Embed Size (px)
Citation preview
HEPATOCELLULAR
CARCINOMA
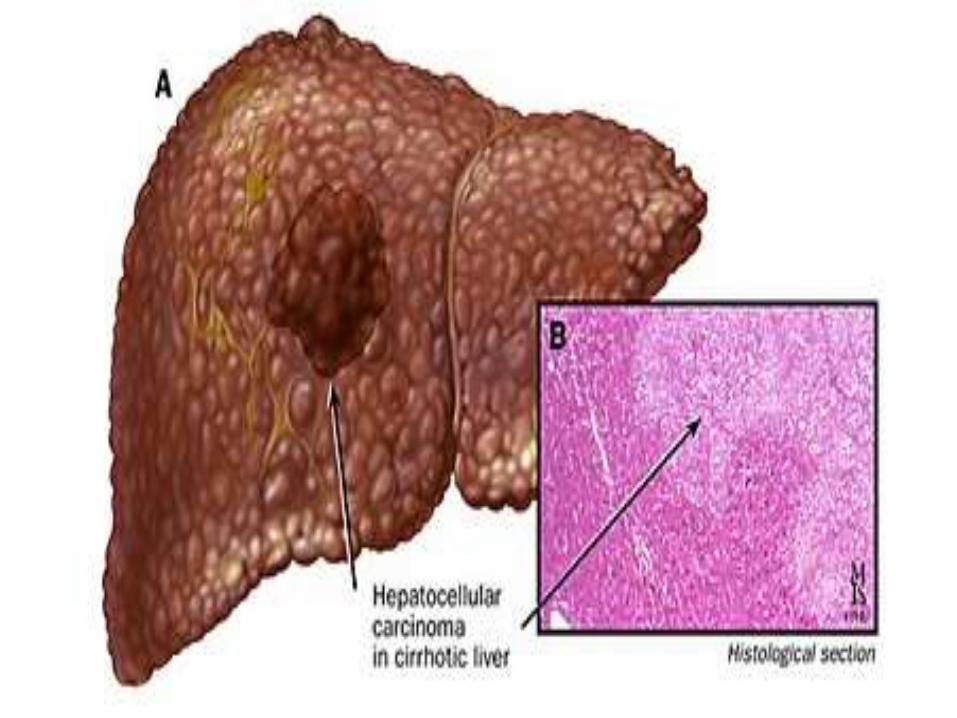
Hepatocellular Carcinoma is a primary cancer
meaning it originated in the Liver(as opposed
to Liver metastases,or secondary Liver Cancers
which have spread to Liver from other organs)
It is commonly associated with Cirrhosis and
Hepatitis.
Male to Female ratio is 4:1 for HCC.
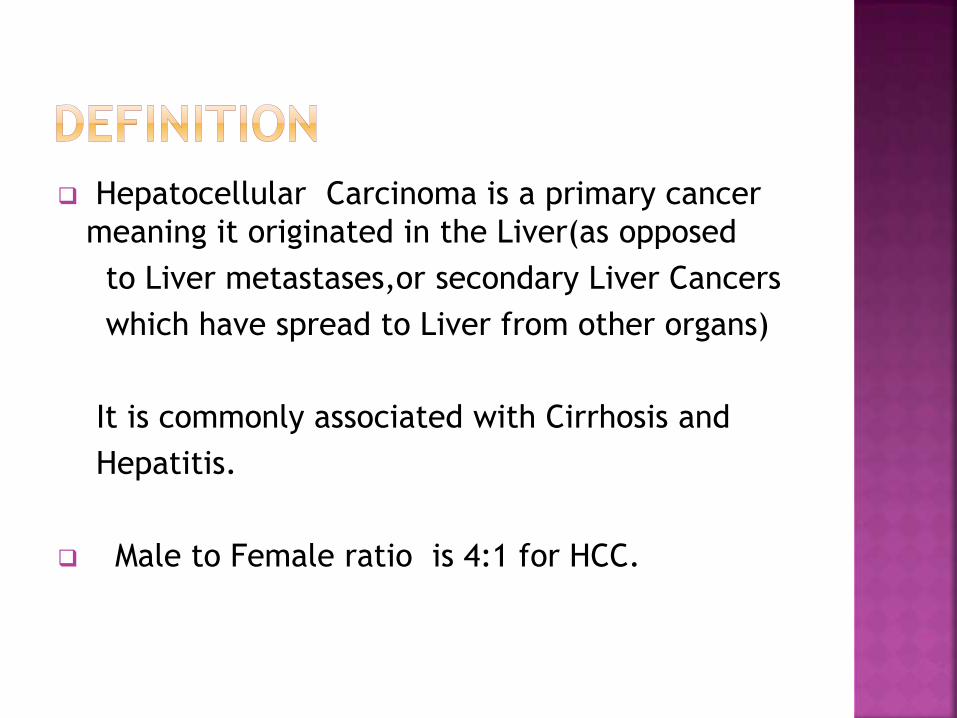
Common Cause:
1.Cirrhosis from any cause
2.Hepatitis B or C chronic infection
3.Ethanol chronic consumption.
