Embed Size (px)
Citation preview

REVIEW
82 Ferner
10.1136/jnnp.2010.206532
Pract Neurol 2010; 10: 82–93
The neurofibromatosesRosalie E Ferner
• Axillary or groin freckling
• Two or more neurofbromas or one plexi-
form neurofi broma
• Lisch nodules in the Iris
• Optic pathway glioma
• Bony dysplasia of the sphenoid wing
• Pseudarthrosis of the long bones
In practice, the diagnosis is straightforward on
clinical inspection in most adults, but note:
• Although café au lait patches are present
in 99% of patients by the age of 5 years,
they fade in some older people or become
obscured in individuals with many cuta-
neous neurofi bromas.
• Café au lait patches may be the only
sign in young children, even without
a family history of NF1, because other
symptoms develop later in childhood or
adolescence.
• About 10% of the general population
have one to two café au lait patches.
• In mosaic NF1, the mutation occurs after
fertilisation in contrast with classical NF1
where the mutation is already present in
the sperm or egg before fertilisation. The
proportion of the body that is affected is
determined by the timing of the mutation.
Neurofi bromatosis 1 (NF1) and neurofi bromatosis 2 (NF2) are inherited autosomal
dominant disorders that have a signifi cant impact on the nervous system and
predispose to tumour formation. The current nomenclature makes NF1 and NF2
awkward bedfellows because they are clinically and genetically separate disorders.
Neurofi bromas are characteristic of NF1, a common condition with major skin
involvement and many clinical complications. By contrast, schwannomas are the
distinctive lesions in NF2, cutaneous signs are less prominent in this rarer disorder
and clinical manifestations are largely restricted to the nervous system and eye.
The current aim of neurofi bromatosis specialists is to provide cohesive standards
of care for everyone with neurofi bromatosis and to devise standardised protocols
for assessment and management within a multidisciplinary setting.
Correspondence to
Dr RE Ferner, Consultant
Neurologist and Lead Clinician for
Neurofi bromatosis Service, Guy’s
and St Thomas’ Hospitals NHS
Trust, and
Honorary Senior Lecturer in
Neurology King’s College London,
Department of Neurology, Guy’s
Hospital, Great Maze Pond, London
SE1 9RT, UK; rosalie.ferner@
kcl.ac.uk
INTRODUCTIONIncreasing cooperation between clinicians
and scientists in recent years has led to a bet-
ter understanding of the clinical and genetic
characteristics of neurofi bromatosis 1 (NF1)
and neurofi bromatosis 2 (NF2). The neurofi -
bromatoses fall fi rmly within the sphere of the
neurologist who is ideally placed to coordinate
the care of these complex disorders.
NEUROFIBROMATOSIS 1Diagnosis and differential diagnosesIn 1882 von Recklinghausen described benign
tumours arising from the peripheral nerve
sheath as ‘neurofi bromas’.1 The condition was
then named after him until the 1987 National
Institutes of Health Consensus Development
Conference formulated the current diagnostic
criteria and proposed that it should be called
NF1.2 The clinical diagnosis is based on the
presence of at least two major disease fea-
tures2 3 out of the following:
• A fi rst degree relative with NF1
• Six or more café au lait patches which
may be present at birth or, if not, they
appear in the fi rst few years of life
04_pn206532.indd 8204_pn206532.indd 82 3/6/2010 4:56:04 PM3/6/2010 4:56:04 PM

83Ferner
www.practical-neurology.com
Mutations occurring early in embryonic
development produce mild generalised
disease indistinguishable from classical
NF1. Later mutations result in disease
manifestations that are restricted to
one segment of the body. For instance,
an individual with segmental NF1 might
present with café au lait patches, neuro-
fi bromas or freckling but only in one body
segment.4 The importance of mosaicism is
that NF1 complications are infrequent in
individuals with mosaic disease and the
risk of passing on classical NF1 is low (see
section on genetic counselling below).
• Patients with the recently reported Legius
syndrome also present with café au lait
patches and axillary freckling in asso-
ciation with mild cognitive problems and
macrocephaly.5 Affected individuals have
no neurofi bromas or other NF1 compli-
cations (this syndrome is associated with
SPRED1 mutations on chromosome 15,5
a member of the SPROUTY/SPRED family
of tumour suppressor proteins). Although
there is clinical overlap between NF1 and
Legius syndrome, they are genetically
separate and Legius syndrome has a sig-
nifi cantly milder phenotype than NF1.
• Symmetrical multiple spinal nerve root
neurofi bromas and café au lait patches
characterise the rare hereditary spinal
neurofi bromatosis in which NF1 muta-
tions have been identifi ed but there are
no other NF1 disease features.
• NF1 can also be confused with syndromes
causing localised tissue overgrowth, and
with different forms of pigmentation.3 For
example, clinicians should be wary when
a patient is referred with ‘nerve sheath
tumours’ without any other neurocutane-
ous problems because multiple lipomas
can be inherited in an autosomal dominant
fashion. Firm, occasionally painful subcu-
taneous lumps develop in the late twen-
ties or early thirties on the distal arms,
trunk and proximal thighs; the diagnosis is
confi rmed by excision and histology.
Epidemiology and geneticsNF1 has a birth frequency of 1 in 2500–3000,
a minimum prevalence of 1 in 4–5000 and
about 50% of affected individuals have new
mutations.6 The gene was cloned on chro-
mosome 17q11.2 in 1990. Neurofi bromin, the
protein product, is widely expressed with high
levels in the nervous system.7–9 It acts as a
tumour suppressor which explains why NF1
Figure 1Cutaneous neurofi bromas in an adult male with neurofi bromatosis 1.
Figure 2Subcutaneous neurofi bromas in an adult male with neurofi bromatosis 1.
