Embed Size (px)
Citation preview

Heart Failure Surgery
The Last Frontier
Gerardo S. Manzo, MD, FPCS, FPCCBringing Global Trends in Cardiology Closer to Home
PHA Convention 26 May 2012

et al. Circulation 2006;113:e684-e685
Copyright © American Heart Association

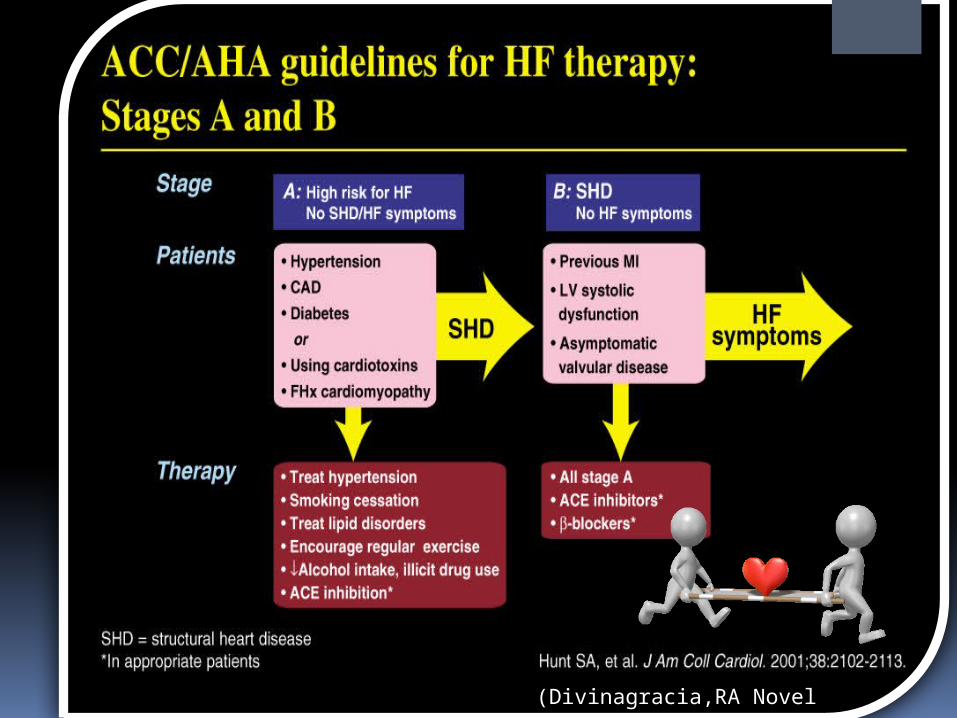
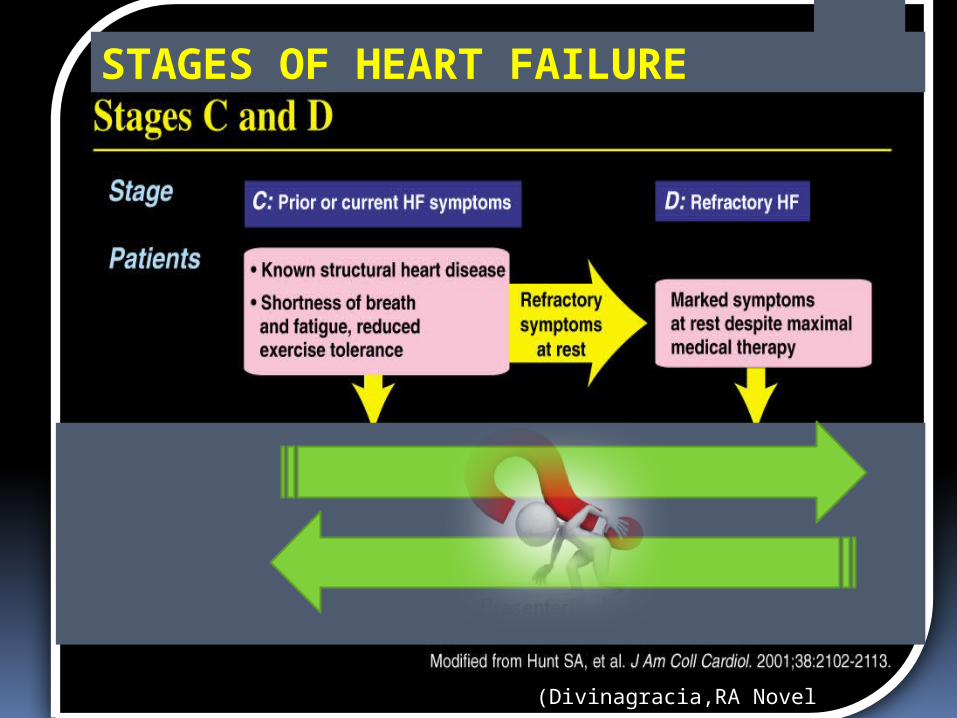
STAGES OF HEART FAILURE
(Divinagracia,RA Novel Therapy HF)
(Divinagracia,RA Novel Therapy HF)
STAGES OF HEART FAILURE
(Divinagracia,RA Novel Therapy HF)

