Embed Size (px)
Citation preview

Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.
Genetic Determinants of Hearing Loss AssociatedWith Vestibular Schwannomas
*†Konstantina M. Stankovic, ‡Maciej M. Mrugala, §Robert L. Martuza,kMichael Silver, kRebecca A. Betensky, *†Joseph B. Nadol, Jr.,
and ¶Anat O. Stemmer-Rachamimov
*Department of Otolaryngology and Eaton Peabody Laboratory, Massachusetts Eye and Ear Infirmary,ÞDepartment of Otology and Laryngology, þDepartment of Neurology, Harvard Medical School,
§Neurosurgical Service, kBiostatistics Center, and ¶Department of Pathology, Massachusetts GeneralHospital, Boston, Massachusetts, U.S.A.
Hypothesis: The severity of hearing loss (HL) associated withvestibular schwannomas (VSs) is influenced by genes ex-pressed by the VSs.Background: Hearing loss is the most common presentingsymptoms in patients with VSs, yet its pathophysiologyremains elusive. Previous studies have suggested that VSscause HL not only by inducing degeneration of the auditorynerve by compression but also by promoting degeneration ofthe inner ear. This study aimed to determine whether there is amolecular basis for differences in HL associated with VSs.Methods: Surgical specimens of VSs were collected from13 patients and were divided into a group associated withgood (word recognition 970% and pure-tone average e30 dB)or poor hearing. Whole-genome expression profiling of VSswas performed with the Affymetrix GeneChip Human X3PArray. The expression of select genes was validated usingreal-time quantitative reverse transcriptionYpolymerase chainreaction and immunohistochemistry. Because of a small samplesize, exact nonparametric tests were used to assess the associa-
tion between good versus poor hearing and specific histologicalfeatures of the tumors and patient demographics.Results: Using gene set enrichment analysis, the chromosomalregion 3q27 was found to be significantly different between the2 groups of tumors. This region includes peroxisomal biogen-esis factor 5Ylike gene, which was underexpressed in VSs withpoor hearing. The expression of 3 other genes from differentchromosomes was significantly different between the 2 groups:RAD54B, prostate-specific membrane antigenYlike, and carci-noembryonic antigen.Conclusion: This study identified several molecular alterationsin VSs stratified by hearing. These alterations may determinethe severity of HL associated with VSs and may representpotential therapeutic targets to prevent or reduce HL in thesespatients. Key Words: Carcinoembryonic antigenVHearinglossVPeroxisomal biogenesis factor 5YlikeVPlatelet factor4VProstate-specific membrane antigenYlikeVRAD54BVVes-tibular schwannoma.Otol Neurotol 30:661Y667, 2009.
Vestibular schwannomas (VSs), also known as acous-tic neuromas, typically arise from Schwann cell of thevestibular nerves, yet most commonly cause hearing loss(HL) rather than vestibular dysfunction. The pathophy-siology of the progressive sensorineural HL associatedwith VSs is uncertain and current treatment is inade-quate. Yet, HL markedly decreases the quality of lifeand social functioning of affected patients. Understand-
ing the elusive pathophysiology of the HL associatedwith VSs was the main objective of this study.
Previous studies have suggested that VSs cause HLnot only by inducing degeneration of the auditorynerve (1,2) but also by promoting degeneration of theinner ear (3,4), possibly by secreting a toxic substanceor substances. An alternative explanation is that VSsinduce a change in the microenvironment, resulting ina deficiency in a factor that is important for normalnerve or receptor function. In an attempt to explorethese hypotheses and identify genetic determinants ofHL associated with VSs, we have undertaken whole-genome expression profiling of VSs stratified by hear-ing. Although high-throughput microarray technologyhas been used to study VSs tumorigenesis (5,6), this
Address correspondence and reprint requests to Konstantina M.Stankovic, M.D., Ph.D., Department of Otolaryngology, MassachusettsEye and Ear Infirmary, 243 Charles Street, Boston, MA 02114; E-mail:[email protected] work has been supported by the Foundation of the Massachu-
setts Eye and Ear Infirmary (J.B.N.) and by the Children’s TumorFoundation (A.O.S.-R.).
Otology & Neurotology30:661Y667 � 2009, Otology & Neurotology, Inc.
661

Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.
is the first study that uses this technology to elucidatemechanisms of HL associated with VSs.
