Embed Size (px)
Citation preview
This package has been developed to assist health care providers interested in the Implementation of the best practice guideline: Management of the Hemi Arm. We hope that you find any of the package contents helpful, and wish you much success. We are also interested in hearing from you. Please feel free to complete the Feedback Form enclosed in this package. Thank-you, The Planning Committee: Dalia Abromaitis, Jennifer Curry, Lorraine Katsios, Janet Liefso, Mary Thomas, Deb Willems, Sharon Wyville.
TABLE OF CONTENTS
Table of Contents _______________________________________________________ 1
Introduction ___________________________________________________________ 2
Purpose of Protocol _____________________________________________________ 2
Getting Started _________________________________________________________ 2
Audit _________________________________________________________________ 3
Feedback Form ________________________________________________________ 4 Appendix A: Best Practice Guidelines for the Management of the Hemiplegic Arm: A Positioning and Handling Protocol in an Acute Care Setting Appendix B: PowerPoint Presentation: Hemiplegic Shoulder Presentation for staff education sessions (on CD) Appendix C: Job Aid: Positioning Hemiplegic Arm: Lying on Hemiplegic Side; and Lying on Unaffected Side. (Right and Left) Appendix D: Job Aid: Independent Transfer of a Stroke Patient Standing up from a Chair. (Right and Left) Appendix E: Job Aid: Two Person Transfer of a Stroke Patient. (Right and Left) Appendix F: Job Aid: Two Person Transfer of a Stroke Patient using a Transfer Belt. (Right and Left) Appendix G: Job Aid: Single Person Transfer of a Stroke Patient. (Right and Left) Appendix H: Job Aid: Arm Sling (Right and Left) Appendix I: Sample Audit Appendix J: Power Point Presentation: Background Information: Management of the Hemiplegic Arm: Implementing a Best Practice Protocol (on CD)
*Please note the content of this package including photographs were based on the equipment likely to be available across a broad range of settings.
For more information regarding this package please contact:
Gina Tomaszewski, Regional Stroke Education Coordinator: [email protected]
OR
Deb Willems, Regional Rehabilitation Coordinator: [email protected]
Best Practice Guidelines for the Management of the Hemiplegic Arm:
A Positioning and Handling Protocol Introduction
In this package you will find a CD that contains the entire contents of the package in electronic form. As well, laminated hard copies of the bedside job aids are also provided. The job aids are organized into 2 sets: Right hemiplegic arm, and Left hemiplegic arm. Be sure to select the correct one when implementing. You may want to attach a “Please return to…” sticker at the back of each job aid so that they are returned to their rightful owner. Purpose of Protocol
This protocol was developed to support best practice guidelines for the management of the hemiplegic arm. The aim of the protocol is to prevent injury to the hemiplegic arm through careful handling and correct positioning. A sample protocol customized and piloted with acute care staff working with stroke patients at University Hospital, LHSC, and Regional Stroke Centre has been provided, (see Appendix A). The protocol on p. 2 of this document is a generic protocol which may be adapted to suit a variety of settings (acute, rehab, long-term care and community).
Getting Started Before implementing the protocol, you will need to:
• Identify target staff caring for the stroke survivor. Target staff are the health care providers
involved in the care of the stroke survivor. • Develop a small working group representative of the target staff who will be impacted by the
protocol. You will need to arrange a meeting with the workgroup to address the following Agenda items:
o Review the Hemiplegic Arm Protocol (p. 2), and the Power Point: Background
Information regarding the Management of the Hemiplegic arm (see Appendix J). o Determine when education sessions of staff will begin, and who is best suited to deliver
the education. (PowerPoint presentation available, see Appendix B). o Equipment needed for the protocol: lap trays, pillows, wheelchairs, and hemi slings. o Are there any policies that would impact the implementation of the Hemiplegic Arm
Protocol? o Target stroke survivors eligible for the protocol will need to be identified. These
patients would need to be identified by a qualified health care professional, using the inclusion criteria identified in # 3, p.2.
o Discuss evaluation, how will the implementation of the protocol be evaluated (see section: Goals of Protocol, Appendix A)
o Will an audit be done? A sample audit has been provided (see Appendix I).
Appendix A
Management of the Hemiplegic Arm: A Positioning and Handling Protocol
1. Education of health care providers on best practice guidelines, including: a. Anatomy of shoulder and pathoanatomy of hemiplegic shoulder. b. Handling of the hemiplegic arm during bed mobility and transfers. c. Application of a hemi-sling. d. Positioning of the hemiplegic arm when patient is in bed or in a chair.
2. To determine eligibility of the stroke survivor for this protocol in your clinical setting, the stroke survivor should be assessed by a qualified health care professional.
3. Inclusion criteria for the protocol:
e. Hemiplegic arm is flaccid f. And/ Or the patient is unable to lift the arm off the bed to 90 degrees g. And/ Or the arm is painful
4. Patients meeting the criteria will receive: h. A hemi sling at bedside. i. A hemi sling *Job Aid (see Appendix H) posted at bedside. j. A positioning *Job Aid (see Appendix C) posted at bedside. d. Eligibility for the protocol will be noted in the Kardex under the treatment section as follows: “Hemi Arm Protocol”. You may use a pink sticker to alert staff that the hemi arm protocol is in place for that particular patient.
5. A healthcare professional will assess the transfer of the patient and place the appropriate Job
Aids (see Appendices C to H) at the bedside. 6. A healthcare professional will provide a laptray and wheelchair to patients who require
assistance to transfer and meet the inclusion criteria.
References: 1. Best Practice Guidelines for Stroke Care. Heart and Stroke Foundation of Ontario. 2003. 2. Tips and Tools for Everyday Living: A Guide for Stroke Caregivers. Heart and Stroke Foundation of Ontario. 2002 3. Management of the Post Stroke Arm and Hand: Treatment Recommendations of the 2001 Consensus Panel. Barreca S (Ed) 2001. Protocol Development Team: Dalia Abromaitis OT, Jennifer Curry PT, Mary Thomas RN, Sharon Wyville RN Acknowledgements: Shari Gibbons OT, Lauralynn Kelly OT, Heather Ballagh PTA, Deb Willems and Gina Tomaszewski, SWO Stroke Strategy
*Job Aids are the laminated photographs of proper positioning techniques (see Appendices C to H) to be used with stroke survivors. These photographs act as prompts to remind and alert the immediate staff caring for the stroke survivor of proper positioning.
Audit
Introduction Purpose of the audit: The purpose of the audit would be to determine compliance with the protocol. It provides the interprofessional team with an indicator of whether the protocol is working and can identify the need for more training. It can be used to share results with staff from time to time. When to do the audit: The audit could be carried out at 3 months and 6 months post implementation; and/or at another time when the implementation team requires more information regarding progress. Who could carry out the audit? Members of the implementation working group or other champion staff representative of the interprofessional team. As well if available, students may also be involved.
See Appendix I for Sample Audit. (A spare form has been provided for photocopying purposes).
Appendix I
Subject Number: _____
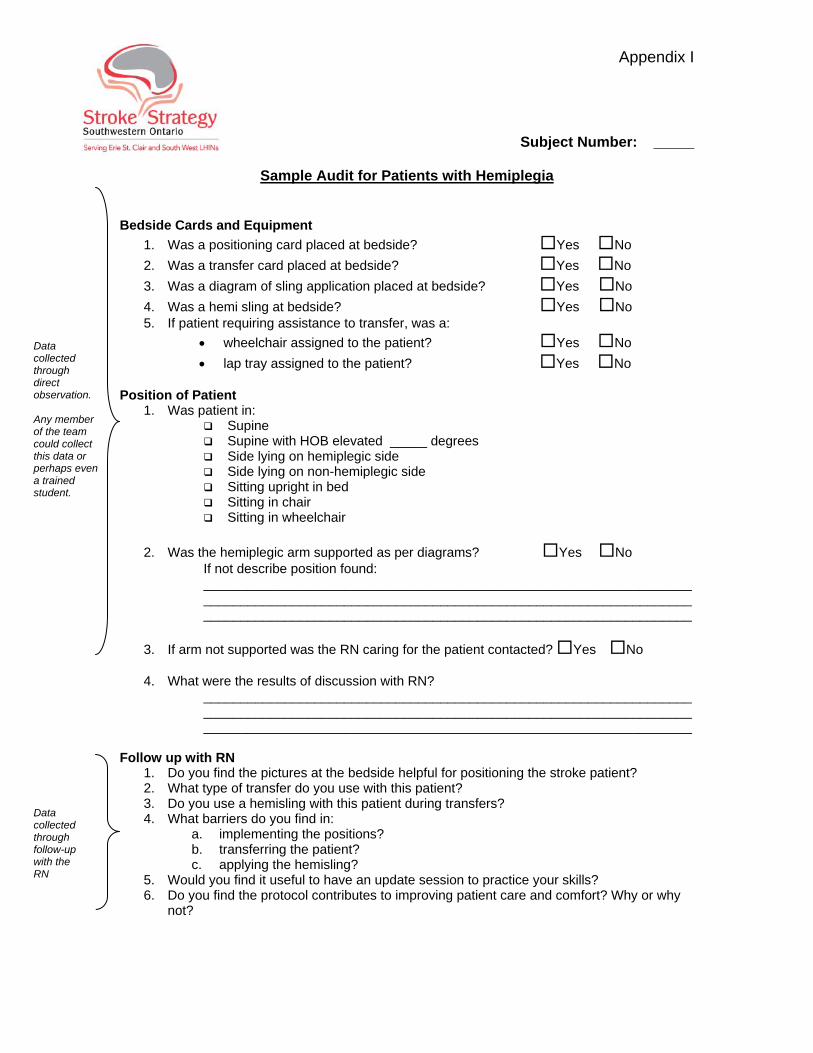
Sample Audit for Patients with Hemiplegia Bedside Cards and Equipment
Data collected through direct observation. Any member of the team could collect this data or perhaps even a trained student.
1. Was a positioning card placed at bedside? Yes No 2. Was a transfer card placed at bedside? Yes No 3. Was a diagram of sling application placed at bedside? Yes No 4. Was a hemi sling at bedside? Yes No 5. If patient requiring assistance to transfer, was a:
• wheelchair assigned to the patient? Yes No • lap tray assigned to the patient? Yes No
Position of Patient
1. Was patient in: Supine Supine with HOB elevated _____ degrees Side lying on hemiplegic side Side lying on non-hemiplegic side Sitting upright in bed Sitting in chair Sitting in wheelchair
2. Was the hemiplegic arm supported as per diagrams? Yes No
If not describe position found: ______________________________________________________________________________________________________________________________________________________________________________________________________
3. If arm not supported was the RN caring for the patient contacted? Yes No 4. What were the results of discussion with RN?
____________________________________________________________________________________________________________________________________ __________________________________________________________________
Follow up with RN
Data collected through follow-up with the RN
1. Do you find the pictures at the bedside helpful for positioning the stroke patient? 2. What type of transfer do you use with this patient? 3. Do you use a hemisling with this patient during transfers? 4. What barriers do you find in:
a. implementing the positions? b. transferring the patient? c. applying the hemisling?
5. Would you find it useful to have an update session to practice your skills? 6. Do you find the protocol contributes to improving patient care and comfort? Why or why
not?
FEEDBACK FORM
Your feedback is important to us. Please take the time to complete the following questions. 1. Did you find this package useful? Please describe: 2. What parts of the package were useful? Please list below: 3. What could be improved? Please describe: Thank you for taking the time to complete this form. Please return feedback form by fax to 519-663-3753 attn: SWO Stroke Strategy
B kg d I f tiAppendix J
Background Information
Management of the Hemiplegic Arm: Implementing a Best Practice Protocol
Dalia Abromaitis, OT Reg (Ont)f CJennifer Curry, PT
www.swostroke.ca
ObjectivesObjectives• Provide tools for identifying best practice needs.Provide tools for identifying best practice needs.
• Describe method to create action plan and • Describe method to create action plan and implement change.
