Embed Size (px)
Citation preview

ARTICLE OPEN ACCESS
Genetic determinants of disease severity in themyotonic dystrophy type 1 OPTIMISTIC cohortSarah A Cumming PhD Cecilia Jimenez-Moreno PhD Kees Okkersen MD Stephan Wenninger MD
Ferroudja Daidj MD Fiona Hogarth PhD Roberta Littleford PhD Grainne Gorman MD
Guillaume Bassez MD Benedikt Schoser MD Hanns Lochmuller MD Baziel GM van Engelen MD PhD and
Darren G Monckton PhD on behalf of the OPTIMISTIC Consortium
Neurologyreg 201993e1-e15 doi101212WNL0000000000008056
Correspondence
Dr Monckton
darrenmonckton
glasgowacuk
AbstractObjectiveTo evaluate the role of genetic variation at the DMPK locus on symptomatic diversity in 250adult ambulant patients with myotonic dystrophy type 1 (DM1) recruited to the ObservationalProlonged Trial in Myotonic Dystrophy Type 1 to Improve Quality of LifemdashStandardsa Target Identification Collaboration (OPTIMISTIC) clinical trial
MethodsWe used small pool PCR to correct age at sampling biases and estimate the progenitor alleleCTG repeat length and somatic mutational dynamics and AciI digests and repeat primed PCRto test for the presence of variant repeats
ResultsWe confirmed disease severity is driven by progenitor allele length is further modified by ageand in some cases sex and that patients in whom the CTG repeat expands more rapidly in thesoma develop symptoms earlier than predicted We revealed a key role for variant repeats inreducing disease severity and quantified their role in delaying age at onset by approximately132 years (95 confidence interval 57ndash207 2-tailed t test t = minus37 p = 00019)
ConclusionsCareful characterization of the DMPK CTG repeat to define progenitor allele length andpresence of variant repeats has increased utility in understanding clinical variability in a trialcohort and provides a genetic route for defining disease-specific outcome measures and thebasis of treatment response and stratification in DM1 trials
From the Institute of Molecular Cell and Systems Biology (SAC DGM) University of Glasgow Institute of Genetic Medicine (CJ-M HL) and Institute of Neurosciences (GG)Newcastle University Newcastle upon Tyne UK Department of Neurology (KO BGMvE) Donders Institute for Brain Cognition and Behaviour Radboud University MedicalCentre Nijmegen the Netherlands Department of Neurology (SW BS) Friedrich-Baur-Institute Ludwig-Maximilians-Universitat Munchen Munich Germany NeuromuscularReference Centre (FD GB) Assistance Publique-Hopitaux de Paris France and Tayside Clinical Trials Unit (FH RL) The University of Dundee UK
Go to NeurologyorgN for full disclosures Funding information and disclosures deemed relevant by the authors if any are provided at the end of the article
OPTIMISTIC Consortium coinvestigators are listed at linkslwwcomWNLA962
The Article Processing Charge was funded by Wellcome Trust
This is an open access article distributed under the Creative Commons Attribution License 40 (CCBY) which permits unrestricted use distribution and reproduction in any mediumprovided the original work is properly cited
Copyright copy 2019 The Author(s) Published by Wolters Kluwer Health Inc on behalf of the American Academy of Neurology e1
Published Ahead of Print on August 8 2019 as 101212WNL0000000000008056
Myotonic dystrophy type 1 (DM1) is a highly variableautosomal dominant inherited disorder affecting individu-als of both sexes and all ages1 DM1 is caused by the ex-pansion of a CTG repeat in the DMPK gene that varies inlength from under 40 repeats in the general population tomore than 1000 repeats in some patients2ndash7 Longer CTGtracts are associated with more severe disease and earlierage at onset8ndash11 However genotype to phenotype rela-tionships determined using the traditional diagnostic testhave low predictive value and the International MyotonicDystrophy Consortium recommends that families are notoffered predictive phenotypic information based on the sizeof the CTG repeat12
Expanded disease-causing alleles are highly unstable andusually increase in length during intergenerationaltransmission813ndash15 explaining the decrease in age at onsetof 20ndash30 years per generation typically observed in DM1families16 The expanded CTG is also highly unstable in thesoma in a process that is expansion-biased age-dependentand tissue-specific17ndash24 Thus the average length of theCTG repeat measured using the traditional diagnosticdepends on the age at which the sample was taken Pre-viously we demonstrated that a sensitive small pool PCR(SP-PCR) analysis of blood DNA could be used to estimatethe progenitor allele length (ePAL) ie the length of theCTG repeat transmitted to the individual by the affectedparent18 In addition we demonstrated that ePAL couldreduce the confounding effects of age at sampling inherentin the traditional test and we could dramatically improve theability to predict age at onset in DM12526
Observational Prolonged Trial in Myotonic Dystrophy Type1 to Improve Quality of LifemdashStandards a Target Identifi-cation Collaboration (OPTIMISTIC) was a large in-ternational multicenter model-based randomized trialdesigned to compare the utility of tailored cognitive be-havioral therapy (CBT) with an optional graded exerciseplan against standard care2728 In order to provide additionalinsight into the genetic basis of variability in DM1 and asa route toward genetic stratification in clinical trials wesought to estimate the progenitor allele length and define therepeat dynamics of the DM1 CTG repeat in the blood DNAof participants recruited to OPTIMISTIC
MethodsStandard protocol approvals registrationsand patient consentsFull details of the OPTIMISTIC protocol including powercalculations for sample size have been reported previously(Clinicaltrialsgov NCT02118779)27 All participants wererecruited with informed consent The protocol was approvedby the National Research Ethics Service Committee NorthEastmdashSunderland (UK) the Comite de Protection des Per-sonnes ile de France V (France) the Ethikkommission bei derLMUMunchen (Germany) and the Concernstaf Kwaliteit enVeiligheid Commissie Mensgebonden Onderzoek RegioArnhem-Nijmegen (Netherlands)
Phenotypic dataAmbulant adult patients (gt18 years of age) with geneticallyproven DM1 capable of providing informed consent withsevere fatigue (Checklist Individual StrengthndashFatigue [CIS-Fatigue] score ge35) were recruited between April 2014 andMay 2015 through 4 clinical centers Nijmegen the Nether-lands Paris France Munich Germany and NewcastleUnited Kingdom (n = 255 [463 female] [118255])2728
Exclusion criteria included neurologic or orthopedic comor-bidity possibly influencing the intervention or outcomes useof psychotropic drugs (except modafinil Ritalin and anti-depressants where the dosing regimen was stable for at least12 months prior to screening) severe depression participa-tion in another interventional clinical trial or inability tocomplete study questionnaires Age at onset of DM1 symp-toms was obtained during the trial recruitment screening visitin answer to the question ldquoAt what age did the first medicalproblems occur that may be related to your myotonic dys-trophyrdquo With the exception of patients recruited throughMunich age at sampling was calculated based on known dateof birth and the date of visit 2 at which the blood sample wasprovided As a local regulatory requirement date of birth wasnot recorded for participants recruited in Munich thereforethe age at sampling used was self-reported by participants atvisit 2 Additional baseline (visit 2) clinical measures wereobtained as described in the OPTIMISTIC protocol andreported previously2728 The majority of participants (n =225) were not known to be related Eight parentndashoffspringpairs 4 sibling pairs and 3 trios of 2 siblings and 1 offspringwere also recruited
Glossary6-MWT = 6-Minute Walk Test ASBQ = Adult Social Behavior Questionnaire BDI-fs = Beck Depression Inventorymdashfastscreen CBT = cognitive behavioral therapy CI = confidence interval CIS-fatigue = Checklist Individual Strength FatiguescoreDM1 = myotonic dystrophy type 1 ePAL = estimated progenitor allele length FDSS = Fatigue and Daytime SleepinessScaleMIRS =Muscle Impairment Rating ScaleOPTIMISTIC =Observational Prolonged Trial in Myotonic Dystrophy Type1 to Improve Quality of LifemdashStandards a Target Identification Collaboration RP-PCR = repeat-primed PCR SP-PCR =small pool PCR SSL = van Sonderen Social Support List SSL-D = van Sonderen Social Support ListmdashDiscrepancies SSL-I =van Sonderen Social Support ListmdashInteractions SSL-N = van Sonderen Social Support ListmdashNegative Interactions TMT =Trail-Making Test
e2 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
DNA samplesA 10-mL venous blood sample was taken from OPTIMISTICparticipants at baseline (time point V2) Blood was collectedinto EDTA tubes and stored locally at minus80degC Frozen bloodwas shipped on dry ice to the Newcastle Biobank for Researchof Neuromuscular Disorders29 where DNA was isolated andshipped to the University of Glasgow Baseline DNA sampleswere available from 250 out of 255 OPTIMISTIC partic-ipants Historical DNA samples from OPTIMISTIC partic-ipants collected during routine molecular diagnosis (from 6months to 21 years previously) were available for 71 partic-ipants and obtained from local diagnostic laboratories via theNewcastle Biobank Historical DNA samples were not avail-able for the 5 participants without baseline DNA samples
SP-PCR and AciI digestionSP-PCR was carried out using flanking primers DM-C andDM-DR as previously described1830 using Custom PCRMaster Mix (Thermo Fisher Scientific [Waltham MA] SM-0005) supplemented with 69 mM 2-mercaptoethanol Taqpolymerase (Sigma-Aldrich UK Gillingham) was used at 1unit per 10 μL Where required reactions were supple-mented with 10 DMSO and the annealing temperaturereduced to 635degC PCR products were digested with AciI(New England Biolabs UK Hitchin) in accordance with themanufacturerrsquos instructions DMSO was removed prior toAciI digestion using the QIAquick (Qiagen Venlo theNetherlands) PCR purification kit DNA fragments wereresolved by agarose gel electrophoresis and Southern blothybridized as described1830 Autoradiographic images werescanned and ePAL and modal allele lengths were estimatedfrom the lower boundary18 and the densest part of the ex-panded allele distribution respectively by comparisonagainst the molecular weight ladder using CLIQS 1D gelanalysis software (TotalLab UK Newcastle upon Tyne)
Repeat-primed PCR (RP-PCR)RP-PCR was performed at the 59-end of the repeat tractusing 1 μM DM-A 01 μM TAG-CAG5 and 1 μM TAGprimer and at the 39-end of the repeat tract using 1 μMDM-DR 01 μM TAG-CTG5 and 1 μM TAG primer as de-scribed previously31
Statistical analysisStatistical analyses were undertaken in R (version 343)32
using RStudio (version 10153)33 There were no repeatedmeasures and all individuals are represented once in eachstatistical analysis All statistical analyses were 2-sided Logtransformations of the age at onset degree of somatic in-stability and Stroop interference score were used to betterapproximate a normal distribution andminimize the influenceof extreme values Participants with missing data were ex-cluded from relevant analyses Multiple linear regressionswere performed using the lm function from the R Statspackage In all regression analyses we report the adjusted r2the p value for the overall model and the coefficient (β) and pvalue for each measure Model selection was based on the
Akaike information criterion for each model using a back-wards stepwise selection procedure implemented using thestep function in R34 Confidence intervals (CI) (95) forpoint estimates were calculated where appropriate
Data availabilityThe de-identified participant genetic data presented here areavailable online (datadryadorgreviewdoi=doi105061dryadt063q70) Requests to access the de-identified partici-pant data from the main OPTMISTIC trial should beaddressed to the trial chief investigator Dr Baziel van Engelen(bazielvanengelenradboudumcnl)
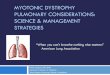
ResultsEstimation of progenitor and modal allele CTGrepeat lengths in the OPTIMISTIC cohortIn order to investigate genetic variation in the OPTIMISTICcohort we used SP-PCR18 to determine the ePAL modalallele length at recruitment and where available (71 partic-ipants) modal allele length at molecular diagnosis for theexpanded CTG repeatDMPK allele (figure 1A) An expandedDMPK CTG repeat allele was readily detected in 241 out of250 participants using our standard SP-PCR procedure In anadditional 7 participants an expanded allele was only detectedafter the addition of 10 DMSO to the PCR consistent withthe presence of GC-rich variant repeats31 In one of theseindividuals even in the presence of DMSO only a smallnumber of expanded alleles was successfully amplified relativeto the non-disease-associated allele and it was not possible todefine the ePAL or modal allele length In 2 remaining indi-viduals we could not successfully amplify an expanded allelealthough in both cases it was possible to amplify a singlenonexpanded allele consistent with the presence of a non-amplifiable expanded allele containing a large number of GC-rich variant repeats (see below for additional analyses) In thecases where we were able to obtain a historical DNA samplethe modal allele length had nearly always noticeably increasedin size between the time of diagnosis and recruitment to thetrial (figure 1A) As expected it was easier to estimate ePALfrom the diagnostic DNA sample obtained at an earlier ageconfirming the value of these historical DNA samples
Identificationof variant repeatswithin theCTGarrays of the OPTIMISTIC cohortAlthough the majority of patients with DM1 likely inherita pure CTG repeat expansion at the DMPK locus it is knownthat a subset of patients contains variant repeat interruptionswithin the disease allele3135 Such variant repeats mostcommonly CCG and CGG have been shown to reduce bothgermline and somatic instability31 and appear to be associatedwith less severe symptoms3135ndash37 Thus we used SP-PCR toamplify the CTG repeat tract and test for the presence ofvariant repeats by post-PCR digestion with AciI (figure 1B)AciI recognizes the sequence CCGC and cleaves both CCGand CGG variant repeats31 Using this approach we identified
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e3
variant repeats in 19 out of 248 expanded alleles (77) Thisincluded all the samples that required the addition of DMSOto facilitate PCR amplification For the 2 samples for which wecould not amplify the expanded allele we used RP-PCR313839
to confirm the presence of an expanded allele (figure 1C) Thepresence of gaps within the repeat ladder of these 2 partic-ipants is consistent with the existence of variant repeats withinthe expanded allele Thus overall the total frequency ofparticipants identified with variant repeats in the expandedallele was 84 (21250 [1321 female] 95 CI54ndash127) This included 1 pair of siblings in both ofwhom we detected variant repeats Interestingly we alsodetected variant repeats in the daughter of a male transmittingparent in whom we did not detect variant repeats consistentwith de novo gain of variant repeats (figure 1B) Similarly we
also detected variant repeats in only 1 of a pair of siblingsconsistent with either a de novo gain or loss of variant repeats(figure 1B) Although the proportion of participants withvariant repeats appeared to differ between centers (Munich 565 [77 95 CI 28ndash178] Newcastle 452 [77 95CI 25ndash194] Nijmegen 966 [136 95 CI68ndash248] Paris 367 [45 95 CI 12ndash134]) thesedifferences were not statistically significant (Fisher exact testp = 032) In one participant we detected variant repeats ina 34-triplet large non-disease-associated allele (figure 1B)
Age at onset correlations in theOPTIMISTIC cohortSelf-reported age at onset of symptoms was available for229 participants and we used linear regression modeling to
Figure 1 Estimation of progenitor and modal CTG repeat length and detection of AciI-sensitive variant repeats
(A) Shown are representative small poolPCR (SP-PCR) analyses of repeat lengthvariation at the DMPK CTG repeat inblood DNA from 5 individuals For eachparticipant the analysis of 2 DNA sam-ples is shown historical sample taken attime of initial diagnosis (H) and at base-line (V2) The age at sampling for eachsample is indicated in years The ap-proximate positions of the molecularweight standards converted into thenumber of CTG triplet repeats are shownon the left The position of the estimatedprogenitor allele length for each in-dividual is indicated with the lowerdashed white line The modal allelelength at each time point is indicated bythe upper dashed white line For eachsample 4 replicate PCRswere performedwith 180ndash300 pg DNA (B) Shown arerepresentative SP-PCR and AciI diges-tions of the DMPK CTG repeat in bloodDNA from 7 individuals For each partic-ipant 3 replicate PCRs were performedwith 500 pg DNA digested (+) or un-digested (minus) with AciI resolved by aga-rose gel electrophoresis and Southernblot hybridized with a repeat unit probeThe approximate positions of the mo-lecular weight standard converted intothe number of CTG triplet repeats ofundigested products is shown on the leftFor each participant the presence (blue)or absence (red) of AciI-sensitive variantrepeats within the expanded allele is in-dicated by filled pedigree symbols NoteOP177 contains AciI-sensitive variantrepeats within the non-disease-associ-ated allele as indicated by the blue tri-angle (C) Detection of expanded allelesusing repeat-primed PCR (RP-PCR)Shown are 59- and 39-RP-PCR assays for 2participants (OP251 and OP121) in whichwe were not able to amplify the ex-panded allele using flanking primers Forboth participants a ladder of productsextending beyond 50 repeats was ob-served using RP-PCR confirming thepresence of a disease-causing expan-sion Notably the ladders were discon-tinuous consistent with the presence ofvariant repeat blocking amplificationfrom the (CAG)5 or (CTG)5 repeat primerat some positions within the array Theapproximate positions of the molecularweight standard converted into thenumber of triplet repeats are shown
e4 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
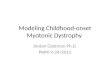
Figure 2 Age at onset and somatic instability correlations
(A) Age at onset is highly correlated with estimated progenitor allele length (ePAL) The scatterplots show the relationship between ePAL and age at onset Therelevant line of best fit under a logarithmic model for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged forall individuals (black linemodel 1a) (table 1) are shown Individualswith (blue) andwithout (red) AciI-sensitive variant repeats are also depicted alongwith thelogarithmic regression line for AciI-sensitive variant repeat carriers (blue line) (B) Effect of variant repeats on age at onset Shown are boxplots for thedifference in observed age at onset minus predicted age at onset for Observational Prolonged Trial in Myotonic Dystrophy Type 1 to Improve Quality ofLifemdashStandards a Target Identification Collaboration (OPTIMISTIC) participants with (yes blue) and without (no red) AciI-sensitive variant repeats in theirexpanded DMPK allele Predicted age at onset was derived usingmodel 1a (Ageo = 803 + [minus234 times log(ePAL)]) (table 1) Themean difference in age at onset forparticipants carrying AciI-sensitive variant repeats was 132 years (95 confidence interval [CI] 57 to 207 2-tailed t test t = minus37 p = 00019) The bottom andtop of the box are the lower and upper quartiles respectively The band near themiddle of the box is themedian and the notches approximate to the 95 CIfor themedians Thewhiskers represent the full range of observations bounded by an upper limit equal to the upper quartile plus 15times the interquartile rangeand a lower limit equal to the lower quartileminus 15times the interquartile range Any points outside these bounds are displayed individually as small circles (C)Modal allele length ePAL and presence of AciI variant repeats The scatterplots show the relationship between ePAL and modal allele length at the V2 timepoint Individuals with (blue) and without (red) AciI-sensitive variant repeats are indicated (D) Sampling bias in the OPTIMISTIC cohort The scatterplots showthe relationship between ePAL and age at onset for the OPTIMISTIC cohort (open diamonds black line) and a family-based DM1 population characterized byMorales et al25 (green triangles and line) The relevant line of best fit under a logarithmic model (model 1a table 1) is shown for each population (for theOPTIMISTIC cohort n = 222 r2 = 0178 p = 31 times 10minus11 and forMorales et al n = 137 r2 = 0640 p lt 22 times 10minus16) Note that theMorales et al cohort hasmore verymildly affected participants with small expansions and more severely affected patients with large expansions (E) ePAL is more informative than thediagnostic measure in predicting age at onset The scatterplots show the relationship between age at onset and ePAL (ePAL open diamonds and black line)and the diagnostic allele length (diagnostic CTGmaroon diamonds and line) for theOPTIMISTIC cohort The relevant line of best fit under a logarithmicmodel(model 1a table 1) is shown for each CTG measure (for ePAL n = 222 r2 = 0178 p = 31 times 10minus11 and for diagnostic CTG n = 105 r2 = 0123 p = 000014)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e5
investigate genotypendashphenotype relationships As expected252640
ePAL was a major modifier of age at onset (figure 2A and table 1model 1a r2 = 0178 p = 31 times 10minus11) The presence of variantrepeats was also highly significantly (p = 22 times 10minus5) associatedwith a later age at onset (figure 2A and table 1 model 1b r2 =0240 p= 34 times 10minus14) In order to better quantify these effects wecalculated the age at onset predicted by ePAL alone (ie model1a) and compared this to the observed age at onset The meandifference in age at onset between individuals with and withoutvariant repeatswas 132 years (95CI 57 to 207 2-tailed t test t=minus37 p = 00019 figure 2B) Recently it has been reported thatthere are substantial sex-dependent differences in the relative in-cidence and severity of some aspects of DM141 Similarly werecently reported some evidence for sex-dependent genotypendashphenotype correlations in age at onset although these appeared tobe driven largely by an excess of mildly affected transmittinggrandfathers40 Here sex was revealed as having a marginally
significant effect (p = 0015) on age at onset (table 1 model 1cr2 = 0257 p = 12 times 10minus14)
Determinants of somatic instability in theOPTIMISTIC cohortWe defined the degree of somatic instability as the differencebetween ePAL and the modal allele at recruitment (time pointV2) As expected2540 the major determinants of the degree ofsomatic instability were ePAL (figure 2C) age at samplingand an interaction between them (table 2 model 2a r2 =0560 p lt 22 times 10minus16) Previously we also demonstrated inone family that the presence of variant repeats reduced thedegree of somatic instability31 Likewise here the presence orabsence of variant repeats (figure 2C) was revealed as a highlysignificant (p = 49 times 10minus8) additional measure in the re-gressionmodel (table 2 model 2b r2 = 0610 p lt 22 times 10minus16)In contrast sex of the participant (p = 048) was found not to
Table 1 Age at onset regression models
Model Adjusted r2 p Value Measure CoefficientStandarderror t Statistic p Value
1a Ageo = β0 + β1Log(ePAL) n = 222 0178 31 times 10minus11 Intercept β0 803 79 102 lt2 times 10minus16
Log(ePAL) β1 minus234 33 minus70 31 times 10minus11
1b Ageo = β0 + β1Log(ePAL) +β2Variant repeats n = 222
0240 34 times 10minus14 Intercept β0 866 77 112 lt2 times 10minus16
Log(ePAL) β1 minus265 33 minus80 55 times 10minus14
Variant repeatsβ2 138 32 43 22 times 10minus5
1c Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex n = 222
0257 13 times 10minus14 Intercept β0 856 77 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 14 times 10minus14
Variant repeatsβ2 146 32 46 70 times 10minus6
Sex β3 38 16 24 0015
1d Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) n = 222
0260 29 times 10minus14 Intercept β0 857 76 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 12 times 10minus14
Variant repeatsβ2 145 32 46 82 times 10minus6
Sex β3 38 16 24 0017
Standardizedresiduals (SI) β4
minus10 08 minus13 0186
1e Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) + β4Standardisedresiduals (SI model 2b) timesLog(ePAL) n = 222
0304 lt22 times 10minus16 Intercept β0 1040 88 118 lt2 times 10minus16
Log(ePAL) β1 minus348 38 minus92 lt2 times 10minus16
Variant repeatsβ2 166 31 53 27 times 10minus7
Sex β3 36 15 23 0020
Standardizedresiduals (SI) β4
250 68 37 29 times 10minus4
Standardizedresiduals (SI) timeslog(ePAL) β5
minus113 29 minus39 15 times 10minus4
Abbreviations Ageo = age at onset SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model The coefficient (β) provides anindication of the relative weight of the contribution of eachmeasure to themodel and its associated standard error The t statistic and corresponding p valueprovide an indication of the statistical significance that the measure is adding explanatory power to the model
e6 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
improve the regression model (table 2 model 2c r2 = 0609p lt 22 times 10minus16)
The role of somatic instability on age at onsetin the OPTIMISTIC cohortAs longer inherited allele lengths precipitate an earlier age at onsetin DM1 and as somatic instability is highly biased toward expan-sions it seems logical to expect that individual-specific differencesin the rate of expansion should modify age at onset Indeed wepreviously established evidence for such an effect in amixed cohortof patients with DM1 from Scotland the United States and CostaRica25 and confirmed this effect in a largeCosta Rican cohort40 IntheOPTIMISTIC cohort incorporating the standardized residualsof somatic instability derived from model 2b into the age at onsetmodel (table 1 model 1d r2 = 0260 p = 30 times 10minus14) improvedthe r2 value slightly from model 1c but the standardized residualsof somatic instability did not reach statistical significance asameasure (p= 019)However when the standardized residuals ofsomatic instability were included with an interaction with ePALthemodel was improved further (table 1 model 1e r2 = 0304 p lt22 times 10minus16) and both the standardized residuals of somatic in-stability alone (p = 29 times 10minus4) and the interaction with ePAL (p =15 times 10minus4) were revealed as highly significant measures
Genetic correlations with progressivephenotypes in the OPTIMISTIC cohortAs part of the OPTIMISTIC protocol several DM1 pheno-types were also quantified at baseline using a variety of direct
and indirect (ie questionnaires) assessment tools27 To in-vestigate the genotypendashphenotype relationships of theseprogressive phenotypes we applied a model selection processincorporating ePAL residual variation in somatic instabilityvariant repeats sex and age at baseline and interactions be-tween ePAL residual variation in somatic instability and ageat baseline (table 3) Highly significant associations with effectsizes comparable to those observed with age at onset wererevealed for many measures (table 3 and figure 3) includingthe Muscle Impairment Rating Scale (MIRS r2 = 032 p = 26times 10minus19) the OPTIMISTIC primary outcome the DM1-Activ-c score (r2 = 023 p = 29 times 10minus13) and key secondaryoutcomes such as the 6-MinuteWalk Test (6-MWT r2 = 031p = 23 times 10minus18) physical activity (accelerometry mean r2 =025 p = 39 times 10minus10 and most active 5-hour r2 = 025 p = 89times 10minus12) the Trail-Making Test (TMT-A r2 = 023 p = 22 times10minus14 and TMT-B r2 = 024 p = 45 times 10minus12) and the Stroopinterference score (r2 = 021 p = 28 times 10minus12) Moderateassociations were observed for the Adult Social BehaviorQuestionnaire (ASBQ r2 = 011 p = 16 times 10minus4) the ApathyEvaluation ScalendashClinician Version (r2 = 010 p = 51 times 10minus5)the Fatigue and Daytime Sleepiness Scale (FDSS) (r2 = 009p = 29 times 10minus5) the Myotonic Dystrophy Health Index totalscore (r2 = 009 p = 34 times 10minus5) and Self-EfficacyndashScale 28 forFatigue (r2 = 007 p = 22 times 10minus4) Only weak or statisticallynonsignificant associations were observed for a number ofmeasures including for van Sonderen Social Support List(SSL) (SSLmdashDiscrepancies [SSL-D] SSLmdashInteractions
Table 2 Regression models of the determinants of the degree of SI
Model Adjusted r2 p Value Measures CoefficientStandarderror t Statistic p Value
2a Log(SI) = β0 + β1Log(ePAL) +β2Ages +β3Log(ePAL) times Agesn = 247
0560 lt22 times 10minus16 Intercept β0 172 073 237 0019
Log(ePAL) β1 020 030 066 0509
Ages β2 minus005 001 minus373 24 times 10minus4
Log(ePAL) times Ages β3 002 001 390 13 times 10minus4
2b Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats n = 247
0610 lt22 times 10minus16 Intercept β0 150 069 219 0029
Log(ePAL) β1 029 028 103 0304
Ages β2 minus005 001 minus394 11 times 10minus4
Log(ePAL) times Ages β3 002 001 417 42 times 10minus5
Variant repeats β4 minus039 007 minus563 49 times 10minus8
2c Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats + β5Sexn = 247
0609 lt22 times 10minus16 Intercept β0 149 069 217 0031
Log(ePAL) β1 030 028 106 0292
Ages β2 minus005 001 minus392 12 times 10minus4
Log(ePAL) times Ages β3 002 001 416 45 times 10minus5
Variant repeats β4 minus039 007 minus567 41 times 10minus8
Sex β5 minus002 004 minus071 0481
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e7
Table 3 Regression models of the determinants of progressive phenotypes
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Muscle impairment rating scale L 247 032 3 times 10minus19 minus006 008 minus01 092
6-min walk test distance (m) H 246 031 2 times 10minus18 289 057 minus627 056
Physical activity (most active 5-h) H 198 025 9 times 10minus12 minus111 5 times 10minus9 minus600 5 times 10minus11
Physical activity (mean) H 198 025 4 times 10minus10 minus010 087 minus164 023
Trail making testmdashA L 234 024 5 times 10minus12 314 020 976 006
Trail making testmdashB L 242 023 2 times 10minus14 082 2 times 10minus15 224 3 times 10minus6
DM1-Activ-c H 246 023 3 times 10minus13 043 057 minus33 084
Log (Stroop interference score) L 238 021 3 times 10minus12 002 3 times 10minus12 07 2 times 10minus5
Adult social behavioural questionnaire L 201 011 00002 099 017 315 003
Apathy evaluation scalemdashclinician score L 241 010 5 times 10minus5 045 038 200 007
Fatigue and daytime sleepiness scale L 242 009 3 times 10minus5 104 004 156 015
Myotonic dystrophy health index L 245 009 3 times 10minus5 043 2 times 10minus5 177 00003
Self-efficacy scale 28 for fatigue H 241 007 00002 minus004 002 minus24 0002
Van Sonderen social supportmdashdiscrepancies L 196 005 001 022 002 97 004
Illness cognition questionnaire H 237 004 002 017 045 35 047
Van Sonderen social supportmdashinteractions H 216 004 002 minus020 006 minus107 009
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
L 245 004 003 minus356 007 minus632 013
Checklist individual strengthmdashfatigue subscale L 247 003 001 007 004
Sickness impact profile L 156 003 002 786 002
McGill pain score L 233 003 002 154 003
Jacobsen fatigue catastrophizing scale L 241 002 003 009 006 54 001
Apathy evaluation scalemdashinformant version L 99 002 032
Beck depression inventorymdashfast screen L 243 001 018 016 036 38 031
Continued
e8
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

