Embed Size (px)
Citation preview
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
Grand Round: Clinical Guidelines for the patient with COVID-‐19
An overview of general management
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
Speakers and housekeeping
Dr James Bartlett-‐ Respiratory Physician, Medical Advisor for Quality, Safety and Patient Experience and Senior Medical Lead for COGS
Dr Michael Augello-‐ Emergency Physician and Deputy Director FootscrayEmergency Department
Dr James Molton-‐ Infectious Diseases Physician and part of the COVID-‐19 Response Team
Dr Claire Burrows-‐ Anaesthetist and Clinical lead for Intubation Team
Questions
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
Introduction
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
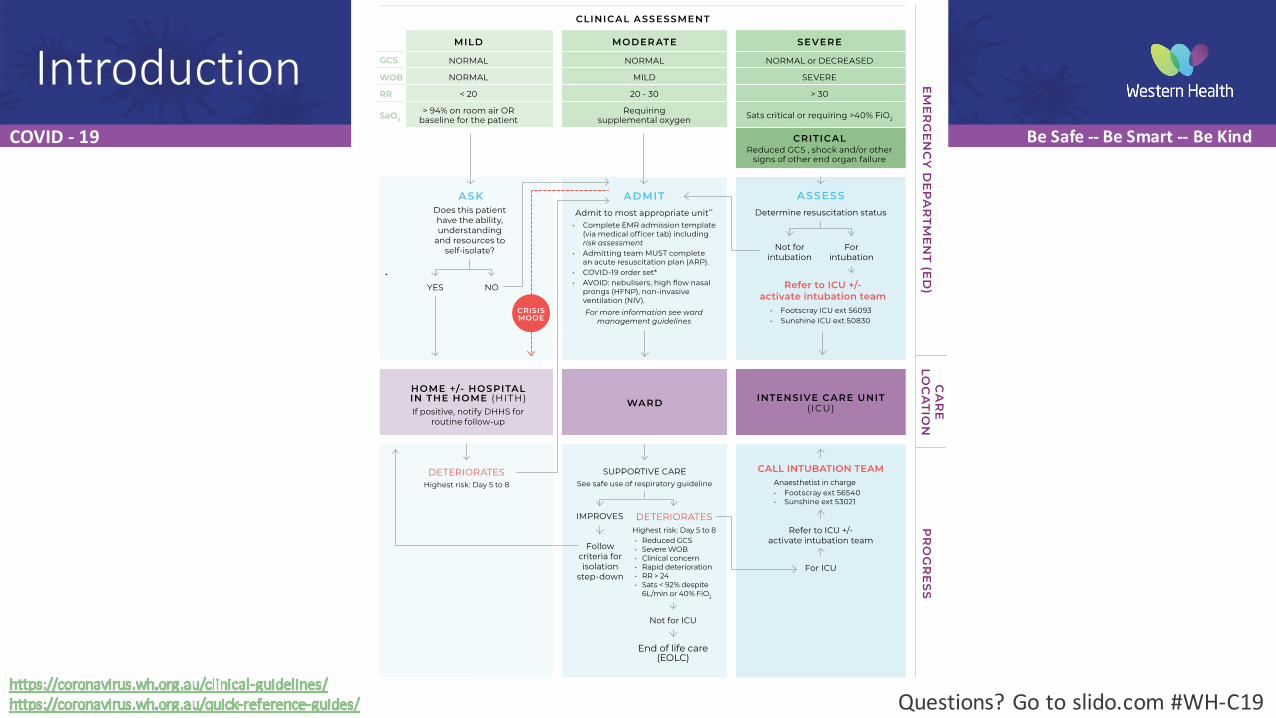
IntroductionCLINICAL ASSESSMENT
MILD MODER ATE SEVERE
NORMAL NORMAL NORMAL or DECREASED
NORMAL MILD SEVERE
< 20 20 - 30 > 30
> 94% on room air OR baseline for the patient
Requiring supplemental oxygen Sats critical or requiring >40% FiO2
CRITICALReduced GCS , shock and/or other
signs of other end organ failure
HOME +/- HOSPITAL IN THE HOME (HITH)If positive, notify DHHS for
routine follow-up
INTENSIVE CARE UNIT (ICU)WARD
Not for ICU
End of life care (EOLC)
ASKDoes this patient have the ability, understanding
and resources to self-isolate?
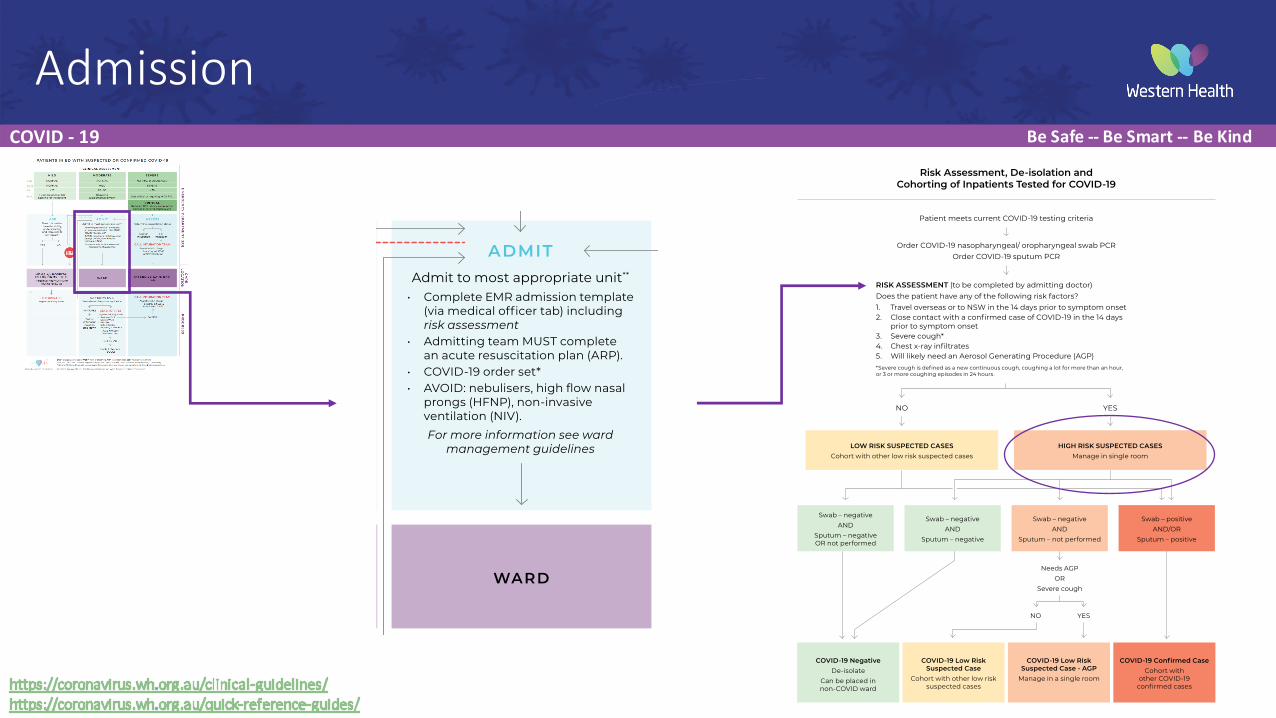
ADMITAdmit to most appropriate unit**
• Complete EMR admission template (via medical officer tab) including risk assessment
• Admitting team MUST complete an acute resuscitation plan (ARP).
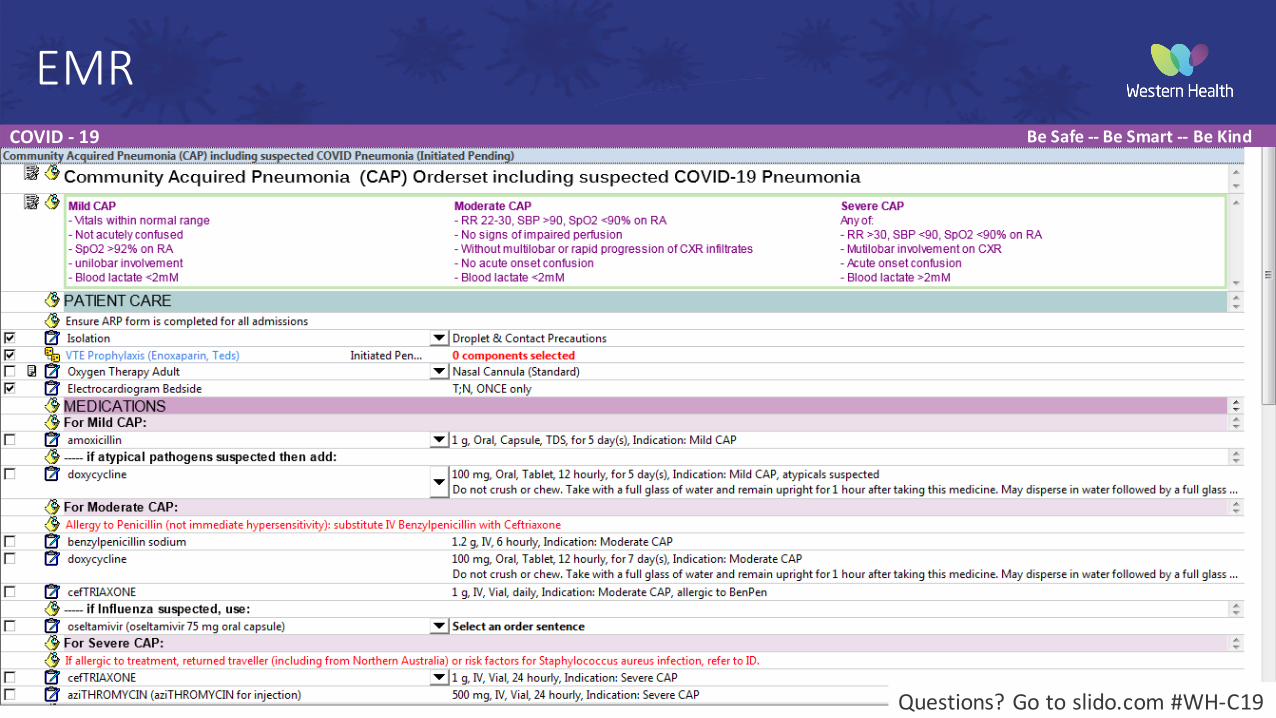
• COVID-19 order set*• AVOID: nebulisers, high flow nasal
prongs (HFNP), non-invasive ventilation (NIV). For more information see ward
management guidelines
ASSESSDetermine resuscitation status
Not for intubation
YES
For intubation
NO
Follow criteria for isolation
step-down
SUPPORTIVE CARESee safe use of respiratory guideline
DETERIORATESHighest risk: Day 5 to 8
EM
ER
GE
NC
Y D
EP
AR
TME
NT (E
D)
PR
OG
RE
SSC
AR
E LO
CA
TION
PATIENTS IN ED WITH SUSPECTED OR CONFIRMED COVID-19
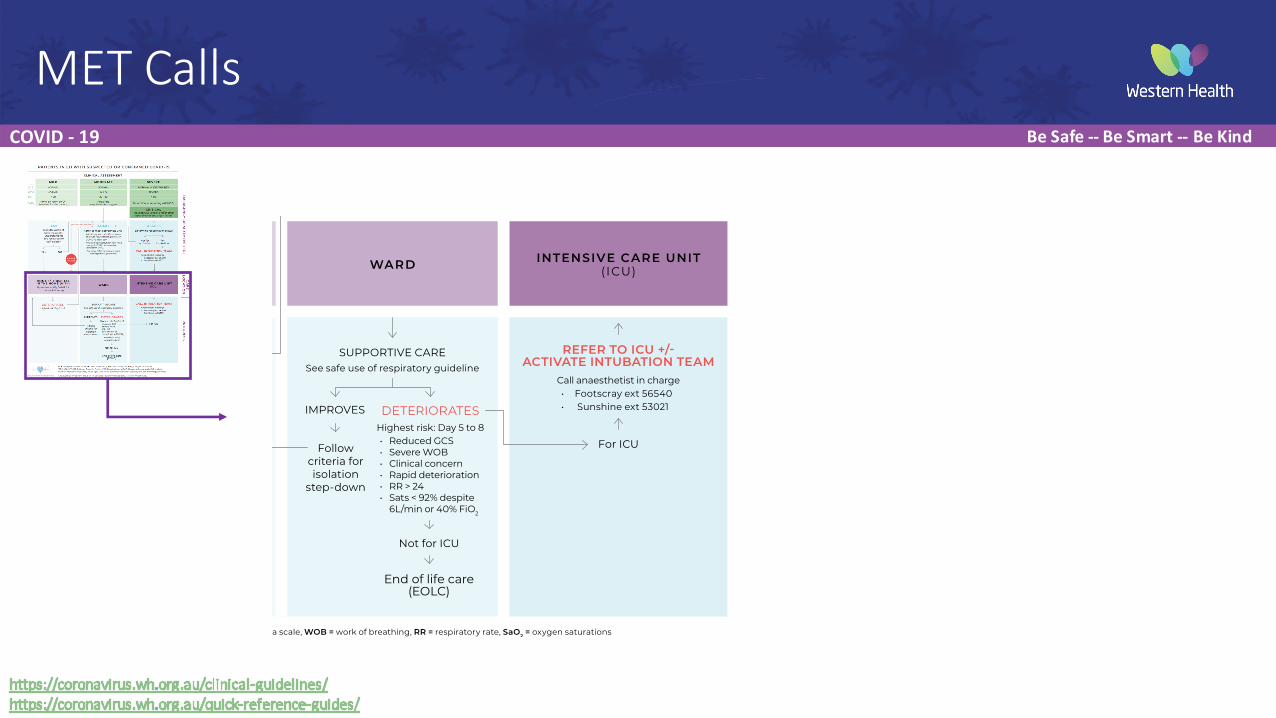
IMPROVES DETERIORATESHighest risk: Day 5 to 8 • Reduced GCS • Severe WOB• Clinical concern• Rapid deterioration• RR > 24• Sats < 92% despite
6L/min or 40% FiO2
CRISIS MODE
GCS
