Embed Size (px)
Citation preview

J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8
ª 2 0 1 8 B Y T H E AM E R I C A N C O L L E G E O F C A R D I O L O G Y F O UN DA T I O N
P U B L I S H E D B Y E L S E V I E R
SPECIAL ISSUE: HEART FAILURE WITHPRESERVED EJECTION FRACTION (HFpEF)
JACC: HEART FAILURE EXPERT SCIENTIFIC PANEL
Heart Failure With Preserved EjectionFraction Expert Panel Report
Current Controversies and Implications for Clinical TrialsKishan S. Parikh, MD,a,b Kavita Sharma, MD,c Mona Fiuzat, PHARMD,a,b Howard K. Surks, MD,d Jyothis T. George, MD,e
Narimon Honarpour, MD, PHD,f Christopher Depre, MD, PHD,f Patrice Desvigne-Nickens, MD,g
Richard Nkulikiyinka, MD,h Gregory D. Lewis, MD,i Mardi Gomberg-Maitland, MD, MSC,j
Christopher M. O’Connor, MD,j Norman Stockbridge, MD,k Robert M. Califf, MD,b,l,m Marvin A. Konstam, MD,n
James L. Januzzi, JR, MD,o Scott D. Solomon, MD,p Barry A. Borlaug, MD,q Sanjiv J. Shah, MD,r
Margaret M. Redfield, MD,q G. Michael Felker, MDa,b
JACC: HEART FAILURE CME/MOC
This article has been selected as the month’s JACC: Heart Failure
CME/MOCactivity, available onlineathttp://www.acc.org/jacc-journals-cme
by selecting the JACC Journals CME/MOC tab.
Accreditation and Designation Statement
The American College of Cardiology Foundation (ACCF) is accredited by
the Accreditation Council for Continuing Medical Education (ACCME) to
provide continuing medical education for physicians.
TheACCFdesignates this Journal-basedCME/MOCactivity for amaximum
of 1 AMA PRA Category 1 Credit(s). Physicians should only claim credit
commensurate with the extent of their participation in the activity.
Method of Participation and Receipt of CME/MOC Certificate
To obtain credit for JACC: Heart Failure CME/MOC, you must:
1. Be an ACC member or JACC subscriber.
2. Carefully read the CME/MOC-designated article available online and
in this issue of the journal.
3. Answer the post-test questions. At least 2 out of the 3 questions
provided must be answered correctly to obtain CME/MOC credit.
4. Complete a brief evaluation.
5. Claim your CME/MOC credit and receive your certificate electronically
by following the instructions given at the conclusion of the activity.
CME/MOC Objectives for This Article: Upon completion of this activity, the
learner should be able to: 1) identify key knowledge gaps relevant to
ISSN 2213-1779/$36.00
From the aDuke Clinical Research Institute, Durham, North Carolina; bDuke UncJohns Hopkins University, Baltimore, Maryland; dSanofi, Bridgewater, New
Ingelheim, Germany; fAmgen, Inc., Thousand Oaks, California; gNational In
Institute, Bethesda, Maryland; hBayer AG, Wuppertal, Germany; iMassachus
Heart and Vascular Institute, Falls Church, Virginia; kU.S. Food and Drug Ad
versity, Stanford, California; mVerily Life Sciences, San Francisco, CalifornoBrigham andWomen’s Hospital, Boston, Massachusetts; pHarvardMedical Sch
clinicians, investigators, industry, and regulators in the current HFpEF
field; 2) discuss results of prior HFpEF trials and potential pitfalls of trial
design; and 3) select appropriate strategies to diagnose HFpEF and
identify subpopulations that may fit a targeted therapy.
CME/MOC Editor Disclosure: Editor-in-Chief Christopher M. O’Connor,
MD, has received consultant fees/honoraria from AbbVie, Inc., Actelion
Pharmaceuticals Ltd., Bayer, Bristol Myers Squibb, Cardiorentis,
Merco & Co., Inc., ResMed, and Roche Diagnostics; and ownership
interest in Biscardia, LLC. Executive Editor Mona Fiuzat, PharmD, has
received research support from ResMed, Gilead, Critical Diagnostics,
Otsuka, and Roche Diagnostics. Tariq Ahmad, MD, MPH, has received a
travel scholarship from Thoratec. Abhinav Sharma, MD, has received
support from Bayer-Canadian Cardiovascular Society, Alberta Innovates
Health Solution, Roche Diagnostics, and Takeda. Mitchell Psotka, MD,
PhD, and Kishan Parikh, MD, have no relationships relevant to the
contents of this paper to disclose.
Author Disclosures: Dr. Fiuzat has received personal fees from ResMed
outside the submittedwork. Dr. Surks is an employee of Sanofi. Dr. George
is an employee of Boehringer Ingelheim. Dr. Honarpour is an employee of
Amgen and has received stock grants from Amgen, Inc. Dr. Depre is an
employee of Amgen, Inc. Dr. Nkulikiyinka is an employee and shareholder
of Bayer AG. Dr. Lewis has received grants from Abbott Vascular, Iron-
wood, National Institutes of Health, and American Heart Association; and
is a consultant for Amgen, Luitpold, and Cytokinetics. Dr. Gomberg-
Maitland has received grants and other support from Actelion; personal
fees from Bayer, Acceleron, Medronic, Arena, Merck, St. Jude’s/Abbott,
https://doi.org/10.1016/j.jchf.2018.06.008
iversity School of Medicine, Durham, North Carolina;
Jersey; eBoehringer Ingelheim Clinical Development,
stitutes of Health, National Heart, Lung, and Blood
etts General Hospital, Boston, Massachusetts; jInova
ministration, Silver Spring, Maryland; lStanford Uni-
ia; nTufts Medical Center, Boston, Massachusetts;
ool,Wellesley, Massachusetts; qMayo Clinic, Rochester,

Parikh et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8
Expert Scientific Panel on HFpEF A U G U S T 2 0 1 8 : 6 1 9 – 3 2
620
and Liquidia; other support from Reata and PCORI; grants, personal fees,
and other support from United Therapeutics; grants from AADi; and per-
sonal fees from Janssen during the conduct of the study. Dr. O’Connor has
received personal fees from ResMed, Bayer, Stealth Peptides, Bristol-
Myers Squibb Foundation, Dey, L.P., and Merck outside the submitted
work. Dr. Califf served as Commissioner for Food and Drugs at the U.S.
Food and Drug Administration from 2016 to 2017 and as Deputy Commis-
sioner forMedical Products and Tobacco from 2015 to 2016; is employed as
a scientific advisor by Verily Life Sciences (Alphabet); has received stock
from Verily Life Sciences; is a consultant for Merck, Amgen, and Boeh-
ringer Ingelheim; and receives consulting payments from Merck.
Dr. Konstam has received other support from Amgen, Bristol-Myers
Squibb, Boehringer Ingelheim, andNovartis; and grants and other support
from Ironwood and Livanova outside the submitted work. Dr. Januzzi has
received grants from Roche Diagnostics, Abbott, Singulex, Prevencio, and
Novartis; grants and personal fees from Janssen; and personal fees from
Critical Diagnostics outside the submitted work. Dr. Solomon has received
grants and personal fees from Novartis, AstraZeneca, Bayer, Bristol-Myers
Squibb, Alnylam, GlaxoSmithKline, Myokardia, and Amgen; grants from
Ionis; and personal fees from Corvia, Roche, and Merck outside the sub-
Minnesota; and rNorthwestern University, Chicago, Illinois. Dr. Fiuzat ha
submitted work. Dr. Surks is an employee of Sanofi. Dr. George is an emp
employee of Amgen and has received stock grants from Amgen, Inc. Dr. Dep
an employee and shareholder of Bayer AG. Dr. Lewis has received grants fro
Health, and American Heart Association; and is a consultant for Amgen, Lu
received grants and other support from Actelion; personal fees from Bayer, A
and Liquidia; other support from Reata and PCORI; grants, personal fees, a
from AADi; and personal fees from Janssen during the conduct of the stu
ResMed, Bayer, Stealth Peptides, Bristol-Myers Squibb Foundation, Dey, L.P
served as Commissioner for Food and Drugs at the U.S. Food and Drug
Commissioner for Medical Products and Tobacco from 2015 to 2016; is emp
(Alphabet); has received stock from Verily Life Sciences; is a consultant for Me
consulting payments from Merck. Dr. Konstam has received other suppo
Ingelheim, and Novartis; and grants and other support from Ironwood and L
received grants from Roche Diagnostics, Abbott, Singulex, Prevencio, and N
personal fees from Critical Diagnostics outside the submitted work. Dr. So
Novartis, AstraZeneca, Bayer, Bristol-Myers Squibb, Alnylam, GlaxoSmithKl
personal fees from Corvia, Roche, and Merck outside the submitted work. Dr
the National Institutes of Health (R01 HL107577, R01 HL127028), the Am
#15CVGPSD27260148), Actelion, AstraZeneca, Corvia, and Novartis; and co
Bayer, Boehringer Ingelheim, Cardiora, Eisai, Ironwood, Merck, Novartis, Sa
received grant funding from National Heart, Lung, and Blood Institute, Am
netics, Merck, and Roche Diagnostics; and consulting for Novartis, Amgen,
GlaxoSmithKline, Cardionomic, Cytokinetics, Myokardia, Stealth, Innolife, an
they have no relationships relevant to the contents of this paper to disclose
this paper.
