Embed Size (px)
Citation preview

Ligation of the Suprarenal Inferior Vena Cava:
Application of a Graphite-Benzalkonium-Heparin CoatedFemoral-to-Jugular Vein Shunt
LEO B. BEILIN,* M.D., ROBERT W. CAMPBELL,fM.D.,ALAN B. GAZZANIGA+ M.D.
From the Department of Surgery, University of California, Irvine, California 92664
CLINICAL experience has shown a highmorbidity and mortality after suprarenalinferior vena cava1 (SRIVC) injury due toblunt trauma, penetrating trauma, or ab-dominal surgical procedures. Repair of thevena cava may be difficult or impossible,and in some cases acute ligation above therenal veins has been the only alternativeto exsanguination.1 2, 4, 6, 8, 10, 13, 16 Thisstudy evaluates the physiological altera-tions following acute SRIVC ligation andpresents a technic for reducing the associ-ated severe renal and hemodynamicchanges.
Material and Methods
Adult dogs each weighing between 18and 24 Kg. were anesthetized with 30mg./Kg. of sodium pentobarbital. Endo-tracheal tubes were inserted and the dogswere allowed to breath spontaneously.Catheters were placed to monitor meanarterial pressure (MAP) on a mercurymanometer; central venous pressure (CVP)and infrarenal inferior vena caval (IRIVC)pressure were monitored on separate saline
Submitted for publication October 22, 1970.*Junior Resident, Surgery, University of Cali-
fornia, Irvine.tSenior Resident, Surgery, University of Cali-
fornia, Irvine.tAssistant Professor of Surgery, University of
California, Irvine.Reprint request: Alan B. Gazzaniga, M. D.,
Department of Surgery, University of Califomia,Irvine, California, 92664.
manometers. Through a midline abdominalincision the entrance of left and right renalveins into the inferior vena cava were ex-posed. Two heavy silk sutures were placedaround the cava cephalad to the renal veinsand blood samples were drawn for deter-mination of BUN and creatinine. After con-trol pressure measurements, the suprarenalinferior vena cava (SIRVC) was doublyligated and pressures were recordedperiodically for 8 hours or until death. Inthree control dogs plasma volumes ( 131Ilabeled human serum albumin) and hema-tocrits were determined immediately be-fore and 4 hours after ligation.5
Fifteen dogs were studied and dividedinto three equal groups. Group I dogsserved as controls. Group II dogs receivedintravenous colloid (plasma or low molec-ular weight dextran) and normal saline inequal amounts necessary to maintain MAPat or above 100 mm. Hg. In Group III dogsthe femoral veins were cannulated withpolyvinyl graphite-benzalkonium-heparin(GBH) coated catheters (I.D. 4 mm.)which were tunneled subcutaneously andinserted into the jugular veins. The GBHcoating was a modification7 of that usedby Gott et al. Patency of the shunts wasconfirmed by inferior vena cavagrams 6 to8 hours after operation. The shunts werekept in place for 48 hours at which timethey were removed. In surviving animalsserum samples were drawn every thirdday during the postoperative course to de-
837

BEILIN, CAMPBELL AND GAZZANIGA Ann. Surg. Nov. 1971Vol. 174- No. 5
MAP - Mean value of 5 dogs601 --- = Survivor dog
E
E
c
0
cnE
._
0
C
E
I RIVC
CVP
4
2
LIG. I 2 3 4 5 E
HOURS
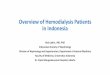
FiG. 1. Changes in mean arterial, IRIVC andSVC pressures following SRIVC ligation.
termine BUN and creatinine levels. Onlong-term survivors inferior vena cava-
grams were performed one month post-operatively and the animals were exploredprior to sacrifice to determine directly thepatency of the inferior vena cava and itsmajor tributaries.
ResultsGroup I (Control)The mean IRIVC pressure was 7 cm.
saline and rose immediately after ligationto greater than 80 cm. saline in four of fivedogs (Fig. 1). Central venous pressure fellfrom a mean of 5 cm. saline to zero. The
MAP dropped from an average controlpressure of 140 mm. Hg to 70 mm. Hg and48 mm. Hg 1 hour and 4 hours, respec-
tively, after ligation. In the one survivor,IRIVC pressure rose to a peak of 57 cm.
saline and then fell to 30 cm. and 25 cm.
