Embed Size (px)
DESCRIPTION
A history of Birmingham Children's Hospital
Citation preview
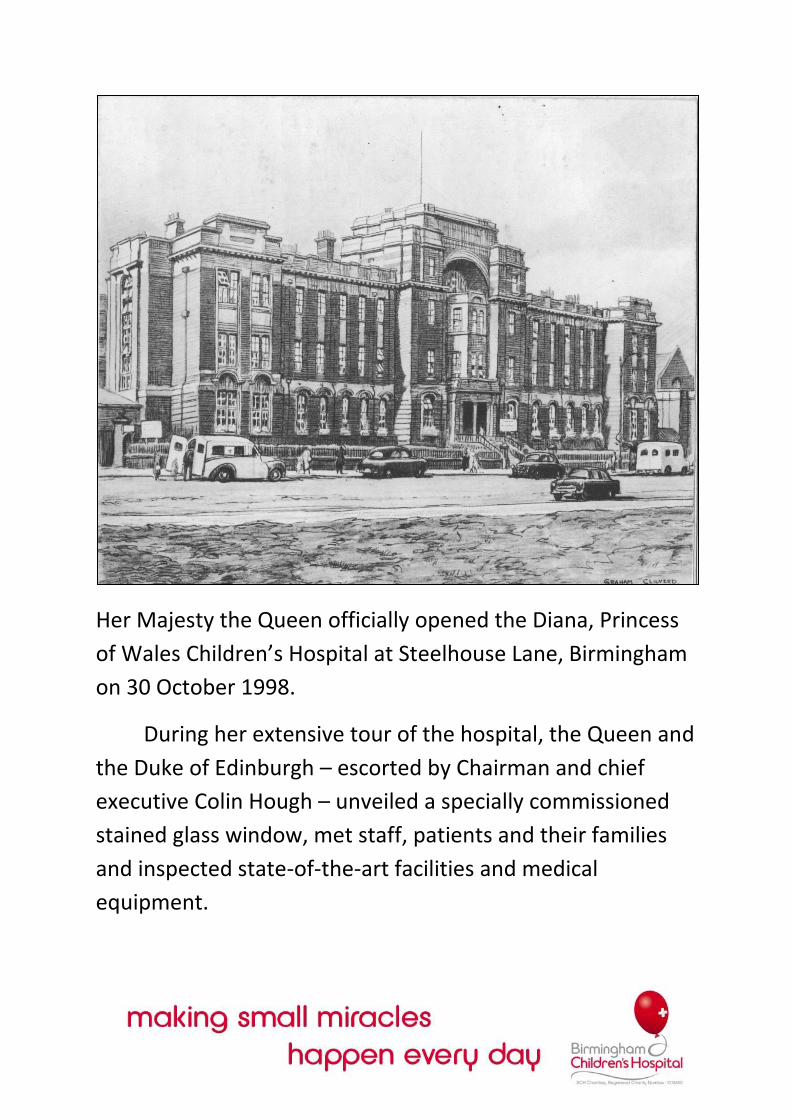
Her Majesty the Queen officially opened the Diana, Princess
of Wales Children’s Hospital at Steelhouse Lane, Birmingham
on 30 October 1998.
During her extensive tour of the hospital, the Queen and
the Duke of Edinburgh – escorted by Chairman and chief
executive Colin Hough – unveiled a specially commissioned
stained glass window, met staff, patients and their families
and inspected state-of-the-art facilities and medical
equipment.
Afterwards, Colin Hough proudly announced that the
visit was a wonderful tribute to the reputation of the Trust
and all those who work so hard to help the many sick
children seen by the hospital each year.
The historic hospital has a new site and a new name, but
is determined to maintain its position as one of the world
leading paediatric centres and a focal point for the local
community.
On 20 May 1998, the West Midlands Ambulance
Services shuttled the final few of a 100 or so young
patients the several miles across town from the old
Children’s Hospital on Ladywood Middleway to the
new Children’s Hospital in Steelhouse Lane.
Just over an hour after the gleaming new Accident
and emergency Department opened, the first
emergency patient was admitted – a six year old boy
who had sprained his fingers while playing. After
decades of hoping and waiting, years of planning and
fundraising and building, the Birmingham Children’s
Hospital had finally arrived in its new city-centre
home.
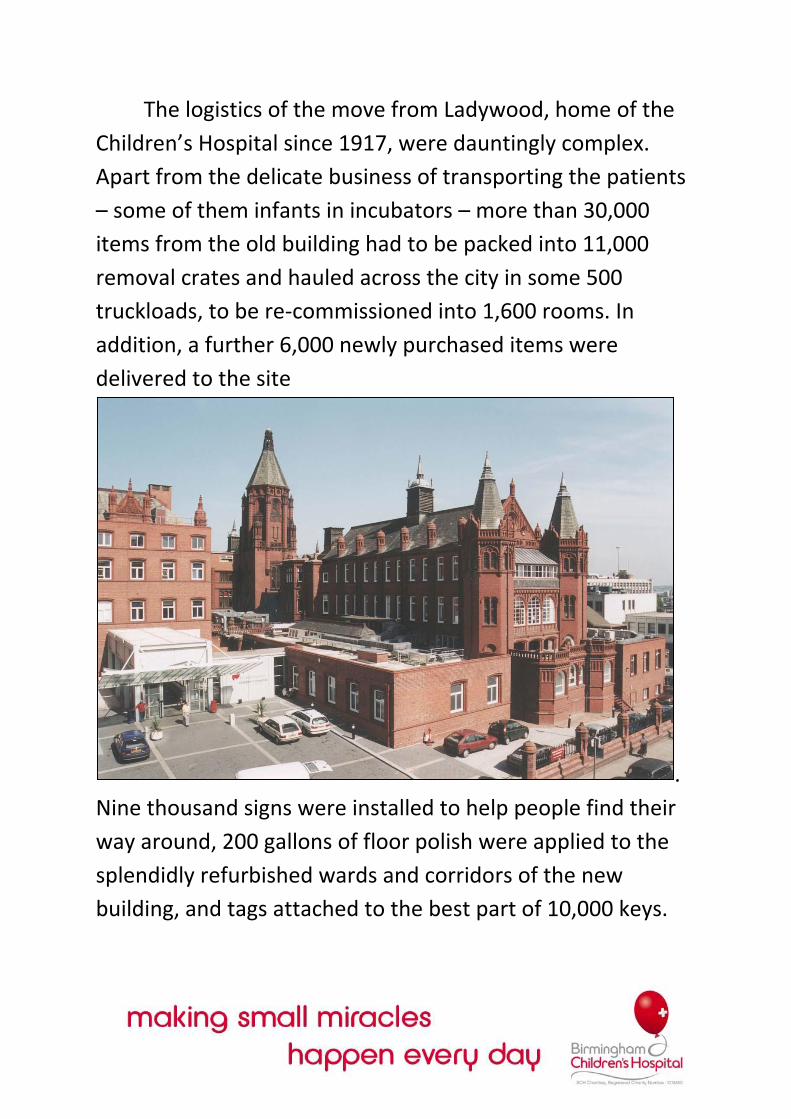
The logistics of the move from Ladywood, home of the
Children’s Hospital since 1917, were dauntingly complex.
Apart from the delicate business of transporting the patients
– some of them infants in incubators – more than 30,000
items from the old building had to be packed into 11,000
removal crates and hauled across the city in some 500
truckloads, to be re-commissioned into 1,600 rooms. In
addition, a further 6,000 newly purchased items were
delivered to the site
.
Nine thousand signs were installed to help people find their
way around, 200 gallons of floor polish were applied to the
splendidly refurbished wards and corridors of the new
building, and tags attached to the best part of 10,000 keys.
As the content of the entire modern hospital were
unpacked and installed, Chief Executive Colin Hough did the
rounds with a trolley, offering cakes and cold drinks.
He says: “I thought my job was to keep their spirits up,
keep them fed, keep them watered. Keep them
supported while this huge move was going on. It’s hard
to think of somewhere else up and down the country
that’s actually done this. There are very few hospitals
that lock, stock and barrel – have uprooted and moved
from one location to another. We ended up with what I
call a party on the park on 22 May where we all
celebrated the move. Everybody was together.
Doctors, nurses, porters, cleaners, managers, all the
clinical support staff. There was a huge sense of
occasion, coming together, celebrating an enormous
task achieved. I think we’ve actually done something
here that is quite special.”