(Divinagracia,RA Novel Therapy HF)
• All Stage A, B and C• Mechanical assist devices• Heart transplantation• Continuous IV inotropic
infusion for palliation• Hospice care
Stage D : Refractory HF
Therapy

Surgical Options for the Failing Ventricle Transmyocardial Revascularization (laser) End-to-End Mitral Repair (Everest Clip/ Alfieri) Cardiomyoplasty CorCap Cardiac Support Device (mesh) Coapsys LV Support Device (intracavitary
rod) Partial Left Ventriculectomy (Batista) Stem Cell Therapy ??? Mechanical Circulatory Support Devices Heart Transplantation
PHA Annual 2005 GSManzo

5th Annual Heart Failure Convention March 08 GSM
Edge-to-Edge Repair EVEREST (Endovascular Valve Edge-to-
Edge REpair Study)
Percutaneous Implantation
Transcatheter joining of mitral valve leaflets
Co-joined leaflets result in dual orifice
Transeptal delivery in cath lab

The CorCap is designed to:
Provide end-diastolic ventricular support to reduce wall stress and myocardial stretch
Negate the stimuli for ventricular remodeling and promote myocardial reverse remodeling
Reverse progressive dilation and improve cardiac function and patient functional status
CorCap™ Cardiac Support Device

5th Annual Heart Failure Convention March 08 GSM
Annuloplasty : Transventricular /Transatrial / Epicardial Approach
Intracavitary shortening
rod connecting two
external pads to shorten
septolateral dimension
of LV and mitral annulus
Myocor Surgical Coapsys System

Surgical Approaches to Heart Failure
HFSA 2010 Recommendations

Lindenfeld J, et al. HFSA 2010 Comprehensive Heart Failure Guideline. J Card Fail 2010;16:e1-e194.
HFSA 2010 Practice GuidelineSurgery
Recommendation 10.1
It is recommended that the decision to undertake surgical intervention for severe HF be made in light of the following: Functional status
Prognosis based on severity of underlying HF co-morbid conditions.
Procedures should be done at centers with the following: Demonstrable expertise
Multidisciplinary medical and surgical teams experienced in the selection, care, and perioperative and long-term management of high risk patients with severe HF
Strength of Evidence = C

Lindenfeld J, et al. HFSA 2010 Comprehensive Heart Failure Guideline. J Card Fail 2010;16:e1-e194.
HFSA 2010 Practice GuidelineHeart Transplantation
Recommendation 10.2
Evaluation for heart transplantation is recommended in selected patients with the following: severe HF
debilitating refractory angina
or ventricular arrhythmia that cannot be controlled despite drug, device or alternative surgical therapy.
Strength of
Evidence = B

Lindenfeld J, et al. HFSA 2010 Comprehensive Heart Failure Guideline. J Card Fail 2010;16:e1-e194.
HFSA 2010 Practice GuidelineMitral Valve Repair or Replacement
Recommendation 10.3
Isolated mitral valve repair or replacement for severe mitral regurgitation secondary to ventricular dilatation in the presence of severe LV systolic dysfunction is not generally recommended.
Strength of Evidence = C