Manuscript received April 6, 2018; revised manuscript received June 20, 20
mitted work. Dr. Shah has received receiving research funding from the
National Institutes of Health (R01 HL107577, R01 HL127028), the American
Heart Association (#16SFRN28780016 and #15CVGPSD27260148), Actelion,
AstraZeneca, Corvia, and Novartis; and consulting fees from Actelion,
Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Cardiora, Eisai, Iron-
wood,Merck, Novartis, Sanofi, Tenax, andUnited Therapeutics. Dr. Felker
has received grant funding from the National Heart, Lung, and Blood
Institute, American Heart Association, Novartis, Amgen, Cytokinetics,
Merck, and Roche Diagnostics; and consulting for Novartis, Amgen, Roche
Diagnostics, Medtronic, Bristol-Myers Squibb, GlaxoSmithKline, Car-
dionomic, Cytokinetics,Myokardia, Stealth, Innolife, andEBRSystems.All
other authors have reported that they haveno relationships relevant to the
contents of this paper to disclose.
Medium of Participation: Print (article only); online (article and quiz).
CME/MOC Term of Approval
Issue date: August 2018
Expiration date: July 31, 2019
s received personal fees from ResMed outside the
loyee of Boehringer Ingelheim. Dr. Honarpour is an
re is an employee of Amgen, Inc. Dr. Nkulikiyinka is
m Abbott Vascular, Ironwood, National Institutes of
itpold, and Cytokinetics. Dr. Gomberg-Maitland has
cceleron, Medronic, Arena, Merck, St. Jude’s/Abbott,
nd other support from United Therapeutics; grants
dy. Dr. O’Connor has received personal fees from
., and Merck outside the submitted work. Dr. Califf
Administration from 2016 to 2017 and as Deputy
loyed as a scientific advisor by Verily Life Sciences
rck, Amgen, and Boehringer Ingelheim; and receives
rt from Amgen, Bristol-Myers Squibb, Boehringer
ivanova outside the submitted work. Dr. Januzzi has
ovartis; grants and personal fees from Janssen; and
lomon has received grants and personal fees from
ine, Myokardia, and Amgen; grants from Ionis; and
. Shah has received receiving research funding from
erican Heart Association (#16SFRN28780016 and
nsulting fees from Actelion, Amgen, AstraZeneca,
nofi, Tenax, and United Therapeutics. Dr. Felker has
erican Heart Association, Novartis, Amgen, Cytoki-
Roche Diagnostics, Medtronic, Bristol-Myers Squibb,
d EBR Systems. All other authors have reported that
. Barry H. Greenberg, MD, served as Guest Editor for
18, accepted June 20, 2018.

J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8 Parikh et al.A U G U S T 2 0 1 8 : 6 1 9 – 3 2 Expert Scientific Panel on HFpEF
621
Heart Failure With Preserved Ejection FractionExpert Panel Report
Current Controversies and Implications for Clinical Trials
Kishan S. Parikh, MD,a,b Kavita Sharma, MD,c Mona Fiuzat, PHARMD,a,b Howard K. Surks, MD,d Jyothis T. George, MD,e
Narimon Honarpour, MD, PHD,f Christopher Depre, MD, PHD,f Patrice Desvigne-Nickens, MD,g
Richard Nkulikiyinka, MD,h Gregory D. Lewis, MD,i Mardi Gomberg-Maitland, MD, MSC,j
Christopher M. O’Connor, MD,j Norman Stockbridge, MD,k Robert M. Califf, MD,b,l,m Marvin A. Konstam, MD,n
James L. Januzzi, JR, MD,o Scott D. Solomon, MD,p Barry A. Borlaug, MD,q Sanjiv J. Shah, MD,r
Margaret M. Redfield, MD,q G. Michael Felker, MDa,b
ABSTRACT
The number of persons with heart failure has continued to rise over the last several years. Approximately one-half of
those living with heart failure have heart failure with preserved ejection fraction, but critical unsolved questions remain
across the spectrum of basic, translational, clinical, and population research in heart failure with preserved ejection
fraction. In this study, the authors summarize existing knowledge, persistent controversies, and gaps in evidence with
regard to the understanding of heart failure with preserved ejection fraction. Our analysis is based on an expert panel
discussion “Think Tank” meeting that included representatives from academia, the National Institutes of Health, the U.S.
Food and Drug Administration, the Centers for Medicare & Medicaid Services, and industry. (J Am Coll Cardiol HF
2018;6:619–32) © 2018 by the American College of Cardiology Foundation.
A pproximately 6.5 million American adults areestimated to have heart failure (HF), and thenumber of persons is projected to increase
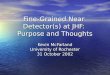
46% by 2030 (1); approximately one-half of these pa-tients have heart failure with preserved ejection frac-tion (HFpEF) (2). Perhaps the most agreed-uponcharacteristic of HFpEF is that a better understandingis needed. Critical unsolved questions remain acrossthe spectrum of basic, translational, clinical, and pop-ulation research in HFpEF. In particular, it remainsunknown whether the term HFpEF applies to a singledisease state or multiple diseases that are character-ized by unique underlying pathophysiologic mecha-nisms. In this expert panel report, we identify gapsin evidence with regard to the understanding ofHFpEF in 3 pivotal areas: 1) definition of thedisease; 2) subtypes of HFpEF; and 3) endpoints inHFpEF clinical trials. Our analysis is based on anexpert panel discussion “Think Tank” meeting thatwas hosted by the Duke Clinical Research Institutein Washington, DC, in June 2017, which includedrepresentatives from academia, the NationalInstitutes of Health, the U.S. Food and DrugAdministration, the Centers for Medicare &Medicaid Services, and industry. In the followingdiscussion, we approach critical HFpEF issues froma variety of perspectives in hopes of elucidatingcommon themes and offering a potential future
roadmap for improved HFpEF care (CentralIllustration). To focus our discussion and avoidoverlap with different disease processes, we do notaddress the HF patient populations with mid-rangeejection fraction (EF) (i.e., 40% to 49%) orrecovered EF while considering these issues.
IS HFpEF A SINGLE ENTITY?
Challenges associated with HFpEF begin with itsdefinition. HFpEF is usually diagnosed afterexcluding noncardiac causes of dyspnea that canmimic HF, and alternate established diseases with leftventricular EF >50% causing HF symptoms (e.g.,constrictive pericarditis, infiltrative cardiomyopa-thies, isolated right-sided HF, valvular heart disease,non–group 2 pulmonary hypertension [PH]) (3). Earlystudies of HFpEF focused on 1 or 2 predominantmechanistic pathways, such as diastolic dysfunction(4,5); however, subsequent key studies demonstratedthat not only was diastolic dysfunction not ubiqui-tously present on resting echocardiography in HFpEF,but several other mechanisms were likely implicated,including atrial dysfunction, systolic impairment,ventricular-vascular stiffening, and chronotropicincompetence (6–8). As a result, the definition ofHFpEF has evolved over the last 2 decades, movingaway from a primary focus on echocardiographic

ABBR EV I A T I ON S
AND ACRONYMS
BNP = B-type natriuretic
peptide
EF = ejection fraction
HF = heart failure
HFpEF = heart failure with
preserved ejection fraction
HFrEF = heart failure with
reduced ejection fraction
PAH = pulmonary arterial
hypertension
PH = pulmonary hypertension
QOL = quality of life
Parikh et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8
Expert Scientific Panel on HFpEF A U G U S T 2 0 1 8 : 6 1 9 – 3 2
622
evidence of diastolic dysfunction in thesetting of an EF $50%, and moving toward adefinition inclusive of (but not restricted to)cardiac structural abnormalities resultingfrom high filling pressures, diastolic abnor-malities, elevated biomarkers, and elevatedleft heart filling pressures by invasive he-modynamic assessment (4,9). Despite het-erogeneous contribution of putativepathomechanisms, HFpEF patients do havecommon patterns of clinical presentation,such as impaired exercise tolerance orphysical limitations in activities of dailyliving. Furthermore, EF $50% remains adefining feature in HFpEF, as illustrated by
variability in patient characteristics and outcomes byEF observed in the TOPCAT (Treatment of PreservedCardiac Function Heart Failure with an AldosteroneAntagonist) trial of spironolactone (10) and similardifferential beta-blocker effects in subjects withEF <40%, 40% to 49%, and $50% (11).