Myotonic dystrophy type 1 (DM1) is a highly variableautosomal dominant inherited disorder affecting individu-als of both sexes and all ages1 DM1 is caused by the ex-pansion of a CTG repeat in the DMPK gene that varies inlength from under 40 repeats in the general population tomore than 1000 repeats in some patients2ndash7 Longer CTGtracts are associated with more severe disease and earlierage at onset8ndash11 However genotype to phenotype rela-tionships determined using the traditional diagnostic testhave low predictive value and the International MyotonicDystrophy Consortium recommends that families are notoffered predictive phenotypic information based on the sizeof the CTG repeat12
Expanded disease-causing alleles are highly unstable andusually increase in length during intergenerationaltransmission813ndash15 explaining the decrease in age at onsetof 20ndash30 years per generation typically observed in DM1families16 The expanded CTG is also highly unstable in thesoma in a process that is expansion-biased age-dependentand tissue-specific17ndash24 Thus the average length of theCTG repeat measured using the traditional diagnosticdepends on the age at which the sample was taken Pre-viously we demonstrated that a sensitive small pool PCR(SP-PCR) analysis of blood DNA could be used to estimatethe progenitor allele length (ePAL) ie the length of theCTG repeat transmitted to the individual by the affectedparent18 In addition we demonstrated that ePAL couldreduce the confounding effects of age at sampling inherentin the traditional test and we could dramatically improve theability to predict age at onset in DM12526
Observational Prolonged Trial in Myotonic Dystrophy Type1 to Improve Quality of LifemdashStandards a Target Identifi-cation Collaboration (OPTIMISTIC) was a large in-ternational multicenter model-based randomized trialdesigned to compare the utility of tailored cognitive be-havioral therapy (CBT) with an optional graded exerciseplan against standard care2728 In order to provide additionalinsight into the genetic basis of variability in DM1 and asa route toward genetic stratification in clinical trials wesought to estimate the progenitor allele length and define therepeat dynamics of the DM1 CTG repeat in the blood DNAof participants recruited to OPTIMISTIC
MethodsStandard protocol approvals registrationsand patient consentsFull details of the OPTIMISTIC protocol including powercalculations for sample size have been reported previously(Clinicaltrialsgov NCT02118779)27 All participants wererecruited with informed consent The protocol was approvedby the National Research Ethics Service Committee NorthEastmdashSunderland (UK) the Comite de Protection des Per-sonnes ile de France V (France) the Ethikkommission bei derLMUMunchen (Germany) and the Concernstaf Kwaliteit enVeiligheid Commissie Mensgebonden Onderzoek RegioArnhem-Nijmegen (Netherlands)
Phenotypic dataAmbulant adult patients (gt18 years of age) with geneticallyproven DM1 capable of providing informed consent withsevere fatigue (Checklist Individual StrengthndashFatigue [CIS-Fatigue] score ge35) were recruited between April 2014 andMay 2015 through 4 clinical centers Nijmegen the Nether-lands Paris France Munich Germany and NewcastleUnited Kingdom (n = 255 [463 female] [118255])2728
Exclusion criteria included neurologic or orthopedic comor-bidity possibly influencing the intervention or outcomes useof psychotropic drugs (except modafinil Ritalin and anti-depressants where the dosing regimen was stable for at least12 months prior to screening) severe depression participa-tion in another interventional clinical trial or inability tocomplete study questionnaires Age at onset of DM1 symp-toms was obtained during the trial recruitment screening visitin answer to the question ldquoAt what age did the first medicalproblems occur that may be related to your myotonic dys-trophyrdquo With the exception of patients recruited throughMunich age at sampling was calculated based on known dateof birth and the date of visit 2 at which the blood sample wasprovided As a local regulatory requirement date of birth wasnot recorded for participants recruited in Munich thereforethe age at sampling used was self-reported by participants atvisit 2 Additional baseline (visit 2) clinical measures wereobtained as described in the OPTIMISTIC protocol andreported previously2728 The majority of participants (n =225) were not known to be related Eight parentndashoffspringpairs 4 sibling pairs and 3 trios of 2 siblings and 1 offspringwere also recruited
Glossary6-MWT = 6-Minute Walk Test ASBQ = Adult Social Behavior Questionnaire BDI-fs = Beck Depression Inventorymdashfastscreen CBT = cognitive behavioral therapy CI = confidence interval CIS-fatigue = Checklist Individual Strength FatiguescoreDM1 = myotonic dystrophy type 1 ePAL = estimated progenitor allele length FDSS = Fatigue and Daytime SleepinessScaleMIRS =Muscle Impairment Rating ScaleOPTIMISTIC =Observational Prolonged Trial in Myotonic Dystrophy Type1 to Improve Quality of LifemdashStandards a Target Identification Collaboration RP-PCR = repeat-primed PCR SP-PCR =small pool PCR SSL = van Sonderen Social Support List SSL-D = van Sonderen Social Support ListmdashDiscrepancies SSL-I =van Sonderen Social Support ListmdashInteractions SSL-N = van Sonderen Social Support ListmdashNegative Interactions TMT =Trail-Making Test
e2 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
DNA samplesA 10-mL venous blood sample was taken from OPTIMISTICparticipants at baseline (time point V2) Blood was collectedinto EDTA tubes and stored locally at minus80degC Frozen bloodwas shipped on dry ice to the Newcastle Biobank for Researchof Neuromuscular Disorders29 where DNA was isolated andshipped to the University of Glasgow Baseline DNA sampleswere available from 250 out of 255 OPTIMISTIC partic-ipants Historical DNA samples from OPTIMISTIC partic-ipants collected during routine molecular diagnosis (from 6months to 21 years previously) were available for 71 partic-ipants and obtained from local diagnostic laboratories via theNewcastle Biobank Historical DNA samples were not avail-able for the 5 participants without baseline DNA samples
SP-PCR and AciI digestionSP-PCR was carried out using flanking primers DM-C andDM-DR as previously described1830 using Custom PCRMaster Mix (Thermo Fisher Scientific [Waltham MA] SM-0005) supplemented with 69 mM 2-mercaptoethanol Taqpolymerase (Sigma-Aldrich UK Gillingham) was used at 1unit per 10 μL Where required reactions were supple-mented with 10 DMSO and the annealing temperaturereduced to 635degC PCR products were digested with AciI(New England Biolabs UK Hitchin) in accordance with themanufacturerrsquos instructions DMSO was removed prior toAciI digestion using the QIAquick (Qiagen Venlo theNetherlands) PCR purification kit DNA fragments wereresolved by agarose gel electrophoresis and Southern blothybridized as described1830 Autoradiographic images werescanned and ePAL and modal allele lengths were estimatedfrom the lower boundary18 and the densest part of the ex-panded allele distribution respectively by comparisonagainst the molecular weight ladder using CLIQS 1D gelanalysis software (TotalLab UK Newcastle upon Tyne)
Repeat-primed PCR (RP-PCR)RP-PCR was performed at the 59-end of the repeat tractusing 1 μM DM-A 01 μM TAG-CAG5 and 1 μM TAGprimer and at the 39-end of the repeat tract using 1 μMDM-DR 01 μM TAG-CTG5 and 1 μM TAG primer as de-scribed previously31
Statistical analysisStatistical analyses were undertaken in R (version 343)32
using RStudio (version 10153)33 There were no repeatedmeasures and all individuals are represented once in eachstatistical analysis All statistical analyses were 2-sided Logtransformations of the age at onset degree of somatic in-stability and Stroop interference score were used to betterapproximate a normal distribution andminimize the influenceof extreme values Participants with missing data were ex-cluded from relevant analyses Multiple linear regressionswere performed using the lm function from the R Statspackage In all regression analyses we report the adjusted r2the p value for the overall model and the coefficient (β) and pvalue for each measure Model selection was based on the
Akaike information criterion for each model using a back-wards stepwise selection procedure implemented using thestep function in R34 Confidence intervals (CI) (95) forpoint estimates were calculated where appropriate
Data availabilityThe de-identified participant genetic data presented here areavailable online (datadryadorgreviewdoi=doi105061dryadt063q70) Requests to access the de-identified partici-pant data from the main OPTMISTIC trial should beaddressed to the trial chief investigator Dr Baziel van Engelen(bazielvanengelenradboudumcnl)
ResultsEstimation of progenitor and modal allele CTGrepeat lengths in the OPTIMISTIC cohortIn order to investigate genetic variation in the OPTIMISTICcohort we used SP-PCR18 to determine the ePAL modalallele length at recruitment and where available (71 partic-ipants) modal allele length at molecular diagnosis for theexpanded CTG repeatDMPK allele (figure 1A) An expandedDMPK CTG repeat allele was readily detected in 241 out of250 participants using our standard SP-PCR procedure In anadditional 7 participants an expanded allele was only detectedafter the addition of 10 DMSO to the PCR consistent withthe presence of GC-rich variant repeats31 In one of theseindividuals even in the presence of DMSO only a smallnumber of expanded alleles was successfully amplified relativeto the non-disease-associated allele and it was not possible todefine the ePAL or modal allele length In 2 remaining indi-viduals we could not successfully amplify an expanded allelealthough in both cases it was possible to amplify a singlenonexpanded allele consistent with the presence of a non-amplifiable expanded allele containing a large number of GC-rich variant repeats (see below for additional analyses) In thecases where we were able to obtain a historical DNA samplethe modal allele length had nearly always noticeably increasedin size between the time of diagnosis and recruitment to thetrial (figure 1A) As expected it was easier to estimate ePALfrom the diagnostic DNA sample obtained at an earlier ageconfirming the value of these historical DNA samples
Identificationof variant repeatswithin theCTGarrays of the OPTIMISTIC cohortAlthough the majority of patients with DM1 likely inherita pure CTG repeat expansion at the DMPK locus it is knownthat a subset of patients contains variant repeat interruptionswithin the disease allele3135 Such variant repeats mostcommonly CCG and CGG have been shown to reduce bothgermline and somatic instability31 and appear to be associatedwith less severe symptoms3135ndash37 Thus we used SP-PCR toamplify the CTG repeat tract and test for the presence ofvariant repeats by post-PCR digestion with AciI (figure 1B)AciI recognizes the sequence CCGC and cleaves both CCGand CGG variant repeats31 Using this approach we identified
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e3
variant repeats in 19 out of 248 expanded alleles (77) Thisincluded all the samples that required the addition of DMSOto facilitate PCR amplification For the 2 samples for which wecould not amplify the expanded allele we used RP-PCR313839
to confirm the presence of an expanded allele (figure 1C) Thepresence of gaps within the repeat ladder of these 2 partic-ipants is consistent with the existence of variant repeats withinthe expanded allele Thus overall the total frequency ofparticipants identified with variant repeats in the expandedallele was 84 (21250 [1321 female] 95 CI54ndash127) This included 1 pair of siblings in both ofwhom we detected variant repeats Interestingly we alsodetected variant repeats in the daughter of a male transmittingparent in whom we did not detect variant repeats consistentwith de novo gain of variant repeats (figure 1B) Similarly we
also detected variant repeats in only 1 of a pair of siblingsconsistent with either a de novo gain or loss of variant repeats(figure 1B) Although the proportion of participants withvariant repeats appeared to differ between centers (Munich 565 [77 95 CI 28ndash178] Newcastle 452 [77 95CI 25ndash194] Nijmegen 966 [136 95 CI68ndash248] Paris 367 [45 95 CI 12ndash134]) thesedifferences were not statistically significant (Fisher exact testp = 032) In one participant we detected variant repeats ina 34-triplet large non-disease-associated allele (figure 1B)
Age at onset correlations in theOPTIMISTIC cohortSelf-reported age at onset of symptoms was available for229 participants and we used linear regression modeling to
Figure 1 Estimation of progenitor and modal CTG repeat length and detection of AciI-sensitive variant repeats
(A) Shown are representative small poolPCR (SP-PCR) analyses of repeat lengthvariation at the DMPK CTG repeat inblood DNA from 5 individuals For eachparticipant the analysis of 2 DNA sam-ples is shown historical sample taken attime of initial diagnosis (H) and at base-line (V2) The age at sampling for eachsample is indicated in years The ap-proximate positions of the molecularweight standards converted into thenumber of CTG triplet repeats are shownon the left The position of the estimatedprogenitor allele length for each in-dividual is indicated with the lowerdashed white line The modal allelelength at each time point is indicated bythe upper dashed white line For eachsample 4 replicate PCRswere performedwith 180ndash300 pg DNA (B) Shown arerepresentative SP-PCR and AciI diges-tions of the DMPK CTG repeat in bloodDNA from 7 individuals For each partic-ipant 3 replicate PCRs were performedwith 500 pg DNA digested (+) or un-digested (minus) with AciI resolved by aga-rose gel electrophoresis and Southernblot hybridized with a repeat unit probeThe approximate positions of the mo-lecular weight standard converted intothe number of CTG triplet repeats ofundigested products is shown on the leftFor each participant the presence (blue)or absence (red) of AciI-sensitive variantrepeats within the expanded allele is in-dicated by filled pedigree symbols NoteOP177 contains AciI-sensitive variantrepeats within the non-disease-associ-ated allele as indicated by the blue tri-angle (C) Detection of expanded allelesusing repeat-primed PCR (RP-PCR)Shown are 59- and 39-RP-PCR assays for 2participants (OP251 and OP121) in whichwe were not able to amplify the ex-panded allele using flanking primers Forboth participants a ladder of productsextending beyond 50 repeats was ob-served using RP-PCR confirming thepresence of a disease-causing expan-sion Notably the ladders were discon-tinuous consistent with the presence ofvariant repeat blocking amplificationfrom the (CAG)5 or (CTG)5 repeat primerat some positions within the array Theapproximate positions of the molecularweight standard converted into thenumber of triplet repeats are shown
e4 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
Figure 2 Age at onset and somatic instability correlations
(A) Age at onset is highly correlated with estimated progenitor allele length (ePAL) The scatterplots show the relationship between ePAL and age at onset Therelevant line of best fit under a logarithmic model for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged forall individuals (black linemodel 1a) (table 1) are shown Individualswith (blue) andwithout (red) AciI-sensitive variant repeats are also depicted alongwith thelogarithmic regression line for AciI-sensitive variant repeat carriers (blue line) (B) Effect of variant repeats on age at onset Shown are boxplots for thedifference in observed age at onset minus predicted age at onset for Observational Prolonged Trial in Myotonic Dystrophy Type 1 to Improve Quality ofLifemdashStandards a Target Identification Collaboration (OPTIMISTIC) participants with (yes blue) and without (no red) AciI-sensitive variant repeats in theirexpanded DMPK allele Predicted age at onset was derived usingmodel 1a (Ageo = 803 + [minus234 times log(ePAL)]) (table 1) Themean difference in age at onset forparticipants carrying AciI-sensitive variant repeats was 132 years (95 confidence interval [CI] 57 to 207 2-tailed t test t = minus37 p = 00019) The bottom andtop of the box are the lower and upper quartiles respectively The band near themiddle of the box is themedian and the notches approximate to the 95 CIfor themedians Thewhiskers represent the full range of observations bounded by an upper limit equal to the upper quartile plus 15times the interquartile rangeand a lower limit equal to the lower quartileminus 15times the interquartile range Any points outside these bounds are displayed individually as small circles (C)Modal allele length ePAL and presence of AciI variant repeats The scatterplots show the relationship between ePAL and modal allele length at the V2 timepoint Individuals with (blue) and without (red) AciI-sensitive variant repeats are indicated (D) Sampling bias in the OPTIMISTIC cohort The scatterplots showthe relationship between ePAL and age at onset for the OPTIMISTIC cohort (open diamonds black line) and a family-based DM1 population characterized byMorales et al25 (green triangles and line) The relevant line of best fit under a logarithmic model (model 1a table 1) is shown for each population (for theOPTIMISTIC cohort n = 222 r2 = 0178 p = 31 times 10minus11 and forMorales et al n = 137 r2 = 0640 p lt 22 times 10minus16) Note that theMorales et al cohort hasmore verymildly affected participants with small expansions and more severely affected patients with large expansions (E) ePAL is more informative than thediagnostic measure in predicting age at onset The scatterplots show the relationship between age at onset and ePAL (ePAL open diamonds and black line)and the diagnostic allele length (diagnostic CTGmaroon diamonds and line) for theOPTIMISTIC cohort The relevant line of best fit under a logarithmicmodel(model 1a table 1) is shown for each CTG measure (for ePAL n = 222 r2 = 0178 p = 31 times 10minus11 and for diagnostic CTG n = 105 r2 = 0123 p = 000014)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e5
investigate genotypendashphenotype relationships As expected252640
ePAL was a major modifier of age at onset (figure 2A and table 1model 1a r2 = 0178 p = 31 times 10minus11) The presence of variantrepeats was also highly significantly (p = 22 times 10minus5) associatedwith a later age at onset (figure 2A and table 1 model 1b r2 =0240 p= 34 times 10minus14) In order to better quantify these effects wecalculated the age at onset predicted by ePAL alone (ie model1a) and compared this to the observed age at onset The meandifference in age at onset between individuals with and withoutvariant repeatswas 132 years (95CI 57 to 207 2-tailed t test t=minus37 p = 00019 figure 2B) Recently it has been reported thatthere are substantial sex-dependent differences in the relative in-cidence and severity of some aspects of DM141 Similarly werecently reported some evidence for sex-dependent genotypendashphenotype correlations in age at onset although these appeared tobe driven largely by an excess of mildly affected transmittinggrandfathers40 Here sex was revealed as having a marginally
significant effect (p = 0015) on age at onset (table 1 model 1cr2 = 0257 p = 12 times 10minus14)
Determinants of somatic instability in theOPTIMISTIC cohortWe defined the degree of somatic instability as the differencebetween ePAL and the modal allele at recruitment (time pointV2) As expected2540 the major determinants of the degree ofsomatic instability were ePAL (figure 2C) age at samplingand an interaction between them (table 2 model 2a r2 =0560 p lt 22 times 10minus16) Previously we also demonstrated inone family that the presence of variant repeats reduced thedegree of somatic instability31 Likewise here the presence orabsence of variant repeats (figure 2C) was revealed as a highlysignificant (p = 49 times 10minus8) additional measure in the re-gressionmodel (table 2 model 2b r2 = 0610 p lt 22 times 10minus16)In contrast sex of the participant (p = 048) was found not to
Table 1 Age at onset regression models
Model Adjusted r2 p Value Measure CoefficientStandarderror t Statistic p Value
1a Ageo = β0 + β1Log(ePAL) n = 222 0178 31 times 10minus11 Intercept β0 803 79 102 lt2 times 10minus16
Log(ePAL) β1 minus234 33 minus70 31 times 10minus11
1b Ageo = β0 + β1Log(ePAL) +β2Variant repeats n = 222
0240 34 times 10minus14 Intercept β0 866 77 112 lt2 times 10minus16
Log(ePAL) β1 minus265 33 minus80 55 times 10minus14
Variant repeatsβ2 138 32 43 22 times 10minus5
1c Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex n = 222
0257 13 times 10minus14 Intercept β0 856 77 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 14 times 10minus14
Variant repeatsβ2 146 32 46 70 times 10minus6
Sex β3 38 16 24 0015
1d Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) n = 222
0260 29 times 10minus14 Intercept β0 857 76 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 12 times 10minus14
Variant repeatsβ2 145 32 46 82 times 10minus6
Sex β3 38 16 24 0017
Standardizedresiduals (SI) β4
minus10 08 minus13 0186
1e Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) + β4Standardisedresiduals (SI model 2b) timesLog(ePAL) n = 222
0304 lt22 times 10minus16 Intercept β0 1040 88 118 lt2 times 10minus16
Log(ePAL) β1 minus348 38 minus92 lt2 times 10minus16
Variant repeatsβ2 166 31 53 27 times 10minus7
Sex β3 36 15 23 0020
Standardizedresiduals (SI) β4
250 68 37 29 times 10minus4
Standardizedresiduals (SI) timeslog(ePAL) β5
minus113 29 minus39 15 times 10minus4
Abbreviations Ageo = age at onset SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model The coefficient (β) provides anindication of the relative weight of the contribution of eachmeasure to themodel and its associated standard error The t statistic and corresponding p valueprovide an indication of the statistical significance that the measure is adding explanatory power to the model
e6 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
improve the regression model (table 2 model 2c r2 = 0609p lt 22 times 10minus16)
The role of somatic instability on age at onsetin the OPTIMISTIC cohortAs longer inherited allele lengths precipitate an earlier age at onsetin DM1 and as somatic instability is highly biased toward expan-sions it seems logical to expect that individual-specific differencesin the rate of expansion should modify age at onset Indeed wepreviously established evidence for such an effect in amixed cohortof patients with DM1 from Scotland the United States and CostaRica25 and confirmed this effect in a largeCosta Rican cohort40 IntheOPTIMISTIC cohort incorporating the standardized residualsof somatic instability derived from model 2b into the age at onsetmodel (table 1 model 1d r2 = 0260 p = 30 times 10minus14) improvedthe r2 value slightly from model 1c but the standardized residualsof somatic instability did not reach statistical significance asameasure (p= 019)However when the standardized residuals ofsomatic instability were included with an interaction with ePALthemodel was improved further (table 1 model 1e r2 = 0304 p lt22 times 10minus16) and both the standardized residuals of somatic in-stability alone (p = 29 times 10minus4) and the interaction with ePAL (p =15 times 10minus4) were revealed as highly significant measures
Genetic correlations with progressivephenotypes in the OPTIMISTIC cohortAs part of the OPTIMISTIC protocol several DM1 pheno-types were also quantified at baseline using a variety of direct
and indirect (ie questionnaires) assessment tools27 To in-vestigate the genotypendashphenotype relationships of theseprogressive phenotypes we applied a model selection processincorporating ePAL residual variation in somatic instabilityvariant repeats sex and age at baseline and interactions be-tween ePAL residual variation in somatic instability and ageat baseline (table 3) Highly significant associations with effectsizes comparable to those observed with age at onset wererevealed for many measures (table 3 and figure 3) includingthe Muscle Impairment Rating Scale (MIRS r2 = 032 p = 26times 10minus19) the OPTIMISTIC primary outcome the DM1-Activ-c score (r2 = 023 p = 29 times 10minus13) and key secondaryoutcomes such as the 6-MinuteWalk Test (6-MWT r2 = 031p = 23 times 10minus18) physical activity (accelerometry mean r2 =025 p = 39 times 10minus10 and most active 5-hour r2 = 025 p = 89times 10minus12) the Trail-Making Test (TMT-A r2 = 023 p = 22 times10minus14 and TMT-B r2 = 024 p = 45 times 10minus12) and the Stroopinterference score (r2 = 021 p = 28 times 10minus12) Moderateassociations were observed for the Adult Social BehaviorQuestionnaire (ASBQ r2 = 011 p = 16 times 10minus4) the ApathyEvaluation ScalendashClinician Version (r2 = 010 p = 51 times 10minus5)the Fatigue and Daytime Sleepiness Scale (FDSS) (r2 = 009p = 29 times 10minus5) the Myotonic Dystrophy Health Index totalscore (r2 = 009 p = 34 times 10minus5) and Self-EfficacyndashScale 28 forFatigue (r2 = 007 p = 22 times 10minus4) Only weak or statisticallynonsignificant associations were observed for a number ofmeasures including for van Sonderen Social Support List(SSL) (SSLmdashDiscrepancies [SSL-D] SSLmdashInteractions
Table 2 Regression models of the determinants of the degree of SI
Model Adjusted r2 p Value Measures CoefficientStandarderror t Statistic p Value
2a Log(SI) = β0 + β1Log(ePAL) +β2Ages +β3Log(ePAL) times Agesn = 247
0560 lt22 times 10minus16 Intercept β0 172 073 237 0019
Log(ePAL) β1 020 030 066 0509
Ages β2 minus005 001 minus373 24 times 10minus4
Log(ePAL) times Ages β3 002 001 390 13 times 10minus4
2b Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats n = 247
0610 lt22 times 10minus16 Intercept β0 150 069 219 0029
Log(ePAL) β1 029 028 103 0304
Ages β2 minus005 001 minus394 11 times 10minus4
Log(ePAL) times Ages β3 002 001 417 42 times 10minus5
Variant repeats β4 minus039 007 minus563 49 times 10minus8
2c Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats + β5Sexn = 247
0609 lt22 times 10minus16 Intercept β0 149 069 217 0031
Log(ePAL) β1 030 028 106 0292
Ages β2 minus005 001 minus392 12 times 10minus4
Log(ePAL) times Ages β3 002 001 416 45 times 10minus5
Variant repeats β4 minus039 007 minus567 41 times 10minus8
Sex β5 minus002 004 minus071 0481
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e7
Table 3 Regression models of the determinants of progressive phenotypes
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Muscle impairment rating scale L 247 032 3 times 10minus19 minus006 008 minus01 092
6-min walk test distance (m) H 246 031 2 times 10minus18 289 057 minus627 056
Physical activity (most active 5-h) H 198 025 9 times 10minus12 minus111 5 times 10minus9 minus600 5 times 10minus11
Physical activity (mean) H 198 025 4 times 10minus10 minus010 087 minus164 023
Trail making testmdashA L 234 024 5 times 10minus12 314 020 976 006
Trail making testmdashB L 242 023 2 times 10minus14 082 2 times 10minus15 224 3 times 10minus6
DM1-Activ-c H 246 023 3 times 10minus13 043 057 minus33 084
Log (Stroop interference score) L 238 021 3 times 10minus12 002 3 times 10minus12 07 2 times 10minus5
Adult social behavioural questionnaire L 201 011 00002 099 017 315 003
Apathy evaluation scalemdashclinician score L 241 010 5 times 10minus5 045 038 200 007
Fatigue and daytime sleepiness scale L 242 009 3 times 10minus5 104 004 156 015
Myotonic dystrophy health index L 245 009 3 times 10minus5 043 2 times 10minus5 177 00003
Self-efficacy scale 28 for fatigue H 241 007 00002 minus004 002 minus24 0002
Van Sonderen social supportmdashdiscrepancies L 196 005 001 022 002 97 004
Illness cognition questionnaire H 237 004 002 017 045 35 047
Van Sonderen social supportmdashinteractions H 216 004 002 minus020 006 minus107 009
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
L 245 004 003 minus356 007 minus632 013
Checklist individual strengthmdashfatigue subscale L 247 003 001 007 004
Sickness impact profile L 156 003 002 786 002
McGill pain score L 233 003 002 154 003
Jacobsen fatigue catastrophizing scale L 241 002 003 009 006 54 001
Apathy evaluation scalemdashinformant version L 99 002 032
Beck depression inventorymdashfast screen L 243 001 018 016 036 38 031
Continued
e8
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