MATERIALS AND METHODS
Study Population and Tissue CollectionSurgical specimens of VSs from 13 adult, nonsmoking
patients who underwent surgical resection at the MassachusettsGeneral Hospital were received from the hospital’s neuro-oncology tumor bank. The specimens were handled accordingto the institutional review board’s study protocol approved bythe Human Studies Committee of the Massachusetts GeneralHospital (Protocol No. 2004-P-2297/2, PI: A.O.S.-R.) and theMassachusetts Eye and Ear Infirmary (Protocol No. 05-02-009X, PI: J.B.N.). The tumors were divided into a group withgood hearing (word recognition 970% and pure-tone average(PTA) e30 dB) or poor hearing. All patients had good hearingin the contralateral ear to reduce the likelihood of an underlyingdegenerative or systemic disease that may contribute to HL.Patient demographics are summarized in Table 1. Immediatelyupon harvest, the specimens were stored at j80-C until thetime of ribonucleic acid (RNA) extraction. Whole-genomeexpression profiling of VSs was performed with the GeneChipHuman X3P Array (Affymetrix, Santa Clara, CA, USA). Thesame set of tumors was used to corroborate the results with real-time quantitative reverse transcriptionYpolymerase chain reac-tion (RT-qPCR) and with immunohistochemistry.
RNA ExtractionTotal RNA was purified using RNeasy spin columns (Qiagen,
Valencia, CA, USA) according to the manufacturer’s protocol.Quantification and quality assessment of the RNA were per-formed using Agilent 2100 Bioanalyzer and RNA Pico Kit (Agi-lent Technologies, Santa Clara, CA, USA). All samples yieldedclean and undegraded RNA based on the appearance of electro-pherograms and RNA integrity numbers greater than 7. TheRNA was reverse-transcribed with Taqman Reverse Transcrip-tion Reagents kit (Applied Biosystems, Foster City, CA, USA),twice amplified, labeled (Life Sciences, Inc., Farmingdale, NY,USA) and submitted to the Massachusetts General Hospitalmicroarray core facility (Charlestown, MA, USA).
Microarray Processing and AnalysisComplementary deoxyribonucleic acid (DNA) was trans-
formed into messenger ribonucleic acid (mRNA) and biotinlabeled with the BioArray High Yield RNA Transcript LabelingKit (Affymetrix). The hybridization of the fragmented biotin-labeled mRNA to the Human X3P GeneChip (Affymetrix),which screens 47,000 transcripts with 61,000 probe sets, andscanning of the chip was performed according to the manufac-turer’s protocol in the microarray core facility. Microarray datawere analyzed using GenePattern 3.0 platform (Broad Institute,Cambridge, MA, USA) (7) as previously described (8). Classneighbors analysis (9) and comparative marker selection (10)were used to determine which genes best characterize a patientgroup whereas knowing a priori whether a sample belonged to agood or a poor hearing group. Genes were ranked using the ttest statistic. The false discovery rate (FDR) statistic was set toless than 10% to adjust for multiple hypothesis testing whereasestimating probabilities that differences in gene expressionrepresent false-positive findings.Gene set enrichment analysis (GSEA) (11) was used to deter-
mine subtle but coordinated differences in expression of pre-viously defined sets of genes. The analyzed gene sets includedthe cytogenetic set that contains 386 gene sets corresponding tocytogenetic bands, the functional set that contains 1687 genesets involved in specific metabolic and signaling pathways, theneighborhood set that contains 427 gene sets defined by expres-sion neighborhood centered on cancer-related genes, and a reg-ulatory motif set that contains 837 gene sets with commonlyconserved regulatory motifs in the promoter regions. Correctionfor multiple hypotheses testing and gene set size was automa-tically implemented using sample permutations. Gene sets thatcontained fewer than 25 genes and more than 500 genes wereignored, which is appropriate for data sets with more than10,000 features (11). We focused on gene sets with an FDRof less than 10% because they are most likely to generate inter-esting hypotheses and drive further research.
Real-Time RT-qPCRReal-time RT-qPCR was used to validate the expression of
7 genes selected from microarray analyses. Real-time RT-qPCRwas carried on all but 1 sample of RNA used for microarrayanalyses (Sample No. 3769; Table 1) because there was notenough RNA to perform the analysis from that sample. Forthe selected genes, 6-FAM linked fluorescent probes and pri-mers were designed and optimized by Applied Biosystems. Themeasurements were performed on an Applied Biosystems 7700Sequence Detection System using 96-well plates and conditionsas previously described (8). Statistical significance of the mea-surements was determined using the bootstrap resamplingmethod (12) with the threshold set to p G 0.05.
