organs: kidney, liver and pancreas. And there are relatively few programs that offer the opportunity to be a certified fellow for all three organs.”
94%
93%
95%
96%
98%
99%
97%
100%
PANCREAS (ALL) TRANSPLANT PROGRAM (2015)SRTR 1 Year Patient Survival Trending
Jan 13 Jul 13 Jan 14 Jul 14 Fall 14 Spring 15 Fall 15
National
HMH Observed
HMH Expected
The summer of 2015 inaugurated a third- and fourth-year hepatology rotation for Texas A&M Health Science Center medical students. Texas A&M encompasses the priorities of Houston Methodist: to develop research and education programs that reflect health care practice in the 21st century.
“This is huge,” said Robert McFadden, MD, senior hepatologist at Houston Methodist Hospital. “Texas A&M students have taken over a whole floor in a building on our campus to be their student center. We have launched a big initiative for educating these students and even have designed an entire teaching program for this hepatology rotation.”
Houston Methodist and Texas A&M Health Science Center share joint faculty appointments and partnerships that bring creative and innovative research, as well as multidisciplinary health care degree programs, to the Texas Medical Center. These programs advance the health initiatives of the state of Texas, and advance health care for patients around the world.
NEW HEPATOLOGY ROTATION FOR TEXAS A&M MEDICAL STUDENTS
Robert McFadden, MD, and Texas A&M medical student

In December 2014, Houston Methodist J.C. Walter Jr. Transplant Center’s annual three-day George P. Noon Conference began with an in-depth examination of the current care models for patients with cholangiocarcinoma. This symposium topic, sponsored by Carol and Burt Keenan, was a Houston Methodist first. The second day’s Wadi N. Suki Conference focused on the cardiorenal axis and recent findings of the systemic inflammatory response caused by renal failure and the role of the heart in acute kidney injury. In addition, this year’s state-of-the-art lectures highlighted new methods of lung preservation, tracheal transplant, and ensuring successful heart and assist-device therapy.
The conference is named in honor of George P. Noon, MD, who, in the 1960s with Michael E. DeBakey, MD, performed some of the world’s first transplants, including the first multiorgan procurement: a heart, lung and two kidneys. Noon subsequently went on to lead the transplant and assist-device programs for many years, and is currently the head of the transplant executive council at the center.
Many have endeavored to make this conference a success, including the namesakes below.
George P. Noon, MD, has focused his surgical career on organ transplant and cardiac assist devices. In 1968, Noon, DeBakey and their surgical team performed their first heart and, later lung, transplant and worked through the early learning phases in transplantation. When the immunosuppressant cyclosporine became available in 1986, Noon and DeBakey reignited the transplant program.
GEORGE P. NOON CONFERENCE: A COLLABORATIVE FORUM TO ELEVATE INNOVATIONS IN TRANSPLANT
For more than 50 years, Noon has served the Houston community as an academic, physician and leader in the development and implementation of cutting-edge procedures and technologies that have made a difference in the lives of countless patients from Houston and around the world.
Carol and Burt Keenan are generous supporters of Houston Methodist J.C. Walter Jr. Transplant Center. Several years ago, Burt had what the majority of physicians told him was an inoperable liver tumor. He received a liver transplant by R. Mark Ghobrial, MD, PhD, in California, and followed his excellent care to Houston Methodist when Ghobrial joined the team in 2009.
Wadi N. Suki, MD, earned his medical degree from the American University of Beirut School of Medicine, and completed his postdoctoral training in internal medicine, hypertension and nephrology at The University of Texas Southwestern Medical School and Parkland Memorial Hospital in Dallas. Suki has written more than 250 articles for scientific publications that address many aspects of renal physiology and disease. He is currently director of nephrology at Houston Methodist. Suki was integral in the initiation of the kidney transplant program at Houston Methodist. His contributions have been recognized by such awards as the President’s Medal of the American Society of Nephrology, 1991; the David M. Hume Award of the National Kidney Foundation, 1994; and President of the American Society of Nephrology, 1997-98.
36
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
houstonmethodist.org/transplant
In September 2015, Houston Methodist hosted the second annual Emerging Topics in Liver Disease Conference. The conference was conceived and hosted by Victor Ankoma-Sey, MD, medical director of liver transplant. Entitled Innovative Trends in Liver Health, the day-long event provided insight into impending developments in hepatology and new approaches to the management of liver diseases.