WOB
RR
SaO2
Created by Western Health in collaboration with beauty within medicine.
GCS = Glasgow coma scale, WOB = work of breathing, RR = respiratory rate, SaO2 = oxygen saturations*FBE, UEC, LFT, CRP, D-Dimer, Troponin, Ferritin, VBG, Blood cultures, COVID-19 swab, influenza swab, CXR (mobile).**General Medicine, Respiratory, Acute Aged Care unless otherwise known to a specialty unit. See admitting guidelines.
Refer to ICU +/- activate intubation team
For ICU
CALL INTUBATION TEAM
Refer to ICU +/- activate intubation team
• Footscray ICU ext 56093 • Sunshine ICU ext 50830
Anaesthetist in charge • Footscray ext 56540• Sunshine ext 53021
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
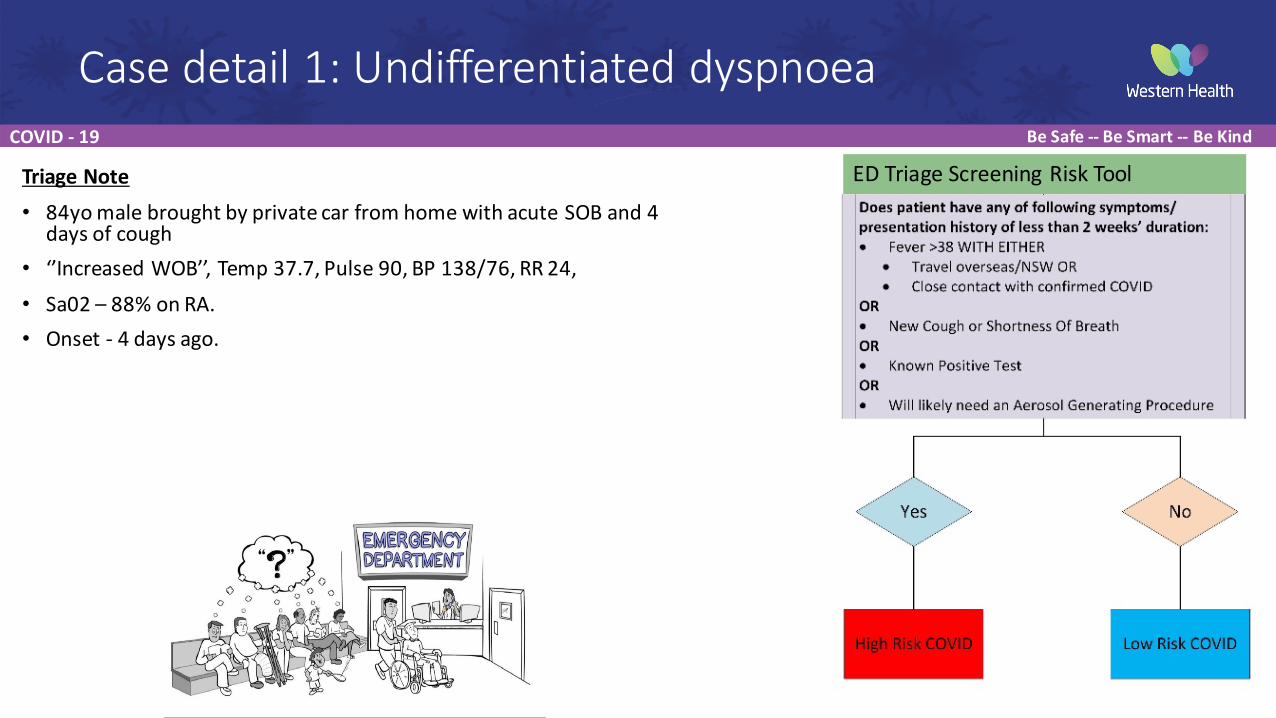
Case detail 1: Undifferentiated dyspnoea
Triage Note• 84yo male brought by private car from home with acute SOB and 4
days of cough• ‘’Increased WOB’’, Temp 37.7, Pulse 90, BP 138/76, RR 24, • Sa02 – 88% on RA. • Onset -‐ 4 days ago.
ED Triage Screening Risk Tool
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
The Emergency Department in the Time of COVID-‐19
• Challenges• Current low community prevalence• Infectious Risk impacting normal practice• Communication• Environment
• ED cubicles• Cohorting in ED unavoidable
• Oxygen therapy and AGP in ED • Numerous changes to usual practices• Additional Cognitive load
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
The Emergency Department in the Time of COVID-‐19
ED must ALWAYSmaintain capacity to receive, assess and manage the next undifferentiated
patient .
How does ED continue to provide BEST CARE to the public during a pandemic ?
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
Emergency Department Flowchart
Questions? Go to slido.com #WH-‐C19
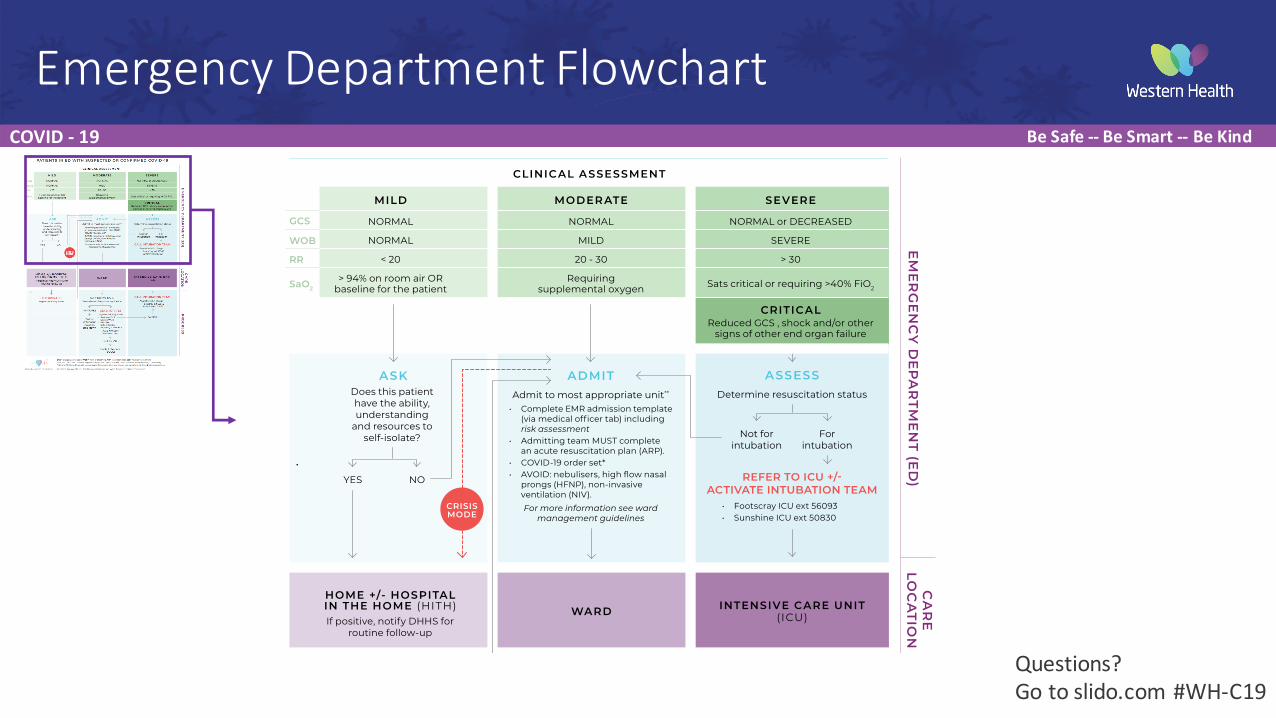
CLINICAL ASSESSMENT
MILD MODER ATE SEVERE
NORMAL NORMAL NORMAL or DECREASED
NORMAL MILD SEVERE
< 20 20 - 30 > 30
> 94% on room air OR baseline for the patient
Requiring supplemental oxygen Sats critical or requiring >40% FiO2
CRITICALReduced GCS , shock and/or other
signs of other end organ failure
HOME +/- HOSPITAL IN THE HOME (HITH)If positive, notify DHHS for
routine follow-up
INTENSIVE CARE UNIT (ICU)WARD
Not for ICU
End of life care (EOLC)
ASKDoes this patient have the ability, understanding
and resources to self-isolate?