DNA samplesA 10-mL venous blood sample was taken from OPTIMISTICparticipants at baseline (time point V2) Blood was collectedinto EDTA tubes and stored locally at minus80degC Frozen bloodwas shipped on dry ice to the Newcastle Biobank for Researchof Neuromuscular Disorders29 where DNA was isolated andshipped to the University of Glasgow Baseline DNA sampleswere available from 250 out of 255 OPTIMISTIC partic-ipants Historical DNA samples from OPTIMISTIC partic-ipants collected during routine molecular diagnosis (from 6months to 21 years previously) were available for 71 partic-ipants and obtained from local diagnostic laboratories via theNewcastle Biobank Historical DNA samples were not avail-able for the 5 participants without baseline DNA samples
SP-PCR and AciI digestionSP-PCR was carried out using flanking primers DM-C andDM-DR as previously described1830 using Custom PCRMaster Mix (Thermo Fisher Scientific [Waltham MA] SM-0005) supplemented with 69 mM 2-mercaptoethanol Taqpolymerase (Sigma-Aldrich UK Gillingham) was used at 1unit per 10 μL Where required reactions were supple-mented with 10 DMSO and the annealing temperaturereduced to 635degC PCR products were digested with AciI(New England Biolabs UK Hitchin) in accordance with themanufacturerrsquos instructions DMSO was removed prior toAciI digestion using the QIAquick (Qiagen Venlo theNetherlands) PCR purification kit DNA fragments wereresolved by agarose gel electrophoresis and Southern blothybridized as described1830 Autoradiographic images werescanned and ePAL and modal allele lengths were estimatedfrom the lower boundary18 and the densest part of the ex-panded allele distribution respectively by comparisonagainst the molecular weight ladder using CLIQS 1D gelanalysis software (TotalLab UK Newcastle upon Tyne)
Repeat-primed PCR (RP-PCR)RP-PCR was performed at the 59-end of the repeat tractusing 1 μM DM-A 01 μM TAG-CAG5 and 1 μM TAGprimer and at the 39-end of the repeat tract using 1 μMDM-DR 01 μM TAG-CTG5 and 1 μM TAG primer as de-scribed previously31
Statistical analysisStatistical analyses were undertaken in R (version 343)32
using RStudio (version 10153)33 There were no repeatedmeasures and all individuals are represented once in eachstatistical analysis All statistical analyses were 2-sided Logtransformations of the age at onset degree of somatic in-stability and Stroop interference score were used to betterapproximate a normal distribution andminimize the influenceof extreme values Participants with missing data were ex-cluded from relevant analyses Multiple linear regressionswere performed using the lm function from the R Statspackage In all regression analyses we report the adjusted r2the p value for the overall model and the coefficient (β) and pvalue for each measure Model selection was based on the
Akaike information criterion for each model using a back-wards stepwise selection procedure implemented using thestep function in R34 Confidence intervals (CI) (95) forpoint estimates were calculated where appropriate
Data availabilityThe de-identified participant genetic data presented here areavailable online (datadryadorgreviewdoi=doi105061dryadt063q70) Requests to access the de-identified partici-pant data from the main OPTMISTIC trial should beaddressed to the trial chief investigator Dr Baziel van Engelen(bazielvanengelenradboudumcnl)
ResultsEstimation of progenitor and modal allele CTGrepeat lengths in the OPTIMISTIC cohortIn order to investigate genetic variation in the OPTIMISTICcohort we used SP-PCR18 to determine the ePAL modalallele length at recruitment and where available (71 partic-ipants) modal allele length at molecular diagnosis for theexpanded CTG repeatDMPK allele (figure 1A) An expandedDMPK CTG repeat allele was readily detected in 241 out of250 participants using our standard SP-PCR procedure In anadditional 7 participants an expanded allele was only detectedafter the addition of 10 DMSO to the PCR consistent withthe presence of GC-rich variant repeats31 In one of theseindividuals even in the presence of DMSO only a smallnumber of expanded alleles was successfully amplified relativeto the non-disease-associated allele and it was not possible todefine the ePAL or modal allele length In 2 remaining indi-viduals we could not successfully amplify an expanded allelealthough in both cases it was possible to amplify a singlenonexpanded allele consistent with the presence of a non-amplifiable expanded allele containing a large number of GC-rich variant repeats (see below for additional analyses) In thecases where we were able to obtain a historical DNA samplethe modal allele length had nearly always noticeably increasedin size between the time of diagnosis and recruitment to thetrial (figure 1A) As expected it was easier to estimate ePALfrom the diagnostic DNA sample obtained at an earlier ageconfirming the value of these historical DNA samples
Identificationof variant repeatswithin theCTGarrays of the OPTIMISTIC cohortAlthough the majority of patients with DM1 likely inherita pure CTG repeat expansion at the DMPK locus it is knownthat a subset of patients contains variant repeat interruptionswithin the disease allele3135 Such variant repeats mostcommonly CCG and CGG have been shown to reduce bothgermline and somatic instability31 and appear to be associatedwith less severe symptoms3135ndash37 Thus we used SP-PCR toamplify the CTG repeat tract and test for the presence ofvariant repeats by post-PCR digestion with AciI (figure 1B)AciI recognizes the sequence CCGC and cleaves both CCGand CGG variant repeats31 Using this approach we identified
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e3
variant repeats in 19 out of 248 expanded alleles (77) Thisincluded all the samples that required the addition of DMSOto facilitate PCR amplification For the 2 samples for which wecould not amplify the expanded allele we used RP-PCR313839
to confirm the presence of an expanded allele (figure 1C) Thepresence of gaps within the repeat ladder of these 2 partic-ipants is consistent with the existence of variant repeats withinthe expanded allele Thus overall the total frequency ofparticipants identified with variant repeats in the expandedallele was 84 (21250 [1321 female] 95 CI54ndash127) This included 1 pair of siblings in both ofwhom we detected variant repeats Interestingly we alsodetected variant repeats in the daughter of a male transmittingparent in whom we did not detect variant repeats consistentwith de novo gain of variant repeats (figure 1B) Similarly we
also detected variant repeats in only 1 of a pair of siblingsconsistent with either a de novo gain or loss of variant repeats(figure 1B) Although the proportion of participants withvariant repeats appeared to differ between centers (Munich 565 [77 95 CI 28ndash178] Newcastle 452 [77 95CI 25ndash194] Nijmegen 966 [136 95 CI68ndash248] Paris 367 [45 95 CI 12ndash134]) thesedifferences were not statistically significant (Fisher exact testp = 032) In one participant we detected variant repeats ina 34-triplet large non-disease-associated allele (figure 1B)
Age at onset correlations in theOPTIMISTIC cohortSelf-reported age at onset of symptoms was available for229 participants and we used linear regression modeling to
Figure 1 Estimation of progenitor and modal CTG repeat length and detection of AciI-sensitive variant repeats
(A) Shown are representative small poolPCR (SP-PCR) analyses of repeat lengthvariation at the DMPK CTG repeat inblood DNA from 5 individuals For eachparticipant the analysis of 2 DNA sam-ples is shown historical sample taken attime of initial diagnosis (H) and at base-line (V2) The age at sampling for eachsample is indicated in years The ap-proximate positions of the molecularweight standards converted into thenumber of CTG triplet repeats are shownon the left The position of the estimatedprogenitor allele length for each in-dividual is indicated with the lowerdashed white line The modal allelelength at each time point is indicated bythe upper dashed white line For eachsample 4 replicate PCRswere performedwith 180ndash300 pg DNA (B) Shown arerepresentative SP-PCR and AciI diges-tions of the DMPK CTG repeat in bloodDNA from 7 individuals For each partic-ipant 3 replicate PCRs were performedwith 500 pg DNA digested (+) or un-digested (minus) with AciI resolved by aga-rose gel electrophoresis and Southernblot hybridized with a repeat unit probeThe approximate positions of the mo-lecular weight standard converted intothe number of CTG triplet repeats ofundigested products is shown on the leftFor each participant the presence (blue)or absence (red) of AciI-sensitive variantrepeats within the expanded allele is in-dicated by filled pedigree symbols NoteOP177 contains AciI-sensitive variantrepeats within the non-disease-associ-ated allele as indicated by the blue tri-angle (C) Detection of expanded allelesusing repeat-primed PCR (RP-PCR)Shown are 59- and 39-RP-PCR assays for 2participants (OP251 and OP121) in whichwe were not able to amplify the ex-panded allele using flanking primers Forboth participants a ladder of productsextending beyond 50 repeats was ob-served using RP-PCR confirming thepresence of a disease-causing expan-sion Notably the ladders were discon-tinuous consistent with the presence ofvariant repeat blocking amplificationfrom the (CAG)5 or (CTG)5 repeat primerat some positions within the array Theapproximate positions of the molecularweight standard converted into thenumber of triplet repeats are shown
e4 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
Figure 2 Age at onset and somatic instability correlations
(A) Age at onset is highly correlated with estimated progenitor allele length (ePAL) The scatterplots show the relationship between ePAL and age at onset Therelevant line of best fit under a logarithmic model for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged forall individuals (black linemodel 1a) (table 1) are shown Individualswith (blue) andwithout (red) AciI-sensitive variant repeats are also depicted alongwith thelogarithmic regression line for AciI-sensitive variant repeat carriers (blue line) (B) Effect of variant repeats on age at onset Shown are boxplots for thedifference in observed age at onset minus predicted age at onset for Observational Prolonged Trial in Myotonic Dystrophy Type 1 to Improve Quality ofLifemdashStandards a Target Identification Collaboration (OPTIMISTIC) participants with (yes blue) and without (no red) AciI-sensitive variant repeats in theirexpanded DMPK allele Predicted age at onset was derived usingmodel 1a (Ageo = 803 + [minus234 times log(ePAL)]) (table 1) Themean difference in age at onset forparticipants carrying AciI-sensitive variant repeats was 132 years (95 confidence interval [CI] 57 to 207 2-tailed t test t = minus37 p = 00019) The bottom andtop of the box are the lower and upper quartiles respectively The band near themiddle of the box is themedian and the notches approximate to the 95 CIfor themedians Thewhiskers represent the full range of observations bounded by an upper limit equal to the upper quartile plus 15times the interquartile rangeand a lower limit equal to the lower quartileminus 15times the interquartile range Any points outside these bounds are displayed individually as small circles (C)Modal allele length ePAL and presence of AciI variant repeats The scatterplots show the relationship between ePAL and modal allele length at the V2 timepoint Individuals with (blue) and without (red) AciI-sensitive variant repeats are indicated (D) Sampling bias in the OPTIMISTIC cohort The scatterplots showthe relationship between ePAL and age at onset for the OPTIMISTIC cohort (open diamonds black line) and a family-based DM1 population characterized byMorales et al25 (green triangles and line) The relevant line of best fit under a logarithmic model (model 1a table 1) is shown for each population (for theOPTIMISTIC cohort n = 222 r2 = 0178 p = 31 times 10minus11 and forMorales et al n = 137 r2 = 0640 p lt 22 times 10minus16) Note that theMorales et al cohort hasmore verymildly affected participants with small expansions and more severely affected patients with large expansions (E) ePAL is more informative than thediagnostic measure in predicting age at onset The scatterplots show the relationship between age at onset and ePAL (ePAL open diamonds and black line)and the diagnostic allele length (diagnostic CTGmaroon diamonds and line) for theOPTIMISTIC cohort The relevant line of best fit under a logarithmicmodel(model 1a table 1) is shown for each CTG measure (for ePAL n = 222 r2 = 0178 p = 31 times 10minus11 and for diagnostic CTG n = 105 r2 = 0123 p = 000014)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e5
investigate genotypendashphenotype relationships As expected252640
ePAL was a major modifier of age at onset (figure 2A and table 1model 1a r2 = 0178 p = 31 times 10minus11) The presence of variantrepeats was also highly significantly (p = 22 times 10minus5) associatedwith a later age at onset (figure 2A and table 1 model 1b r2 =0240 p= 34 times 10minus14) In order to better quantify these effects wecalculated the age at onset predicted by ePAL alone (ie model1a) and compared this to the observed age at onset The meandifference in age at onset between individuals with and withoutvariant repeatswas 132 years (95CI 57 to 207 2-tailed t test t=minus37 p = 00019 figure 2B) Recently it has been reported thatthere are substantial sex-dependent differences in the relative in-cidence and severity of some aspects of DM141 Similarly werecently reported some evidence for sex-dependent genotypendashphenotype correlations in age at onset although these appeared tobe driven largely by an excess of mildly affected transmittinggrandfathers40 Here sex was revealed as having a marginally
significant effect (p = 0015) on age at onset (table 1 model 1cr2 = 0257 p = 12 times 10minus14)
Determinants of somatic instability in theOPTIMISTIC cohortWe defined the degree of somatic instability as the differencebetween ePAL and the modal allele at recruitment (time pointV2) As expected2540 the major determinants of the degree ofsomatic instability were ePAL (figure 2C) age at samplingand an interaction between them (table 2 model 2a r2 =0560 p lt 22 times 10minus16) Previously we also demonstrated inone family that the presence of variant repeats reduced thedegree of somatic instability31 Likewise here the presence orabsence of variant repeats (figure 2C) was revealed as a highlysignificant (p = 49 times 10minus8) additional measure in the re-gressionmodel (table 2 model 2b r2 = 0610 p lt 22 times 10minus16)In contrast sex of the participant (p = 048) was found not to
Table 1 Age at onset regression models
Model Adjusted r2 p Value Measure CoefficientStandarderror t Statistic p Value
1a Ageo = β0 + β1Log(ePAL) n = 222 0178 31 times 10minus11 Intercept β0 803 79 102 lt2 times 10minus16
Log(ePAL) β1 minus234 33 minus70 31 times 10minus11
1b Ageo = β0 + β1Log(ePAL) +β2Variant repeats n = 222
0240 34 times 10minus14 Intercept β0 866 77 112 lt2 times 10minus16
Log(ePAL) β1 minus265 33 minus80 55 times 10minus14
Variant repeatsβ2 138 32 43 22 times 10minus5
1c Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex n = 222
0257 13 times 10minus14 Intercept β0 856 77 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 14 times 10minus14
Variant repeatsβ2 146 32 46 70 times 10minus6
Sex β3 38 16 24 0015
1d Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) n = 222
0260 29 times 10minus14 Intercept β0 857 76 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 12 times 10minus14
Variant repeatsβ2 145 32 46 82 times 10minus6
Sex β3 38 16 24 0017
Standardizedresiduals (SI) β4
minus10 08 minus13 0186
1e Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) + β4Standardisedresiduals (SI model 2b) timesLog(ePAL) n = 222
0304 lt22 times 10minus16 Intercept β0 1040 88 118 lt2 times 10minus16
Log(ePAL) β1 minus348 38 minus92 lt2 times 10minus16
Variant repeatsβ2 166 31 53 27 times 10minus7
Sex β3 36 15 23 0020
Standardizedresiduals (SI) β4
250 68 37 29 times 10minus4
Standardizedresiduals (SI) timeslog(ePAL) β5
minus113 29 minus39 15 times 10minus4
Abbreviations Ageo = age at onset SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model The coefficient (β) provides anindication of the relative weight of the contribution of eachmeasure to themodel and its associated standard error The t statistic and corresponding p valueprovide an indication of the statistical significance that the measure is adding explanatory power to the model
e6 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
improve the regression model (table 2 model 2c r2 = 0609p lt 22 times 10minus16)
The role of somatic instability on age at onsetin the OPTIMISTIC cohortAs longer inherited allele lengths precipitate an earlier age at onsetin DM1 and as somatic instability is highly biased toward expan-sions it seems logical to expect that individual-specific differencesin the rate of expansion should modify age at onset Indeed wepreviously established evidence for such an effect in amixed cohortof patients with DM1 from Scotland the United States and CostaRica25 and confirmed this effect in a largeCosta Rican cohort40 IntheOPTIMISTIC cohort incorporating the standardized residualsof somatic instability derived from model 2b into the age at onsetmodel (table 1 model 1d r2 = 0260 p = 30 times 10minus14) improvedthe r2 value slightly from model 1c but the standardized residualsof somatic instability did not reach statistical significance asameasure (p= 019)However when the standardized residuals ofsomatic instability were included with an interaction with ePALthemodel was improved further (table 1 model 1e r2 = 0304 p lt22 times 10minus16) and both the standardized residuals of somatic in-stability alone (p = 29 times 10minus4) and the interaction with ePAL (p =15 times 10minus4) were revealed as highly significant measures
Genetic correlations with progressivephenotypes in the OPTIMISTIC cohortAs part of the OPTIMISTIC protocol several DM1 pheno-types were also quantified at baseline using a variety of direct
and indirect (ie questionnaires) assessment tools27 To in-vestigate the genotypendashphenotype relationships of theseprogressive phenotypes we applied a model selection processincorporating ePAL residual variation in somatic instabilityvariant repeats sex and age at baseline and interactions be-tween ePAL residual variation in somatic instability and ageat baseline (table 3) Highly significant associations with effectsizes comparable to those observed with age at onset wererevealed for many measures (table 3 and figure 3) includingthe Muscle Impairment Rating Scale (MIRS r2 = 032 p = 26times 10minus19) the OPTIMISTIC primary outcome the DM1-Activ-c score (r2 = 023 p = 29 times 10minus13) and key secondaryoutcomes such as the 6-MinuteWalk Test (6-MWT r2 = 031p = 23 times 10minus18) physical activity (accelerometry mean r2 =025 p = 39 times 10minus10 and most active 5-hour r2 = 025 p = 89times 10minus12) the Trail-Making Test (TMT-A r2 = 023 p = 22 times10minus14 and TMT-B r2 = 024 p = 45 times 10minus12) and the Stroopinterference score (r2 = 021 p = 28 times 10minus12) Moderateassociations were observed for the Adult Social BehaviorQuestionnaire (ASBQ r2 = 011 p = 16 times 10minus4) the ApathyEvaluation ScalendashClinician Version (r2 = 010 p = 51 times 10minus5)the Fatigue and Daytime Sleepiness Scale (FDSS) (r2 = 009p = 29 times 10minus5) the Myotonic Dystrophy Health Index totalscore (r2 = 009 p = 34 times 10minus5) and Self-EfficacyndashScale 28 forFatigue (r2 = 007 p = 22 times 10minus4) Only weak or statisticallynonsignificant associations were observed for a number ofmeasures including for van Sonderen Social Support List(SSL) (SSLmdashDiscrepancies [SSL-D] SSLmdashInteractions
Table 2 Regression models of the determinants of the degree of SI
Model Adjusted r2 p Value Measures CoefficientStandarderror t Statistic p Value
2a Log(SI) = β0 + β1Log(ePAL) +β2Ages +β3Log(ePAL) times Agesn = 247
0560 lt22 times 10minus16 Intercept β0 172 073 237 0019
Log(ePAL) β1 020 030 066 0509
Ages β2 minus005 001 minus373 24 times 10minus4
Log(ePAL) times Ages β3 002 001 390 13 times 10minus4
2b Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats n = 247
0610 lt22 times 10minus16 Intercept β0 150 069 219 0029
Log(ePAL) β1 029 028 103 0304
Ages β2 minus005 001 minus394 11 times 10minus4
Log(ePAL) times Ages β3 002 001 417 42 times 10minus5
Variant repeats β4 minus039 007 minus563 49 times 10minus8
2c Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats + β5Sexn = 247
0609 lt22 times 10minus16 Intercept β0 149 069 217 0031
Log(ePAL) β1 030 028 106 0292
Ages β2 minus005 001 minus392 12 times 10minus4
Log(ePAL) times Ages β3 002 001 416 45 times 10minus5
Variant repeats β4 minus039 007 minus567 41 times 10minus8
Sex β5 minus002 004 minus071 0481
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e7
Table 3 Regression models of the determinants of progressive phenotypes
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Muscle impairment rating scale L 247 032 3 times 10minus19 minus006 008 minus01 092
6-min walk test distance (m) H 246 031 2 times 10minus18 289 057 minus627 056
Physical activity (most active 5-h) H 198 025 9 times 10minus12 minus111 5 times 10minus9 minus600 5 times 10minus11
Physical activity (mean) H 198 025 4 times 10minus10 minus010 087 minus164 023
Trail making testmdashA L 234 024 5 times 10minus12 314 020 976 006
Trail making testmdashB L 242 023 2 times 10minus14 082 2 times 10minus15 224 3 times 10minus6
DM1-Activ-c H 246 023 3 times 10minus13 043 057 minus33 084
Log (Stroop interference score) L 238 021 3 times 10minus12 002 3 times 10minus12 07 2 times 10minus5
Adult social behavioural questionnaire L 201 011 00002 099 017 315 003
Apathy evaluation scalemdashclinician score L 241 010 5 times 10minus5 045 038 200 007
Fatigue and daytime sleepiness scale L 242 009 3 times 10minus5 104 004 156 015
Myotonic dystrophy health index L 245 009 3 times 10minus5 043 2 times 10minus5 177 00003
Self-efficacy scale 28 for fatigue H 241 007 00002 minus004 002 minus24 0002
Van Sonderen social supportmdashdiscrepancies L 196 005 001 022 002 97 004
Illness cognition questionnaire H 237 004 002 017 045 35 047
Van Sonderen social supportmdashinteractions H 216 004 002 minus020 006 minus107 009
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
L 245 004 003 minus356 007 minus632 013
Checklist individual strengthmdashfatigue subscale L 247 003 001 007 004
Sickness impact profile L 156 003 002 786 002
McGill pain score L 233 003 002 154 003
Jacobsen fatigue catastrophizing scale L 241 002 003 009 006 54 001
Apathy evaluation scalemdashinformant version L 99 002 032
Beck depression inventorymdashfast screen L 243 001 018 016 036 38 031
Continued
e8
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