Consequently, there is controversy about whetherHFpEF patients respond similarly to interventions ornot. How HFpEF should be categorized has over-arching implications for future treatment goals andapproaches to drug development, and both perspec-tives are discussed next.
YES, HFpEF IS A SINGLE-DISEASE ENTITY. A singledisease can be defined by a phenotype or constella-tion of signs, biomarkers, and symptoms that sharea common denominator (12). Left ventricular diastolicdysfunction is a common denominator among HFpEFpatients, but varying degrees of other pathophysio-logic components are observed, including abnormal-ities in left ventricular systolic function, conduitvessel stiffening, pulmonary vascular disease, rightventricular function, microvascular function, skeletalmuscle function, and changes in body composition.A key unanswered question is whether these differ-ential expressions arise from a common mechanism,or whether they are caused by different discreteprocesses. Paulus and Tschöpe (13) proposed a uni-fying hypothesis that is consistent with the formerscheme: an underlying proinflammatory state (causedby 1 or more of the commonly associated comorbidconditions in HFpEF, including obesity, diabetes,and hypertension) triggers a cascade of events thatleads to decreased nitric oxide bioavailability,cyclic guanosine monophosphate, and protein kinaseG activity, thereby causing increased cardiomyo-cyte stiffness (due to titin hypophosphorylation)and/or interstitial myocardial fibrosis, and increased
ventricular wall stiffness. In this model, HFpEF ismediated by endothelial dysfunction involvingboth arterial and venous systems, in contrast toprimary myocardial injury caused by cardiomyocyteloss as in HF with reduced EF (HFrEF). This patho-physiology provides a distinct potential therapeutictarget for new drug candidates that can be developedto modify disease course.
NO, HFpEF COMPRISES MANY DIFFERENT DISEASES.
However, the Paulus and Tschöpe (13) hypothesisis weakened by prior negative trials of statins,renin-angiotensin-aldosterone system inhibition,and phosphodiesterase-5 inhibitors—therapies thatshould stabilize vascular inflammation and promoteendothelial function. Contrasting to the theorythat HFpEF may result from a single underlyingcause is the possibility that HFpEF is a multiorgandisease resulting from not only primary cardiacabnormalities, but also noncardiac comorbiditiesimplicated in the development of clinical HF.These noncardiac conditions may have independentmechanistic implications that do not all result in acommon pathway of inflammation and subsequentmyocardial damage. Limitations in systolic reserve,vascular function, nitric oxide bioavailability, leftatrial function, chronotropic incompetence, changesin body composition, skeletal muscle function, andother mechanisms (all of which have been assessedby hemodynamic, imaging, and biomarker studies)have been associated with HFpEF (6). Many of theseperturbations occur with aging and, therefore, age-associated changes in cardiovascular structure andfunction become “partners” with pathophysiologicaldisease mechanisms to determine the threshold,severity, and prognosis of HFpEF (14). Additionalinfluential factors have been explored. For example,obesity (84% prevalence in a U.S. HFpEF population)has a U-shaped relationship with survival, as it doesin HFrEF patients (15), and displays unique patho-physiological features compared with those foundin nonobese HFpEF patients (16); furthermore, weightloss in obese patients with HFpEF improves peakoxygen consumption (17). Other factors influencingHFpEF severity include hypertension ($80%), dia-betes mellitus (20% to 45%), chronic lung disease,atrial fibrillation, and chronic kidney disease.The complexity of interactions between HFpEF andcomorbid conditions complicates development ofa universal HFpEF animal model. Instead, currentHFpEF animal models recapitulate isolated featuresof HFpEF. The ability of an animal model toprovide pathophysiological insights and predict

CENTRAL ILLUSTRATION Key Questions With Critical Gaps Identified in HFpEF
Parikh, K.S. et al. J Am Coll Cardiol HF. 2018;6(8):619–32.
HFpEF ¼ heart failure with preserved ejection fraction; HFrEF ¼ heart failure with reduced ejection fraction.
J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8 Parikh et al.A U G U S T 2 0 1 8 : 6 1 9 – 3 2 Expert Scientific Panel on HFpEF
623

TABLE 1 Summary of Major Published HFpEF Randomized Clinical Trials (Phase 2–3)
Drug/Intervention(Ref. #) Phase Study Size Primary Endpoint Result
Candesartan (31) 3 3,023 Composite of cardiovascular mortality or HF hospitalization Neutral
Irbesartan (30) 3 4,128 Composite of all-cause mortality or cardiovascular hospitalization Neutral
Perindopril (29) 3 850 Composite of all-cause mortality and HF hospitalization Neutral
Nebivolol (60) 3 752 Composite of all-cause mortality or cardiovascular hospitalization Neutral
Carvedilol (61) 2 245 Composite of cardiovascular mortality or HF hospitalization Neutral
Digoxin (62) 3 988 Composite of HF mortality or HF hospitalization Neutral
Spironolactone (63) 2 422 E/e’ on echocardiography; peak oxygen consumption Positive; neutral
Spironolactone (64) 3 3,445 Composite of death from cardiovascular cause, aborted cardiac arrest,or HF hospitalization
Neutral
Eplerenone (65) 2 44 6-min-walk distance Neutral
Sildenafil (66) 2 216 Peak oxygen consumption Neutral
Ivabradine (67) 2 61 Exercise capacity/peak oxygen consumption Positive
Ivabradine (68) 2 44 Peak oxygen consumption Negative
Ivabradine (69) 2 179 E/e’ on echocardiography; 6-min-walk distance; NT-proBNP Neutral; neutral;neutral
Exercise training (70) N/A 64 Peak oxygen consumption Positive
Sacubitril/valsartan (71) 2 301 NT-proBNP Positive
Vericiguat (72) 2 477 NT-proBNP; left atrial volume Neutral; neutral
Isosorbide mononitrate (57) 2 110 Daily activity level Negative
HF ¼ heart failure; HFpEF ¼ heart failure with preserved ejection fraction; NT-proBNP ¼ N-terminal pro–B-type natriuretic peptide.
Parikh et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8
Expert Scientific Panel on HFpEF A U G U S T 2 0 1 8 : 6 1 9 – 3 2
624
human HFpEF therapeutic response to preclinicalintervention testing is uncertain (18).
Therefore, evidence exists on both sides, but it isincreasingly accepted that the clinical presentationof HFpEF is influenced to varying degrees by morethan 1 physiological perturbation or risk factor.Relative influences of contributing etiologies andpossible links between them must be better under-stood at both individual and population levels. Theapplicability of animal models to human HFpEF re-mains a matter of controversy and requires furtherstudy.
IS A CLINICALLY BASED SCHEME THE RIGHT
APPROACH TO HFpEF CLASSIFICATION?
Regardless of whether HFpEF is a single disease or acommon presentation of multiple pathophysiologicalprocesses, the condition encompasses a broad spec-trum of clinical phenotypes. The need to categorizepatients is increasingly evident as the disease burdengrows, with more therapeutic interventions beingstudied and failing. Merits of various methods ofclassification, including pathophysiologic, etiologic,clinical presentation, and phenomapping, have beenpreviously explored (19) and reveal several possiblefuture directions. We believe whatever scheme isdeveloped should be flexible (i.e., have the capacityto adapt to new findings) and practical (i.e., can be
classified in a variety of settings), with the goalof driving specific therapies in distinct subgroups.With this in mind, we must consider the initialbroad distinction of a clinically versus mechanisti-cally based classification scheme in HFpEF.
