Embed Size (px)
Citation preview

Germ-Line Mutations of the p16INK4(MTS1 ) Gene Occur in aSubset of Patients With Hepatocellular Carcinoma
PASCAL CHAUBERT,1 RENE GAYER,2 ARTHUR ZIMMERMANN,2 CHARLOTTE FONTOLLIET,1 BERNHARD STAMM,3 FRED BOSMAN,1
AND PHILLIP SHAW1
inactivation of p53 by the virally encoded protein HBX.7 AThe molecular mechanisms of hepatocarcinogenesisrecent study on potential familial HCC in Alaskan nativesare poorly understood. Only very recently has thereexcluded mutation of the p53 gene as the responsible geneticbeen a suggestion of familial hepatocellular carcinomalesion.1 This suggests that another tumor-suppressor gene(HCC). We have analyzed the status of the p16INK4(MTS1)may be involved in the development of familial HCC. Degene, a cyclin-dependent kinase inhibitor, in 26 patientsSouza et al. reported 70% of human HCC exhibited loss ofwith HCC of different etiologies. Four patients car-heterozygosity (LOH) at 6q26-7.8 They further showed thatried hemizygous germ-line point mutations of the25% of HCC with LOH contain a point mutation in the man-p16INK4(MTS1) gene, suggesting the existence of familialnose 6-phosphate/insulin-like growth factor.9HCC involving this gene. The wild-type allele was lost
Recently a new tumor-suppressor gene, p16INK4(MTS1 ),in the tumor in 2 of these 4 patients. Three of the patientscoding for an inhibitor of cyclin-dependent kinase 4,10 wascarrying a germ-line mutation had non–cirrhosis-associ-isolated and mapped to chromosome 9p21, a locus frequentlyated HCC. No somatic mutations of p16INK4(MTS1) werelost in diverse malignancies.11 Germ-line mutations of theobserved in the 26 cases of HCC. The most common so-p16INK4(MTS1 ) gene have been identified in hereditary mela-matic alteration of the p16INK4(MTS1) gene in HCC wasnomas.12 In addition, the gene is homozygously deleted orde novo methylation, which was detected in 48% of themutated in uncultured tumors of diverse origin,13 includingcases. Low levels (21%) of p16INK4(MTS1) gene allele losspancreatic adenocarcinomas,14 melanomas,12 esophageal car-were observed. Altogether, these results indicate thatcinomas,15,16 and gliomas.17 Most recently, it has been re-alteration of the p16INK4(MTS1) gene plays an importantported that silencing of the p16INK4(MTS1 ) gene promoter byrole in the genesis of HCC. (HEPATOLOGY 1997;25:1376-de novo methylation occurs in a variety of tumors.181381.)
We analyzed the 3 exons of the p16INK4(MTS1 ) gene bysingle-strand conformation polymorphism (SSCP) and DNAHepatocellular carcinoma (HCC) is one of the most fre- sequencing in 26 patients with HCC with different etiologi-quent human malignancies worldwide. Its incidence shows cal/pathological backgrounds. In addition, we determined thea striking geographic variability, with a high prevalence in methylation status and allele-loss frequency of thepopulations exposed to aflatoxin B1. Other major etiologic p16INK4(MTS1 ) gene in HCC. Our results suggest that (1) afactors for HCC development are hepatitis B or C virus infec- subset of noncirrhotic HCC cases could be familial, as sug-tion and cirrhosis. Recently, the existence of familial inheri- gested by germ-line mutations of p16INK4(MTS1 ); and (2) so-tance of HCC in an Alaskan population has been suggested.1 matic inactivation of the p16INK4(MTS1 ) gene by methylationThe molecular mechanisms involved in hepatocarcinogen- or deletion is frequently observed in human hepatocarcino-esis remain poorly understood. The most widely known can- genesis.cer-associated gene in HCC is p53. Somatic mutations in co-
don 249 have been identified at a high frequency in HCC PATIENTS AND METHODSfrom African and Chinese populations exposed to aflatoxin
Patients. Twenty-six patients who underwent partial hepatec-B1.2,3 However, transfection of a murine p53 gene mutated tomy for HCC in the Departments of Surgery of the University Hospi-at the position corresponding to human codon 249 into hepa- tals of Bern or Lausanne (Switzerland) were studied. Tumor andtocytes is insufficient to transform hepatocytes.4 In Western nontumor liver tissue samples were available for histological exami-and other low–aflatoxin B1–exposed countries, somatic p53 nation and DNA extraction. In all cases, the tumor-free liver paren-
chyma surrounding the tumor was carefully examined histopatholog-gene alterations are infrequently associated with HCC.5,6
ically. Alcohol abuse–related HCC with cirrhosis is the most commonAlso, hepatitis B– and C–related HCC display a low inci-type observed in Switzerland. Because it is rarely treated with sur-dence of p53 mutations, possibly because of the functionalgery, our HCC samples lacking cirrhosis are overrepresented relativeto actual incidence. The relevant clinicopathological characteristicsare summarized in Table 1. All patients were white Swiss citizensexcept patient 11, who was a Bengali refugee. A control group of