variant repeats in 19 out of 248 expanded alleles (77) Thisincluded all the samples that required the addition of DMSOto facilitate PCR amplification For the 2 samples for which wecould not amplify the expanded allele we used RP-PCR313839
to confirm the presence of an expanded allele (figure 1C) Thepresence of gaps within the repeat ladder of these 2 partic-ipants is consistent with the existence of variant repeats withinthe expanded allele Thus overall the total frequency ofparticipants identified with variant repeats in the expandedallele was 84 (21250 [1321 female] 95 CI54ndash127) This included 1 pair of siblings in both ofwhom we detected variant repeats Interestingly we alsodetected variant repeats in the daughter of a male transmittingparent in whom we did not detect variant repeats consistentwith de novo gain of variant repeats (figure 1B) Similarly we
also detected variant repeats in only 1 of a pair of siblingsconsistent with either a de novo gain or loss of variant repeats(figure 1B) Although the proportion of participants withvariant repeats appeared to differ between centers (Munich 565 [77 95 CI 28ndash178] Newcastle 452 [77 95CI 25ndash194] Nijmegen 966 [136 95 CI68ndash248] Paris 367 [45 95 CI 12ndash134]) thesedifferences were not statistically significant (Fisher exact testp = 032) In one participant we detected variant repeats ina 34-triplet large non-disease-associated allele (figure 1B)
Age at onset correlations in theOPTIMISTIC cohortSelf-reported age at onset of symptoms was available for229 participants and we used linear regression modeling to
Figure 1 Estimation of progenitor and modal CTG repeat length and detection of AciI-sensitive variant repeats
(A) Shown are representative small poolPCR (SP-PCR) analyses of repeat lengthvariation at the DMPK CTG repeat inblood DNA from 5 individuals For eachparticipant the analysis of 2 DNA sam-ples is shown historical sample taken attime of initial diagnosis (H) and at base-line (V2) The age at sampling for eachsample is indicated in years The ap-proximate positions of the molecularweight standards converted into thenumber of CTG triplet repeats are shownon the left The position of the estimatedprogenitor allele length for each in-dividual is indicated with the lowerdashed white line The modal allelelength at each time point is indicated bythe upper dashed white line For eachsample 4 replicate PCRswere performedwith 180ndash300 pg DNA (B) Shown arerepresentative SP-PCR and AciI diges-tions of the DMPK CTG repeat in bloodDNA from 7 individuals For each partic-ipant 3 replicate PCRs were performedwith 500 pg DNA digested (+) or un-digested (minus) with AciI resolved by aga-rose gel electrophoresis and Southernblot hybridized with a repeat unit probeThe approximate positions of the mo-lecular weight standard converted intothe number of CTG triplet repeats ofundigested products is shown on the leftFor each participant the presence (blue)or absence (red) of AciI-sensitive variantrepeats within the expanded allele is in-dicated by filled pedigree symbols NoteOP177 contains AciI-sensitive variantrepeats within the non-disease-associ-ated allele as indicated by the blue tri-angle (C) Detection of expanded allelesusing repeat-primed PCR (RP-PCR)Shown are 59- and 39-RP-PCR assays for 2participants (OP251 and OP121) in whichwe were not able to amplify the ex-panded allele using flanking primers Forboth participants a ladder of productsextending beyond 50 repeats was ob-served using RP-PCR confirming thepresence of a disease-causing expan-sion Notably the ladders were discon-tinuous consistent with the presence ofvariant repeat blocking amplificationfrom the (CAG)5 or (CTG)5 repeat primerat some positions within the array Theapproximate positions of the molecularweight standard converted into thenumber of triplet repeats are shown
e4 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
Figure 2 Age at onset and somatic instability correlations
(A) Age at onset is highly correlated with estimated progenitor allele length (ePAL) The scatterplots show the relationship between ePAL and age at onset Therelevant line of best fit under a logarithmic model for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged forall individuals (black linemodel 1a) (table 1) are shown Individualswith (blue) andwithout (red) AciI-sensitive variant repeats are also depicted alongwith thelogarithmic regression line for AciI-sensitive variant repeat carriers (blue line) (B) Effect of variant repeats on age at onset Shown are boxplots for thedifference in observed age at onset minus predicted age at onset for Observational Prolonged Trial in Myotonic Dystrophy Type 1 to Improve Quality ofLifemdashStandards a Target Identification Collaboration (OPTIMISTIC) participants with (yes blue) and without (no red) AciI-sensitive variant repeats in theirexpanded DMPK allele Predicted age at onset was derived usingmodel 1a (Ageo = 803 + [minus234 times log(ePAL)]) (table 1) Themean difference in age at onset forparticipants carrying AciI-sensitive variant repeats was 132 years (95 confidence interval [CI] 57 to 207 2-tailed t test t = minus37 p = 00019) The bottom andtop of the box are the lower and upper quartiles respectively The band near themiddle of the box is themedian and the notches approximate to the 95 CIfor themedians Thewhiskers represent the full range of observations bounded by an upper limit equal to the upper quartile plus 15times the interquartile rangeand a lower limit equal to the lower quartileminus 15times the interquartile range Any points outside these bounds are displayed individually as small circles (C)Modal allele length ePAL and presence of AciI variant repeats The scatterplots show the relationship between ePAL and modal allele length at the V2 timepoint Individuals with (blue) and without (red) AciI-sensitive variant repeats are indicated (D) Sampling bias in the OPTIMISTIC cohort The scatterplots showthe relationship between ePAL and age at onset for the OPTIMISTIC cohort (open diamonds black line) and a family-based DM1 population characterized byMorales et al25 (green triangles and line) The relevant line of best fit under a logarithmic model (model 1a table 1) is shown for each population (for theOPTIMISTIC cohort n = 222 r2 = 0178 p = 31 times 10minus11 and forMorales et al n = 137 r2 = 0640 p lt 22 times 10minus16) Note that theMorales et al cohort hasmore verymildly affected participants with small expansions and more severely affected patients with large expansions (E) ePAL is more informative than thediagnostic measure in predicting age at onset The scatterplots show the relationship between age at onset and ePAL (ePAL open diamonds and black line)and the diagnostic allele length (diagnostic CTGmaroon diamonds and line) for theOPTIMISTIC cohort The relevant line of best fit under a logarithmicmodel(model 1a table 1) is shown for each CTG measure (for ePAL n = 222 r2 = 0178 p = 31 times 10minus11 and for diagnostic CTG n = 105 r2 = 0123 p = 000014)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e5
investigate genotypendashphenotype relationships As expected252640
ePAL was a major modifier of age at onset (figure 2A and table 1model 1a r2 = 0178 p = 31 times 10minus11) The presence of variantrepeats was also highly significantly (p = 22 times 10minus5) associatedwith a later age at onset (figure 2A and table 1 model 1b r2 =0240 p= 34 times 10minus14) In order to better quantify these effects wecalculated the age at onset predicted by ePAL alone (ie model1a) and compared this to the observed age at onset The meandifference in age at onset between individuals with and withoutvariant repeatswas 132 years (95CI 57 to 207 2-tailed t test t=minus37 p = 00019 figure 2B) Recently it has been reported thatthere are substantial sex-dependent differences in the relative in-cidence and severity of some aspects of DM141 Similarly werecently reported some evidence for sex-dependent genotypendashphenotype correlations in age at onset although these appeared tobe driven largely by an excess of mildly affected transmittinggrandfathers40 Here sex was revealed as having a marginally
significant effect (p = 0015) on age at onset (table 1 model 1cr2 = 0257 p = 12 times 10minus14)
Determinants of somatic instability in theOPTIMISTIC cohortWe defined the degree of somatic instability as the differencebetween ePAL and the modal allele at recruitment (time pointV2) As expected2540 the major determinants of the degree ofsomatic instability were ePAL (figure 2C) age at samplingand an interaction between them (table 2 model 2a r2 =0560 p lt 22 times 10minus16) Previously we also demonstrated inone family that the presence of variant repeats reduced thedegree of somatic instability31 Likewise here the presence orabsence of variant repeats (figure 2C) was revealed as a highlysignificant (p = 49 times 10minus8) additional measure in the re-gressionmodel (table 2 model 2b r2 = 0610 p lt 22 times 10minus16)In contrast sex of the participant (p = 048) was found not to
Table 1 Age at onset regression models
Model Adjusted r2 p Value Measure CoefficientStandarderror t Statistic p Value
1a Ageo = β0 + β1Log(ePAL) n = 222 0178 31 times 10minus11 Intercept β0 803 79 102 lt2 times 10minus16
Log(ePAL) β1 minus234 33 minus70 31 times 10minus11
1b Ageo = β0 + β1Log(ePAL) +β2Variant repeats n = 222
0240 34 times 10minus14 Intercept β0 866 77 112 lt2 times 10minus16
Log(ePAL) β1 minus265 33 minus80 55 times 10minus14
Variant repeatsβ2 138 32 43 22 times 10minus5
1c Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex n = 222
0257 13 times 10minus14 Intercept β0 856 77 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 14 times 10minus14
Variant repeatsβ2 146 32 46 70 times 10minus6
Sex β3 38 16 24 0015
1d Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) n = 222
0260 29 times 10minus14 Intercept β0 857 76 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 12 times 10minus14
Variant repeatsβ2 145 32 46 82 times 10minus6
Sex β3 38 16 24 0017
Standardizedresiduals (SI) β4
minus10 08 minus13 0186
1e Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) + β4Standardisedresiduals (SI model 2b) timesLog(ePAL) n = 222
0304 lt22 times 10minus16 Intercept β0 1040 88 118 lt2 times 10minus16
Log(ePAL) β1 minus348 38 minus92 lt2 times 10minus16
Variant repeatsβ2 166 31 53 27 times 10minus7
Sex β3 36 15 23 0020
Standardizedresiduals (SI) β4
250 68 37 29 times 10minus4
Standardizedresiduals (SI) timeslog(ePAL) β5
minus113 29 minus39 15 times 10minus4
Abbreviations Ageo = age at onset SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model The coefficient (β) provides anindication of the relative weight of the contribution of eachmeasure to themodel and its associated standard error The t statistic and corresponding p valueprovide an indication of the statistical significance that the measure is adding explanatory power to the model
e6 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
improve the regression model (table 2 model 2c r2 = 0609p lt 22 times 10minus16)
The role of somatic instability on age at onsetin the OPTIMISTIC cohortAs longer inherited allele lengths precipitate an earlier age at onsetin DM1 and as somatic instability is highly biased toward expan-sions it seems logical to expect that individual-specific differencesin the rate of expansion should modify age at onset Indeed wepreviously established evidence for such an effect in amixed cohortof patients with DM1 from Scotland the United States and CostaRica25 and confirmed this effect in a largeCosta Rican cohort40 IntheOPTIMISTIC cohort incorporating the standardized residualsof somatic instability derived from model 2b into the age at onsetmodel (table 1 model 1d r2 = 0260 p = 30 times 10minus14) improvedthe r2 value slightly from model 1c but the standardized residualsof somatic instability did not reach statistical significance asameasure (p= 019)However when the standardized residuals ofsomatic instability were included with an interaction with ePALthemodel was improved further (table 1 model 1e r2 = 0304 p lt22 times 10minus16) and both the standardized residuals of somatic in-stability alone (p = 29 times 10minus4) and the interaction with ePAL (p =15 times 10minus4) were revealed as highly significant measures
Genetic correlations with progressivephenotypes in the OPTIMISTIC cohortAs part of the OPTIMISTIC protocol several DM1 pheno-types were also quantified at baseline using a variety of direct
and indirect (ie questionnaires) assessment tools27 To in-vestigate the genotypendashphenotype relationships of theseprogressive phenotypes we applied a model selection processincorporating ePAL residual variation in somatic instabilityvariant repeats sex and age at baseline and interactions be-tween ePAL residual variation in somatic instability and ageat baseline (table 3) Highly significant associations with effectsizes comparable to those observed with age at onset wererevealed for many measures (table 3 and figure 3) includingthe Muscle Impairment Rating Scale (MIRS r2 = 032 p = 26times 10minus19) the OPTIMISTIC primary outcome the DM1-Activ-c score (r2 = 023 p = 29 times 10minus13) and key secondaryoutcomes such as the 6-MinuteWalk Test (6-MWT r2 = 031p = 23 times 10minus18) physical activity (accelerometry mean r2 =025 p = 39 times 10minus10 and most active 5-hour r2 = 025 p = 89times 10minus12) the Trail-Making Test (TMT-A r2 = 023 p = 22 times10minus14 and TMT-B r2 = 024 p = 45 times 10minus12) and the Stroopinterference score (r2 = 021 p = 28 times 10minus12) Moderateassociations were observed for the Adult Social BehaviorQuestionnaire (ASBQ r2 = 011 p = 16 times 10minus4) the ApathyEvaluation ScalendashClinician Version (r2 = 010 p = 51 times 10minus5)the Fatigue and Daytime Sleepiness Scale (FDSS) (r2 = 009p = 29 times 10minus5) the Myotonic Dystrophy Health Index totalscore (r2 = 009 p = 34 times 10minus5) and Self-EfficacyndashScale 28 forFatigue (r2 = 007 p = 22 times 10minus4) Only weak or statisticallynonsignificant associations were observed for a number ofmeasures including for van Sonderen Social Support List(SSL) (SSLmdashDiscrepancies [SSL-D] SSLmdashInteractions
Table 2 Regression models of the determinants of the degree of SI
Model Adjusted r2 p Value Measures CoefficientStandarderror t Statistic p Value
2a Log(SI) = β0 + β1Log(ePAL) +β2Ages +β3Log(ePAL) times Agesn = 247
0560 lt22 times 10minus16 Intercept β0 172 073 237 0019
Log(ePAL) β1 020 030 066 0509
Ages β2 minus005 001 minus373 24 times 10minus4
Log(ePAL) times Ages β3 002 001 390 13 times 10minus4
2b Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats n = 247
0610 lt22 times 10minus16 Intercept β0 150 069 219 0029
Log(ePAL) β1 029 028 103 0304
Ages β2 minus005 001 minus394 11 times 10minus4
Log(ePAL) times Ages β3 002 001 417 42 times 10minus5
Variant repeats β4 minus039 007 minus563 49 times 10minus8
2c Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats + β5Sexn = 247
0609 lt22 times 10minus16 Intercept β0 149 069 217 0031
Log(ePAL) β1 030 028 106 0292
Ages β2 minus005 001 minus392 12 times 10minus4
Log(ePAL) times Ages β3 002 001 416 45 times 10minus5
Variant repeats β4 minus039 007 minus567 41 times 10minus8
Sex β5 minus002 004 minus071 0481
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e7
Table 3 Regression models of the determinants of progressive phenotypes
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Muscle impairment rating scale L 247 032 3 times 10minus19 minus006 008 minus01 092
6-min walk test distance (m) H 246 031 2 times 10minus18 289 057 minus627 056
Physical activity (most active 5-h) H 198 025 9 times 10minus12 minus111 5 times 10minus9 minus600 5 times 10minus11
Physical activity (mean) H 198 025 4 times 10minus10 minus010 087 minus164 023
Trail making testmdashA L 234 024 5 times 10minus12 314 020 976 006
Trail making testmdashB L 242 023 2 times 10minus14 082 2 times 10minus15 224 3 times 10minus6
DM1-Activ-c H 246 023 3 times 10minus13 043 057 minus33 084
Log (Stroop interference score) L 238 021 3 times 10minus12 002 3 times 10minus12 07 2 times 10minus5
Adult social behavioural questionnaire L 201 011 00002 099 017 315 003
Apathy evaluation scalemdashclinician score L 241 010 5 times 10minus5 045 038 200 007
Fatigue and daytime sleepiness scale L 242 009 3 times 10minus5 104 004 156 015
Myotonic dystrophy health index L 245 009 3 times 10minus5 043 2 times 10minus5 177 00003
Self-efficacy scale 28 for fatigue H 241 007 00002 minus004 002 minus24 0002
Van Sonderen social supportmdashdiscrepancies L 196 005 001 022 002 97 004
Illness cognition questionnaire H 237 004 002 017 045 35 047
Van Sonderen social supportmdashinteractions H 216 004 002 minus020 006 minus107 009
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
L 245 004 003 minus356 007 minus632 013
Checklist individual strengthmdashfatigue subscale L 247 003 001 007 004
Sickness impact profile L 156 003 002 786 002
McGill pain score L 233 003 002 154 003
Jacobsen fatigue catastrophizing scale L 241 002 003 009 006 54 001
Apathy evaluation scalemdashinformant version L 99 002 032
Beck depression inventorymdashfast screen L 243 001 018 016 036 38 031
Continued
e8
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