• Illustrate process of implementing best practice
BackgroundBackground• Coordinated Stroke Strategy and Heart and Stroke Foundation of
Ontario published “Best Practice Guidelines for Stroke Care” in 2003.
• The best practice guideline for acute care post stroke is management in p g p gan organized stroke unit by specially trained staff with the goal of preventing complications and ensuring early rehabilitation.
• The guidelines listed numerous complications including dysphagia and aspiration, deep vein thrombosis, depression and shoulder injuries.
Identifying Best Practice GapsIdentifying Best Practice Gaps• The interdisciplinary stroke team at London Health Sciences Centre -p y
University Hospital held a retreat in May 2005.
• The retreat was facilitated by the Regional Stroke Education Coordinator.
• The team identified gaps between current practice and best practice guidelines.
• The gaps were then prioritized by the team.
• Working groups or subcommittees were formed for each of the prioritized gaps identified.
Hemiplegic Arm SubcommitteeHemiplegic Arm Subcommittee• Team Members: Two Registered Nurses, an Occupational g
Therapist, a Physiotherapist, Regional Stroke Education Coordinator, Regional Rehab Coordinator.
• Reviewed a number of references (see Appendix 1) for best practice management of the hemiplegic arm.
• Determined that correct positioning and handling the hemiplegic arm using an interprofessional model was the priority.
Hemiplegic Arm Protocol Development
• Questions to guide protocol development:Q g p p• What is the gap between the current practice and best
practice?
• How will the gap be bridged?
• Who will champion the change in practice?
• What education will be needed to assist the change in practice?
Hemiplegic Arm Protocol Development
• Questions continued:Questions continued:• What resources (equipment and human) will be needed
to assist the change in practice?
• How will the change in practice be evaluated?
• Are ethics approval required for implementation of the protocol?protocol?
Facilitating Change in Practice
Model of ImprovementModel of Improvement
The ProtocolThe Protocol
Hemiplegic Shoulder Best Practice Positioning And Hemiplegic Shoulder Best Practice Positioning And Handling Protocol
ObjectiveObjectiveThe hemiplegic upper extremity will be protected The hemiplegic upper extremity will be protected from injury by being properly handled during mobility and transfers and properly positioned in bed or wheelchair, according to the positioning protocol diagrams for all patients meeting the
it i f th t lcriteria for the protocol.
Inclusion CriteriaInclusion Criteria• Hemiplegic arm is flaccid.Hemiplegic arm is flaccid.
• And/or patient is unable to lift arm off bed to 90°• And/or patient is unable to lift arm off bed to 90 .
• And/or the arm is painful• And/or the arm is painful.
ProcedureProcedure
• OT, PT or RN assesses patients for protocol inclusion criteria
• Patients meeting criteria will receive:• A hemi sling at bedside• Hemi sling application directions posted at bedside• Eligibility for the protocol noted in the kardex
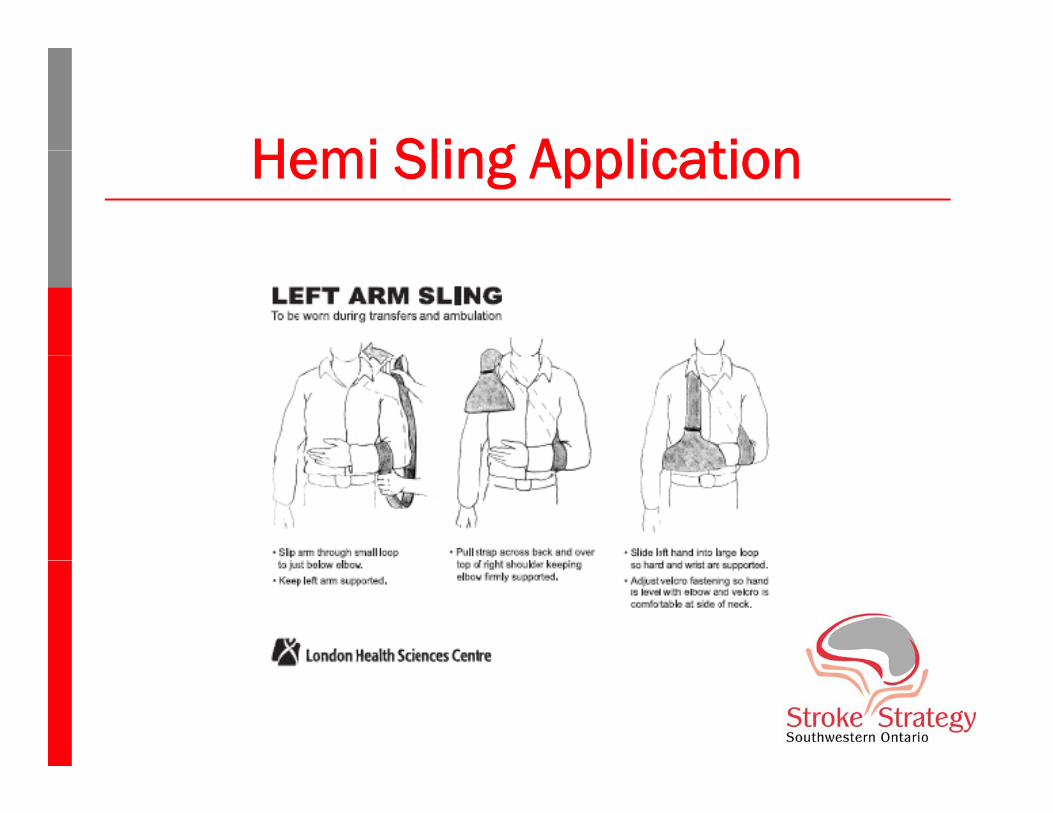
Hemi Sling ApplicationHemi Sling Application
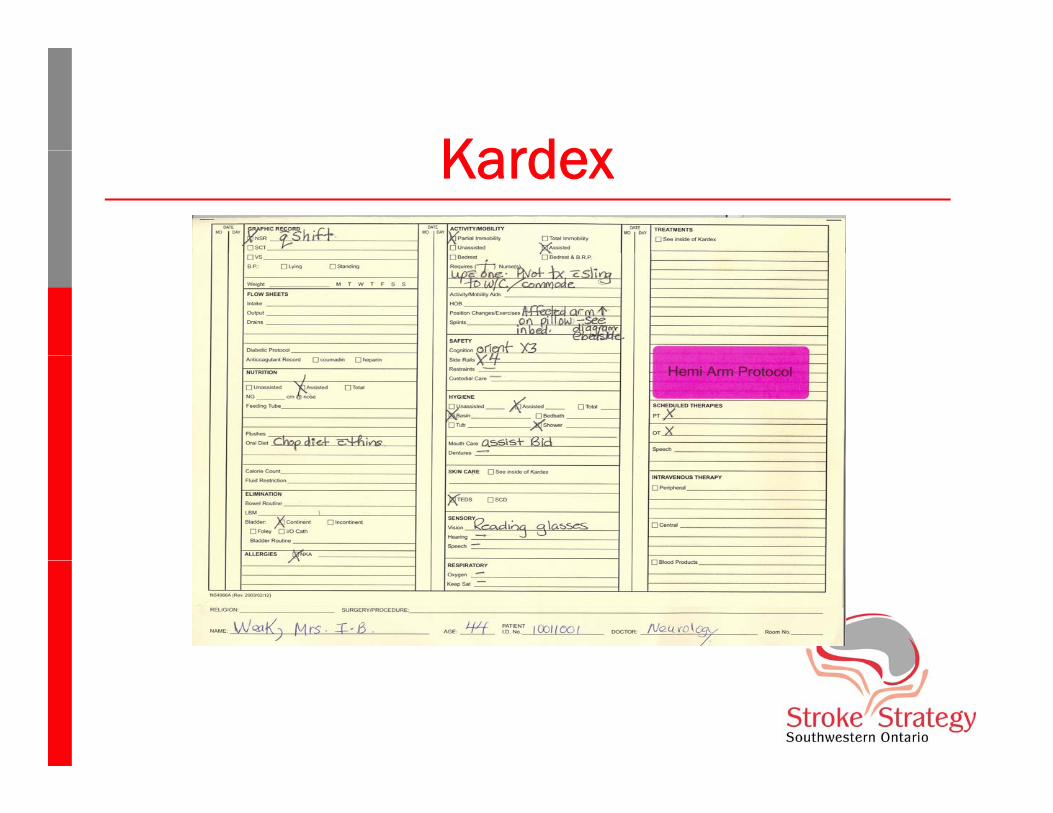
KardexKardex
Procedure (cont’d)Procedure (cont’d)• PT to assess transfer and post transfer card at bedsidep• OT/OTA/PT/PTA to provide laptray and wheelchair for
patients meeting criteria and who require assist with t ftransfers
• PT to assess and document Chedoke McMaster Stroke Assessment (CMSA) shoulder pain score on admission and ssess e t (C S ) s ou de pa sco e o ad ss o a ddischarge

Lying On Hemiplegic SideLying On Hemiplegic Side
Lying on Unaffected SideLying on Unaffected Side
Sitting In BedSitting In Bed

Sitting In WheelchairSitting In Wheelchair

Independent TransferIndependent Transfer

Single Person TransferSingle Person Transfer
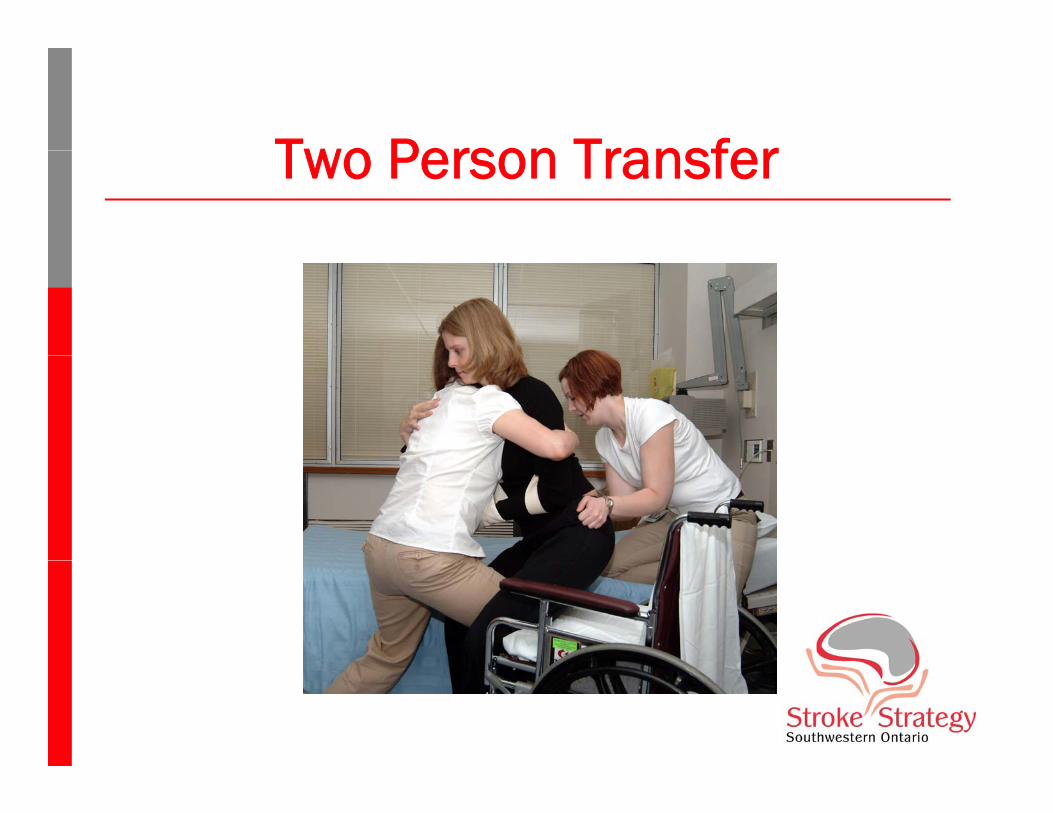
Two Person TransferTwo Person Transfer

2 P T f T f B lt2 Person Transfer-Transfer Belt
Protocol SynopsisProtocol SynopsisHemi Arm Protocol
Who qualifies?Any patient who has:• Flaccid arm• Inability to lift arm to 90 degrees when lying in the bed• Painful shoulder or arm
Who assesses the patient for eligibility?RN OT PT
What to do if patient requires hemi arm protocol:Place “Hemi Arm Protocol” sticker in treatment section of Kardex.Post or place the following at bedside:Post or place the following at bedside:
o Positioning of the hemiplegic arm photo pageo Sling application diagram
Hemi sling Lap tray (Best if combined with appropriate wheelchair which OT or PT will provide when equipment is available.)
o Transfer card (PT to post once transfer assessed) o Assess Chedoke McMaster Shoulder Pain Inventory on admission and discharge (PT or OT to do).