4.Aflatoxin B1 or other mycotoxins
Unusual Cause:
1.Primary Biliary Cirrhosis
2.Hemochromatosis
3.Alpha 1 Antitrypsin deficiency
4.Hemochromatosis
5.Wilson’s Disease
Abdominal Pain
Weight Loss
Weakness
Abdominal Fullness and swelling
Jaundice
Nausea
Hepatomegaly (50 to 90% of patients)
Ascites(30 to 60%)
Abdominal Bruits
Splenomegaly
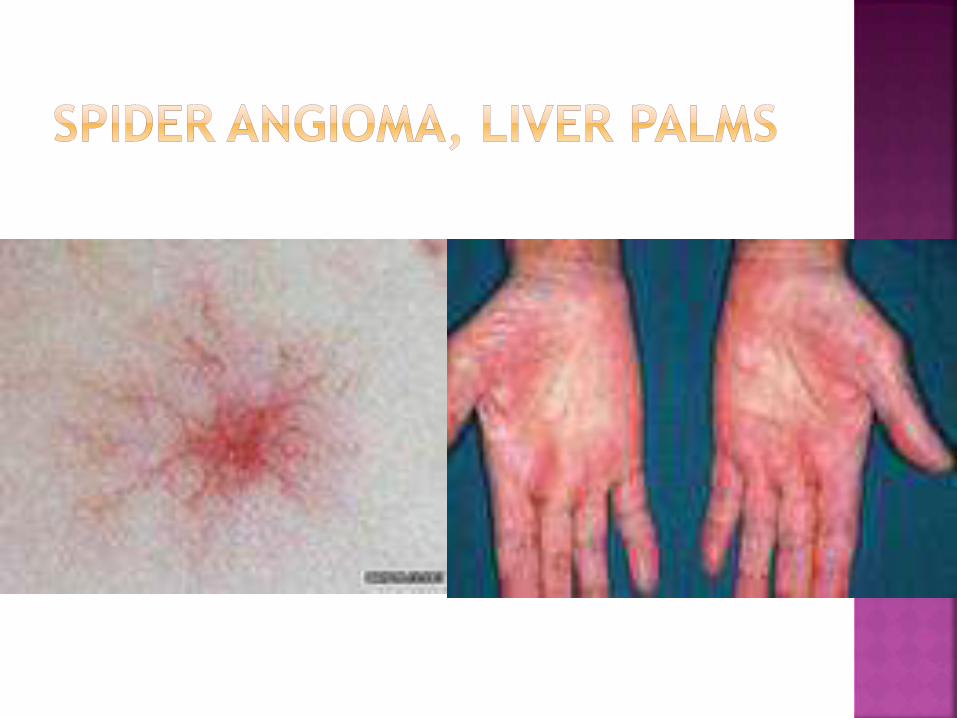
Spider Angioma
Obstructive Jaundice
Paraneoplastic Syndromes
Erythrocytosis
Persistent fever
Hypoglycemia
Hypercalcemia
Hypercholesterolemia
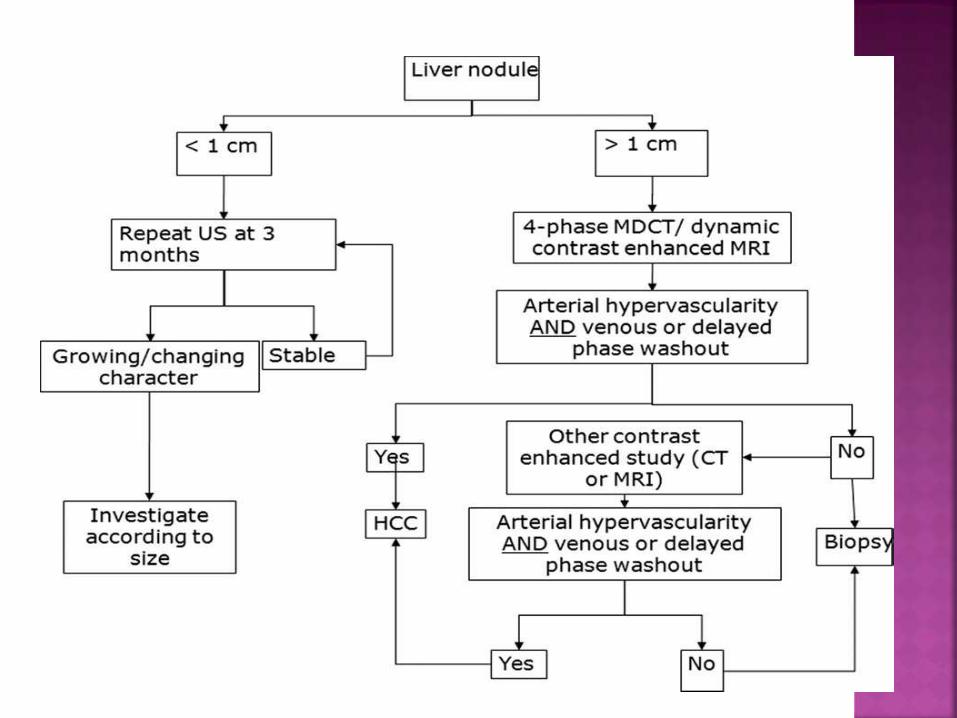
Diagnosis of HCC should be bases on followings:
History & P/E
IMAGING(CT,MRI)
