Embed Size (px)
Citation preview
Immunisation policy
Dr Rosemary LesterAsst Director, Health ProtectionCommunicable Disease Prevention and Control Unit & Deputy Chief Health OfficerDepartment of Health
Immunisation Policy
National Immunisation Program
–Program of vaccines delivered at no cost to the population
–Extends from birth to old age
–Collaborative agreement between Cwlth and states/territories
Role of NHMRC
–Publish recommended immunisation schedule and handbook (on advice from Australian Technical Advisory Group on Immunisation (ATAGI))
–changes according to new vaccines, new combinations, changing epidemiology of disease, cost effectiveness assessment
Immunisation Policy
Role of ATAGI
Determine whether vaccine is suitable for NIP, PBS etc based
on efficacy, epidemiology of disease, whether population based immunisation will lead to additional positive outcomes for the community, eg herd immunity effect
Write handbook for endorsement by NHMRC
Role of PBAC
Take ATAGI recommendation and perform cost-benefit analysis
Make recommendation to Australian government as to whether fits cost-benefit criteria for NIP or PBS.
Immunisation Policy
National Immunisation Committee
Australian Government
States and Territories
Local government
RACGP
ADGP
Role is to implement the NIP
Australian Government
Policy development
central co-ordination and secretariat services to NIC
encourage research
report to the Health Minister and AHMAC
Funding
Vaccines
Some service delivery
Part ACIR notification payment
Parent and GP incentive payments
Australian Government
Immunisation Hotline 1800 671 811
http://immunise.health.gov.au/
Education and Research
National Centre for Immunisation Research & Surveillance of
Vaccine preventable diseases
www.ncirs.usyd.edu.au
National Immunisation Program (NIP) 1 July 2011
• birth hepatitis B
• 2 months DTPa/IPV/Hib/hep B, 13vPCV, ORV
• 4 months DTPa/IPV/Hib/hep B, 13vPCV, ORV
• 6 months DTPa/IPV/Hib/hep B, 13vPCV, ORV
• 12 months MMR, Hib, MenC
• 18 months varicella
• 4 years DTPa/IPV, MMR
National Immunisation Program (NIP) 1 July 2011
• 10-13 years hepatitis B, varicella, HPV (girls
only)
• 15-17 years dTpa
• 50 years ADT
• adults 65+ influenza (every year)
pneumococcal
States and Territories
• implement the National Immunisation Program
• allocate funds for free vaccine in efficient and effective
manner
• ensure services equitable, acceptable and appropriate
to the population
• Provide funding to local government to conduct
immunisation – both fee for service and incentive
payments
• appropriate management systems
States and Territories (cont.)
• purchase and provide vaccines to all immunisation
providers
• establish vaccine distribution system which maintains
cold chain standards
• surveillance of
– immunisation coverage (ACIR, school
coverage)
– incidence of VPD’s (including
outbreak investigation)
States and Territories (cont.)
• surveillance of
vaccine wastage levels
adverse events following immunisation
• liaise with the Australian Government through the NIC
• develop regional targets for immunisation coverage
Immunisation in Victoria
• Immunisation is provided by:
local government (pre-school) 45%
– Community sessions
– small number M&CH nurses
– School based 90%
general practitioners 50% under school age
others eg.hospitals, Aboriginal Health Services 5%
General practitioners vast majority of vaccines in older adults
Immunisation in local government
• Legislative framework
Public Health and Wellbeing Act 2008
non-delegable statutory obligation on Victorian councils
• “The function of every council under this Act is to seek to prevent diseases......through organised programs....by co-ordinating and providing immunisation services to children living or being educated within the municipal district”
• All local governments provide immunisation services for under school age children, and school based programs in secondary schools.
