Embed Size (px)
Citation preview

The Oedematous Mr H
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H
Student Grand Round 09.12.2003

HISTORY
Mr H 58 yr old taxi driver
PC• 3/12 Hx persistent productive cough, with yellow sputum production
HPC
• Abx – relieved symptoms initially, however cough returned coinciding with ‘flu jab
• Pt was sent for CXR & subsequently referred to Rapid Access Chest Clinic
• Symptoms/ signs on presentation Cough and sputum production 7 kg weight loss over 3/12 Fatigue over 2/52, which has stopped Pt working Difficulty swallowing solids over 3-4/52 6/7 Hx facial swelling & mild headache SOB:
Worsens at night, but no orthopnea (sleeps with 2 pillows) Onset after walking ~100 yards
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

HISTORY
PMH• Rheumatic fever as a child• Early 1980’s – Frozen shoulder, treated conservatively• Mid 1980’s
Dx Diabetes Mellitus Type II following 1yr Hx paraesthesia on dorsal aspect of both feet Blood tests also highlighted some degree of liver dysfunction, managed conservatively – Pt ↓ alcohol intake
• August 1999 – MI• May 2000 – MI• Angina – drug managed• Stress headaches• ºAllergies
DH• Lanspoprazole 30mg od• Asprin 75mg od• Isosorbide Mononitrate 10mg bd• GTN spray• Fenofibrate 267mg od
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

HISTORY
SE
• CVS - Angina (drug managed), nil of note
• Resp - Difficulty with full inspiration – “taking a full deep breath in”
• GI - ↓ appetite
- Weight loss since onset of cough
• GU - nil of note
• MSS - nil of note
• CNS - Peripheral neuropathy 2º to Diabetes
• THREADS
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

HISTORY
FH
• Two sons & one daughter (1st marriage).
• Now remarried, with one step son.
• Significant FHx Diabetes & Heart Failure on mother’s side.
• Father died aged 64 of lung Ca, mother died in late 80’s of Heart Failure.
SH
• Lives with 2nd wife, in 4th floor flat in Clapham.
• Flat does have lift but Pt likes to walk where possible.
• No problems with ADL.
• Smoked ~20/day for 50years; currently trying to stop but has had many previous failed quit attempts.
• Drinks ~5-6pints/wk, but previous Hx v heavy drinking (~14 bottles whiskey/wk).
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

OBSERVATIONS & EXAMINATION
• Obs PR - 85 RR - 20 BP - 130/80 Temp - 36°C BM - 6.6 General - Facial swelling and significant periorbital oedema Large palpable R cervical LN, ° palpable axillary LN Nicotine stained hands
• CVS - NAD
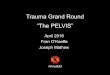
• Resp - Bronchial breathing RUL posteriorly with decreased air entry.
• GI - No palpable masses, liver, kidneys or spleen.
• Neuro - NAD
• JACCOL
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SUMMARY AND IMPRESSION
Summary
• Mr H is a 58 year old taxi driver
• Presented with Hx cough + SOB over 3/12
• O/E: Bronchial breathing RUL posteriorly with ↓ air entry and palpable R cervical LN
• Co-morbidity: Diabetes mellitus and ischaemic heart disease
• Has a 50 pack year history and has been a heavy drinker
Clinical impression prior to any Ix
1. Probable bronchial Ca, with cervical LN involvement and Superior Vena Cava Obstruction (SVCO)
2. Chronic infection
Plan
• Admit Pt
• FNA of cervical LN to determine histology
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

MANAGEMENT
• Admitted to ward under c/o Dr Rees
• Immediate management: 8mg of dexamethasone b.d.
Further tests
• CXR
• Blood test
• FNA cervical LN- SCLC confirmed by other histological tests
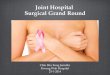
• CT scan thorax and abdomen
• Bone scan
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

CXR
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

CT 1
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

CT 2
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

BONE SCAN
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

MANAGEMENT
21/11
• Started on chemotherapy: etoposide 100mg b.d.
23/11
• Generally well
• Stable
• Symptoms improved
• Discharged
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

