Embed Size (px)
Citation preview
GIANT CEMENTIFYING F/BROMAISHWAR SINGH,ROHIT SHARMA
LATA GATHWALASANJAY SAXENA
SPS YADAV
Department of Otolaryngology, Pathology and Oral SurgeryMedical College and Hospital,
Rohtak-124001, (INDIA).
A 36 year old female with giant cementifying fibroma is presented. The tumour had replacedone half of the body of the mandible. The management policy and brief review of the diseaseis discussed.
C ementifying fibroma is also called cementoossifying fibr'ma, cementoblastoma,
periapical fibrous dysplasia, periapicalosteofibroma, osteofibrosis, cementoma andlocalised fibro-osteoma5. It constitutes about 2%of the odontogenic tumours3. Cementifyingfibroma is a separate entity which needs to bedifferentiated from fibrous dysplasia and othervarious osseous lesions5 According to Shaferand Waldron (1982) there is close histogeneticrelationship between central cementifyingfibroma and the central ossifying fibroma, basicneoplastic process being the same, the onlydifference is in the cell involved and its endproduct; cementum in one case, bone in theother. We present a case of giant sizecementifying fibroma seen by us.
CASE REPORTB.D., 36 years female reported to ENT services
for gradually increasing painless swelling overright side of face for last 2 years. There washistory of losening of teeth and change in voicefor last 3 months. The clinical examinationrevealed a smooth, lobulated swelling extendingfrom right lower 1st premolar to 3rd molar tooth.The bulge was both inside the oral cavity andpushing the tongue to opposite side as well asoutside. Patient had marked difficulty inmestication. The teeth were' loose and displacedoutward with, open bite. It was non tender,lobulated, smooth, mucosa over the swellingwas normal. X-ray of the mandible showed acircumscribed radiolucent area extending fromro, ii rc /Vnf A7 V;, I in AT UFAn rune
the 2nd incisor to 3rd molar. There was radioopaque shadow in between the lesion. Excisionof the tumor was done by external approach.Operative finding showed that both the inner andouter cortex of the mandible were eroded.
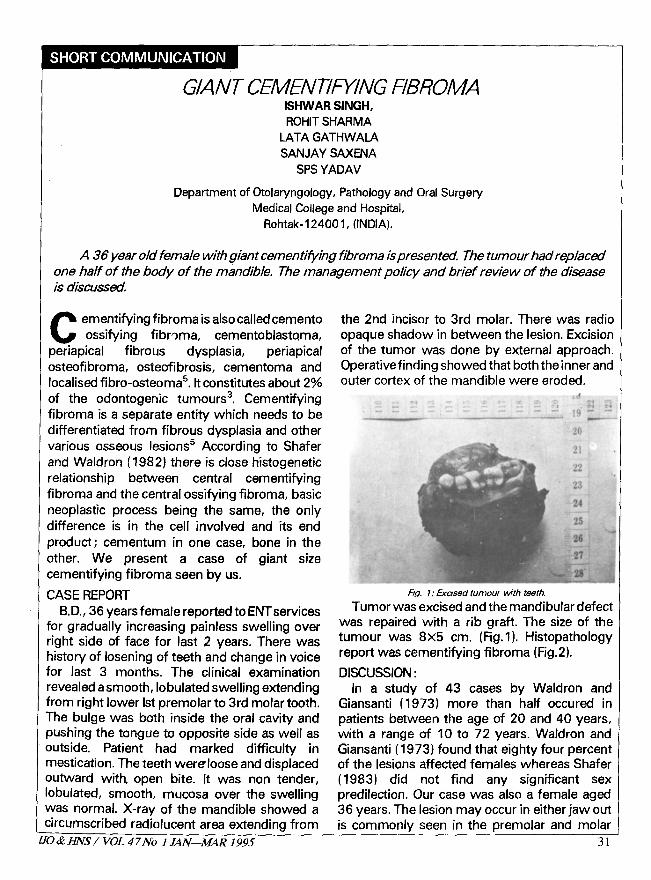
Fig. 1: Erased tumour with teeth.
Tumor was excised and the mandibular defectwas repaired with a rib graft. The size of thetumour was 8x5 cm. (Fig.1). Histopathologyreport was cementifying fibroma (Fig.2).