School entry certificate
• school entry immunisation status certificate is required
to be produced on entry to primary school
• Can be issued by local government, medical
practitioner or any immunisation provider
• ACIR Child History statement is accepted as an
immunisation status certificate
Australian Childhood Immunisation Register (ACIR)
• enrolment via Medicare, children 0-6 years
• data on child, vaccine/s, provider
• payment $6 per completed immunisation encounter
• cost shared between Australian Government/States
Australian Childhood Immunisation Register (ACIR)
• immunisation program evaluation
• measure coverage in terms of national goals and
targets
• assist with opportunistic immunisation
• child history statements
5 year old statement acts as the SEIC in Victoria

Immunisation coverage
Immunisation coverage Victoria
12 months 91.6% (rank 3)
2 years 93.4% (rank 2)
5 years 91.1% (rank 1)
Source ACIR (30 June 2011)
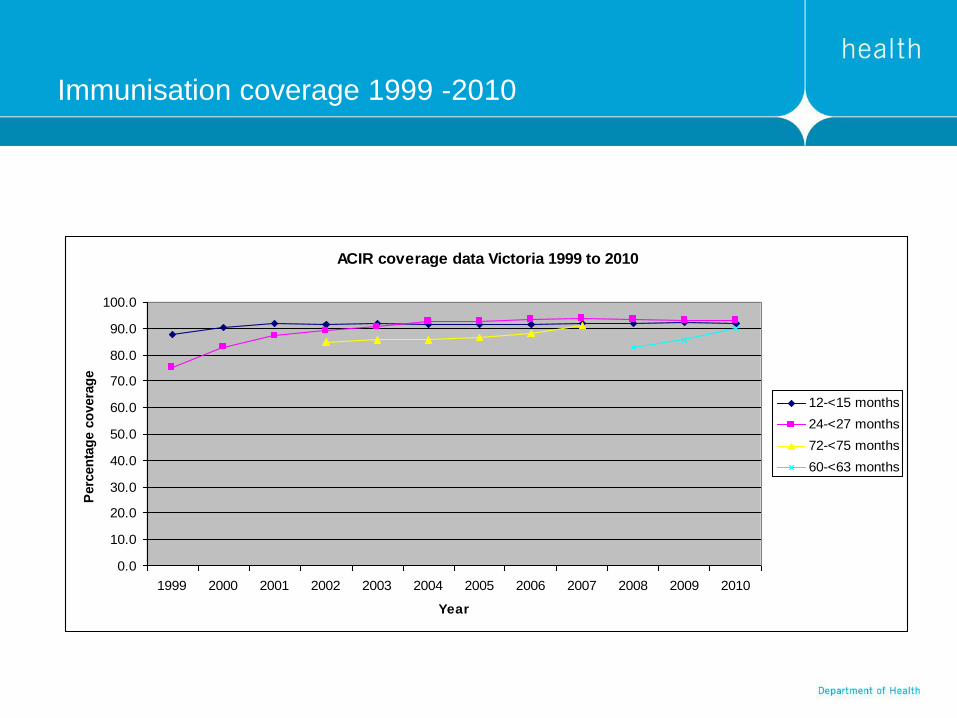
Immunisation coverage 1999 -2010
ACIR coverage data Victoria 1999 to 2010
0.0
10.0
20.0
30.0
40.0
50.0
60.0
70.0
80.0
90.0
100.0
1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Year
Perc
en
tag
e c
overa
ge
12-<15 months
24-<27 months
72-<75 months
60-<63 months

Immunisation coverage - indigenous
Immunisation coverage - indigenous
12 months 84.1% (rank 5)
2 years 93.0% (rank 3)
5 years 86.5% (rank 5)
Source ACIR (30 June 2011)
Improving Victoria’s program
New immunisation strategy 2009-2012
Key action areas
Whole of life immunisation
– Advocate for WoL register
– Improve data and coverage for key groups, eg older adults
Immunisation of high risk groups
– Occupational groups, eg HCWs, carers of elderly
– ATSI people, chronic medical conditions, juvenile justice/prisoners
– Address inequalities and gaps
Service quality
– Cold chain
– Right vaccine at right time
Immunisation strategy
• Public communication and participation
Public communication campaigns, including culturally relevant
Support consumer involvement and advocacy
• Partnerships
Encourage regional partnerships between providers, eg local
government, GPs, AMS
Stakeholder conference & recognition
• Research and development
Local research priorities, especially best practice service
delivery
SAEFVIC
Surveillance of Adverse Events Following Vaccination In
the Community (SAEFVIC)
Rationale:
Promote community confidence in immunisation
Rapidly detect & research vaccine safety concerns
Monitor & feedback adverse events local/nationally
Broad referral service
– Infants and children
– Adolescents and adults
Timely follow up and feedback for the reporter and the public
SAEFVIC
Enhanced passive reporting system
RCH lead agency for SAEFVIC
Referral service to:
• Royal Children’s Hospital – child AEFI
• VIDS - Royal Melbourne Hospital – adult AEFI
• Monash Medical service – child/adult AEFI
Question
• You are the newly appointed immunisation co-ordinator
for your local shire council
How would you go about setting up and monitoring
the immunisation program?