Where to find the above items:In clean equipment room in east hallway.
• Look for clear container marked “hemi slings”.
Further Questions contact: : Jennifer Curry PT Dalia Abromaitis OT Sharon Wyville RN Mary Thomas RNQ y y y
GoalsGoals• 100% of patients meeting the criteria will have :p g
• Hemi sling at bedside• Hemi sling directions posted at bedside
Eligibility for protocol noted in kardex• Eligibility for protocol noted in kardex
• 100% of patients meeting protocol criteria and requiring assist for transfers will have a laptray and wheelchair assigned to them
Goals (cont’d)Goals (cont’d)• 100% of stroke patients will have CMSA shoulder 100% of stroke patients will have CMSA shoulder
pain score completed by PT on admission and discharge.
• 100% of CNS RN’s, OT’s, PT’s, OTA’s, PTA’s will be educated in the use and procedures contained in the protocol
Hemiplegic Arm EvaluationHemiplegic Arm Evaluation• AuditsAudits
• Conducted pre implementation and 1,2,7 and 8 months post implementation.
• Patients identified from the OT/PT caseload.
• Utilized PT student for the first audits and an RN student for the last two audits.for the last two audits.
Hemiplegic Arm EvaluationHemiplegic Arm Evaluation• Audit Content (see Appendix 3)
• Check of Kardex for Hemi Arm sticker• Observation at bedside for:
o Job aids (positioning diagrams, sling application diagrams and transfer cards)
o Hemislingo Wheelchair
P iti f ti to Position of patient• Interview of nurse re: use of job aids and barriers to implementation• Did not audit for CMSA score due to restrictions with time and
health recordshealth records.
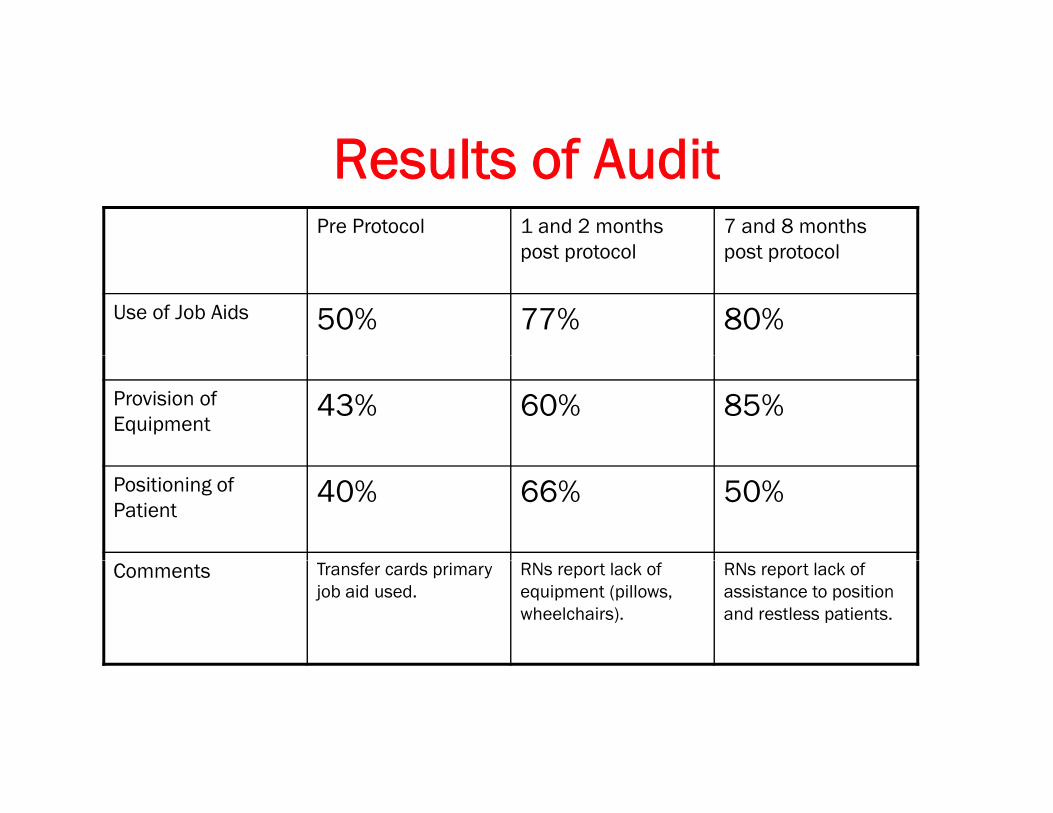
Results of AuditResults of AuditPre Protocol 1 and 2 months
post protocol7 and 8 months post protocolpost protocol post protocol
Use of Job Aids 50% 77% 80%
Provision of Equipment
43% 60% 85%
Positioning of Patient
40% 66% 50%
Comments Transfer cards primary job aid used.
RNs report lack of equipment (pillows, wheelchairs).
RNs report lack of assistance to position and restless patients.

Hemiplegic Arm EducationHemiplegic Arm Education• Developed presentation covering:Developed presentation covering:
• Anatomy of shoulder complex• Pathoanatomy of hemiplegic arm• Causes of hemiplegic shoulder pain• Management of hemiplegic arm
o Hemiplegic Arm Protocolo Practical session of positioning, sling application and transfers
H i l gi A Ed tiHemiplegic Arm Education• Inservice Education
• Began education using this method• Given twice a month • Sessions lasted 30 minutes.
• Review of Effectiveness• Review of Effectiveness• Not effective use of time.• Lack of staff attendance as staff required for clinical
duties.
H i l gi A Ed tiHemiplegic Arm Education• Formal Education
• Given concurrently with another stroke initiative teaching session.N id t tt d d ti i t id f • Nurses paid to attend education session outside of working hours.
• Focussed on education and had time to do practical session.
• Able to educate 95% of current RN staff using this method.
Hemiplegic Arm EducationHemiplegic Arm Education• Evaluation of Effectiveness
• Evaluation of pre and post workshop knowledge and skill.E l ti t d k l dg f ifi it ifi • Evaluations rated knowledge of specific items or specific skills on a scale of 1 to 5.
• See Appendix 2 for questionnaire given• RESULTS: Post workshop, the average showed an
improvement in knowledge and skill by one mark on the rating scale.g
Barriers to ImplementationBarriers to Implementation• Lack of sufficient equipment:q p
• Pillows• Appropriate wheelchairs• Slings • Laptrays
• Inconsistent orientation of new RN staff
• Lack of nurse champions for each shift and wing
Lessons LearnedLessons Learned• Timing of educational sessions relative to protocol g
implementation.
• Importance of RN “champions”• Importance of RN champions .
• RN student auditor
• OT’s and PT’s initiating protocol
• Need for Right and Left Hemi pictures and sufficient quantities of pictures
Next StepsNext Steps• Audit completion of CMSA pain score.p p
• OT and PT to further assess our own practice (treatment) of hemi arm as well as role delineation.

Questions?Questions?
Appendix B
H i l gi Sh ldHemiplegic ShoulderPower Point for staff education sessions
Jennifer CurryPhysiotherapist,
London Health Sciences Centre
www.swostroke.ca
AcknowledgementsAcknowledgements• Maria Lung BSc (PT), MScMaria Lung BSc (PT), MSc
• Train the Trainer Sessions 2003.
• Tips and Tools “Mobility Powerpoint”• Presented by therapists in Hamilton
OverviewOverview• Anatomy of Shoulder Complexy p
• Low Tone Shoulder
• High Tone Upper Limb
• Hemiplegic Shoulder Pain
• Practical Session
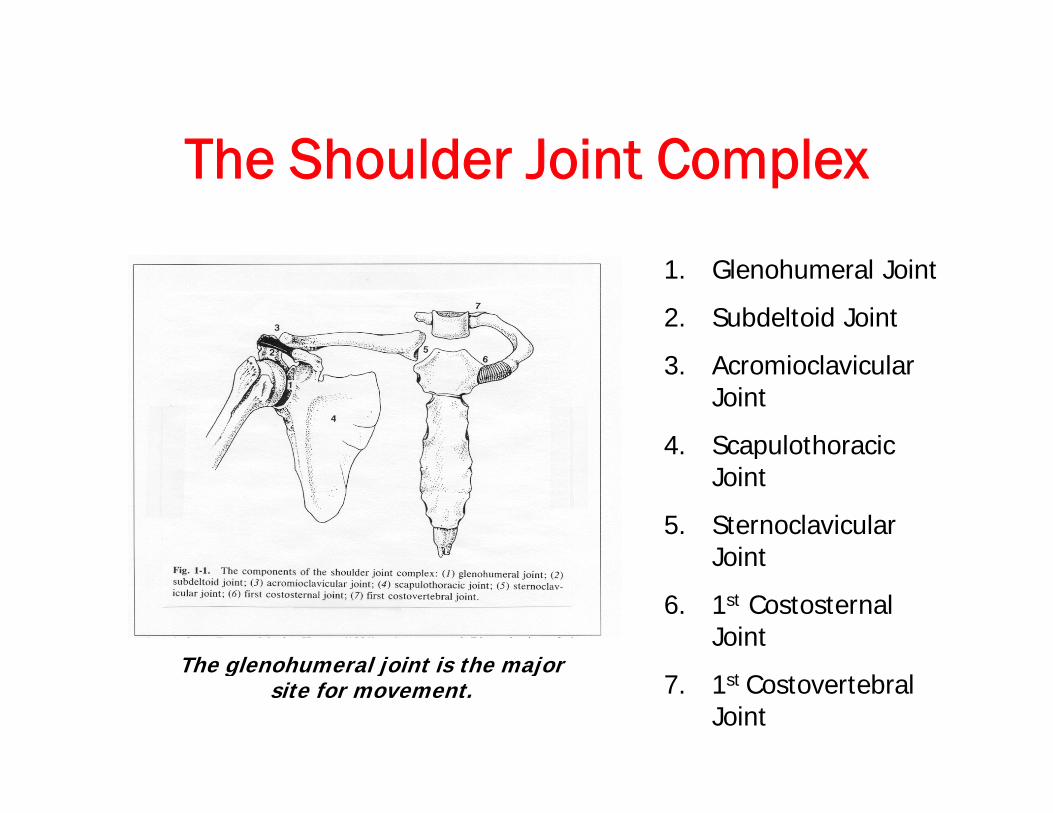
The Shoulder Joint ComplexThe Shoulder Joint Complex
1. Glenohumeral Joint
2. Subdeltoid Joint
3 A i l i l3. Acromioclavicular Joint
4. Scapulothoracic pJoint
5. Sternoclavicular JointJoint
6. 1st Costosternal Joint
The glenohumeral joint is the major7. 1st Costovertebral
Joint
The glenohumeral joint is the major site for movement.
Anatomy: Glenohumeral JointAnatomy: Glenohumeral Joint• Ball and socket joint.Ball and socket joint.
• Stability sacrificed for mobility• Stability sacrificed for mobility.
• Only 1/3 of humeral head in contact with glenoid • Only 1/3 of humeral head in contact with glenoid fossa at any time during movement.