LUNG CANCER
• Most common cause of cancer death worldwide.
• Males>>females.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H
Un-modifiable
Gender
Race
Genetic predisposition
Modifiable
Smoking
Passive smoking
Pollution
Exposure to occupational carcinogens
Diet
Risk factors

SMALL CELL LUNG CANCER
• 15-20% of all lung ca
• Central/hilar tumours which arise from Kulchitsky cells
• Rapid onset
• Aggressive course
• Widespread metastasis
• Extremely sensitive to chemotherapy & radiotherapy
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SCLC
Symptoms:
• Cough• Chest pain• Haemoptypsis• Wheezing• Anorexia• Weight loss• Distant spread• No symptoms
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H
Signs:
• Reduced BS• Dullness to percussion• Hepatomegaly• Lymphadenopathy• Clubbing• SVCO
Paraneoplastic syndromes in SCLC:
• SIADH• Ectopic Cushing's• Rare neurological syndromes

SCLC
Investigations:
• CXR
• FBC
• U&E
• Bone scan
• CT (to include liver & adrenals)
• LFTs
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SCLC
Treatment:
• Surgery - limited in value except in limited stage disease.
• Radiation - limited as curative, but useful in prophylaxis or as palliative treatment.
• Chemotherapy - combination therapy better than single agent therapy,
standard combinations: CDV, PE, CAVE, alternating EP and CAV • Palliative treatment - for progressive non-curable SCLC.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SUPERIOR VENA CAVA SYNDROME
• Occurs when the vena cava is occluded.
• Obstruction - External (e.g. tumour, lymphadenopathy)
- Intra-luminal (e.g. tumour, thrombosis).
• Malignancy → 90% of SVCS cases. SVCS poor prognostic indicator.
• Advanced lung cancer, specifically small cell carcinoma (SCLC), accounts for 75% of malignant SVCS causes.
• Other malignant causes: Non-Hodgkins (and more rarely, Hodgkins) lymphoma, and mediastinal metastases from Breast Ca, Kaposi’s sarcoma, thymoma, fibrous mesothelioma and germ cell cancers.
• Non malignant causes: goitre, aortic aneurysm and granulomatous infection secondary to TB.
• Iatrogenic causes: venous thrombosis due to central line; fibrosis due to mediastinum radiotherapy.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SUPERIOR VENA CAVA SYNDROME
Patients with cancer at increased risk of SVCS:
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H
1. Patients with small cell lung cancer or, less frequently, non-small cell lung carcinoma (e.g. squamous cell carcinoma) and those with right lung involvement.
2. Patients with non-Hodgkins lymphoma.
3. Male patients aged 50-70 years who have primary or metastatic tumours of the mediastinum.
4. Patients with breast carcinoma and mediastinal metastasis, Kaposi’s sarcoma with mediastinal involvement, thymoma, fibrous mesothelioma, and germ cell neoplasms.
5. Patients with central venous catheters and pacemaker catheters.
6. Patients who have received previous radiation therapy to the mediastinum.
7. Patients with cancer who have comorbid conditions such as tuberculosis, histoplasmosis, or aortic aneurysm.

SUPERIOR VENA CAVA SYNDROME
Common presenting symptoms of SVCS:
• Dyspnoea (most common symptom) and non-productive cough.
• Swelling of the face, arms, fingers, or neck (usually the first sign, often subtle).
• Feeling of fullness of the head.
• Difficulty buttoning shirt collars (Stoke's sign); women also may experience breast swelling.
• Dysphagia and hoarseness.
• Chest pain.
Later symptoms that may occur include:
• Life-threatening symptoms of respiratory distress, such as orthopnoea.
• Headache, visual disturbances, dizziness, and syncope.
• Lethargy, irritability, and mental status changes.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SUPERIOR VENA CAVA SYNDROME
Common clinical signs elicited on examination:
• Oedema of the face, neck, upper thorax, breasts, and upper extremities.
• Prominent venous pattern (i.e., dilated veins of face, neck, and thorax).
• Jugular vein distension.
• Periorbital oedema and redness and oedema of conjunctivae.
• Facial plethora (ruddy complexion of face or cheeks).
• Compensatory tachycardia.
Clinical signs indicating progression of SVCS:
• Cyanosis of the face or upper torso.
• Engorged conjunctivae.
• Mental status changes.
• Tachypnoea, orthopnoea, stridor, and respiratory distress.
• Stupor, coma, seizure, and death.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

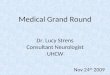
SUPERIOR VENA CAVA SYNDROME
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H
1. Dilated veins on neck and chest.
2. Jugular engorgement.
4. Suffused (flushed) face.
5. Tongue angiomata.
3. Oedema and conjunctival haemorrhage.