Special is certainly the word to describe the new
premises. The handsome redbrick building in Steelhouse Lane
was originally completed in 1897 to house the Birmingham
General Hospital. Although by the 1990s it had become little
more than an accident centre, for most of the twentieth
century the General has been a much loved Birmingham
landmark. A total of £30 million of NHS cash had been spent
on transforming this Victorian gem, which might have been
knocked down had the Children’s not moved here, into a hi-
tech modern hospital. The aim was to achieve the right blend
between preserving the best of this Grade II Listed building
and creating an uncompromisingly up-to-date facility capable
of improving and developing health services for children well
into the next future.
Within the outer Victorian shell, the big old “Nightingale
wards” were converted into new cubicle wards, with 2-6 bed
bays and some single bed areas. There is room for 300 in-
patients – up from 270 at the old site. Ceilings have been
lowered while brighter colours and patterned floors have
been introduced to make the wads feel more child-friendly.
The original out-patients department has been preserved,
although heavy, brown Victorian tiles have been painted
over. Elsewhere in the hospital, original tiling has been
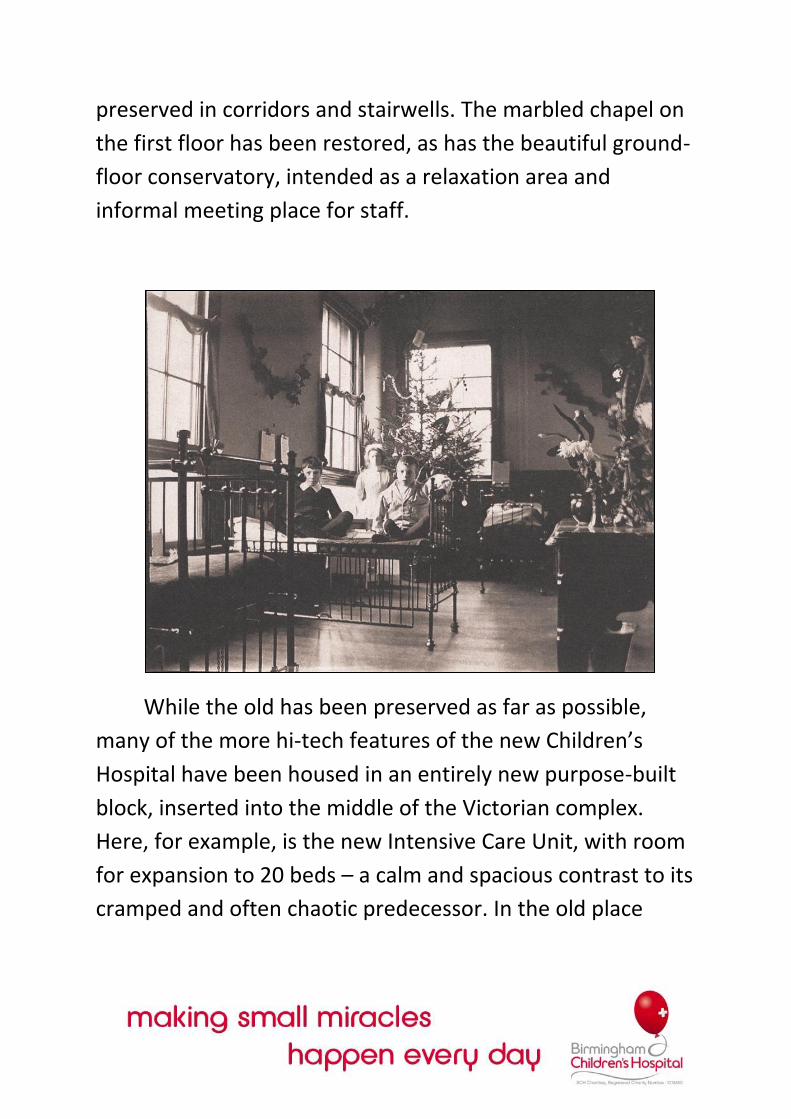
preserved in corridors and stairwells. The marbled chapel on
the first floor has been restored, as has the beautiful ground-
floor conservatory, intended as a relaxation area and
informal meeting place for staff.
While the old has been preserved as far as possible,
many of the more hi-tech features of the new Children’s
Hospital have been housed in an entirely new purpose-built
block, inserted into the middle of the Victorian complex.
Here, for example, is the new Intensive Care Unit, with room
for expansion to 20 beds – a calm and spacious contrast to its
cramped and often chaotic predecessor. In the old place
there were wires everywhere. Here each intensive care bed is
fitted with state-of-the-art monitoring equipment, attached
to specifically designed stands which can be suspended from
ceiling to floor and neatly swivelled around the bed.
The new block also includes four operating theatres,
making a total of seven in the hospital. One is dedicated to
cardiac surgery, allowing the Children’s to further develop its
pioneering work in sophisticated open-heart techniques.
Another operating theatre, which will be used by the
hospital’s neurosurgeons, is kitted out with a £250,000
“Surgiscope” – a device which guides doctors by laser
through the complexities of a human brain. The radiology
department is in the new block too, enhanced with both a
new CT scanner to replace the ten-year-old model that was in
use at Ladywood, and an MRSI scanner, the hospital’s first.
One of the many problems at the old site was the lack of
accommodation for parents. Sometimes mothers and fathers
wishing to comfort their children had to sleep on camp beds
in the narrow spaces between beds. In the new hospital
there is dedicated parent accommodation on the wards, and
a residential house run in conjunction with the Edwards Trust
and capable of catering for up to 35 families. There are also
vastly improved refreshment and waiting areas.
Spaciousness is in every way the key. At Ladywood, just
about anywhere it had been possible to put a new building,
they’d already dropped one in. World-class surgeons were
working out of Portakabins. Where once there had been
expansive gardens, there was just one last piece of grass left,
offering a single bench and a tree. If the move had been
delayed any longer, this final haven would probably also have
disappeared. Now at Steelhouse Lane there are quiet
corners, shady gardens, spaces for colleagues t meet and
greet and keep in touch.
The staff of 2,000 surgeons, doctors and nurses, catering
staff and clerical workers, physiotherapist and lab technicians
– are all proud of this new home. And both the shared
experience of all the move’s complexities, and the room to
stretch out which the new site offers, have fostered a new
sense of community within the hospital, brought them closer
together than ever before.
Says Colin Hough: “We’ve built the platform here on
which we can go on to achieve the opportunities of
being a centre of excellence in terms of clinical care,
research and development, teaching and education –
all those kinds of things that we’re here to do. Now
finally we’ve got the foundation that we need.”
The biggest irony of the move is that, in looking to the
future, it has also brought the Children’s very close to
its past. For it was in the Steelhouse Lane, back in the
mid-nineteenth century, where the story of the
hospital began.
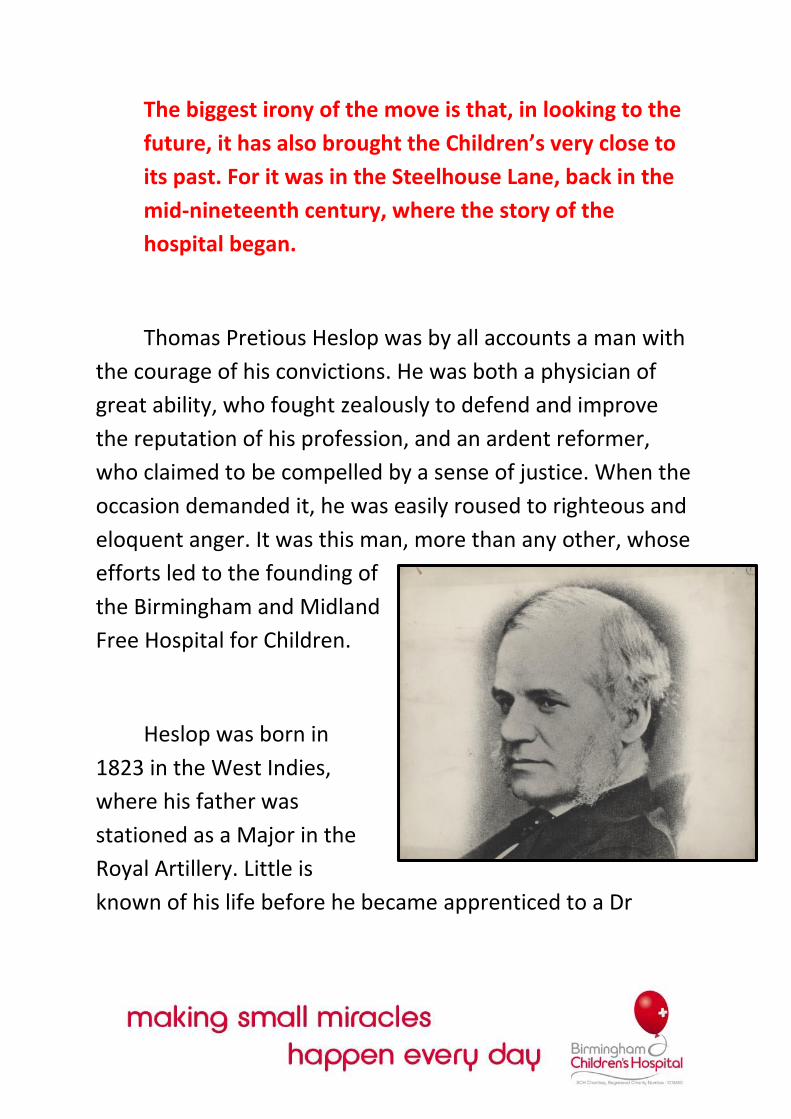
Thomas Pretious Heslop was by all accounts a man with
the courage of his convictions. He was both a physician of
great ability, who fought zealously to defend and improve
the reputation of his profession, and an ardent reformer,
who claimed to be compelled by a sense of justice. When the
occasion demanded it, he was easily roused to righteous and
eloquent anger. It was this man, more than any other, whose
efforts led to the founding of
the Birmingham and Midland
Free Hospital for Children.
Heslop was born in
1823 in the West Indies,
where his father was
stationed as a Major in the
Royal Artillery. Little is
known of his life before he became apprenticed to a Dr
Thomas Underhill of Tipton, Staffordshire, the husband of
Heslop’s aunt. Later he studied in Dublin under a Professor
Stokes, who was both an outstanding physician and a
distinguished man of letters. In Ireland Heslop also gained
invaluable clinical experience, taking on the unpaid post of
clinical clerk at Meath Hospital: “I had exclusively charge of
the whole medical work of the institution, under the
physicians. The gentleman who holds the office obtains
clinical practice for nothing, in consequences of the labours
imposed upon him.”
From Dublin, Heslop moved on to Edinburgh. There he
took his M.D. in 1848, while also leaping at the opportunity
to work briefly in the Royal Edinburgh Infirmary. His courage
and enthusiasm are self-evident. “Three times, owing mainly
to the frightful number of deaths, and because no resident
medical man would go in at a particular moment in 1848, I
had the great good fortune to go in to reside for several
weeks as a substitute.”
Later that year he returned to the Midlands, where he
spent three years as resident medical officer and tutor to the
Birmingham General Hospital. His duties might have daunted
a lesser man. For a salary of £100 a year, Heslop had to
attend to the physicians’ out-patients, do the rounds of the
in-patients, and then write up all their case notes every day.
He also had responsibility for the studies of the three or four
resident pupils This meant not only talking them through
clinical experience and instructing them on medical matters,
but also supervising their reading – scientific tomes as well as
general literature – tutoring them in Latin, French and
German, and making sure they all went to church on Sunday.
Arduous this all might have been, but the post provided great
experience of the workings of a hospital – experience Heslop
would later put to use when setting up the Children’s
Hospital.
He eventually resigned on a matter of principle and set
up in private practice on Temple Row – in those days
Birmingham’s equivalent of Harley Street. But patients failed
to turn up in droves and in 1852 he took an appointment as
Professor of Physiology at Queen’s Hospital. For a while this
offered Heslop scope to develop both his clinical and
educational abilities. But in 1858 he again resigned on a point
of principle. The immediate cause seems to have been the
critism of irregulaties in the wards. What these may have

been has not been recovered, but an earlier letter he wrote
to the Weekly Board perhaps provides some indication.
“On Tuesday last I was informed by Mr John Davis,
now residing in this hospital, that on the evening
previously he had seen a patient of mine, a young girl,
aged 13, labouring under St Vitus Dance, scrubbing the
upper large Female Ward at half past eleven o’clock.
This appeared to be no very uncommon circumstance
and from what I have observed myself I judge that
cleaning or rather wetting the wards in the evening is
very frequent... I entreat the Committee of Council to
call before them the whole body of Nurse, and I will
then aske them if they believe that such persons are
competent to carry out the orders of the Medical
Staffs.”
Heslop was by this time convinced that children could
not be adequately treated in general hospitals. Indeed, they
were rarely admitted to the wards. Without a hospital
appointment, he now found time to think through his
arguments for a children’s hospital and to start shaping his
plans for its foundation. Certainly, reading medical literature
or even just looking around the city in which he lived, he was
aware of the shockingly high level of childhood mortality.
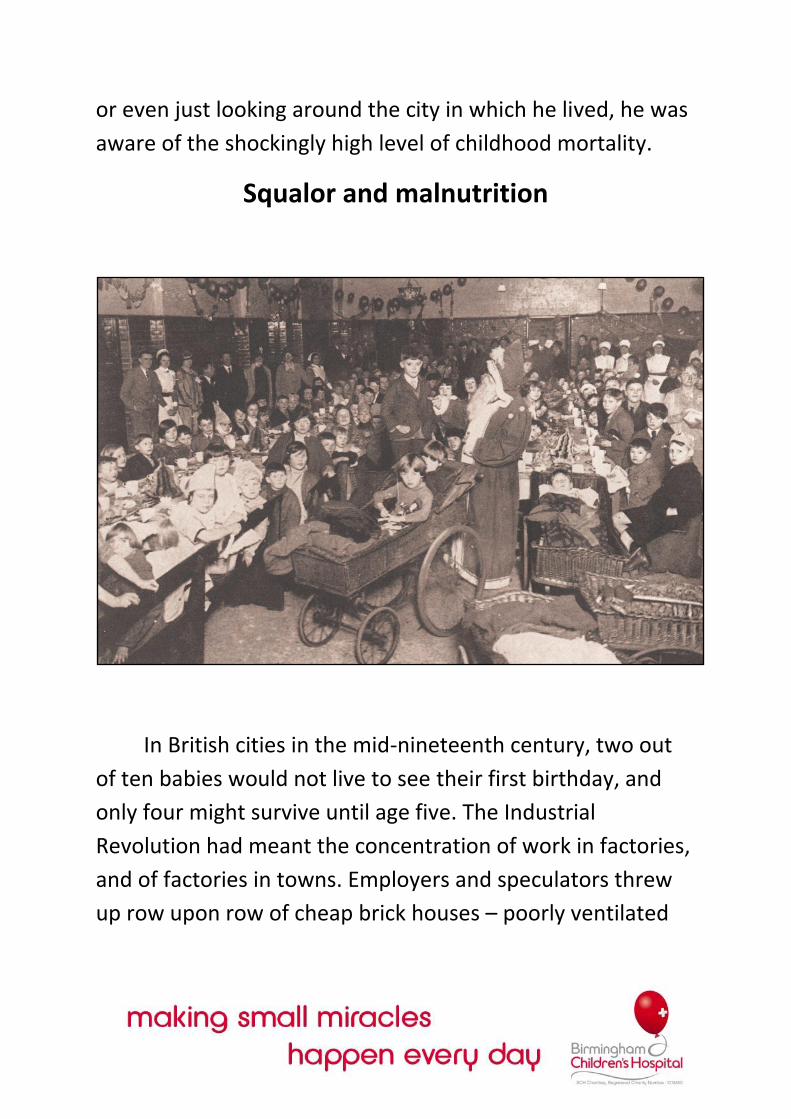
Squalor and malnutrition
In British cities in the mid-nineteenth century, two out
of ten babies would not live to see their first birthday, and
only four might survive until age five. The Industrial
Revolution had meant the concentration of work in factories,
and of factories in towns. Employers and speculators threw
up row upon row of cheap brick houses – poorly ventilated

