Embed Size (px)
Citation preview

LIVER CANCERSDr. MANISH DUTT

• ANATOMY
• EPIDEMIOLOGY
• ETIOLOGY
• PATHOLOGY
• PROGNOSTIC FACTORS
• WORKUP
• STAGING

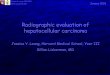
anatomy

Couinaud segments

Clinical significance
Each segment can be resected without damaging those remaining
resections must proceed along the vessels
Dual blood supply:
Portal vein: 3/4
Hepatic artery:1/4
Venous outflow:
Hepatic veins: left, right and middle
Drains into IVC

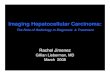
HEPATIC LOBULES


EPIDEMIOLOGY• 782,000 new cases worldwide 2012
• fifth most common cancer in men, 7.5% of the total) and the ninth in women (3.4%)
• high incidence in Eastern and South-Eastern Asia (ASRs 31.9 and 22.2 respectively)
• lowest rates in Northern Europe (4.6) and South-Central Asia (3.70
• second most common cause of death from cancer 746,000 deaths in 2012 (9.1% of the total)
• prognosis very poor (overall ratio of mortality to incidence of 0.95


INDIAN STATS• men 0.9-7.5 per 100,000
• women 0.2 -2.2 per 100,000
• male:female ratio for HCC in India is 4:1
• age of presentation 40 to 70 years
• highest AAIR was reported from Sikkim(7.5)and Mizoram(6.4)
• 4–8% of the cancers were due to HCC
• annual incidence rate of 1.6% (Paul et al) in cirrhotics
• age standardized mortality rate for men is 6.8 ,women 5.1/100,000.
• incidence of HCC in cirrhotics in India is 1.6% per year
• 70–97% of patients with HCC at the time of diagnosis had underlying cirrhosis of liver
• incidence of HCC is increasing in India

ETIOLOGY
• Viral hepatitis- HBV
1. 98 fold greater risk
2. Asymptomatic HbsAg+ - 12 times RR
3. MECHANISM-indirect/direct
4. 70% HBV related HCC- with cirrhosis
5. Risk of HCC in hepB cirrhotic 0.5%
• HCV-
1. Chronic infection(60-80%)
2. 20 fold more and advanced cirrhosis
3. Risk of HCC in hepC cirrhotic 5%
Mi-R-155 accumulation

Etiology contd.• Alcohol- carcinogenic, acetaldehyde, oxidative stress
• NASH(24%)
• METABOLIC DISEASES-haemochromatosis, Wilson, alpha1 AT def.
• Chemical carcinogens- aflatoxin
• Anabolic steroids, estrogens
• Pesticides, insecticides
• Obesity, DM
• Cumulative tobacco use
• Male, old age, specific promotor mutations, higher viremia levels

STAGING

PROGNOSTIC FACTORS
• large size,
• multiple tumors
• vascular invasion
• lymph node spread
• Macroscopic or microscopic vascular invasions
• severity of underlying liver disease- CHILD PUGH, CLIP, V-CLIP, (JIS), BCLC

DIAGNOSTIC W/U
• Labs: CBC, LFTs, chemistries, coagulation panel, serum AFP(10–15% false negative), Hepatitis B/C panels.
• Abdominal CT scan (special contrast protocol).
• FNAC can be performed but is not always needed.

W/U Contd.
Radiological/non invasive
• Lesions>2cm-
• arterial hyperenhancement on two different imaging modalities, or on one imaging modality alongside with a serum AFP of 400 ng/dL
• both arterial hyperenhancement and venous washout in a single imaging modality concomitant with an AFP >200 ng/mL
• sensitivity and specificity of 64.9% and 62.8%
pathological
• Core biopsies- liver/portal vein
• stromal invasion
• sensitivity and specificity of 89.1% and 100%