Lindenfeld J, et al. HFSA 2010 Comprehensive Heart Failure Guideline. J Card Fail 2010;16:e1-e194.
HFSA 2010 Practice GuidelineSurgery
Recommendation 10.4
“Batista Procedure”
Partial left ventricular resection is not recommended in nonischemic cardiomyopathy.
Strength of Evidence = B

Lindenfeld J, et al. HFSA 2010 Comprehensive Heart Failure Guideline. J Card Fail 2010;16:e1-e194.
HFSA 2010 Practice GuidelineMechanical Support
Recommendation 10.5
Patients awaiting heart transplantation who have become refractory to all means of medical circulatory support should be considered for a mechanical support device as a bridge to transplant.
Strength of Evidence = B

Lindenfeld J, et al. HFSA 2010 Comprehensive Heart Failure Guideline. J Card Fail 2010;16:e1-e194.
HFSA 2010 Practice GuidelinePermanent Mechanical Assistance
Recommendation 10.6
Permanent mechanical assistance using an implantable assist device may be considered in highly selected patients with severe HF refractory to conventional therapy who are not candidates for heart transplantation, particularly those who cannot be weaned from IV inotropic support at an experienced HF center. Strength of Evidence = B

Lindenfeld J, et al. HFSA 2010 Comprehensive Heart Failure Guideline. J Card Fail 2010;16:e1-e194.
HFSA 2010 Practice Guideline“Bridge to Decision”
Recommendation 10.7 (NEW in 2010)
The following patients should be considered for urgent mechanical circulatory support as a “bridge to decision”:
Patients with refractory HF and hemodynamic instability
and/or compromised end-organ function
with relative contraindications to cardiac transplantation or permanent mechanical circulatory assistance, who are expected to improve with time or restoration of an improved hemodynamic profile
These patients should be referred to a center with expertise in the management of patients with advanced HF
Strength of Evidence = C


The Role Of INTERMACS in Patient Selection for Longer Term
Mechanical Circulatory Support
Lynne Warner Stevenson
Investigational indications will be discussed
No conflicts related to MCS
For Extended Use / Durable
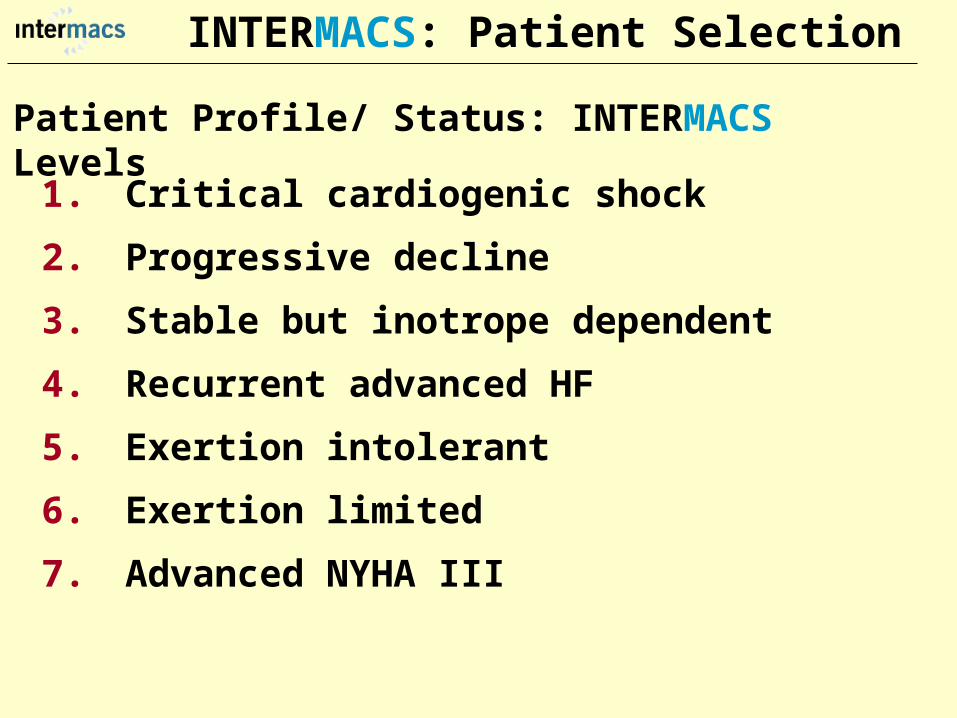
Patient Profile/ Status: INTERMACS Levels
1. Critical cardiogenic shock
2. Progressive decline
3. Stable but inotrope dependent
4. Recurrent advanced HF
5. Exertion intolerant
6. Exertion limited
7. Advanced NYHA III
INTERMACS: Patient Selection