A group of nationally renowned experts focused on four primary areas: hot topics in liver disease, end-stage liver disease, chronic viral hepatitis and primary care concerns. The new findings in liver disease were presented in a clinical context, beneficial in the multidisciplinary management of unique and complex liver disorders.
“The conference is a mixture of case presentations and lectures, panel discussions and debates about current issues in the treatment of liver disease,” said Ankoma-Sey. “It is an interactive conference with an audience response system that allows participants to ask questions and respond to polls.”
Attendees learned about the natural history and outcome of fatty liver disease and its relationship to patient management, as well as how to evaluate current therapeutic modalities and develop more effective treatment algorithms for hepatitis C and B patients. Participants identified the current and potential emerging therapies for specific liver diseases and discussed the dilemmas facing clinicians who are treating patients with end-stage liver diseases.
CURRENT DILEMMAS IN LIVER DISEASE AND EFFECTIVE TREATMENT APPROACHES
Ashish Saharia, MD, associate director, kidney and pancreas transplant
From left: R. Mark Ghobrial, MD, PhD; Sherilyn Gordon Burroughs, MD; Ashish Saharia, MD
38
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
WORLD-CLASS EDUCATION IN THE HOUSTON METHODIST CLASSROOM
“ This teaching platform allows us to help integrate the translation of recent research in liver preservation with our heart transplant practice.” BARRY TRACHTENBERG, MD
On the first Wednesday of every month, Houston Methodist hosts a transplant physician or researcher in the grand rounds program. “This is an amazing opportunity for our staff to have world-class education right at home,” said Ashish Saharia, MD, associate director of kidney and pancreas transplant and assistant professor of surgery at Weill Cornell Medicine.
The list of speakers has included national and international transplant experts such as: Francis D. Pagani, MD, PhD, University of Michigan Health System; Stefan G. Tullius, MD, PhD, Brigham and Women’s Hospital; John Julian Fung, MD, PhD, Cleveland Clinic; Nancy L. Ascher, MD, PhD, University of California San Francisco Medical Center; Christophe Legendre, MD, Paris Descartes University; and Marwan S. Abouljoud, MD, Henry Ford Medical Group.
“Besides education, these center-based grand rounds create amazing opportunities for collaboration,” said Sherilyn Gordon Burroughs, MD, transplant surgeon and director of the transplant surgery fellowship program.
With a vast array of topics covered, different organ groups have the opportunity to hear the latest advances from one another.
“This teaching platform allows us to help integrate the translation of recent research in liver preservation with our heart transplant practice,” said Barry Trachtenberg, MD, cardiologist at Houston Methodist DeBakey Heart & Vascular Center. “It is all about educating our staff and nurses. They get to learn the latest in transplantation, and it shows in the high level of care they deliver to our patients.”

Richard Knight, MD, surgical director, pancreas and kidney-pancreas transplant