ADMITAdmit to most appropriate unit**
• Complete EMR admission template (via medical officer tab) including risk assessment
• Admitting team MUST complete an acute resuscitation plan (ARP).
• COVID-19 order set*• AVOID: nebulisers, high flow nasal
prongs (HFNP), non-invasive ventilation (NIV). For more information see ward
management guidelines
ASSESSDetermine resuscitation status
Not for intubation
YES
For intubation
NO
Follow criteria for isolation
step-down
SUPPORTIVE CARESee safe use of respiratory guideline
DETERIORATESHighest risk: Day 5 to 8
EM
ER
GE
NC
Y D
EP
AR
TME
NT (E
D)
PR
OG
RE
SSC
AR
E LO
CA
TION
PATIENTS IN ED WITH SUSPECTED OR CONFIRMED COVID-19
IMPROVES DETERIORATESHighest risk: Day 5 to 8 • Reduced GCS • Severe WOB• Clinical concern• Rapid deterioration• RR > 24• Sats < 92% despite
6L/min or 40% FiO2
CRISIS MODE
GCS
WOB
RR
SaO2
Created by Western Health in collaboration with beauty within medicine.
GCS = Glasgow coma scale, WOB = work of breathing, RR = respiratory rate, SaO2 = oxygen saturations*FBE, UEC, LFT, CRP, D-Dimer, Troponin, Ferritin, VBG, Blood cultures, COVID-19 swab, influenza swab, CXR (mobile).**General Medicine, Respiratory, Acute Aged Care unless otherwise known to a specialty unit. See admitting guidelines.
REFER TO ICU +/- ACTIVATE INTUBATION TEAM
For ICU
CALL INTUBATION TEAM
REFER TO ICU +/- ACTIVATE INTUBATION TEAM
• Footscray ICU ext 56093 • Sunshine ICU ext 50830
Anaesthetist in charge • Footscray ext 56540• Sunshine ext 53021
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
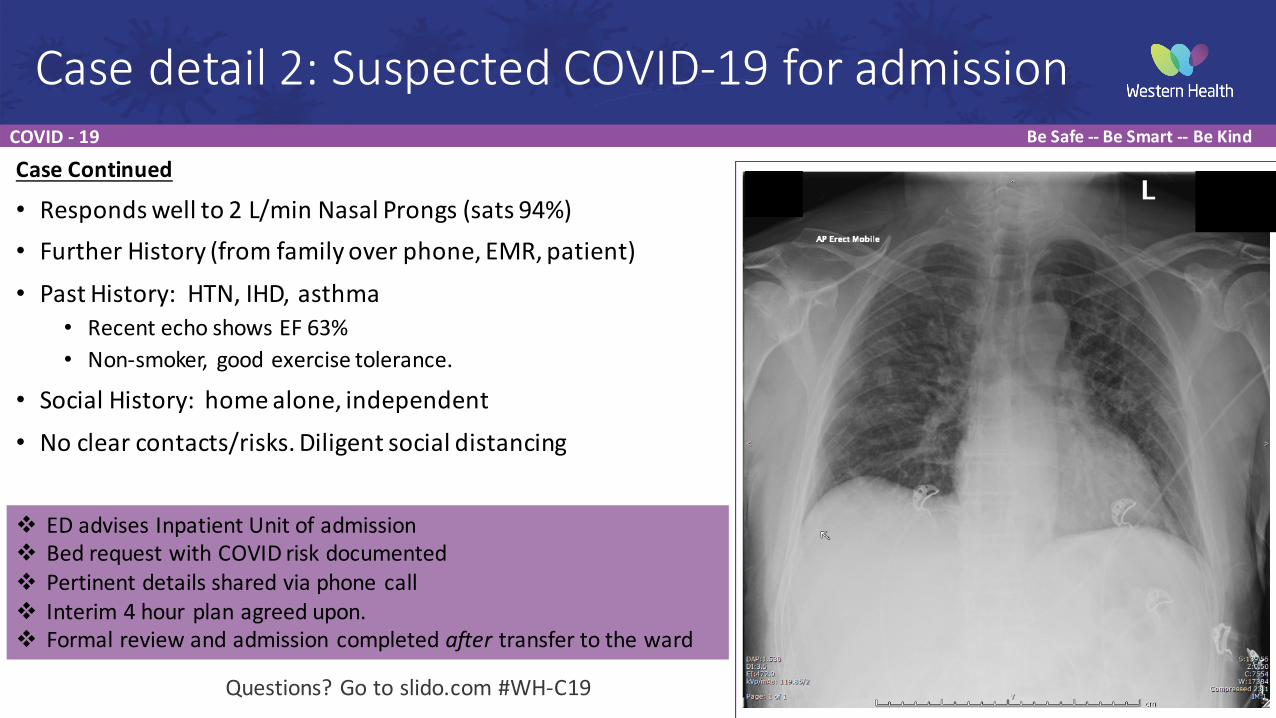
Case Continued
• Responds well to 2 L/min Nasal Prongs (sats 94%)• Further History (from family over phone, EMR, patient) • Past History: HTN, IHD, asthma
• Recent echo shows EF 63%• Non-‐smoker, good exercise tolerance.
• Social History: home alone, independent• No clear contacts/risks. Diligent social distancing
Case detail 2: Suspected COVID-‐19 for admission
v ED advises Inpatient Unit of admissionv Bed request with COVID risk documentedv Pertinent details shared via phone callv Interim 4 hour plan agreed upon. v Formal review and admission completed after transfer to the ward
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
Admission
Created by Western Health in collaboration with beauty within medicine.
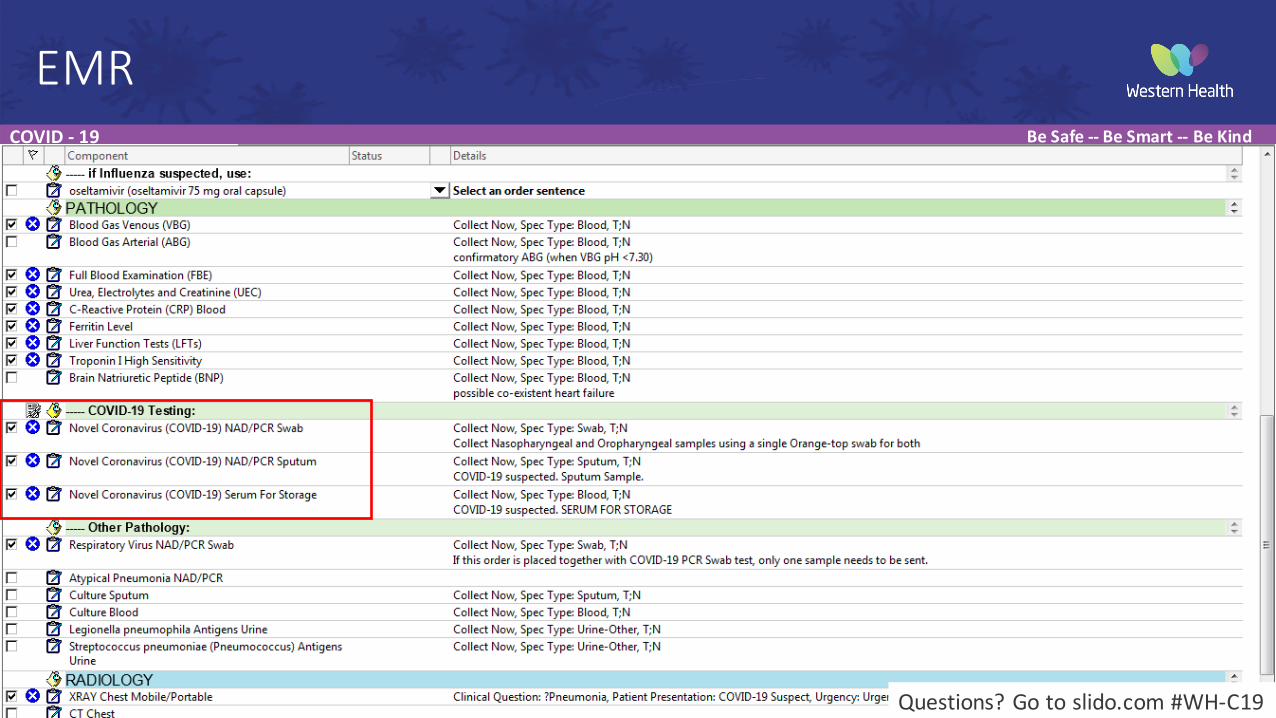
Order COVID-19 nasopharyngeal/ oropharyngeal swab PCROrder COVID-19 sputum PCR
Patient meets current COVID-19 testing criteria
NO
NO
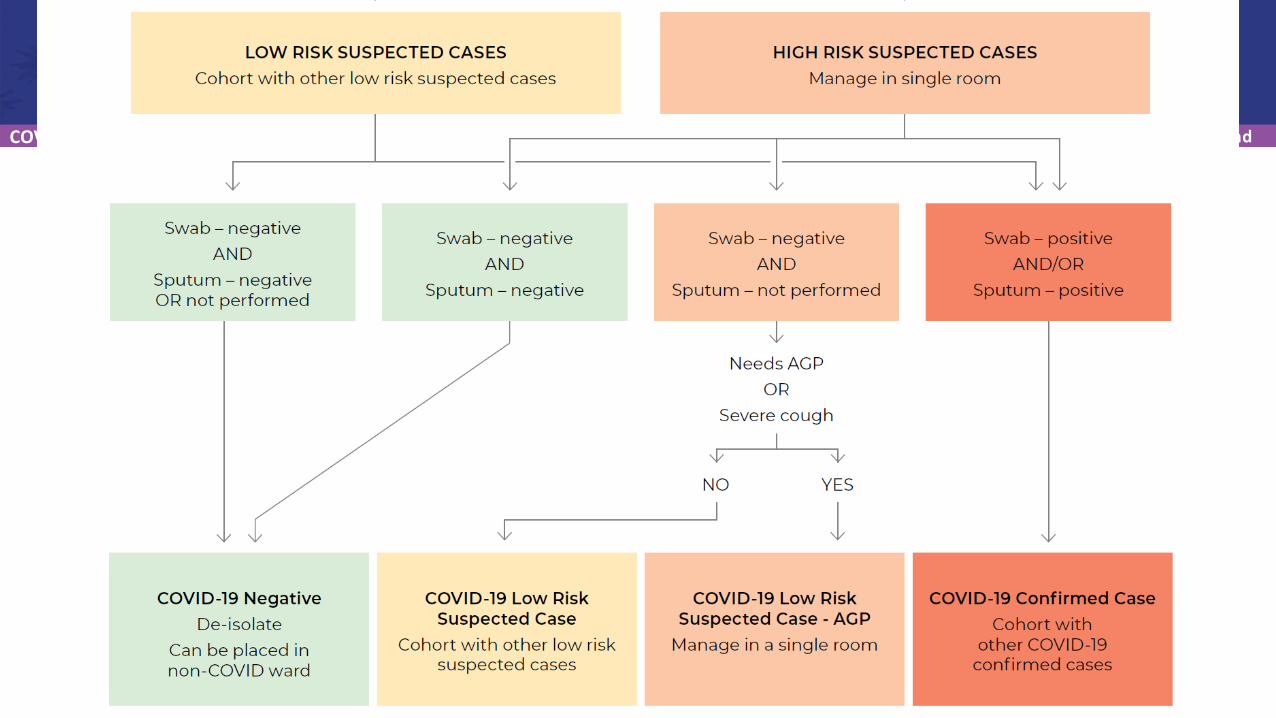
Swab – negativeAND
Sputum – negative OR not performed
COVID-19 NegativeDe-isolate
Can be placed in non-COVID ward
Swab – negativeAND
Sputum – not performed
COVID-19 Low Risk Suspected Case - AGP
Manage in a single room
Swab – negativeAND