PROFILENTERMACS LEVEL
# PtsYr 1
Official Shorthand General time frame for support
LEVEL 1 Cardiogenic Shock
82 “Crash and burn” Hours
LEVEL 2 Progressive
Decline
81 “Sliding fast” Days to week
LEVEL 3 Stable On Inotropes
18 Stable but Dependent
Weeks
LEVEL 4 Recurrent
Advanced HF
9 “Frequent flyer” Weeks to few months, if baseline restored
Level 5Exertion Tolerant
4 “Housebound” Weeks to months
LEVEL 6 Exercise Limited
3 “Walking wounded” Months, if nutrition and activity maintained
INTERMACSAdvance NYHA III
4 Advanced Class III

The Fourth INTERMACS Annual Report: 4,000 implants and counting
James K. Kirklin, MD, David C. Naftel, PhD, Robert L. Kormos, MD, Lynne W. Stevenson, MD, Francis D. Pagani, MD, PhD, Marissa A. Miller, DVM, MPH, J. Timothy
Baldwin, PhD and James B. Young, MD
The Journal of Heart and Lung TransplantationVolume 31, Issue 2, Pages 117-126 (February 2012)
DOI: 10.1016/j.healun.2011.12.001
Copyright © 2012 Terms and Conditions
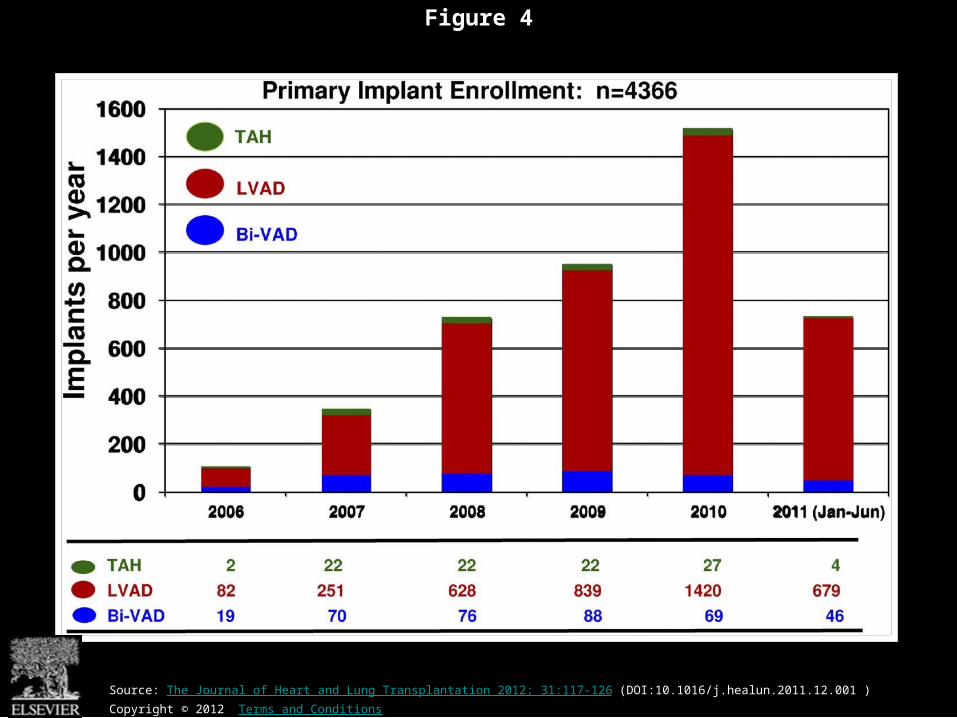
Figure 4
Source: The Journal of Heart and Lung Transplantation 2012; 31:117-126 (DOI:10.1016/j.healun.2011.12.001 )
Copyright © 2012 Terms and Conditions