TRANSPLANT LEADERSHIPA. Osama Gaber, MD, FACS Director, Houston Methodist J.C. Walter Jr. Transplant Center
Vice chair, administration and faculty affairs, Department of Surgery
George P. Noon, MD Director, Transplant Executive Council
CARDIAC TRANSPLANT & ASSIST DEVICES
Scott Scheinin, MD, FACS Surgical director, thoracic transplant
Jerry D. Estep, MD, FACC Medical director, heart and heart-lung transplant
Brian Bruckner, MD Director, mechanical circulatory support
LUNG TRANSPLANT Scott Scheinin, MD, FACS Surgical director, thoracic transplant
Thomas Kaleekal, MD Medical director, lung transplant
ECMOBrian Bruckner, MD Surgical director
John Fetter, MD Medical director
INTESTINAL FAILURE PROGRAMSherilyn Gordon Burroughs, MD, FACS Director
RENAL & PANCREAS TRANSPLANTA. Osama Gaber, MD, FACS Surgical director, kidney transplant
Richard Knight, MD, FACS Surgical director, pancreas and kidney-pancreas transplant
Juan Gonzalez, MD Co-medical director, kidney, pancreas and kidney-pancreas transplant
Horacio J. Adrogué, Sr., MD Co-medical director, kidney, pancreas and kidney-pancreas transplant
Ashish Saharia, MD Associate director, kidney and pancreas transplant
Elie Saber, MD Living donor advocate
PROCUREMENTHemangshu Podder, MD, PhD Director, abdominal procurement
Dewei Ren, MD Director, thoracic procurement
Brian J. Dunkin, MD, FACS Co-director, living donor procurement
Richard E. Link, MD, PhD Co-director, living donor procurement
LIVER TRANSPLANTR. Mark Ghobrial, MD, PhD, FACS, FRCS (Ed) Surgical director, liver transplant
Director, Sherrie and Alan Conover Center for Liver Disease & Transplantation
Victor Ankoma-Sey, MD Medical director, liver transplant
Joseph S. Galati, MD, FACGT Medical director, Sherrie and Alan Conover Center for Liver Disease & Transplantation
Howard P. Monsour, Jr., MD Chief, hepatology, Department of Medicine
BONE MARROW TRANSPLANTHelen Heslop, MD Director, Center for Cell & Gene Therapy
George Carrum, MD Director, adult outpatient clinic for cell & gene therapy
Director, National Marrow Donor Program
IMMUNOBIOLOGY RESEARCH CENTERXian C. Li, MD, PhD Director
ADMINISTRATIONMichael Garcia, JD, RN Senior vice president
Scott Flowers Vice president
Susan A. Zylicz, BSN, MHA, RN, CCTC Director, transplant administration
Julie Corkrean, BSN, RN, CCTC Liver transplant manager
Anthony Flores Financial manager
Deborah Harvey, BSN, RN, CCTC Lung transplant manager
Jordan Jeon, BA, CTBS, CPTC Transplant operations manager
Laurie Loza, BSN, RN, CCTC Heart transplant and VAD manager
Marty Martin, BSN, RN, CCTC Transplant clinical operations manager
Lisa B. Yoder, BSN, RN, CCTC Kidney and pancreas transplant manager
PSYCHIATRYInna D’Empaire, MD Pyschiatry lead
40
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
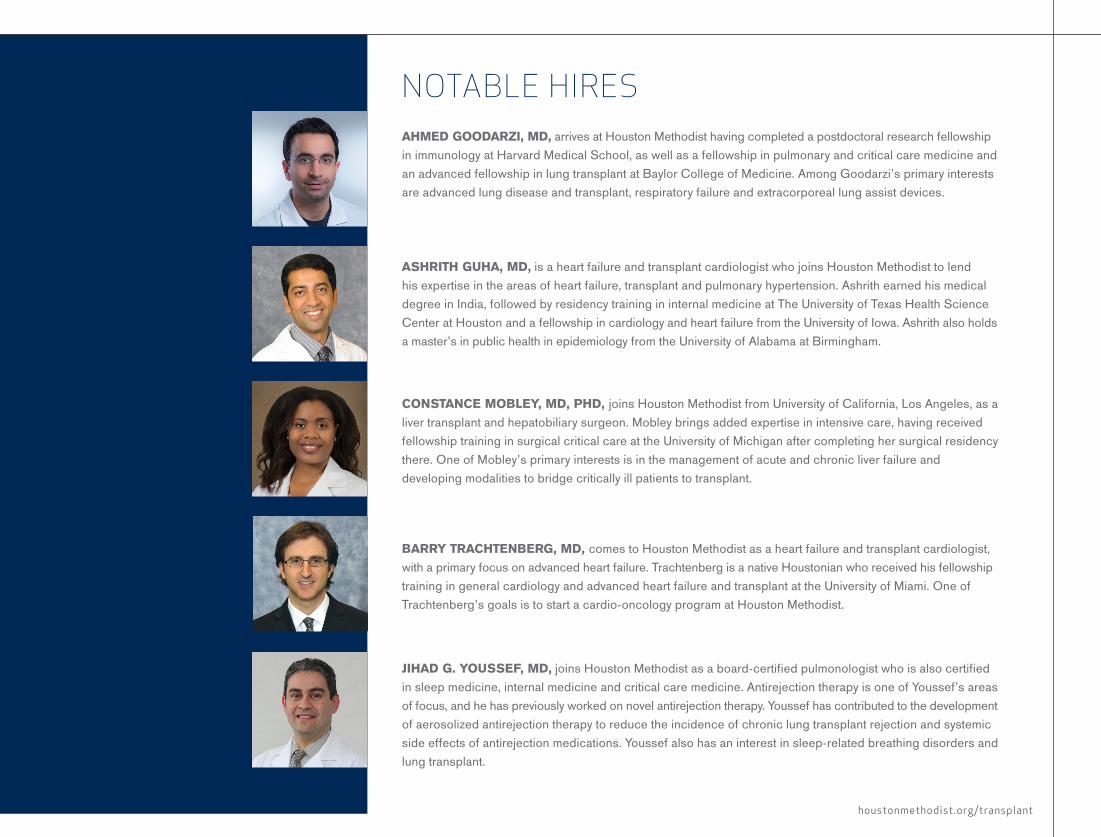
houstonmethodist.org/transplant
AHMED GOODARZI, MD, arrives at Houston Methodist having completed a postdoctoral research fellowship in immunology at Harvard Medical School, as well as a fellowship in pulmonary and critical care medicine and an advanced fellowship in lung transplant at Baylor College of Medicine. Among Goodarzi’s primary interests are advanced lung disease and transplant, respiratory failure and extracorporeal lung assist devices.