LIVER BIOPSY(For Confirmation)
Elevated Serum AFP(more than 400ng/ml)
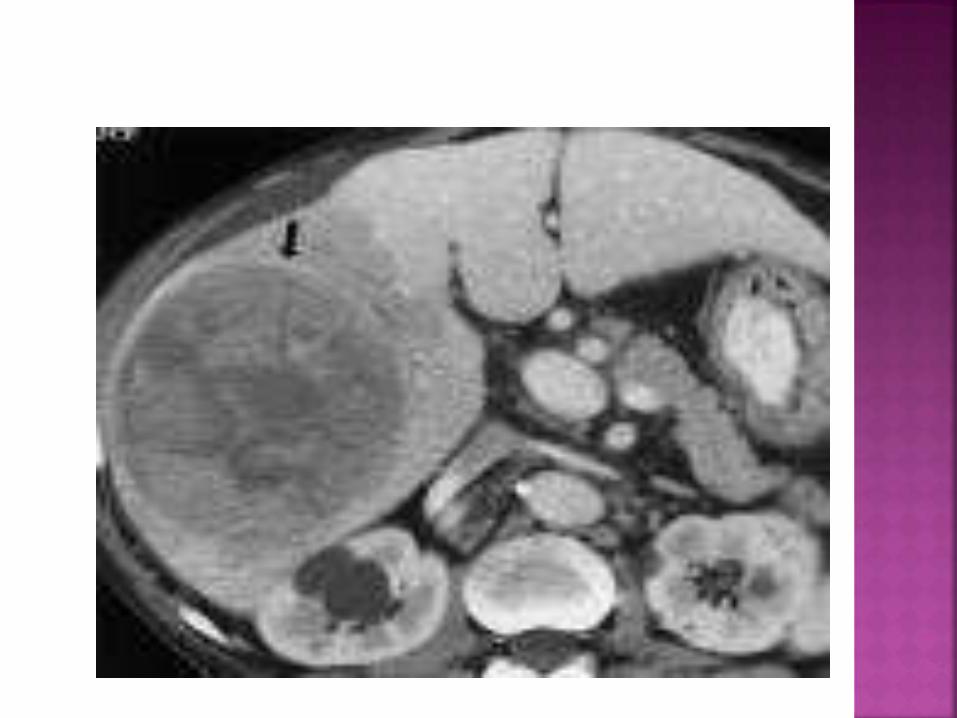
In patient with higher suspicion of HCC the
best method of diagnosis involves:
CT scan of the abdomen using IV Contrast
agent and three phase scanning:
Before contrast administration
Immediately after contrast administration
After Delay
Biopsy is not needed if following criteria are met
on CT:
o Hypervascularity in the arterial phase scans
o Washout or deenhancement in the Portal and
delayed phase studies
o Pseudocapsule and Mosaic Pattern
Liver Biopsy is not needed if these criteria are met
on CT