YES, HFpEF CLASSIFICATION SHOULD BE CLINICALLY
ORIENTED. There are basically 2 approaches that canbe used together. One is hypothesis-driven based onclinical observations. HFpEF patients are divided intophenotypes, such as obese HFpEF/HFpEF with pul-monary vascular disease/HFpEF with arterial stiff-ening/HFpEF with endothelial dysfunction. Anotheris an agnostic, machine-learning approach where thecomputer identifies groups that differ to create clin-ical groups. Integration of both approaches and useof both inductive- and reductionist-type approachesis needed. Relative contributions of cardiac andvascular etiologies could be quantified in thismanner.
NO, HFpEF CLASSIFICATION SHOULD BE BASED ON
MECHANISTIC PATHWAYS. Using identified mecha-nistic processes to categorize HFpEF patients mayprovide opportunities to study targeted therapeutics(20). In contrast to focusing on clinical presentation,a system detailing specific, underlying biologicprocesses can assess the specific pathophysiologicalfactors contributing to a patient’s HFpEF diseaseburden. Lewis et al. (20) have recently proposedinclusion of dysfunction in vascular beds, kidneys,

J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8 Parikh et al.A U G U S T 2 0 1 8 : 6 1 9 – 3 2 Expert Scientific Panel on HFpEF
625
mitochondrial function, calcium handling, and car-diac diastole, among others. However, many of theseHFpEF variables are dynamic, so routine measure-ment followed by synthesis seems to be a formidabletask. Even in the case of HFrEF, these underlyingmechanisms may or may not be accurate or sufficientto pinpoint a specific disease entity.
The previous discussion suggests that furthercomparisons of clinically and biologically based clas-sifications are needed. An alternative way to viewHFpEF clinical/biologic phenotypes is to look throughdifferent lenses into this complex syndrome. Forexample, we are just beginning to examine variationin presentation and outcomes by sex, race, ethnicity,socioeconomic factors, hemodynamics, biomarkers,imaging, or responses to physiologic perturbations,such as exercise (21,22). Techniques, such as machinelearning, that can integrate data from various sourcesmay lead to discovery of biologically distinct pheno-types and potentially differentiate responsiveness totherapy. However, ultimately machine learning isonly as good as the input variables, and if the criticalpathophysiologic features that drive HFpEF are notdirectly or indirectly represented within the inputvariables, the analysis can be unhelpful or evenmisleading.
SHOULD CLINICAL TRIALS CONTINUE TO
ADDRESS ALL HFpEF SIMILARLY?
To date, randomized trials of a variety of potentiallypromising interventions have been unable todemonstrate a definitive benefit in HFpEF patients(Table 1). What is unclear is whether this lack ofdemonstrative benefit was caused by failed trialdesigns or inefficacious study interventions. A clin-ical trial that results in negative findings is certainlynot a failure because knowledge is obtained fromthese results, but negative findings resulting from apotential therapy compel us to reconsider clinicaltrial design in the context of prior efforts in HFpEF. Inthe following 2 sections, we consider 2 divergent ap-proaches to identifying appropriate HFpEF clinicaltrial populations to maximize the chances of finding atherapeutic intervention: 1) trials that would includea broad group of subjects; and 2) trials that wouldbe smaller, focusing on individual subpopulations.
YES, HFpEF CLINICAL TRIALS SHOULD INCLUDE A
BROAD GROUP OF SUBJECTS. When compared withobservational registries and epidemiological studies,patients included in HFrEF clinical trials are often atlower risk for adverse outcomes, largely because theeligibility criteria for HFrEF trials in general exclude
the sickest patients (e.g., the very elderly and thosewith advanced chronic kidney disease, frailty,high-risk comorbidities). The standard therapeuticHFrEF treatment regimen (including newer agents)has been built on large randomized controlled trials,and consequently, many HFrEF patients have seensignificant improvements in survival and other HFoutcomes including hospitalizations. In HFrEF,diverse etiologic categories (i.e., ischemic and non-ischemic dilated cardiomyopathies) have showngenerally similar therapeutic responses to neurohu-moral antagonists.
To date, HFpEF clinical trials have also adoptedbroad inclusion criteria. Ensuring adequate statisticalpower to detect signals may be especially important inHFpEF trials, given the many comorbid conditions inHFpEF, which may influence clinical endpointsbeyond HF severity and therapeutic effect. Targetingtrials to specific phenotypes posited to respond tothe tested intervention may increase the ability toidentify efficacy, but this approach may also limitability to enroll enough patients for a sufficientlypowered trial.
Enrichment strategies must be assessed carefully.Many HFrEF outcome trials have enriched a broadHFrEF population for event rates by requiringelevated natriuretic peptide assays for enrollment toenhance power with a smaller study size. Similarly,HFpEF studies have commonly required elevatedBNP levels to ensure participants have HF andto enrich event rates. Although B-type natriureticpeptide (BNP) levels are prognostic in HFpEF (23),numerous studies have shown that BNP levels inHFpEF are lower than in HFrEF for any given HFseverity and that a significant proportion of HFpeFpatients do not have elevated BNP assay levels(24,25). Further, post hoc analyses from 2 clinicaltrials, I-PRESERVE (Irbesartan in Heart Failure WithPreserved Systolic Function) and TOPCAT, showedactive therapy (irbesartan or spironolactone) wasassociated with treatment benefit in subjects withlower natriuretic peptide levels, but not in subjectswith higher levels (26,27). These observations maychallenge the common practice of using natriureticpeptide assays to enrich HFpEF trials for event rates.
NO, HFpEF CLINICAL TRIALS NEED TO BE NARROWER
AND FOCUSED ON INDIVIDUAL SUBPOPULATIONS. For aHFpEF trial to be successful, the right patientsneed to be matched to the therapies from whichthey are most likely to benefit. Even in HFrEF,certain therapies (cardiac resynchronization therapyand defibrillators) are helpful only in specific HFrEFphenotypes. A large number of ongoing HFpEF

TABLE 2 Representative Summary of Registered Current and Upcoming Clinical Trials for HFpEF at Time of Publication
Study (Intervention) Phase Target HFpEF Population Primary Outcomes
CAPACITY-HFpEF (IW-1973, solubleguanylate cyclase stimulator)
2 EF $45%Peak VO2 <80% predicted
Peak VO2
6-min-walk
SPIRRIT (spironolactone) 4 EF $40% MortalityHF hospitalization
SERENADE (macitentan) 2 EF $40%Pulmonary vascular disease or right
heart failure
Natriuretic peptides
PARAGON-HF (sacubitril/valsartan) 3 EF $45% Cumulative events of CV death and total HFhospitalizations
DYNAMIC (riociguat) 2 EF $50%Pulmonary hypertension
HemodynamicsMRI parameters
PARALLAX (sacubitril/valsartan) 3 EF $45%KCCQ summary score <75
Natriuretic peptidesQuality of life
VITALITY-HFpEF (vericiguat) 2 EF $45% Quality of life
SOUTHPAW (oral treprostinil) 3 EF $45%Pulmonary hypertension
6-min-walk
KNO3CK OUT HFpEF (potassium nitrate) 2 EF >50% Peak VO2
EMPEROR-PRESERVED (empagliflozin) 3 EF >40% Time to CV death or HF hospitalization
OPTIMIZE-HFPEF(screening/treatment of comorbidities)
3 EF $50%Age >60 yrs
Composite including quality of life
FAIR-HFpEF (ferric carboxymaltose) 2 EF $45%Diastolic dysfunctionIron deficiency
Exercise capacity6-min-walk
CELLpEF (cell therapy) 2 EF >50%Diastolic dysfunction
Diastolic function by MRIExercise capacity
PH-HFpEF (sodium nitrite) 2 EF $40%Pulmonary hypertension