ASHRITH GUHA, MD, is a heart failure and transplant cardiologist who joins Houston Methodist to lend his expertise in the areas of heart failure, transplant and pulmonary hypertension. Ashrith earned his medical degree in India, followed by residency training in internal medicine at The University of Texas Health Science Center at Houston and a fellowship in cardiology and heart failure from the University of Iowa. Ashrith also holds a master’s in public health in epidemiology from the University of Alabama at Birmingham.
CONSTANCE MOBLEY, MD, PHD, joins Houston Methodist from University of California, Los Angeles, as a liver transplant and hepatobiliary surgeon. Mobley brings added expertise in intensive care, having received fellowship training in surgical critical care at the University of Michigan after completing her surgical residency there. One of Mobley’s primary interests is in the management of acute and chronic liver failure and developing modalities to bridge critically ill patients to transplant.
BARRY TRACHTENBERG, MD, comes to Houston Methodist as a heart failure and transplant cardiologist, with a primary focus on advanced heart failure. Trachtenberg is a native Houstonian who received his fellowship training in general cardiology and advanced heart failure and transplant at the University of Miami. One of Trachtenberg’s goals is to start a cardio-oncology program at Houston Methodist.
JIHAD G. YOUSSEF, MD, joins Houston Methodist as a board-certified pulmonologist who is also certified in sleep medicine, internal medicine and critical care medicine. Antirejection therapy is one of Youssef’s areas of focus, and he has previously worked on novel antirejection therapy. Youssef has contributed to the development of aerosolized antirejection therapy to reduce the incidence of chronic lung transplant rejection and systemic side effects of antirejection medications. Youssef also has an interest in sleep-related breathing disorders and lung transplant.
NOTABLE HIRES

TRANSPLANT TEAM MEMBERSDIRECTORA. Osama Gaber, MD, FACS
CARDIOLOGYArvind Bhimaraj, MDJerry D. Estep, MD, FACCAshrith Guha, MDMyung H. Park, MDGuillermo Torre-Amione, MD,
PhD, FACCBarry Trachtenberg, MDDanelle McLain, NPLoren Semones, NP
HEART TRANSPLANTSURGERYBrian Bruckner, MDScott Scheinin, MD, FACSErik Suarez, MD
PULMONOLOGYThomas Kaleekal, MDNeeraj Sinha, MDJihad Youssef, MDAhmad Goodarzi, MD
LUNG TRANSPLANTSURGERYBrian Bruckner, MDScott Scheinin, MD, FACSErik Suarez, MDEdward Chan, MD
NEPHROLOGYAbdul Abdellatif, MDHoracio J. Adrogué, Sr., MDMario Assouad, MDSandra Barrow, MDStephen Brennan, MDJoey Buquing, MDJoslyn Campbell, MDLazaro Cherem, MDJuan Gonzalez, MD
Namrata Goel, MDAnna Kagan, MD, PhD, FASNA. Jabbar Khan, MDMehreen Khan, MDUday Khosla, MDSreedhar Mandayam, MDJustin Merszei, MDGeorge Nassar, MD, FASNPeter Tuan Nguyen, MD, FASNRahman Noor, MDJuan Jose Olivero, MD, FACP, FASNJuan Jorge Olivero, MD, FASNRupal Patel, MDVenkataraman Ramanathan, MDEdward Rhee, MDAnand Saranathan, MDWadi N. Suki, MD, FACP