04_pn206532.indd 8304_pn206532.indd 83 3/6/2010 4:56:04 PM3/6/2010 4:56:04 PM

84 Practical Neurology
10.1136/jnnp.2010.206532
patients are prone to developing benign and
malignant tumours. It also reduces cell growth
and proliferation by negative regulation of
the cellular proto-oncogene p21RAS and by
control of the serine threonine kinase MTOR
(mammalian target of rapamycin).10 11
Table 1 Clinical manifestations of neurofi bromatosis 1
Skin Café au lait patchesAxillary and groin frecklingFreckling under breasts and around neck
Hypopigmented macules
Cutaneous angiomas
Xanthogranulomas—orange papules (occur
transiently in childhood)
Cutaneous neurofi bromasSubcutaneous neurofi bromas
Glomus tumour
Nervous system Plexiform neurofi bromasMalignant peripheral nerve sheath tumour
Neurofi bromatous neuropathy
Aqueduct stenosis
Chiari 1 malformation
Sphenoid wing dysplasia
Macrocephaly
EpilepsyCognitive impairmentMultiple sclerosis
Cerebrovascular disease
Brain tumours (astrocytomas)
Optic pathway gliomaThe eye Lisch nodules
Bilateral congenital ptosis
Glaucoma
Choroidal abnormalitiesBone Scoliosis—idiopathic and dystrophic
Pseudarthrosis of a long bone
Osteoporosis
Short stature
Cardiovascular disease Congenital heart disease—pulmonary
stenosis
HypertensionRenal artery stenosis
Respiratory disease Compression from neurofi broma causing
restrictive lung defect
Pulmonary metastases from malignant
peripheral nerve sheath tumour
Gastrointestinal disease Gastrointestinal stromal tumour
Dysplasia
Duodenal carcinoid tumour
Other tumours Breast carcinoma
Phaeochromocytoma
Common clinical features are in bold typeface.
Clinical featuresThe complications of NF1 vary between individ-
uals, involve many of the body systems and are
unpredictable within families.3 Many of the seri-
ous complications occur in childhood, including
orthopaedic problems, disfi guring plexiform
neurofi bromas, optic pathway gliomas, renal
artery stenosis and cognitive impairment.
The skinSkin manifestations are listed in table 1.
Recently, glomus tumours have been described
in association with NF1 but their frequency is
unknown. Glomus bodies are the normal small
dermal arteriovenous anastomoses that control
body temperature, found mostly in the skin of
the fi ngers and toes. The tumours can be sin-
gle or multiple and are located under the nail
bed. They cause pain, sensitivity to cold and
exquisite localised tenderness.12 Sometimes a
bluish discolouration is noticeable under the
nail bed. MRI can be helpful in showing the
lesions. If there is a high index of suspicion,
surgical exploration should be considered
because removal alleviates the symptoms
Neurological complicationsNeurological complications affect both the
peripheral and central nervous systems, account-
ing for signifi cant morbidity and mortality in NF1.
Neurofi bromas
Neurofi bromas are the cardinal manifestation
of NF1. These benign peripheral nerve sheath
tumours contain a mixture of Schwann cells,
fi broblasts, perineurial cells, mast cells and
axons embedded in an extracellular matrix.13
The distinction between the different types of
neurofi bromas produces heated debate among
‘neurofi bromatologists’; this stems from the
importance of identifying the neurofi bromas
that cause signifi cant neurological defi cit or have
malignant potential. Neurofi bromas can form as
localised cutaneous (fi gure 1) or subcutaneous
(fi gure 2) growths, spinal nerve root tumours, or
plexiform lesions (fi gure 3) that involve multi-
ple fascicles or large nerves, frequently infi ltrat-
ing surrounding tissue and blood vessels.3 They
should be distinguished from schwannomas.
Cutaneous neurofi bromas develop in 99% of
patients, usually in early adulthood, but they
can appear in childhood. They increase in size
and number during pregnancy but are unaf-
fected by hormonal contraceptives. Emerging
lesions have a purplish colour, and itching and
04_pn206532.indd 8404_pn206532.indd 84 3/6/2010 4:56:51 PM3/6/2010 4:56:51 PM

85Ferner
www.practical-neurology.com
MRI can show the site and extent of the
tumour but 18[F] 2-fl uoro-2-deoxy-D-glucose
positron emission computerised tomography
with delayed imaging and targeted biopsy
is the most sensitive and specifi c diagnostic
strategy.20 The goal of treatment is complete
removal of the tumour with clear margins.
Radiotherapy is administered for high grade or
incompletely excised lesions, and chemother-
apy with ifosfamide and doxorubicin provides
palliation for patients with extensive disease.15
Spinal nerve root neurofi bromas
These can be asymptomatic or cause pressure
on the adjacent spinal nerve root or spinal
cord.3 High cervical nerve root neurofi bromas
are prone to compress the cord but the neuro-
logical defi cit is frequently mild in comparison
with the neuroimaging appearances. Patients
require careful evaluation by a multidisciplin-
ary team conversant with the variable natural
history of these neurofi bromas and the risks of
NF1 related surgery.
Axonal symmetrical neurofi bromatous
neuropathy
This affects as least 1% of NF1 adults. They
present with mild distal sensory and motor
symptoms. Thickened peripheral nerves are
infi ltrated with neurofi bromatous tissue.18
Although NF1 neurofi bromatous neuropathy
is not progressive, affected individuals require
assiduous monitoring because they are at
risk of developing malignant peripheral nerve
sheath tumours.18
Cerebral malformations
Chiari 1 malformation and aqueduct stenosis
due to subependymal glial cell proliferation are
encountered in 1.5% of NF1 patients. Sphenoid
wing dysplasia is noticeable as pulsating
exophthalmos without visual compromise; the
absent sphenoid wing allows the temporal lobe
to prolapse forwards into the orbit but surgical
correction is not usually undertaken.3
Epilepsy
Epilepsy is diagnosed in about 6% of NF1
patients, it is frequently mild and it tends to
start between childhood and middle age.3 There
are several underlying causes, including brain
trauma and infection unrelated to NF1 as well
as mesial temporal sclerosis, NF1 related glio-
mas and anecdotal reports of dysembryoblas-
tic neuroepithelial tumours. All seizure types
stinging unresponsive to antihistamines are
common symptoms. Excision, albeit with a risk
of thickened scarring, is the usual treatment
but laser treatment is helpful for small lesions.