Figure 2 Age at onset and somatic instability correlations
(A) Age at onset is highly correlated with estimated progenitor allele length (ePAL) The scatterplots show the relationship between ePAL and age at onset Therelevant line of best fit under a logarithmic model for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged forall individuals (black linemodel 1a) (table 1) are shown Individualswith (blue) andwithout (red) AciI-sensitive variant repeats are also depicted alongwith thelogarithmic regression line for AciI-sensitive variant repeat carriers (blue line) (B) Effect of variant repeats on age at onset Shown are boxplots for thedifference in observed age at onset minus predicted age at onset for Observational Prolonged Trial in Myotonic Dystrophy Type 1 to Improve Quality ofLifemdashStandards a Target Identification Collaboration (OPTIMISTIC) participants with (yes blue) and without (no red) AciI-sensitive variant repeats in theirexpanded DMPK allele Predicted age at onset was derived usingmodel 1a (Ageo = 803 + [minus234 times log(ePAL)]) (table 1) Themean difference in age at onset forparticipants carrying AciI-sensitive variant repeats was 132 years (95 confidence interval [CI] 57 to 207 2-tailed t test t = minus37 p = 00019) The bottom andtop of the box are the lower and upper quartiles respectively The band near themiddle of the box is themedian and the notches approximate to the 95 CIfor themedians Thewhiskers represent the full range of observations bounded by an upper limit equal to the upper quartile plus 15times the interquartile rangeand a lower limit equal to the lower quartileminus 15times the interquartile range Any points outside these bounds are displayed individually as small circles (C)Modal allele length ePAL and presence of AciI variant repeats The scatterplots show the relationship between ePAL and modal allele length at the V2 timepoint Individuals with (blue) and without (red) AciI-sensitive variant repeats are indicated (D) Sampling bias in the OPTIMISTIC cohort The scatterplots showthe relationship between ePAL and age at onset for the OPTIMISTIC cohort (open diamonds black line) and a family-based DM1 population characterized byMorales et al25 (green triangles and line) The relevant line of best fit under a logarithmic model (model 1a table 1) is shown for each population (for theOPTIMISTIC cohort n = 222 r2 = 0178 p = 31 times 10minus11 and forMorales et al n = 137 r2 = 0640 p lt 22 times 10minus16) Note that theMorales et al cohort hasmore verymildly affected participants with small expansions and more severely affected patients with large expansions (E) ePAL is more informative than thediagnostic measure in predicting age at onset The scatterplots show the relationship between age at onset and ePAL (ePAL open diamonds and black line)and the diagnostic allele length (diagnostic CTGmaroon diamonds and line) for theOPTIMISTIC cohort The relevant line of best fit under a logarithmicmodel(model 1a table 1) is shown for each CTG measure (for ePAL n = 222 r2 = 0178 p = 31 times 10minus11 and for diagnostic CTG n = 105 r2 = 0123 p = 000014)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e5
investigate genotypendashphenotype relationships As expected252640
ePAL was a major modifier of age at onset (figure 2A and table 1model 1a r2 = 0178 p = 31 times 10minus11) The presence of variantrepeats was also highly significantly (p = 22 times 10minus5) associatedwith a later age at onset (figure 2A and table 1 model 1b r2 =0240 p= 34 times 10minus14) In order to better quantify these effects wecalculated the age at onset predicted by ePAL alone (ie model1a) and compared this to the observed age at onset The meandifference in age at onset between individuals with and withoutvariant repeatswas 132 years (95CI 57 to 207 2-tailed t test t=minus37 p = 00019 figure 2B) Recently it has been reported thatthere are substantial sex-dependent differences in the relative in-cidence and severity of some aspects of DM141 Similarly werecently reported some evidence for sex-dependent genotypendashphenotype correlations in age at onset although these appeared tobe driven largely by an excess of mildly affected transmittinggrandfathers40 Here sex was revealed as having a marginally
significant effect (p = 0015) on age at onset (table 1 model 1cr2 = 0257 p = 12 times 10minus14)
Determinants of somatic instability in theOPTIMISTIC cohortWe defined the degree of somatic instability as the differencebetween ePAL and the modal allele at recruitment (time pointV2) As expected2540 the major determinants of the degree ofsomatic instability were ePAL (figure 2C) age at samplingand an interaction between them (table 2 model 2a r2 =0560 p lt 22 times 10minus16) Previously we also demonstrated inone family that the presence of variant repeats reduced thedegree of somatic instability31 Likewise here the presence orabsence of variant repeats (figure 2C) was revealed as a highlysignificant (p = 49 times 10minus8) additional measure in the re-gressionmodel (table 2 model 2b r2 = 0610 p lt 22 times 10minus16)In contrast sex of the participant (p = 048) was found not to
Table 1 Age at onset regression models
Model Adjusted r2 p Value Measure CoefficientStandarderror t Statistic p Value
1a Ageo = β0 + β1Log(ePAL) n = 222 0178 31 times 10minus11 Intercept β0 803 79 102 lt2 times 10minus16
Log(ePAL) β1 minus234 33 minus70 31 times 10minus11
1b Ageo = β0 + β1Log(ePAL) +β2Variant repeats n = 222
0240 34 times 10minus14 Intercept β0 866 77 112 lt2 times 10minus16
Log(ePAL) β1 minus265 33 minus80 55 times 10minus14
Variant repeatsβ2 138 32 43 22 times 10minus5
1c Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex n = 222
0257 13 times 10minus14 Intercept β0 856 77 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 14 times 10minus14
Variant repeatsβ2 146 32 46 70 times 10minus6
Sex β3 38 16 24 0015
1d Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) n = 222
0260 29 times 10minus14 Intercept β0 857 76 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 12 times 10minus14
Variant repeatsβ2 145 32 46 82 times 10minus6
Sex β3 38 16 24 0017
Standardizedresiduals (SI) β4
minus10 08 minus13 0186
1e Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) + β4Standardisedresiduals (SI model 2b) timesLog(ePAL) n = 222
0304 lt22 times 10minus16 Intercept β0 1040 88 118 lt2 times 10minus16
Log(ePAL) β1 minus348 38 minus92 lt2 times 10minus16
Variant repeatsβ2 166 31 53 27 times 10minus7
Sex β3 36 15 23 0020
Standardizedresiduals (SI) β4
250 68 37 29 times 10minus4
Standardizedresiduals (SI) timeslog(ePAL) β5
minus113 29 minus39 15 times 10minus4
Abbreviations Ageo = age at onset SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model The coefficient (β) provides anindication of the relative weight of the contribution of eachmeasure to themodel and its associated standard error The t statistic and corresponding p valueprovide an indication of the statistical significance that the measure is adding explanatory power to the model
e6 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
improve the regression model (table 2 model 2c r2 = 0609p lt 22 times 10minus16)
The role of somatic instability on age at onsetin the OPTIMISTIC cohortAs longer inherited allele lengths precipitate an earlier age at onsetin DM1 and as somatic instability is highly biased toward expan-sions it seems logical to expect that individual-specific differencesin the rate of expansion should modify age at onset Indeed wepreviously established evidence for such an effect in amixed cohortof patients with DM1 from Scotland the United States and CostaRica25 and confirmed this effect in a largeCosta Rican cohort40 IntheOPTIMISTIC cohort incorporating the standardized residualsof somatic instability derived from model 2b into the age at onsetmodel (table 1 model 1d r2 = 0260 p = 30 times 10minus14) improvedthe r2 value slightly from model 1c but the standardized residualsof somatic instability did not reach statistical significance asameasure (p= 019)However when the standardized residuals ofsomatic instability were included with an interaction with ePALthemodel was improved further (table 1 model 1e r2 = 0304 p lt22 times 10minus16) and both the standardized residuals of somatic in-stability alone (p = 29 times 10minus4) and the interaction with ePAL (p =15 times 10minus4) were revealed as highly significant measures
Genetic correlations with progressivephenotypes in the OPTIMISTIC cohortAs part of the OPTIMISTIC protocol several DM1 pheno-types were also quantified at baseline using a variety of direct
and indirect (ie questionnaires) assessment tools27 To in-vestigate the genotypendashphenotype relationships of theseprogressive phenotypes we applied a model selection processincorporating ePAL residual variation in somatic instabilityvariant repeats sex and age at baseline and interactions be-tween ePAL residual variation in somatic instability and ageat baseline (table 3) Highly significant associations with effectsizes comparable to those observed with age at onset wererevealed for many measures (table 3 and figure 3) includingthe Muscle Impairment Rating Scale (MIRS r2 = 032 p = 26times 10minus19) the OPTIMISTIC primary outcome the DM1-Activ-c score (r2 = 023 p = 29 times 10minus13) and key secondaryoutcomes such as the 6-MinuteWalk Test (6-MWT r2 = 031p = 23 times 10minus18) physical activity (accelerometry mean r2 =025 p = 39 times 10minus10 and most active 5-hour r2 = 025 p = 89times 10minus12) the Trail-Making Test (TMT-A r2 = 023 p = 22 times10minus14 and TMT-B r2 = 024 p = 45 times 10minus12) and the Stroopinterference score (r2 = 021 p = 28 times 10minus12) Moderateassociations were observed for the Adult Social BehaviorQuestionnaire (ASBQ r2 = 011 p = 16 times 10minus4) the ApathyEvaluation ScalendashClinician Version (r2 = 010 p = 51 times 10minus5)the Fatigue and Daytime Sleepiness Scale (FDSS) (r2 = 009p = 29 times 10minus5) the Myotonic Dystrophy Health Index totalscore (r2 = 009 p = 34 times 10minus5) and Self-EfficacyndashScale 28 forFatigue (r2 = 007 p = 22 times 10minus4) Only weak or statisticallynonsignificant associations were observed for a number ofmeasures including for van Sonderen Social Support List(SSL) (SSLmdashDiscrepancies [SSL-D] SSLmdashInteractions
Table 2 Regression models of the determinants of the degree of SI
Model Adjusted r2 p Value Measures CoefficientStandarderror t Statistic p Value
2a Log(SI) = β0 + β1Log(ePAL) +β2Ages +β3Log(ePAL) times Agesn = 247
0560 lt22 times 10minus16 Intercept β0 172 073 237 0019
Log(ePAL) β1 020 030 066 0509
Ages β2 minus005 001 minus373 24 times 10minus4
Log(ePAL) times Ages β3 002 001 390 13 times 10minus4
2b Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats n = 247
0610 lt22 times 10minus16 Intercept β0 150 069 219 0029
Log(ePAL) β1 029 028 103 0304
Ages β2 minus005 001 minus394 11 times 10minus4
Log(ePAL) times Ages β3 002 001 417 42 times 10minus5
Variant repeats β4 minus039 007 minus563 49 times 10minus8
2c Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats + β5Sexn = 247
0609 lt22 times 10minus16 Intercept β0 149 069 217 0031
Log(ePAL) β1 030 028 106 0292
Ages β2 minus005 001 minus392 12 times 10minus4
Log(ePAL) times Ages β3 002 001 416 45 times 10minus5
Variant repeats β4 minus039 007 minus567 41 times 10minus8
Sex β5 minus002 004 minus071 0481
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e7
Table 3 Regression models of the determinants of progressive phenotypes
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Muscle impairment rating scale L 247 032 3 times 10minus19 minus006 008 minus01 092
6-min walk test distance (m) H 246 031 2 times 10minus18 289 057 minus627 056
Physical activity (most active 5-h) H 198 025 9 times 10minus12 minus111 5 times 10minus9 minus600 5 times 10minus11
Physical activity (mean) H 198 025 4 times 10minus10 minus010 087 minus164 023
Trail making testmdashA L 234 024 5 times 10minus12 314 020 976 006
Trail making testmdashB L 242 023 2 times 10minus14 082 2 times 10minus15 224 3 times 10minus6
DM1-Activ-c H 246 023 3 times 10minus13 043 057 minus33 084
Log (Stroop interference score) L 238 021 3 times 10minus12 002 3 times 10minus12 07 2 times 10minus5
Adult social behavioural questionnaire L 201 011 00002 099 017 315 003
Apathy evaluation scalemdashclinician score L 241 010 5 times 10minus5 045 038 200 007
Fatigue and daytime sleepiness scale L 242 009 3 times 10minus5 104 004 156 015
Myotonic dystrophy health index L 245 009 3 times 10minus5 043 2 times 10minus5 177 00003
Self-efficacy scale 28 for fatigue H 241 007 00002 minus004 002 minus24 0002
Van Sonderen social supportmdashdiscrepancies L 196 005 001 022 002 97 004
Illness cognition questionnaire H 237 004 002 017 045 35 047
Van Sonderen social supportmdashinteractions H 216 004 002 minus020 006 minus107 009
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
L 245 004 003 minus356 007 minus632 013
Checklist individual strengthmdashfatigue subscale L 247 003 001 007 004
Sickness impact profile L 156 003 002 786 002
McGill pain score L 233 003 002 154 003
Jacobsen fatigue catastrophizing scale L 241 002 003 009 006 54 001
Apathy evaluation scalemdashinformant version L 99 002 032
Beck depression inventorymdashfast screen L 243 001 018 016 036 38 031
Continued
e8
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