Sputum – negative
COVID-19 Low Risk Suspected Case
Cohort with other low risk suspected cases
Swab – positiveAND/OR
Sputum – positive
COVID-19 Confirmed CaseCohort with
other COVID-19 confirmed cases
HIGH RISK SUSPECTED CASESManage in single room
YES
YES
Needs AGPOR
Severe cough
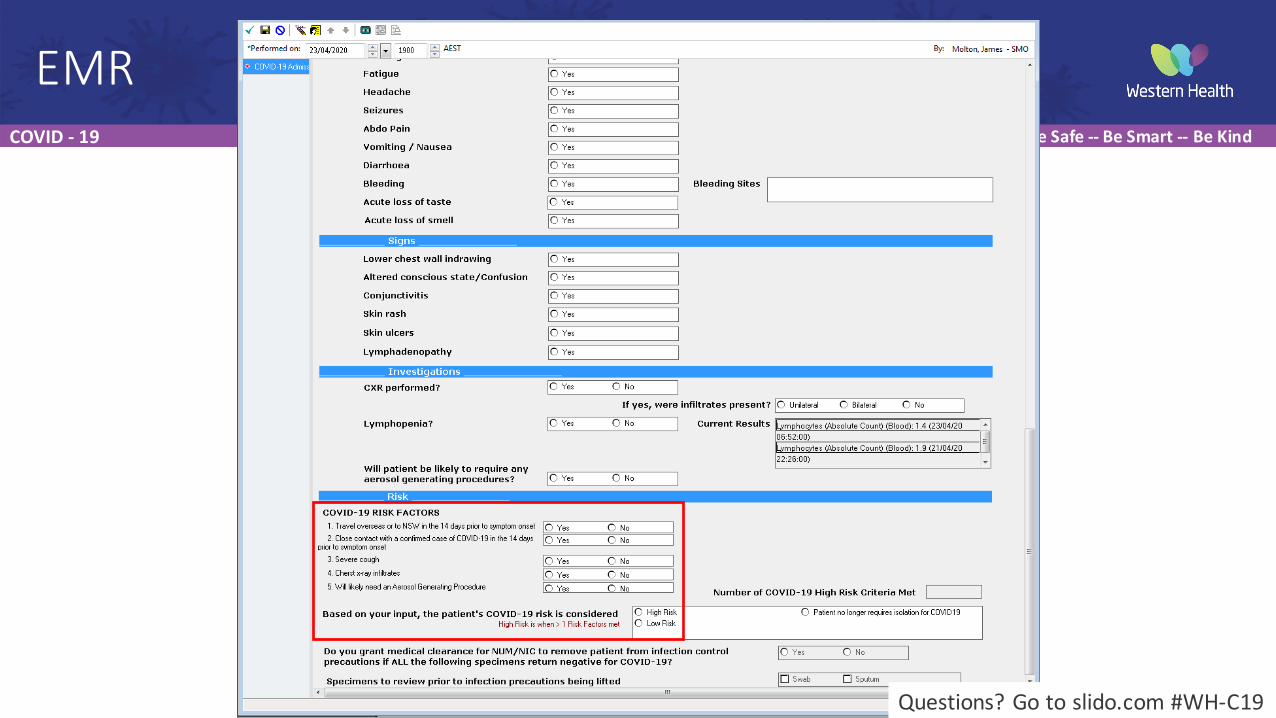
RISK ASSESSMENT (to be completed by admitting doctor)Does the patient have any of the following risk factors?1. Travel overseas or to NSW in the 14 days prior to symptom onset2. Close contact with a confirmed case of COVID-19 in the 14 days
prior to symptom onset3. Severe cough*4. Chest x-ray infiltrates5. Will likely need an Aerosol Generating Procedure (AGP)*Severe cough is defined as a new continuous cough, coughing a lot for more than an hour, or 3 or more coughing episodes in 24 hours.
LOW RISK SUSPECTED CASESCohort with other low risk suspected cases
Risk Assessment, De-isolation and Cohorting of Inpatients Tested for COVID-19
CLINICAL ASSESSMENT
MILD MODER ATE SEVERE
NORMAL NORMAL NORMAL or DECREASED
NORMAL MILD SEVERE
< 20 20 - 30 > 30
> 94% on room air OR baseline for the patient
Requiring supplemental oxygen Sats critical or requiring >40% FiO2
CRITICALReduced GCS , shock and/or other
signs of other end organ failure
HOME +/- HOSPITAL IN THE HOME (HITH)If positive, notify DHHS for
routine follow-up
INTENSIVE CARE UNIT (ICU)WARD
Not for ICU
End of life care (EOLC)
ASKDoes this patient have the ability, understanding
and resources to self-isolate?
ADMITAdmit to most appropriate unit**
• Complete EMR admission template (via medical officer tab) including risk assessment
• Admitting team MUST complete an acute resuscitation plan (ARP).
• COVID-19 order set*• AVOID: nebulisers, high flow nasal
prongs (HFNP), non-invasive ventilation (NIV). For more information see ward
management guidelines
ASSESSDetermine resuscitation status
Not for intubation
YES
For intubation
NO
Follow criteria for isolation
step-down
SUPPORTIVE CARESee safe use of respiratory guideline
DETERIORATESHighest risk: Day 5 to 8
EM
ER
GE
NC
Y D
EP
AR
TME
NT (E
D)
PR
OG
RE
SSC
AR
E LO
CA
TION
PATIENTS IN ED WITH SUSPECTED OR CONFIRMED COVID-19
IMPROVES DETERIORATESHighest risk: Day 5 to 8 • Reduced GCS • Severe WOB• Clinical concern• Rapid deterioration• RR > 24• Sats < 92% despite
6L/min or 40% FiO2
CRISIS MODE
GCS
WOB
RR
SaO2
Created by Western Health in collaboration with beauty within medicine.
GCS = Glasgow coma scale, WOB = work of breathing, RR = respiratory rate, SaO2 = oxygen saturations*FBE, UEC, LFT, CRP, D-Dimer, Troponin, Ferritin, VBG, Blood cultures, COVID-19 swab, influenza swab, CXR (mobile).**General Medicine, Respiratory, Acute Aged Care unless otherwise known to a specialty unit. See admitting guidelines.