Cutaneous neurofi bromas are a major source
of psychological distress but unlike subcutane-
ous and plexiform neurofi bromas, they do not
undergo malignant change.
Subcutaneous neurofi bromas are fi rm periph-
eral nerve tumours that frequently cause pain,
neurological symptoms and defi cit. They can
be mistaken for glomus tumours because the
symptoms are misinterpreted as arising from
a neurofi broma. Women with subcutaneous
breast lumps should be referred to a specialist
breast unit because carcinoma cannot be dis-
tinguished clinically from a neurofi broma. NF1
females have an 8% cumulative risk of devel-
oping breast cancer before the age of 50 years
compared with 2% in the general population.14
About 60% of NF1 individuals have plexiform
neurofi bromas. The period of maximum growth
is in childhood and adolescence. Extensive
plexiform neurofi bromas can cause neurologi-
cal defi cit and disfi gurement. They are diffi cult
to remove, and indeed surgery can cause disas-
trous bleeding and delayed wound healing.3
Malignant peripheral nerve sheath
tumours
These usually arise from pre-existing focal
subcutaneous neurofi bromas or plexiform
neurofi bromas but they can develop de novo.15
People with NF1 have about a 10% lifetime
risk of developing one and most present in
the second and third decades.16 Risk factors
include a personal history or a family history
of cancer, prior treatment with radiotherapy,
deep seated plexiform neurofi bromas, neuro-
fi bromas involving the brachial and lumbosa-
cral plexuses, neurofi bromatous neuropathy
and microdeletion of the NF1 gene.15 17–19
Malignant peripheral nerve sheath tumours
are diffi cult to diagnose because they arise
in individuals who are accustomed to devel-
oping lumps, and the symptoms can overlap
with benign tumours. Urgent referral to a spe-
cialist neurofi bromatosis unit is imperative
when patients complain of one or more of the
following:
• Persistent or nocturnal pain associated with
a plexiform/subcutaneous neurofi broma
• Rapid increase in size of a neurofi broma
• New or unexplained neurological defi cit
• Neurofi broma changes to hard texture15
04_pn206532.indd 8504_pn206532.indd 85 3/6/2010 4:56:51 PM3/6/2010 4:56:51 PM

86 Practical Neurology
10.1136/jnnp.2010.206532
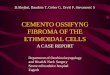
Figure 3Plexiform neurofi broma of the abdominal wall in an adult male with neurofi bromatosis 1.
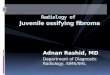
Figure 4MR T2 hyperintensities in the globus pallidi in a young child with neurofi bromatosis 1.
occur but complex partial seizures predomi-
nate and usually respond to carbamazepine or
lamotrigine. When considering whether to use,
and which antiepileptic drugs to use, neurolo-
gists should remember that NF1 patients have
an increased risk of developing osteoporosis
and cognitive impairment (see sections on
cognitive problems and bone below).
Cognitive problems
Cognitive impairment is the commonest neu-
rological manifestation and is characterised by
an IQ in the low average range, specifi c learn-
ing diffi culties and behavioural problems.3 21
About 5% of patients have an IQ less than 70,
and learning problems occur in at least 60%
of children. Visual spatial diffi culties, impaired
attention, inability to interpret non-verbal
cues, reduced working memory, speech and
language defi cits and disordered executive
function are all documented. These cognitive
problems do not appear to worsen with age and
severe intellectual disability is unusual, occur-
ring in about 5% of patients.21 Asymptomatic
hyperintense lesions on T2 weighted brain MRI
are evident in most children with NF1, pre-
dominantly in the basal ganglia, brainstem and
cerebellum, they usually resolve in early adult-
hood and probably refl ect delayed myelination
(fi gure 4).21 They are not thought to play a key
role in the pathogenesis of NF1 related learn-
ing problems which remain unexplained
Learning problems improve with learning
support, and attention defi cit hyperactivity
disorder responds to judicious use of methyl-
phenidate.21 Statins reverse p21RAS activity and
hippocampal learning defi cits in an NF1 mouse
model. Short term trials of these drugs have
shown a good safety profi le in NF1 children, and
their effect on attention, working memory and
visual spatial problems is being evaluated.22
Multiple sclerosis
Primary progressive multiple sclerosis occurs
with increased frequency in NF1 and relaps-
ing remitting disease has also been reported.23
Although NF1 is a tumour suppressor condi-
tion, immunosuppressant therapy is not con-
traindicated and so far there is no evidence of
an increase in malignancy in NF1 patients with
multiple sclerosis.
Cerebrovascular disease
Cerebrovascular disease is part of the spectrum
of the NF1 vasculopathy. Moya moya syndrome,
04_pn206532.indd 8604_pn206532.indd 86 3/6/2010 4:56:51 PM3/6/2010 4:56:51 PM

87Ferner
www.practical-neurology.com
The eyeAsymptomatic iris Lisch nodules can be seen
reliably on slit lamp examination and are
found in most NF1 individuals.2 3 We have also
encountered families with bilateral congenital
ptosis of uncertain aetiology, congenital and
acquired glaucoma, and choroidal abnormal-
ities. Neurofi bromas of the eyelid and orbit
have been reported.3
BoneBone abnormalities are a prominent prob-
lem in NF1 due to defects in the mainte-
nance of bone structure, bony overgrowth,
and erosion by plexiform neurofi bromas.3 26
Approximately 30% of NF1 patients have
short stature between the 10th and 25th cen-
tiles that affects the limbs and axial skeleton
in proportion.3 About half of NF1 individuals
have reduced bone mineral density but it is
uncertain whether there is an increased risk of
fracture and indeed whether specifi c preven-
tative treatment is warranted in every patient.