Abbreviations: HCC, hepatocellular carcinoma; HBX, X protein encoded by hepatitis B159 individuals without manifest neoplasms was also analyzed forvirus; LOH, loss of heterozygosity; MTS1, multiple tumor suppressor 1; SSCP, single-strandp16INK4(MTS1 ) germ-line alterations.conformation polymorphism; PCR, polymerase chain reaction; bp, base pairs; CEPH, Centre
DNA Extraction. The tissues analyzed were either frozen or forma-d’Etude du Polymorphisme Humain.From the 1Institut Universitaire de Pathologie, Lausanne, Switzerland; 2Pathologisches lin-fixed and paraffin-embedded. For frozen tissues, DNA was ex-
Institut der Universitat Bern, Bern, Switzerland; and the 3Pathologisches Institut, Kantons- tracted from five 20-mm-thick cryostat sections using the Elu-Quickspital, Aarau, Switzerland. DNA purification kit (Schleicher & Schuell, Dassel, Germany) ac-
Received October 16, 1996; accepted February 18, 1997. cording to the manufacturer’s specifications. For formalin-fixed tis-Supported in part by the Swiss National Research Foundation (P.S.) and the Swiss sues, the regions of interest were identified, and the corresponding
Cancer League (P.S.).tissues were scraped directly from the paraffin blocks, boiled 10 min-Address reprint requests to: Pascal Chaubert, M.D., Institut Universitaire de Pathologie,utes at 1007C in 50 mL of TE buffer (10 mmol/L Tris-HCl, 1 mmol/LRue du Bugnon 25, CH-1011 Lausanne, Switzerland. Fax: (41) 21-314-71-15.ethylenediaminetetraacetic acid [EDTA], pH 8.0). Three microlitersCopyright q 1997 by the American Association for the Study of Liver Diseases.
0270-9139/97/2506-0014$3.00/0 were used for polymerase chain reaction (PCR).
1376
AID Hepa 0027 / 5p21$$$521 05-20-97 20:27:13 hptas WBS: Hepatology

HEPATOLOGY Vol. 25, No. 6, 1997 CHAUBERT ET AL. 1377
PCR. A 204–base pair (bp) fragment containing exon 1 of the lower intensity of the wild-type bands suggests a deletion ofp16INK4(MTS1 ) gene was amplified using the following primers: 1x, the wild-type allele (Fig. 2A). Deletion of a p16INK4(MTS1 )GGGAGCAGCATGGAGCCG; 1y, AGTCGCCCGCCATCCCCT. For gene allele in the HCC of patient 8 was confirmed by D9S171exon 2, three overlapping fragments, 2A (171 bp), 2B (170 bp), and microsatellite analysis (Table 1). The family histories of these2C (169 bp), were amplified separately using the following primers: two patients did not provide any indication for any other2Ax, CTGGCTCTGACCATTCTGT; 2Ay, AGCACCACCAGCGTG-
tumors, including HCC, in family members.TCC; 2Bx, GACCCCGCCACTCTCACC; 2By, AGGTACCGTGCG-Patient 11 carried a hemizygous germ-line substitution atACATCGC; 2Cx, GATGCCTGGGGCCGTCT; 2Cy, CAGGGTACA-
position 04 of the splice acceptor site in intron 1 (GCAG rAATTCTCAGAT. For exon 3, the following primers were used: 3x,GTAGGGACGGCAAGAGA; 3y, ACCTTCGGTGACTGATG; yielding CCAG). By SSCP analysis, the alteration resulted in twoa fragment of 159 bp. The thermal cycle profile was 30 seconds at additional bands (Fig. 2B). In the nontumor tissue, the inten-947C, 45 seconds at 557C (exons 2C and 3) or 587C (exons 1, 2A, and sities of the bands corresponding to the mutant and wild-2B), and 45 seconds at 737C. This cycle was repeated 30 times. type alleles were similar. In the HCC tissue, the wild-type
The D9S 171 microsatellite was analyzed as described.18
bands were weaker than the mutant bands (Fig. 2B), indicat-SSCP. PCR products were directly subjected to nonradioactive ing wild-type allele deletion. Unfortunately, this patient wasSSCP analysis according to the method of Chaubert et al.19 Briefly,
not informative for the microsatellite marker D9S171. The10 to 20 ng of PCR product were denaturated in 10 mL of 50 mmol/patient’s family history was not available. The absence ofL NaOH and 1 mmol/L EDTA at 507C for 10 minutes. After thethis alteration in the 159 control patients suggests a muta-addition of 1.5 mL of formamide dye mixture, the samples were imme-
diately loaded on a 10% nondenaturating polyacrylamide gel (acryl- tion rather than a polymorphism. The sequence alteration,amide/bisacrylamide, 49:1) containing 5% glycerol and run at 20 V/ lying between the polypyrimidine tract and the invariant 3*cm in 0.51 Tris-borate EDTA buffer for approximately 3 hours. The AG dinucleotide, may affect messenger RNA (mRNA) splicingtemperature was maintained at 207C. After electrophoresis, the gels and, consequently, appropriate protein expression.21
were stained using the Silver Stain Plus kit (Bio-Rad, Hercules, CA). Patient 20 displayed a hemizygous germ-line substitutionExons 2C and 3, amplified by PCR, were digested with KspI and in p16INK4(MTS1 ) codon 148 (GCG r ACG; Ala r Thr). ByMspI, respectively.