ImmunohistochemistryImmunohistochemistry was performed on 8-Km sections of
formalin-fixed, paraffin-embedded representative samples fromthe same frozen tumors used for the microarray analyses. Sec-tions were immunostained using primary monoclonal antibodyagainst neurofilament (Nf, Catalog No. M0762, clone 2F11;DAKO, Fort Collins, CO, USA), polyclonal antibody againstRad45B (Catalog No. LS-C9872/L7101868; Lifespan Bios-ciences, Seattle, WA, USA), polyclonal antibody againstplatelet factor 4 (Pf4, Catalog No. 500-P05; PeproTech, Inc.,Rocky Hill, NJ, USA), and polyclonal antibody against carci-noembryonic antigen (CEA, Catalog No. 7602507; VentanaMedical, Tucson, AZ, USA). Antigen retrieval techniques
TABLE 1. Patient demographics
PatientID Sex
Age(yr)
CPAdiameterof VSs(mm)
PTA(dB)
Worddiscrimination
(%)
PTA (dB)/Worddiscrimination
(%) incontralateral ear
3405 M 48 G5 30 64 5/1003356 M 42 20 45 40 15/1003286 M 61 20 60 24 20/903175 M 43 30 45 32 5/1003144 F 32 29 15 100 2/1003088 M 32 55 30 96 2/1003827 F 37 25 22 94 10/963277 F 43 28 2 100 0/1003200 F 14 20 12 92 0/1003383 F 32 20 20 98 7/1003683 M 50 30 30 96 15/1003722 M 56 15 30 78 22/903769 M 49 27 30 84 5/100
Samples highlighted in gray are from the poor hearing group.CPA indicates cerebellopontine angle; F, female; M, male.
662 K. M. STANKOVIC ET AL.
Otology & Neurotology, Vol. 30, No. 5, 2009

Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.
included microwaving with Tris buffer, pH 10 (for Nf ) orsodium citrate, pH 6 (for Rad45B and Pf4) at just subboilingtemperatures for 10 to 15 minutes. Appropriate positive andnegative controls (with the primary antibody omitted) wereprocessed in parallel. Immunohistochemical and histologicalanalyses were performed by a pathologist (A.O.S.-R.) blindedto the phenotypic identity of the tumors.
Statistical AnalysisExact nonparametric tests were used to assess association
between good versus poor hearing and tumor histologic diag-nosis and patient demographics. The two-sided Fisher exact testwas used to assess whether sex, size, histological, and immu-nohistochemical features of the tumors are differently distribu-ted between the 2 hearing groups. The Wilcoxon rank-sum testwas used to assess the relationship between hearing and age.Owing to the small sample size, the formal statistical analysesare exploratory, and we did not apply corrections for multiplecomparisons in the analyses of the clinical data.
RESULTS
In the patients we studied, hearing was independent ofage ( p = 0.27), sex ( p = 0.1), tumor size ( p = 0.56),vessel density ( p = 1.00), and fat content of tumors( p = 1.00). Of 47,000 transcripts assayed with the micro-arrays, 5,767 were at least 2-fold increased and 2,567were at least 2-fold decreased in tumors associatedwith poor hearing. A scatter plot of the fold differencein expression and the associated p values for all tran-scripts is shown in Figure 1. None of the genes met thecriterion for a statistically significant difference inexpression when accounting for multiple comparisonsimplicit in microarray data. Nonetheless, the microarraydata pointed to trends in differential gene expression, asdepicted in the heat map shown in Figure 2.
To determine whether the trends observed in the mi-croarray data are relevant, we verified with RT-qPCR
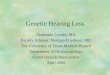
expression of 5 genes with substantial, albeit not sta-tistically significant, difference in expression betweenthe 2 groups. These genes included PF4 whose expres-sion was higher in samples with poor than good hearing,and 4 genes whose expression was lower in samples withpoor hearing: long chain acyl-coA synthetase 2 (LACS2),lysyl oxidase (LOX), RAD54 homolog B (RAD54B), andprostate-specific membrane antigenYlike (PSMAL). Theresults are summarized in Figure 3 and Table 2. Thistable shows that the RT-qPCR data were in overall
FIG. 3. Normalized levels of expression of select genes in VSswith poor hearing expressed relative to VSs with good hearing. Sta-tistically significant differences are marked by an asterisk. For sim-plicity, theexpressionof genes inVSswith poor hearingwas set to 1,although the relative expression of these genes in decreasing abun-dance was PSMAL:LOX:GNB4:RAD54B:PEX5L:LACS2:PF4 =2140:1905:398:104:91:45:1. Error bars indicate SEM. The verticalcoordinate is logarithmic.
FIG. 1. Scatter plot of the abundance ratio of transcripts from VSsassociated with poor versus good hearing and the p value for eachfold ratio. Vertical lines indicate transcripts with 2-fold change inabundance. The horizontal line indicates p value of 0.05.
FIG. 2. Heat map of microarray data based on class neighborsanalysis applied to VSs stratified by hearing. First 9 columns arefrom tumors associated with good hearing and last 4 columns arefrom tumors associated with poor hearing. Red indicates high;blue, low levels of gene expression. Only 20 genes or expressedsequence tags (ESTs) are shown. Horizontal labels indicate Affy-metrix feature and then gene name.