Refer to ICU +/- activate intubation team
For ICU
CALL INTUBATION TEAM
Refer to ICU +/- activate intubation team
• Footscray ICU ext 56093 • Sunshine ICU ext 50830
Anaesthetist in charge • Footscray ext 56540• Sunshine ext 53021
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
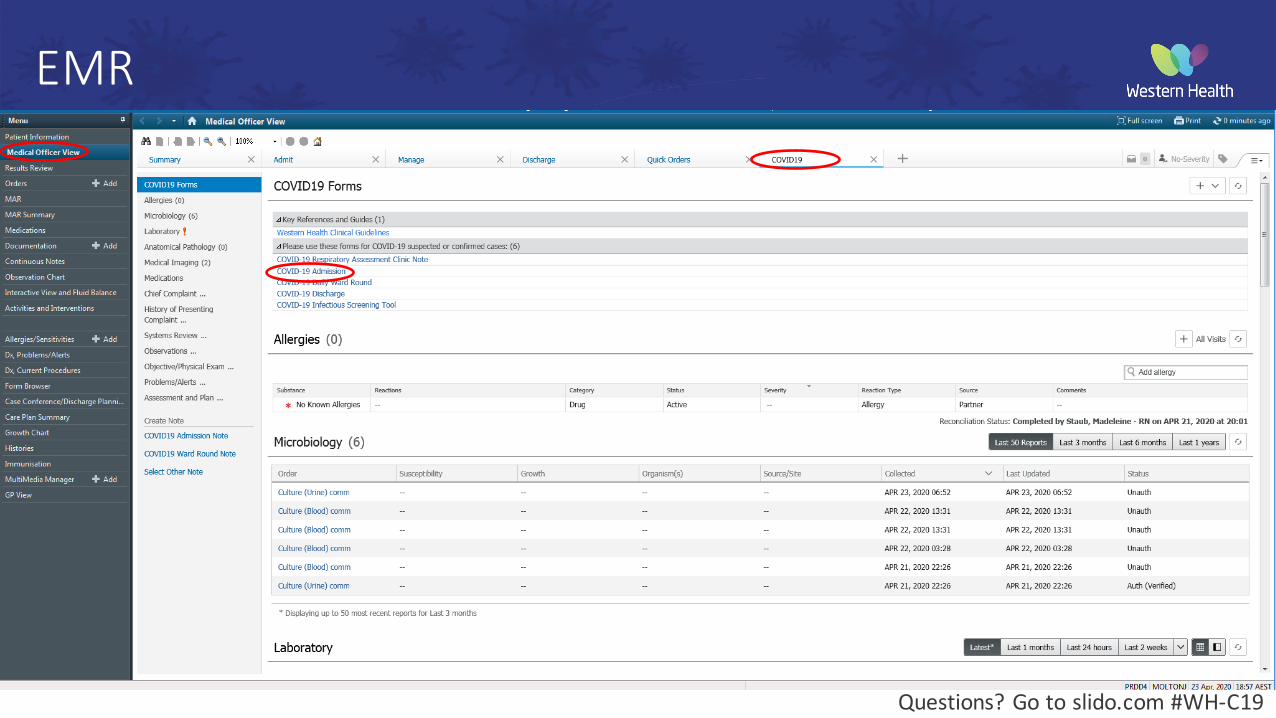
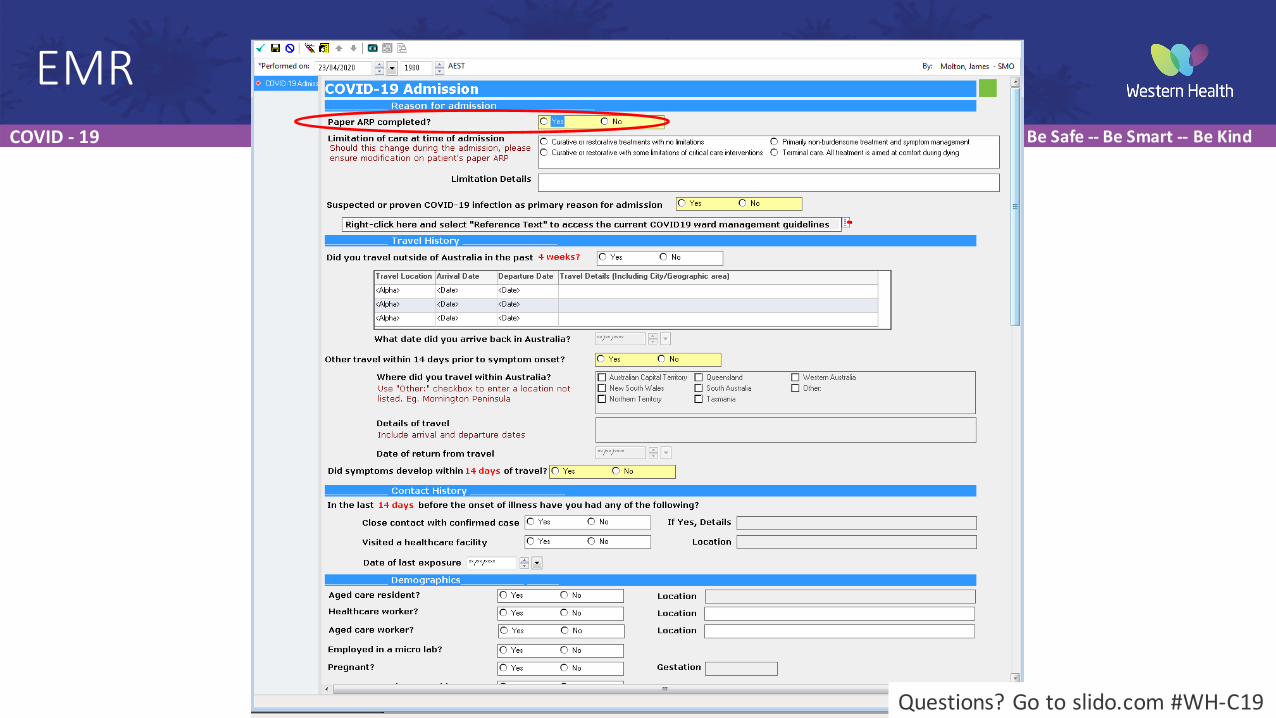
EMR
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
EMR
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
EMR
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
EMR
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
EMR
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
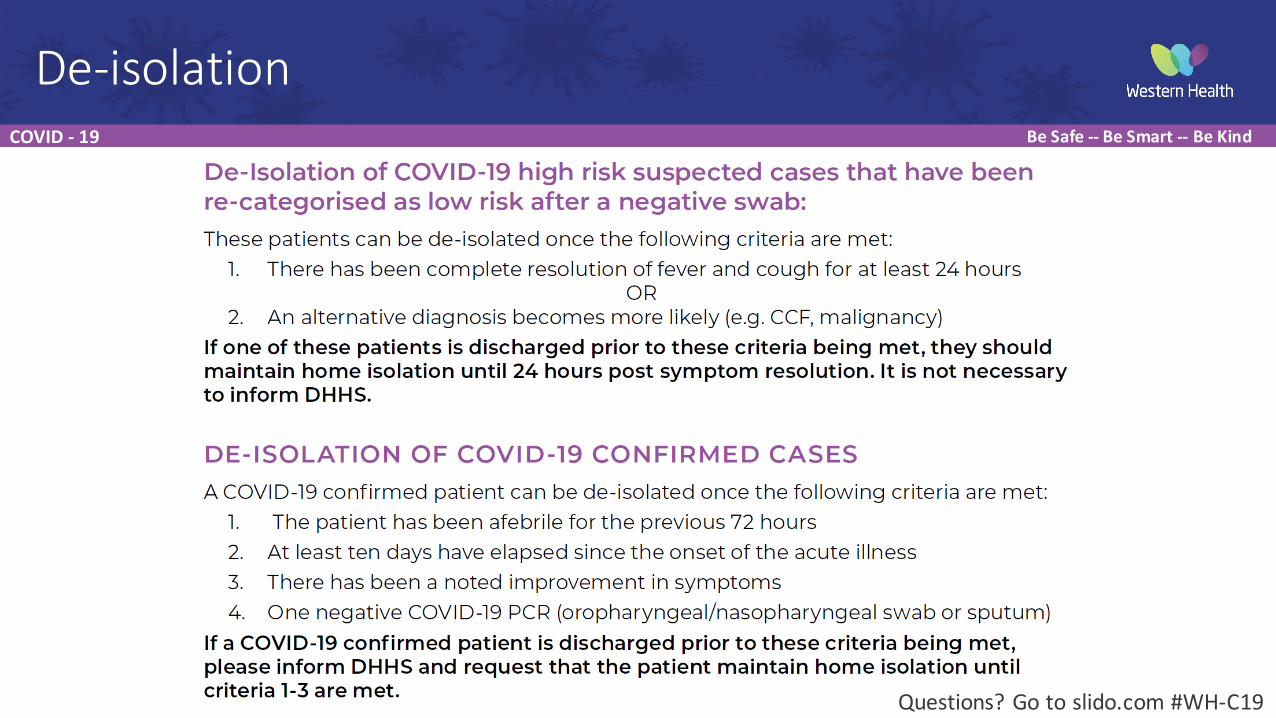
De-‐isolation
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
Fluids – run them dry• Restrictive fluid strategies, 1-‐2 litres of IV fluid per day (if no oral intake, acute kidney injury or clinically dehydrated)
• If hypotensive, give up to 3 x 250ml fluid boluses then call ICU
Indications for antibiotics – treat as CAP• hypoxaemic (oxygen saturation <92% on room air) • pleural effusion (uncommon, assess alternative cause) • purulent (yellow/green) sputum
Antiviral agents – not yet• Currently no RCT evidence of benefit (and potential exists for harm)• Avoid use outside context of a trial
Principles of ward management
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
Created by Western Health in collaboration with beauty within medicine.
Not achieving target O2 sat
Not achieving target O2 sat
Not achieving target O2 sat
Not achieving target O2 sat
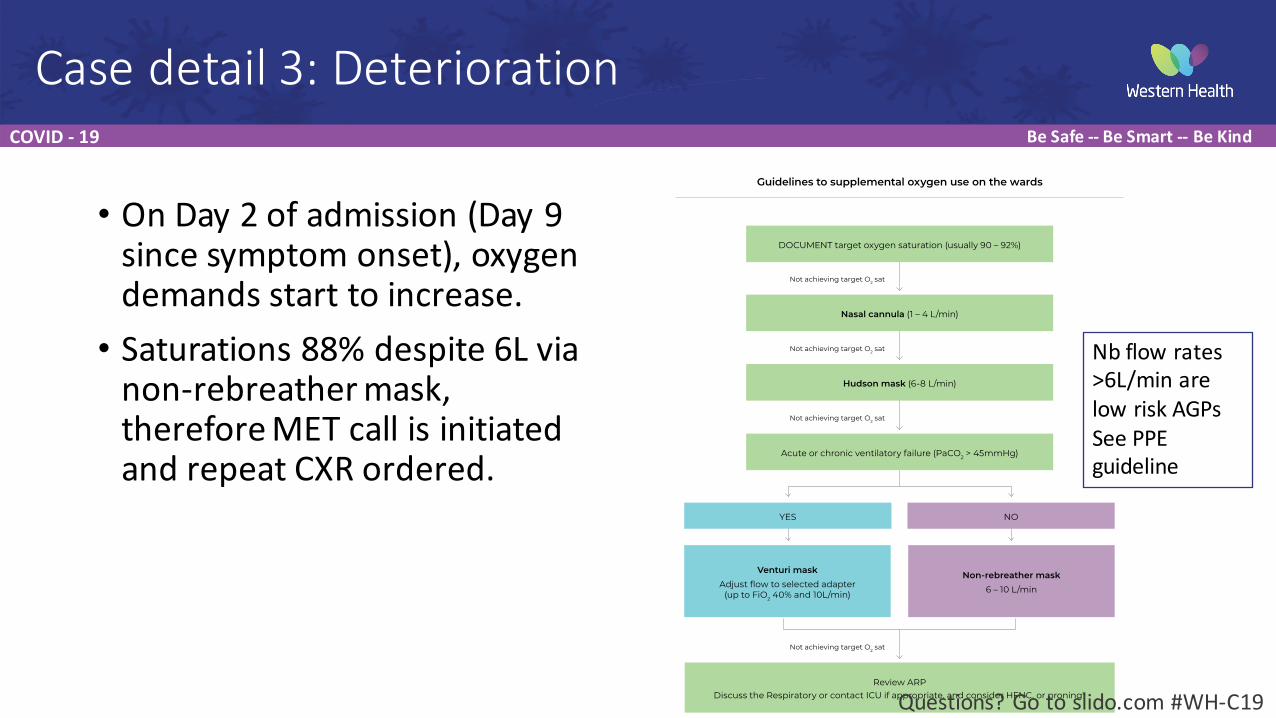
Guidelines to supplemental oxygen use on the wards
DOCUMENT target oxygen saturation (usually 90 – 92%)
Nasal cannula (1 – 4 L/min)
Hudson mask (6-8 L/min)
Acute or chronic ventilatory failure (PaCO2 > 45mmHg)
Review ARPDiscuss the Respiratory or contact ICU if appropriate, and consider HFNC, or proning*
NO
Non-rebreather mask6 – 10 L/min
YES
Venturi maskAdjust flow to selected adapter
(up to FiO2 40% and 10L/min)
ARP = acute resuscitation plan, ICU = intensive care unit, HFNC = high flow nasal cannula
*There is new evidence suggesting that HFNC may assist in oxygenating the patient with COVID-19. However approval requirements persist. Talk to respiratory/ICU for more information.