SSCP analysis, the novel allele (A2) was characterized byDNA Sequencing. PCR products were cloned into the pGEM-T vec-three bands in addition to the single band corresponding totor (Promega, Madison, WI) according to the manufacturer’s recom-the normal allele (A1). This substitution alters a Ksp I restric-mendations. The DNA from each clone was screened by PCR-SSCP
to identify clones containing either a wild-type or a mutated allele. tion site. Only half of the HCC PCR product of patient 20Both strands of two independent clones for each SSCP pattern were could be digested, indicating that no allele loss had occurredsequenced on a Pharmacia L.K.B. A.L.F. automatic sequencer (Phar- (data not shown). This sequence alteration has been de-macia P-L Biochemicals, Milwaukee, WI). scribed previously in different tumor types.13,22 Because it
Methylation of p16INK4(MTS1) First Exon. The methylation status has also been found in DNA from Centre d’Etude du Polymor-of the first exon of p16INK4(MTS1 ) was determined essentially as phisme Humain (CEPH) reference families, it is considereddescribed.20 The oligonucleotide primers used were as follows: 1x,
a polymorphism.12GGGAGCAGCATGGAGCCG; 1mety, CTGGATCGGCCTCCGACC-
SSCP Analysis of the p16INK4(MTS1) Alternative Promoter—GTA. All DNA samples were digested with the restriction enzymesEncoded p19ARF (ORF2) Exon 1b. Recently, it has been dem-Msp I, Ksp I and Hpa II, extracted with chloroform/phenol and pre-
cipitated before PCR. PCR (22 cycles) products were separated on onstrated that an alternative promoter of the p16INK4(MTS1 )1.5% agarose gels before transfer and hybridization with a gene can be used, resulting in a novel first exon 1b splicedp16INK4(MTS1 ) complementary DNA (cDNA) probe as described.20 to the previously described exon 2 of p16INK4(MTS1 ). This
alternatively spliced mRNA encodes a novel protein se-RESULTS quence, referred to as ORF2 (open reading frame 2) in hu-
mans and p19ARF in mice, from the common nucleic acid se-Genomic DNA from 26 HCC samples and the correspond-ing nontumor tissue were screened for p16INK4(MTS1 ) se- quence of exon 2.23-25 Overexpression of p19ARF (in mouse)
results in cell-cycle arrest.24 We examined exon 1b of ORF2quence alterations (exons 1-3) by PCR-SSCP. PCR productsexhibiting novel bands by SSCP were cloned and sequenced. in our 26 patients by PCR-SSCP. No mutations were detected
(Chaubert, data not shown). The germ-line exon 2 mutations,A summary of the p16INK4(MTS1 ) gene alterations observedin the 26 HCC patients is given in Table 1. None of the described above, would alter both the p16 and ORF2 proteins,
as indicated in Figs. 1 and 2.observed germ-line mutations of the p16INK4(MTS1 ) genewere found in the 159 control patients examined by PCR- De Novo Methylation of Exon 1 of the p16INK4(MTS1) Gene
in HCC. Several groups have recently demonstrated a corre-SSCP.Germ-Line p16INK4(MTS1) Mutations in HCC. In patient 4, lation between the methylation status of exon 1 and expres-
sion of p16INK4(MTS1 ) mRNA.18,20,26 When exon 1 of thea hemizygous germ-line substitution in p16INK4(MTS1 ) codon54 (ATG r ATT; Met r Ile) was observed. On SSCP analysis, p16INK4(MTS1 ) gene is methylated, no p16INK4(MTS1 ) mRNA
expression is detected either in cell lines or in primary tu-the mutant allele was characterized by three additionalbands (Fig. 1). No evidence of allele loss was found in the mors.18 Digestion of patient DNAs with methylation-sensitive
restriction enzymes (Ksp I and Hpa II) with sites within exonHCC. The family history revealed that the patient’s motherdied 11 years earlier and that a neoplasm was identified in 1 of p16INK4(MTS1 ) before PCR amplification allows the de-
termination of methylation status of the original genomicher liver at that time. Histologically and immunohistologi-cally, the tumor was of a mixed hepatocellular/cholangiocellu- DNA.20 If the p16INK4(MTS1 ) gene exon 1 is methylated, the
restriction enzymes will not cut, and a PCR product will belar carcinoma character. PCR-SSCP and sequencing of clonedp16INK4(MTS1 ) DNA from a biopsy specimen from the mother obtained.