Anatomy: Glenohumeral JointAnatomy: Glenohumeral Joint• Static StabilizersStatic Stabilizers
• Glenoid Labrum• Ligaments
o Glenohumeralo Coracohumeral
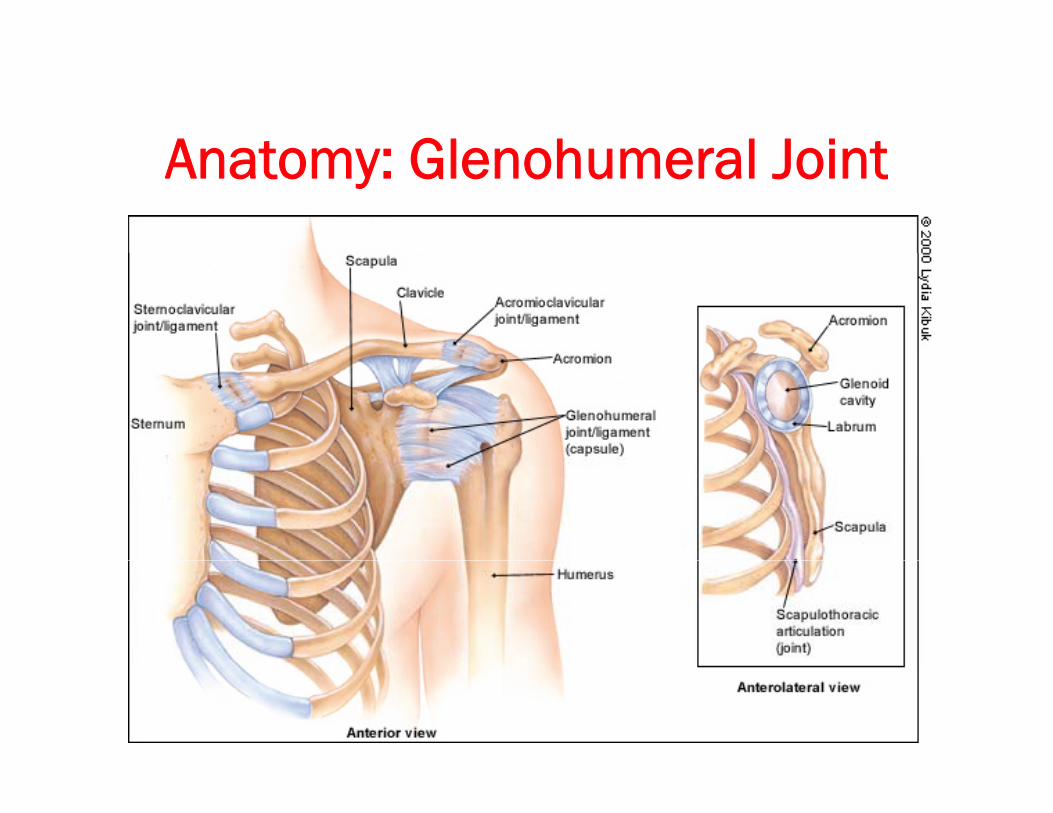
Anatomy: Glenohumeral JointAnatomy: Glenohumeral Joint
Anatomy: Glenohumeral JointAnatomy: Glenohumeral Joint• Dynamic Stabilizersy
• Rotator Cuff Muscleso Deltoid causes superior translation of humeral head during arm
elevationelevationo Rotator cuff muscles play a very important in “steering” humeral
head in glenoid fossao Deltoid and rotator cuff muscles work in a fine balance to o Deltoid and rotator cuff muscles work in a fine balance to
elevate the armo Supraspinatus muscle is important in stabilizing shoulder when
arm dependent (by side)
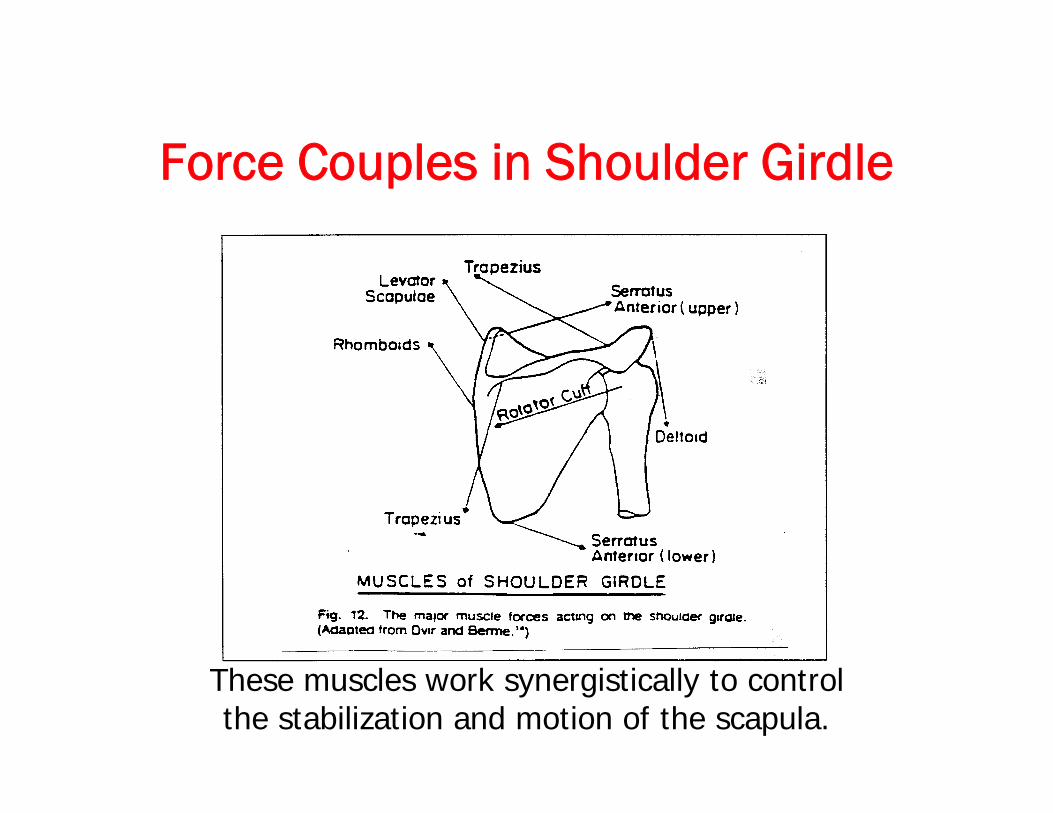
F C l i Sh ld Gi dlForce Couples in Shoulder Girdle
These muscles work synergistically to control the stabilization and motion of the scapula.
Anatomy: Arm ElevationAnatomy: Arm Elevation• 0-30 degreesg
• Setting of scapula• Primarily glenohumeral movement
30 150 d• 30-150 degrees• Scapulohumeral rhythm (2:1 GH:scapula)• External rotation and depression of humeral head to clear acromial
arch
• Beyond 150 degrees• Thoracic extension to complete elevation• Thoracic extension to complete elevation
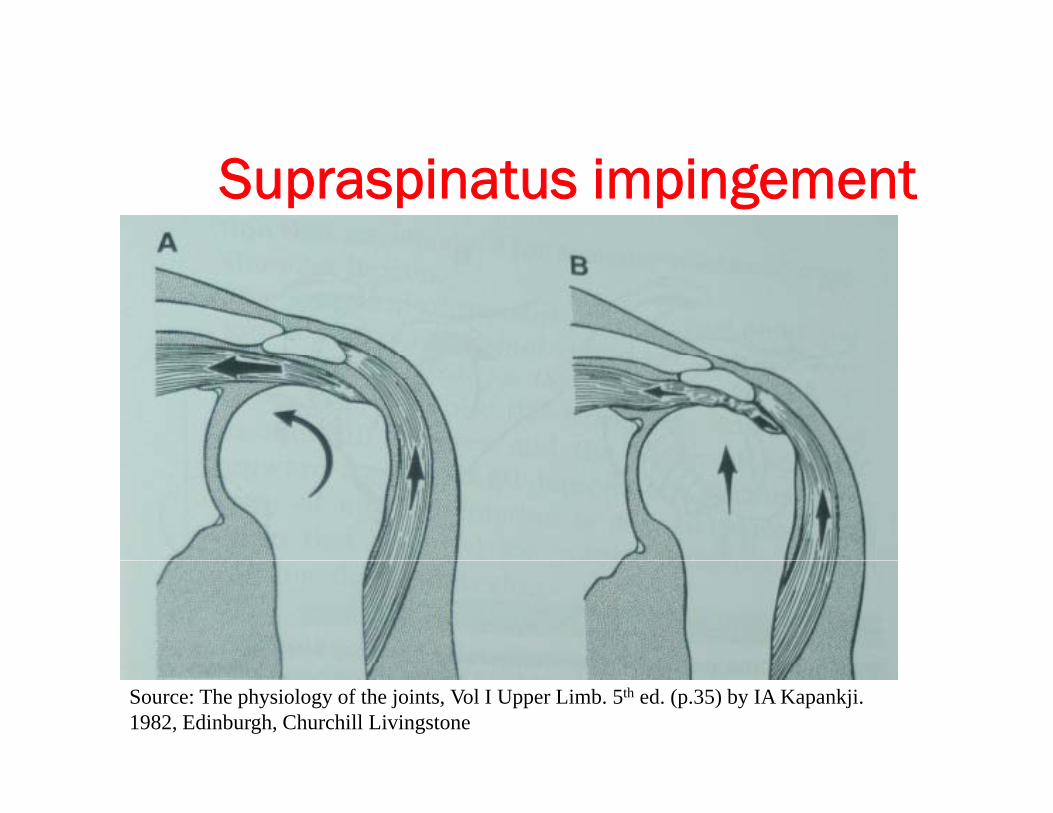
Supraspinatus impingement
Source: The physiology of the joints, Vol I Upper Limb. 5th ed. (p.35) by IA Kapankji. 1982, Edinburgh, Churchill Livingstone
Low Tone ShoulderLow Tone Shoulder• Most common in initial stages following stroke.g g
• Results from damage to the motor pathways innervating the upper limb musclesthe upper limb muscles.
• Low tone shoulders are highly susceptible to damage of the structures surrounding the shoulder (muscles, tendons, ligaments).
• Preventing subluxation is crucial in the early stages of stroke recovery- critical role for all team members
Low Tone ShoulderLow Tone Shoulder• Pathoanatomy of Subluxed Shouldery
• Flaccid or low tone muscles at shoulder and trunk lead to altered alignment of scapula and humerus.
• Dynamic stabilizers not present
• Reliance on static stabilizers which overstretch due to weight of arm in dependent position.
• Inferior subluxation is most common
Shoulder SubluxationShoulder Subluxation• Consequences of shoulder subluxation:Consequences of shoulder subluxation:
• Irreversible stretching of ligaments, tendons and capsule Irreversible stretching of ligaments, tendons and capsule leading to instability at the joint.
• Structural changes hamper recovery of muscle activity in shoulder complex.
• Traction injury to brachial plexus neurovascular bundle.
M f L T Sh ldManagement of Low Tone Shoulder
• Positioning• Positioning• Support low tone arm at all times:
o Use pillows, slings, lap traysp g p yo Slings should be worn during transfers or ambulation
only. They should be removed during sitting or in bed.o In sitting, position shoulder in slight flexion, abduction
and external rotation; forearm in pronation and hand in open weightbearing position.p g g p
o Pay attention to position of pelvis and trunk alignment when sitting.