An alternative to a CT imaging study would be the
MRI. MRI's are more expensive and not as available
because fewer facilities have MRI machines
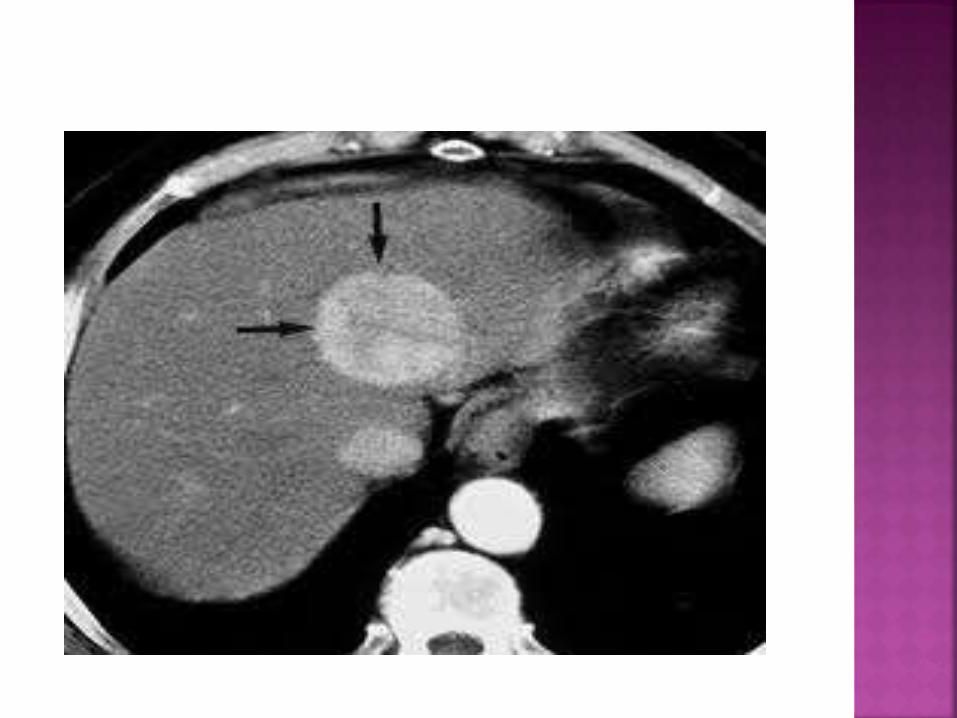
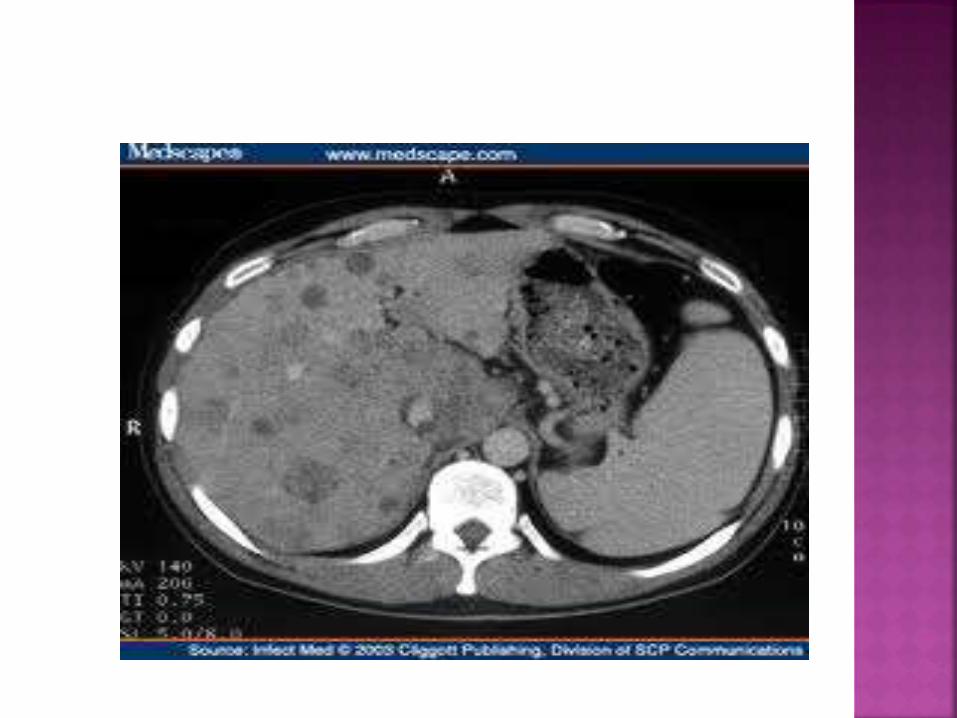
On CT, HCC can have three distinct patterns
of growth:
A single large tumor
Multiple tumors
Poorly defined tumor with an infiltrative
growth pattern

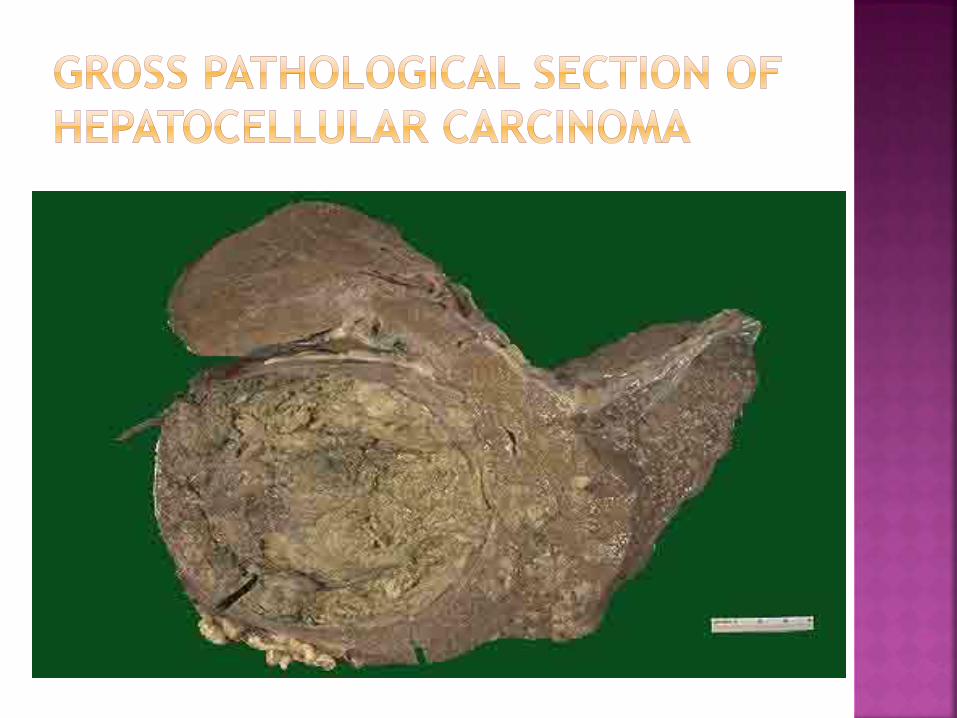
Hepatocellular Carcinoma may appear grossly
as:
1.Unifocal(usually large mass)
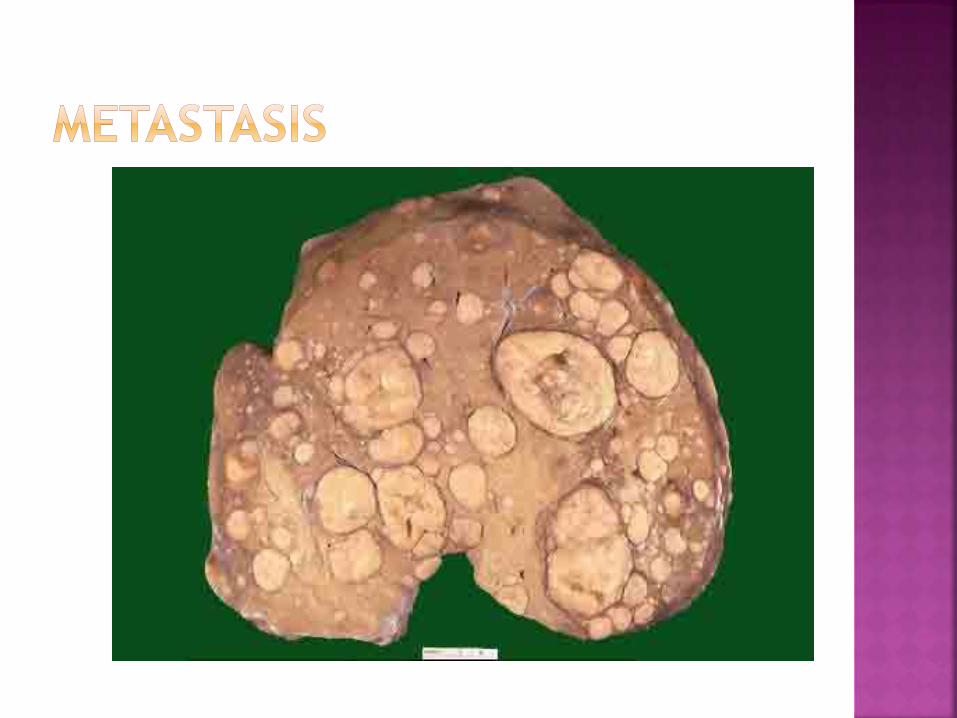
2.Multifocal(widely distributed nodules of
variable size)
3.Diffusely Infiltrative(Cancer,permeating