investigate genotypendashphenotype relationships As expected252640
ePAL was a major modifier of age at onset (figure 2A and table 1model 1a r2 = 0178 p = 31 times 10minus11) The presence of variantrepeats was also highly significantly (p = 22 times 10minus5) associatedwith a later age at onset (figure 2A and table 1 model 1b r2 =0240 p= 34 times 10minus14) In order to better quantify these effects wecalculated the age at onset predicted by ePAL alone (ie model1a) and compared this to the observed age at onset The meandifference in age at onset between individuals with and withoutvariant repeatswas 132 years (95CI 57 to 207 2-tailed t test t=minus37 p = 00019 figure 2B) Recently it has been reported thatthere are substantial sex-dependent differences in the relative in-cidence and severity of some aspects of DM141 Similarly werecently reported some evidence for sex-dependent genotypendashphenotype correlations in age at onset although these appeared tobe driven largely by an excess of mildly affected transmittinggrandfathers40 Here sex was revealed as having a marginally
significant effect (p = 0015) on age at onset (table 1 model 1cr2 = 0257 p = 12 times 10minus14)
Determinants of somatic instability in theOPTIMISTIC cohortWe defined the degree of somatic instability as the differencebetween ePAL and the modal allele at recruitment (time pointV2) As expected2540 the major determinants of the degree ofsomatic instability were ePAL (figure 2C) age at samplingand an interaction between them (table 2 model 2a r2 =0560 p lt 22 times 10minus16) Previously we also demonstrated inone family that the presence of variant repeats reduced thedegree of somatic instability31 Likewise here the presence orabsence of variant repeats (figure 2C) was revealed as a highlysignificant (p = 49 times 10minus8) additional measure in the re-gressionmodel (table 2 model 2b r2 = 0610 p lt 22 times 10minus16)In contrast sex of the participant (p = 048) was found not to
Table 1 Age at onset regression models
Model Adjusted r2 p Value Measure CoefficientStandarderror t Statistic p Value
1a Ageo = β0 + β1Log(ePAL) n = 222 0178 31 times 10minus11 Intercept β0 803 79 102 lt2 times 10minus16
Log(ePAL) β1 minus234 33 minus70 31 times 10minus11
1b Ageo = β0 + β1Log(ePAL) +β2Variant repeats n = 222
0240 34 times 10minus14 Intercept β0 866 77 112 lt2 times 10minus16
Log(ePAL) β1 minus265 33 minus80 55 times 10minus14
Variant repeatsβ2 138 32 43 22 times 10minus5
1c Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex n = 222
0257 13 times 10minus14 Intercept β0 856 77 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 14 times 10minus14
Variant repeatsβ2 146 32 46 70 times 10minus6
Sex β3 38 16 24 0015
1d Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) n = 222
0260 29 times 10minus14 Intercept β0 857 76 112 lt2 times 10minus16
Log(ePAL) β1 minus270 33 minus83 12 times 10minus14
Variant repeatsβ2 145 32 46 82 times 10minus6
Sex β3 38 16 24 0017
Standardizedresiduals (SI) β4
minus10 08 minus13 0186
1e Ageo = β0 + β1Log(ePAL) +β2Variant repeats + β3Sex +β4Standardised residuals (SImodel 2b) + β4Standardisedresiduals (SI model 2b) timesLog(ePAL) n = 222
0304 lt22 times 10minus16 Intercept β0 1040 88 118 lt2 times 10minus16
Log(ePAL) β1 minus348 38 minus92 lt2 times 10minus16
Variant repeatsβ2 166 31 53 27 times 10minus7
Sex β3 36 15 23 0020
Standardizedresiduals (SI) β4
250 68 37 29 times 10minus4
Standardizedresiduals (SI) timeslog(ePAL) β5
minus113 29 minus39 15 times 10minus4
Abbreviations Ageo = age at onset SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model The coefficient (β) provides anindication of the relative weight of the contribution of eachmeasure to themodel and its associated standard error The t statistic and corresponding p valueprovide an indication of the statistical significance that the measure is adding explanatory power to the model
e6 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
improve the regression model (table 2 model 2c r2 = 0609p lt 22 times 10minus16)
The role of somatic instability on age at onsetin the OPTIMISTIC cohortAs longer inherited allele lengths precipitate an earlier age at onsetin DM1 and as somatic instability is highly biased toward expan-sions it seems logical to expect that individual-specific differencesin the rate of expansion should modify age at onset Indeed wepreviously established evidence for such an effect in amixed cohortof patients with DM1 from Scotland the United States and CostaRica25 and confirmed this effect in a largeCosta Rican cohort40 IntheOPTIMISTIC cohort incorporating the standardized residualsof somatic instability derived from model 2b into the age at onsetmodel (table 1 model 1d r2 = 0260 p = 30 times 10minus14) improvedthe r2 value slightly from model 1c but the standardized residualsof somatic instability did not reach statistical significance asameasure (p= 019)However when the standardized residuals ofsomatic instability were included with an interaction with ePALthemodel was improved further (table 1 model 1e r2 = 0304 p lt22 times 10minus16) and both the standardized residuals of somatic in-stability alone (p = 29 times 10minus4) and the interaction with ePAL (p =15 times 10minus4) were revealed as highly significant measures
Genetic correlations with progressivephenotypes in the OPTIMISTIC cohortAs part of the OPTIMISTIC protocol several DM1 pheno-types were also quantified at baseline using a variety of direct
and indirect (ie questionnaires) assessment tools27 To in-vestigate the genotypendashphenotype relationships of theseprogressive phenotypes we applied a model selection processincorporating ePAL residual variation in somatic instabilityvariant repeats sex and age at baseline and interactions be-tween ePAL residual variation in somatic instability and ageat baseline (table 3) Highly significant associations with effectsizes comparable to those observed with age at onset wererevealed for many measures (table 3 and figure 3) includingthe Muscle Impairment Rating Scale (MIRS r2 = 032 p = 26times 10minus19) the OPTIMISTIC primary outcome the DM1-Activ-c score (r2 = 023 p = 29 times 10minus13) and key secondaryoutcomes such as the 6-MinuteWalk Test (6-MWT r2 = 031p = 23 times 10minus18) physical activity (accelerometry mean r2 =025 p = 39 times 10minus10 and most active 5-hour r2 = 025 p = 89times 10minus12) the Trail-Making Test (TMT-A r2 = 023 p = 22 times10minus14 and TMT-B r2 = 024 p = 45 times 10minus12) and the Stroopinterference score (r2 = 021 p = 28 times 10minus12) Moderateassociations were observed for the Adult Social BehaviorQuestionnaire (ASBQ r2 = 011 p = 16 times 10minus4) the ApathyEvaluation ScalendashClinician Version (r2 = 010 p = 51 times 10minus5)the Fatigue and Daytime Sleepiness Scale (FDSS) (r2 = 009p = 29 times 10minus5) the Myotonic Dystrophy Health Index totalscore (r2 = 009 p = 34 times 10minus5) and Self-EfficacyndashScale 28 forFatigue (r2 = 007 p = 22 times 10minus4) Only weak or statisticallynonsignificant associations were observed for a number ofmeasures including for van Sonderen Social Support List(SSL) (SSLmdashDiscrepancies [SSL-D] SSLmdashInteractions
Table 2 Regression models of the determinants of the degree of SI
Model Adjusted r2 p Value Measures CoefficientStandarderror t Statistic p Value
2a Log(SI) = β0 + β1Log(ePAL) +β2Ages +β3Log(ePAL) times Agesn = 247
0560 lt22 times 10minus16 Intercept β0 172 073 237 0019
Log(ePAL) β1 020 030 066 0509
Ages β2 minus005 001 minus373 24 times 10minus4
Log(ePAL) times Ages β3 002 001 390 13 times 10minus4
2b Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats n = 247
0610 lt22 times 10minus16 Intercept β0 150 069 219 0029
Log(ePAL) β1 029 028 103 0304
Ages β2 minus005 001 minus394 11 times 10minus4
Log(ePAL) times Ages β3 002 001 417 42 times 10minus5
Variant repeats β4 minus039 007 minus563 49 times 10minus8
2c Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats + β5Sexn = 247
0609 lt22 times 10minus16 Intercept β0 149 069 217 0031
Log(ePAL) β1 030 028 106 0292
Ages β2 minus005 001 minus392 12 times 10minus4
Log(ePAL) times Ages β3 002 001 416 45 times 10minus5
Variant repeats β4 minus039 007 minus567 41 times 10minus8
Sex β5 minus002 004 minus071 0481
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e7
Table 3 Regression models of the determinants of progressive phenotypes
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Muscle impairment rating scale L 247 032 3 times 10minus19 minus006 008 minus01 092
6-min walk test distance (m) H 246 031 2 times 10minus18 289 057 minus627 056
Physical activity (most active 5-h) H 198 025 9 times 10minus12 minus111 5 times 10minus9 minus600 5 times 10minus11
Physical activity (mean) H 198 025 4 times 10minus10 minus010 087 minus164 023
Trail making testmdashA L 234 024 5 times 10minus12 314 020 976 006
Trail making testmdashB L 242 023 2 times 10minus14 082 2 times 10minus15 224 3 times 10minus6
DM1-Activ-c H 246 023 3 times 10minus13 043 057 minus33 084
Log (Stroop interference score) L 238 021 3 times 10minus12 002 3 times 10minus12 07 2 times 10minus5
Adult social behavioural questionnaire L 201 011 00002 099 017 315 003
Apathy evaluation scalemdashclinician score L 241 010 5 times 10minus5 045 038 200 007
Fatigue and daytime sleepiness scale L 242 009 3 times 10minus5 104 004 156 015
Myotonic dystrophy health index L 245 009 3 times 10minus5 043 2 times 10minus5 177 00003
Self-efficacy scale 28 for fatigue H 241 007 00002 minus004 002 minus24 0002
Van Sonderen social supportmdashdiscrepancies L 196 005 001 022 002 97 004
Illness cognition questionnaire H 237 004 002 017 045 35 047
Van Sonderen social supportmdashinteractions H 216 004 002 minus020 006 minus107 009
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
L 245 004 003 minus356 007 minus632 013
Checklist individual strengthmdashfatigue subscale L 247 003 001 007 004
Sickness impact profile L 156 003 002 786 002
McGill pain score L 233 003 002 154 003
Jacobsen fatigue catastrophizing scale L 241 002 003 009 006 54 001
Apathy evaluation scalemdashinformant version L 99 002 032
Beck depression inventorymdashfast screen L 243 001 018 016 036 38 031
Continued
e8
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

improve the regression model (table 2 model 2c r2 = 0609p lt 22 times 10minus16)
The role of somatic instability on age at onsetin the OPTIMISTIC cohortAs longer inherited allele lengths precipitate an earlier age at onsetin DM1 and as somatic instability is highly biased toward expan-sions it seems logical to expect that individual-specific differencesin the rate of expansion should modify age at onset Indeed wepreviously established evidence for such an effect in amixed cohortof patients with DM1 from Scotland the United States and CostaRica25 and confirmed this effect in a largeCosta Rican cohort40 IntheOPTIMISTIC cohort incorporating the standardized residualsof somatic instability derived from model 2b into the age at onsetmodel (table 1 model 1d r2 = 0260 p = 30 times 10minus14) improvedthe r2 value slightly from model 1c but the standardized residualsof somatic instability did not reach statistical significance asameasure (p= 019)However when the standardized residuals ofsomatic instability were included with an interaction with ePALthemodel was improved further (table 1 model 1e r2 = 0304 p lt22 times 10minus16) and both the standardized residuals of somatic in-stability alone (p = 29 times 10minus4) and the interaction with ePAL (p =15 times 10minus4) were revealed as highly significant measures
Genetic correlations with progressivephenotypes in the OPTIMISTIC cohortAs part of the OPTIMISTIC protocol several DM1 pheno-types were also quantified at baseline using a variety of direct
and indirect (ie questionnaires) assessment tools27 To in-vestigate the genotypendashphenotype relationships of theseprogressive phenotypes we applied a model selection processincorporating ePAL residual variation in somatic instabilityvariant repeats sex and age at baseline and interactions be-tween ePAL residual variation in somatic instability and ageat baseline (table 3) Highly significant associations with effectsizes comparable to those observed with age at onset wererevealed for many measures (table 3 and figure 3) includingthe Muscle Impairment Rating Scale (MIRS r2 = 032 p = 26times 10minus19) the OPTIMISTIC primary outcome the DM1-Activ-c score (r2 = 023 p = 29 times 10minus13) and key secondaryoutcomes such as the 6-MinuteWalk Test (6-MWT r2 = 031p = 23 times 10minus18) physical activity (accelerometry mean r2 =025 p = 39 times 10minus10 and most active 5-hour r2 = 025 p = 89times 10minus12) the Trail-Making Test (TMT-A r2 = 023 p = 22 times10minus14 and TMT-B r2 = 024 p = 45 times 10minus12) and the Stroopinterference score (r2 = 021 p = 28 times 10minus12) Moderateassociations were observed for the Adult Social BehaviorQuestionnaire (ASBQ r2 = 011 p = 16 times 10minus4) the ApathyEvaluation ScalendashClinician Version (r2 = 010 p = 51 times 10minus5)the Fatigue and Daytime Sleepiness Scale (FDSS) (r2 = 009p = 29 times 10minus5) the Myotonic Dystrophy Health Index totalscore (r2 = 009 p = 34 times 10minus5) and Self-EfficacyndashScale 28 forFatigue (r2 = 007 p = 22 times 10minus4) Only weak or statisticallynonsignificant associations were observed for a number ofmeasures including for van Sonderen Social Support List(SSL) (SSLmdashDiscrepancies [SSL-D] SSLmdashInteractions
Table 2 Regression models of the determinants of the degree of SI
Model Adjusted r2 p Value Measures CoefficientStandarderror t Statistic p Value
2a Log(SI) = β0 + β1Log(ePAL) +β2Ages +β3Log(ePAL) times Agesn = 247
0560 lt22 times 10minus16 Intercept β0 172 073 237 0019
Log(ePAL) β1 020 030 066 0509
Ages β2 minus005 001 minus373 24 times 10minus4
Log(ePAL) times Ages β3 002 001 390 13 times 10minus4
2b Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats n = 247
0610 lt22 times 10minus16 Intercept β0 150 069 219 0029
Log(ePAL) β1 029 028 103 0304
Ages β2 minus005 001 minus394 11 times 10minus4
Log(ePAL) times Ages β3 002 001 417 42 times 10minus5
Variant repeats β4 minus039 007 minus563 49 times 10minus8
2c Log(SI) = β0 + β1Log(ePAL) +β2Ages + β3Log(ePAL) times Ages+ β4VariantRepeats + β5Sexn = 247
0609 lt22 times 10minus16 Intercept β0 149 069 217 0031
Log(ePAL) β1 030 028 106 0292
Ages β2 minus005 001 minus392 12 times 10minus4
Log(ePAL) times Ages β3 002 001 416 45 times 10minus5
Variant repeats β4 minus039 007 minus567 41 times 10minus8
Sex β5 minus002 004 minus071 0481
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each model andthe coefficient (β) standard error t statistic and statistical significance (p) associated with each measure in the model
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e7
Table 3 Regression models of the determinants of progressive phenotypes
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Muscle impairment rating scale L 247 032 3 times 10minus19 minus006 008 minus01 092
6-min walk test distance (m) H 246 031 2 times 10minus18 289 057 minus627 056
Physical activity (most active 5-h) H 198 025 9 times 10minus12 minus111 5 times 10minus9 minus600 5 times 10minus11
Physical activity (mean) H 198 025 4 times 10minus10 minus010 087 minus164 023
Trail making testmdashA L 234 024 5 times 10minus12 314 020 976 006
Trail making testmdashB L 242 023 2 times 10minus14 082 2 times 10minus15 224 3 times 10minus6
DM1-Activ-c H 246 023 3 times 10minus13 043 057 minus33 084
Log (Stroop interference score) L 238 021 3 times 10minus12 002 3 times 10minus12 07 2 times 10minus5
Adult social behavioural questionnaire L 201 011 00002 099 017 315 003
Apathy evaluation scalemdashclinician score L 241 010 5 times 10minus5 045 038 200 007
Fatigue and daytime sleepiness scale L 242 009 3 times 10minus5 104 004 156 015
Myotonic dystrophy health index L 245 009 3 times 10minus5 043 2 times 10minus5 177 00003
Self-efficacy scale 28 for fatigue H 241 007 00002 minus004 002 minus24 0002
Van Sonderen social supportmdashdiscrepancies L 196 005 001 022 002 97 004
Illness cognition questionnaire H 237 004 002 017 045 35 047
Van Sonderen social supportmdashinteractions H 216 004 002 minus020 006 minus107 009
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
L 245 004 003 minus356 007 minus632 013
Checklist individual strengthmdashfatigue subscale L 247 003 001 007 004
Sickness impact profile L 156 003 002 786 002
McGill pain score L 233 003 002 154 003
Jacobsen fatigue catastrophizing scale L 241 002 003 009 006 54 001
Apathy evaluation scalemdashinformant version L 99 002 032
Beck depression inventorymdashfast screen L 243 001 018 016 036 38 031
Continued
e8
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