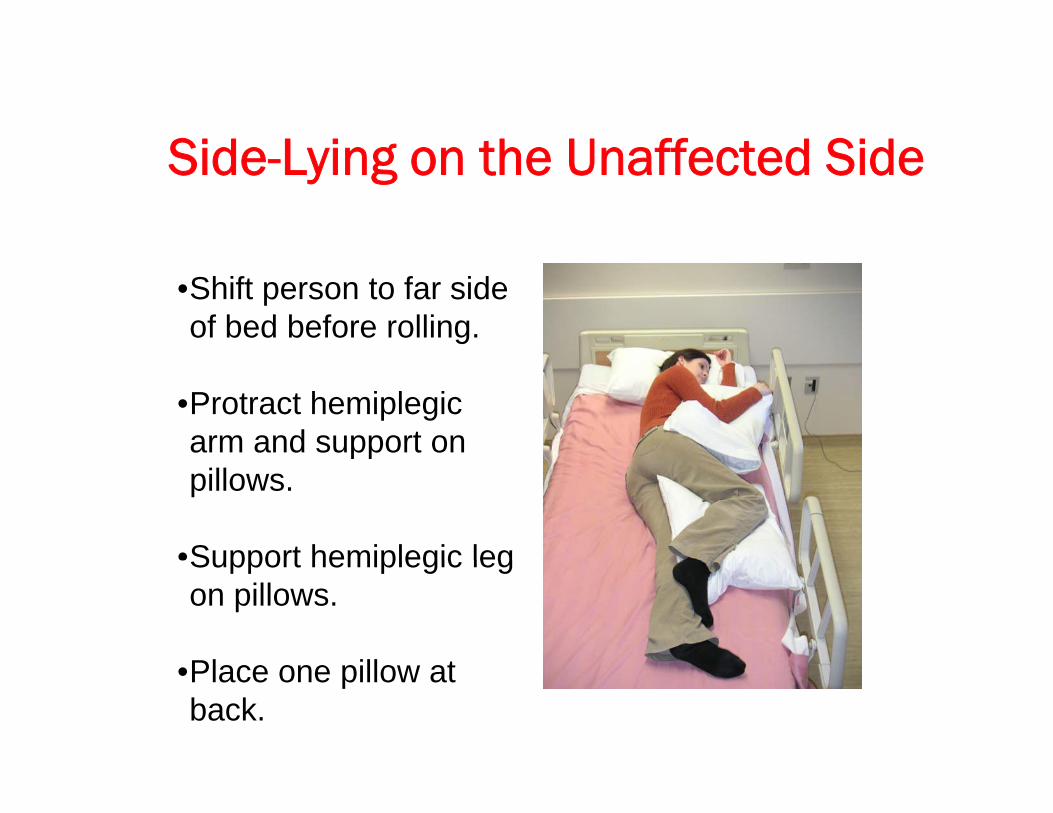
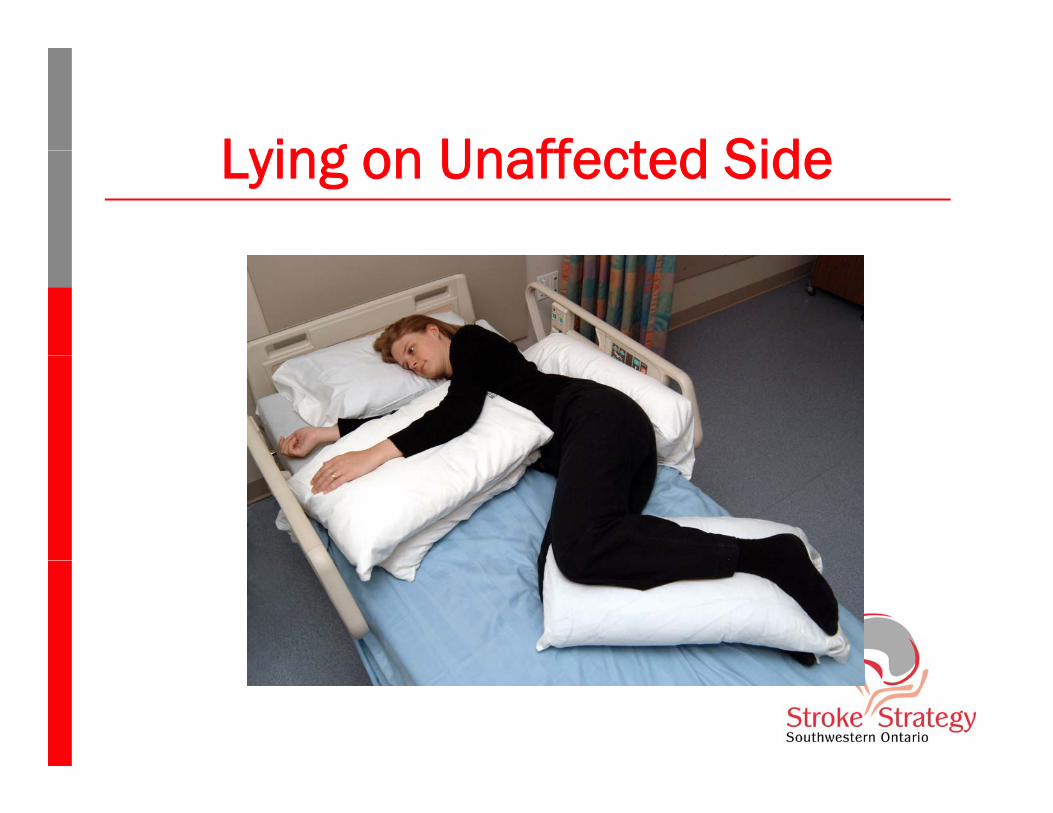
Side Lying on the Unaffected SideSide-Lying on the Unaffected Side
•Shift person to far side of bed before rolling.
•Protract hemiplegic arm and support on pppillows.
•Support hemiplegic legSupport hemiplegic leg on pillows.
Pl ill t•Place one pillow at back.
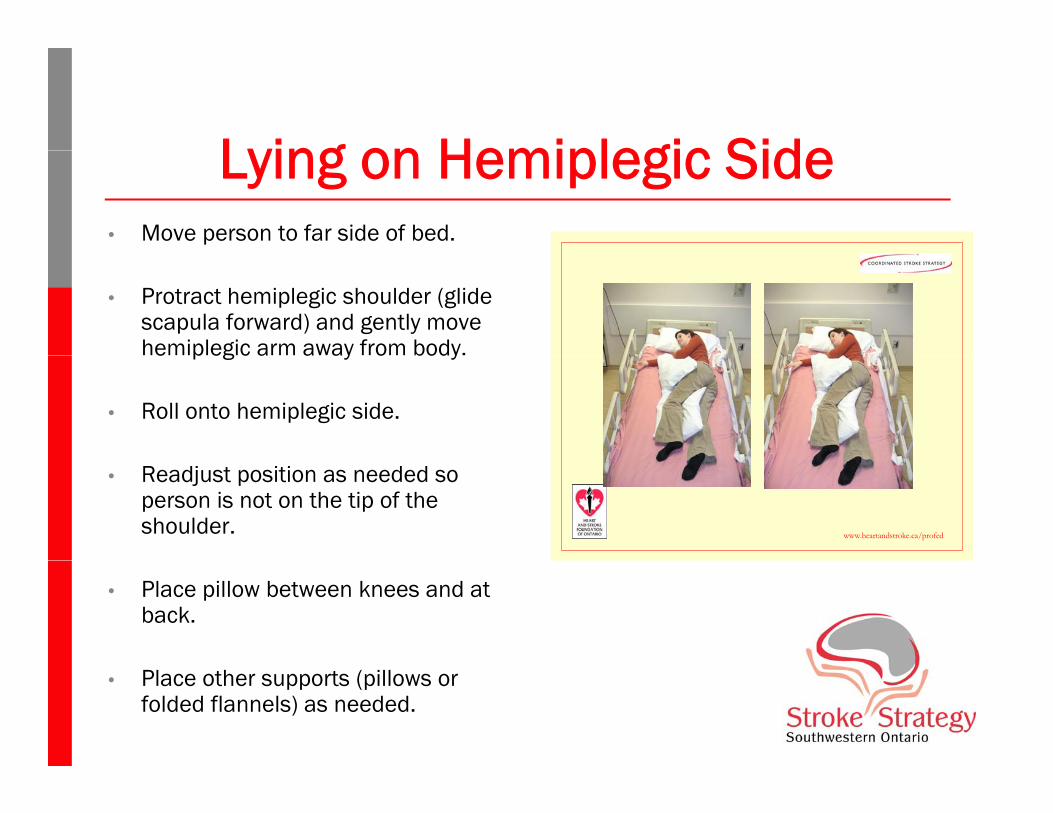
Lying on Hemiplegic SideLying on Hemiplegic Side• Move person to far side of bed.
• Protract hemiplegic shoulder (glide scapula forward) and gently move hemiplegic arm away from body.e p eg c a a ay o body
• Roll onto hemiplegic side.
• Readjust position as needed so person is not on the tip of the shoulder. www.heartandstroke.ca/profed
• Place pillow between knees and at back.
• Place other supports (pillows or folded flannels) as needed.
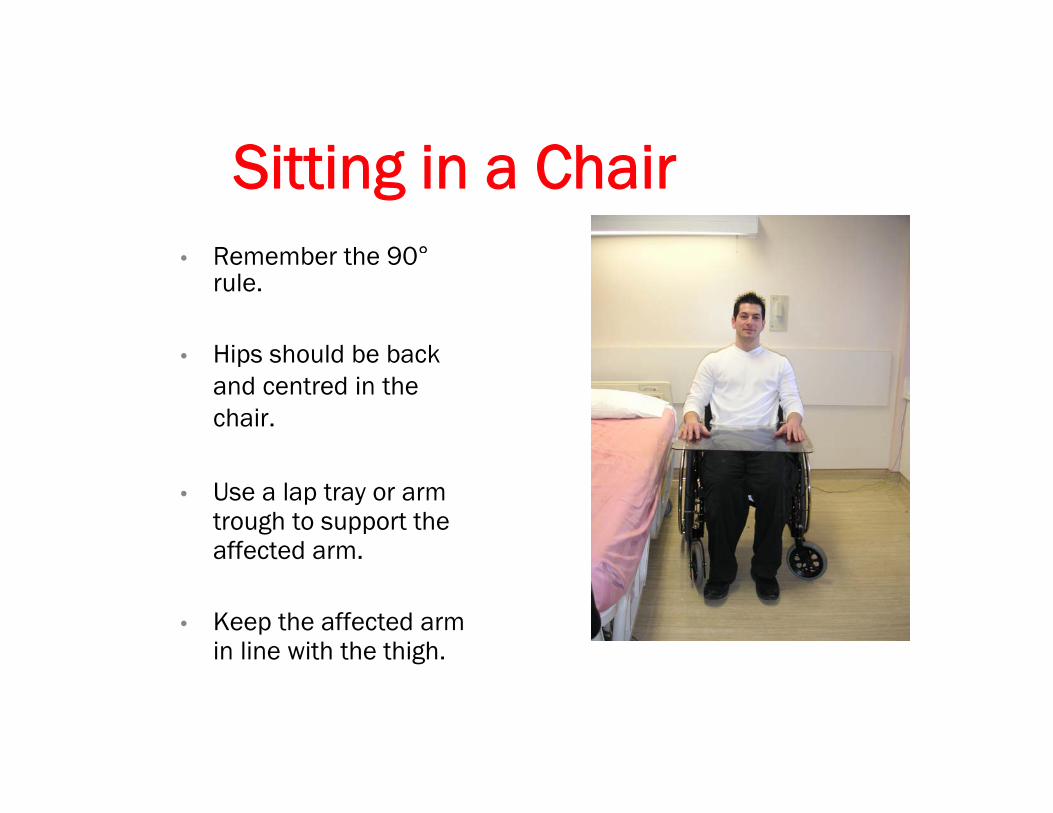
Sitti i Ch iSitting in a ChairRemember the 90°• Remember the 90rule.
• Hips should be back • Hips should be back and centred in the chair.
• Use a lap tray or arm trough to support the affected arm.
• Keep the affected arm in line with the thigh.g
M f h L T Sh ldManagement of the Low Tone Shoulder• Handling
B g tl• Be gentleo Avoid lifting through axilla or pulling on arm to move patient. Instead
grasp upper trunk near scapula to move person.
o Support both the humerus and hand when moving the affected limb to position or dress patient.
o Do not move arm beyond 90 degrees elevation unless have shoulder external rotation and scapular rotation.
o Dressing Rule for hemiplegia: “First on; last off”o Dressing Rule for hemiplegia: First on; last off .