p16INK4(MTS1 ) methylation status was analyzed in 25 ofrevealed the same hemizygous mutation in codon 54 as wasfound in her son (Fig. 1). the 26 patients with HCC (Table 1). Both undigested and
non–methyl-sensitive Msp I–digested samples served as pos-A hemizygous germ-line mutation in p16INK4(MTS1 ) codon58 (CGA r TGA; Arg r STOP), previously identified in a itive and negative controls, respectively, for each patient ana-
lyzed. Examples of these analyses are presented for patientsmelanoma family,12 was found in nontumor tissue in patients5 and 8. The SSCP pattern was characterized by the presence 6 and 9 in Fig. 3. All nontumor liver samples examined were
unmethylated within exon 1. Twelve of 25 HCCs (48%) exhib-of two additional bands (Fig. 2A). The intensity of the bandscorresponding to the mutant and wild-type alleles was simi- ited de novo methylation of the p16INK4(MTS1 ) gene exon 1
(Table 1).lar in nontumor tissue. In the HCC tissue from patient 8, the
AID Hepa 0027 / 5p21$$$521 05-20-97 20:27:13 hptas WBS: Hepatology

1378 CHAUBERT ET AL. HEPATOLOGY June 1997
TABLE 1. Clinicopathological Data and p16INK4(MTS1) Status in 26 Patients With HCC
p16 Sequence‡ LOHSex/Age Etiologic Meth
Patient (yr) Cirrhosis?* Factors Grade† HCC Nontumor Exon 1§ Other\ D9S171Ø
1 M/67 U 3 wt wt / NI 02 M/64 N Hemo 1 wt wt 0 0 NI3 M/33 N 2 wt wt 0 NI 04 M/64 N 2 54 ATG r ATT 54 ATG r ATT 0 0 05 M/76 N 2 58 CGA r TGA 58 CGA r TGA 0 0 NI6 M/75 N 2 wt wt / NI NI7 M/62 Y 2 wt wt 0 NI 08 M/69 N 3 58 CGA r TGA 58 CGA r TGA / / /9 M/78 N 2 wt wt / NI NI
10 M/78 Y HBV 1 wt wt 0 NI 011 M/29 Y HBV 1 G r C intron 1 G r C intron 1 0 / NI12 F/54 N 1 wt wt / NI 013 F/52 Y HCV 3 wt wt / 0 NI14 F/55 Y HCV 2 wt wt / NI NI15 M/62 Y OH 1 wt wt 0 NI 016 M/79 Y OH 2 wt wt / / /17 M/71 Y OH 1 wt wt 0 NI 018 M/51 N 2 wt wt ND NI 019 M/67 Y HBV 2 wt wt / NI NI20 F/36 N 2 148 GCG r ACG 148 GCG r ACG / 0 021 M/76 N 3 wt wt / NI 022 M/57 Y OH 2 wt wt 0 NI 023 M/69 N 4 wt wt 0 NI NI24 M/37 N 2 wt wt 0 NI /25 M/67 Y HCV 2 wt wt / NI NI26 M/69 Y OH 1 wt wt 0 NI NI
U, undetermined; hemo, hemochromatosis; HBV, hepatitis B virus infection; HCV, hepatitis C virus infection; OH, alcohol abuse; wt, wild-type sequence;/, methylation; 0, no methylation; ND, not done; NI, not informative; /, allele loss; 0, no allele loss.
* Presence or absence of cirrhotic changes in the tumor-free liver parenchyma as determined by histological examination.† Histological grade of the HCC according to Edmondson and Steiner.33
‡ p16 sequence of exons 1-3 in HCC tissues and tumor-free liver tissues.§ Methylation status of p16 exon 1 in HCC tissues.\ Loss of heterozygosity in HCC tissue determined by studying the C to G polymorphism localized 29 bp downstream of p16 exon 3 or one of the heterozygous
substitutions in exon 2.Ø Loss of heterozygosity in HCC tissue determined by microsatellite D9S171 analysis.
p16INK4(MTS1) Gene Allele Loss in HCC. p16INK4(MTS1 )gene allele loss (Table 1) was assessed by three differenttechnical approaches: (1) SSCP analysis of normal and tumortissue of patients containing a p16INK4(MTS1 ) germ-line mu-tation (Fig. 2); (2) SSCP analysis of an Msp I polymorphismdownstream of the coding region in exon 3 (Fig. 4); and (3)LOH as determined by the microsatellite marker D9S171adjacent to the p16INK4(MTS1 ) gene (Fig. 4).18
Patients 8 and 11, both of whom had germ-line mutations,displayed wild-type allele loss in their HCCs, which could bedetected by SSCP analysis (Fig. 2). Only the allele loss inpatient 8 could be confirmed by LOH with the microsatellitemarker, D9S171. Patient 11 was not informative at this lo-cus.