and cramped – accommodate those who had flocked into the
cities to work. Conditions were appalling: lack of pure water,
outside toilets shared between several families, insufficient
drainage and an overcrowding so severe that some surveys
put average bed occupancy at 2.8 persons per bed. In 1875
the death rate in the centre of Birmingham was 26.82 per
1,000 – fully twice that of leafy Edgebaston nearby.
I have penetrated court behind court, in which the
space between a high wall on one side and the doors of
the houses on the other was so narrow that it would
not permit my umbrella being placed horizontally
between them. In this very place were two cases of
smallpox and one of scarlet fever, and noxious odours
were its prevailing atmosphere. The infant mortality in
such areas is frightful. If we had accurate statistics, the
testimonies of the people themselves would be
sufficient on this point. In one court of five houses I got
such replies as “Buried four, only this one left”; “Buried
six, been married twelve years”; “Buried two”, and so
on ad infinitum.
William White, chairman of the Improvement
Committee, on conditions near the hospital before
slum clearance programmes. (Improvement Scheme,
1875)
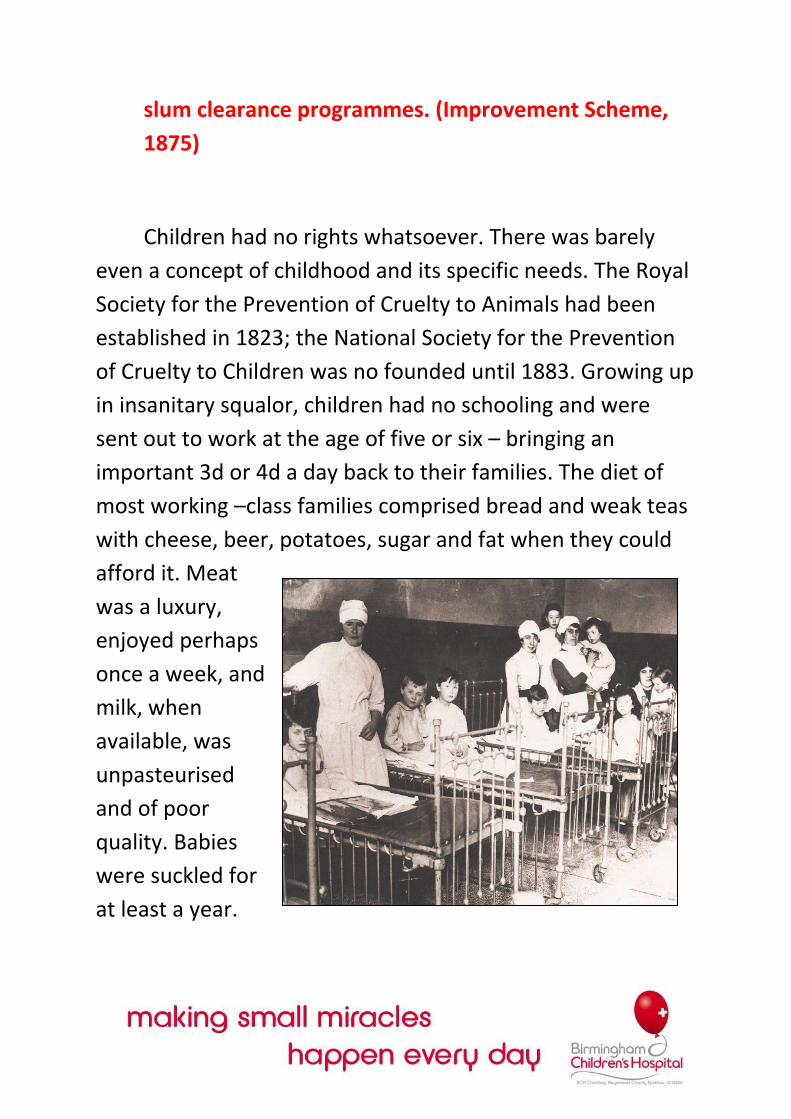
Children had no rights whatsoever. There was barely
even a concept of childhood and its specific needs. The Royal
Society for the Prevention of Cruelty to Animals had been
established in 1823; the National Society for the Prevention
of Cruelty to Children was no founded until 1883. Growing up
in insanitary squalor, children had no schooling and were
sent out to work at the age of five or six – bringing an
important 3d or 4d a day back to their families. The diet of
most working –class families comprised bread and weak teas
with cheese, beer, potatoes, sugar and fat when they could
afford it. Meat
was a luxury,
enjoyed perhaps
once a week, and
milk, when
available, was
unpasteurised
and of poor
quality. Babies
were suckled for
at least a year.
Not only was this cheap and natural, but it was also
commonly believed that a woman could not conceive while
still breast-feeding. Otherwise babies were fed pap-a bread
and water paste flavoured with sugar or treacle. It was
common for mothers to chew the crusts before dropping
them into the bowl.
Under-nourishment and bad feeding inevitably took
their toll, causing many babies to become restless and bad
tempered. Often they succumbed to diarrhoea. Difficult
infants were dosed with patent remedies such as Godfrey’s
Cordial, Atkinson’s Infant Preservative or Street’s Infant
Quietener. These did the job very effectively – mainly
because they all contained opium.
Many babies died from opium poisoning, or one answer:
starved from resultant lack of appetite. Suffocation by over-
laying in a crowded bed was another widespread cause of
infant mortality. The commonest time for this to happen was
on the Sunday morning following a Saturday night of drinking
down the weekly wages in jugs of chip gin.
Working-class children were rarely taken to see a
doctor. A private practitioner was simply too expensive.
Applying to see the parish doctor carried the stigma of
pauperism. There were sick-club doctors, but these were
grossly overworked and seriously underpaid. To the
philanthropic middle-classes, appalled by city-centre squalor
and motivated by both compassion and concern for social
control, there seemed to be one answer: children’s hospitals.
These could supply care in the outpatient department, home
visits, and the temporary removal of the seriously ill child
into a more wholesome environment as an in-patient. In the
age of Florence Nightingale, the training of nurses had also
become attractive. Not only could they tend sick children in
hospital and at home, but they could also play a part in
spreading the right ideas about feeding, clothing, ventilation
and the general care of children.
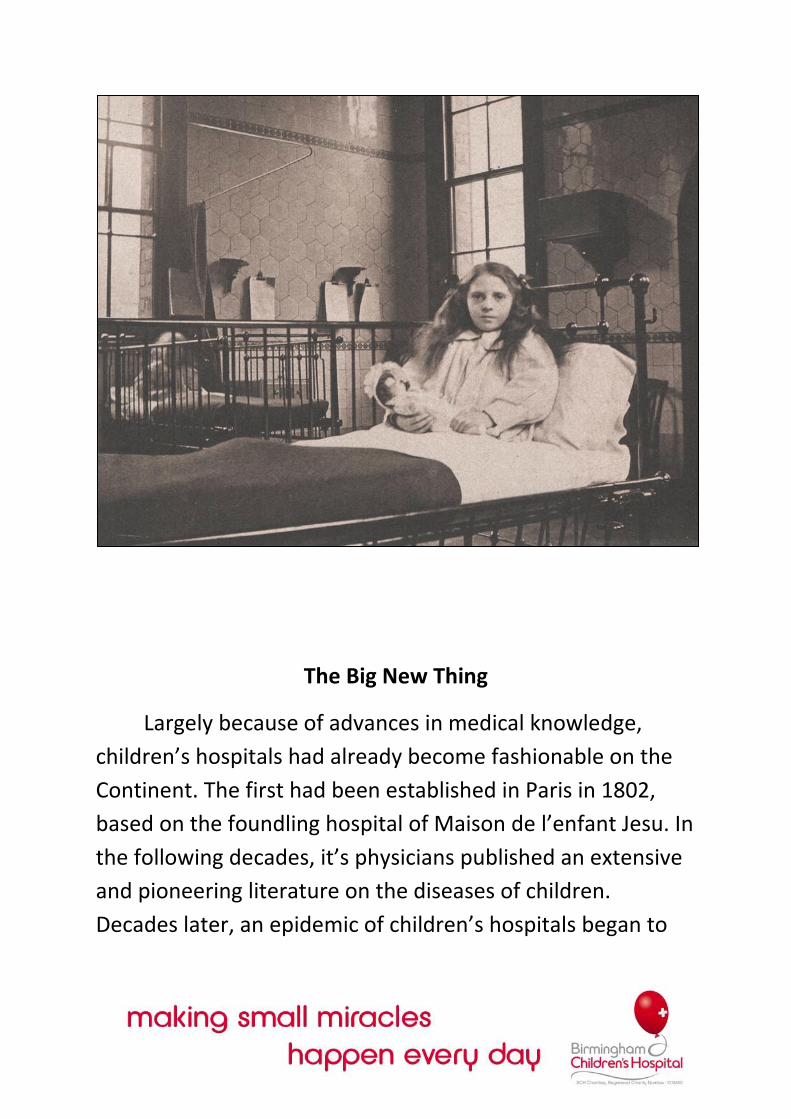
The Big New Thing
Largely because of advances in medical knowledge,
children’s hospitals had already become fashionable on the
Continent. The first had been established in Paris in 1802,
based on the foundling hospital of Maison de l’enfant Jesu. In
the following decades, it’s physicians published an extensive
and pioneering literature on the diseases of children.
Decades later, an epidemic of children’s hospitals began to
spread across Europe: St Petersburg (1834), Vienna (1837),
Pest (1839), Prague (1842), Moscow (1842), Berlin (1843),
Turin (1843), Copenhagen (1845), Munich (1846) and
Stockholm (1854). Many of these had royal of imperial
patronage. Several were integrated with medical schools.
Great Ormond Street Hospital in London, Britain’s first
children’s hospital, was opened in 1851 in the wake of this
international development. Similar children’s hospitals were
shortly founded in Liverpool, Manchester and Edinburgh. It
was only to be expected that Birmingham should soon follow
where these other great cities had led. At a meeting in his
house on 25 June 1861, Thomas Heslop presented his
proposal for a hospital to a carefully chosen group of leading
citizens.
A Town’s Meeting to further discuss the project was
held on 12 July in the Public Office. There was a letter from
the governors of the Queen’s Hospital setting out their view
that no further provision for children was necessary beyond
their hastily cobbled-together plans to open a new children’s
ward. Clearly they were worried about a potential loss of
funds. Criticism came also from S.S. Lloyd, who noted the
Queen’s and General Hospitals habitual state of
indebtedness. Heslop, however, maintained that the new
foundation would not divert monies from existing charities.
“It would be another rill in the stream of charity; persons
would give to this who would give to no other, and
subscribers to existing charities would not withdraw their
subscriptions to give to the new institution.” History would
prove him to be correct.
The Town’s Meeting unanimously passed a resolution “that
it was desirable to establish a Hospital for Sick Children in
Birmingham having for its objects:
1. The medical and surgical treatment of poor children.
2. The attainment and diffusion of knowledge regarding
the diseases of children
3. The training of nurses for children.”
A provisional committee was appointed, charged with the
tasks of finding a building and drafting a constitution. C.E.
Mathews, then a young man of 27, was appointed Honorary
Secretary responsible for much of the project’s
administrative and legal work. A passionate reformer and a
lifelong friend of Joseph Chamberlain, he formed a highly

effective partnership with Heslop and can in many ways be
regarded as the co-founder of the Children’s Hospital.
Mathews set about raising funds, circulating 400 letters of
appeal and publishing the receipts in the “Birmingham Daily
Post” and other papers. Committee members canvassed
friends and acquaintances. By September donations totalled
£685 with a further £134 in subscriptions. Meanwhile,
Thomas Lloyd chaired the Buildings Sub-Committee. Lloyd
was also chairman of the Eye Infirmary and knew that it was
about to move from its premises at 138-139 Steelhouse Lane,
which soon became the favourite out of several possible
sites. The eighteen-century building had previously been a
private house, a bank and a polytechnic. It could be used
immediately without extensive alternations, had a central
location that was convenient for out-patients, could
accommodate 16 in-patient beds, and was “situated amongst
that portion of the population by whom its benefits will be
most readily appreciated”. In other words, the poor.
Not everyone saw it this way, though, as exemplified by a
letter to the Mayor believed to have been written by Queen’s
Hospital Surgeon Sampson Gamgee:

“How can one conceive of a place less fitted for a child’s
infirmary than the one named in Steelhouse Lane, with
its crowded neighbourhood, with Weaman Street and its
thronged garrets and workshops on one side, and that
nest of filth and worse abominations, Slaney Street, on
the other, and last, but very assuredly not least, with the
tannery in its immediate rear?”
Nevertheless, a mortgage on the Steelhouse Lane premises
was taken out, the first medical staff were appointed, and an
appeal was launched for furnishings and equipment. Within
five days the manufacturers and trades people of
Birmingham had contributed everything that was needed.
The list of gits included cots, beds, tables, chairs, inkstands,
hatstands, brooms, mops, crockery, needles, bottles for the
dispensary, clocks, sponges, thermometers, toys, dolls,
instruments, drugs, papier-mâché prescription boards and –
showing that some traditions never change – a bunch of
grapes.
The Out-patients Department was finally ready to open its
door on New Year’s Day, 1862. The In-patient Department
followed a fortnight later. The Birmingham and Midland Free
Hospital for Sick Children had finally become a reality.
A Free Hospital
Then as now, the healthcare of children was at the heart
of the new hospital’s concerns. But Heslop and Mathews had
always intended the Children’s to be something more than
an institution for the treatment of sick youngsters. With a
number of far-sighted reforms, they founded the hospital
also to be both a working model of good management and a

beacon in the struggle against privilege. There can be no
better tribute to their work than to note that so many of
their objectives today seem obvious and commonplace. At
the same they were no such thing.
They separated the business of administration from the
practice of medicine, thus challenging one of the main
obstacles to reform: the domination of hospital policy by
ageing medical men with inflexible views. They also reformed
the process by which honorary surgeons and physicians were
elected. This was to ensure that medical officers were chosen
for their professional qualifications rather than the extent of
their local contacts, or the amount of money they could
splash out on a campaign. One contemporary estimate if the
bill for election to a position at the Birmingham General
Hospital was the then staggering sum of £1,000. Professional
canvassers had been employed to remind subscribers of their
duties. Carts had trundles through the city streets with
placards pleading “Vote for Doctor X” or “Vote for Doctor Y”.
In place of this ridiculous process, Heslop created a Special
Committee of Election that was broad in its composition and
competent to judge medical credentials, while also small
enough to render expensive electioneering unnecessary.
But the most important reforms were in the systems of
admission. In the mid-nineteenth century, general hospitals
were still part of a wide though increasingly outmoded
system of patronage. Wealthy subscribers to local hospitals
expected to receive the right to recommend for admission,
and would pass out ‘tickets’ as favours to servants and
dependants. This might have worked more efficiently –and
for the hospitals at least it was some kind of guarantee that
an applicant was genuinely in need of treatment – but for the
fact that they were also expected to admit accident victims
and emergencies for free, thus upsetting any financial
calculations based on subscribers’ privileges. Meanwhile,
anxious parents of sick children would end up traipsing from
door to door trying to find someone with a ticket to spare.
In London this system was already being challenged –
the Royal Free Hospital had been founded in 1828 – But
Heslop was also influenced by his experiences at the
Edinburgh Infirmary, where the admission of patients
depended only on their need for treatment. Heslop and
Mathews intended the new hospital to be a practical
demonstration of the free principle. The Birmingham and
Midland Free Hospital for Sick Children was the first free
hospital in town. Subscribers were given no tickets of
recommendation to distribute. Instead Heslop sought
safeguards to reassure supporters of the charity that their
money was being properly spent, and on the right people.
The hospital’s constituency was defined as “that class of sick
persons, suffering from whatever serious ailment, who are
above pauperism, and yet below the capacity of paying for a
medical man.” Paupers living on a parochial relief were to be
dealt with by the parish doctor or the workhouse infirmary.
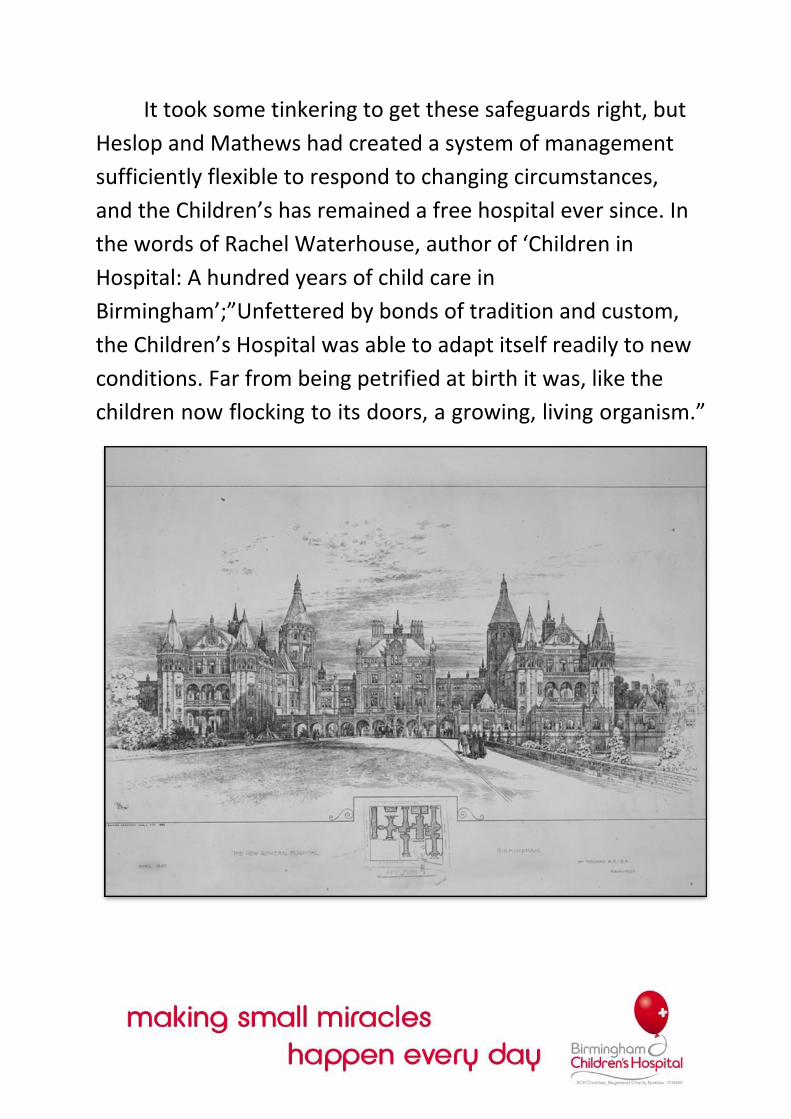
It took some tinkering to get these safeguards right, but
Heslop and Mathews had created a system of management
sufficiently flexible to respond to changing circumstances,
and the Children’s has remained a free hospital ever since. In
the words of Rachel Waterhouse, author of ‘Children in
Hospital: A hundred years of child care in
Birmingham’;”Unfettered by bonds of tradition and custom,
the Children’s Hospital was able to adapt itself readily to new
conditions. Far from being petrified at birth it was, like the
children now flocking to its doors, a growing, living organism.”
Trivial Complaints?
And flock they did, although it had proved usual
wherever a children’s hospital opened that parents would at
first be reluctant to leave their children behind for treatment.
In Birmingham too the number of in-patients built up very
slowly. Just two were admitted in January 1862, followed by
16 in February. There were in any case at the beginning only
16 beds.
It was different with out-patients. Almost from the off,
the waiting room would be filled with mothers and their
ailing offspring, 762 of whom had been seen by the end of
March. The initial system required parents to bring along, not
a subscriber’s ticket, but a certificate of eligibility signed by
two ‘respectable householders’. This quickly proved useless
as people living in the vicinity of Steelhouse Lane were only
too happy to endorse anyone who asked for their signature.
Crowds in the waiting room swelled until the annual onset of
summer diarrhoea caused such out-patient chaos that the
hospital tried limiting the issue of tickets to 30 a day, served
out to the first-comers. The injustice of this soon became
apparent – those who fought their way to the front of the
queue were invariably the strongest, roughest and rudest
and often the least deserving.
In November 1863 a form of means test was introduced.
This proved so successful in managing patient numbers and
preventing ‘abuse of the charity’ that it was to remain in
force for over half a century. The House Surgeon, before
handing out
tickets, would
enquire into the
earnings and
number in a
family, the nature
of the illness, and
whether the
applicant was on
parochial relief.
For a family with three or fewer children, their total earnings
were not to exceed 25 shillings; for those with four or more
children, 30 shillings. The regulations were waived only in
cases of unusual severity, for those requiring delicate surgery,
or anticipating a jet feature of the modern health system –
for those who had brought a certificate from a medical
attendant who had already been treating the case.

This system worked, but still failed to stem the steady
increase in the number of out-patients. “All the gossips of the
neighbourhood were reputed to foregather to exchange
news and to waste the time of medical officers with their
children’s trivial complaints.” Meanwhile, paupers denying
that they were on parish relief still flocked into the Out-
patient Department. With the Children’s limited facilities in
danger of being swamped, Heslop proposed a remedy. A
charge of sixpence, he considered, would exclude paupers
but be affordable for the working poor who were the
intended objects of the charity. With this amendment,
established in 1871, the rules of admission were to remain
the same up until World War 1 and the move to Ladywood.