widely and sometimes involving whole Liver)
Macroscopically,the tumour usually appears as
single mass in the absence of Cirrhosis,or as a
single/ multiple nodules in the presence of cirrho-
-sis
It takes its blood supply from the hepatic artery and
tends to spread by invasion into the portal vein and
its radicles.
Lymph node metastases are common but Lung and
bone metastases are rare.
Microscopically,the tumour resembles hepatocytes
when well differentiated and can be difficult to
distinguish from normal Liver.
The status of the non-tumorous liver:
Underlying cirrhosis.
Non-cirrhotic liver (HBV).
Size and extension of the tumour:
Is it ≤5 cm in size/≤3 lesions ≤ 3 cm ?
Vascular involvement.
General condition of patient, the age and
expected life expectancy.
24
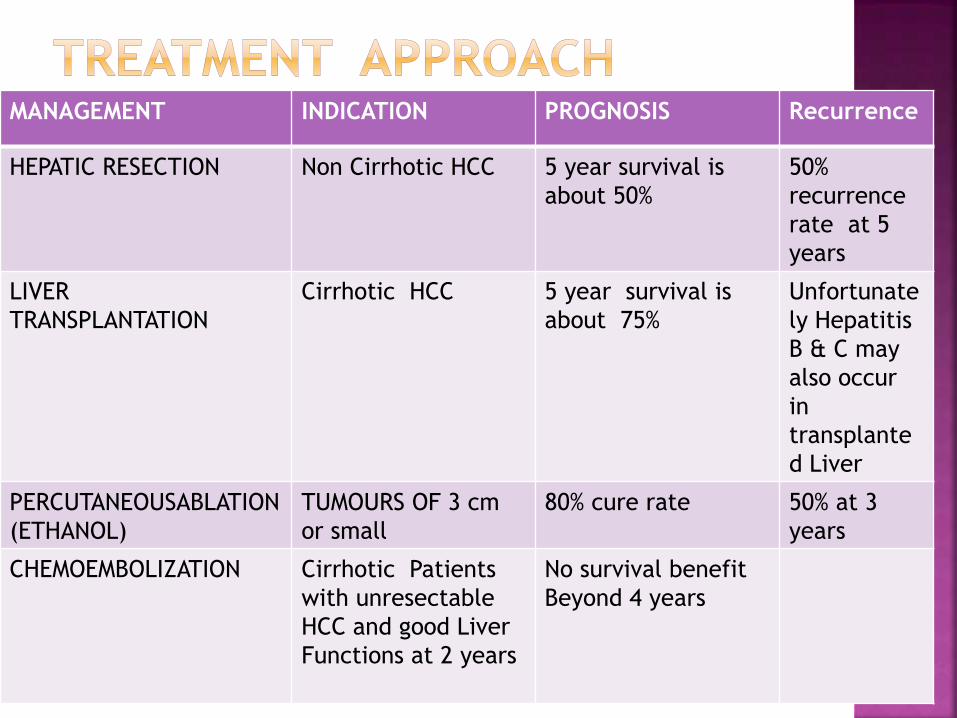
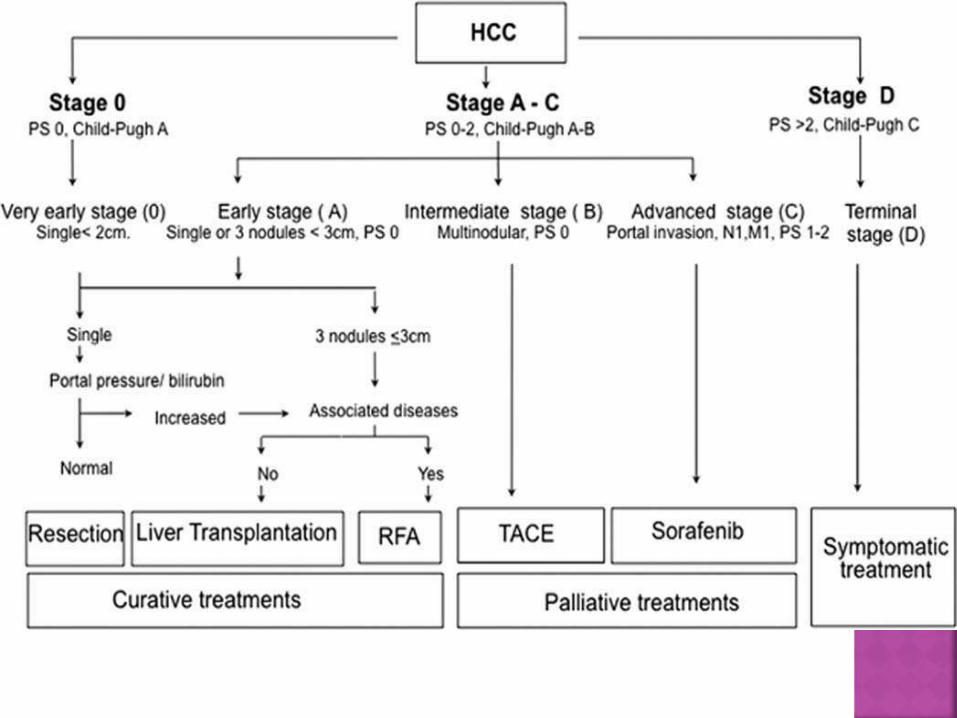
MANAGEMENT INDICATION PROGNOSIS Recurrence
HEPATIC RESECTION Non Cirrhotic HCC 5 year survival is
about 50%
50%
recurrence
rate at 5
years
LIVER
TRANSPLANTATION
Cirrhotic HCC 5 year survival is
about 75%
Unfortunate
ly Hepatitis
B & C may
also occur
in
transplante
d Liver
PERCUTANEOUSABLATION
(ETHANOL)
TUMOURS OF 3 cm
or small
80% cure rate 50% at 3
years
CHEMOEMBOLIZATION Cirrhotic Patients
with unresectable