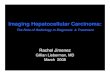
Patients 2, 13, and 16 were heterozygous for a germ-linepolymorphism (C r G), affecting an MspI restriction site iden-tified 29 bp downstream of the coding region in exon 3. BySSCP analysis, the allele with an Msp I restriction site wascharacterized by three additional bands (Fig. 4). The PCRproducts were also digested with MspI to quantify the A1and A2 alleles (Fig. 4). In nontumor tissues from all 3 pa-tients, the band intensity of the two alleles was equivalent,as expected for heterozygotes. By contrast, in HCC tissuefrom patient 16, the A1 bands were weaker than the A2 bands(Fig. 4), indicating A1-allele deletion. Allele deletion of theFIG. 1. Germ-line mutation of p16INK4(MTS1 ) exon 2 in the family of pa-
tient 4. Family members affected by liver neoplasm are indicated by filled-in p16INK4(MTS1 ) gene in patient 16 was confirmed by D9S171symbols. SSCP analysis of the mother (row 2) and the son (patient 4; row 1) microsatellite analysis (Fig. 4 and Table 1).is presented with wild-type allele controls. Analysis of tumor tissue is shown. Analysis of p16INK4(MTS1 ) allele loss for the 26 HCC withSequence alteration in these two patients is given at right. The affected codon
the D9S171 microsatellite marker (informative in 15/26for both p16INK4(MTS1 ) and ORF2 is indicated. T, tumor; NT, nontumor tissue.*Novel SSCP bands; WT, wild-type allele bands. cases) revealed an additional HCC with p16INK4(MTS1 ) allele
AID Hepa 0027 / 5p21$$$521 05-20-97 20:27:13 hptas WBS: Hepatology

HEPATOLOGY Vol. 25, No. 6, 1997 CHAUBERT ET AL. 1379
FIG. 2. Germ-line mutations ofp16INK4(MTS1 ). (A) Patients 5 and 8carry the same mutation in exon 2. TheSSCP analysis of patient 8 is shown. Lossof the wild-type allele in the HCC of thispatient is shown by the lower intensityof wild-type allele bands. No allele loss inthe HCC of patient 5 was evident. PCR-SSCP of wild-type and mutant clonesare included. The sequence alteration isindicated at right with the alteredp16INK4(MTS1 ) and ORF2 codons. (B) Anintron 1 splice acceptor mutation in pa-tient 11. SSCP analysis and sequence de-termination are shown. Loss of the wild-type allele in the HCC from this patientis shown by the lower intensity of wild-type allele bands. Sequence alteration isindicated at right. T, tumor; NT, nontu-mor tissue. *Novel SSCP bands; WT,wild-type allele bands.
loss (patient 24, Table 1). Combining the results of the three p16INK4(MTS1) Gene Involvement in HCC. The involvementof p16INK4(MTS1 ) gene inactivation in HCC has been pro-techniques, we observed LOH in 4 of 19 informative HCCs
(21%). posed recently by Hui et al.28 This group reported that 50%of HCC cell lines and 34% of primary HCC lacked detectable
DISCUSSION p16 protein, and they suggested that p16INK4(MTS1 ) is dereg-ulated posttranscriptionally.The p16INK4(MTS1 ) gene has recently been confirmed to be
We have analyzed the sequence, the allele number, and thea tumor-suppressor gene by the analysis of p16 gene knock-methylation status of the p16INK4(MTS1) gene in 26 HCC andout mice.27 The development of homozygous null p16 micecorresponding nontumor tissues. We found that 61% of HCC (16/is normal, but spontaneous tumors arise precociously.27 The26) exhibited alterations of the p16INK4(MTS1) gene. The major-predominant tumor types are B-cell lymphomas and soft tis-ity of these alterations was somatic (tumor-specific methylationsue sarcomas. Although germ-line mutations have been iden-of p16 promoter, tumor-specific LOH). Four patients were foundtified in the p16INK4(MTS1 ) gene in both familial melanoma12
to have a germ-line p16INK4(MTS1) mutation. Two of these pa-and pancreatic cancer,14 no melanomas or pancreatic carcino-mas were observed in homozygous null knock-out mice. tients showed loss of the wild-type allele in their HCCs.
FIG. 3. De novo methylation of the p16INK4(MTS1 ) gene. Genomic DNA ofnontumor (A) and tumor tissue (B) from patients 6 and 9 were digested withMsp I, Ksp I, and Hpa II (see Patients and Methods) before PCR amplificationof p16INK4(MTS1 ) exon 1. Undigested genomic DNA was included as a control.PCR reactions were continued for 22 cycles and separated on 1.5% agarose gelsand transferred to positively charged membranes before hybridization with ap16INK4(MTS1 ) cDNA probe. Both nontumor tissues are unmethylated, becauseno amplification by PCR can be seen after digestion with Ksp I and Hpa II. Incontrast, the HCC DNA is methylated, because digestion with Ksp I and Hpa IIdoes not affect amplification by PCR. NT, nontumor.