Exercise hemodynamics6-min-walk
Neladenoson bialanate 2 EF $45% 6-min-walk
CoQ10 and D-ribose 2 EF $50% Quality of life
Nebivolol 4 Pulmonary hypertension Hemodynamics6-min-walk
ONOH (sodium nitrite) 2 EF $40%Age $70 yrs
Peak VO2
INABLE (inhaled sodium nitrite) 2 EF $50% Peak VO2
PRESERVED-HF (dapagliflozin) 4 EF $45%Diabetes mellitus type 2
Natriuretic peptides
Levosimendan 2 Pulmonary hypertension Exercise hemodynamics
CRpEF (cardiac rehabilitation) 3 EF $50%Moderate/severe diastolic dysfunctionAge $50 yrs
Peak VO2
Continued on the next page
Parikh et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8
Expert Scientific Panel on HFpEF A U G U S T 2 0 1 8 : 6 1 9 – 3 2
626
studies are testing interventions that target uniquemechanistic hypotheses (Table 2) but are not neces-sarily targeting specific subphenotypes selected to beuniquely responsive to the tested therapeutic. Po-tential HFpEF subpopulations that may have uniquepathophysiology and potential response to targetedtherapies are described next, and include: 1) at-risk/metabolic disorders; 2) pulmonary vascular disease;and 3) elevated left atrial pressure.Subpopulat ion : at - r i sk/metabol i c d i sorders . It ispossible that prevention, or delay in progression,of HFpEF may be effective in high-risk populations.Prior studies of neurohormonal modulators in overtHFpEF populations have demonstrated overall neutralfindings for beta-blockers (11,28) and angiotensin-converting enzyme inhibitor-I/angiotensin receptor
blocker therapy (29–31). Yet findings from theRENAAL (Reduction of Endpoints in Non–Insulin-Dependent Diabetes Mellitus with the Angiotensin IIAntagonist Losartan) and HOPE (Heart OutcomesPrevention Evaluation) trials showed that renin-angiotensin-aldosterone system inhibition reducedincident HF in patients with risk factors for cardio-vascular events (32,33). However, the type of HFprevented was not assessed in these studies. InALLHAT (Antihypertensive and Lipid-LoweringTreatment to Prevent Heart Attack Trial), which diddefine the type of HF participants developed, chlor-thalidone was superior to lisinopril in reducing inci-dent HFpEF (34). More recently, 2 studies of differentsodium-glucose cotransporter-2 inhibitors showedreduced HF (type unknown) incidence in patients

TABLE 2 Continued
Study (Intervention) Phase Target HFpEF Population Primary Outcomes
PERSPECTIVE (sacubitril/valsartan) 3 EF $40% Cognitive score
PIROUETTE (pirfenidone) 2 EF $45%Myocardial fibrosis
MRI myocardial extracellular volume fraction
ERADICATE-HF (ertugliflozin) 2 EF $20% (HFrEF and HFpEF)Diabetes mellitus type 2
Proximal tubule sodium reabsorption
REDUCE LAP-HF II (interatrial shuntdevice)
N/A EF $40%Age >40 yrsElevated left atrial pressure
CV mortality or strokeQuality of life
Regress-HFpEF (allogeneic-derivedcells)
2 EF $50%Age $50 yrs
Quality of lifeExercise hemodynamics
PERFECTUS (biventricular pacemaker) N/A EF $50%Chronotropic incompetence
Diastolic function
WTLSSCHF (weight loss) N/A EF $45%BMI >30 kg/m2
6-min-walkQuality of life
RAPID-HF (atrial pacing) N/A EF $50%Chronotropic incompetence
Peak VO2
BEAT-HFpEF (albuterol) 2 EF $50%Elevated LV filling pressures
Exercise hemodynamics
INDIE-HFpEF (inorganic nitrite) 2 EF $50%Age $40 yrsPeak VO2 #75% predicted
Peak VO2
ROPA-DOP (diuretics strategy anddopamine)
4 EF >50%Acute HF
Renal function
Levosimendan, calcium sensitizer/K-ATPactivator
2 EF $40%Pulmonary hypertension
Exercise hemodynamics
TROPHY 2 (pulmonary arterydenervation)
2 EF $40%Pulmonary hypertension
Exercise hemodynamics
This list is not intended to be comprehensive.
BMI¼ body mass index; CV ¼ cardiovascular; EF ¼ ejection fraction; HFrEF ¼ heart failure with reduced ejection fraction; KCCQ ¼ Kansas City Cardiomyopathy Questionnaire;LV ¼ left ventricular; MRI ¼ magnetic resonance imaging; N/A ¼ not applicable; VO2 ¼ oxygen consumption; other abbreviations as in Table 1.
J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8 Parikh et al.A U G U S T 2 0 1 8 : 6 1 9 – 3 2 Expert Scientific Panel on HFpEF
627
with diabetes with known cardiovascular disease(35,36). Two HF prevention trials using natriureticpeptide screening of patients with clinical cardiovas-cular risk factors to target cardiovascular specialistevaluation and management showed reduction innew systolic or diastolic dysfunction and HF (37)and HF (type unknown) incidence (38). HF guidelinesnow endorse use of natriuretic peptide assays totarget patients for HF prevention interventions (39).Assessing the impact of these types of preventiveinterventions on HFpEF versus HFrEF will be animportant endeavor moving forward.
Obesity, an important risk factor for HFpEF, mayrepresent another target for prevention and/or treat-ment. In 1 center’s experience, several novel mecha-nistic differences in obese versus nonobese HFpEFpatients were demonstrated, suggesting the potentialfor obesity-specific therapies in this large HFpEFsubgroup (16).Subpopulat ion : pu lmonary vascu lar d isease .Many HFpEF patients have PH (40,41), which isassociated with increased symptom burden, hospi-talizations, and mortality (42,43) and unique histo-pathology (44). A subgroup analysis of an implantablepulmonary artery pressure monitor for patients with
HF demonstrated that pulmonary artery pressure–guided HF therapy was associated with improve-ments in hemodynamics and the composite endpointof HF hospitalization/death in HFpEF (45). Thesmaller cohort of patients with HFpEF and combinedpre- and post-capillary PH (Table 3) is receivingincreasing attention as a possible population tobenefit from pulmonary vasodilator therapy (43,46).Nonetheless, this enthusiasm is tempered by cautionrelated to inducing pulmonary edema in patients withsignificant pulmonary venous hypertension, andprior negative trial results of pulmonary vasodilatorsin HF populations (47). However, the RELAX (Phos-phodiesterase-5 Inhibition to Improve Clinical Statusand Exercise Capacity in Diastolic Heart Failure)study did not specifically target HFpEF PH, and pul-monary pressures were not invasively measured. Asmaller randomized trial of sildenafil in patients withHFpEF PH reported improvements in right heartfunction (48), which is the central determinant of PHoutcomes, but, these right heart function improve-ments could not be confirmed in subsequenttrials (49,50).
Although routine use of pulmonary arterial hy-pertension (PAH) therapies is not recommended, the

TABLE 3 Hemodynamic Distinction Within Pulmonary Hypertension as Pre-Capillary, Isolated Post-Capillary, or Combined Pre- and Post-Capillary Has
Important Implications for Management
PH Subgroup mPAP PCWP PVR Other Therapeutic Targets Clinical Trial Implications
Pre-capillary PH
Typical PAH $25 mm Hg #15 mm Hg >3 Wood units PH; right ventricle
Atypical PAH $25 mm Hg #15 mm Hg >3 Wood units With multiple risk factorsfor left heart disease*or elevation in PCWPexclusively duringstress
PH; right ventricle;consider HFpEF
Growing population; morediscriminatory tools/phenotyping neededbecause PAH and HFpEFsymptoms overlap
Isolated post-capillary PH
$25 mm Hg >15 mm Hg #3 Wood units Some may have PCWPelevation duringstress
HFpEF
Combined pre- andpost-capillary PH
$25 mm Hg >15 mm Hg >3 Wood units HFpEF; right ventricle;consider PH
Ongoing studies to evaluatePH treatment; may havea differentpathophysiology frompre-capillary; carefulphenotyping needed
*Risk factors include coronary artery disease, hypertension, diabetes/metabolic syndrome, obesity, and atrial fibrillation.mPAP ¼ mean pulmonary artery pressure; PAH ¼ pulmonary arterial hypertension; PCWP ¼ pulmonary capillary wedge pressure; PH ¼ pulmonary hypertension; PVR ¼ pulmonary vascular
resistance; other abbreviations as in Table 1.