HCC and good Liver
Functions at 2 years
No survival benefit
Beyond 4 years
This Scoring system is used to assess the
prognosis of Chronic Liver Disease,mainly
Cirrhosis.
It is now used to determine the prognosis
as well as required strength of treatment
and the neccesity of Liver transplantation.
Scoring is done by following methods:
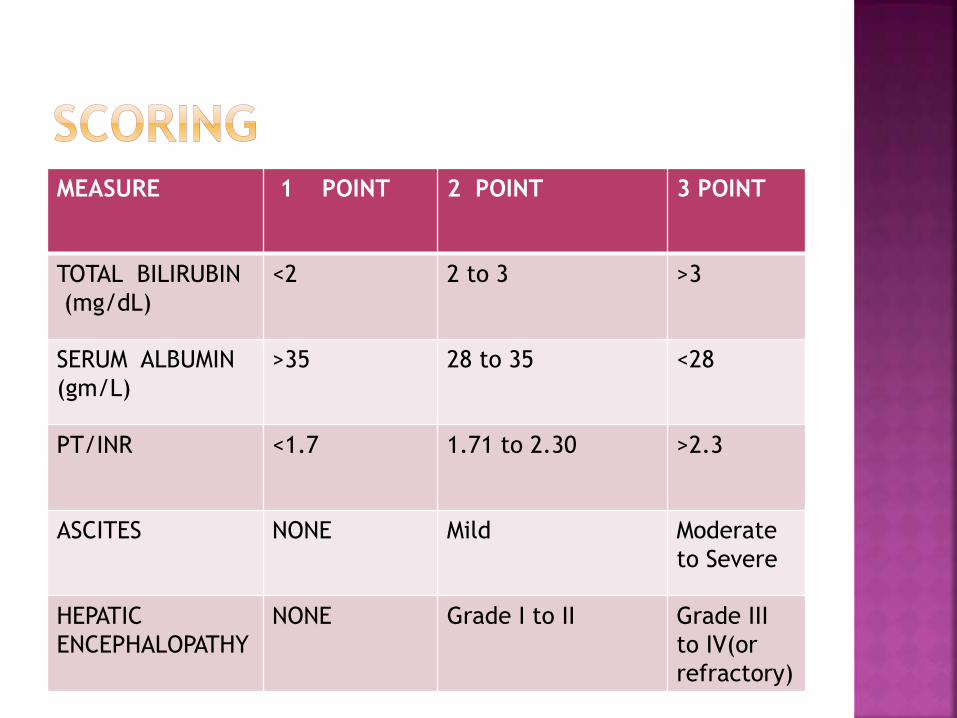
MEASURE 1 POINT 2 POINT 3 POINT
TOTAL BILIRUBIN
(mg/dL)
<2 2 to 3 >3
SERUM ALBUMIN
(gm/L)
>35 28 to 35 <28
PT/INR <1.7 1.71 to 2.30 >2.3
ASCITES NONE Mild Moderate
to Severe
HEPATIC
ENCEPHALOPATHY
NONE Grade I to II Grade III
to IV(or
refractory)