Pseudarthrosis of the long bones presents
in infancy as bowing of the affected limb
or spontaneous fracture with delayed heal-
ing, and formation of a false joint (fi gure 6).3
Meticulous assessment is required to avoid an
erroneous diagnosis of non-accidental injury.
About 10% of children with NF1 develop
idiopathic or dystrophic scoliosis that pre-
dominantly involves the lower cervical and
upper thoracic spine. Idiopathic scoliosis has
the same natural history in NF1 as in the gen-
eral population. Dystrophic scoliosis manifests
at a younger age than the idiopathic type,
characteristically involves only a few verte-
brae, producing a short, sharply angulated
curve with distortion of the vertebral bodies
Figure 5Optic pathway gliomas in a child with
neurofi bromatosis 1 involving both
optic nerves which are grossly enlarged
(arrowed)—axial MR scan.
cerebral aneurysm, internal carotid and cerebral
artery stenosis/occlusion have all been reported
and can be exacerbated by radiotherapy.3 13
Brain and optic pathway tumours
Gliomas can develop in any part of the cen-
tral nervous system, generally in the optic
pathways, cerebellum and brainstem.3 24 Most
slow growing gliomas are pilocytic astrocyto-
mas but gliomas outside the optic pathways,
tumours diagnosed in adulthood and symp-
tomatic lesions are higher grade astrocytomas
and have a more aggressive course.
About 15% of NF1 children have optic path-
way gliomas but only 5% develop symptoms
or signs (fi gure 5). They usually present before
the age of 6 years and can cause impaired
visual acuity and colour vision, squint, prop-
tosis, afferent pupillary defect, optic atrophy,
visual fi eld defects and precocious puberty.24
Adult onset or tumour progression are unusual
and visual screening is not required in adult-
hood.24 Young children rarely complain of visual
loss and the best method of diagnosis is regu-
lar visual screening, at least until the age of 7
years. Ideally visual acuity, colour vision, visual
fi elds and fundoscopy should be performed at
6 monthly intervals but many children are not
able to cooperate with such full visual testing.3 24
MR screening is unhelpful because young chil-
dren need to be anaesthetised and neuroimag-
ing does not identify optic pathway gliomas that
will necessarily progress and require treatment.
Children with diagnosed optic pathway glio-
mas should have regular MRI and visual assess-
ment by ophthalmologists conversant with NF1.
There is still debate about when to treat but
decline in visual acuity (greater than two lines) is
usually the main deciding factor in combination
with tumour progression on MRI.25 Radiotherapy
is contraindicated in NF1 children because of the
risk of a second malignancy, neuroendocrine and
neuropsychological sequelae and moya moya.24
Current fi rstline therapy is with vincristine and
carboplatin but the long term visual outcome is
uncertain and a retrospective multicentre study
is investigating this issue.24
Drugs that block RAS (farnesyl transferase
inhibitors) and MTOR pathways are of poten-
tial benefi t for NF1 plexiform neurofi bromas,
malignant peripheral nerve sheath tumours as
well as for optic pathway gliomas. Clinical tri-
als are underway but it is premature to predict
the outcome.3
04_pn206532.indd 8704_pn206532.indd 87 3/6/2010 4:56:57 PM3/6/2010 4:56:57 PM

88 Practical Neurology
10.1136/jnnp.2010.206532
Respiratory complicationsRespiratory compromise can arise as a conse-
quence of severe scoliosis and from restrictive
defect caused by compression by plexiform
neurofi bromas. The lung is the principal site of
metastatic spread from malignant peripheral
nerve sheath tumours.15
Gastrointestinal problemsMesenchymal gastrointestinal stromal tumours
occur mainly in the small bowel and are more
indolent than their sporadic counterparts.25
They can be confused with malignant periph-
eral nerve sheath tumours as both are positive
on 18[F] 2-fl uoro-2-deoxy-D-glucose positron
emission computerised tomography. They
cause gastrointestinal bleeding and anaemia,
some require excision and imatinib therapy is
being evaluated.
Dysplasia of the colon can cause consti-
pation, and duodenal carcinoid tumours have
been encountered in NF1 patients, occasion-
ally coexisting with phaeochromocytomas.3
PhaeochromocytomaPhaeochromocytoma is detected in 0.7%
of NF1 individuals but routine screening is
unrewarding; NF1 patients should be advised
to start a 24 h urinary catecholamine col-
lection only when they are symptomatic.
Clinicians should evaluate NF1 individuals
with unexplained paroxysmal palpitations
associated with headache, dizziness and
sweating.3
Genetic counsellingGenetic counselling is advised for everyone
with NF1 before they attempt to have chil-
dren; both prenatal mutation testing and pre-
implantation genetic diagnosis are available.
There is a one in two chance of transmitting
NF1 to an offspring and the risk of having a
severely affected child is 1 in 12.3 People with
mosaic NF1 have a small but unquantifi able
risk of passing on generalised NF1 to an infant
(we have encountered a patient with unilateral
groin freckling who produced a child with gen-
eralised NF1).