Table 3 Regression models of the determinants of progressive phenotypes
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Muscle impairment rating scale L 247 032 3 times 10minus19 minus006 008 minus01 092
6-min walk test distance (m) H 246 031 2 times 10minus18 289 057 minus627 056
Physical activity (most active 5-h) H 198 025 9 times 10minus12 minus111 5 times 10minus9 minus600 5 times 10minus11
Physical activity (mean) H 198 025 4 times 10minus10 minus010 087 minus164 023
Trail making testmdashA L 234 024 5 times 10minus12 314 020 976 006
Trail making testmdashB L 242 023 2 times 10minus14 082 2 times 10minus15 224 3 times 10minus6
DM1-Activ-c H 246 023 3 times 10minus13 043 057 minus33 084
Log (Stroop interference score) L 238 021 3 times 10minus12 002 3 times 10minus12 07 2 times 10minus5
Adult social behavioural questionnaire L 201 011 00002 099 017 315 003
Apathy evaluation scalemdashclinician score L 241 010 5 times 10minus5 045 038 200 007
Fatigue and daytime sleepiness scale L 242 009 3 times 10minus5 104 004 156 015
Myotonic dystrophy health index L 245 009 3 times 10minus5 043 2 times 10minus5 177 00003
Self-efficacy scale 28 for fatigue H 241 007 00002 minus004 002 minus24 0002
Van Sonderen social supportmdashdiscrepancies L 196 005 001 022 002 97 004
Illness cognition questionnaire H 237 004 002 017 045 35 047
Van Sonderen social supportmdashinteractions H 216 004 002 minus020 006 minus107 009
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
L 245 004 003 minus356 007 minus632 013
Checklist individual strengthmdashfatigue subscale L 247 003 001 007 004
Sickness impact profile L 156 003 002 786 002
McGill pain score L 233 003 002 154 003
Jacobsen fatigue catastrophizing scale L 241 002 003 009 006 54 001
Apathy evaluation scalemdashinformant version L 99 002 032
Beck depression inventorymdashfast screen L 243 001 018 016 036 38 031
Continued
e8
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable Direction
Overall model
Parameter
Age Log(ePAL)
n r2 p Value β p Value β p Value
Illness management questionnaire L 241 001 028 044 042 111 033
Van Sonderen social supportmdashnegative interactions L 218 000 035 14 022
Physical activity (least active 5-hour) L 198 minus002 082
Caregiver strain index L 98 minus007 098
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Muscle impairment rating scale 03 2 times 10minus8 minus08 6 times 10minus5 004 002
6-min walk test distance (m) minus252 00001 1152 1 times 10minus5 519 00001 minus324 013
Physical activity (most active 5-h) minus43 003 222 0003 90 002
Physical activity (mean) 336 012 96 0001 22 013 minus014 060 minus145 012 minus064 014 026 017
Trail making testmdashA minus1588 006 minus302 0007 minus045 066 714 005 293 009 minus132 008
Trail making testmdashB minus89 004
DM1-Activ-c minus16 010 124 0001 minus048 014
Log (Stroop interference score) minus05 0001
Adult social behavioural questionnaire minus885 00004 minus56 007 44 0007 minus040 019 370 00007 188 0001 minus080 0001
Apathy evaluation scalemdashclinician score minus468 0009 minus70 0002 minus015 049 225 0004 081 002 minus039 001
Fatigue and daytime sleepiness scale minus65 001 minus37 0005 minus036 009
Myotonic dystrophy health index 17 010 minus66 011
Self-efficacy scale 28 for fatigue minus05 001 08 002
Van Sonderen social supportmdashdiscrepancies minus61 008 36 008
Illness cognition questionnaire 167 004 14 0007 minus008 044 minus75 003 minus033 004 015 004
Van Sonderen social supportmdashinteractions 219 003 62 015 minus56 001 minus96 003
Continued
Neurolo
gyorgN
Neurology
|Volum
e93N
umber
10|
Septem
ber32019
e9
Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

Table 3 Regression models of the determinants of progressive phenotypes (continued)
Dependent variable
Standardizedresiduals (SImodel 2b) Variant repeats Sex (Male) Log(ePAL) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b)
Standardizedresiduals (SImodel 2b) times Age
Log(ePAL) timesStandardizedresiduals (SImodel 2b) timesAge
β p Value β p Value β p Value β p Value β p Value β p Value β p Value
Individualised neuromuscular quality of lifequestionnairemdashsubscale quality of life
901 019 178 004 minus42 016 minus226 010 107 008
Checklist individual strengthmdashfatigue subscale minus40 001 009 0006
Sickness impact profile
McGill pain score minus65 006
Jacobsen fatigue catastrophizing scale
Apathy evaluation scalemdashinformant version
Beck depression inventorymdashfast screen minus171 0007 minus006 042 76 0005 029 002 minus013 002
Illness management questionnaire minus256 017 minus018 044 115 015 064 009 minus029 008
Van Sonderen social supportmdashnegativeinteractions
minus36 010 16 009
Physical activity (least active 5-hour)
Caregiver strain index
Abbreviation SI = somatic instabilityThe table shows the number of observations (n) adjusted squared coefficient of correlation (adjusted r2) and statistical significance (p) for each overall model for each dependent variable (phenotype) and the coefficient (β)and statistical significance (p) associated with eachmeasure in themodel and their interactions (times) The direction indicates whether a higher (H) or lower (L) score for the phenotype represents a better (ie ldquohealthierrdquo) result forthe individual Note that the blank cells correspond to independent variables that were rejected by the model selection procedure as their inclusion did not significantly improve the overall regression model for the givenphenotype
e10
Neurology
|Vo
lume93N
umber
10|
Septem
ber
32019NeurologyorgN
[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

[SSL-I] and SSLmdashNegative Interactions [SSL-N]) CIS-Fatigue the McGill Pain Questionnaire the Sickness ImpactProfile and the Beck Depression Inventorymdashfast screen(BDI-fs) all r2 lt 005 p gt 001 and n gt 150 (table 3) For all
of the highly associated measures (r2 gt 015) age ePAL andpresence of variant repeats were revealed as important ex-planatory variables (table 3) The relative degree of somaticmosaicism was also an important explanatory variable for all
Figure 3 Estimated progenitor allele length (ePAL) and variant repeat correlations with age-dependent phenotypes
The scatterplots show the relationship between ePAL and a number of age-dependent phenotypes The relevant line of best fit under a logarithmic model(dependent variable = β0 + β1Log[ePAL]) for female individuals (circles orange line) male individuals (squares lavender line) and sex-averaged for allindividuals (black line) are shown Individuals with (blue) and without (red) AciI-sensitive variant repeats are also depicted along with the logarithmicregression line for AciI-sensitive variant repeat carriers (blue line)
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e11
bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

bar the Stroop interference score and TMT-A Sex was also animportant modifier for the 6-MWT and physical activity(accelerometry mean and most active 5-hour) (table 3)
DiscussionWe analyzed the length and dynamics of the disease-causingCTG repeat expansion in the DMPK gene to reveal the pri-mary genetic determinants of symptomatic variation in theOPTIMISTIC cohort As expected we were able to establishePAL as a major determinant of self-reported age at onset (table1 model 1a) However it is notable that the proportion ofvariance in age at onset explained by ePAL (r2 = 0178) wasmuch lower than observed in previous studies (eg r2 = 0640 inMorales et al25) This is attributable to the eligibility constraintsfor recruitment to OPTIMISTIC that dictated that participantsmust be aged at least 18 years have severe fatigue (CIS-Fatigueseverity score ge35) but nonetheless retain the ability to walkindependently and be able to provide informed consent and bemotivated to undergo CBT Thus OPTIMISTIC has fewervery mildly affected participants with small expansions andfewer severely affected patients with very large DM1 expansions(figure 2D) Selection of moderately affected patients is likely tobe a common feature of many of the early DM1 trials sug-gesting that the genetic characteristics and phenotypic rela-tionships of the OPTIMISTIC cohort will likely berepresentative of other DM1 trial cohorts Although age at onsetis an important aspect of the disease phenotype it is somewhatsubjective in its assessment as it may depend on patient recallpatient knowledge and relative cognition and insight42 More-over age at onset is unlikely in the near term to be an outcomemeasure in clinical trials We have also revealed that ePAL is animportant contributor to multiple age-dependent phenotypesthat were also assessed as part of the OPTIMISTIC protocolincluding key measures of muscle function and activity such asthe MIRS 6MWT DM1-Activ-c and accelerometry data andkey CNS phenotypes such as the TMT and Stroop test Incontrast other phenotypes such as SSL-DIN CIS-FatigueMcGill pain and BDI-fs were not well-explained by geneticfactors It seems reasonable to assume that in general symp-toms that are strongly associated with the causative mutation inDM1 are most directly linked to the underlying disease processand may be the most responsive to therapeutic interventionstargeting the underlying pathology It is also possible that someof the more subjective self-reported measures may also becompromised by reduced patient insight42 further confound-ing genotype to phenotype associations
For many years it was assumed that expanded alleles at theDMPK locus comprised pure CTG repeat arrays However ithas become apparent that a subset of DM1 expansions con-tains variant repeats3135374344 Previous estimates for thefrequency of such variants in unselected DM1 cohorts varyfrom 3 to 53135ndash37 Here we determined the overallfrequency of variant repeats as 84 of the total cohort (21250) In the Nijmegen subcohort the frequency of variants
was 136 (966 95 CI 68ndash248) while in the Parissubcohort it was only 45 (367 95 CI 12ndash134)Although there was 1 pair of siblings from Nijmegen whoshared variant repeats none of the other participants fromNijmegen with variant repeat containing expanded alleleswere known to be related to each other Thus chance sam-pling of one or a few large families segregating variant repeatalleles does not explain the higher frequency of variant repeatalleles observed in the Nijmegen subcohort While it is pos-sible that this may reflect some sort of site-specific recruitmentbias this difference was not statistically significant and maysimply represent random sampling error Regardless thepresence of variant repeats clearly influences disease severitywith individuals carrying such alleles having an age at onsetdelayed by an average of 13 years relative to that predictedusing the 1a regression model It is possible that the reduceddisease severity observed inDM1 carriers of repeat alleles led totheir overselection in OPTIMISTIC conceivably mediated bya reduced neuropsychological effect of the disease and highermotivation among this subcohort In addition to modifying ageat onset these data also reveal the protective effect of variantrepeats on many of the progressive phenotypes likely to beoutcomes in clinical trials If variant repeat carriers are over-recruited this may reduce sensitivity to correctly evaluate ef-ficacy of a therapeutic intervention in a clinical trial Theseconsiderations suggest that testing for the presence of variantrepeats should be included in DM1 trial design
Recently it has been demonstrated that the absolute frequencyand severity of different aspects of the complex DM1 phenotypeare differentially expressed in male and female patients41 Simi-larly we have presented preliminary evidence that suggest theremay also be subtle repeat-length-independent sex effects on ageat onset40 Here we also observed a marginally significant sexeffect (p = 0015) when including sex as a measure in the age atonset model (table 1 model 1c) However the direction of thiseffect was the opposite to that previously observed Theseobservations suggest sex has only a subtle effect on overall age atonset Nonetheless sex was revealed as an important cofactor forsome phenotypes such as the 6MWT the ASBQ and the FDSS(table 3) and should be considered as an important factor inclinical trials
We recently demonstrated that residual variation in somaticinstability not accounted for by age at sampling and ePAL wasinversely correlated with residual variation in age at onset notaccounted for by ePAL ie patients in whom the repeatexpands more rapidly in the soma have earlier ages at onsetthan expected2540 Here we have used SP-PCR to calculatethe modal length change during the lifetime of the patient asa measure of somatic instability and shown variation in thismeasure is explained by the expected measures ie ePAL ageat sampling and a strong interaction between them (table 2model 2a) In addition we have confirmed that somatic in-stability is reduced by the presence of variant repeats We havealso provided additional evidence that somatic mutationaldynamics directly modify disease severity with residual
e12 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

variation in somatic instability accounting for approximately47 of the total variation in age at onset and detectablycontributing to many age-dependent phenotypes and con-firming somatic expansion as an important therapeutic target
Traditionally DM1 is diagnosed using Southern blot hybrid-ization of restriction digested genomic DNA The low pre-dictive value of this measure and additional complicationsmediated by a failure to fully consider the effects of age-dependent somatic expansion on interpreting intergenerationallength changes prompted the International Myotonic Dystro-phy Consortium to recommend that families not be offeredpredictive phenotypic information based on the number ofCTG repeats12 While this recommendation is not universallyobserved this suggestion coupled with the technical challengesof Southern blot hybridizations and the availability of a simpleyesno RP-PCR test39 has led to a situation where many di-agnostic laboratories do not even attempt to measure thenumber of CTG repeats For example within the OPTIMIS-TIC cohort a diagnostic CTG repeat length was available foronly 121 out of 255 participants As expected the predictivevalue of this measure was relatively low the diagnostic CTGlength measure accounting for only 12 of the variation in ageat onset (figure 2E n = 103 r2 = 0123 p = 000014) Thiscontrasts sharply with the30 of variation accounted for byestimating progenitor allele length quantifying somatic mosa-icism and determining the presence or absence of variantrepeats (table 1 model 1e) These data suggest that it may betime to revisit the recommended diagnostic criteria for DM1and the potential value of reporting more informative prog-nostic information to families by estimating progenitor allelelength and testing for the presence of variant repeats
We have defined the genetic characteristics of the DMPKexpansion in the cohort of patients with DM1 recruited to theOPTIMISTIC clinical trial These baseline data have alreadyyielded important insights into genotype to phenotype rela-tionships in DM1 and should provide a route to determiningthe possible effect of genotype on intervention response anda basis for genetic stratification of DM1 trial participants
AcknowledgmentThe authors thank Berit A Adam Josephine McGhieStephanie L Baross Roxanna J Boyd and Stuart S Martin(all University of Glasgow) for acquisition of some of thegenetic data the participants and family members of theOPTIMISTIC cohort colleagues at all 4 clinical recruitmentcenters for collection and transfer of the blood samples andclinical data Mojgan Reza and staff at the Newcastle Biobankfor Research of Neuromuscular Disorders for preparing andshipping the OPTIMISTIC DNA samples the local di-agnostic laboratories for provision of the historical DNAsamples Shaun Treweek (University of Aberdeen) for trialdesign and implementation the Tayside Clinical TrialsUnit for collation and provision of participant data andcolleagues in the DGM group at the University of Glasgow fordiscussions on this work
Study fundingStudy funded by European Unionrsquos Seventh FrameworkProgramme (FP72007-2013) under grant agreement num-ber 305697 (the OPTIMISTIC project) and donations to theDGM group from the Myotonic Dystrophy Support GroupThe funders had no role in the study design data collectionanalysis interpretation of data writing the report or decisionsregarding when to submit publications
DisclosureS Cumming reports no disclosures relevant to the manu-script D Monckton has been a consultant for Biogen Idecand Vertex has received an honorarium from Charles Riverfor delivering a lecture is a consultant for and had a researchcontract with AMO Pharma is on the scientific advisoryboard of the Myotonic Dystrophy Foundation is a medicaladvisor for the Myotonic Dystrophy Support Group andreceived research funding from the European Union and theMyotonic Dystrophy Support Group B Schoser is a memberof the neuromuscular advisory board of Audentes Thera-peutics San Francisco received speaker honoraria fromSanofi Genzyme Biomarin Amicus Therapeutics LupinPharmaceuticals Recordati Pharma and CSL Behring duringthe last 3 years and received an unrestricted research grantfrom Sanofi Genzyme (2016ndash2017) K Okkersen CJimenez-Moreno S Wenninger F Daidj R Littleford HLochmuller and G Gorman report no disclosures relevant tothe manuscript G Bassez reports grants fromAFM-Telethonpersonal fees and other from Lupin Pharmaceuticals non-financial support and other from the Myotonic DystrophyFoundation and nonfinancial support from AMO Pharmaoutside the submitted work B van Engelen reports grantsfrom European Unionrsquos Horizon 2020 research and in-novation programme (Murab) grants from NetherlandsOrganisation for Scientific Research (NWO) grants fromThe Netherlands Organisation for Health Research and De-velopment (ZonMw) grants from Global FSH grants fromPrinses Beatrix Spierfonds grants from Stiching Spieren voorSpieren grants from Association Francaise contre les Myo-pathies and grants from Dutch FSHD Foundation duringthe conduct of the study Go to NeurologyorgN for fulldisclosures
Publication historyReceived by Neurology July 2 2018 Accepted in final formApril 10 2019
Appendix 1 Authors
Name Location Role Contribution
Sarah ACummingPhD
University ofGlasgow
Author andsiteinvestigator
Major role in acquisitionof genetic data analysisand interpretation ofdata critical revision ofmanuscript forintellectual content
Continued
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e13
References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

