Embed Size (px)
Citation preview

Short reports 237Weiss, C. F., Glazko, A. J., and Weston, J. K. (1960).
Chloramphenicol in the newborn infant. A physiologicexplanation of its toxicity when given in excessive doses. NewEngland Journal of Medicine, 262, 787.
A. W. CRAFT,* J. T. BROCKLEBANK, E. N. HEY, andR. H. JACKSONDepartment of Chiild Health, Royal VictoriaInfirmary, Newcastle upon Tyne NEI 4LP.
*Correspondence to Dr. A. W. Craft.
Effect of head rotation on jugularvein blood flow
During a cardiac investigation blood oxygensaturations in the innominate veins were noticed tovary when the child moved his head. It seemed
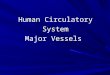
(a) (b)FIG. 1.-Right internal jugular venogram. (a) Head turned to left showing free downwardflow, (b) head turned to right
showing vein occluded; escape of medium to smaller veins.
possible that alterations in jugular vein flow wereresponsible, particularly in view of the well-knownchanges in cervical venous hums caused by rotationof the head. To study this effect, internal jugularvenography was performed by manual injections ofradio-opaque medium under fluoroscopy at thebeginning of cardiac catheterization in 60 infantsand children who had various congenital cardiacanomalies but no other major malformations.
MethodA catheter introduced from the leg was passed into one
or both of the internal jugular veins where this could bedone with a minimum of manipulation and withoutinconvenience to the child. The head was then rotatedto varying degrees, as far as the child could maintain byhimself if unanaesthetized. 16 children wereanaesthetized for the cardiac investigation, and the otherswere sedated with trimeprazine, except for small infantswho received no sedation. Though the 60 patientsrepresented only a minority of the total number under-going investigation, it is unlikely that the results wereaffected.
ResultsFlow in an internal jugular vein was not affected
by contralateral rotation of the head (Fig. la), but
on Septem
ber 1, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.49.3.237 on 1 March 1974. D
ownloaded from

ipsilateral rotation by 450 or more caused narrowingof the middle third of the vein, presumably by softtissues related to the sternomastoid muscle.Ipsilateral rotation of the head to almost 90° causedcomplete occlusion of the vein in 41 children (Fig.lb), in all 16 children who were anaesthetized, andin 25 of the remaining 44. In 24 of these 41children only 75° rotation was needed, and in 15 ofthem only 60° rotation, to interrupt downward flowin the vein completely. Withdrawal of the catheterjust after an injection did not affect the obstruction.
Sedation other than anaesthesia, age, anddiagnosis were not factors in determining theproduction of obstruction. In the minority ofchildren where both internal jugular veins wereentered, ipsilateral head rotation usually affectedeach vein similarly.
In some cases medium injected into the upperpart of an internal jugular vein occluded by headrotation escaped entirely into smaller veins, butmore commonly some medium flowed retrogradelyinto the lateral sinus. It then sometimes dis-appeared rapidly, but in about half the children withan occluded vein the medium remained visible in thelateral sinus for 1 to 3 minutes and sometimeslonger, even though by this time no medium could
be seen outside the skull (Fig. 2). Downward flowin a vein obstructed by head rotation was notrestored by digital occlusion of the opposite internaljugular vein, though the face sometimes becamesuffused.Mean pressure gradients between the upper and
lower thirds of the internal jugular veins, normally 0to 2 mmHg, rose to 1 to 31 mm during occlusion.
Effect on venous oxygen saturations. Bloodoxygen saturations in the internal jugular,innominate, and superior caval veins are usuallysimilar during a cardiac investigation; the highersaturations in tributaries such as the subclavianveins, often 80 to 8500 in asymptomatic children,are outweighed by the large cerebral flow, usually at60 to 700% saturation. In 5 cases rotation of thehead to one side caused the ipsilateral innominatevein saturation to rise by over 25 %, well outside theusual sampling variation of 5 to 10%. Presumablythis occurred through deviation of the lower-saturation internal jugular flow to the other side.This effect might conceivably raise the suspicion ofpartial pulmonary venous flow into the leftinnominate vein should the head happen to beturned to the left.
(a) (b)
FIG. 2.-Left internal jugular venogram. (a) Head turned to left showing retrograde filling of left lateral sinus (arrow),(b) 3 minutes later, medium still present in left lateral sinus.
238 Short reports
on Septem
ber 1, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.49.3.237 on 1 March 1974. D
ownloaded from

Short reportsComment
No references to similar observations have beenfound, though neurosurgeons are aware of the effectof unusual head positions on cerebral congestion atoperation. The observations may also be relevantin the following situations.
(1) In children undergoing manipulationsinvolving an internal jugular vein, since the head isoften turned fully to the other side.
(2) In children who already have occlusion of oneoftheir internal jugular veins (more particularly if itsupper tributaries are involved).
(3) In the management of children with cyanoticheart lesions or infective lesions predisposing tothrombosis (if stasis is indeed a further provocativefactor).
(4) In the management of hydrocephalus and ofpossible intracranial haemorrhage.
SummaryRotation of the head to one side causes obstruction
of the ipsilateral internal jugular vein in mostanaesthetized and many nonanaesthetized children,and may cause intracranial venous stasis.
G. H. WATSON*Royal Manchester Children's Hospital, and theDepartment of Child Health, University ofManchester.
*Correspondence to G.H.W., Royal Manchester Children'sHospital, Pendlebury, Manchester M27 IHA.
239
on Septem
ber 1, 2020 by guest. Protected by copyright.
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.49.3.237 on 1 March 1974. D
ownloaded from







![Jugular Vein Obstruction Caused by Turning of the Head · The routine use of jugular venous catheterization during the past 10 years [1] has revolutionized treatment of seriously](https://img.pdfslide.us/doc/110x75/5fd24776808ec6345d62e523/jugular-vein-obstruction-caused-by-turning-of-the-the-routine-use-of-jugular-venous.jpg)




![Case Report Preservation of the External Jugular Vein in ...Case Reports in Medicine e preservation of the external jugular vein (EJV) was rst proposed by Leclerc and Roy in [ ]andlater](https://img.pdfslide.us/doc/110x75/611de40f865fe31a6c784dee/case-report-preservation-of-the-external-jugular-vein-in-case-reports-in-medicine.jpg)








![Ultrasound guidance versus anatomical landmarks for ...€¦ · [Intervention Review] Ultrasound guidance versus anatomical landmarks for internal jugular vein catheterization Patrick](https://img.pdfslide.us/doc/110x75/5f9beef95154c7333f47d212/ultrasound-guidance-versus-anatomical-landmarks-for-intervention-review-ultrasound.jpg)