Current laboratory techniques can detect
the causative NF1 mutation in 95% of cases
but usually the phenotype cannot be predicted
from the type of mutation. However, families
with café au lait patches and freckling with-
out neurofi bromas have a mild phenotype due
and ribs. Dystrophic scoliosis can be associ-
ated with respiratory impairment, and surgery
is required to fuse the spine in severe rapidly
progressive cases.3
Cardiovascular diseaseNeurofi bromin is expressed in vascular endo-
thelium and smooth muscle. Loss of neurofi -
bromin through gene mutation is thought to
be the basis for an NF1 vasculopathy.27 High
blood pressure and congenital heart disease,
particularly pulmonary stenosis, occur in asso-
ciation with NF1.3 Renal artery stenosis may be
bilateral and is diagnosed in about 1% of NF1
individuals. Cerebrovascular disease is cited
as a cause of early death in NF1 but this has
not been the experience in the large UK neu-
rofi bromatosis services and requires further
verifi cation.
Figure 6Pseudarthrosis of the tibia in a young
child with neurofi bromatosis 1.
04_pn206532.indd 8804_pn206532.indd 88 3/6/2010 4:56:59 PM3/6/2010 4:56:59 PM

89Ferner
www.practical-neurology.com
can have an earlier age of onset. In children,
the fi rst manifestation is likely to be cranial
or orbital meningioma, spinal schwannoma or
meningioma, cutaneous schwannoma, focal
amyotrophy or cataracts.29
The diagnosis can be made if two of the
following features are present: meningioma,
schwannoma, glioma, neurofi broma, posterior
subcapsular lens opacity plus a unilateral ves-
tibular schwannoma or a fi rst degree relative
with NF2. Alternatively, a unilateral vestibular
schwannoma plus multiple meningiomas or a
fi rst degree relative with NF2 is suffi cient for
diagnosis30
Recent evidence suggests that 20–30% of
NF2 patients without a family history of the
disease are mosaic. Mosaicism can present with
mild generalised NF2 or with any type of NF2
related tumour occurring just on one side of the
body; the NF2 mutation is detected in tumours
but not in the blood of these patients4 29
NF2 should be distinguished from NF1 (see
above) and from schwannomatosis. In this
latter condition, patients develop multiple
schwannomas affecting the peripheral nerves
and spinal nerve roots without vestibular
schwannomas or other NF2 related tumours.31
Schwannomatosis can occur in families and
the predominant symptom is pain. In seg-
mental schwannomatosis the schwannomas
are restricted to one segment of the body. The
gene for schwannomatosis has been identifi ed
either to a specifi c mutation in exon 17 of the
NF1 gene, or to Legius syndrome, and muta-
tion testing will confi rm a good prognosis in
these patients.3 5 It is important to diagnose
patients with Legius syndrome and mosaic
NF1 because they have a milder phenotype
and will not require monitoring for widespread
disease complications.
Genetic testing should be considered in
children with three to fi ve café au lait patches,
no other disease features and no family his-
tory, and in individuals with an unusual phe-
notype. This will ensure that other conditions
with abnormal pigment are not confused with
NF1 (see above).
SurveillanceFor children, the annual visit should include
a developmental assessment, enquiry about
schooling, examination of the skin, long bones
and spine, monitoring of blood pressure and
the heart for congenital heart disease, visual
assessment and measurement of height,
weight, head circumference, and checks for
delayed or precocious puberty.3
In our NF unit we hold transitional clinics
for teenagers with NF1 to provide education,
support and encourage independence, advis-
ing them to know when and where to seek
help in adulthood. Individuals over 25 years
with mild NF1 need to have yearly blood
pressure checks and to be aware of symp-
toms indicating possible malignant change
in a neurofi broma. They require prompt
access to specialist advice if they develop
symptoms suggesting an NF1 complication.
Ideally, NF clinical nurse specialists and the
UK Neurofi bromatosis Association advisors
should facilitate access to the appropriate
clinician. Doctors in the UK caring for adults
with NF1 should discuss complex problems
with the nationally commissioned NF1 units
in London and Manchester (box).
NEUROFIBROMATOSIS 2Diagnosis and differential diagnosisNF2 was fi rst described by Wishart in 1822
and was formerly known as bilateral acoustic
or central neurofi bromatosis.28 The charac-
teristic defi ning feature is bilateral vestibular
schwannomas.29 30 Because these tumours do
not usually develop before adolescence, the
NF2 diagnostic criteria include features that
Box The nationally commissioned complex NF1 Service. Guy’s and St Thomas’ NHS Foundation Trust and St Mary’s Hospital, Manchester
NF1 patients with ‘complex NF1’ have rare complications that cause signifi cant
morbidity and mortality
NF1 complications requiring direct referral to complex NF1 service• Plexiform or subcutaneous neurofi bromas associated with one or more of
the following requires urgent referral: persistent pain, new/unexplained
neurological defi cit, rapid growth, hard texture
• high cervical neurofi bromas causing cord compression
• unusual NF1 phenotypes
NF1 complications requiring liaison with complex NF1 service via a clinical nurse specialist
This ensures a cohesive pattern of care, adherence to national protocols (eg,
for visual screening) and awareness of special needs of NF1 patients
• Optic pathway glioma, brain and spinal cord glioma
• Pseudarthrosis of long bones
• Neurofi bromatous neuropathy
• Multiple sclerosis
Cutaneous
signs are not
conspicuous in NF2
04_pn206532.indd 8904_pn206532.indd 89 3/6/2010 4:57:13 PM3/6/2010 4:57:13 PM

90 Practical Neurology
10.1136/jnnp.2010.206532
proximal to the NF2 gene on chromosome 22,
and mutations have been detected in the INI/
SMARB1 tumour suppressor gene in some
families.32
Epidemiology and geneticsThe birth frequency of NF2 is 1 in 25 000 and
recent data show a disease prevalence of 1 in
60 000.6 This high prevalence is due to ear-
lier diagnosis and longer survival because of
improved treatment. The NF2 gene was cloned
on chromosome 22q11.2 and the gene protein
merlin acts as a tumour suppressor, controlling
proliferation of schwann and leptomeningeal
cells by interaction with multiple intercellular
signalling pathways.33 34
Table 2 Clinical manifestations of neurofi bromatosis 2
Skin Café au lait patches mostly just 1–3Cutaneous schwannomas plaque lesionsSubcutaneous schwannomasCutaneous neurofi broma (uncommon)
Nervous system Vestibular schwannomasCranial nerve schwannomas (not 1 and 2)
Spinal schwannomasPeripheral nerve schwannomasCranial meningiomasSpinal meningiomasSpinal/brainstem ependymomas
Spinal/cranial astrocytoma
Focal amyotrophy
Facial mononeuropathy
Neurofi bromatosis 2 neuropathy
Epilepsy
The eye Cataracts subcapsular/wedge
Epiretinal membrane
Retinal hamartoma
Optic nerve meningioma
Common clinical features are in bold typeface.