Some ideas
Current immunisation coverage?
Current incidence of VPDs?
Immunisation providers – your council immunisation
nurses, MCH nurses, GPs, local hospital?
Geographic accessibility of sessions?
Community “feel” of sessions?
Equipment for vaccine storage, administration, consent,
recording, reporting to ACIR
Adverse events management and reporting
Some ideas
Evaluation of sessions – consumer feedback
Evaluation of sessions – coverage achieved
Process for following up overdue children?
School immunisation certificates – process to check?
School immunisation- relationship with schools

Invasive Meningococcal Disease
Meningococcal C vaccine
• Meningococcal C conjugate vaccine
• Given as single dose at 12 months
• Phase 1 commenced 1 January 2003
Children 1 to 5 years
Adolescents 15 to 19 years
• Phase 2 commenced 1 July 2003
Children 6 to 14 years
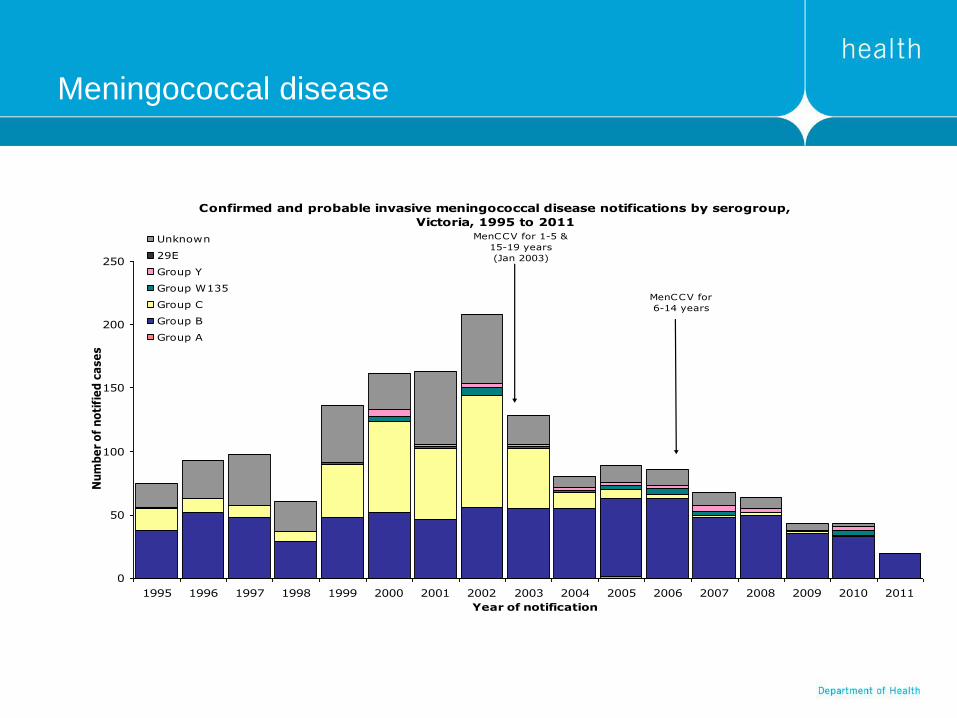
Meningococcal disease
Confirmed and probable invasive meningococcal disease notifications by serogroup,
Victoria, 1995 to 2011
0
50
100
150
200
250
1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011
Year of notification
Nu
mb
er
of
no
tifi
ed
ca
se
s
Unknown
29E
Group Y
Group W135
Group C
Group B
Group A
MenCCV for 1-5 &
15-19 years
(Jan 2003)
MenCCV for
6-14 years
Pneumococcal disease
Meningitis
Septicaemia
Pneumonia
Otitis media
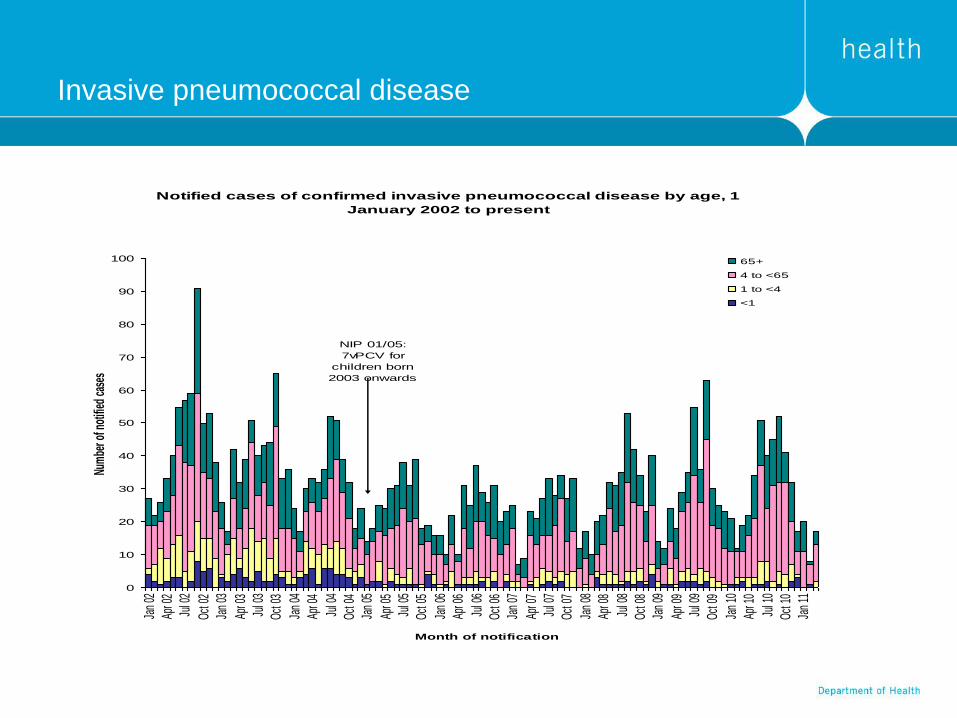
Invasive pneumococcal disease
Notified cases of confirmed invasive pneumococcal disease by age, 1
January 2002 to present
0
10
20
30
40
50
60
70
80
90
100
Jan
02
Apr 0
2
Jul 0