I write to inform you of an evil which increases every
visiting day, viz: that of the parents and friends of the
children bringing cakes, apples, and other indigestible
foot to the children. Every available means are taken to
prevent it, the housemaid stands at the entrance door,
questions and examines everyone as they enter – a
nurse is continually in each ward and the beds are
searched when the friends leave; not withstanding all
these precautions such things are continually being
given to the children which are not detected until they
show signs of being worse some hours afterwards, this
happens almost every visiting day and although a great
deal is attributable to the excitement of seeing their
parents and friends very much is owing to indigestible
food given surreptitiously.
Dr Underhill, House Medical Surgeon, writing in 1870
A nightmare upon the soul
Though it was considered sociologically beneficial or the
poor to contribute to the cost of their own treatment, all
those sixpences were even then but a drop in the stream of
the hospital’s finances. Like other hospitals at the time, the
Children’s was supported by subscriptions, donations and
legacies. Bigger hospitals employed professional collectors
and canvassers to chase up cash, but most of them lived up
to or beyond the limits of their income. Until the NHS came
along, hospital governors were as preoccupied with raising
money as they were with spending it.
The Children’s was no different, except in offering no
privileges to subscribers, and in the principle of spending no
more money than they had at their disposal at any given time.
The hospital practised careful economies, scrutinising the
prices of equipment, food and drugs and keeping the
prescription of alcohol to a minimum. Legacies were invested
and only the interest was used. Though sensible enough, this
policy also explains the slow growth of the hospital in the last
quarter of the nineteenth century. The only expansion that
took place was financed by appeals.
In 1865 the list of donations to a Children’s Hospital appeal
includes £25 from one Joseph Chamberlain. That same year
he had been elected to the Committee. Just 28 years old and
yet to rise to national prominence, Chamberlain was already
a widower with two young children. He brought to the
hospital his own brand of hard-headed financial ability – that
first appeal successfully raised a sum sufficient to pay off the
remaining mortgage debt on the Steelhouse Lane building. It
also allowed Chamberlain and Mathews to look towards
expanding services for the ever-increasing number of out-
patients.
The Children’s soon acquired a lease on a 585-square-
yard site at the corner of Upper Priory and Steelhouse Lane,
and set about constructing a new Out-patients Department.
John Henry Chamberlain, a devotee of Ruskin, drew up the
plans and eventual building, opened at the Annual General
Meeting of 1869, attracted much praise. George Dawson, a
prominent supporter of the project, was minuted to have
said that:
“Birmingham was filled with architecture which –
especially on a foggy morning – lay like a nightmare
upon the soul, and he was delighted that there was in
this town one committee wise enough to understand
that a little beauty cost a little money but gave great
joy. He congratulated the Children’s Hospital upon
having done something to relieve that sad disease:
deformity, hideousness, misconstruction, rickets and
ugliness in architecture ugliness in architecture."
The new building also showed up the fundamental
inadequacies of the original Steelhouse Lane premises, now
expanded to include 33 beds for in-patients. The lack of an
isolation ward had created great difficulties in handling
patients with infectious diseases such as scarlet fever,
diphtheria or measles. Scarlet fever was particularly
widespread and virulent throughout England and Wales in
the i86os, and many patients admitted to the hospital were
suffering from its after-effects and complications.
Hospital regulations insisted that parents not bring in
any patient suffering from scarlet fever or measles. Instead
they should apply for a home visit. Some patients, however,
were admitted to the wards only to develop one of these
infections later. The rules said they were to be sent home,
often when they were most in need of medical care, proper
food and a sanitary environment. This problem was eased by
Heslop, who had been able to obtain, out of his own pocket,
a seven-year lease on the property next door. In November
1862 he transferred it to the hospital to be used as a
contagious ward. The facility was inadequate, however, and
the lack of isolation beds was a big factor in spurring a move
out of the original premises.
Moving out to Broad Street
In March 1869, the opportunity arose to acquire a
building in Broad Street then occupied by a more-or-less
obsolete Lying-in Hospital.
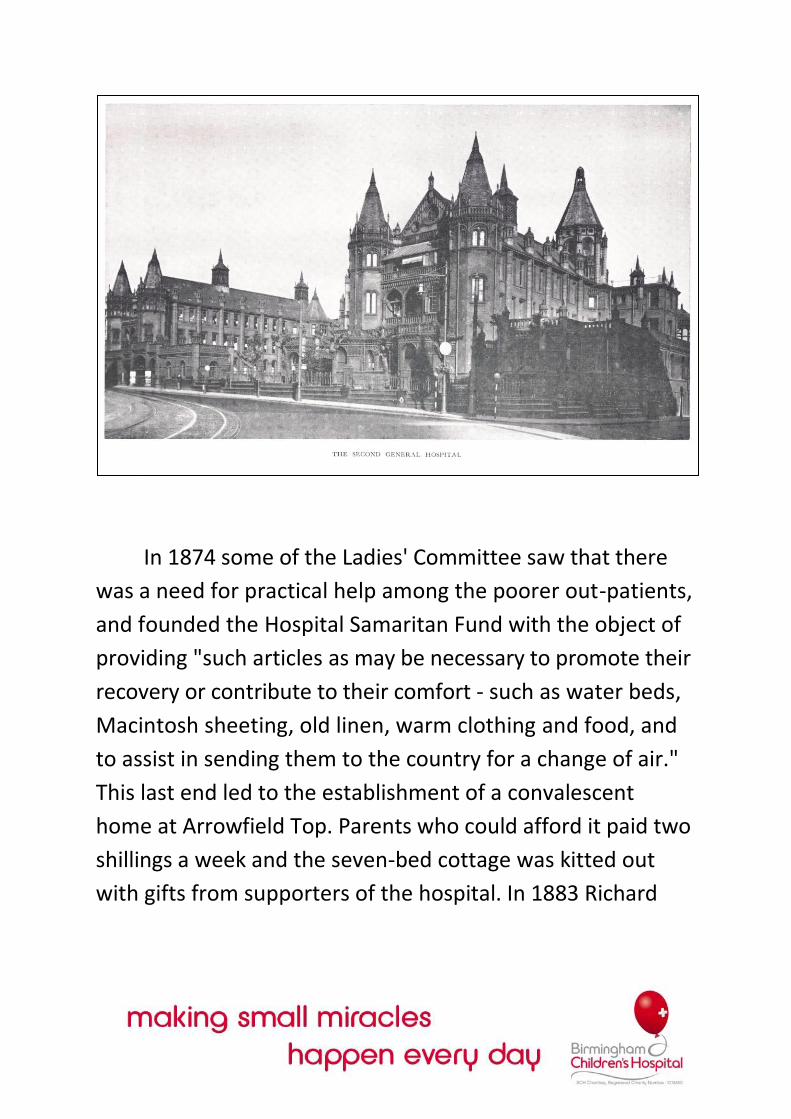
Reports were favourable: the building was
"far enough from the centre of town to secure abundance of
light and air, and near enough to be readily accessible by
patients... It possesses an ample space of ground more than
sufficient to provide an admirable playground for
convalescent children. The central department, built for a
private house, is everything that could be desired for Hospital
administration."
The Committee acquired a 5O-year lease on the Broad
Street buildings. Improvements and alterations were to cost
£248, while Heslop and Mathews personally forked out for a
new set of railings and gates and for laying out the garden
around the building with shrubbery and lawns. Particular care
was taken with the construction of an isolation block, finally
completed in 1877, consisting of two six-bedded scarlet fever
wards, a quarantine ward, and a four-bedded diphtheria
ward. They incorporated every improvement then known to
sanitary science, including glazed tiles for the walls and floors
of closely grained oak. There was separate accommodation
for the nurses and a dedicated laundry.
On the main road into town from Edgbaston, the
Children's was now in a position-both geographically and in
terms of facilities-to impress its existence upon the life of the
city. No longer pushed for space or endeavouring to treat
patients under impossible conditions, the hospital was now
able properly to begin tackling some of its original objectives
and to begin extending its influence beyond Birmingham to
the Midlands, the rest of the UK, and the world at large.
Her babby had to go in. There was no other option. She
had to have the op, the doctors had said so and these
were the doctors that the whole of Brum trusted. The
pair of them reached Five Ways, turned right down
Lady wood Road and crossed over to mount the steps of
the Children's Hospital. Inside, as if in a daze, the
mother instructed her daughter to 'Be good. Do as
you're told. And say your prayers each night'-and then
watched as a kindly nurse led the babby off to the
ward.
No one saw the tears well up in the mom's face and no
one heard her calls to God to mind her child-no one bar
that nurse who turned her head and mouthed: 'Don't
worry. We'll look after her.'
Dr Carl Chinn,from his Yesterday's World column in the
Evening Mail
Raising funds
Heslop and Mathews stood back from the day-to-day
running of the hospital in 1872, but the work of the Children's
continued. As services were developed, the number of
patients continued to rise. The year 1881 saw the total
number of patients treated since the hospital opened reach
250,000. But subscriptions, the hospital's mainstay from the
beginning, were by this time in decline. The year the
isolation wards were built also marked the start of the
depression that ended the great era of Victorian free trade.
In 1878 the Children's registered an annual loss for the first
time, and began to face a recurring cycle of increasing
expenditure, insufficient funding to admit every deserving
patient and the consequent development of waiting lists.
Two innovative funding streams were developed in
Birmingham. The first was the Hospital Sunday Fund, the
inspiration of Dr J.C. Miller, Rector of St Martin's. He
organised a simultaneous collection at all places of worship
in Birmingham to be devoted to local hospital charities.
The Christian world has offered no greater spectacle
than that of our clergy, rhe last two autumns,
forgetting all differences, in the Name of One God,
labouring lor one suffering people. The stern Calvinist
relaxed to do good cheerfully, as with a brother, with
the Romanist, the high Churchman descended, and the
low one rose, to the conviction that charity has no
sect; while the faithful Israelite made the largest
concession, bowing in his temple on the Christian
Sabbath, that his prayers might be one not only in
thought and word but in the very instant of
expression.
Sampson (jamgee, writing as 'Hospital Surgeon'on the
pan-denominational
Hospital Sunday Fund
From 1865, the Children's received a more than useful
lump sum every three years. Its 1868 share was £620, money
that helped establish the new Out-patient Department. In
1870 the £835 provided by the Sunday Fund was a great help
in the costs of moving to Broad Street. By this time, another
fund was being inaugurated: the Hospital Saturday Fund.