DISCUSSION:In a study of 43 cases by Waldron and
Giansanti (1973) more than half occured inpatients between the age of 20 and 40 years,with a range of 10 to 72 years. Waldron andGiansanti (1973) found that eighty four percentof the lesions affected females whereas Shafer(1983) did not find any significant sexpredilection. Our case was also a female aged36 years. The lesion may occur in either jaw outis commonly seen in the premolar and molar
Z1
Giant Cementifying Fibroma—L Singh, et al
region and majority of the cases have beenreported in the mandible (Shafer 1983).Hammer et al (1968) and others reported that80% of the cases occurred in the mandible. Thelesion is asymptomatic until a noticeableswelling and mild deformity is caused by the
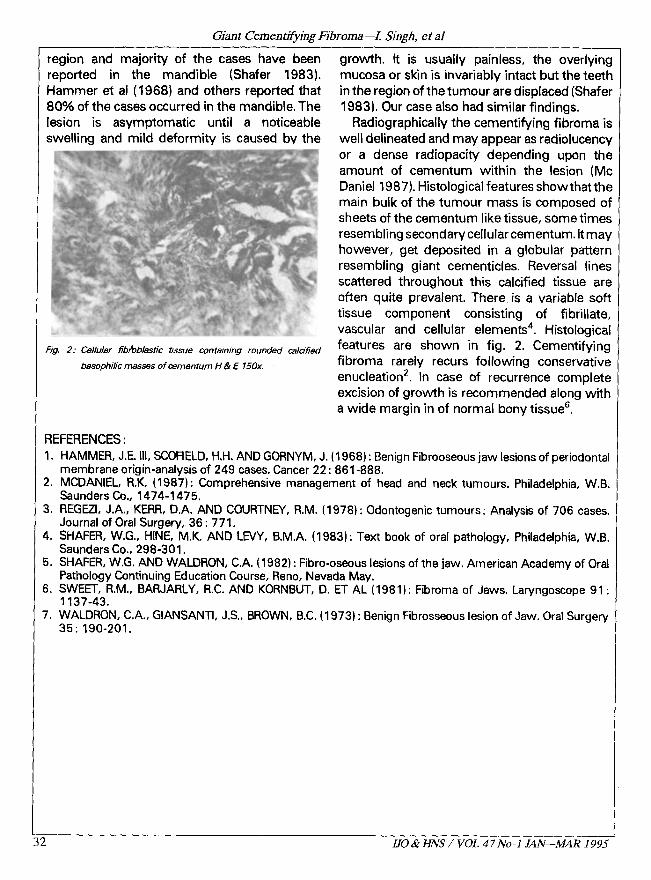
Fig. 2: Cellular fibroblastic tissue containing rounded calcified
basophilic masses of cementurn H & E 150x.
growth. It is usually painless, the overlyingmucosa or skin is invariably intact but the teethin the region of the tumour are displaced (Shafer1983). Our case also had similar findings.
Radiographically the cementifying fibroma iswell delineated and may appear as radiolucencyor a dense radiopacity depending upon theamount of cementum within the lesion (McDaniel 1987). Histological features showthat themain bulk of the tumour mass is composed ofsheets of the cementum like tissue, some timesresembling secondary cellular cementum. It mayhowever, get deposited in a globular patternresembling giant cementicles. Reversal linesscattered throughout this calcified tissue areoften quite prevalent. There is a variable softtissue component consisting of fibrillate,vascular and cellular elements'. Histologicalfeatures are shown in fig. 2. Cementifyingfibroma rarely recurs following conservativeenucleation 2 . In case of recurrence completeexcision of growth is recommended along witha wide margin in of normal bony tissue s.
REFERENCES:1. HAMMER, J.E. III, SCOFIELD, H.H. AND GORNYM, J. (1968) : Benign Fibrooseous jaw lesions of periodontal
membrane origin-analysis of 249 cases. Cancer 22: 861-888.2. MCDANIEL, R.K. (1987): Comprehensive management of head and neck tumours. Philadelphia, W.B.
Saunders Co., 1474-1475.3. REGEZI, J.A., KERR, D.A. AND COURTNEY, R.M. (1978): Odontogenic tumours: Analysis of 706 cases.
Journal of Oral Surgery,. 36; 771.4. SHAFER, W.G., HINE, M.K. AND LEVY, B.M.A. (1983): Text book of oral pathology, Philadelphia, W.B.
Saunders Co., 298-301.5. SHAFER, W.G. AND WALDRON, C.A. (1982) : Fibro-oseous lesions of the jaw. American Academy of Oral
Pathology Continuing Education Course, Reno, Nevada May.6. SWEET, R.M., BARJARLY, R.C. AND KORNBUT, D. ET AL (1981) : Fibroma of Jaws. Laryngoscope 91:
1137-43.7. WALDRON, C.A., GIANSANTI, J.S., BROWN, B.C. (1973) : Benign Fibrosseous lesion of Jaw. Oral Surgery
35: 190-201.
.S L IJO & ENS / VOL 47 No-I JAN—MAR 1995