Figure 7Plaque schwannoma in an adult male
with neurofi bromatosis 2.
Clinical featuresThe skinCutaneous signs are not conspicuous in NF2
(table 2).29 Although 70% of patients have
skin tumours, the majority have fewer than
10 lesions (fi gure 7). Café au lait patches
are reported in 40% of patients but are less
numerous than in NF1.
Neurological complicationsSchwannomas, meningiomas and
ependymomas
Schwannomas are benign tumours arising
from the peripheral nerve sheath and are com-
posed entirely of schwann cells.29 Unlike neu-
rofi bromas, malignant change is rare and 18[F]
2-fl uoro-2-deoxy-D-glucose positron emis-
sion computerised tomography is not helpful
because it is so frequently positive, even wth
benign lesions.
Vestibular schwannomas occur in 95%
of NF2 patients (fi gure 8). They present with
progressive unilateral or bilateral sensorineu-
ral deafness.29 Patients may also complain of
tinnitus and impaired balance, and have signs
of raised intracranial pressure and encroach-
ment on the brainstem. The growth rate varies,
independently of the type of NF2 mutation,
and tends to be maximal in patients less than
30 years of age.29 They are managed differently
from sporadic tumours because NF2 tumours
are often multilobular and occur in the con-
text of multiple nervous system tumours; it is
crucial that management decisions are taken
by a specialist team. The goal of treatment
is preservation of hearing and neurologi-
cal function. Tumours showing progressive
growth, brainstem compression and hearing
loss require removal and there is an option to
insert an auditory brainstem implant at the
time of surgery.35 This electronic device pro-
vides a sense of sound to a person with pro-
found sensorineural hearing loss but patients
do require intensive specialist rehabilitation
to achieve improved lip reading and environ-
mental sound. Some specialist centres are
attempting hearing preservation surgery or
insertion of cochlear implants if there is integ-
rity of the cochlear nerve (these provide supe-
rior hearing to auditory brainstem implants).36
Stereotactic radiosurgery can be considered
for tumours smaller than 3 cm or for patients
who decline surgery or are too frail; the tumour
control rate is about 50%, with 40% retaining
04_pn206532.indd 9004_pn206532.indd 90 3/6/2010 4:57:13 PM3/6/2010 4:57:13 PM

91Ferner
www.practical-neurology.com
removal and as cortical wedge opacities
(peripheral cortical cataracts). Orbital menin-
giomas and retinal hamartomas can impair
vision, and epiretinal membrane affecting
the macula and of varying severity has been
described.29
Genetic counselling• There is a 50% chance of transmitting
NF2 to an offspring but NF2 mosaics have
a less than one in two chance of passing
on generalised NF2 to a child.4 29
• About 6% of people younger than 30 years
old with unilateral vestibular schwan-
noma will go on to develop other features
of NF2 compared with only 1% who are
over 30 years of age.
• 10% of individuals with multiple meningi-
omas have NF2.29
Prenatal testing and preimplantation genetic
diagnosis are available. NF2 gene mutation
testing is useful in every patient as there is
a phenotype–genotype correlation.29 Severe
disease is associated with frameshift or non-
sense mutations and a milder phenotype is
linked with large deletions, missense muta-
tions or inframe deletions. Early detection
of tumours aids management of NF2, and
presymptomatic testing is an integral part of
NF2 care in families where the genetic muta-
tion is known. If the NF2 mutation is identifi ed
in two separate tumour specimens, the diag-
nosis can be verifi ed in mosaic patients.
Screening and surveillanceVision assessment, and examination of the
skin and nervous system should be undertaken
Figure 8Bilateral vestibular schwannomas
distorting the brainstem in a
young man with neurofi bromatosis
2—enhanced axial MR scan.
pretreatment hearing for 3 years.29 37 However,
there is a small risk of radiation induced malig-
nancy and surgical removal of a tumour after
radiotherapy is diffi cult with poor facial nerve
preservation. A recent study noted improved
hearing in some patients and reduction in
tumour size with bevacizumab (vascular endo-
thelial growth factor inhibitor).38
Schwannomas on other cranial nerves are
slower growing and do not usually require sur-
gical intervention.
90% of NF2 patients have extramedullary
spinal schwannomas or meningiomas but only
a third cause symptoms (fi gure 9).29
Cranial meningiomas develop in 45% of
patients, are frequently multiple and cause sig-
nifi cant neurological problems and mortality.29
Ependymomas and pilocytic astrocyto-
mas occur predominantly in the upper cervi-
cal cord and brainstem and can be associated
with a syrinx.29 They can remain stable for
many years although some cause progressive
neurological defi cit.
Epilepsy
There has been no systematic study of sei-
zures in NF2 but 10% of our NF2 patients have
epilepsy that is not exclusively related to any
tumours. Cortical dysplasia has been reported
in NF2. Further studies are needed to address
the cause of seizures in this group of patients.
Neuropathy and amyotrophy
NF2 neuropathy is an axonal peripheral neu-
ropathy which can be severe and progres-
sive.39 It has been suggested that it is caused
by compression from multiple schwannn cell
tumourlets arising along the length of periph-
eral nerves on adjacent nerve fi bres. Care
should be taken to ensure that the neurolog-
ical defi cit is not arising from cauda equina
schwannomas, particularly if surgical inter-
vention is contemplated.