AID Hepa 0027 / 5p21$$$521 05-20-97 20:27:13 hptas WBS: Hepatology

1380 CHAUBERT ET AL. HEPATOLOGY June 1997
Genetic Complexity in HCC. It is striking that the age ofonset of non–cirrhosis-associated HCC in patients withgerm-line p16INK4(MTS1 ) mutations is not particularly preco-cious. A possible explanation for the late appearance of famil-ial HCC might be that a large number of genes is involvedin HCC. That HCC is a genetically complex tumor fits withthe number of chromosomal regions exhibiting significantLOH (1p, 4q, 5q, 8p, 11p, 13q, 16q, and 17p).29,30 Chromo-somal region 6q26-7 has been also shown to be frequentlylost in HCCs.8 The mannose 6-phosphate/insulin-like growthfactor II receptor gene at this chromosomal locus was foundmutated in 25% of the HCCs exhibiting 6q26 LOH.9 Unfortu-nately, attempts to identify genes corresponding to the otherregions of LOH have been unsuccessful thus far, with theexception of the p53 gene on 17p.
Somatic Alterations of the p16INK4(MTS1) Gene in HCC.Genes in which lesions have been identified in hereditarysyndromes are often altered somatically in sporadic tumorsas well, e.g., the Rb gene and sporadic retinoblastoma. In thepresent series, none of the patients with HCC had a somaticmutation in the p16INK4(MTS1 ) gene.
LOH analysis of the p16INK4(MTS1 ) gene in the HCC sam-ples showed that 4 of the 19 informative cases (21%) exhibiteddeletion of one p16INK4(MTS1 ) allele. In 3 cases (patients 8,11, and 16), the loss of one allele was associated with analteration of the other allele (germ-line mutation or methyla-tion), indicating complete gene inactivation. In the fourthcase (patient 24), the remaining allele was apparently nor-mal.
De novo methylation, an alternative means of functionallysilencing the p16INK4(MTS1 ) gene, has recently been de-FIG. 4. Msp I polymorphism 29 bp downstream from the p16INK4(MTS1 )scribed.18 Cell lines and tumors exhibiting methylation of thethird exon. Two of the 3 patients (patients 2, 13, 16) observed to be heterozy-
gous for this polymorphism are presented. (A) PCR-SSCP of patients 2 and CpG island adjacent to the p16INK4(MTS1 ) gene do not ex-16. HCC from patient 16 displays loss of the A2 allele. Analysis of the cloned press p16INK4(MTS1 ) mRNA.18 In the present series, 48% ofalleles is included for comparison. (B) PCR products corresponding to the SSCP the HCCs analyzed were found to be de novo methylated inanalysis were digested with Msp I and separated on 3% agarose gel. Allele
the first exon of p16INK4(MTS1 ). Thus, de novo methylationloss in the HCC from patient 16 is shown by the lower-intensity A2 allelebands. (C) Analysis of the D9S171 microsatellite marker in patients 2 and 16. (silencing) is the predominant somatic mechanism ofPatient 2 is not informative at this locus. Patient 16 is heterozygous (informa- p16INK4(MTS1 ) gene inactivation in HCC.tive). LOH was observed in the patient’s tumor, as shown by the disappearance Globally, half (6/12) of the HCCs associated with one of theof one band (*). A1, allele 1 bands; A2, allele 2 bands; L, position of denatured
major etiologic factors (cirrhosis, hepatitis B and C viruses)linear DNA; T, tumor; NT, nontumor tissue.showed a tumor-specific alteration in the p16INK4(MTS1 )gene (methylation, LOH, or both), indicating that somaticp16INK4(MTS1 ) alterations may also be involved in the gene-p16INK4(MTS1) Germ-Line Mutations–Familial HCC? The
present findings strongly suggest that lesions of the sis of classical nonfamilial HCC. It has been shown that de-regulation of the cell cycle by alterations of p16INK4(MTS1 )p16INK4(MTS1 ) gene are involved in a familial form of hepato-
cellular carcinoma. We found a p16INK4(MTS1 ) hemizygous requires an intact Rb gene.31 Analysis of the Rb gene in HCCindicated that mutation and deletion are rarely observed,32germ-line mutation in 4 HCC patients, three of whom lacked
cirrhosis as well as other well-known etiologic factors. In consistent with the idea that a frequent cause of cell-cyclegrowth deregulation in HCC might be p16INK4(MTS1 ) geneother words, 23% of non–cirrhosis-related HCCs (3/13) were
associated with a germ-line mutation of the p16INK4(MTS1 ) alterations.Clinical Implications. A subset of HCCs developing in non-gene. The wild-type allele of p16INK4(MTS1 ) was lost in the
HCC in 2 of the 4 patients with germ-line mutations. An cirrhotic liver might be familial, as suggested by the presenceof germ-line p16INK4(MTS1 ) gene mutations. Consequently, aidentical germ-line mutation in p16INK4(MTS1 ) codon 54 was
found in 1 HCC patient as well as in the liver neoplasm of closer examination of patients with non–cirrhosis-associatedHCC and their families should be undertaken. Analysis ofhis mother, supporting the existence of a familial HCC form
involving the p16INK4(MTS1 ) gene. The confirmation of a fa- the p16INK4(MTS1 ) gene should be included as a standardprotocol for these patients. Members of families carrying amilial component in HCC awaits further studies of complete
families. Because there was no suspicion of a familial compo- germ-line p16INK4(MTS1 ) gene mutation should be followedup carefully, and preventive measures such as immunizationnent in HCC until only very recently, such families are diffi-
cult to find.1 against hepatitis B virus should be considered.Patient 11, displaying a germ-line splice acceptor site mu-
tation of p16INK4(MTS1 ), had serology positive for hepatitis Acknowledgment: The authors thank M. M. Bertholet, J.B virus. He underwent surgery for HCC at 29 years of age. Maillardet, and C. Chiesa for technical assistance.The precocious appearance of this HCC may suggest thata germ-line p16INK4(MTS1 ) mutation in conjunction with REFERENCEShepatitis B infection can accelerate the development of HCC.