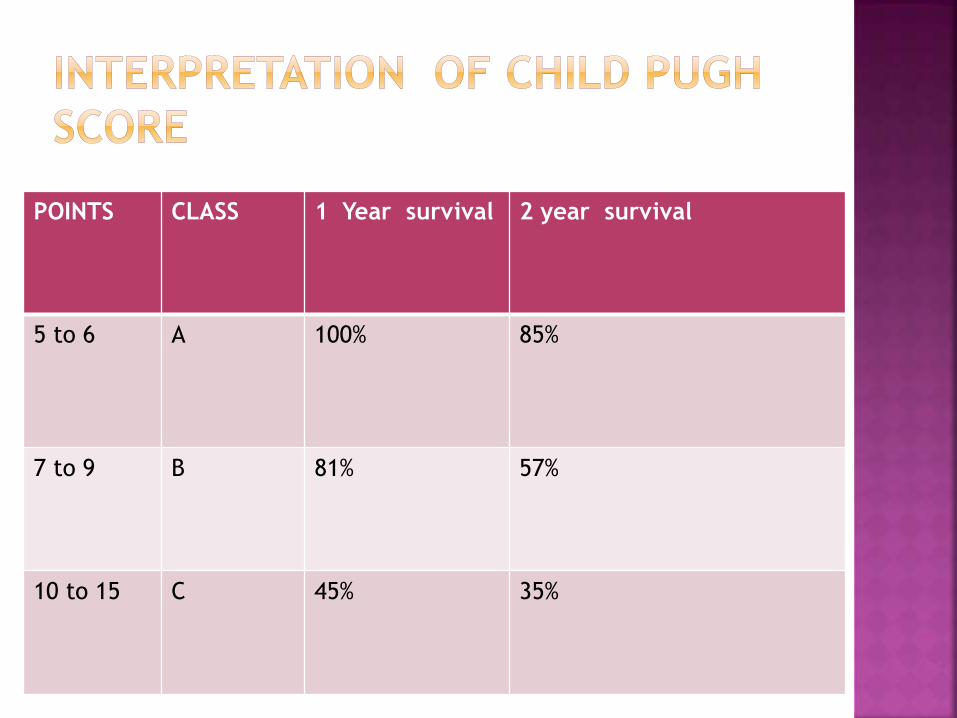
POINTS CLASS 1 Year survival 2 year survival
5 to 6 A 100% 85%
7 to 9 B 81% 57%
10 to 15 C 45% 35%
SORAFENIB(multitargeted oral tyrosine
kinase inhibitor)
SUNITINIB,DOXORUBICIN,CISPLATIN,FLURO-
-URACIL are commonly used
chemotherapeutic
agents.
Unfortunately HCC is relatively
chemotherapy resistant
BCLC Classification
TNM Classification
OKUDA Classification
CLIP Score for HCC
ECOG performance scale
Gastrointestinal Bleeding
Liver Failure
Distant Metastases
www.cancer.net
www.cancer.org
www.aapf.org
www.esmo.org
www.mayoclinic.com
DAVIDSON:Internal Medicine
ROBBINS:Pathology

THANK YOU