663HEARING LOSS AND VESTIBULAR SCHWANNOMAS
Otology & Neurotology, Vol. 30, No. 5, 2009

Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.
good agreement with the microarray data, although themagnitude of the divergence between the groups differedsomewhat between the 2 techniques. Moreover, by virtueof testing few genes, RT-qPCR was more sensitive thanmicroarrays in detecting statistically significant differ-ences in gene expression from a relatively small numberof samples. Two genes, PSMAL and RAD54B, met thestatistical criterion for decreased expression in tumorsassociated with poor hearing.
In addition to analyzing individual genes, GSEA wasused to test whether sets of related genes were system-atically altered between the 2 groups. A cytogenetic geneset within the chromosomal band 3q27 was found to bemost significantly different (FDR G10%) between the2 groups suggesting that regional effects within thatchromosomal band affect hearing. No gene sets wereenriched within the functional, neighborhood, or regula-tory motif sets. The 3q27 band includes 87 genes, pseu-dogenes, and loci. Within 3q27, we selected genes thathave known roles in hearing or encode secreted proteinsand whose microarray-assayed expression was at lest2.5-fold different between the 2 groups. Two genesmet these criteria, namely, peroxisomal biogenesis factor5Ylike (PEX5L) and guanine nucleotide binding proteinbeta polypeptide 4 (GNB4), and were validated with RT-qPCR. As summarized in Table 2 and Figure 3, theexpression of PEX5L but not GNB4 was significantly dif-
ferent between the 2 groups with PEX5L being 23.4 T 20less expressed in tumors associated with poor hearing.
Immunohistochemistry was used to verify RT-qPCRdata at the protein level, to determine cellular localizationof the gene products of interest, and to test mechanistichypotheses. The results are summarized in Table 3. Ves-tibular schwannomas consist of nonmyelinating tumorcells (13). Using antibodies against neurofilament, weevaluated the hypothesis that higher levels of peroxi-somal gene PEX5L in tumors with good hearing reflectthe presence of functional, myelinated axons withinthese tumors. Although axons could be observed with-in (Bintratumoral distribution[) or at the periphery(Bperipheral distribution[) of some tumors, there wasno correlation between the presence of axons and thepreservation of hearing ( p = 0.56). Peroxisomal disorderscan also be associated with pathologic accumulation offat (14) but we found no correlation between the presenceof fat within the tumors and the severity of HL ( p = 1.00).
Although RT-qPCR did not detect statistically signifi-cant difference in expression of PF4, we pursued thegene product with immunohistochemistry because PF4had a tendency for increased expression in tumors asso-ciated with poor hearing, and it encodes a secreted pro-tein. A majority of the tumors (4/4 in the poor hearingand 7/9 in the good hearing group) were positive for Pf4but there was no correlation between HL and cellulardistribution of Pf4 ( p = 1.00); exclusively perivascularor diffuse pattern was noted in both groups. We alsosemiquantitatively evaluated the number of blood vesselsin tumors because Pf4 is a negative regulator of angio-genesis (15). We found no correlation between vesseldensity in tumors and HL ( p = 1.00). There was a ten-dency for a correlation between vessel density and tumorsize: 3 of 8 large tumors (92.5 cm) and none of the smalltumors had many blood vessels, whereas 4 of 6 smalltumors and only 1 large tumor had rare vessels; thesedifferences were not statistically significant.
Cellular expression of Rad54B, a member of the com-plex involved in the recombinational repair of DNA
TABLE 3. Results of immunohistochemical and histological analyses
Patient ID Nf Fat Pf4 Vessels Rad54B; cytoplasmic Rad54B; nuclear CEA
3405 Intratumoral 0 Perivascular 0 1 0 13356 0 0 Diffuse 0 1 0 33286 Intratumoral and peripheral 1 Perivascular 1 1 1 13175 Peripheral 0 Perivascular 2 0 0 23144 0 0 0 0 1 1 13088 0 1 Diffuse 1 1 1 13827 0 0 Diffuse 2 2 1 13277 0 0 Perivascular 0 1 2 13200 0 0 Perivascular 0 0 2 13383 Intratumoral and peripheral 0 0 0 0 0 13683 Intratumoral and peripheral 0 Diffuse 2 0 0 23722 Peripheral 0 Perivascular 1 0 0 13769 Peripheral 0 Perivascular 1 0 0 1
Immunostaining for Nf, Pf4, and Rad54B and is classified by the site of distribution and the intensity of staining where 0 = no staining, 1 = intensestaining, 2 = very intense staining. An additional category of 3 = extremely intense staining was used for CEA. The category Bfat[ is classified as absent(0) or present (1). The category Bvessels[ indicates whether no (0), some (1), or many (2) vessels were noted. Highlighted samples are from the poorhearing group.