• NOTE: Shoulder pain occurs more frequently i ti t h d d t f t fin patients who are dependent for transfers.
High Tone Upper LimbHigh Tone Upper Limb• Frequently occurs later post stroke.y
• Causes of high tone are multifactorial:Altered CNS > reflexive contractions• Altered CNS-> reflexive contractions
• Altered musculotendinous properties->stiffness• Position dependent.
• Consequences of high tone:• Impaired skin care (axilla and hand)• Impaired ADLs (dressing)• Impaired range of motion• Shoulder pain
High Tone Upper LimbHigh Tone Upper Limb• “Flexor Pattern”Flexor Pattern
• Scapular retraction• Shoulder internal rotation and adduction• Elbow flexion• Forearm pronation• Wrist and finger flexion
Management of the High Tone U Li bUpper Limb
• PositioningPositioning
• Promote position that is opposite to flexor pattern Promote position that is opposite to flexor pattern • Position for extended periods of time (up to 1 hour or
more) to promote lengthening of the tight muscles• Use pillows, airsplints, thermoplastic splints or casting
as required
Management of the High Tone U Li bUpper Limb
• Pharamcological Management:Pharamcological Management:
• Baclofen or TizanidineBaclofen or Tizanidineo CNS depressants that can decrease tone.
• Botoxo Blocks neuromuscular junction to cause relaxation at the
muscleo Lasts for 3 months
Hemiplegic Shoulder PainHemiplegic Shoulder Pain• Incidence of Shoulder Pain
• Up to 70% of stroke patients will have pain.
• Signs and Symptoms• Pain located in shoulder, may radiate down arm.
• Pain worse with movement especially ext rotn, abduction and flexion of GH joint.
• Pain may be present constantly and interferewith sleepwith sleep.
Hemiplegic Shoulder PainHemiplegic Shoulder Pain• TreatmentTreatment