SUPERIOR VENA CAVA SYNDROME
Diagnosis concerned with identifying cause of SVCS:
• Identify obstruction of SVCS → CXR and trunk CT.
• History indicative of diseases previously mentioned directly (e.g. lung cancer) or via risk factors (e.g. heavy smoker) → carry out appropriate investigations.
• Dx Lung cancer → sputum cytology; lymph node biopsy/FNA histology.
Aims:
• Relief of SVC obstruction.
• Restoration of normal SVC flow and/or development of collateral pathways of venous blood flow.
• Relief of oedema and associated symptoms.
• Cure, halt or slow progression of underlying pathology.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SUPERIOR VENA CAVA SYNDROME
Management:
• Dyspnoea: Elevate head of bed, provide O2.
• IV access: ↓ flow rate in upper thorax, arms and head contra-indicated for venepuncture and IV. Central line required.
• Fluid: Fluid and electrolyte balance should be monitored as over-hydration may exacerbate the symptoms. Diuretic use also monitored.
• Blood pressure: Compression on the upper arm from BP cuff avoided.
• Side-effects of treatment: Treatment has multiple diverse side-effects. Many of these side-effects may be more uncomfortable than the patients’ own experience of SVCS. Symptomatic relief → treatments more bearable.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SUPERIOR VENA CAVA SYNDROME
Treatment:
• Pharmacotherapy: Corticosteroids (prednisolone or dexamethasone) and diuretics used to reduce oedematous swelling, inflammation and fluid load. Thrombolysis in obstruction of SVC by thrombus. Anticoagulant therapy to deter malignancy-induced thrombus is controversial.
• Radiotherapy: Local treatment of non-small cell lung and other malignancies. Symptom relief 85-90% patients within 3/52. Radiotherapy vs chemotherapy in ↓ SVCS symptoms is controversial.
• Chemotherapy: Local and systemic treatment of malignancies. Most common regimen for small cell lung cancer is a platinum-based compound (cisplatin, carboplatin) with etoposide. Relief of symptoms usually occurs within 7-14 days in most patients.
• Surgery: SVC stent insertion or bypass are occasional interventions. Secondary to other modalities.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SUPERIOR VENA CAVA SYNDROME
Cochrane review:
• Radiotherapy & chemotherapy VS surgical stent insertion VS steroids.
• SVCS present at diagnosis in 10% patients with SCLC (small cell lung carcinoma) and 1.7% NSCLC (non small cell lung carcinoma).
• SCLC - chemotherapy and/or radiotherapy symptom relief - 77%.
- recurrence rate - 17%.
• NSCLC - chemotherapy and/or radiotherapy symptom relief - 60%.
- recurrence rate - 19%.
• Stent insertion relieved symptoms in 95%, with a recurrence rate of 11%.
Rate of symptom relief was greater than other modalities.
Primary treatment option, or best-suited for treatment resistant cases?
• Not sufficient evidence concerning steroids.
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

SUPERIOR VENA CAVA SYNDROME
Outcome:
• Dependent upon prognostic factors of underlying pathology.
• Radiotherapy with chemotherapy - 50%-90% effective in ↓ SVCS.
• Evidence of ↑ effectiveness utilising both modalities if disease not responsive to either given alone.
• 70% treated remain SVCS-free prior to death.
• Recurrence of SVCS after initial treatment → poor prognosis.
• Severity and outcome of SVCS not good predictors of underlying pathology (e.g. tumour size, thrombus resolution).
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H

END OF PRESENTATION
• Questions?
Student Grand Round 09.12.2003 - Dr Rees’ Firm: C. Tucker, I. Rajkomar & R. Green
The Oedematous Mr H