saline 1 hour and 4 hours, respectively(Fig. 1). The MAP dropped to 80 mm. Hgand remained there for 7 hours and beganto rise when the dog awakened from anes-
thesia.There was a 26% reduction in total
blood volume and a 16% increase inhematocrit 4 hours following ligation(Table 1). Reduction in total blood volumewas primarily a result of plasma loss.Four of the five dogs died within 6 hours
of operation and the one survivor hadsevere lethargy and moderate swelling ofthe hind limbs for approximately 5 dayspostoperatively. Its BUN was 45 mg./100 ml. and creatinine 3.4 mg./100 ml. on
the first postoperative day but both were
normal by the third postoperative day.Venography performed on this dog one
month after ligation showed prominentcollateral return via the paravertebal plexusand inferior epigastric veins (Fig. 2). Atsacrifice the IRIVC and both renal veinswere completely thrombosed, which con-
firmed the impression gained from phlebog-raphy. The remarkable dilated renalcapsular venous system furnished venous
drainage adequate to maintain normalrenal function.Postmortem examination of non-surviv-
ing animals showed grossly engorged kid-neys, severe retroperitoneal hemorrhagicsequestrations, and venae cavae below theligation site were patent.
Group II (Medical)
Changes in IRIVC, CVP, and MAP pres-sures after ligation were similar to thosein the control group. When the MAPdropped below 100 mm. Hg, the IRIVCpressure began to fall. With infusions of
838
6

Ann. Surg. Nov. 1971 LIGATION OF THE SUPRARENAL INFERIOR VENA CAVAV'ol. 174 No. 5 839
TABLE 1. Blood Volume Changes after SRI VC Ligation in Control Dogs
Pre-Ligation 4 Hours Post-Ligation)Hema- Hema-
Dog Blood Plasma Red Cell tocrit Blood Plasma Red Cell tocrit
1 1,552 792 760 49 1,261 593 688 532 1,702 885 817 48 1,105 453 652 593 1,312 682 630 48 1,139 467 672 59Mean 1,522 786 735 48 Mean: 1,135 504 664 57
either saline or low molecular weightdextran or both, MAP rose to 100 mm. Hgfollowed by a prompt rise in IRIVC pres-sure to previous levels. After cessation ofthe infusion the MAP drifted to less than100 mm. Hg, requiring further transfusion.Colloid and saline infusions averaged 3,000cc. per animal.Two dogs died with refactory hypo-
tension 3 hours after operation. Six hoursafter ligation IRIVC pressure was less than60 cm. saline in one of the remaining dogsand less than 40 cm. saline in the othertwo. The MAP at the same time was over100 mm. Hg. Two dogs died 24 hours fol-lowing operation with such massive swel-ling of the hind limbs that they were un-able to stand. One survivor was able tostand and move about. Its serum BUN andcreatinine levels, although initially elevated,were normal one week postoperatively.Postmortem examination showed patency
of the inferior venae cavae but there wasmassive retroperitoneal hemorrhage greaterthan in control dogs. Phlebography in thesole survivor one month postoperativelyshowed collateral circulation via the para-vertebral venous plexuses and epigastricsystem. The IRIVC was patent at sacrifice.
Group III (GBH Shunt)Immediately after caval ligation IRIVC
pressure rose to a mean above 78 cm. salineand CVP fell from a mean of 4 to a meanof 1 cm. saline. MAP changed from anaverage of 144 mm. Hg to 116 mm. Hg.Shunts were opened within 5 minutes afterligation and IRIVC pressure dropped to a
mean of 31 mm. Hg. The MAP was over120 mm. Hg 6 hours postoperatively, andthe animals were fully awake from anes-thesia.One dog died 24 hours postoperatively
from vomiting and aspiration. The retro-peritoneum was free of hemorrhage, thekidneys were not engorged, and the venacava below the ligation site was patent.There was thrombus at the tips of the GBHshunt. A second dog died 7 days postopera-tively from peritonitis due to a retainedsponge. In this dog there was no swellingof the hind limbs and initial postoperativeBUN and creatinine levels were normal.The vena cava below the ligation site waspatent. Three dogs survived and hadbenign courses without swelling of the hindlimbs. Postoperative BUN and creatininelevels were normal. Shunts were all closedat 48 hours and generally had some throm-bus projecting from the tips of thecatheters.Phlebography was performed in all dogs
approximately 6 hours postoperatively andin each instance patency of the shunt wasconfirmed (Fig. 3). Phlebography was re-peated in survivors one month postopera-tively and showed patency of the inferiorvenae cavae up to the ligation site. Collat-eral circulation was via the epigastric andparavertebral vessels (Fig. 4). These find-ings were confirmed at sacrifice.