• Respect the pain• Use NSAIDs and analgesics as indicated• Use modalities: heat, ice or TENS• Support the arm in position of comfort• Gentle range of motion exercises in painfree range with
correct biomechanics (no overhead pulleys!)
Practical SessionPractical Session• Putting on hemi-slingPutting on hemi sling• Positioning in bed:
• On hemiplegic sideOn hemiplegic side• On non-hemiplegic side• Upright in bed
• Two person front-back transfer
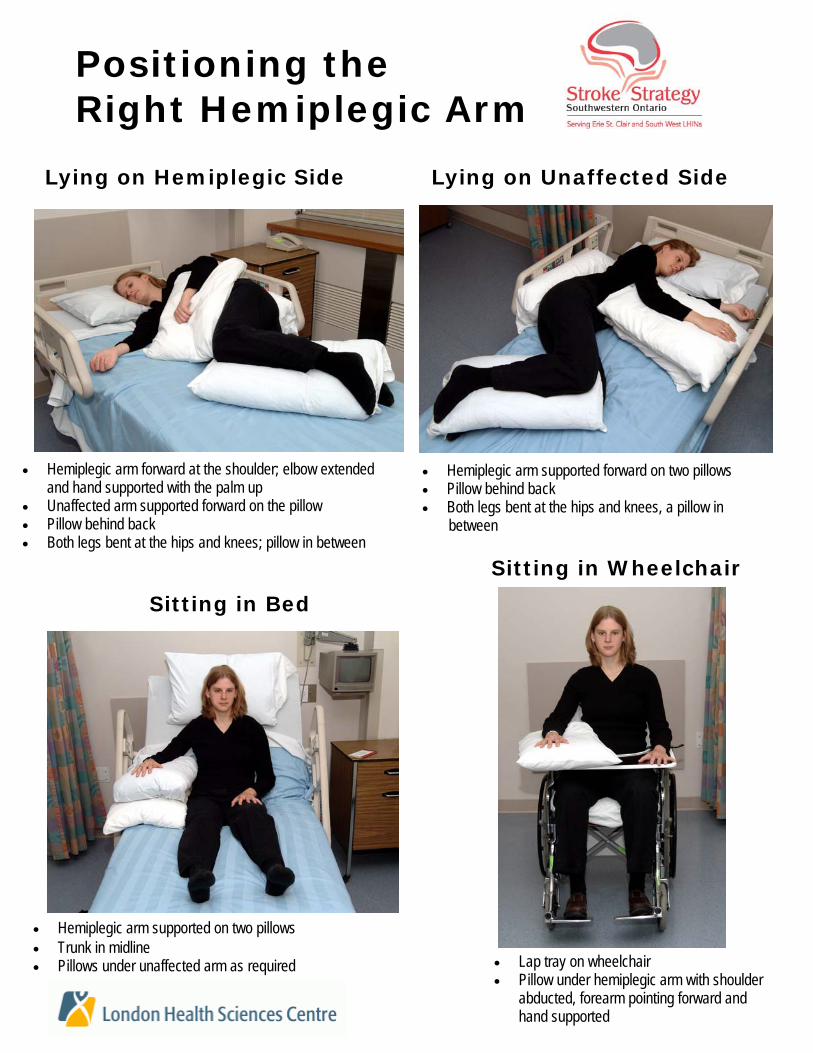
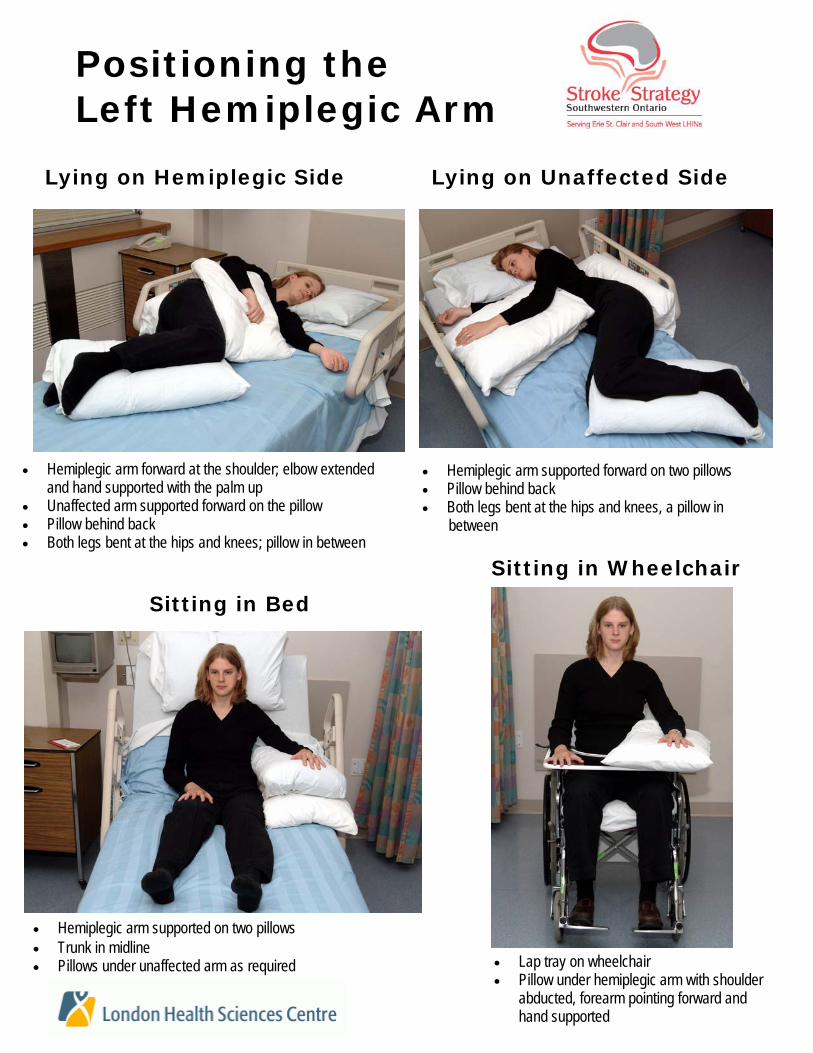
• Hemiplegic arm supported on two pillows • Trunk in midline • Pillows under unaffected arm as required
Sitting in Wheelchair
• Lap tray on wheelchair • Pillow under hemiplegic arm with shoulder
abducted, forearm pointing forward and hand supported
Lying on Hemiplegic Side
• Hemiplegic arm forward at the shoulder; elbow extended and hand supported with the palm up
• Unaffected arm supported forward on the pillow • Pillow behind back • Both legs bent at the hips and knees; pillow in between
• Hemiplegic arm supported forward on two pillows • Pillow behind back • Both legs bent at the hips and knees, a pillow in between
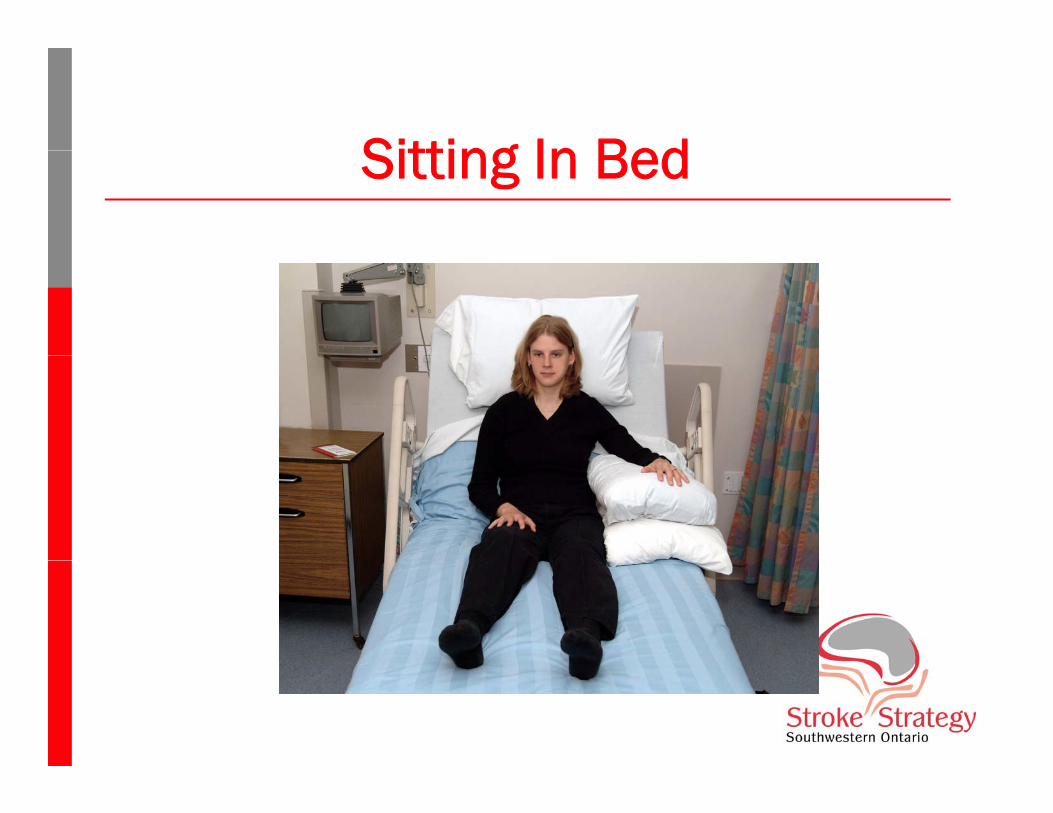
Sitting in Bed
Positioning the Right Hemiplegic Arm
Lying on Unaffected Side
• Hemiplegic arm supported on two pillows • Trunk in midline • Pillows under unaffected arm as required
Sitting in Wheelchair
• Lap tray on wheelchair • Pillow under hemiplegic arm with shoulder
abducted, forearm pointing forward and hand supported
Lying on Hemiplegic Side
• Hemiplegic arm forward at the shoulder; elbow extended and hand supported with the palm up
• Unaffected arm supported forward on the pillow • Pillow behind back • Both legs bent at the hips and knees; pillow in between