Figure 10
Source: The Journal of Heart and Lung Transplantation 2012; 31:117-126 (DOI:10.1016/j.healun.2011.12.001 )
Copyright © 2012 Terms and Conditions

Device Strategy1.Bridge to Recovery (BTR)2.Bridge to “Decision”3.Bridge to a Bridge4.Bridge to Transplant (BTT)5.Destination Therapy6.Rescue Therapy

The CentriMag & PediVas:
Magnetically Levitated Pumps
for ECMO & VAD’s;
Neonates to Adults
Stephen Harwood, CCP, CPC, BA

CentriMag & PediVas

CentriMag®
System Components
Pump Motor Console

Indications
The CentriMag and PediVas pumps are classified as short term devices (30 days)
Are often used as a ‘bridge’ from one point in treatment to another
They are well suited in the critical setting because they are extremely easy to institute
They have been widely used as ventricular support devices, but also are popular in ECMO /ECLS circuits as well
Longest duration : 304 days followed by HeartMate II

J138-0711
Contemporary Outcomes With the HeartMate II® LVAS
David J. Farrar, PhDVice President, Research and Scientific AffairsThoratec Corporation

A surgically implanted, rotary continuous-flow device in parallel with the native left ventricle
Left ventricle to ascending aorta
Percutaneous driveline
Electrically powered
Batteries and line power
Fixed-speed operating mode
Home discharge with ability to return to activities of daily life (work, school, exercise, hobbies, etc.)
Implantable
Pump
Controller
PercutaneousLead
Batteries
HeartMate II® LVAS

HeartMate II is the first and only FDA-approved continuous-flow device for both Bridge-to-Transplantation (BTT) and Destination Therapy (DT).
Bridge-to-Transplantation
Risk of imminent death from nonreversible left ventricular failure
Candidate for cardiac transplantation
Destination Therapy
NYHA Class IIIB or IV heart failure
Optimal medical therapy 45 of last 60 days
Not a candidate for cardiac transplantation
HeartMate II—Indications for Use

Boyle, Ascheim, Russo, et al. JHLT. 2011;30:4.
Clinical Outcomes Based on INTERMACS Profile
Length of Stay Post-VAD Actuarial Survival Post-VAD
Less acutely ill, ambulatory patients in INTERMACS profiles 4–7 had better survival and reduced length of stay compared to patients who were more accurately ill in profiles 1–3.
Group 1: INTERMACS 1Group 2: INTERMACS 2–3Group 3: INTERMACS 4–7
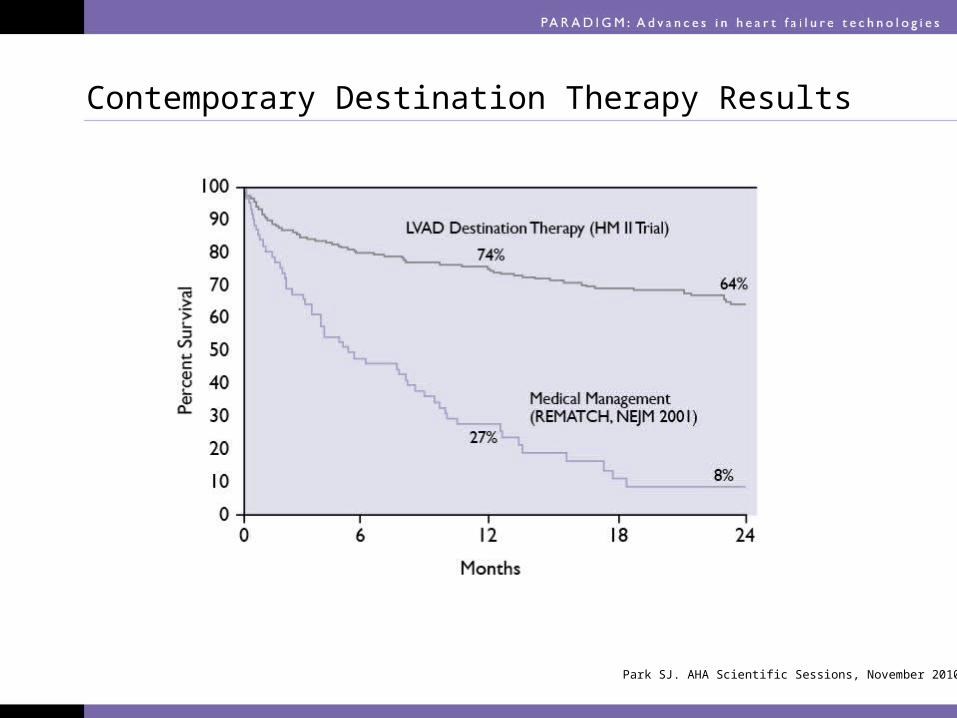
Contemporary Destination Therapy Results
Park SJ. AHA Scientific Sessions, November 2010.