1. De Benedetti VM, Welsh JA, Trivers GE, Horpster A, Parkinson AJ, LanierThis possibility is currently being investigated using a AP, McMahon BJ. p53 is not mutated in hepatocellular carcinomas fromp16INK4(MTS1 ) gene analysis in a human population with Alaska Natives. Cancer Epidemiol Biomarkers Prev 1995;4:79-82.
2. Bressac B, Kew M, Wands J, Ozturk M. Selective G to T mutations of p53high hepatitis B exposure.
AID Hepa 0027 / 5p21$$$521 05-20-97 20:27:13 hptas WBS: Hepatology

HEPATOLOGY Vol. 25, No. 6, 1997 CHAUBERT ET AL. 1381
gene in hepatocellular carcinoma from southern Africa. Nature 1991;350: 18. Merlo A, Herman JG, Mao L, Lee DJ, Gabrielson E, Burger PC, BaylinSB, et al. 5* CpG island methylation is associated with transcriptional429-431.
3. Hsu IC, Metcalf RA, Sun T, Welsh JA, Wang NJ, Harris CC. Mutational silencing of the tumour suppressor p16/CDKN2/MTS1 in human cancers.Nat Med 1995;1:686-692.hotspot in the p53 gene in human hepatocellular carcinomas. Nature 1991;
350:427-428. 19. Chaubert P, Bautista D, Benhattar J. An improved method for rapidscreening of DNA mutations by nonradioactive single-strand conformation4. Dumenco L, Oguey D, Wu J, Messier N, Fausto N. Introduction of a murine
p53 mutation corresponding to human codon 249 into a murine hepatocyte polymorphism procedure. Biotechniques 1993;15:586.20. Gonzalez-Zulueta M, Bender CM, Yang AS, Nguyen T, Beart RW, Vancell line results in growth advantage, but not in transformation. HEPATOL-
OGY 1995;22:1279-1288. Tornout JM, Jones PA. Methylation of the 5¢ CpG island of the p16/CDKN2 tumor suppressor gene in normal and transformed human tissues5. Challen C, Lunec J, Warren W, Collier J, Bassendine MF. Analysis of the
p53 tumor-suppressor gene in hepatocellular carcinomas from Britain. correlates with gene silencing. Cancer Res 1995;55:4531-4535.HEPATOLOGY 1992;16:1362-1366. 21. Jaruzelska J, Abadie V, d’Aubenton-Carafa Y, Brody E, Munnich A, Marie
6. Kress S, Jahn UR, Buchmann A, Bannasch P, Schwarz M. p53 mutations J. In vitro splicing deficiency induced by a C to T mutation at position 03in human hepatocellular carcinomas from Germany. Cancer Res 1992;52: in the intron 10 acceptor site of the phenylalanine hydroxylase gene in a3220-3223. patient with phenylketonuria. J Biol Chem 1995;270:20370-20375.