Isolated facial mononeuropathy that predates
and is distinct from vestibular schwannoma
onset is due to schwann cell proliferation.
Focal amyotrophy appears as focal wasting
and weakness in the affected limb. The cause
is uncertain but localised schwann cell infi ltra-
tion has been proposed.29 40
EyesCataracts present as posterior subcapsu-
lar lens opacities that do not usually require
04_pn206532.indd 9104_pn206532.indd 91 3/6/2010 4:57:20 PM3/6/2010 4:57:20 PM

92 Practical Neurology
10.1136/jnnp.2010.206532
annually from birth in at risk individuals. Brain
MRI should be performed every 2 years from
age 12 until 20 years and every 3–5 years until
age 40 years. Spinal MRI is undertaken every
3 years.29 Patients with symptomatic NF2 are
best managed by specialist multidisciplin-
ary teams. Once vestibular schwannomas are
detected, brain MRI is required at least annu-
ally with concomitant speech and pure tone
audiometry.29 Ongoing psychological support
and access to hearing therapy services are
also crucial for patient welfare.
CONCLUSIONSOptimal care of the neurofi bromatoses
requires a multidisciplinary team of clini-
cians, nurses and therapists in partnership
with the patient and family. The UK National
Commissioning Group has funded specialist
services in London and Manchester for ‘com-
plex NF1’, and from April 2010 there will be
specialist NF2 centres in Manchester, London,
Oxford, Cambridge and Sheffi eld (radiosur-
gery). These exciting developments will facili-
tate a high standard of multidisciplinary care
for patients with neurofi bromatosis through-
out the country. The challenge is to match the
advances in molecular biology with meticu-
lous recording of phenotype, and monitoring
of clinical response to emerging therapies.
ACKNOWLEDGEMENTSThis article was reviewed by Wayne Lam,
Edinburgh.
Provenance and peer review Commissioned and
externally peer reviewed.
Competing interests None.
REFERENCES 1. Von Recklinghausen FD. Uber die multiplen fi brome
der haut und ihre Beziehung zu den multiplen
neuromen. Berlin: A Hirschwald, 1882.
2. Neurofi bromatosis. Conference statement. National
Institutes of Health Consensus Development
Conference. Arch Neurol 1988;45:575–78.
3. Ferner RE, Huson SM, Thomas N, et al. Guidelines
for the diagnosis and management of individuals
with neurofi bromatosis 1. J Med Genet
2007;44:81–8.
4. Ruggieri M, Huson SM. The clinical and diagnostic
implications of mosaicism in the neurofi bromatoses.
Neurology 2001;56:1433–43.
5. Brems H, Chmara M, Sahbatou M, et al. Germline
loss-of-function mutations in SPRED1 cause a
neurofi bromatosis 1-like phenotype. Nat Genet
2007;39:1120–6.
Practice points
• Histological distinction between neurofi broma and schwannoma is crucial
as there are diagnostic and management implications; neurofi bromas are
indicative of NF1 and schwannomas of NF2 or schwannomatosis.
• Schwannomas only rarely undergo malignant change.
• There is a 10% lifetime risk that plexiform/subcutaneous neurofi bromas will
become malignant peripheral nerve sheath tumours.
• Individuals with subcutaneous lumps on the arms, proximal thighs and trunk
without other fi ndings are likely to have lipomas, not neurofi bromatosis,
and should have biopsy confi rmation.
• NF1 optic pathway gliomas rarely progress in adulthood and visual screening
is unnecessary after age 18 years.
• Vestibular schwannomas and meningiomas are features of NF2 and do not
occur in NF1; screening for these tumours in NF1 is inappropriate.
• Cutaneous or spinal schwannomas, cranial or spinal meningiomas, focal
amyotrophy or cataracts may be the fi rst signs of NF2 in young people.
Figure 9Spinal schwannomas arrowed in an
adult male with neurofi bromatosis
2—saggital enhanced MR scan.
04_pn206532.indd 9204_pn206532.indd 92 3/6/2010 4:57:21 PM3/6/2010 4:57:21 PM

93Ferner
www.practical-neurology.com
6. Evans, DG, Howard E, Giblin C et al. Birth incidence
and prevalence of tumour prone syndromes:
estimates from a UK genetic family register service.
Am J Med Genet A 2010;152A:327–32
7. Viskochil D, Buchberg AM, Xu G, et al. Deletions
and a translocation interrupt a cloned gene
at the neurofi bromatosis type 1 locus. Cell
1990;62:187–92.
8. Wallace MR, Marchuk DA, Andersen LB, et al. Type
1 neurofi bromatosis gene: identifi cation of a large
transcript disrupted in three NF1 patients. Science
1990;249:181–6.
9. Daston MM, Scrable H, Nordlund M, et al. The
protein product of the neurofi bromatosis type 1
gene is expressed at highest abundance in neurons,
Schwann cells, and oligodendrocytes. Neuron
1992;8:415–28.
10. Xu GF, O’Connell P, Viskochil D, et al. The
neurofi bromatosis type 1 gene encodes a protein
related to GAP. Cell 1990;62:599–608.
11. Johannessen CM, Reczek EE, James MF et al.
The NF1 tumour suppressor critically regulates
TSC2 and mTOR. Proc Natl Acad Sci USA
2005;102:8573–78.
12. De Smet L, Sciot R, Legius E. Multifocal
glomus tumours of the fi ngers in two patients
with neurofi bromatosis type 1. J Med Genet
2002;39:e45.
13. Kimura M, Kamata Y, Matsumoto K, et al.
Electron microscopical study on the tumor of von
Recklinghausen’s neurofi bromatosis. Acta Pathol
Jpn 1974;24:79–91.