In Summary
Over 7,000 patients implanted with HeartMate II—long-term durability
Improvements in Bridge-to-Transplant and Destination Therapy survival and adverse event rates
Adverse-event differences in LVAD patients may lead to targeted approaches for men and women
Driveline infections can possibly be reduced by new tunneling techniques
New HeartMate II risk model along with INTERMACS profiles may help guide future patient selection

• All Stage A, B and C• Mechanical assist devices• Heart transplantation• Continuous IV inotropic
infusion for palliation• Hospice care
Stage D : Refractory HF
Therapy
Is Device Therapy unaffordable for Filipino patients?


About 250,000 Americans each year have an ICD implanted at the cost of about $100,000 each. Weisfeldt, Myron L., and Susan L. Zeiman. "Advances in the Prevention and Treatment of Cardiovascular Disease: One of the most important contributors to improved human survival is the treatment of cardiovascular disease". Health Affairs. Vol. 26, No. 1, pp. 25-37 January 2007

DESCRIPTION Unit PriceICD (Single) 600,000ICD (Dual) 750,000
CRTD 1,000,000
Total ICD CRT
2007-2011
1 2 3 4 50
10
20
30
40
50
60
17 18
3238
54
Series1
2007 2008 2009 2010 2011
ICD CRT in the Philippines
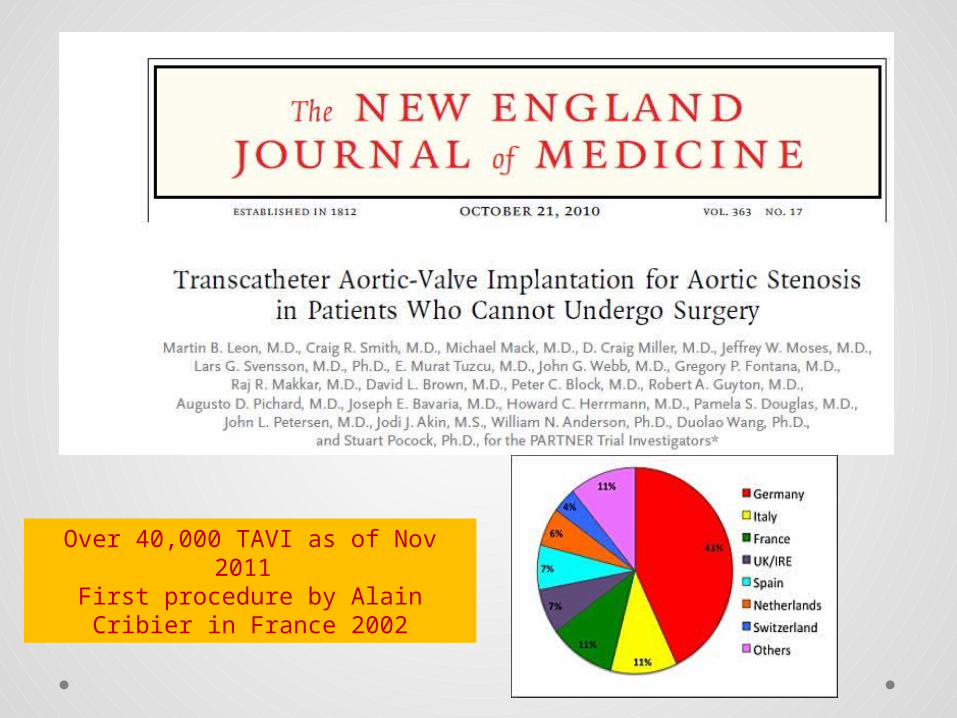
Over 40,000 TAVI as of Nov 2011 First procedure by Alain Cribier in
France 2002