Case detail 3: Deterioration
• On Day 2 of admission (Day 9 since symptom onset), oxygen demands start to increase.• Saturations 88% despite 6L via non-‐rebreather mask, therefore MET call is initiated and repeat CXR ordered.
Questions? Go to slido.com #WH-‐C19
Nb flow rates >6L/min are low risk AGPsSee PPE guideline
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
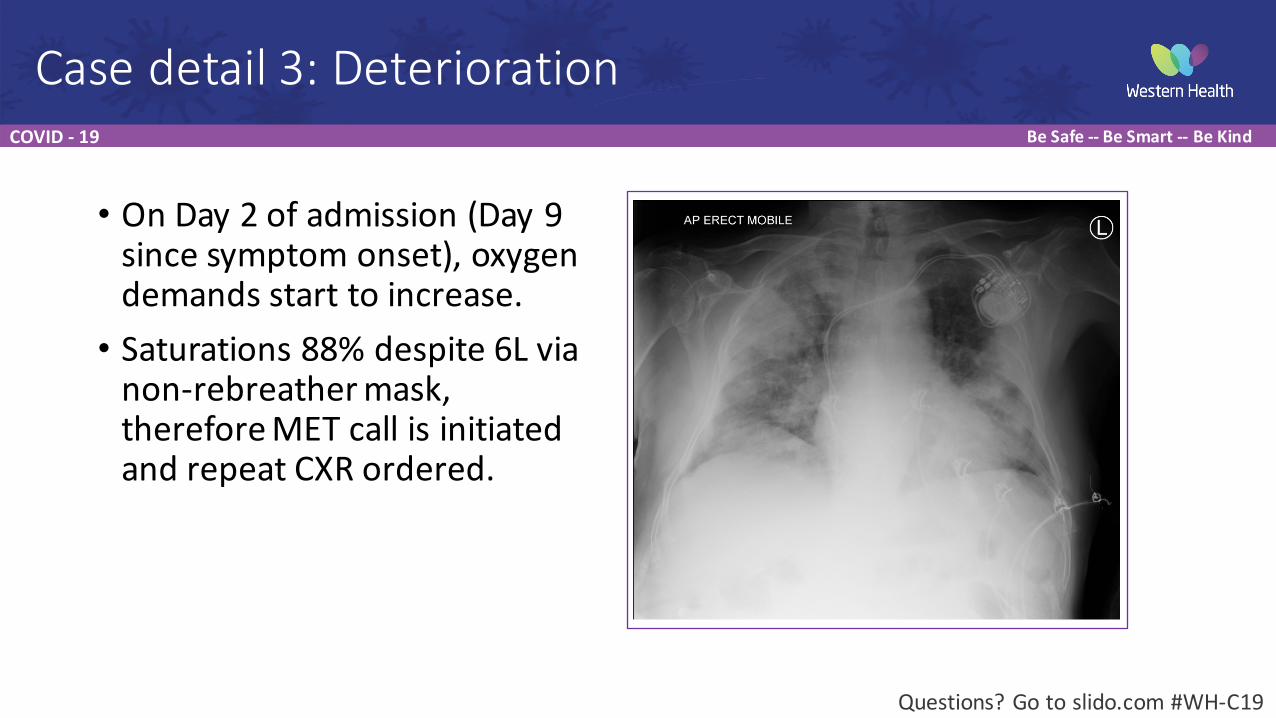
Case detail 3: Deterioration
• On Day 2 of admission (Day 9 since symptom onset), oxygen demands start to increase.• Saturations 88% despite 6L via non-‐rebreather mask, therefore MET call is initiated and repeat CXR ordered.
Ward CXR
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
CLINICAL ASSESSMENT
MILD MODER ATE SEVERE
NORMAL NORMAL NORMAL or DECREASED
NORMAL MILD SEVERE
< 20 20 - 30 > 30
> 94% on room air OR baseline for the patient
Requiring supplemental oxygen Sats critical or requiring >40% FiO2
CRITICALReduced GCS , shock and/or other
signs of other end organ failure
HOME +/- HOSPITAL IN THE HOME (HITH)If positive, notify DHHS for
routine follow-up
INTENSIVE CARE UNIT (ICU)WARD
Not for ICU
End of life care (EOLC)
ASKDoes this patient have the ability, understanding
and resources to self-isolate?
ADMITAdmit to most appropriate unit**
• Complete EMR admission template (via medical officer tab) including risk assessment
• Admitting team MUST complete an acute resuscitation plan (ARP).
• COVID-19 order set*• AVOID: nebulisers, high flow nasal
prongs (HFNP), non-invasive ventilation (NIV). For more information see ward
management guidelines
ASSESSDetermine resuscitation status
Not for intubation
YES
For intubation
NO
Follow criteria for isolation
step-down
SUPPORTIVE CARESee safe use of respiratory guideline
DETERIORATESHighest risk: Day 5 to 8
EM
ER
GE
NC
Y D
EP
AR
TME
NT (E
D)
PR
OG
RE
SSC
AR
E LO
CA
TION
PATIENTS IN ED WITH SUSPECTED OR CONFIRMED COVID-19
IMPROVES DETERIORATESHighest risk: Day 5 to 8 • Reduced GCS • Severe WOB• Clinical concern• Rapid deterioration• RR > 24• Sats < 92% despite
6L/min or 40% FiO2
CRISIS MODE
GCS
WOB
RR
SaO2
Created by Western Health in collaboration with beauty within medicine.
GCS = Glasgow coma scale, WOB = work of breathing, RR = respiratory rate, SaO2 = oxygen saturations*FBE, UEC, LFT, CRP, D-Dimer, Troponin, Ferritin, VBG, Blood cultures, COVID-19 swab, influenza swab, CXR (mobile).**General Medicine, Respiratory, Acute Aged Care unless otherwise known to a specialty unit. See admitting guidelines.
REFER TO ICU +/- ACTIVATE INTUBATION TEAM
For ICU
REFER TO ICU +/- ACTIVATE INTUBATION TEAMCall ICU department at hospital location:
• Footscray ICU ext 56093 • Sunshine ICU ext 50830
Call anaesthetist in charge • Footscray ext 56540 • Sunshine ext 53021
MET Calls
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
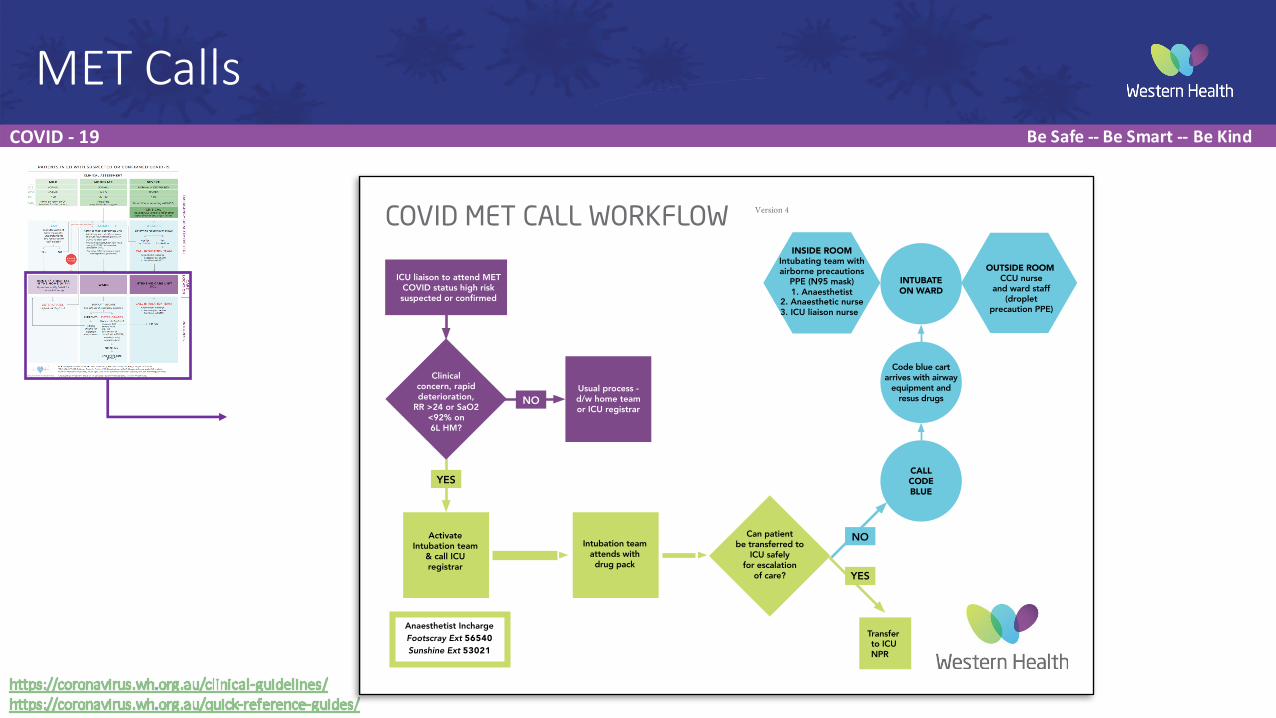
MET Calls
ICU liaison to attend MET COVID status r sk suspected or con r ed
Clinicalconcern, rapiddeterioration,
RR >24 or SaO2 <92% on 6L HM?
Anaesthetist Incharge Footscray Ext 56540 Sunshine Ext 53021
Activate Intubation team
& call ICU registrar
Usual process -d/w home team or ICU registrar
Intubation teamattends with drug pack
Can patient be transferred to
ICU safely for escalation
of care?