14. Sharif S, Moran A, Huson SM, et al. Women with
neurofi bromatosis 1 are at a moderately increased
risk of developing breast cancer and should
be considered for early screening. J Med Genet
2007;44:481–4.
15. Ferner RE, Gutmann DH. International consensus
statement on malignant peripheral nerve
sheath tumors in neurofi bromatosis. Cancer Res
2002;62:1573–7.
16. Evans DG, Baser ME, McGaughran J, et al.
Malignant peripheral nerve sheath tumours in
neurofi bromatosis 1. J Med Genet 2002;39:311–14.
17. Sharif S, Ferner R, Birch JM, et al. Second primary
tumors in neurofi bromatosis 1 patients treated for
optic glioma: substantial risks after radiotherapy. J
Clin Oncol 2006;24:2570–5.
18. Ferner RE, Hughes RA, Hall SM, et al.
Neurofi bromatous neuropathy in
neurofi bromatosis 1 (NF1). J Med Genet
2004;41:837–41.
19. De Raedt T, Brems H, Wolkenstein P, et al. Elevated
risk for MPNST in NF1 microdeletion patients. Am J
Hum Genet 2003;72:1288–92.
20. Ferner RE, Golding JF, Smith M, et al. [18F]2-
fl uoro-2-deoxy-D-glucose positron emission
tomography (FDG PET) as a diagnostic tool for
neurofi bromatosis 1 (NF1) associated malignant
peripheral nerve sheath tumours (MPNSTs): a long-
term clinical study. Ann Oncol 2008;19:390–4.
21. North KN, Riccardi V, Samango-Sprouse C, et al.
Cognitive function and academic performance in
neurofi bromatosis. 1: consensus statement from
the NF1 Cognitive Disorders Task Force. Neurology
1997;48:1121–7.
22. Krab LC, de Goede-Bolder A, Aarsen FK, et al. Effect
of simvastatin on cognitive functioning in children
with neurofi bromatosis type 1: a randomized
controlled trial. JAMA 2008;300:287–94.
23. Ferner RE, Hughes RA, Johnson MR.
Neurofi bromatosis 1 and multiple sclerosis. J
Neurol Neurosurg Psychiatry 1995;58:582–85.
24. Listernick R, Ferner RE, Liu GT, et al. Optic pathway
gliomas in neurofi bromatosis-1: controversies and
recommendations. Ann Neurol 2007;61:189–98.
25. Miettinen M, Fetsch JF, Sobin LH, et al.
Gastrointestinal stromal tumors in patients with
neurofi bromatosis 1: a clinicopathologic and
molecular genetic study of 45 cases. Am J Surg
Pathol 2006;30:90–6.
26. Schindeler A, Little DG. Recent insights into bone
development, homeostasis, and repair in type 1
neurofi bromatosis (NF1). Bone 2008;42:616–22.
27. Friedman JM, Arbiser J, Epstein JA, et al.
Cardiovascular disease in neurofi bromatosis 1:
report of the NF1 Cardiovascular Task Force. Genet
Med 2002;4:105–11.
28. Wishart JH. Case of tumours in the skull, dura
mater, and brain. Edinburgh Med Surg J 1822;18;
393–97.
29. Evans DG, Baser ME, O’Reilly B, et al. Management
of the patient and family with neurofi bromatosis 2:
a consensus conference statement. Br J Neurosurg
2005;19:5–12.
30. Baser ME, Friedman JM, Wallace AJ, et al.
Evaluation of clinical diagnostic criteria for
neurofi bromatosis 2. Neurology 2002;59:1759–65.
31. MacCollin M, Chiocca EA, Evans DG, et al.
Diagnostic criteria for schwannomatosis. Neurology
2005;64:1838–45.
32. Hadfi eld KD, Newman WG, Bowers NL et al.
Germline mutation of INI/SMARCB1 in familial
schwannomatosis. Am J Hum Genet 2007;80:805–10.
33. Trofatter JA, MacCollin MM, Rutter JL, et al.
A novel moesin-, ezrin-, radixin-like gene is a
candidate for the neurofi bromatosis 2 tumor
suppressor. Cell 1993;72:791–800.
34. Rouleau GA, Merel P, Lutchman M, et al. Alteration
in a new gene encoding a putative membrane-
organizing protein causes neuro-fi bromatosis type
2. Nature 1993;363:515–21.
35. Kanowitz SJ, Shapiro WH, Golfi nos JG, et al.
Auditory brainstem implantation in patients
with neurofi bromatosis type 2. Laryngoscope
2004;114:2135–46.
36. Lustig LR, Yeagle J, Driscoll CL, et al. Cochlear
implantation in patients with neurofi bromatosis
type 2 and bilateral vestibular schwannoma. Otol
Neurotol 2006;27:512–18.
37. Rowe JG, Radatz MW, Walton L, et al. Clinical
experience with gamma knife stereotactic
radiosurgery in the management of vestibular
schwannomas secondary to type 2 neurofi bromatosis.
J Neurol Neurosurg Psychiatry 2003;74:1288–93.
38. Plotkin SR, Stemmer-Rachamimov AO, Barker FG
2nd, et al. Hearing improvement after bevacizumab
in patients with neurofi bromatosis type 2. N Engl J
Med 2009;361:358–67.
39. Sperfeld AD, Hein C, Schröder JM, et al. Occurrence
and characterization of peripheral nerve
involvement in neurofi bromatosis type 2. Brain
2002;125:996–1004.
40. Trivedi R, Byrne J, Huson SM , et al. Focal
amyotrophy in neurofi bromatosis 2.. J Neurol
Neurosurg Psychiatry 2000;69:257–61.
04_pn206532.indd 9304_pn206532.indd 93 3/6/2010 4:57:22 PM3/6/2010 4:57:22 PM