Originally based on a simultaneous appeal in the various
working places of the city, it developed into weekly
contributions paid by workers and given over annually to the
Fund. It was a revolutionary step. Until now hospitals had
been financed by the rich. For the first time they were partly
funded by the working classes they were intended to serve.
The share paid over to the Children's grew from £390 in 1873
to a regular £800 a year in the run-up to World War I.
These were funds to benefit all local charities, but the
Children's also developed its own special support. An annual
Sunday Schools collection-like a junior version of the Hospital
Sunday Fund-was the first successful initiative to involve the
children of the city in the well-being of the hospital. From 1880
onwards, it brought in a steady £2OO-£3OO a year. A Private
and Public Schools Hospital Cot Fund was also created -
schools would maintain a cot named after them. The Jewish
Children's League of Kindness also supplied £45 a year to
maintain a cot.
Ridiculously, women were barred from sitting on the
Committee for the first 50 years of the hospital's existence,
but from 1862 a separate Ladies' Committee had been
formed. In a typically Victorian mix of practicality and
sentiment, the duties of lady visitors were "to go through the
whole House; to take notice of its general cleanliness,
regularity and economy; to report in the Visitors' Book any
observations which may suggest themselves after inspection;
and to take some convenient time for conversing with and
contributing to the amusement of the children."
In 1874 some of the Ladies' Committee saw that there
was a need for practical help among the poorer out-patients,
and founded the Hospital Samaritan Fund with the object of
providing "such articles as may be necessary to promote their
recovery or contribute to their comfort - such as water beds,
Macintosh sheeting, old linen, warm clothing and food, and
to assist in sending them to the country for a change of air."
This last end led to the establishment of a convalescent
home at Arrowfield Top. Parents who could afford it paid two
shillings a week and the seven-bed cottage was kitted out
with gifts from supporters of the hospital. In 1883 Richard
and George Tangye presented it with a donkey and carriage.
"This is of the greatest service to us, enabling those who
cannot walk to get out more than they otherwise could, and
fetching from the station the delicate children who arrive. It
is besides a source of unfailing delight to the little patients."
Over 1,300 children passed through Arrowfield Top before in
1890 it was rendered obsolete when Richard Cadbury
presented Moseley Hall for use as a children's convalescent
home, 20 beds of which were reserved for the use of the
Children's Hospital.
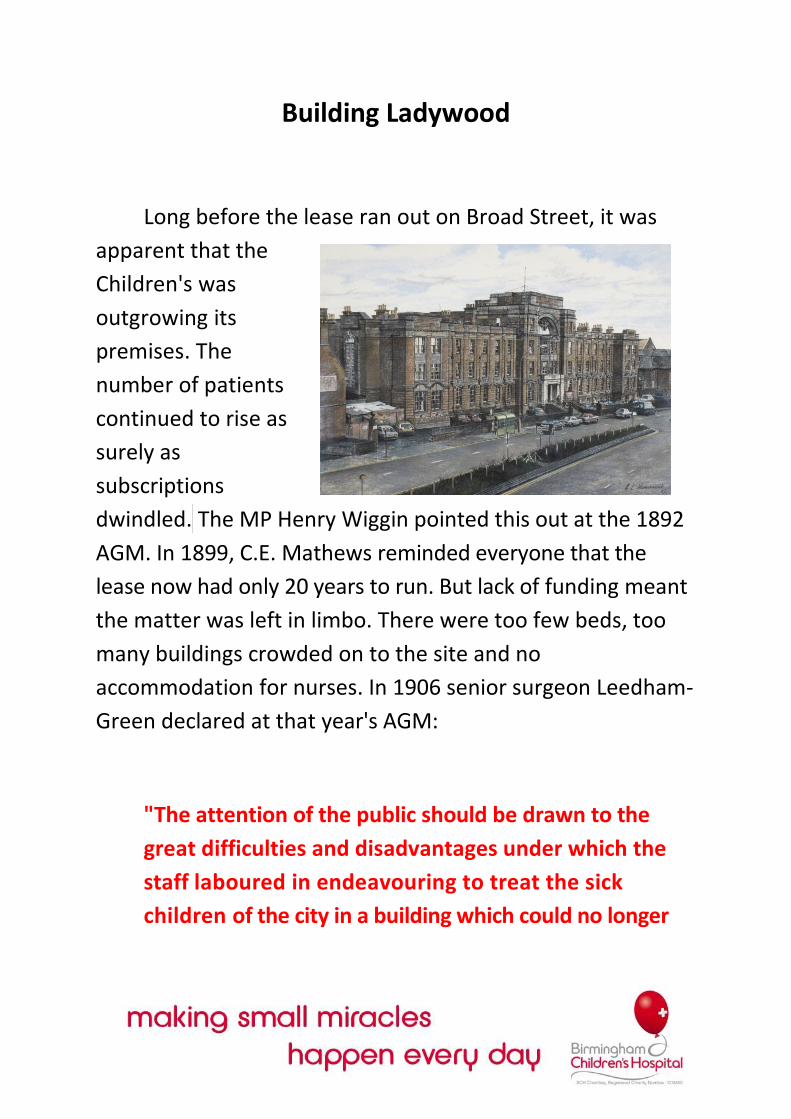
Building Ladywood
Long before the lease ran out on Broad Street, it was
apparent that the
Children's was
outgrowing its
premises. The
number of patients
continued to rise as
surely as
subscriptions
dwindled. The MP Henry Wiggin pointed this out at the 1892
AGM. In 1899, C.E. Mathews reminded everyone that the
lease now had only 20 years to run. But lack of funding meant
the matter was left in limbo. There were too few beds, too
many buildings crowded on to the site and no
accommodation for nurses. In 1906 senior surgeon Leedham-
Green declared at that year's AGM:
"The attention of the public should be drawn to the
great difficulties and disadvantages under which the
staff laboured in endeavouring to treat the sick
children of the city in a building which could no longer
be described as either adequate or suitable for the
purpose."
In 1907 the governors resolved to build a completely
new hospital and a promising two-and-a-half-acre site was
found in Ladywood Road. But the following year an appeal to
raise the necessary £90,000 shook up only £19,904. After the
cost of the freehold this left only £6,500 and the Committee
refused to proceed with so small a sum. The project was
shelved until 1910 when the death of King Edward VII evoked
a wave of patriotic emotion that was channelled into support
for the nation's hospitals. The 'Birmingham Daily Mail'
inaugurated the local memorial fund. After a statue of the late
monarch had been erected in the centre of town, the balance
of the proceeds -just under £30,000-was placed at the
disposal of the Children's Hospital. Extra cash was raised
through bazaars, concerts and other charitable events. On St
George's Day 1913, the foundation stone at the Ladywood site
was laid by Her Royal Highness the Princess Louise, Duchess of
Argyll.
In the same year, Mrs F.E. Player, one of the first two
women appointed to the Committee of Management two
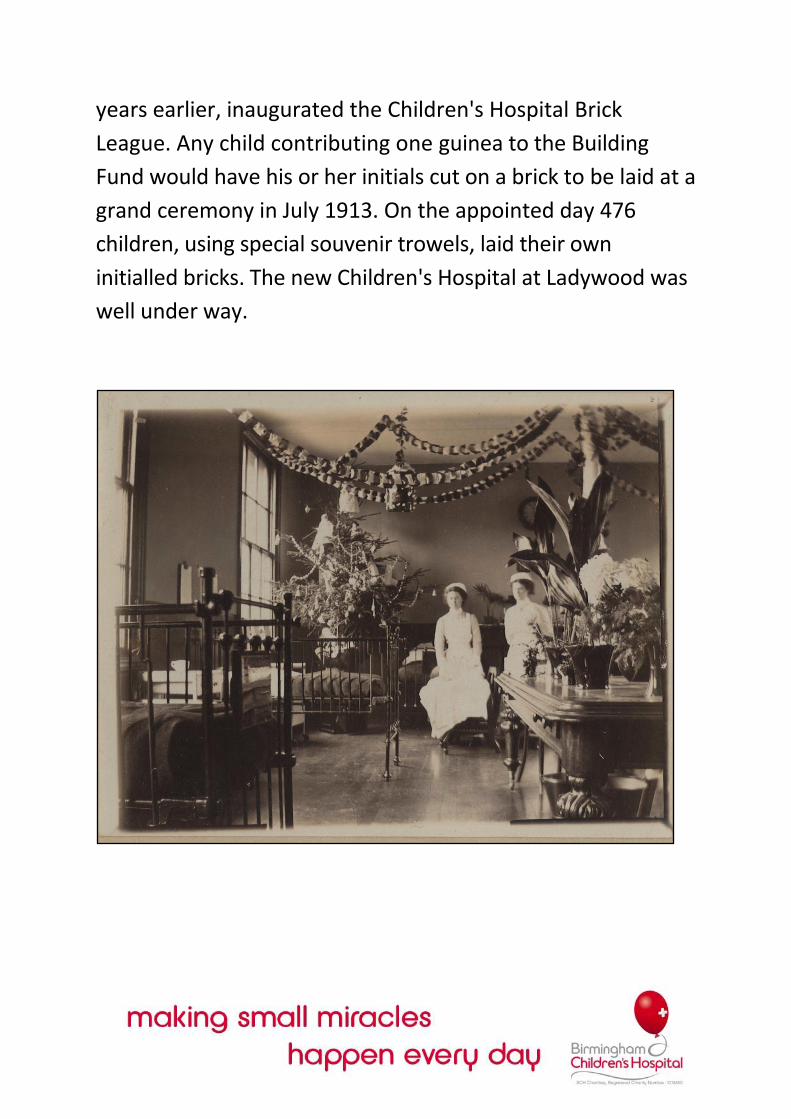
years earlier, inaugurated the Children's Hospital Brick
League. Any child contributing one guinea to the Building
Fund would have his or her initials cut on a brick to be laid at a
grand ceremony in July 1913. On the appointed day 476
children, using special souvenir trowels, laid their own
initialled bricks. The new Children's Hospital at Ladywood was
well under way.
The Paediatric Pioneers
Breakthroughs in medical and scientific research had a
profound effect on the development of the Birmingham
Children’s Hospital during the first half of the twentieth
century. It was to become one of the most forward-looking
institutions of its kind.
Just as Thomas Heslop dominated the story of the
Children's Hospital in its earlier years, so Leonard Parsons was
to prove its guiding light in the first half of the twentieth
century. Born in Aston in 1879, Leonard Gregory Parsons
was educated at the local branch of King Edward's Grammar
School (where Heslop had been Bailiff and chairman of the
School Committee) and then at Mason's College (where
Heslop had been Bailiff and chairman of the Education
Committee). At Mason's, Parsons was highly successful in
zoology and anatomy, qualifying with flying colours and
bagging four prizes-including the Heslop Gold Medal.
Thus was the baton passed from one innovator to the
next. But though both men were gifted physicians and
intimately concerned with child healthcare in Birmingham, it
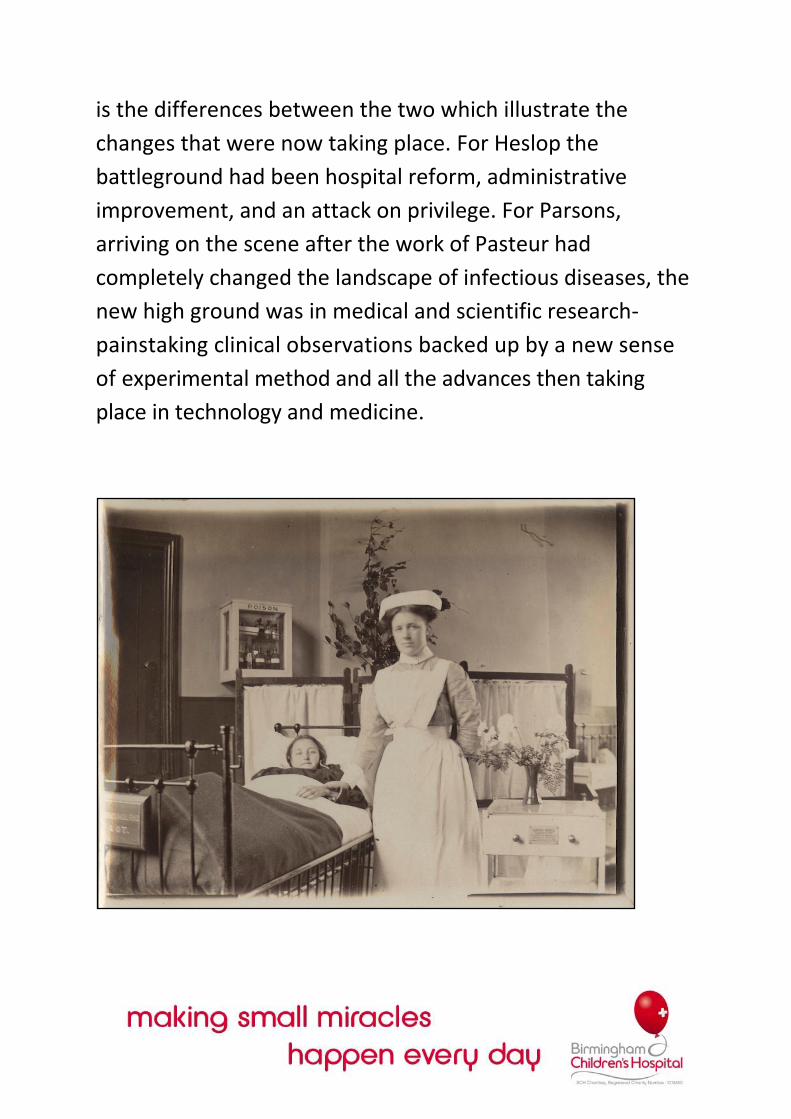
is the differences between the two which illustrate the
changes that were now taking place. For Heslop the
battleground had been hospital reform, administrative
improvement, and an attack on privilege. For Parsons,
arriving on the scene after the work of Pasteur had
completely changed the landscape of infectious diseases, the
new high ground was in medical and scientific research-
painstaking clinical observations backed up by a new sense
of experimental method and all the advances then taking
place in technology and medicine.
After finishing his studies, Parsons worked for some
years in general practice but then took the post of casualty
officer at Great Ormond Street. In 1910 he moved back to
Birmingham to become Physician to Out-patients at the
Children's Hospital. Just five years later he'd already gained
sufficient reputation in paediatrics to be appointed Lecturer
in the Diseases of Childhood at Birmingham University. By
1928, the Medical Faculty had created a personal chair for
him, making Parsons England's first Professor in the Diseases
of Childhood. A gifted teacher who played a leading role in
the establishment of both the British Medical Association and
the British Paediatric Association, he introduced a strong
research philosophy into the hospital and conducted
pioneering work into paediatric problems of his day, such as
anaemia, rickets, scurvy and skeletal disorders.
His first success came at the Children's in 1912 with a
series of lectures he delivered at the Royal College of
Surgeons 'On The Mechanism and Treatment of Shock'. The
work that had led up to this was an object lesson in
teamwork and careful planning-the hallmarks of all Parsons'
later successes. But at the Broad Street site possibilities for
progress were limited and then in 1914 the Great War broke
out. Parsons ended up in faraway Salonika, Officer-in-Charge
of the Medical Division of the Birmingham Territorial
Hospital.
Sunshine and fresh air
World War I had also frustrated plans for the new
building at Ladywood. Not only were labour and materials
hard to come by, but there was also a year-long strike by the
Plumbers' and Heating Engineers' Unions. Meanwhile the
lease on Broad Street was running out fast, so the first
patients finally arrived on Christmas Eve 1917 to take
occupancy of an only partially completed building. There was
little in the way of a formal opening, although the Mayor and
the Bishop both showed up. Two years later, on 21 May 1919,
King George V and Queen Mary visited the new hospital and
toured the wards for an hour.
The wards had been built in a gentle curve facing from
the north-west to the south-east to provide the optimum
amount of sunshine. Each of the eight main wards also had
south-facing windows and balconies with easy access to fresh
air. When the hospital was first opened, they overlooked
pleasant lawns and gardens. Their Majesties, by all accounts,
were most impressed.
Some of these wards, however, remained closed for
several years after the Armistice. The problem was lack of
funds, exacerbated by the increasing costs of equipment and
maintenance, and the need for new laboratories, theatres
and other special departments. Meanwhile, members of the
burgeoning lower middle-class-neither poor enough for the
hospitals nor rich enough for private nursing home—were
being squeezed out of the healthcare equation. The
Children's decided to open one of the wards for fee-paying
patients-in 1921 it cost three guineas a week to cover
maintenance, dressings and medicines, plus a further fee for
the attendant physician or surgeon. This was an important
development. No longer was the Children's solely a
charitable institution. But it was a change that went hand in
hand with completely new conditions in medical treatment.
From the first we had lectures and classes and
wonderfulbedside reaching by .sisters, the Final
Examination took place and they were very
thorough:medical and surgical nursing papers; viva
voce examinations taken by a Physician and Surgeon in
their respective wards at the bedside; and very
practical tests by Matron. After gaining my certificate,
together with a certain nurse also certificated, I started
studying for the examination then held by the
Incorporated Society of Trained Masseuses.
We had to do a great deal of study in off-duty times
and attended lectures at the Queen's and did a great
deal of the practical training there.
I am glad to say that we both passed the examination,
and I was put in charge of the Out-patient Department
at Steelhouse Lane and with d very early type of
apparatus gave the Massage and Electrical Treatment
in the Hospital.
Edith Lockeram, Later a Matron of the Children's,
recalling her training after arriving us a young trainee
nurse in July 1902.
A flame of anger
The end of the war brought back Parsons and other
staff. Full of new ideas and catching the mood of national
optimism, they arrived at the new Children's Hospital with its
state-of-the-art buildings, open-air wards and modern
theatres, and set about transforming it into one of the most
forward-looking institutions of its kind. This meant
introducing new scientific departments and increasing
specialisation.
In 1920 the Children's began setting up an X-Ray
Department. Radiology in those days covered pretty well
anything electrical, so in 1924 it was this department that
established the so-called Sunlight Clinic to administer ultra-
violet rays, a fashionable treatment that reached its peak in
the late 19205. The first Massage and Therapeutical
Department-offering three masseuses, four electrical baths
and lots of Swedish exercises-opened in 1925, expanding into
the space left behind when the Children's finally opened a
new Out-patients Department.
The Department of Bacteriology and Pathology was
opened in 1919. The facility was small, but it enabled the
hospital to meet its own needs in these fields and no longer
have to rely on the University laboratories. The new
biochemistry lab was even smaller, but from 1923 under
Evelyn Hickmans did important clinical and research work,
partly supported by grants from the University and Medical
Research Council. Also during the 19205, the Dental
Department was re-equipped, the Ophthalmic Department
was reorganised, anaesthetics and orthopaedics were
enhanced with extra appointments, and for the first time
the Children's established a department for Ear Nose and
Throat. From 1923 the hospital boasted a Tonsil and Adenoid
Detention Ward.
But despite all the up-to-date facilities, the Children's still had
a long way to go if it was to establish more than a regional
reputation. Ever since the war, the hospital had been engaged
in a friendly rivalry with the Glasgow Children's Hospital.
Later, Parsons wrote of a trip he had made to the USA:
Glass cubicles
Changes in medicine also meant a growing demand for
trained nurses. True to one of the original aims of the
hospital,
the
Children's
set up its
own
Training
School for
Nurses in
1920.
Around the
same time
it became
apparent
that a Nurses' Home would be needed. It took until 1929 for
the Hospital to buy up, one by one, eleven houses in adjacent
Frances Road. These were demolished and in their place
arose a block with no bedrooms, while the remaining space
was used to lay out an attractive oasis of greenery in the
centre of the hospital site.
The other major building project of the period was a
new Babies' Block. Throughout the 19305, the hospital
conducted a prolonged study of childhood anaemias,
involving close co-operation between physicians, biochemists
and pathologists. Apart from all the information that was
published, this research had the result of focusing attention
on younger children and infants. As babies could not be
taken into the main wards for risk of infection, the Babies'
Block was a necessity. The first stone was laid in 1937, but
World War II slowed construction and the block was not
completed until 1941. Soon after it was finally opened, with
66 cots and a system of separating babies in glass cubicles to
prevent cross-infection, it was officially christened The
Leonard Parsons Block.
After decades in which, under his inspiration, the
Children's Hospital had won fame and recognition at home
and abroad, Leonard Parsons retired in 1946. He was knighted
that year and elected to the Fellowship of the Royal Society in
1948, a final tribute to a brilliant career. As H.C. Cameron
wrote in 'The British Paediatric Association 1928-1952': "The
contributions of Parsons to our knowledge of disease in
childhood were, without doubt, the most notable of his
time."
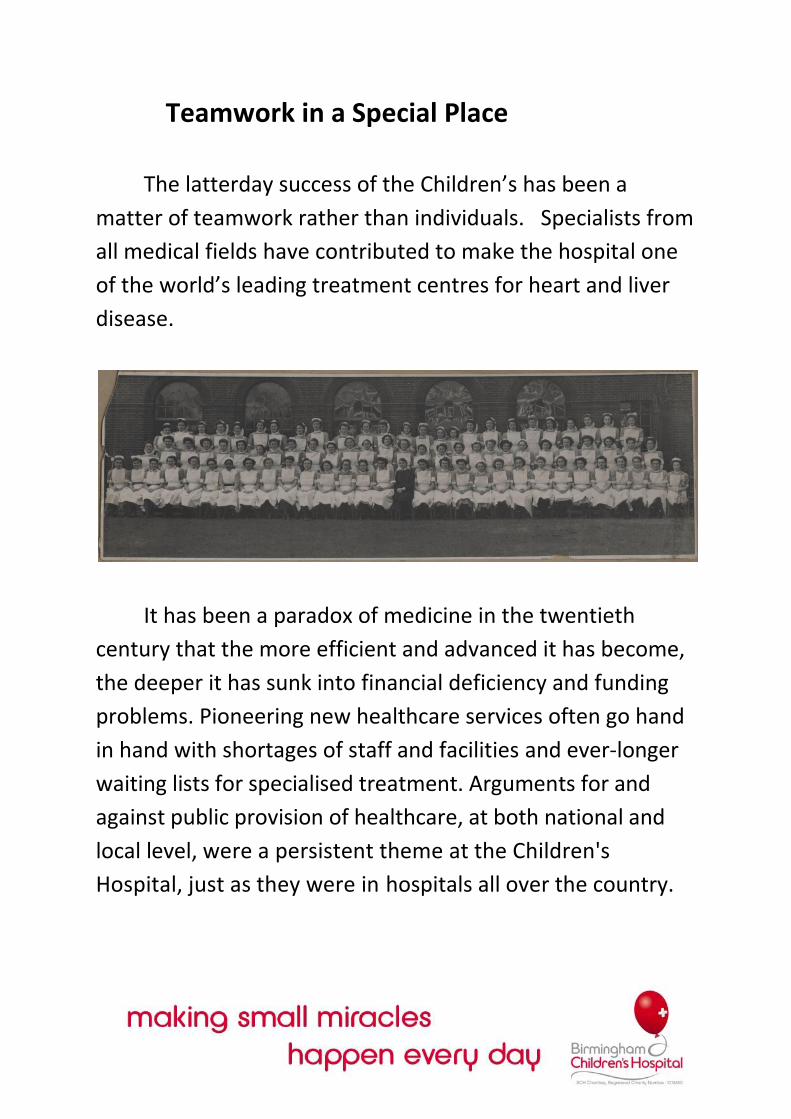
Teamwork in a Special Place
The latterday success of the Children’s has been a
matter of teamwork rather than individuals. Specialists from
all medical fields have contributed to make the hospital one
of the world’s leading treatment centres for heart and liver
disease.
It has been a paradox of medicine in the twentieth
century that the more efficient and advanced it has become,
the deeper it has sunk into financial deficiency and funding
problems. Pioneering new healthcare services often go hand
in hand with shortages of staff and facilities and ever-longer
waiting lists for specialised treatment. Arguments for and
against public provision of healthcare, at both national and
local level, were a persistent theme at the Children's
Hospital, just as they were in hospitals all over the country.
Up until the inception of the NHS, subscriptions,
legacies, appeals and donations continued to fund the
Children's Hospital. From the late 19208, the hospital also
received income from the Birmingham Contributory Fund.
After its initial successes, the Brick League turned its
attention to raising money for the new Out-patient
Department which was opened in 1925. A second brick-laying
ceremony was held on 24 November 1923, attended by over
300 children. In the post-war era the Brick League evolved into
the Children's Hospital League of Friends, and continued
valuable fundraising efforts that equipped Physiotherapy and
Occupational Therapy Departments, furnished
accommodation for the parents of patients, upgraded all the
baby wards, sent nurses on courses and refurbished the
Nurses' Home from time to time.
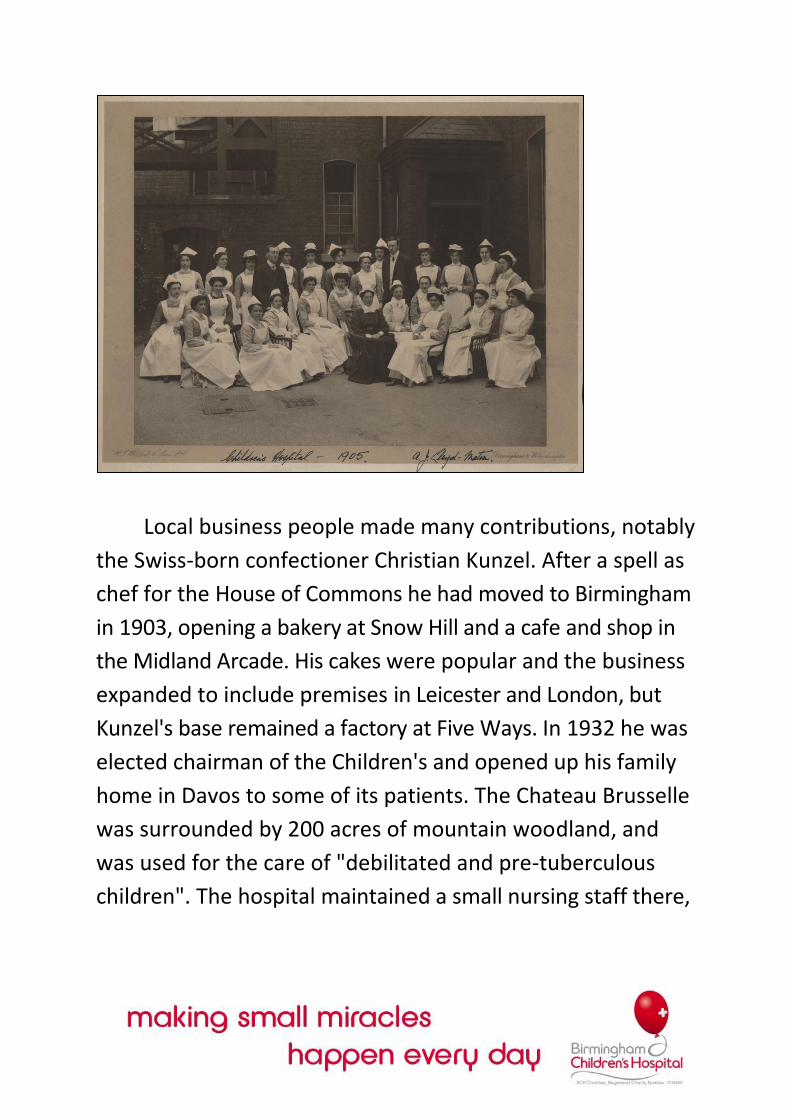
Local business people made many contributions, notably
the Swiss-born confectioner Christian Kunzel. After a spell as
chef for the House of Commons he had moved to Birmingham
in 1903, opening a bakery at Snow Hill and a cafe and shop in
the Midland Arcade. His cakes were popular and the business
expanded to include premises in Leicester and London, but
Kunzel's base remained a factory at Five Ways. In 1932 he was
elected chairman of the Children's and opened up his family
home in Davos to some of its patients. The Chateau Brusselle
was surrounded by 200 acres of mountain woodland, and
was used for the care of "debilitated and pre-tuberculous
children". The hospital maintained a small nursing staff there,