INTERNAL MEDICINEEllie Saber, MD
KIDNEY TRANSPLANTSURGERYBrian James Dunkin, MD, FACSA. Osama Gaber, MD, FACSAlvin Goh, MDR. Mark Ghobrial, MD, PhD, FACS,
FRCS(Ed)Sherilyn Gordon Burroughs, MD,
FACSRichard Knight, MD, FACSRichard E. Link, MD, PhDHemangshu Podder, MD, PhDAshish Saharia, MDLaura Lessard, NP
HEPATOLOGYVictor Ankoma-Sey, MDChukwuma Egwim, MDJoseph S. Galati, MD, FACGTRashid Khan, MDRobert McFadden, MDHoward P. Monsour, Jr., MD
Malakel Rahy, MDDavid Victor, MDJanine Hyden, NPHung Nguyen, NP
LIVER TRANSPLANTSURGERYA. Osama Gaber, MD, FACSR. Mark Ghobrial, MD, PhD, FACS,
FRCS(Ed)Sherilyn Gordon Burroughs, MD,
FACSConstance Mobley, MDHemangshu Podder, MD, PhDAshish Saharia, MD
PSYCHIATRYInna D’Empaire, MD
PROCUREMENT Hemangshu Podder, MDDewei Ren, MD
ANESTHESIOLOGYMohamad Abdalla, MDAnna Allred, MDNicolas Athanassiou, MDRebecca Bauer, MDSteve Boozalis, MDJessica Brown, MDGhazala Butt, MDJames Carter, MDJane Carter, MDPatrick Giam, MDDiane Gibson, MDAlfred Groen, MDElizabeth Herrera, MDChristopher L. Hutson, MDCraig Ignacio, MDSaras Karri, MDScott Lindberg, MDLingen Lu, MDGary Monteiro, MD
Joseph Naples, MDHany Samir, MDVikram Shenoy, MDKaranbir Singh, MDZbigniew Wojciechowski, MD
BONE MARROW TRANSPLANTMalcolm Brenner, MD, PhDGeorge Carrum, MDHelen Heslop, MDRammurti Kamble, MDRobert Krance, MDPremal Lulla, MDRavi Pingali, MDCarlos Ramos, MD
CRITICAL CAREJohn Fetter, MDFaisal Masud, MD, FCCP, FCCMConstance Mobley, MDTariq Nabil, MDRobert Ochoa, MDIqbal Ratnani, MDKamlesh Thaker, MDDavina Tuazon, MDFaisal Uddin, MDSaleem Zaidi, MDAsma Zainab, MD
ENDOCRINOLOGYDale J. Hamilton, MD, FACe, FACPAbishek Kansara, MDArchana Sadhu, MDSaundra Hendricks, NPEunice Ihaza, NPDena Rose, NPFang Ye, NPJohn Mucha, PA
INFECTIOUS DISEASEDipti Agrawal, MDAshley Drews, MD, FACP
Victor Fainstein, MD, FACPKevin Grimes, MD, MPHRichard Harris, MD
DONOR ADVOCATEElie Saber, MD
INTERVENTIONALRADIOLOGYJett R. Brady, MDMark Brodie, MDJerry Gibbs, MDThomas D. Hedrick, MDJohn S. Labis, MDChenwei Lee, MDDavid W. Light, MDLucho Rossman, MDSteve L. Sax, MDMorris A. Weiner, MDAdrian Wong, MDNam Yu, MD
PATHOLOGY & LABORATORYRoberto Barrios, MDSmaroula Dilioglou, PhDNicholas DiPaolo, MDTodd Eagar, PhDLillian Gaber, MDLuan Truoung, MD
RESEARCHWenhao Chen, MD, PhDDaniel Fraga, MBA, BSMalgorzata Kloc, PhD, DScXian Li, MD, PhDLinda W. Moore, MS, RD, CCRPTadashi Motomura, MD, PhDOmaima Sabek, PhDXiang (Johnny) Xiao, PhDZhiqiang Zhang, PhD
42
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T

houstonmethodist.org/transplant
Houston Methodist J.C. Walter Jr. Transplant Center staff
44
LEA
DIN
G M
ED
ICIN
E: A
DVA
NC
ED O
RG
AN
FAILU
RE M
AN
AG
EMEN
T AN
D TR
AN
SP
LAN
T
From humble beginnings as a 30-bed hospital more than 90 years ago, Houston Methodist Hospital has evolved into one of the nation’s largest private nonprofit hospitals, an academic medical center and a center for visionary medical research.