TABLE 2. Fold increase in expression of genes in the poorhearing group compared with the good hearing group as
determined from microarray and RT-qPCR analyses
Gene Microarray RT-qPCR
PF4 40 5.1 T 10.2 ( p = 0.2)GNB4 0.3 1 T 1.5 ( p = 0.9)LACS2 0.06 0.3 T 0.5 ( p = 0.3)RAD54B 0.08 0.2 T 0.1 ( p = 0.001)LOX 0.08 0.08 T 0.1 ( p = 0.07)PSMAL 0.08 0.06 T 0.08 ( p = 0.047)PEX5L 0.3 0.04 T 0.05 ( p = 0.008)
For RT-qPCR, data are expressed as mean T SEM.
664 K. M. STANKOVIC ET AL.
Otology & Neurotology, Vol. 30, No. 5, 2009

Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.
damage, appeared to differ in the 2 groups of tumors.Cytoplasmic staining (without nuclear staining) wasnoted in 2 of 4 tumors associated with poor hearing andin no tumors associated with good hearing. The reversepattern of nuclear staining (but no cytoplasmic staining, orwith nuclear staining more intense than cytoplasmic stain-ing) was observed in 2 tumors associated with good hear-ing but in no tumors associated with poor hearing.However, these differences did not meet statistical criteriafor significance ( p = 0.69 for nuclear Rad54B and p = 0.77for cytoplasmic Rad54B). There was a significant correla-tion between the presence of nuclear Rad54B staining andthe absence of neurofilament staining ( p = 0.04). Bothgroups included tumors with equal or no staining in eitherthe cytoplasm or the nucleus.
The final gene that we studied is CEA-related celladhesion molecule 7 (CEACAM7) because of its higherexpression in tumors associated with poor hearing(Fig. 2). This gene belongs to the family that includesCEA (also known as CEACAM5)Va widely used tumormarker in serum immunoassay determinations of carcino-mas. Immunostaining for CEA corroborated the tran-scriptional data: higher levels of CEA were found intumors associated with poor hearing (Fig. 4). Two of4 tumors with poor hearing and only 1 of 9 tumors withgood hearing expressed CEA abundantly (Fig. 4A). Mostof the tumors associated with good hearing expressedCEA at very low levels (Fig. 4B). These differenceswere not statistically significant ( p = 0.20). Nonetheless,the observed trends cannot be attributed to known benignconditions that can elevate serum CEA levels such assmoking, infections, pancreatitis, or cirrhosis (16) be-cause none of the patients in the study experiencedthese conditions.
DISCUSSION
Although several reports have described the use of ex-pression microarrays to examine VSs (5,6), this study isthe first to screen the entire human genome for alterationsin gene expression that could account for differences inHL associated with VSs. Despite the limited sample size
and significant intersample variability, this study hasidentified several possibly relevant genes by validatingmicroarray data with 2 complementary techniquesVRT-qPCR and immunohistochemistry. Four genes seem to bestrongly associated with HL, namely, PEX5L, RAD54B,PSMAL, and CEA. None of these genes have been pre-viously reported in association with VSs or normal ves-tibulocochlear nerve.
Peroxisome biogenesis factor 5Ylike gene is mostlyexpressed in the brain, and it is thought to regulate per-oxisomal protein import (17). Peroxisomes are ubiqui-tous organelles that participate in the metabolism offatty acids and other metabolites. Although baselineexpression of PEX5L in normal vestibular or cochlearnerve has not been reported, current data suggest thatperoxisomal dysfunction contributes to HL based on dif-ferentially decreased expression of PEX5L in VSs asso-ciated with poor hearing. Peroxisomal dysfunction maymanifest as pathologic accumulation of fat and/or demye-lination and neurodegeneration in the adjacent acousticnerve (14). Neither of these mechanisms could be defini-tively supported by the current data, leaving the possibi-lity that novel pathologic mechanisms are at play or thataltered PEX5L expression in VSs is an epiphenomenon.Future studies in a larger study set may be able to deline-ate these possibilities. Nonetheless, the hypothesis thatperoxisomal dysfunction and demyelination contribute toHL associated with VSs, through as of yet unidentifiedmechanisms, is intriguing for several reasons. First, bothperoxisomal disorders (14) and hereditary myelopathies(18Y20) lead to the type of HL that is characteristic ofVSsVprogressive sensorineural HL with decreased abil-ity to discriminate speech, which is typically signifi-cantly worse than anticipated from the ability to detectpure tones. Second, VSs have been suggested to causedemyelination of the vestibular nerve based on the ana-lysis of hyperventilation-induced nystagmus in patientswith VSs (21). Third, histological analyses of VSs andthe associated nerve have reported demyelinatingchanges in the nerve (22,23).
The 3q27 chromosomal region that includes PEX5Lhas not been previously implicated in tumorigenesis of
FIG. 4. Immunohistochemistry for CEA in a tumor with poor (A; Sample No. 3356) versus good hearing (B; Sample No. 3769). Thereaction product is shown in brown. In (A), there is a large cluster of positive cells, which include macrophages and Schwann cells. In (B),there is a single positive cell (arrow) and a few positive cells inside small blood vessels (not shown).
