Embed Size (px)
Citation preview

Eddy Lo
Department of SurgeryUCH
Joint Hospital Grand Round

Sclerotherapy for thyroid cysts

Outline
Background information on thyroid cysts
Treatment modalities
Sclerotherapy
Conclusion

Thyroid cysts
Thyroid nodule is a common clinical problem
6-26% of solitary thyroid nodules are cystic lesions
Often benign ( 0.9 to 10% malignant)Most derived from hyperplastic nodulesCauses
Haemorrhage into and degeneration of a pre-existing nodule
Retention cystsInfarcted adenomaHuge follicles
Miller JM et al 1981De Los Santos ET et al 1990Yasuda K et al 1992

Thyroid nodule

Treatment
IndicationsSymptomaticCosmesisPatient’s preference
Modalitiessimple aspirationsurgerypercutaneous sclerotherapy

Simple aspiration
Satisfactory non-operative treatment
Fluid sent for cytological examination
Recurrence rate varies from 10-80%
Crile GJ 1966Jensen F et al 1976

Surgery
Usually hemithyroidectomyCurativeDefinite histologyGA risksSurgical risks
BleedingWound CxScarRLN injury

Sclerotherapy for thyroid cysts
Minimal invasive procedureGeneral anaesthesia not requiredDone as day caseMinimal side effectsEasy to performCan be repeatedLow cost

Methods
USG guided FNA of the cyst
Followed by injection of the sclerosant
No anaesthesia required
FU with USG
Procedure will be repeated if necessary

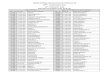
USG image of normal thyroid gland

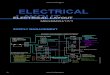
Thyroid cyst




Agents
Tetracycline
OK-432
Ethanol

TetracyclineOne of the earliest sclerosant used
Mechanism is thought to be related to its low pH
Cyst resolution percentage up to 59% to 95%
Significantly higher success rate than simple aspiration

Tetracycline
S/ELocal pain
Haematoma
Fatigue
Febrile sensation
Vocal cord paralysis
Treece GL et al 1983Goldfarb WB et al 1987Lee JK et al 1989

Tetracycline
No significant difference in effect when compared to NS in RCTTetracycline (43%) vs NS (47%)
Not commonly used
Hegedus L et al 1988

OK-432
Lyophilized mixture of low-virulence group A streptococcus pyogenes and pen G potassium
Mechanism of actionInduce inflammatory reaction in cyst wallsFluid drainageShrinkageFibrotic adhesion

OK-432Cure rate ranges from 67-73% 25-89% showed reduction in cyst volumeNot readily a/v in HKChance of success
No. of previous aspirationsCyst volume
S/ELocal painTemporary feverHaematoma Roh JL et al 2008
Cho SH et al 2008Roh JL et al 2006Chang HS et al 1998

Ethanol
Induce functional ablation and shrinkage
Success rate up to 95%
RCT showed ethanol is superior to NS
FailureLarge cystMulti-cystic lesions Yasuda K et al 1992
Bennedbaek FN et al 2003
Campatelli A et al 1994

Ethanol
S/E:Local pain and burning sensationLocal haematomaDrunken feelingVocal cord paralysisRespiratory arrest (single case report)
Leakage of ethanol causing toxic necrosis of larynx and paraglandular fibrosis
Extensive scarring making subsequent operation difficult
Iacconi P et al 1996Mauz PS et al 2004

Summary
Sclerotherapy is effective
small cyst (<4cm)
solitary
simpleYasuda K et al 1992

Summary
surgery sclerotherapy
Success rate (%) 100 70-80
histology yes no
risk GA risk / surgical risk minimal
No. of procedure one May need multiple attempts
cost expensive cheap
recurrence no <10%

Thyroid cyst
simple
<4cm
aspiration sclerotherapy
surgery
complex
>4cm

Conclusion
Percutaneous sclerotherapy with ethanol or OK-432 is simple, safe and effective non-operative alternative for the treatment of benign cystic lesions of thyroid
SolitarySmall (<4cm)simple

Thank you
























![Nuevo Pcge 2012 - Uch 02.Pptx [Reparado]](https://img.pdfslide.us/doc/110x75/5572108a497959fc0b8d541b/nuevo-pcge-2012-uch-02pptx-reparado.jpg)