$ 25,000 ~ P1M for device only
Transcatheter Aortic Valve Implantation TAVI Devices
Transapical TAVI
Transfemoral TAVI


EVARTEVAR
$12,000 ~ P 500,000For Device

CentriMag®
System Components
Pump Motor Console$10,500 ~ P 590,000For Patient Device
$70,000 ~ P 3.9MFor Hospital

HEART TRANSPLANTATION
Overall
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132

NUMBER OF HEART TRANSPLANTS REPORTED BY YEAR
0
500
1000
1500
2000
2500
3000
3500
4000
4500
5000
1982
1983
1984
1985
1986
1987
1988
1989
1990
1991
1992
1993
1994
1995
1996
1997
1998
1999
2000
2001
2002
2003
2004
2005
2006
2007
2008
2009
Nu
mb
er
of
Tra
ns
pla
nts
Other
EuropeNorth America
NOTE: This figure includes only the heart transplants that are reported to the ISHLT Transplant Registry. As such, the presented data may not mirror the changes in the number of heart transplants performed worldwide
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132

ADULT HEART TRANSPLANTATION Kaplan-Meier Survival by Era
(Transplants: 1/1982 – 6/2009)
0
20
40
60
80
100
0 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15
Years
1982-1991 (N=20,504)
1992-2001 (N=36,879)
2002-6/2009 (N=22,477)
1982-1991 vs. 1992-2001: p = 0.84601982-1991 vs. 2002-6/2009: p < 0.00011992-2001 vs. 2002-6/2009: p < 0.0001
HALF-LIFE 1982-1991: 10.2 years; 1992-2001: 10.7 years; 2002-6/2009: NA
Su
rviv
al (
%)
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132

ADULT HEART RECIPIENTSCross-Sectional Analysis
Functional Status of Surviving Recipients (Follow-ups: 1995 - June 2010)
0%
20%
40%
60%
80%
100%
1 Year (N = 16,087) 3 Years (N = 14,235) 5 Years (N = 12,181)
No Activity Limitations Performs with Some Assistance Requires Total Assistance
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132

ADULT HEART RECIPIENTSEmployment Status of Surviving Recipients
Age at Follow-up: 25-55 Years (Follow-ups: 1995 - June 2010)
0%
20%
40%
60%
80%
100%
1 Year (N = 9,115) 3 Year (N = 6,967) 5 Year (N = 5,163)
Retired
Not Working
Working Part Time
Working Full Time
Working (FT/PTstatus unknown)
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132

ADULT HEART RECIPIENTSRehospitalization Post-transplant of Surviving Recipients
(Follow-ups: 1995 - June 2010)
0%
20%
40%
60%
80%
100%
Up to 1 Year Between 2 and 3 Years Between 4 and 5 Years
No Hospitalization Hospitalized: Not Rejection/Not Infection
Hospitalized: Rejection Only Hospitalized: Infection Only
Hospitalized: Rejection + Infection
(N = 22,651) (N = 26,546) (N = 19,481)
ISHLT 2011ISHLTJ Heart Lung Transplant. 2011 Oct; 30 (10): 1071-1132

Global Burden of Heart Disease

Global Burden of Heart Disease
Focused on Prevention & Risk Modificationo genetic susceptibilityo marked environmental changes usually secondary to
• urbanization• increasing affluence• influences from early childhood to
adulthood.

Individual Burden of Heart Failure
Direct Costs of Careo Inpatient : Frequent Re-hospitalizationo Rehabilitationo Follow-up careo Cost of DevicesIndirect Costso Loss of employmento “Medicare” benefitso Family expenses

Heart Failure Surgeryin the Philippines
• Create Multidisciplinary medical and surgical teams experienced in the selection, care, and perioperative and long-term management of high risk patients with severe HF
• Implement evidence based HF therapies• Develop expertise on appropriate surgical
procedures for HF• Increase patient awareness on available
treatment options
We need to stop condemning our Stage D Heart Failure
patients…
…and conquer the last frontiers of Philippine cardiology...
THANK YOU