7. Wang XW, Forrester K, Yeh H, Feitelson MA, Gu JR, Harris CC. Hepatitis 22. Hatta Y, Hirama T, Takeuchi S, Lee E, Pham E, Miller CW, StrohmeyerB virus X protein inhibits p53 sequence-specific DNA binding, transcrip- T, et al. Alterations of the p16(MTS1 ) gene in testicular, ovarian, andtional activity, and association with transcription factor ERCC3. Proc Natl endometrial malignancies. J Urol 1995;154:1954-1957.Acad Sci U S A 1994;91:2230-2234. 23. Stone S, Jiang P, Dayananth P, Tavtigian SV, Katcher H, Parry D, Peters
8. De Souza AT, Hankins GR, Washington MK, Fine RL, Orton TC, Jirtle G, et al. Complex structure and regulation of the p16(MTS1 ) locus. CancerRL. Frequent loss of heterozygosity on 6q at the mannose 6-phosphate/ Res 1995;55:2988-2994.insulin-like growth factor II receptor locus in human hepatocellular tu- 24. Quelle DE, Zindy F, Ashmun RA, Sherr CJ. Alternative reading framesmors. Oncogene 1995;10:1725-1729. of the INK4a tumor suppressor gene encode two unrelated proteins capable
9. De Souza AT, Hankins GR, Washington MK, Orton TC, Jirtle RL. M6P/ of inducing cell cycle arrest. Cell 1995;83:993-1000.IGF2R gene is mutated in human hepatocellular carcinomas with loss of 25. Mao L, Merlo A, Bedi G, Shapiro GI, Edwards CD, Rollins BJ, Sidranskyheterozygosity. Nat Genet 1995;11:447-449. D. A novel p16INK4A transcript. Cancer Res 1995;55:2995-2997.
10. Serrano M, Hannon GJ, Beach D. A new regulatory motif in cell-cycle 26. Herman JG, Merlo A, Mao L, Lapidus RG, Issa JPJ, Davidson NE, Sidran-control causing specific inhibition of cyclin D/CDK4. Nature 1993;366:704- sky D, et al. Inactivation of the CDKN2/p16/MTS1 gene is frequently707. associated with aberrant DNA methylation in all common human cancers.11. Cannon-Albright LA, Goldgar DE, Meyer LJ, Lewis CM, Anderson DE, Cancer Res 1995;55:4525-4530.Fountain JW, Hegi ME, et al. Assignment of a locus for familial melanoma, 27. Serrano M, Lee HW, Chin L, Cordon-Cardo C, Beach D, Depinho RA. RoleMLM, to chromosome 9p13-p22. Science 1992;258:1148-1152.
of the INK4a locus in tumor suppression and cell mortality. Cell 1996;85:12. Hussussian CJ, Struewing JP, Goldstein AM, Higgins PAT, Ally DS, Shea-27-37.han MD, Clark WH, et al. Germline p16 mutations in familial melanoma.
28. Hui AM, Sakamoto M, Kanai Y, Ino Y, Gotoh M, Yokota J, Kirohashi S.Nat Genet 1994;8:15-21.Inactivation of p16INK4 in hepatocellular carcinoma. HEPATOLOGY 1996;13. Spruck CH, Gonzalez-Zulueta M, Shibata A, Simoneau AR, Lin MF, Gon-24:575-579.zales F, Tsai YC, et al. p16 gene in uncultured tumours. Nature 1994;370:
29. Konishi M, Kikuchi-Yanoshita R, Tanaka K, Sato C, Tsuruta K, Maeda183-184.Y, Koike M, et al. Genetic changes and histopathological grades in human14. Caldas C, Hahn SA, da Costa LT, Redston MS, Schutte M, Seymour AB,hepatocellular carcinomas. Jpn J Cancer Res 1993;84:893-899.Weinstein CL, et al. Frequent somatic mutations and homozygous dele-
30. Kitagawa T, Miyasaka K, Kanda H, Yasui H, Hino O. Hepatocarcinogen-tions of the p16(MTS1 ) gene in pancreatic adenocarcinoma. Nat Genetesis in rodents and humans. J Cancer Res Clin Oncol 1995;121:511-515.1994;8:27-32.
31. Guan KL, Jenkins CW, Li Y, Nichols MA, Wu X, O’Keefe CL, Matera15. Mori T, Miura K, Aoki T, Nishihira T, Mori S, Nakamura Y. FrequentAG, et al. Growth suppression by p18, a p16INK4/MTS1- and p14INK4B/somatic mutation of the MTS1/CDK4I (multiple tumor suppressor/cyclin-MTS2-related CDK6 inhibitor, correlates with wild-type pRb function.dependent kinase 4 inhibitor) gene in esophageal squamous cell carcinoma.Genes Dev 1994;8:2939-2952.Cancer Res 1994;54:3396-3397.
32. Puisieux A, Galvin K, Troalen F, Bressac B, Marcais C, Galun E, Ponchel16. Zhou X, Tarmin L, Yin J, Jiang HY, Suzuki H, Rhyu MG, Abraham JM,F, et al. Retinoblastoma and p53 tumor suppressor genes in human hepa-et al. The MTS1 gene is frequently mutated in primary human esophagealtoma cell lines. FASEB J 1993;7:1407-1413.tumors. Oncogene 1994;9:3737-3741.
33. Edmondson HA, Steiner PE. Primary carcinoma of the liver: a study of17. Giani C, Finocchiaro G. Mutation rate of the CDKN2 gene in malignantgliomas. Cancer Res 1994;54:6338-6339. 100 cases among 48900 necropsies. Cancer 1954;7:462-503.
AID Hepa 0027 / 5p21$$$521 05-20-97 20:27:13 hptas WBS: Hepatology