Parikh et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8
Expert Scientific Panel on HFpEF A U G U S T 2 0 1 8 : 6 1 9 – 3 2
628
question of pulmonary vasodilator use in a subsetof the HFpEF PH population remains open(42,47,51). Furthermore, registry data and clinicaltrial demographics over the last several years sug-gest that the overall PAH population is getting olderwith more comorbidities (52–54). Sometimesreferred to as having “atypical PAH,” a subgroup ofpatients meeting hemodynamic criteria for PAH(including a low pulmonary capillary wedge pres-sure) with $3 cardiovascular risk factors were foundto resemble HFpEF PH patients phenotypically, butexhibited response to PAH therapies, which sug-gests that treatment response may not beadequately defined by traditional categorical di-visions (31). Methods for provocative testing to riskstratify and identify responders, including volumechallenge and exercise testing in the catheterizationlaboratory, may help delineate patients in this grayarea (42). Additionally, clinical trials are ongoing,testing inhaled b-adrenergic agonists (Inhaled Beta-adrenergic Agonists to Treat Pulmonary VascularDisease in Heart Failure With Preserved EF [BEATHFpEF]; NCT02885636), oral endothelin antagonists(A Study to Evaluate Whether Macitentan is anEffective and Safe Treatment for PatientsWith Heart Failure With Preserved Ejection Fractionand Pulmonary Vascular Disease [SERENADE];NCT03153111), and oral prostanoids (Study of OralTreprostinil in Subjects With Pulmonary Hyperten-sion Associated With Heart Failure With PreservedEjection Fraction [SOUTHPAW]; NCT03043651) inpatients with HFpEF and pulmonary vasculardisease.
Subpopulat ion: e levated lef t at r ia l pressure . Amechanical intervention to unload the left atrium viacreation of an interatrial shunt with a device tostandardize the shunt size has been shown to reduceexercise pulmonary capillary wedge pressure at 1month in a phase 2 trial, and further testing isongoing (55). Treatment with intravenous, inhaled, ororal inorganic nitrite or nitrate has also been shown toimprove exercise capacity and/or reduce pulmonarycapillary wedge pressure in early single-centerstudies, but the recent INDIE-HFpEF (Inorganic Ni-trite Delivery to Improve Exercise Capacity in HFpEF;NCT02742129) trial did not show benefit of inhaledinorganic nitrite on peak oxygen consumption. Morestudies using a variety of inorganic nitrite/nitrateformulations are ongoing.
SHOULD HFpEF TRIALS USE
QUALITY-OF-LIFE METRICS AS
MAIN ENDPOINTS?
Changes in quality of life (QOL) and functional ca-pacity in patients living with chronic diseases areoften overlooked or underemphasized as importantendpoints (56). These measures, although not neces-sarily correlated with morbidity and mortality, maybe particularly relevant for HFpEF, which oftenmanifests in advanced age, reducing exercise toler-ance and causing dyspnea, thereby pervading all as-pects of daily life by impairing function andindependence, 2 things that are commonly importantto older adults. Given that HFpEF studies have notachieved morbidity/mortality endpoints in any trial

J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8 Parikh et al.A U G U S T 2 0 1 8 : 6 1 9 – 3 2 Expert Scientific Panel on HFpEF
629
to date, we must consider whether focusing on end-points related to functional or symptom improve-ment may improve QOL outcomes; this wouldrepresent a paradigm shift. Both perspectives areexplored next.
NO, MORBIDITY AND MORTALITY SHOULD REMAIN
PRIMARY TARGETS OF HFpEF TRIALS. Survival andhospitalizations are the key endpoints that havedriven drug development in HFrEF and offer directrelevance to patients, health systems, and payers.They currently represent the standard in assess-ment of HFrEF interventions. For these reasons, thevalue placed on improvements in exercise toleranceand QOL, unaccompanied by morbidity/mortalitybenefits, can seem less significant when contrastedwith established benefits of standard HFrEFtherapies.
YES, HFpEF STUDIES SHOULD FOCUS ON QOL AND
EXERCISE ENDPOINTS. Preventing morbidity andmortality is the most critical goal for providerswhen considering the best HFpEF treatment for anindividual patient; however, HFpEF patients’ pri-mary focus is often finding ways to be less limitedby increasing their own functional capacity. TheNEAT-HFpEF (Nitrate’s Effect on Activity Tolerancein Heart Failure with Preserved Ejection Fraction)study of isosorbide mononitrate demonstrated thatemployment of novel methods to measure dailyactivity is not only feasible but is correlated withother measures of HF severity (57). Changes in ac-tivity measures were not associated with changes in6-min-walk distance or Kansas City CardiomyopathyQuestionnaire results (57,58), perhaps because ofdecreased sensitivity of the changes in standardassessments to deterioration or improvement.Nevertheless, patient-centric endpoints are beingused in increasing numbers of HFpEF trials. From astudy design perspective, QOL/exercise primaryendpoints may be helpful, as the increased non-cardiovascular comorbid burden and older age ofHFpEF patients compared with the HFrEF popula-tion presents greater challenges in showing thera-peutic efficacy and assessing cardiovascularmortality (59).
However, payers may not be willing to coverexpensive drugs and devices for QOL indications.This represents a challenge to both industry and in-vestigators and may be a limiting influence on clinicaltrial design considerations.
Beyond the previously mentioned subphenotypes,given the heterogeneity of HFpEF presentations andlikely biologic pathways, the interventions that may
benefit this growing patient population may vary indelivery (e.g., mechanical devices, inhaled therapy,lifestyle modification, activity tracking) and desiredeffect. Investigators could ideally select differentcategories of endpoints targeting different patientpresentations and goals. For example, exercise-limited and primarily dyspneic HFpEF patients maynot decompensate in a way that would require hos-pitalization, but they may benefit from an increase inwalking distance and functional capacity. Other pa-tients may have more difficulty with volume status/redistribution and benefit from interventions to pre-vent or address volume overload and frequent hos-pitalizations. To refine endpoints and increase therelevancy of findings, we believe it is necessary todevelop more sophisticated clinical phenotyping andtarget testing of interventions to the goals of patientsin subphenotypes.
CONCLUSIONS
In this summary of current controversies in HFpEF,we outline the findings from our Think Tank meeting,which was an expert panel discussion on existingevidence, persistent controversies, and gaps inHFpEF care. We approach critical HFpEF issues froma variety of perspectives. The HFpEF controversiesexplored throughout this paper are interrelated andcodependent and but serve to highlight gaps andopportunities in the field. The design of meaningfulHFpEF research should involve the full scope ofstakeholders, including investigators, regulators, in-dustry, and payers, and must consider the lessonslearned thus far to understand how future trials andobservational studies will close critical knowledgegaps and lead to optimal care for the patient withHFpEF.
ACKNOWLEDGMENTS The authors thank all ThinkTank participants for their ideas and unique per-spectives shared at the Think Tank meeting.Furthermore, the authors specifically acknowledgeBishow Adhikari, Javed Butler, Julie Catini, MathewMaurer, Gail Pearson, Matthew Roe, Lothar Roessig,Leo Seman, and Robert Temple for their contributionsat the meeting, and for providing feedback andeditorial recommendations for this manuscript. Theauthors also acknowledge Erin Campbell and MorganDeblecourt for their editorial contributions.
ADDRESS FOR CORRESPONDENCE: Dr. Kishan S.Parikh, Duke Clinical Research Institute, PO Box17969, Durham, North Carolina 27715. E-mail: [email protected].

PERSPECTIVES
COMPETENCY IN MEDICAL KNOWLEDGE: The
number of persons with HF in the United States has
continued to rise; approximately one-half of these
patients have HFpEF, which is not well understood.
Central to developing an improved understanding of
HFpEF is the determination as to whether this condition is
caused by a single disease state or multiple diseases
characterized by unique underlying pathophysiological
mechanisms.
TRANSLATIONAL OUTLOOK: The design of mean-
ingful HFpEF research should involve the full scope of
stakeholders, including investigators, regulators, indus-
try, and payers, and must consider the lessons learned
thus far to understand how future trials and observational
studies will close critical knowledge gaps and lead to
optimal care for the patient with HFpEF.
Parikh et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8
Expert Scientific Panel on HFpEF A U G U S T 2 0 1 8 : 6 1 9 – 3 2
630
RE F E RENCE S
1. Heidenreich PA, Albert NM, Allen LA, et al.Forecasting the impact of heart failure in theUnited States: a policy statement from theAmerican Heart Association. Circ Heart Fail 2013;6:606–19.
2. Go AS, Mozaffarian D, Roger VL, et al. Heartdisease and stroke statistics—2014 update: areport from the American Heart Association. Cir-culation 2014;129:e28–292.
3. Yancy CW, Jessup M, Bozkurt B, et al. 2013ACCF/AHA guideline for the management of heartfailure: a report of the American College of Car-diology Foundation/American Heart AssociationTask Force on practice guidelines. J Am Coll Car-diol 2013;62:e147–239.