and hundreds of Birmingham children enjoyed some Alpine
fresh air in the years before World War II.
Wartime roots of the NHS
In the early years of World War II, the Children's set
aside two-thirds of its bed capacity at the
behest of the Emergency Medical Service.
These beds were paid for even if
unoccupied, allowing the hospital to
reduce its deficit to almost nothing in
1939. But as casualties proved fewer than
at first anticipated, later in the war some
of these wards opened again. The
Children's also contributed Leonard
Parsons to the war effort-in 1940 he was
made Regional Hospital Officer.
These were the years when the NHS
was being planned and discussed. The
voluntary hospitals were at first jealous of
their independence, but the war years
had also introduced healthcare professionals to a necessary
pooling of skills and resources. In the wartime Emergency
Medical Services were the seeds of a homogenous hospital
system, and it was in any case becoming clear that few
voluntary institutions would survive without state assistance.
When the NHS was finally established in 1948, it was to
Leonard Parsons' credit that the Children's became part of
the Teaching Group of Birmingham United Hospitals. He had
long insisted that paediatrics should be a compulsory subject
in the medical curriculum. By the end of the war this
argument had been won and it was logical that the
Children's, by this time a vital teaching centre for
undergraduates and nurses and with a full-time unit tying it
to the University, should continue and develop its educational
activities along with the other major hospitals of the city. At
the same time, the improvement in salary scales encouraged
more doctors to take up paediatrics and contributed to the
closer integration of child healthcare in its various aspects.
Bringing professionals together
Parsons' other great legacy was the Institute of Child
Health, established as a department of the University of
Birmingham. From the' earliest days of the hospital there had
been personal links with the local authority. Later Parsons
was involved with some of the city's child welfare clinics. The
point of the ICH was to formalise direct cooperation between
the Children's Hospital, the University and the city's Child
Welfare and School Medical Services. This would provide a
forum for discussion, collaborative research, and both
undergraduate and postgraduate education. Parsons had
been thinking about this all through the 19308, and in 1945 it
finally became a reality