DiscussionA review of the experimental report 8, 11,
12, 14, 17 indicates that survival rates in un-treated dogs following SRIVC ligation

BEILIN, CAMPBEL:
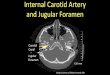
FiG. 2 A and B. Anteroposterior and lateralviews of venogram in surviving dogs one monthafter acute ligation of the SRIVC. The vena cavais not visualized and collateral return is via theepigastric and vertebral veins.
L AND GAZZANIGA Ann. Surg. * Nov. 1971Vol. 174 * No. 5
varies from 0%o to 40%, although one
author cites 83%o survival. Death usuallyoccurs within 5 to 72 hours following liga-tion. Wittenberger and Huggins believedthat death was due to hypovolemia as a
result of retroperitoneal accumulation ofblood. Other investigators 9,14 however,placed a stronger emphasis on renal dam-age since pathological changes on micro-scopic examination and decreased renalfunction have been reported in both sur-
vivors and non-survivors. The inferencethat death was related to renal deteriora-tion has little support since the dogs diedso rapidly. It has been pointed out thateven in experimental bilateral nephrectomyit may take as long as 8 days for deathfrom uremia to occur.14The rise in hematocrit and fall in plasma
and red cell volumes in control dogs in thisstudy indicated loss of blood from theintravascular compartment rather thanvenous pooling. This is confirmed by au-
topsy findings of severe retroperitonealhemorrhagic sequestration. This transuda-tion results from caval hypertension andincreased capillary hydrostatic pressure.
The degree of caval hypertension is re-
lated to the number of existing venous
collaterals and the level of systemic MAP.The latter is influenced immediately by thesudden decrease in venous return and con-
currently but more slowly by whole bloodloss. Dogs infused with colloid and crystal-loid responded with elevations of arterialpressure but at the expense of raisingIRIVC pressure to severe peak post ligationlevels. Although in some treated animalslevels of IRIVC consistent with the ac-
quisition of adequate collateral channelsare reached, this is at the expense of suchsevere retroperitoneal and lower extremityswelling that survival is compromised.
Figures quoted state that complete col-lateralization after ligation requires 7 to 14days. Data obtained from our non-operateddogs seem to indicate that under the stressof severe venous hypertension due toSRIVC ligation, the dogs develop enough
840

Ann. Surg. Nov. 1971 LIGATION OF THE SUPRARENAL INFERIOR VENA CAVAV'ol. 174 No. 5 841
FIG. 3. Six hours postoperative venogram in a FIG. 4. Anteroposterior venogram one monthdog with GBH coated shunt. Patency of the shunt following SRIVC ligation in a dog with a previousis confirmed and the vertebral veins are filled via GBH shunt. The inferior cava below the renalthe lumbar veins. veins in patent and collateral return is via the
paravertebral and epigastric veins.
collaterals in 8 hours or less to keep IRIVCpressure less than 40 cm. of water whilemaintaining mean arterial pressure at or
above 100 mm. Hg.Data from our GBH shunted dogs which
had moderate caval hypertension indicatethat only 24 hours or less were needed forfunctionally adequate (for survival) col-laterals to develop without the severe
morbidity of non-operated dogs. It is our
supposition that these GBH shunts stayopen for as long as high pressure gradientsand flow rates exist, and thrombose whenthese conditions are no longer present. Inother words, these shunts probably stayedpatent for as long as they were needed.Two other modes of therapy have been
proposed to reduce the high morbidityand mortality following IRIVC ligation.Lejeune-Ledant and Sapirstein both re-
ported marked improvement in survival ifright nephrectomy were done concomi-
tantly with SRIVC ligation. The rationaleof Sapirstein was as follows: "The rightnephrectomy was performed to diminishthe load on the developing anastomoticcirculation until it was well established;the anastomoses and the renal hypertrophyapparently developing at compatible rates."The clinical correlate to this is that themajority of reports of survival followingSRIVC ligation have been during thecourse of a difficult right nephrectomy.The observation has been made that mostof these nephrectomies were done fortumors, and thus a greater degree of col-lateral circulation than normal may havebeen present. There are, however, two re-ports of survival following right nephrec-tomy (normal right kidney) combinedSRIVC ligation for gunshot and blunttrauma.1' 5The other therapeutic suggestion stems
from a clinical report 3 that has no experi-

842 BEILIN, CAMPBELL AND GAZZANIGA Ann. Surg. Nov. 1971
inienltal verificationl. In the coturse of re-
miioving a pyolhydronicphlrotic right kidney,injury to the inferior vena cava occurredsuch that SRIVC ligation was necessary.An immediate splenorenal shunt wvas per-formed and the patient survived. It isprobable that as collateralization occurredand the pressure gradient across the anas-tomosis decreased, the shunt thrombosed.