2
Oct 0
2
Jan
03
Apr 0
3
Jul 0
3
Oct 0
3
Jan
04
Apr 0
4
Jul 0
4
Oct 0
4
Jan
05
Apr 0
5
Jul 0
5
Oct 0
5
Jan
06
Apr 0
6
Jul 0
6
Oct 0
6
Jan
07
Apr 0
7
Jul 0
7
Oct 0
7
Jan
08
Apr 0
8
Jul 0
8
Oct 0
8
Jan
09
Apr 0
9
Jul 0
9
Oct 0
9
Jan
10
Apr 1
0
Jul 1
0
Oct 1
0
Jan
11
Month of notification
Num
ber o
f not
ified
cas
es
65+
4 to <65
1 to <4
<1
NIP 01/05:
7vPCV for
children born
2003 onwards
Pertussis
• Bacterial respiratory illness caused by Bordetella pertussis
Infants less than 6 months of age are at highest risk of severe
illness
50% of infants under 6 months hospitalised and some require
ICU admission
Protection not adequate until after 3 doses at 6 months of age
Combat increased incidence with “cocoon” strategy
Boostrix (adult DTPa vaccine) offered free to all parents of
infants born since 15 June 2009
Program currently running until June 2012
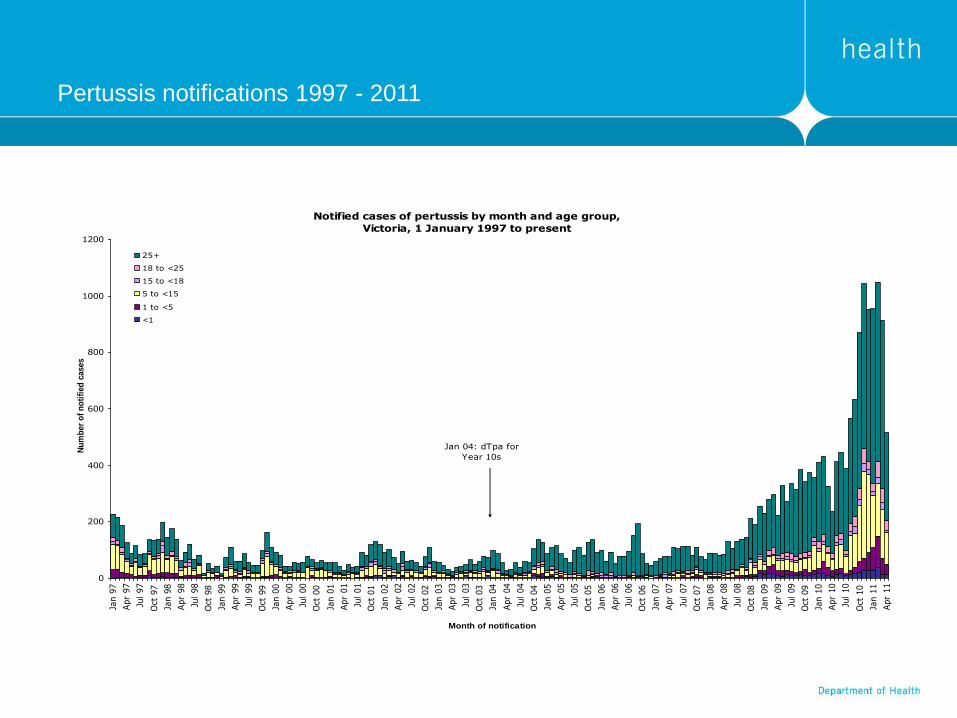
Pertussis notifications 1997 - 2011
Notified cases of pertussis by month and age group,
Victoria, 1 January 1997 to present
0
200
400
600
800
1000
1200
Jan 9
7
Apr
97
Jul 97
Oct
97
Jan 9
8
Apr
98
Jul 98
Oct
98
Jan 9
9
Apr
99
Jul 99
Oct
99
Jan 0
0
Apr
00
Jul 00
Oct
00
Jan 0
1
Apr
01
Jul 01
Oct
01
Jan 0
2
Apr
02
Jul 02
Oct
02
Jan 0
3
Apr
03
Jul 03
Oct
03
Jan 0
4
Apr
04
Jul 04
Oct
04
Jan 0
5
Apr
05
Jul 05
Oct
05
Jan 0
6
Apr
06
Jul 06
Oct
06
Jan 0
7
Apr
07
Jul 07
Oct
07
Jan 0
8
Apr
08
Jul 08
Oct
08
Jan 0
9
Apr
09
Jul 09
Oct
09
Jan 1
0
Apr
10
Jul 10
Oct
10
Jan 1
1
Apr
11
Month of notification
Nu
mb
er
of
no
tifi
ed
cases
25+
18 to <25
15 to <18
5 to <15