Transfer to ICU
CALL
CODE
BLUE
Code blue cartarrives with airway
equipment and resus drugs
INTUBATE
ON WARD
INSIDE ROOM
Intubating team with airborne precautions
PPE (N95 mask)1. Anaesthetist
2. Anaesthetic nurse3. ICU liaison nurse
OUTSIDE ROOM CCU nurse
and ward staff (droplet
precaution PPE)
NO
YES
YES
NO
COVID MET CALL WORKFLOW
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
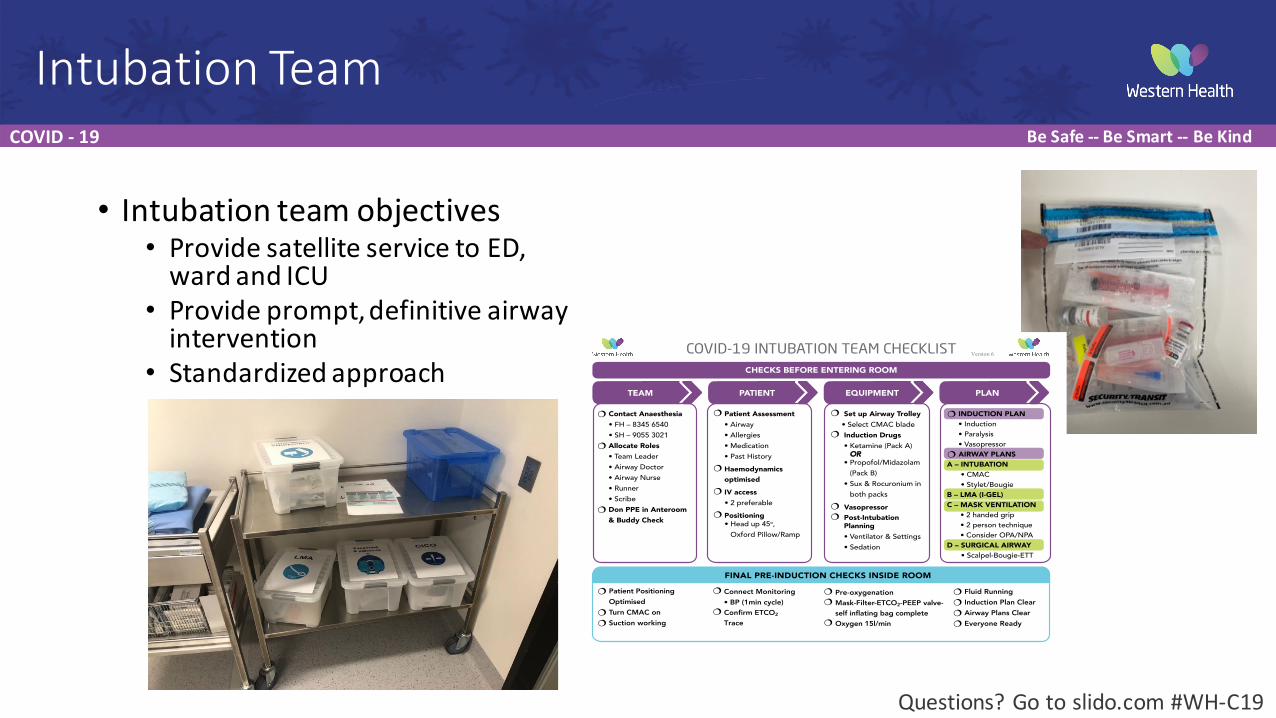
• Intubation team objectives• Provide satellite service to ED, ward and ICU
• Provide prompt, definitive airway intervention
• Standardized approach
Intubation Team
COVID-19 INTUBATION TEAM CHECKLIST
PATIENT EQUIPMENT PLAN
¦ Set up Airway Trolley• Select CMAC blade
¦ Induction Drugs• Ketamine (Pack A) OR
• Propofol/Midazolam (Pack B)
• Sux & Rocuronium in both packs
¦ Vasopressor¦ Post-Intubation
Planning• Ventilator & Settings
• Sedation
¦ Patient Assessment• Airway
• Allergies
• Medication
• Past History
¦ Haemodynamics optimised
¦ IV access• 2 preferable
¦ Positioning• Head up 45o,
Oxford Pillow/Ramp
� Contact Anaesthesia• FH – 8345 6540
• SH – 9055 3021
� Allocate Roles• Team Leader
• Airway Doctor
• Airway Nurse
• Runner
• Scribe
� Don PPE in Anteroom& Buddy Check
� INDUCTION PLAN• Induction
• Paralysis
• Vasopressor
� AIRWAY PLANSA – INTUBATION
• CMAC
• Stylet/Bougie
B – LMA (I-GEL)C – MASK VENTILATION
• 2 handed grip
• 2 person technique
• Consider OPA/NPA
D – SURGICAL AIRWAY • Scalpel-Bougie-ETT
� Patient PositioningOptimised
� Turn CMAC on� Suction working
¦ Connect Monitoring• BP (1min cycle)
¦ Confirm ETCO2 Trace
¦ Pre-oxygenation¦ a - ilter-ETCO2-PEEP al e-
elf inflating ag com lete¦ Oxygen 15l/min
� Fluid Running� Induction Plan Clear� Airway Plans Clear� E eryone ea y
CHECKS BEFORE ENTERING ROOM
FINAL PRE-INDUCTION CHECKS INSIDE ROOM
TEAM
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
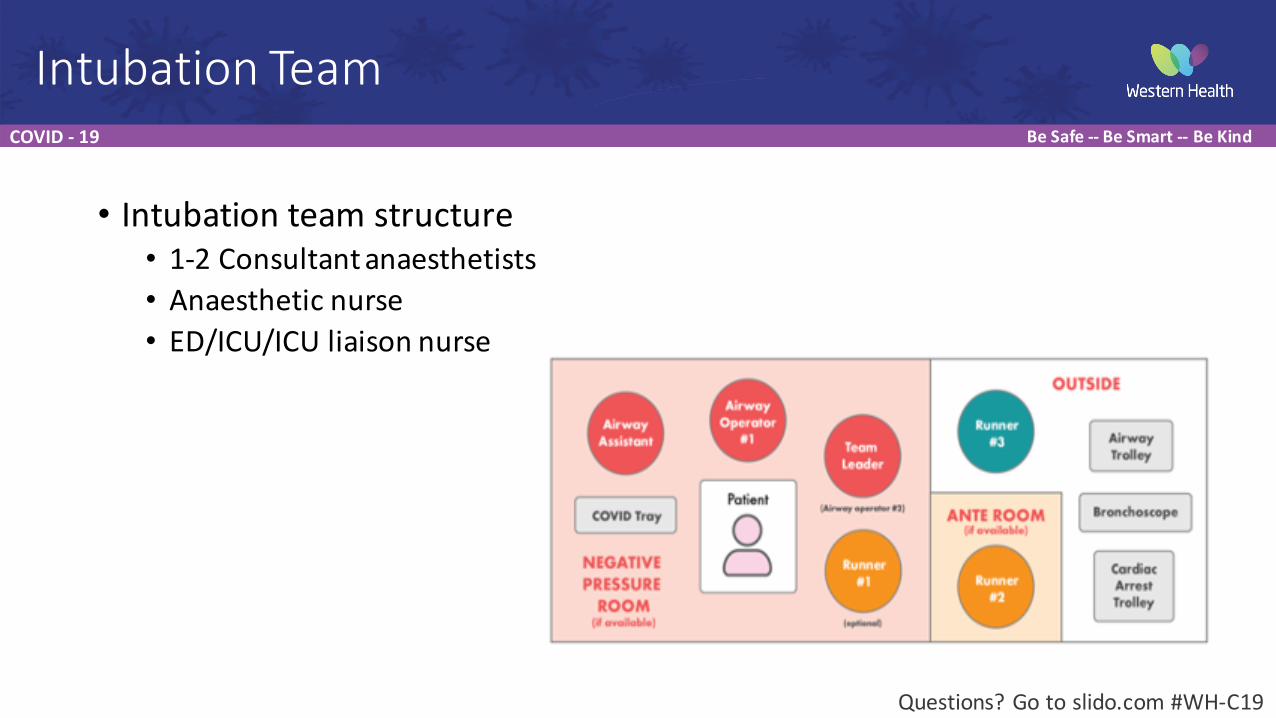
• Intubation team structure• 1-‐2 Consultant anaesthetists• Anaesthetic nurse• ED/ICU/ICU liaison nurse
Intubation Team
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
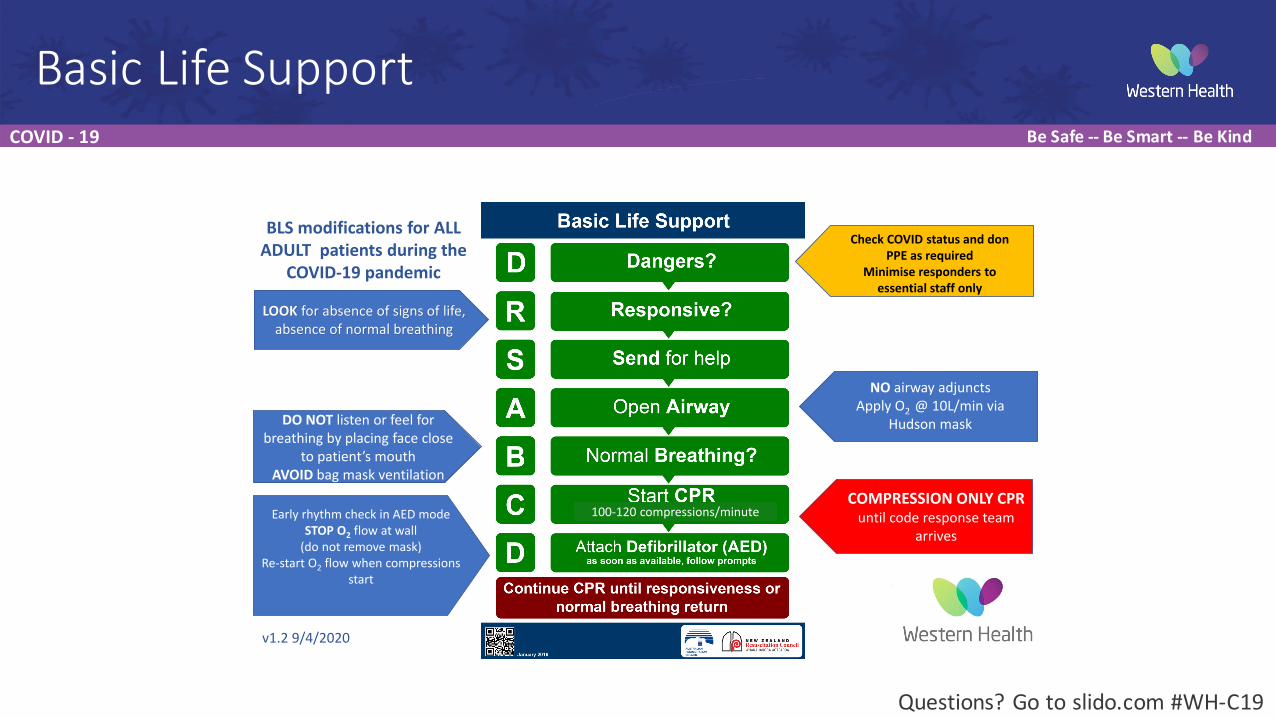
Basic Life Support
LOOK for absence of signs of life,
absence of normal breathing
Check COVID status and don PPE as required
Minimise responders to essential staff only
NO airway adjuncts