Neither of these latter therapeutic pro-posals is ideal. The first would often in-volve extirpation of a normal organ, andthe second might lead to splenic veinthrombosis.The studies we have undertaken indicate
that a temporaiy external GBH coatedshunt between the femoral and jugularvein is the most satisfactory solution andone which involves the least alteration ofthe circulatory system and precludes thenecessity of sacrificing one of a pair ofvital organs.
Summary1. Acute suprarenal inferior vena caval
ligation resulted in 80% mortality in un-treated dogs.
2. Mortality is due to hypotension causedby whole blood (primarily plasma) se-questration in the retroperitoneum and in-adequate venous return.
3. Large volume fluid therapy does notincrease survival.
4. Survival can be achieved by a tempo-rary femoral to jugular vein bypass witha polyvinyl graphite-benzalkonium-heparincoated catheter shunt.
References1. Bolot, F., Germain, J., Ponsan, R. and Mas-
sotte, J.: Blessure par Balle de la VeineCave Inferieure Au-dessus des PediculesRenaux. Ligature de la Veine Cave Inferi-
cure, Cuer isoii. (Rapport de J. Quenut)Miem. Acad. Cliir., 81:394, 1955. Cited byDetrie.
2. Caplan, B. B., 11alasz, N. A. and Bloomer,W. E.: Resection and Ligation of the Supra-renal Inferior Vena Cava. J. Urol., 92:25,1964.
3. Dietrick, W., Wakabayashi, A. and Connolly,J. E.: Athrombogenic Left Ventricular By-pass. Amer. J. Surg., 118:244, 1969.
4. Fitzsimmons, L. E. and Garvey, F. K.: Infe-rior Vena Cava Injury. J. Urol., 82:285,1959.
5. Gazzaniga, A. B., Cahill, J. L., Replogle, R.L. and Tilney, N. L.: Changes in BloodVolume and Renal Function Following Li-gation of the Inferior Vena Cava. Surgery,62:417, 1967.
6. Gazzaniga, A. B. and Colodny, A. H.: LongTerm Survival After Acute Ligation of theVena Cava Above the Renal Veins. In Press.
7. Gott, V. L., Whiffen, J. D., Koepke, D. E.,Daggett, R. L., Boake, W. C. and Young,W. P.: Techniques of Applying a Graphite-Benzalkonium-Heparm Coating to VariousPlastics and Metals. Trans. Amer. Soc. Artif.Intern. Organs, 10:213, 1964.
8. Herendeen, T., Judd, D. and Siderys, H.:Ligation of the Suprarenal Vena Cava inDogs. Arch. Surg., 88:1045, 1964.
9. LeJeune-Ledant, G.: A Propos de la Ligaturede la Veine Cave Inferieure Au-dessus desVeines Ranales et Surrenales: Etude Experi-mentale. Minerva Cardioangiologica Europa,3:303, 1957.
10. Mehta, A. R., Rajpal, R. M. and Jussawalla,D. J.: Suprarenal Ligation of the InferiorVena Cava with a Solitary Horseshoe Kid-ney. Amer. J. Surg., 116:925, 1968.
11. Nesbit, R. M. and Wear, J. B.: Ligation ofthe Inferior Vena Cava Above the RenalVeins. Ann. Surg., 154:332, 1961.
12. Polkey, H. J.: The PhenolsulfonphthaleinOutput after Ligation of the Vena Cavaand the Renal Veins. Urol. and Cutan. Rev.,33:294, 1929.
13. Ramnath, R., Walden, E. C. and Cagiun, F.:Ligation of the Suprarenal Vena Cava andRight Nephrectomy with Complete Recov-ery. Amer. J. Surg., 112:88, 1966.
14. Ripstein, C., Seropian, D., Schor, G. and Le-vine, A.: Obstruction of the Inferior VenaCava above the Renal Veins. Surg. Forum,3:292, 1952.
15. Sapirstein, L. A. and Reininger, E. J.: Cathe-ter Induced Error in Hepatic Venous Sam-pling. Circ. Res., 4:493, 1956.
16. Waltuck, T. L., Crow, R. W., Humphrey, L.J. and Kauffman, H. M.: Avulsion Iniuriesof the Vena Cava Following Blunt Abaomi-nal Trauma. Ann. Surg., 171:67, 1970.
17. Whittenberger, J. L. and Huggins, C.: Liga-tion of the Inferior Vena Cava. Arch. Surg.,41:1334, 1940.