4. Prasad A, Hastings JL, Shibata S, et al. Charac-terization of static and dynamic left ventriculardiastolic function in patients with heart failurewith a preserved ejection fraction. Circ Heart Fail2010;3:617–26.
5. Zile MR, Brutsaert DL. New concepts in diastolicdysfunction and diastolic heart failure. Part I:diagnosis, prognosis, and measurements of dia-stolic function. Circulation 2002;105:1387–93.
6. Borlaug BA. The pathophysiology of heart fail-ure with preserved ejection fraction. Nat RevCardiol 2014;11:507–15.
7. Borlaug BA, Kass DA. Ventricular-vascular inter-action in heart failure. Heart Fail Clin 2008;4:23–36.
8. Melenovsky V, Borlaug BA, Rosen B, et al.Cardiovascular features of heart failure with pre-served ejection fraction versus nonfailing hyper-tensive left ventricular hypertrophy in the urbanBaltimore community: the role of atrial remodel-ing/dysfunction. J Am Coll Cardiol 2007;49:198–207.
9. Sharma K, Kass DA. Heart failure with preservedejection fraction: mechanisms, clinical features,and therapies. Circ Res 2014;115:79–96.
10. Solomon SD, Claggett B, Lewis EF, et al. In-fluence of ejection fraction on outcomes and ef-ficacy of spironolactone in patients with heartfailure with preserved ejection fraction. Eur HeartJ 2016;37:455–62.
11. Cleland JGF, Bunting KV, Flather MD, et al.Beta-blockers for heart failure with reduced, mid-range, and preserved ejection fraction: anindividual patient-level analysis of double-blindrandomized trials. Eur Heart J 2018;39:26–35.
12. Kitzman DW, Shah SJ. The HFpEF Obesityphenotype: the elephant in the room. J Am CollCardiol 2016;68:200–3.
13. Paulus WJ, Tschope C. A novel paradigm forheart failure with preserved ejection fraction:comorbidities drive myocardial dysfunction andremodeling through coronary microvascularendothelial inflammation. J Am Coll Cardiol 2013;62:263–71.
14. Lakatta EG, Levy D. Arterial and cardiac aging:major shareholders in cardiovascular disease en-terprises. Part I: aging arteries: a “set up” forvascular disease. Circulation 2003;107:139–46.
15. Dalos D, Mascherbauer J, Zotter-Tufaro C,et al. Functional status, pulmonary artery pres-sure, and clinical outcomes in heart failure withpreserved ejection fraction. J Am Coll Cardiol2016;68:189–99.
16. Obokata M, Reddy YNV, Pislaru SV,Melenovsky V, Borlaug BA. Evidence supportingthe existence of a distinct obese phenotype ofheart failure with preserved ejection fraction. Cir-culation 2017;136:6–19.
17. Kitzman DW, Brubaker P, Morgan T, et al.Effect of caloric restriction or aerobic exercisetraining on peak oxygen consumption andquality of life in obese older patients withheart failure with preserved ejection fraction:a randomized clinical trial. JAMA 2016;315:36–46.
18. Valero-Munoz M, Backman W, Sam F. Murinemodels of heart failure with preserved ejectionfraction: a “fishing expedition”. J Am Coll CardiolBasic Trans Science 2017;2:770–89.
19. Shah SJ, Katz DH, Deo RC. Phenotypic spec-trum of heart failure with preserved ejectionfraction. Heart Fail Clin 2014;10:407–18.
20. Lewis GA, Schelbert EB, Williams SG,Cunnington C, Fozia A, McDonah TA. Biologicalphenotypes of heart failure with preserved
ejection fraction. J Am Coll Cardiol 2017;70:2186–200.
21. Houstis NE, Eisman AS, Pappagianopoulos PP,et al. Exercise intolerance in heart failure withpreserved ejection fraction: diagnosing andranking its causes using personalized O2 pathwayanalysis. Circulation 2018;137:148–61.
22. Shah SJ, Katz DH, Selvaraj S, et al. Pheno-mapping for novel classification of heart failurewith preserved ejection fraction. Circulation 2015;131:269–79.
23. van Veldhuisen DJ, Linssen GC, Jaarsma T,et al. B-type natriuretic peptide and prognosis inheart failure patients with preserved and reducedejection fraction. J Am Coll Cardiol 2013;61:1498–506.
24. Anjan VY, Loftus TM, Burke MA, et al. Preva-lence, clinical phenotype, and outcomes associ-ated with normal B-type natriuretic peptide levelsin heart failure with preserved ejection fraction.Am J Cardiol 2012;110:870–6.
25. Reddy YNV, Carter RE, Obokata M,Redfield MM, Borlaug BA. A simple, evidence-based approach to help guide diagnosis of heartfailure with preserved ejection fraction. Circulation2018 May 23 [E-pub ahead of print].
26. Anand IS, Claggett B, Liu J, et al. Interactionbetween spironolactone and natriuretic peptidesin patients with heart failure and preserved ejec-tion fraction: from the TOPCAT Trial. J Am CollCardiol HF 2017;5:241–52.
27. Anand IS, Rector TS, Cleland JG, et al. Prog-nostic value of baseline plasma amino-terminalpro-brain natriuretic peptide and its interactionswith irbesartan treatment effects in patients withheart failure and preserved ejection fraction:findings from the I-PRESERVE trial. Circ Heart Fail2011;4:569–77.
28. Hernandez AF, Hammill BG, O’Connor CM,Schulman KA, Curtis LH, Fonarow GC. Clinicaleffectiveness of beta-blockers in heart failure:findings from the OPTIMIZE-HF (Organized Pro-gram to Initiate Lifesaving Treatment in Hospital-ized Patients with Heart Failure) Registry. J AmColl Cardiol 2009;53:184–92.

J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8 Parikh et al.A U G U S T 2 0 1 8 : 6 1 9 – 3 2 Expert Scientific Panel on HFpEF
631
29. Cleland JG, Tendera M, Adamus J, et al. Theperindopril in elderly people with chronic heartfailure (PEP-CHF) study. Eur Heart J 2006;27:2338–45.
30. Massie BM, Carson PE, McMurray JJ, et al.Irbesartan in patients with heart failure and pre-served ejection fraction. N Engl J Med 2008;359:2456–67.
31. Yusuf S, Pfeffer MA, Swedberg K, et al. Effectsof candesartan in patients with chronic heart fail-ure and preserved left-ventricular ejection frac-tion: the CHARM-Preserved Trial. Lancet 2003;362:777–81.
32. Brenner BM, Cooper ME, de Zeeuw D,et al. Effects of losartan on renal and car-diovascular outcomes in patients with type 2diabetes and nephropathy. N Engl J Med2001;345:861–9.
33. Heart Outcomes Prevention Evaluation StudyI, Yusuf S, Sleight P, et al. Effects of anangiotensin-converting-enzyme inhibitor, ramipril,on cardiovascular events in high-risk patients.N Engl J Med 2000;342:145–53.
34. Davis BR, Kostis JB, Simpson LM, et al. Heartfailure with preserved and reduced left ventricularejection fraction in the antihypertensive andlipid-lowering treatment to prevent heart attacktrial. Circulation 2008;118:2259–67.
35. Zinman B, Wanner C, Lachin JM, et al. Empa-gliflozin, Cardiovascular outcomes, and mortalityin type 2 diabetes. N Engl J Med 2015;373:2117–28.
36. Neal B, Perkovic V, Matthews DR. Canagli-flozin and cardiovascular and renal events in type2 diabetes. N Engl J Med 2017;377:2099.
37. Ledwidge M, Gallagher J, Conlon C, et al.Natriuretic peptide-based screening and collabo-rative care for heart failure: the STOP-HF ran-domized trial. JAMA 2013;310:66–74.
38. Huelsmann M, Neuhold S, Resl M, et al.PONTIAC (NT-proBNP selected prevention of car-diac events in a population of diabetic patientswithout a history of cardiac disease): a prospectiverandomized controlled trial. J Am Coll Cardiol2013;62:1365–72.
39. Yancy CW, Jessup M, Bozkurt B, et al. 2017ACC/AHA/HFSA Focused Update of the 2013ACCF/AHA Guideline for the Management ofHeart Failure: a report of the American Collegeof Cardiology/American Heart Association TaskForce on Clinical Practice Guidelines and theHeart Failure Society of America. J Am CollCardiol 2017;70:776–803.
40. Gerges M, Gerges C, Pistritto AM, et al. Pul-monary hypertension in heart failure. epidemi-ology, right ventricular function, and survival. AmJ Respir Crit Care Med 2015;192:1234–46.