Apply O2 @ 10L/min via
Hudson maskDO NOT listen or feel for
breathing by placing face close
to patient’s mouthAVOID bag mask ventilation
COMPRESSION ONLY CPR until code response team
arrives
Early rhythm check in AED mode
STOP O2 flow at wall
(do not remove mask)
Re-start O2 flow when compressions
start
100-120 compressions/minute
BLS modifications for ALL ADULT patients during the
COVID-19 pandemic
v1.2 9/4/2020
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
• If not for intubation-‐ what then?• Supportive management• Consider Palliation
• Consult service only, due to hospital wide limitation on transport of patients• Due to risk to staff and public, community palliative care would not be available
• Can be considered on case by case basis
Palliation
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
• Submit questions to slido.com #WH-‐19
• Special thanks to Dr Lucy Desmond from Beauty Within Medicine for her assistance with graphics
• Next week: Dr Richard Horton speaks about the roll out of telehealth in our clinics
Questions
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
Questions
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
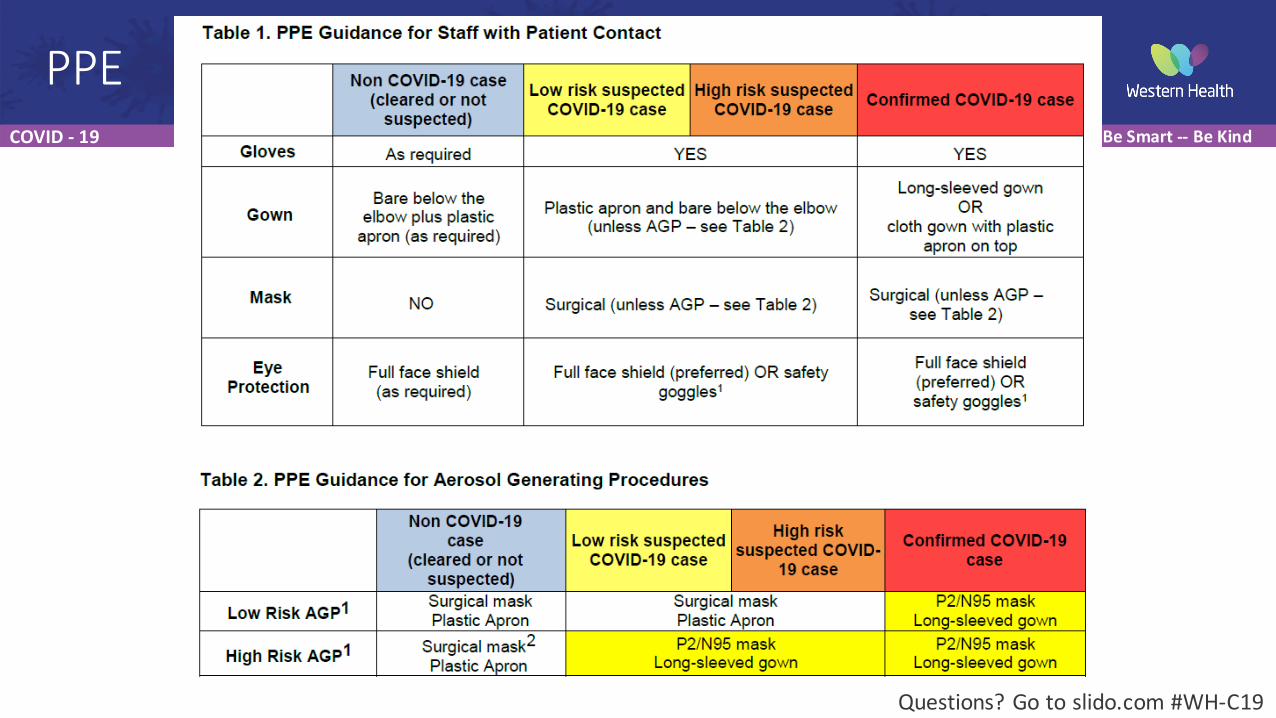
PPE
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
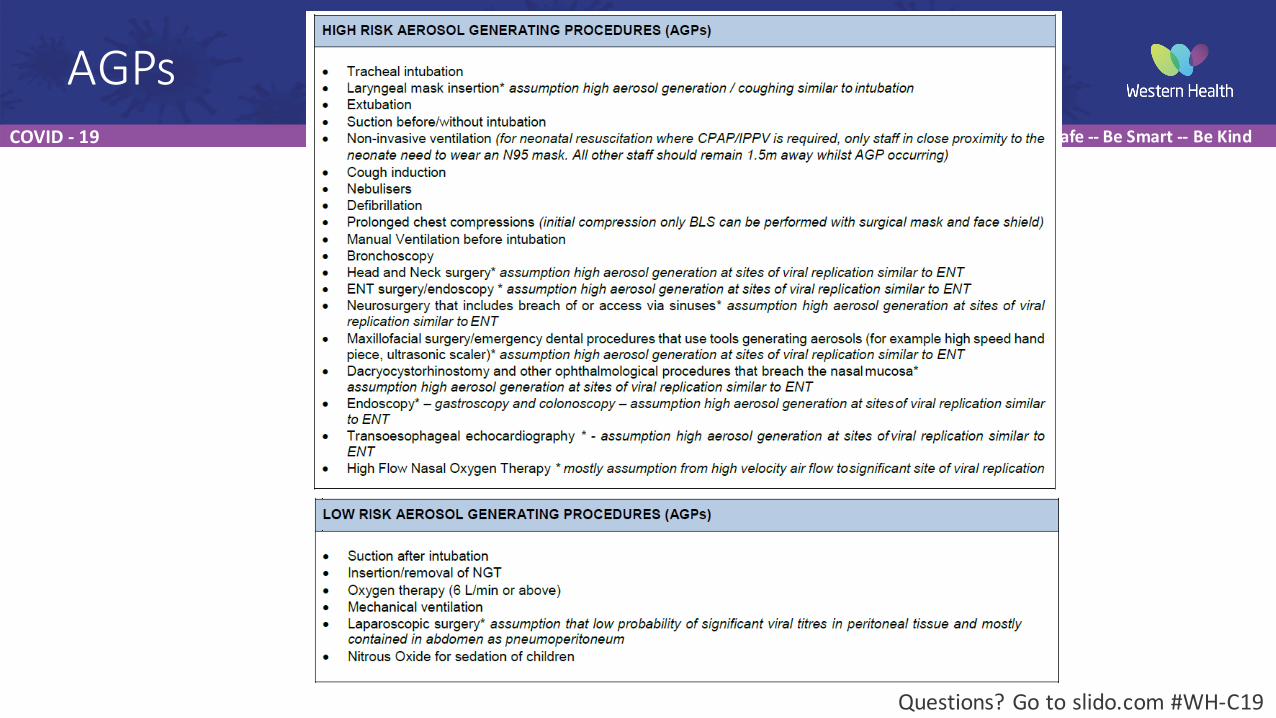
AGPs
Questions? Go to slido.com #WH-‐C19
COVID -‐ 19 Be Safe -‐-‐ Be Smart -‐-‐ Be Kind
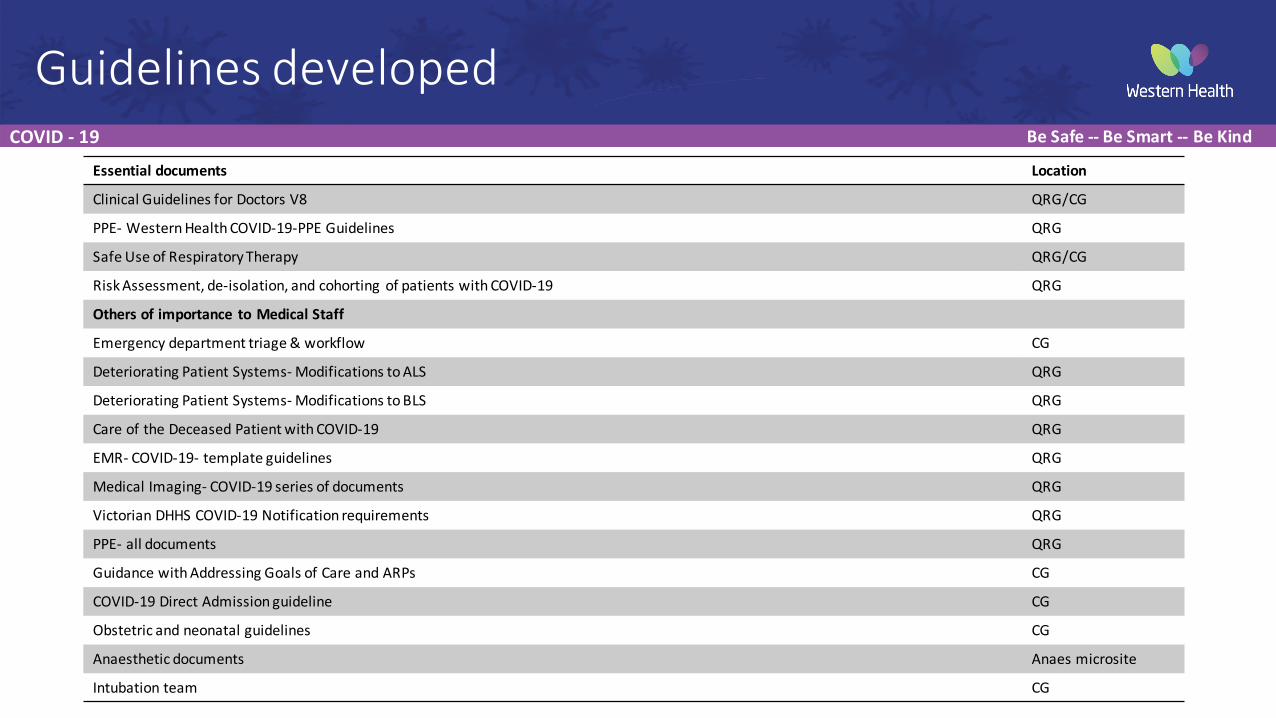
Essential documents Location
Clinical Guidelines for Doctors V8 QRG/CG
PPE-‐ Western Health COVID-‐19-‐PPE Guidelines QRG
Safe Use of Respiratory Therapy QRG/CG
Risk Assessment, de-‐isolation, and cohorting of patients with COVID-‐19 QRG
Others of importance to Medical Staff
Emergency department triage & workflow CG
Deteriorating Patient Systems-‐ Modifications to ALS QRG
Deteriorating Patient Systems-‐ Modifications to BLS QRG
Care of the Deceased Patient with COVID-‐19 QRG
EMR-‐ COVID-‐19-‐ template guidelines QRG
Medical Imaging-‐ COVID-‐19 series of documents QRG
Victorian DHHS COVID-‐19 Notification requirements QRG
PPE-‐ all documents QRG
Guidance with Addressing Goals of Care and ARPs CG
COVID-‐19 Direct Admission guideline CG
Obstetric and neonatal guidelines CG
Anaesthetic documents Anaes microsite
Intubation team CG
Guidelines developed