665HEARING LOSS AND VESTIBULAR SCHWANNOMAS
Otology & Neurotology, Vol. 30, No. 5, 2009

Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.
sporadic VSs (24,25). However, the GSEA from thisstudy suggests that regional alterations within 3q27,including chromosomal deletions or amplifications,dosage compensation, and epigenetic silencing, may con-tribute to the difference in HL associated with VSs.Given that GSEA optimization is sensitive to initializa-tion, future studies with more samples may be able toincrease the accuracy of GSEA.
Another gene found to be expressed at lower levels inVSs associated with poor hearing than good hearing isRAD54B. This gene is part of a complex involved in therecombinational repair of DNA damage. Mutations inRAD54B have been identified in nonYHodgkin lym-phoma and colon cancer (26), whereas RAD51, whichinteracts with RAD54B, has been associated with breasttumorYsusceptibility genes (27). The tendency for prefer-ential cytoplasmic distribution of Rad54B in VSs asso-ciated with good hearing and nuclear distribution in VSsassociated with poor hearing suggests different abilitiesto respond to DNA damage. In other systems, Rad54 hasbeen detected in the cytoplasm (28) and it moves to thenucleus after DNA damage to assist with DNA repair(26). Similarly, Rad51 can be detected in the cytoplasm(29), although it is reported to be a nuclear protein (30).Multiple functions for cytoplasmic Rad51 have been pro-posed: further processing of DNA that underwent repairin the nucleus, termination of recombination repairinitiated in the nucleus, indication of early stages ofcell death, or as yet unidentified function (29). It remainsto be investigated how putative impaired ability to repairDNA damage in VSs associated with poor hearing con-tributes to HL. Furthermore, the absence of any immu-noreactivity in some tumors despite the presence ofRAD54B mRNA suggests impaired translation to a func-tional protein, which may be compensated by upregula-tion of other genes involved in DNA repair.
A final gene expressed at substantially lower levels inVSs associated with poor hearing than good hearing isPSMAL also known as glutamate carboxypeptidase III.Although PSMAL is expressed at high levels in the brain(31), biological significance of PSMAL is not yet known(32). However, PSMAL is 98% homologous to prostate-specific membrane antigen whose inhibition has beenshown to be neuroprotecitive in animal models of stroke,neuropathic pain, and other neurodegeneration (33,34).
In contrast to the 3 genes discussed thus far, CEA-CAM7 gene and CEA protein were expressed at higherlevels in tumors associated with poor hearing. CEA is aglycoprotein whose elevated levels in the serum and cer-ebrospinal fluid (CSF) are frequently associated withepithelial malignancies and metastases to the central ner-vous system (35Y37). In addition, elevated CSF levels ofCEA have been found in primary malignant (36) orbenign (38) lesions of the central nervous system. Inter-estingly, elevated CEA in CSF has been associated withHL (38Y42), and normalization of CEA levels usingintrathecal methotraxate for treatment of leptomenin-geal carcinomatosis leads to improvement in hearing(41). Our findings suggest that CEA may contribute to
HL associated with VSs through as of yet unidentifiedmechanisms.
There may be a link between putative peroxisomaldysfunction and altered CEA levels in VSs associatedwith poor hearing because activation of the nuclear hor-mone peroxisome proliferatorYactivated receptor gammainduces CEA (43). The other 2 genes identified in thisstudy (RAD54B and PSMAL) may play indirect rolesin causing degeneration of the inner ear rather thanby secreting a toxic substance. Such indirect roles in-clude, and are not limited to, decreased production ordecreased responsiveness to putative factors requiredfor normal function of the auditory nerve and the innerear. More data are needed to delineate these mechanisticpossibilities.
Our finding suggesting that tumor size is positivelycorrelated with vessel density is consistent with a pre-vious report that tumor size and clinical growth index areproportional to the total number of vessels (44).
CONCLUSION
Progressive sensorineural HL associated with VSs is amajor clinical problem for which curative therapies arelacking and molecular pathogenesis remains elusive. Theuse of high-throughput microarray technology validatedby RT-qPCR and immunohistochemistry has led to theidentification of 4 genes (PEX5L, RAD54B, PSMAL, andCEA) as possible determinants of HL associated withVSs. These findings need to be verified on large and in-dependent data sets in the future. Nonetheless, the iden-tified genes are potential therapeutic targets to prevent orreduce HL associated with VSs.
REFERENCES
1. Eckermeier L, Pirsig W, Mueller D. Histopathology of 30 non-operated acoustic schwannomas. Arch Otorhinolaryngol 1979;222:1Y9.