1 to <5
<1
Jan 04: dTpa for
Year 10s
Newer programs - HPV
• virus with over 100 different types
40 to 50 types affect the genital area
Classified as low-risk and high-risk types
– Low-risk types cause genital warts and/or changes to cervical cells
– High-risk types (~15) are linked to cervical cancer
• The virus can lie dormant in the body for a long time without causing a problem; often no noticeable symptoms
• 70-80% of cervical cancer cases in Australia are linked to HPV virus types 16 & 18
• Gardasil® protects against types 16 & 18 as well as types 6 & 8 (genital warts)
Newer programs - Rotavirus
• Characterised by sudden onset of fever,
vomiting and watery diarrhoea
• Highly contagious
• Generally transmitted by oral-faecal route
• Infects and replicates in cells of small intestine
• Average disease duration 6 days (3 - 8 days)
• Multiple infections in first few years of life
• Most Australian families will experience
rotavirus infection before their child turns five
References: Clark FH, Rotavirus Vaccines, WB Saunders, 1999; Parashar et al., Emerg Infect Dis, 2003.
Newer programs - Rotavirus
• Rotateq
Direct, serotype-specific protection against
all five common serotypes
• 98% efficacy against severe RGE
• 96% efficacy against hospitalisations
• 3 doses given at 2, 4 and 6 months of age
• Time limits for doses – all doses by 32 weeks; no catch
up
• TGA approved for all infants aged 6-32 weeks,
including pre-term
Reference: RotaTeq PI, May 2006

Immunisation website
www.health.vic.gov.au/immunisation





