41. Lam CS, Roger VL, Rodeheffer RJ, Borlaug BA,Enders FT, Redfield MM. Pulmonary hypertensionin heart failure with preserved ejection fraction: acommunity-based study. J Am Coll Cardiol 2009;53:1119–26.
42. Borlaug BA, Obokata M. Is it time to recognizea new phenotype? Heart failure with preserved
ejection fraction with pulmonary vascular disease.Eur Heart J 2017;38:2874–8.
43. Hoeper MM, Lam CSP, Vachiery JL, et al.Pulmonary hypertension in heart failure with pre-served ejection fraction: a plea for proper pheno-typing and further research. Eur Heart J 2017;38:2869–73.
44. Fayyaz AU, Edwards WD, Maleszewski JJ,et al. Global pulmonary vascular remodeling inpulmonary hypertension associated with heartfailure and preserved or reduced ejection fraction.Circulation 2018;137:1796–810.
45. Benza RL, Raina A, Abraham WT, et al. Pul-monary hypertension related to left heart dis-ease: insight from a wireless implantablehemodynamic monitor. J Heart Lung Transplant2015;34:329–37.
46. Dixon DD, Trivedi A, Shah SJ. Combined post-and pre-capillary pulmonary hypertension in heartfailure with preserved ejection fraction. Heart FailRev 2016;21:285–97.
47. Ben-Yehuda O, Rubin LJ. Pulmonary hyper-tension overlap syndromes: a real entity? J AmColl Cardiol 2016;68:379–81.
48. Guazzi M, Vicenzi M, Arena R, Guazzi MD.Pulmonary hypertension in heart failure with pre-served ejection fraction: a target ofphosphodiesterase-5 inhibition in a 1-year study.Circulation 2011;124:164–74.
49. Hoendermis ES, Liu LC, Hummel YM, et al.Effects of sildenafil on invasive haemodynamicsand exercise capacity in heart failure patients withpreserved ejection fraction and pulmonary hyper-tension: a randomized controlled trial. Eur Heart J2015;36:2565–73.
50. Liu LC, Hummel YM, van der Meer P, et al.Effects of sildenafil on cardiac structure andfunction, cardiopulmonary exercise testing andhealth-related quality of life measures in heartfailure patients with preserved ejection fractionand pulmonary hypertension. Eur J Heart Fail2017;19:116–25.
51. Opitz CF, Hoeper MM, Gibbs JS, et al. Pre-capillary, combined, and post-capillary pulmonaryhypertension: a pathophysiological continuum.J Am Coll Cardiol 2016;68:368–78.
52. Frost AE, Badesch DB, Barst RJ, et al. Thechanging picture of patients with pulmonaryarterial hypertension in the United States: howREVEAL differs from historic and non-USContemporary Registries. Chest 2011;139:128–37.
53. Hoeper MM, Huscher D, Ghofrani HA, et al.Elderly patients diagnosed with idiopathic pul-monary arterial hypertension: results from theCOMPERA registry. Int J Cardiol 2013;168:871–80.
54. Ling Y, Johnson MK, Kiely DG, et al. Changingdemographics, epidemiology, and survival of inci-dent pulmonary arterial hypertension: results fromthe pulmonary hypertension registry of the UnitedKingdom and Ireland. Am J Respir Crit Care Med2012;186:790–6.
55. Feldman T, Mauri L, Kahwash R, et al. Trans-catheter Interatrial Shunt Device for the
Treatment of Heart Failure With Preserved Ejec-tion Fraction (REDUCE LAP-HF I [Reduce ElevatedLeft Atrial Pressure in Patients With Heart Fail-ure]): a phase 2, randomized, sham-controlledtrial. Circulation 2018;137:364–75.
56. Hamo CE, Gheorghiade M, Butler J. Novelendpoints for heart failure clinical trials. CurrHeart Fail Rep 2017;14:210–6.
57. Redfield MM, Anstrom KJ, Levine JA, et al.Isosorbide mononitrate in heart failure with pre-served ejection fraction. N Engl J Med 2015;373:2314–24.
58. Snipelisky D, Kelly J, Levine JA, et al.Accelerometer-measured daily activity in heartfailure with preserved ejection fraction: clinicalcorrelates and association with standard heartfailure severity indices. Circ Heart Fail 2017;10:e003878.
59. Henkel DM, Redfield MM, Weston SA,Gerber Y, Roger VL. Death in heart failure: acommunity perspective. Circ Heart Fail 2008;1:91–7.
60. van Veldhuisen DJ, Cohen-Solal A, Bohm M,et al. Beta-blockade with nebivolol in elderlyheart failure patients with impaired and pre-served left ventricular ejection fraction: datafrom SENIORS (Study of Effects of NebivololIntervention on Outcomes and Rehospitalizationin Seniors With Heart Failure). J Am Coll Cardiol2009;53:2150–8.
61. Yamamoto K, Origasa H, Hori M,Investigators JD. Effects of carvedilol on heartfailure with preserved ejection fraction: the Japa-nese Diastolic Heart Failure Study (J-DHF). Eur JHeart Fail 2013;15:110–8.
62. Ahmed A, Rich MW, Fleg JL, et al. Effectsof digoxin on morbidity and mortality in dia-stolic heart failure: the ancillary digitalisinvestigation group trial. Circulation 2006;114:397–403.
63. Edelmann F, Wachter R, Schmidt AG, et al.Effect of spironolactone on diastolic functionand exercise capacity in patients with heartfailure with preserved ejection fraction: theAldo-DHF randomized controlled trial. JAMA2013;309:781–91.
64. Pitt B, Pfeffer MA, Assmann SF, et al. Spi-ronolactone for heart failure with preservedejection fraction. N Engl J Med 2014;370:1383–92.
65. Deswal A, Richardson P, Bozkurt B, Mann DL.Results of the Randomized Aldosterone Antago-nism in Heart Failure with Preserved EjectionFraction trial (RAAM-PEF). J Card Fail 2011;17:634–42.
66. Redfield MM, Chen HH, Borlaug BA, et al.Effect of phosphodiesterase-5 inhibition onexercise capacity and clinical status in heartfailure with preserved ejection fraction: arandomized clinical trial. JAMA 2013;309:1268–77.
67. Kosmala W, Holland DJ, Rojek A, Wright L,Przewlocka-Kosmala M, Marwick TH. Effect of If-channel inhibition on hemodynamic status andexercise tolerance in heart failure with preserved

Parikh et al. J A C C : H E A R T F A I L U R E V O L . 6 , N O . 8 , 2 0 1 8
Expert Scientific Panel on HFpEF A U G U S T 2 0 1 8 : 6 1 9 – 3 2
632
ejection fraction: a randomized trial. J Am CollCardiol 2013;62:1330–8.
68. Pal N, Sivaswamy N, Mahmod M, et al. Effectof selective heart rate slowing in heart failure withpreserved ejection fraction. Circulation 2015;132:1719–25.
69. Komajda M, Isnard R, Cohen-Solal A, et al.Effect of ivabradine in patients with heart failurewith preserved ejection fraction: the EDIFY ran-domized placebo-controlled trial. Eur J Heart Fail2017;19:1495–503.
70. Edelmann F, Gelbrich G, Dungen HD, et al.Exercise training improves exercise capacity anddiastolic function in patients with heart failure
with preserved ejection fraction: results of theEx-DHF (Exercise training in Diastolic HeartFailure) pilot study. J Am Coll Cardiol 2011;58:1780–91.
71. Solomon SD, Zile M, Pieske B, et al. Theangiotensin receptor neprilysin inhibitor LCZ696in heart failure with preserved ejection fraction: aphase 2 double-blind randomised controlled trial.Lancet 2012;380:1387–95.
72. Pieske B, Maggioni AP, Lam CSP, et al. Ver-iciguat in patients with worsening chronic heartfailure and preserved ejection fraction: results ofthe SOluble guanylate Cyclase stimulatoR inheArT failurE patientS with PRESERVED EF
(SOCRATES-PRESERVED) study. Eur Heart J2017;38:1119–27.
KEY WORDS classification scheme,diagnosis, diastolic, ejection fraction,endpoints, heart failure, pathophysiology,preserved ejection fraction, pulmonaryhypertension, subject eligibility, treatment
Go to http://www.acc.org/jacc-journals-cme to takethe CME/MOC quiz forthis article.