2. Kaga K, Iwasaki S, Tamura A, Suzuki J, Haebara H. Temporalbone pathology of acoustic neuroma correlating with presence ofelectrocochleography and absence of auditory brainstem response.J Laryngol Otol 1997;111:967Y72.
3. Nadol JB Jr, Diamond PF, Thornton AR. Correlation of hearingloss and radiologic dimensions of vestibular schwannomas (acous-tic neuromas). Am J Otol 1996;17:312Y6.
4. Mahmud MR, Khan AM, Nadol JB Jr. Histopathology of the innerear in unoperated acoustic neuroma. Ann Otol Rhinol Laryngol2003;112:979Y86.
5. Welling DB, Lasak JM, Akhmametyeva E, Ghaheri B, Chang LS.cDNA microarray analysis of vestibular schwannomas. Otol Neu-rotol 2002;23:736Y48.
6. Lasak JM, Welling DB, Akhmametyeva EM, Salloum M, ChangLS. Retinoblastoma-cyclinYdependent kinase pathway deregulationin vestibular schwannomas. Laryngoscope 2002;112:1555Y61.
7. GenePattern 3.0.Available at: http://www.broad.mit.edu/genepattern/.Accessed December 2007.
8. Stankovic KS, Goldsztein H, Reh DD, Platt MP, Metson R.Gene expression profiling of nasal polyps associated with chronicsinusitis and aspirin-sensitive asthma. Laryngoscope 2008;118:881Y9.
9. Golub TR, Slonim DK, Tamayo P, et al. Molecular classification ofcancer: class discovery and class prediction by gene expressionmonitoring. Science 1999;286:531Y7.
666 K. M. STANKOVIC ET AL.
Otology & Neurotology, Vol. 30, No. 5, 2009

Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.Copyright @ 2009 Otology & Neurotology, Inc. Unauthorized reproduction of this article is prohibited.
10. Gould J, Getz G, Monti S, Reich M, Mesirov JP. Comparative genemarker selection suite. Bioinformatics 2006;22:1924Y5.
11. Subramanian A, Tamayo P, Mootha VK, et al. Gene set enrichmentanalysis: a knowledge-based approach for interpreting genome-wideexpression profiles. Proc Natl Acad Sci U S A 2005;102:15545Y50.
12. Efron B, Tibshirani RJ. An Introduction to the Bootstrap. NewYork, NY: Chapman & Hall, 1993.
13. Hung G, Colton J, Fisher L, et al. Immunohistochemistry study ofhuman vestibular nerve schwannoma differentiation. Glia 2002;38:363Y70.
14. Chedrawi A, Clark G. Peroxisomal disorders. eMedicine. Availableat: http://emedicine.medscape.com/article/1177387-overview.Accessed December 2008.
15. Maurer AM, Zhou B, Han ZC. Roles of platelet factor 4 in hema-topoiesis and angiogenesis. Growth Factors 2006;24:242Y52.
16. Martin EW, Kibbey WE, di Vecchia L, Anderson G, Catalano P,Minton JP. Carcinoembryonic antigen: clinical and histologicalaspects. Cancer 1976;37:62Y81.
17. Amery L, Sano H, Mannaerts GP, et al. Identification of PEX5p-related novel peroxisome-targeting signal 1 (PTS1)-binding pro-teins in mammals. Biochem J 2001;357:635Y46.
18. Starr A, Michalewski HJ, Zeng FG, et al. Pathology and physiol-ogy of auditory neuropathy with a novel mutation in the MPZ gene(Tyr145-9Ser). Brain 2003;126:1604Y19.
19. Kilfoyle DH, Dyck PJ, Wu Y, et al. Myelin protein zero mutationHis39Pro: hereditary motor and sensory neuropathy with variableonset, hearing loss, restless legs and multiple sclerosis. J NeurolNeurosurg Psychiatry 2006;77:963Y6.
20. Ionasescu VV, Searby C, Greenberg SA. DejerineYSottas diseasewith sensorineural hearing loss, nystagmus, and peripheral facialnerve weakness: de novo dominant point mutation of the PMP22gene. J Med Genet 1996;33:1048Y9.
21. Minor LB, Haslwanter T, Straumann D, Zee DS. Hyperventilation-induced nystagmus in patients with vestibular schwannoma. Neu-rology 1999;53:2158Y68.
22. Neely JG, Hough JV. Histologic findings in two very small intra-canalicular solitary schwannomas of the eighth nerve: II. BOnionbulbs.[ Am J Otol 1988;9:216Y21.
23. Kanda T, Komatsuzaki A, Yaku Y. Histological changes of ves-tibular nerves and ganglion cells in the acoustic tumor in relation toclinical functions. Acta Otolaryngol Suppl 1991;481:97Y102.