By connecting the hospital with public welfare clinics
the ICH finally brought together the preventative and
curative aspects of paediatrics. Registrars from the Children's
went to the welfare clinics, and staff from the Child Welfare
Service came to the hospital. Arrangements were made for
students to study the clinical aspects of the Health
Department, visit child welfare and antenatal clinics, learn
about the School Medical Services, and receive some training
in midwifery and home nursing. It was also a centre for
postgraduates specialising in paediatrics, for GPs on refresher
courses, and for public authority medical officers concerned
with child welfare.
The ICH had no home of its own until 1961, when the
Nuffield Provincial Hospitals Trust provided £40,000 to
complete a two-storey building fronting Francis Road and
with direct access to the hospital at the rear. This contained
offices, conference rooms, a library and laboratories. Under
the guidance and inspiration of Sir Douglas Hubble the ICH
proved an effective catalyst for research and collaboration
and nurtured many of the new clinical services for which the
Children's was to become well-known: clinical genetics,
nephrology, nutritional disorders, neurology and neurological
handicap, haematology and oncology.
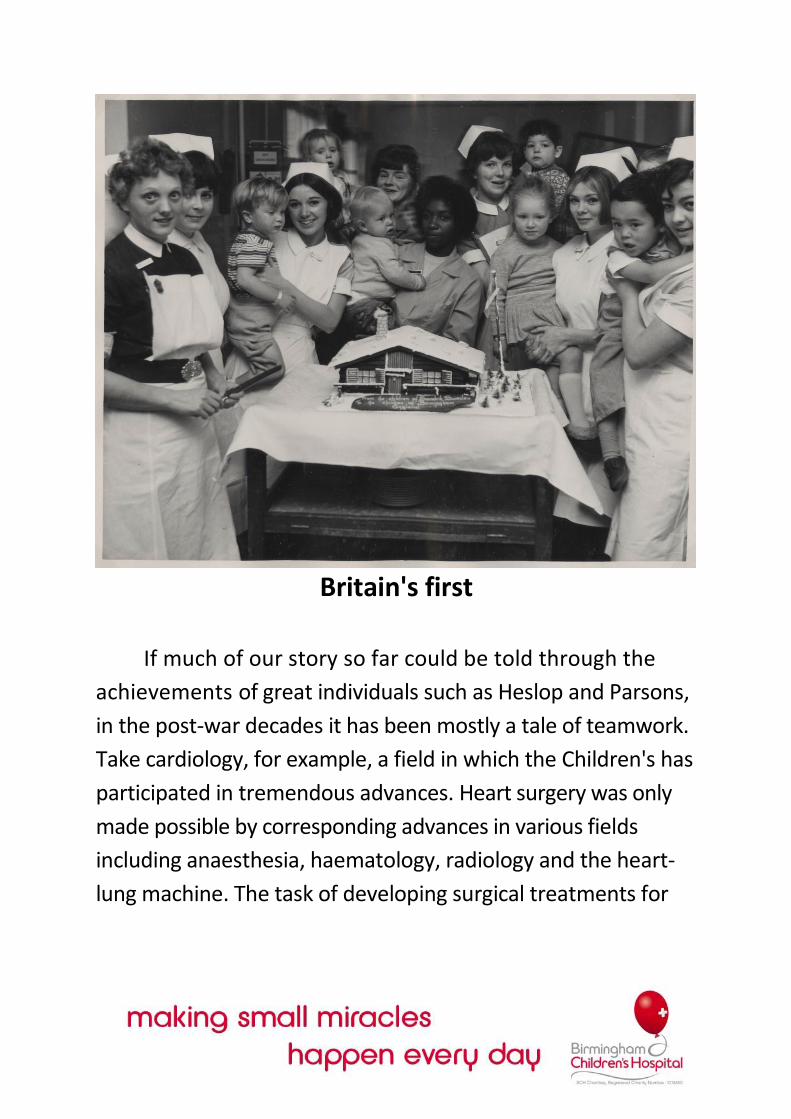
Britain's first
If much of our story so far could be told through the
achievements of great individuals such as Heslop and Parsons,
in the post-war decades it has been mostly a tale of teamwork.
Take cardiology, for example, a field in which the Children's has
participated in tremendous advances. Heart surgery was only
made possible by corresponding advances in various fields
including anaesthesia, haematology, radiology and the heart-
lung machine. The task of developing surgical treatments for
congenital heart diseases therefore exemplifies the close
interdependence between the various branches of medical
knowledge which are represented at the hospital.
It was at the Children's in 1951 that Leon D'Abreu
performed Britain's first successful hole-in-the-heart
operation. These days holes in the heart can be repaired
without open-heart surgery, using a technique known as
cardiac catheterisation. In 1995 the Children's became Britain's
first hospital to use this technique, in which a tube is inserted
through the groin and manipulated through blood vessels into
the heart. The hole in the heart is thus plugged with a device
made from a metal invented for American submarines. Cardiac
catheterisation is also useful in treating cases of abnormal
heart rhythm, a condition which can now be treated as a day
case.
The Heart Unit at the Children's-one of the largest in
Europe, performing over 400 serious operations every year-
takes referrals from all over the UK and abroad. This is partly
the result of its specialist expertise in hypoplastic left heart
syndrome, a rare condition in which only half of the heart is
properly formed, causing babies to die from low blood
pressure and Jack of oxygen. The pioneering operation, with
which the Children's has the highest success rate in Europe,
involves the
complete
reorganisati
on of a
series of
arteries
connecting
the heart
and lungs.
The aim of the Heart Unit is to mend hearts as early as
possible -preferably within the first year of life. The sooner
conditions are identified the better and to this end the Unit
has developed an ultrasound ante-natal diagnosis service,
which can pick up signs of certain congenital heart diseases
while a baby is still in the mother's womb. Clearly, heart surgery
involves a big team effort: medical and surgical consultants,
laboratory services, dietitians, the Intensive Care Unit and
nurses all play an important part. The Children's also has a
Cardiac Liaison Service which acts as the interface between the
hospital, wider community services, the parents and patients,
making sure that their needs are met and that they get the
right support.

Teamwork is also the key in the Liver Unit, another area
in which the special expertise of the Children's draws
patients from beyond the region. In this field too there has
been pioneering surgery. The first British operation to give a
child a cut-down liver, in which a portion of an adult liver is
transplanted, was performed in Birmingham in 1989. Since
then the Liver Unit has pioneered 'split-liver' operations, in
which a chronic shortage of donors is ameliorated by dividing
livers between transplant patients. In 1993 the Unit
performed Europe's first combined liver and bowel transplant
operation and in 1998 Britain's first triple-transplant of small
bowel, liver and pancreas.
The team responsible for this extraordinary work
includes not just doctors and surgeons, nursing staff and
intensive care personnel but also dietitians, social workers,
psychologists and physiotherapists. The Liver Unit is
committed to family-centred care and a holistic approach in
which the child's entire needs are taken into account, thus
involving teamwork right across the hospital. This aspect of
care has even been the subject of considerable research, with
a major investigation into the quality of life for children and
families following transplantation.
Teamwork, collaboration, multi-disciplinary care and a
holistic approach are also a feature of the oncology
department, one of the largest such units in Europe. Twenty
years ago, there was little hope for victims of the commonest
children's cancers-leukaemias, brain tumours and other "rare
tumours of childhood". But now the Children's achieves cure
rates of 60-70 per cent from acute lymphoblastic leukaemia
(formerly less than i per cent); 85-90 per cent from Wilm's
Tumour (cancer of the kidney); and 80-90 per cent from
Hodgkin's Disease. The dramatic improvement in the odds is
due to better management of chemotherapy and surgical
techniques, as well as new screening methods to detect
childhood cancers as early as possible.
“We've loved you, we've hated you"
These achievements are all the more
extraordinary given deteriorating conditions at
Ladywood. The oncology unit was operating out of
a Portakabin in the hospital grounds. Patients were
camping out on chairs and makeshift beds in the
narrow corridors of overcrowded Ward 6.
The increasing costs and complexity of modern
medicine (in 1961, to give one stark example, the
hospital performed
9,785 biochemical
tests; by 1996 that
annual figure had
mushroomed to
272,084) and its
demands for more
and more personnel,
were creating a
similarly intolerable
situation in most of
the hospital's
departments. Demands for a new hospital had begun
way back in 1957, when it was decided that a
sanatorium-type hospital was no longer suitable for
the complex medical services of the late-twentieth
century. In the subsequent decades, plan after plan
was mooted and shelved as conditions at Ladywood
deteriorated.
Small amounts of cash, much of it raised by dedicated
volunteers and often with celebrity aid, helped to allay the
dilapidation. One problem was that the site had become an
essentially unconnected collection of buildings. In 1986 a
special appeal, helped by a Paul McCartney concert, funded
'The Covered Way'-a plastic corridor that saved patients
from being pushed out into the snow and rain to get from one
place to another. But every time it rained, the water would
collect underneath. In the course of their daily duties,
hospital staff had to paddle through a small river. Despite its
worldwide reputation for excellence, the Children's had
become very run down.
Even so, the work of the hospital had always inspired a
certain affection. When the staff finally left for Steelhouse
Lane - some of them after waiting 40 years for the move -
many left behind graffiti on the walls:
"Thank you for sharing your final moments with us -
this was a special place!"; "For all those babbies we've
looked after, the memories will linger forever"; "We've
loved you, we've hated you, but we'll never forget you."
Our New Home
Birmingham Children’s Hospital, Birmingham is hi-tech,
comfortable and friendly; the sort of place that staff can bring
their colleagues from all over the world and feel proud to
show them around.
"As the principal provider of children's services in
Britain's second city and the only centre for specialist
children's care in England's largest health region,

Birmingham Children's Hospital NHS Trust has a vision
for its future role-locally, nationally and
internationally," says Dr Mike Stevens, Medical
Director. "It sees its place not only in providing
excellence in care, but also in teaching and research.
Such a position offers a mandate for wider advocacy
of the health of children and the Trust intends to
develop its relationships with other agencies in
education and social services, in public health and the
research community. Leadership in local strategies for
children's health care; the development of a new
national children's clinical trials unit; and links with
children's hospitals overseas are all examples of the
way this vision is being implemented. The future is as
exciting as the past and Birmingham Children's Hospital
NHS Trust plans to lead the way."
"What we've got here" says Colin Hough, sitting in his
new office in Steelhouse Lane, "is a modern classic
which provides the necessary accommodation to
deliver the highest quality patient care. Outside it's a
lovely old building, but inside it's modern and hi-tech
as if it was built today."

No longer do world-class physicians and surgeons work
out of rickety Portakabins, or traipse along waterlogged
corridors. Quite the reverse. Now they have a facility they
can be proud of. "It's a different world," says Hough. "This
is the sort of place where staff can bring their colleagues
from all over the world and feel proud to show them
around."
There is not an area of the hospital's work that has not
been greatly enhanced by the move. The several dozen
departments now have decent office space, modern
facilities, room to work and breathe. There is space for
children to play, for parents to stay. Space for staff to meet
and mingle and keep in touch with each other's work.
Whereas at Ladywood, the buildings were only
connected by the leaky plastic "Covered Way", the Children's
new home is run through by a proper corridor. "It probably
sounds like a daft thing to say," shrugs Hough, "but
corridors are the lifeblood of a hospital. They're places
where people meet, have a chat. Here you can get from
anywhere to anywhere and it's all under cover. It's all in a
modern, clean, heated, lit sort of area. We shouldn't be
saying things like this in the iggos, really, but that's where
we've just moved from."
Individualised care will be planned and negotiated
with the child and family. They will be supported to participate in all aspects of care, as they feel able.
In each case setting the child and family will be introduced to a named person who will be responsible for planning and coordinating their care, respecting and valuing the contribution of the healthcare team.
Care will be provided within a safe and friendly child-centred environment.
Each child and family will be listened to, their wishes and feelings acknowledged and their right to privacy, dignity and worth respected.
To enable participation in decision-making, the child will have access to information through education and play, relevant to their age and understanding.
The cultural, spiritual and religious needs of the child and family will be met in a sensitive and respectful manner.
Play and education will be part of each child's planned care.
Birmingham Children's Hospital's Philosophy of care for
the Child and Family, 1998
Integrated care
The move to Steelhouse Lane has been not only a physical
shift, but also a move in mind-set. The new city-centre
location in a much-
loved old building is
important in
emphasising the
Children's role and
history in the
community. Unlike the
better-known Great
Ormond Street, which
takes only specialist
referrals, the Diana
Princess of Wales
Children's Hospital is
very much part of the
life of the city where it
operates, and in the future is aiming to become more so. As
an NHS Trust, says Hough, the Children's "is committed to
providing truly integrated care and we are putting a renewed
emphasis on working in partnership with other Trusts,
primary care groups, statutory and voluntary agencies and, of
course, the children and the carers."
A number of innovative schemes are being set up in
conjunction with the Departments of Education and Social
Services in Birmingham. These are intended to give the
children and young people of Birmingham an opportunity to
have a say in the strategic direction of the hospital,
particularly in the areas of research and development. Efforts
will be made to further improve the quality of life for
children at the hospital, and to minimise the duration of in-
patient stay.
Ongoing community-based schemes and initiatives
include speech and language therapy, audiology, eye
screening, occupational therapy, social work, respite care,
community and schools nursing, interpreting services, child
and family care, diabetes home care and psychotherapy.
Child health in the community is also one of the central
themes of the extensive research going on at the Children's.
New facilities allow this research to be better coordinated
than it ever was before. Given the importance of cooperation
between the Children's Hospital Research & Development
Directorate and the Institute of Child Health, perhaps the only
drawback of the move has been a greater distance from the
University campus. New communications media and
sophisticated data links have compensated for this, however,
and the Children's is developing both an extensive website
tapping into skills around the Trust, and an intranet to enable
front-line staff to access national and international data about
conditions and treatments. The hospital's Education
Department is also working on and, through its school and
expanded play centre, testing computer programmes that
will help children learn about their own diseases.
Hope for the next century
All hospital staff are involved in ongoing training
schemes, aimed at maintaining and improving the quality of
healthcare for children. These initiatives are multi-disciplinary
in scope, and will increasingly involve the various universities
surrounding the hospital. In addition, a patient and family
health centre has been established specifically to cater for the

needs of the wider ethnic community in the Birmingham and
West Midlands area.
Other areas for future research include clinical trials and
work on diseases that affect specific organs and systems. Over
the next half-century significant developments can be
expected in transplantation, neurosurgery and cardiac
surgery. But Ian Booth, the current Leonard Parsons Professor
of Child Health, stresses that the vision for paediatrics is also
one of increased care in the community, and of treating the
child as a whole person, rather than merely as a disease. "I
think we can say," smiles Ian Booth, "that the research future
is extremely bright."
Ever since the Children's first opened in 1862, it has been
an innovator. The infectious diseases that were originally one
of its main concerns-scarlet fever, typhoid, whooping cough,
polio, cholera, summer diarrhoea, smallpox, measles-have all
now been eradicated or are under control. Now, in the age of
high-tech medicine and intricate treatments, the hospital is
equipped to look ahead and meet the challenges of the
future.
"We're looking forward," says Colin Hough, "to
designing services which will deliver consistently high
standards in the full range of hospital and community
child health services."
As a hospital, and as a centre for education, research and
community services, the Birmingham Children's Hospital NHS
Trust is now equipped to offer hope for the next century, not
just for the people of Birmingham, but for children all over
the world.