Our reputation for excellence in patient care and commitment to improving outcomes represent a significant motivation in the development of six multidisciplinary centers of excellence.
• Houston Methodist Cancer Center• Houston Methodist DeBakey Heart & Vascular Center• Houston Methodist J.C. Walter Jr. Transplant Center• Houston Methodist Lynda K. and David M. Underwood Center for
Digestive Disorders• Houston Methodist Neurological Institute• Houston Methodist Orthopedics & Sports Medicine
Primary academic affiliates of Houston Methodist are top-ranked Weill Cornell Medicine and NewYork-Presbyterian Hospital. Houston Methodist also has affiliations with The Texas A&M University System and the University of Houston.
HOUSTON METHODIST HOSPITAL: BUILDING A LEGACY OF INGENUITYTogether, we collaborate to advance clinical medical research and train the next generation of physicians and researchers.
For Houston Methodist clinicians and researchers, leading medicine is a call for excellence in every aspect of patient care. We consistently rank in U.S. News & World Report’s “Best Hospitals” list. The 2015 issue named Houston Methodist among the country’s top hospitals in 11 specialties, No. 1 in the metro area and No. 1 hospital in Texas. Additionally, Houston Methodist unfailingly achieves Magnet distinction for exceptional nursing. Our research ranks in the top 20 for federal funding, and supports early phase clinical trials and FDA-certified manufacturing for research. Because of this commitment to excellence, the finest researchers and clinicians are joining us to accelerate the discovery and delivery of better care and better cures. That’s the difference between practicing medicine and leading it.
MORE THAN 790 clinical studies and trials
$130 MILLION total research portfolio
2015 HOUSTON METHODIST HOSPITAL STATISTICS
12,406 INTERNATIONAL
PATIENT ENCOUNTERS
(from 84 foreign countries)
36,720 INPATIENTS
72,399 EMERGENCY ROOM VISITS
1,479 AFFILIATED PHYSICIANS
603FACULTY
44 GME
PROGRAMS
36 RESIDENCY PROGRAMS
326,534 OUTPATIENT
VISITS
830 OPERATING
BEDS

Our commitment to advancing medicine with global impact
begins in Houston, Texas, where we pioneer a better tomorrow
through research, innovation and breakthroughs to rewrite the
future of health.
THAT’S THE DIFFERENCE BETWEEN PRACTICING MEDICINE AND LEADING IT.
Visit houstonmethodist.org/research to see all the ways we’re leading research.
©2015 Time Inc. FORTUNE and 100 Best Companies to Work For are registered trademarks of Time Inc. and are used under license. FORTUNE and Time Inc. are not affiliated with, and do not endorse products or services of Houston Methodist.
LEADERS IN RESEARCH At Houston Methodist, we are dedicated to defining the future of
medicine. We engineer discoveries in the lab to become clinically
useful products, channel the best innovations through early-stage
clinical trials, and actively transition those innovations to our
industry partners. Our commitment to the full cycle of discovery
and delivery sets us apart as leaders who provide patients from
around the world access to the latest health care advances.

LEADING MEDICINE YESTERDAY, TODAY AND TOMORROWAt Houston Methodist, we have a proud tradition of
revolutionizing medicine. Our past achievements
have built a legacy that spans multiple decades and
disciplines, and that same culture of excellence
inspires us to be the pioneers of tomorrow.
Houston Methodist Hospital
6565 Fannin St., Houston, TX 77030
713.441.5451
houstonmethodist.org/transplant
LEADING MEDICINE ADVANCED ORGAN FAILURE AND TRANSPLANT
2 0 1 4 - 2 0 1 5 Y E A R I N R E V I E W





