• Hemiplegic arm supported forward on two pillows • Pillow behind back • Both legs bent at the hips and knees, a pillow in between
Sitting in Bed
Positioning the Left Hemiplegic Arm
Lying on Unaffected Side
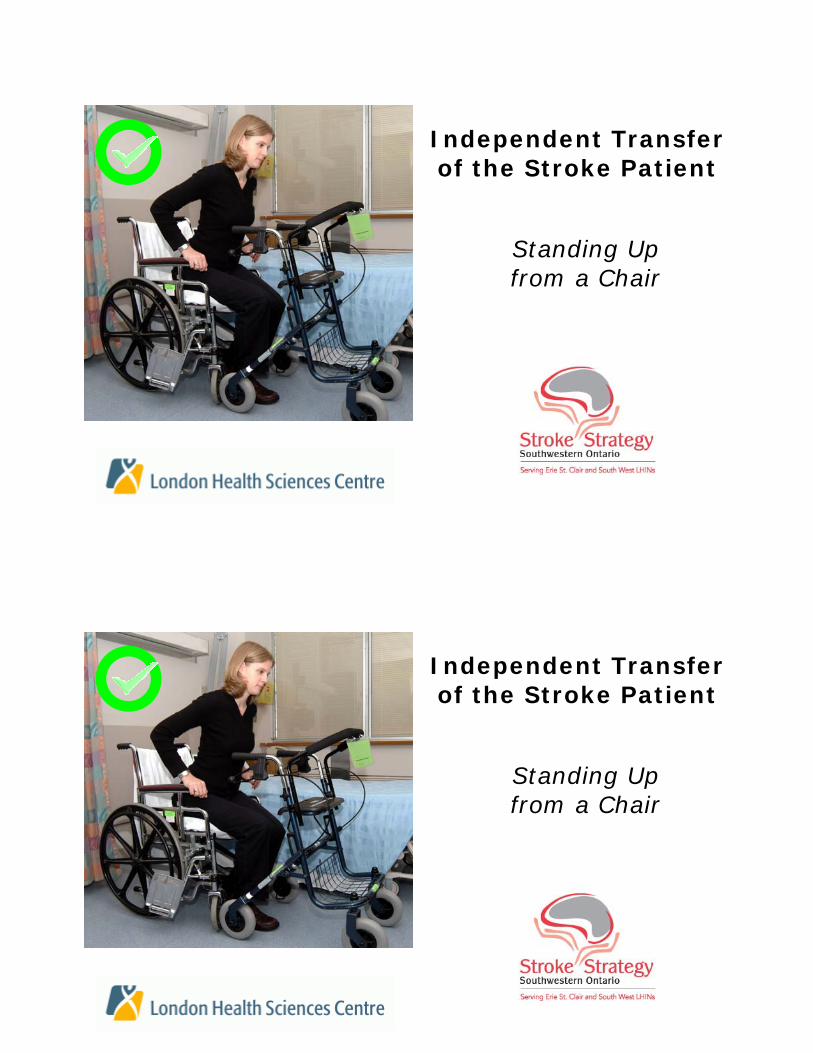
Independent Transfer of the Stroke Patient
Standing Up from a Chair
Independent Transfer of the Stroke Patient
Standing Up from a Chair
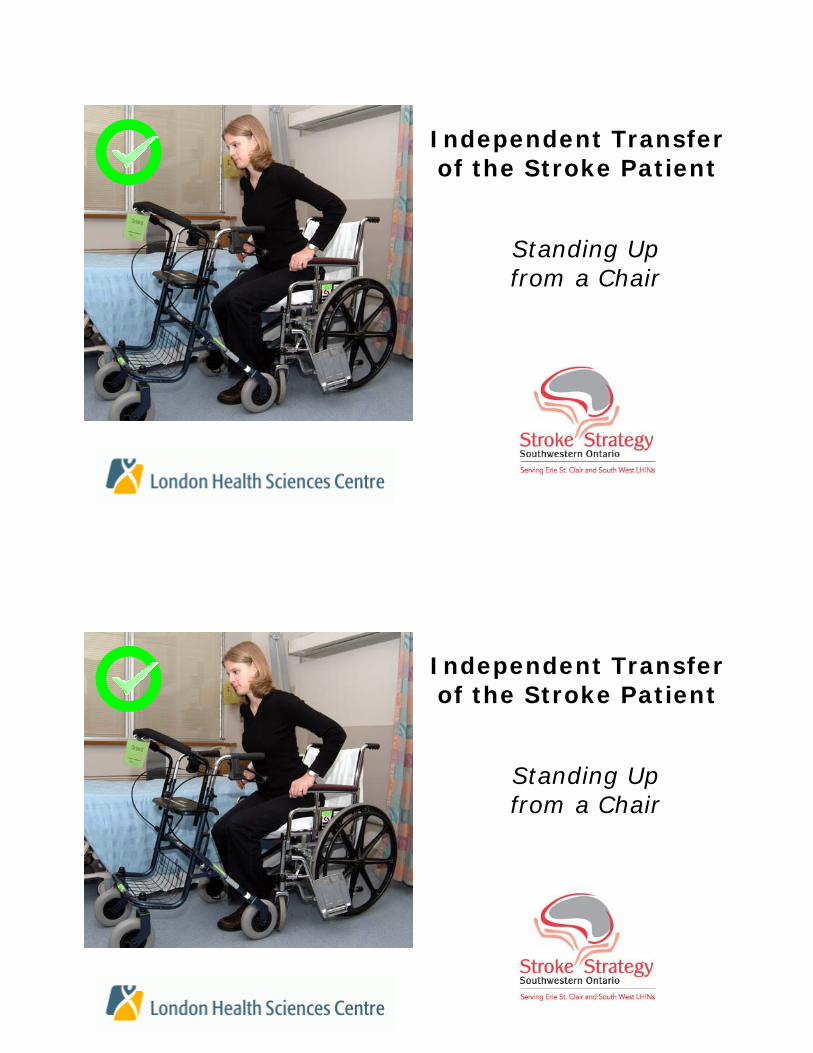
Independent Transfer of the Stroke Patient
Standing Up from a Chair
Independent Transfer of the Stroke Patient
Standing Up from a Chair
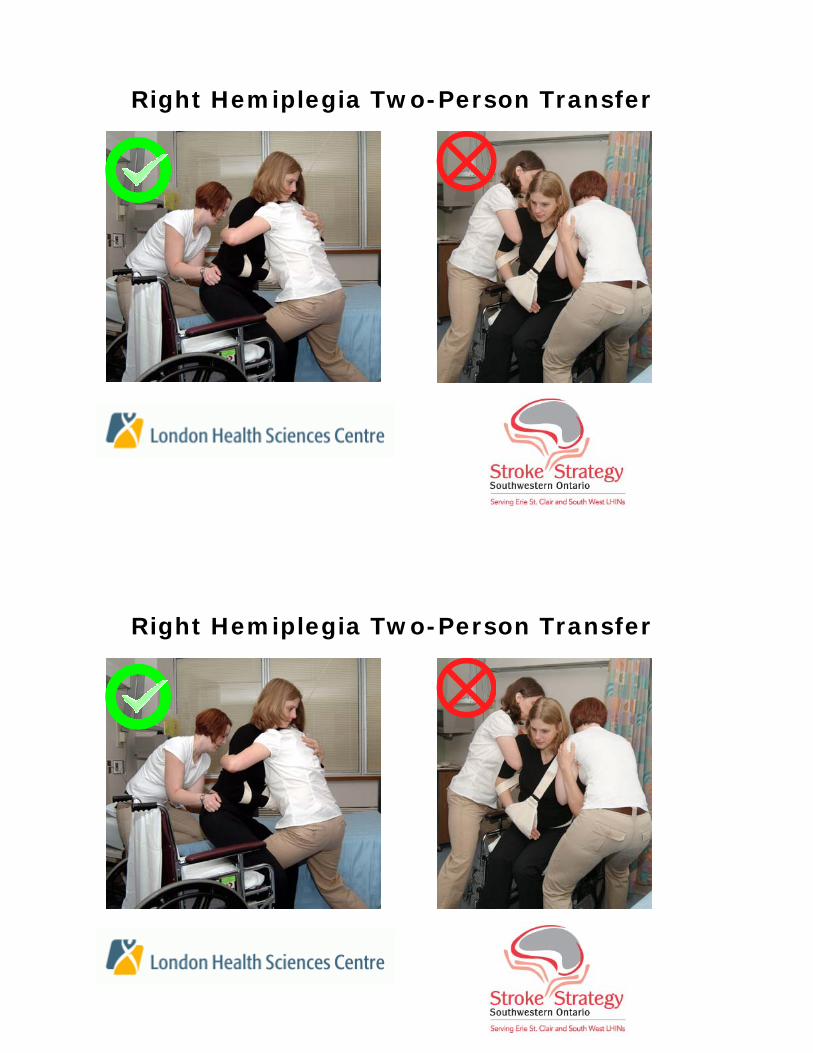
Right Hemiplegia Two-Person Transfer
Right Hemiplegia Two-Person Transfer
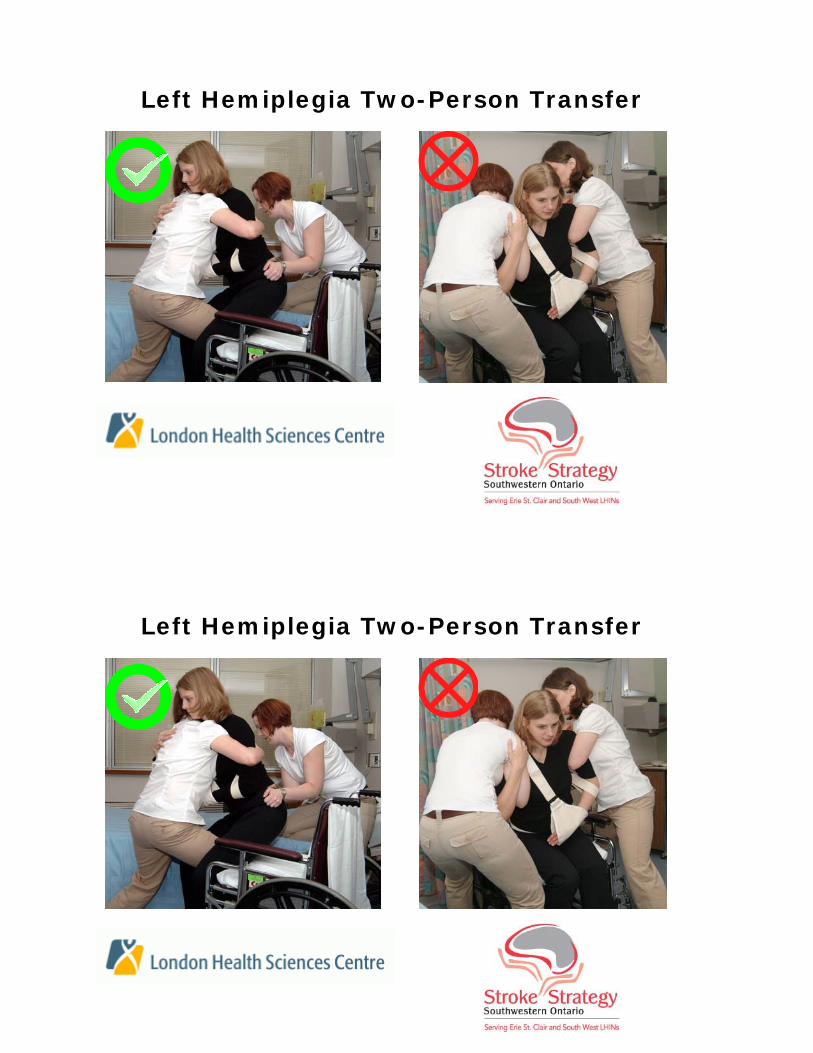
Left Hemiplegia Two-Person Transfer
Left Hemiplegia Two-Person Transfer
Right Hemiplegia Two-Person Transfer
Using a Transfer Belt
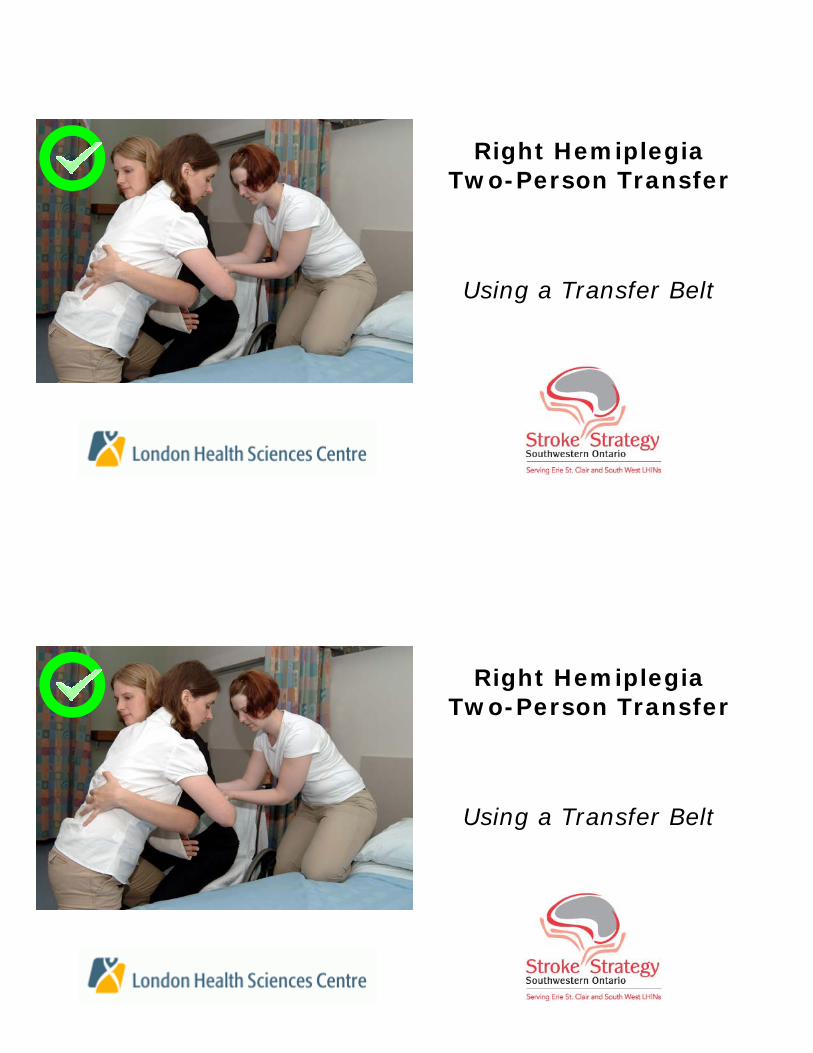
Right Hemiplegia Two-Person Transfer
Using a Transfer Belt
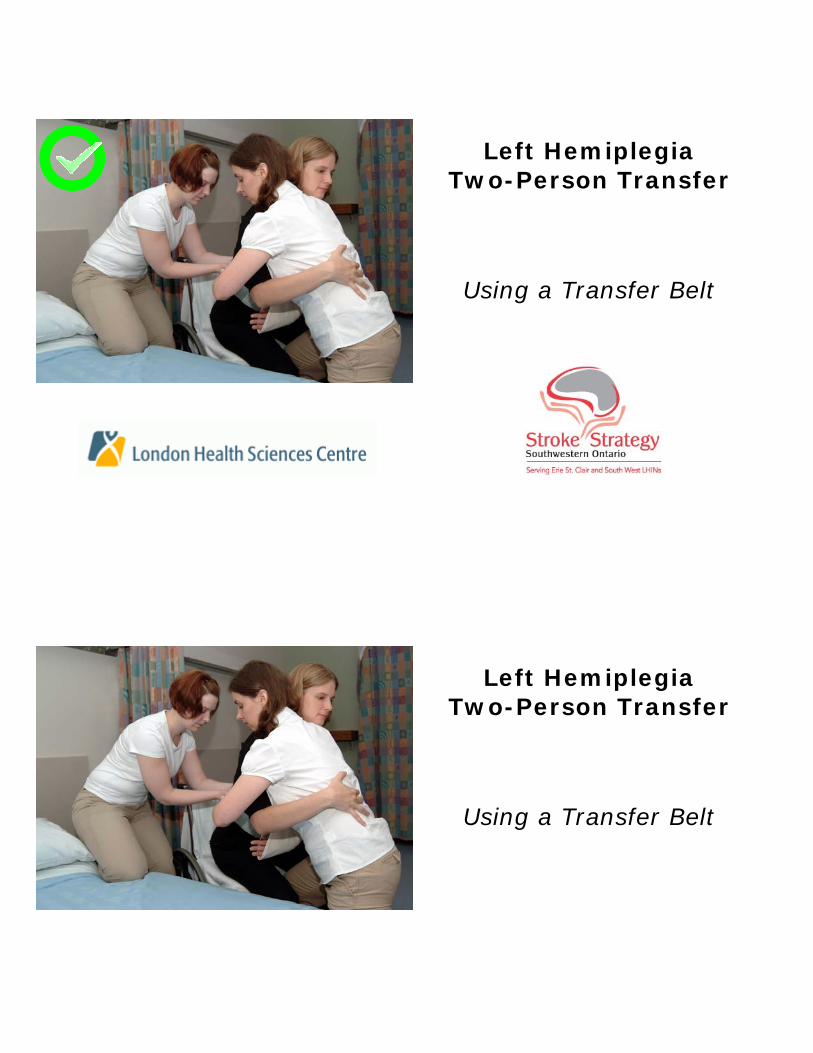
Left Hemiplegia Two-Person Transfer
Using a Transfer Belt
Left Hemiplegia Two-Person Transfer
Using a Transfer Belt
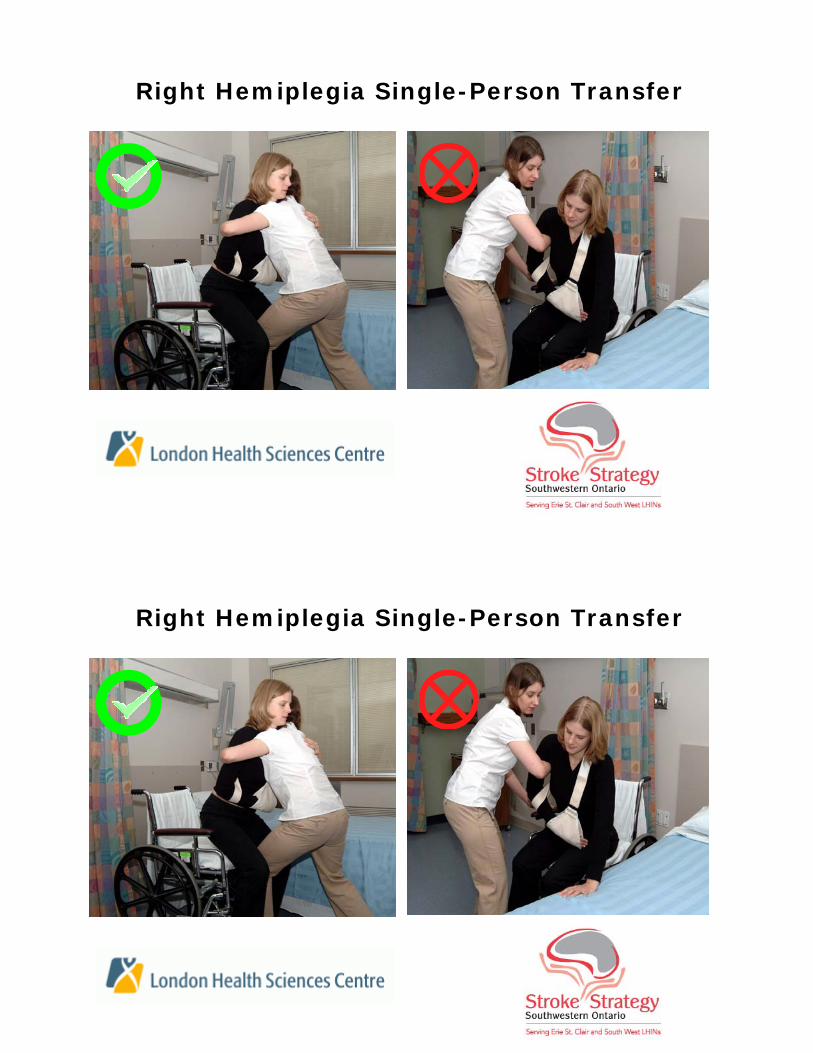
Right Hemiplegia Single-Person Transfer
Right Hemiplegia Single-Person Transfer
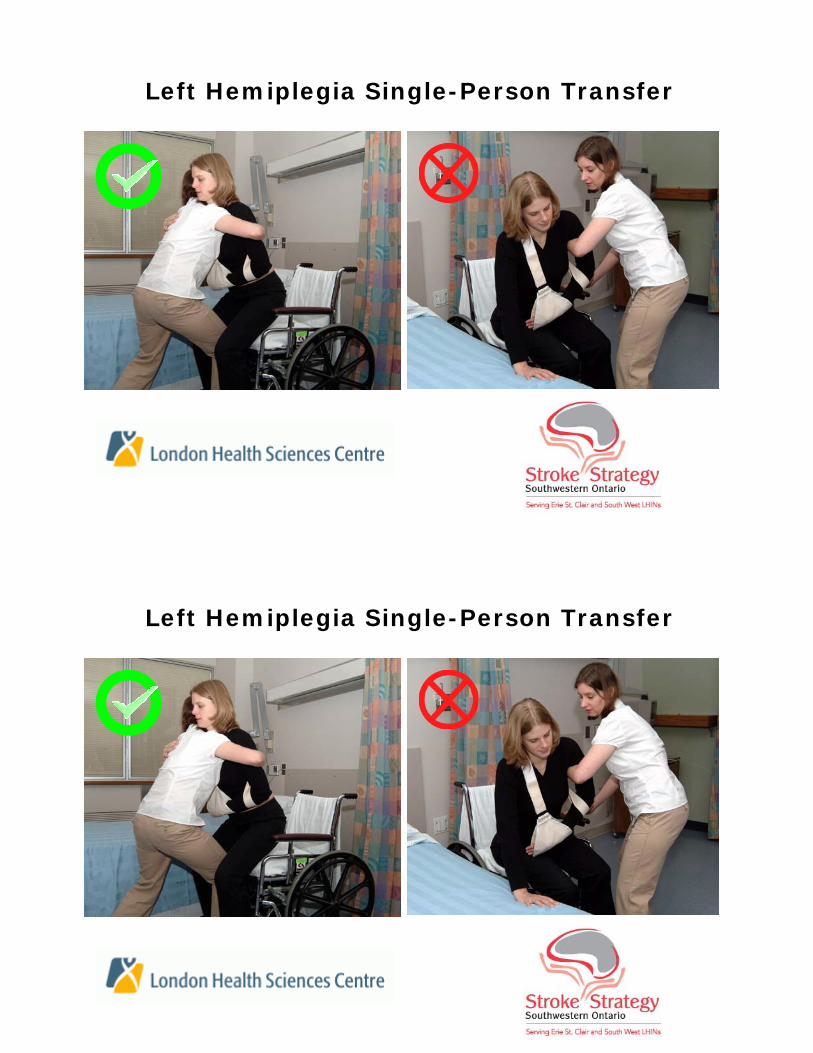
Left Hemiplegia Single-Person Transfer
Left Hemiplegia Single-Person Transfer









![Package ‘arm’ - The Comprehensive R Archive Network · Package ‘arm ’ April 13, 2018 ... Maria Grazia Pittau [ctb], Jouni Kerman [ctb], Tian Zheng [ctb], Vincent Dorie [ctb]](https://img.pdfslide.us/doc/110x75/5af7d0be7f8b9a7444913dbb/package-arm-the-comprehensive-r-archive-network-arm-april-13-2018.jpg)



