24. Antinheimo J, Sallinen SL, Sallinen P, et al. Genetic aberrations insporadic and neurofibromatosis 2 (NF2)-associated schwannomasstudied by comparative genomic hybridization (CGH). Acta Neu-rochir (Wien) 2000;142:1099Y104; discussion 1104Y5.
25. Warren C, James LA, Ramsden RT, et al. Identification of recurrentregions of chromosome loss and gain in vestibular schwannomasusing comparative genomic hybridisation. J Med Genet 2003;40:802Y6.
26. Hiramoto T, Nakanishi T, Sumiyoshi T, et al. Mutations of a novelhuman RAD54 homologue, RAD54B, in primary cancer. Oncogene1999;18:3422Y6.
27. Sharan SK, Morimatsu M, Albrecht U, et al. Embryonic lethalityand radiation hypersensitivity mediated by Rad51 in mice lackingBrca2. Nature 1997;386:804Y10.
28. Lopez-Casamichana M, Orozco E, Marchat LA, Lopez-Camarillo
C. Transcriptional profile of the homologous recombinationmachinery and characterization of the EhRAD51 recombinase inresponse to DNA damage in Entamoeba histolytica. BMC Mol Biol2008;9:35.
29. Christodoulopoulos G, Malapetsa A, Schipper H, Golub, et al.Chlorambucil induction of HsRad51 in B-cell chronic lymphocyticleukemia. Clin Cancer Res 1999;5:2178Y84.
30. Solinger JA, Kiianitsa K, Heyer WD. Rad54, a Swi2/Snf2Ylikerecombinational repair protein, disassembles Rad51:dsDNA fila-ments. Mol Cell 2000;10:1175Y88.
31. O’Keefe DS, Bacich DJ, Heston WD. Comparative analysisof prostate-specific membrane antigen (PSMA) versus a prostate-specific membrane antigen-like gene. Prostate 2004;58:200Y10.
32. Hlouchova K, Barinka C, Klusak V, et al. Biochemical character-ization of human glutamate carboxypeptidase III. J Neurochem2007;101:682Y96.
33. Slusher BS, Vornov JJ, Thomas AG, et al. Selective inhibition ofNAALADase, which converts NAAG to glutamate, reducesischemic brain injury. Nat Med 1999;5:1396Y402.
34. Ghadge GD, Slusher BS, Bodner A, et al. Glutamate carboxypep-tidase II inhibition protects motor neurons from death in familialamyotrophic lateral sclerosis models. Proc Natl Acad Sci U S A2003;100:9554Y9.
35. Twijnstra A, Nooyen WJ, van Zanten AP, et al. Cerebrospinal fluidcarcinoembryonic antigen in patients with metastatic and nonmeta-static neurological diseases. Arch Neurol 1986;43:269Y72.
36. Jacobi C, Reiber H, Felgenhauer K. The clinical relevance oflocally produced carcinoembryonic antigen in cerebrospinal fluid.J Neurol 1986;233:358Y61.
37. Flaschka G, Desoye G. CEA plasma levels in patients with intra-cranial tumours. Neurochirurgia (Stuttg) 1987;30:5Y7.
38. Louis DN, Hamilton AJ, Sobel RA, Ojemann RG. Pseudopsammo-matous meningioma with elevated serum carcinoembryonic anti-gen: a true secretory meningioma. Case report. J Neurosurg 1991;74:129Y32.
39. Mochizuki H, Satoh S, Saikawa M, et al. A 74-year-old man withurinary incontinence, right leg weakness and multiple cranial nervepalsies. No To Shinkei 1995;47:199Y209.
40. Kan S, Ikeda T. Gd-DTPA enhancement of cranial nerves on MRimaging. Neoplastic lesions. Acta Neurol Scand 1999;100:400Y6.
41. Miura M, Iijima N, Hayashida K, et al. Case of leptomeningealcarcinomatosis effectively treated with intrathecal chemotherapyusing ventriculoperitoneal shunt. Rinsho Shinkeigaku 2006;46:404Y9.
42. Shen Y, Blumenthal DT, Digre K, Cessna MH, Gopez EV. Carci-nomatous meningitis as the presenting manifestation of gallbladdercarcinoma: case report and review of the literature. J Neurooncol2004;70:67Y71.
43. Gupta RA, Brockman JA, Sarraf P, Willson TM, DuBois RN.Target genes of peroxisome proliferator-activated receptorgamma in colorectal cancer cells. J Biol Chem 2001;276:29681Y7.
44. Labit-Bouvier C, Crebassa B, Bouvier C, et al. Clinicopathologicgrowth factors in vestibular schwannomas: a morphological andimmunohistochemical study of 69 tumours. Acta Otolaryngol2000;120:950Y4.
667HEARING LOSS AND VESTIBULAR SCHWANNOMAS
Otology & Neurotology, Vol. 30, No. 5, 2009