References1 Harper PS Myotonic Dystrophy London WB Saunders 20012 Aslanidis C Jansen G Amemiya C et al Cloning of the essential myotonic
dystrophy region and mapping of the putative defect Nature 1992355548ndash551
3 Brook JD McCurrach ME Harley HG et al Molecular basis of myotonic dystrophyexpansion of a trinucleotide (CTG) repeat at the 3rsquo end of a transcript encodinga protein kinase family member Cell 199268799ndash808
4 Buxton J Shelbourne P Davies J et al Detection of an unstable fragment ofDNA specific to individuals with myotonic dystrophy Nature 1992355547ndash548
5 Fu YH Pizzuti A Fenwick RG et al An unstable triplet repeat in a gene related tomyotonic muscular dystrophy Science 19922551256ndash1258
6 Harley HG Brook JD Rundle SA et al Expansion of an unstable DNA region andphenotypic variation in myotonic dystrophy Nature 1992355545ndash546
7 MahadevanM Tsilfidis C Sabourin L et al Myotonic dystrophy mutation an unstableCTG repeat in the 3rsquo untranslated region of the gene Science 19922551253ndash1255
8 Harley HG Rundle SA MacMillan JC et al Size of the unstable CTG repeat se-quence in relation to phenotype and parental transmission in myotonic dystrophyAm J Hum Genet 1993521164ndash1174
9 Hunter A Tsilfidis C Mettler G et al The correlation of age of onset with CTGtrinucleotide repeat amplification in myotonic dystrophy J Med Genet 199229774ndash779
10 Redman JB Fenwick RG Fu YH Pizzuti A Caskey CT Relationship between pa-rental trinucleotide GCT repeat length and severity of myotonic dystrophy in off-spring J Am Med Assoc 19932691960ndash1965
11 Salehi LB Bonifazi E Stasio ED et al Risk prediction for clinical phenotype inmyotonic dystrophy type 1 data from 2650 patients Genet Test 20071184ndash90
12 The International Myotonic Dystrophy Consortium Gonzalez I Ohsawa N et alNew nomenclature and DNA testing guidelines for myotonic dystrophy type 1(DM1) Neurology 2000541218ndash1221
13 Ashizawa T Dubel JR Dunne PW et al Anticipation in myotonic dystrophy IIcomplex relationships between clinical findings and structure of the GCT repeatNeurology 1992421877ndash1883
14 Brunner HG Bruggenwirth HT Nillesen W et al Influence of sex of the transmittingparent as well as of parental allele size on the CTG expansion in myotonic dystrophy(DM) Am J Hum Genet 1993531016ndash1023
15 Lavedan C Hofmann-Radvanyi H Shelbourne P et al Myotonic dystrophy size- andsex-dependent dynamics of CTG meiotic instability and somatic mosaicism Am JHum Genet 199352875ndash883
16 Howeler CJ Busch HFM Geraedts JPM Niermeijer MF Staal A Anticipation inmyotonic dystrophy fact or fiction Brain 1989112779ndash797
17 Jansen G Willems P Coerwinkel M et al Gonosomal mosaicism in myotonic dys-trophy patients involvement of mitotic events in (CTG)n variation and selectionagainst extreme expansion in sperm Am J Hum Genet 199454575ndash585
18 Monckton DG Wong LJ Ashizawa T Caskey CT Somatic mosaicism germlineexpansions germline reversions and intergenerational reductions in myotonic dys-trophy males small pool PCR analyses Hum Mol Genet 199541ndash8
19 Wong LJ Ashizawa T Monckton DG Caskey CT Richards CS Somatic heteroge-neity of the CTG repeat in myotonic dystrophy is age and size dependent Am J HumGenet 199556114ndash122
Appendix 1 (continued)
Name Location Role Contribution
CeciliaJimenez-MorenoPhD
NewcastleUniversity
Author andsiteinvestigator
Major role in recruitmentof participants andacquisition of biologicalsamples and clinical datacritical revision ofmanuscript forintellectual content
KeesOkkersenMD
RadboudUniversity
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
StephanWenningerMD
Ludwig-Maximilians-UniversitatMunchen
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FerroudjaDaidj
AssistancePublique-Hopitaux deParis
Author andsiteinvestigator
Major role inrecruitment ofparticipants andacquisition of biologicalsamples and clinicaldata critical revision ofmanuscript forintellectual content
FionaHogarthPhD
University ofDundee
Author andsiteinvestigator
Major role in collation ofclinical data criticalrevision of manuscriptfor intellectual content
RobertaLittlefordPhD
University ofDundee
Author andsiteinvestigator
Major role in studydesign and collation ofclinical data criticalrevision of manuscriptfor intellectual content
GrainneGormanMD PhD
NewcastleUniversity
Author andpartnerlead
Supervision ofrecruitment data andsample acquisition andclinical study designcritical revision ofmanuscript forintellectual content
GuillaumeBassez MD
AssistancePublique-Hopitaux deParis
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
BenediktSchoser MD
Ludwig-Maximilians-UniversitatMunchen
Author andpartnerlead
Supervision ofrecruitment data andsample acquisitionclinical study designcritical revision ofmanuscript forintellectual content
HannsLochmullerMD
NewcastleUniversity
Author andsiteinvestigator
Coordination of DNAsample collectionclinical study designcritical revision ofmanuscript forintellectual content
Appendix 1 (continued)
Name Location Role Contribution
Baziel GMvan EngelenMD PhD
RadboudUniversity
Author andchiefinvestigator
Supervision ofrecruitment data andsample acquisition andthe overall study clinicalstudy design criticalrevision of manuscriptfor intellectual content
Darren GMoncktonPhD
University ofGlasgow
Author andpartnerlead
Genetic study conceptand design studysupervision dataanalysis drafting ofmanuscript criticalrevision of manuscriptfor intellectualcontent
Appendix 2 Coinvestigators
Coinvestigators are listed at linkslwwcomWNLA962
e14 Neurology | Volume 93 Number 10 | September 3 2019 NeurologyorgN
20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

20 Anvret M Ahlberg G Grandell U Hedberg B Johnson K Edstrom L Largerexpansions of the CTG repeat in muscle compared to lymphocytes from patients withmyotonic dystrophy Hum Mol Genet 199321397ndash1400
21 Ashizawa T Dubel JR Harati Y Somatic instability of CTG repeat in myotonicdystrophy Neurology 1993432674ndash2678
22 Thornton CA Johnson K Moxley RT Myotonic dystrophy patients have larger CTGexpansions in skeletal muscle than in leukocytes Ann Neurol 199435104ndash107
23 Ishii S Nishio T Sunohara N et al Small increase in triplet repeat length of cere-bellum from patients with myotonic dystrophy Hum Genet 199698138ndash140
24 Jinnai K Mitani M Futamura N Kawamoto K Funakawa I Itoh K Somatic instabilityof CTG repeats in the cerebellum of myotonic dystrophy type 1 Muscle Nerve 201348105ndash108
25 Morales F Couto JM Higham CF et al Somatic instability of the expanded CTGtriplet repeat in myotonic dystrophy type 1 is a heritable quantitative trait andmodifier of disease severity Hum Mol Genet 2012213558ndash3567
26 Morales F Vasquez M Cuenca P et al Parental age effects but no evidence for anintrauterine effect in the transmission of myotonic dystrophy type 1 Eur J HumGenet201523646ndash653
27 van Engelen B The OPTIMISTIC Consortium Cognitive behaviour therapy plusaerobic exercise training to increase activity in patients with myotonic dystrophy type1 (DM1) compared to usual care (OPTIMISTIC) study protocol for randomisedcontrolled trial Trials 201516224
28 Okkersen K Jimenez-MorenoCWenninger S et al Cognitive behavioural therapy withoptional graded exercise therapy in patients with severe fatigue withmyotonic dystrophytype 1 a multicentre single-blind randomised trial Lancet Neurol 201817671ndash680
29 Reza M Cox D Phillips L et al MRC Centre Neuromuscular Biobank (Newcastleand London) supporting and facilitating rare and neuromuscular disease researchworldwide Neuromuscul Disord 2017271054ndash1064
30 Gomes-Pereira M Bidichandani SI Monckton DG Analysis of unstable triplet repeatsusing small-pool polymerase chain reaction Methods Mol Biol 200427761ndash76
31 Braida C Stefanatos RK Adam B et al Variant CCG and GGC repeats within theCTG expansion dramatically modify mutational dynamics and likely contribute to-ward unusual symptoms in some myotonic dystrophy type 1 patients Hum MolGenet 2010191399ndash1412
32 The R Core Team R A Language and Environment for Statistical Computing ViennaR Foundation for Statistical Computing Available at R-projectorg Accessed January15 2018
33 The RStudio Team RStudio Integrated Development for R Boston RStudio IncAvailable at rstudiocom Accessed August 21 2017
34 Venables WN Ripley BD Modern Applied Statistics with S New York Springer2002495 xi
35 Musova Z Mazanec R Krepelova A et al Highly unstable sequence interruptions of theCTG repeat in themyotonic dystrophy gene Am JMedGenet A 2009149A1365ndash1374
36 Botta A Rossi G Marcaurelio M et al Identification and characterization of 59 CCGinterruptions in complex DMPK expanded alleles Eur J Hum Genet 201725257ndash261
37 SantoroMMasciulloM Pietrobono R et al Molecular clinical andmuscle studies inmyotonic dystrophy type 1 (DM1) associated with novel variant CCG expansionsJ Neurol 20132601245ndash1257
38 Jeffreys AJ MacLeod A Tamaki K Neil DL Monckton DG Minisatellite repeatcoding as a digital approach to DNA typing Nature 1991354204ndash209
39 Warner JP Barron LH Goudie D et al A general method for the detection of largeCAG repeat expansions by fluorescent PCR J Med Genet 1996331022ndash1026
40 Morales F Vasquez M Santamarıa C Cuenca P Corrales E Monckton DG Apolymorphism in the MSH3 mismatch repair gene is associated with the levels ofsomatic instability of the expanded CTG repeat in the blood DNA of myotonicdystrophy type 1 patients DNA Repair 20164057ndash66
41 Dogan C De Antonio M Hamroun D et al Gender as a modifying factor influencingmyotonic dystrophy type 1 phenotype severity and mortality a nationwide multipledatabases cross-sectional observational study PLoS ONE 201611e0148264
42 Baldanzi S Bevilacqua F Lorio R et al Disease awareness in myotonic dystrophy type1 an observational cross-sectional study Orphanet J Rare Dis 20161134
43 Santoro M Fontana L Masciullo M et al Expansion size and presence of CCGCTCCGG sequence interruptions in the expanded CTG array are independentlyassociated to hypermethylation at the DMPK locus in myotonic dystrophy type 1(DM1) Biochim Biophys Acta 201518522645ndash2652
44 Tome S Dandelot E Dogan C et al Unusual association of a unique CAG in-terruption in 5 rsquo of DM1 CTG repeats with intergenerational contractions and lowsomatic mosaicism Hum Mutat 201839970ndash982
NeurologyorgN Neurology | Volume 93 Number 10 | September 3 2019 e15
DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

DOI 101212WNL0000000000008056 published online August 8 2019Neurology
Sarah A Cumming Cecilia Jimenez-Moreno Kees Okkersen et al OPTIMISTIC cohort
Genetic determinants of disease severity in the myotonic dystrophy type 1
This information is current as of August 8 2019
ServicesUpdated Information amp
056fullhttpnneurologyorgcontentearly20190807WNL0000000000008including high resolution figures can be found at
Citations
056fullotherarticleshttpnneurologyorgcontentearly20190807WNL0000000000008This article has been cited by 1 HighWire-hosted articles
Subspecialty Collections
httpnneurologyorgcgicollectiontrinucleotide_repeat_diseasesTrinucleotide repeat diseases
httpnneurologyorgcgicollectionmuscle_diseaseMuscle disease
y_cohort_case_controlhttpnneurologyorgcgicollectionclinical_trials_observational_studClinical trials Observational study (Cohort Case control)following collection(s) This article along with others on similar topics appears in the
Errata
content94104593fullpdf or page
nextAn erratum has been published regarding this article Please see
Permissions amp Licensing
httpwwwneurologyorgaboutabout_the_journalpermissionsits entirety can be found online atInformation about reproducing this article in parts (figurestables) or in
Reprints
httpnneurologyorgsubscribersadvertiseInformation about ordering reprints can be found online
ISSN 0028-3878 Online ISSN 1526-632XWolters Kluwer Health Inc on behalf of the American Academy of Neurology All rights reserved Print1951 it is now a weekly with 48 issues per year Copyright Copyright copy 2019 The Author(s) Published by
reg is the official journal of the American Academy of Neurology Published continuously sinceNeurology
Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

Disputes amp Debates Editorsrsquo ChoiceSteven Galetta MD FAAN Section Editor
Reader response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisVilija G Jokubaitis (Melbourne) and Ruth Dobson (London)
Neurologyreg 202094455ndash456 doi101212WNL0000000000009063
We read with interest the article by Zuluaga et al1 which used the uniquely valuable BarcelonaCIS (clinically isolated syndrome) cohort2 However evolving multiple sclerosis (MS) di-agnostic and treatment landscapes must be taken into account when using this cohort to informcurrent practice
Of those included in the analysis1 47did not have a second clinical attack 39did notmeet theMcDonald 2010 criteria and 32 did not meet the Barkhof criteria for the diagnosis ofMS This
Editorsrsquo note Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisIn the article ldquoMenarche pregnancies and breastfeeding do not modify long-term prog-nosis in multiple sclerosisrdquo Zuluaga et al reported that age at menarche pregnancy beforeor after the diagnosis of clinically isolated syndrome (CIS) and breastfeeding did notsubstantially modify the risk of progressing to clinically definite multiple sclerosis (CDMS)or disability accrual per the Expanded Disability Status Scale (EDSS) in a cohort of 501female participants with CIS In response Drs Jokubaitis and Dobson argued that thepatients with CDMS should be examined separately for the EDSS outcomes becausea substantial proportion of the overall cohort did not have a second clinical attack and didnotmeet either theMcDonald 2010 or Barkhof criteria forMS They seek additional detailsregarding the propensity scorendashmatched score analysis because a smaller number ofmatched pairs could limit the generalizability of the results In addition they noted that theanalyses for the association of pregnancy and breastfeeding on time to EDSS 30 were notadjusted for relapse and that the differences between exclusive breastfeeding and mixedfeeding strategies merit further exploration in prospective studies They also argue that theharmful effects of suspending disease-modifying treatments (DMTs) in those with ag-gressive disease who become pregnant should be considered Responding to these com-ments Drs Tintore et al noted that they built the model for time to EDSS 30 over theCDMS subcohort in addition to providing further details of the propensity scorendashmatchedanalyses They reported additional analyses for the adjusted hazard ratio for pregnancy (butnot for breastfeeding) on considering the annualized relapse rate over the first 3 and 5 yearsof disease and acknowledged that additional details of breastfeeding were unavailableRegarding the problem of suspending DMTs in pregnant patients they noted that they areanalyzing a subgroup of women treated with natalizumab or fingolimod As greaternumbers of young women become eligible for DMTs with more inclusive revisions of theMcDonald criteria neurologists are likely to encounter challenging questions about theassociation of pregnancies and breastfeeding with MS disease activity and the attendantDMT-related dilemmas in their practice
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094455 doi101212WNL0000000000009064
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 455
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

raises questions about cohort baseline heterogeneity because 2 of the primary outcomemeasuresare confirmed Expanded Disability Status Scale (EDSS) 30 or 60 There is an argument in favorof examining the clinically definite multiple sclerosis (CDMS) cohort separately to the non-CDMS cohort
Regarding the propensity score-matched analyses we are interested to know the matchingstrategy used how many matched pairs were included in this analysis the matching ratio themedian follow-up duration and censoring strategy Only 142 respondents had pregnancies aftera CIS1 it is thus possible that fewer than 142 matched pairs were included limiting the gen-eralizability of these results
It appears that the analyses of the impact of pregnancy and breastfeeding on time to EDSS 30were not adjusted for relapse Relapse particularly early in the disease phase and relapse recoveryare among the strongest predictors of future disability accumulation34
Breastfeeding was studied as both a dichotomous variable (breastfeeding vs not) and a time-dependent event1 However exclusive breastfeeding may be protective in a way that mixedfeeding is not5 A truly prospective design is required to address the subtleties of this question
The authors concluded that MS prognosis is not significantly affected by pregnancy once allother variables are considered1 However in the current era of highly active disease-modifyingtreatment (DMT) use pregnancy does not occur in isolation The potentially harmful effects ofsuspending DMT in those with aggressive disease must be taken into account when discussingfamily planning in MS We look forward to future studies to help answer the questions that thisstudy raises which is of prime importance to women with MS
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
2 TintoreM Rovira A Rıo J et al Defining high medium and low impact prognostic factors for developing multiple sclerosis Brain 20151381863ndash1874
3 Bermel RA You X Foulds P et al Predictors of long-term outcome in multiple sclerosis patients treated with interferon β Ann Neurol20137395ndash103
4 Jokubaitis VG Spelman T Kalincik T et al Predictors of long-term disability accrual in relapse-onset multiple sclerosis Ann Neurol20168089ndash100
5 Hellwig K Rockhoff M Herbstritt S et al Exclusive breastfeeding and the effect on postpartum multiple sclerosis relapses JAMANeurol 2015721132ndash1138
Copyright copy 2020 American Academy of Neurology
Author response Menarche pregnancies and breastfeeding do notmodify long-term prognosis in multiple sclerosisMar Tintore (Barcelona Spain) Santiago Perez-Hoyos (Barcelona Spain) and Susana Otero-Romero
(Barcelona Spain)
Neurologyreg 202094456ndash457 doi101212WNL0000000000009065
We thank Drs Jokubaitis and Dobson for the comment on our article1
We built the model for the time to Expanded Disability Status Scale (EDSS) 30 over theclinically definite multiple sclerosis (CDMS) subcohort The adjusted hazard ratio (aHR [CI95]) associated to pregnancy is aHR = 126 CI 95 (062 259)
Regarding the propensity scorendashmatched analyses we decided to perform inverse probability(IP) weighting to create the new pseudocohort to minimize the association between covariatesand pregnancy status Thus no matching was performed but we assigned IP weights to each ofthe patients in the cohort The probability of being pregnant at any time given the set of
456 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

covariates was estimated via a logistic regression adjusted for age at clinically isolated syndrome(CIS) topography of the CIS oligoclonal bands (OB) number of T2 baseline lesions treat-ment status (as time dependent) number of T2 lesions at first year and CDMS (as timedependent)
We totally agree with the issue noted about not adjusting for relapse in the analyses of impact ofpregnancy and breastfeeding on time to EDSS 30 Incorporating relapses in the adjusted modelis key to predict disability The adjusted hazard ratio for pregnancy considering the annualizedrelapse rate over the first 3 years of disease is aHR = 115 CI 95 (056 236) Whencomputing the annualized relapse rate within the first 5 years of disease we obtain an aHR =145 CI 95 (070 302) A further step that we are exploring for this analysis is to includerelapses as a time-varying event with the aim of approaching in a more realistic way the dynamicnature of the disease We also agree that future research must focus on more precise modalitiesof breastfeeding such as mixed or exclusive breastfeeding Unfortunately this information wasmissing in our study1
In the era of high-efficacy drugs suspending disease-modifying treatments may be harmful forpatients with aggressive multiple sclerosis To answer the questions our study raised we are inthe process of independently analyzing a subgroup of pregnant women treated with natalizu-mab or fingolimod
1 Zuluaga MI Otero-Romero S Rovira A et al Menarche pregnancies and breastfeeding do not modify long-term prognosis in multiplesclerosis Neurology 201992e1507ndashe1516
Copyright copy 2020 American Academy of Neurology
Editorsrsquo note Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainIn the article ldquoTeaching NeuroImages A rare case of Jacobsen syndrome with global diffusehypomyelination of brainrdquo Patel et al presented MRI fluid-attenuated inversion recovery(FLAIR) images at 18months and 3 years of age in a boywith Jacobsen syndrome due to an11q23-11q24 deletion The images showed improvement in white matter abnormalitieswhich were termed hypomyelination by the authors In response Wolf et al argued thathypomyelination is a permanentmyelin deficit and is associated with a less hyperintense T2white matter signal than is seen in this patient They noted that the patientrsquos deletionencompasses HEPACAM a gene for which haploinsufficiency is associated with leuko-dystrophy that improves with time They noted that the case is representative of limitationsin extant classifications of leukodystrophies as either hypomyelinating or demyelinatingResponding to these comments Patel et al agreed that HEPACAM loss of function mayaccount for some of the imaging abnormalities in Jacobsen syndrome but noted thatmacrocephaly and cysts (classical findings with HEPACAM mutations) are not typicallyseen in this syndrome They noted that the original neuroradiologist interpretation termedthe findings as global diffuse hypomyelination This exchange highlights current uncer-tainties in the terminology surrounding the white matter abnormalities particularly in thepediatric population
Aravind Ganesh MD DPhil and Steven Galetta MD
Neurologyreg 202094457 doi101212WNL0000000000009066
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 457
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

Reader response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainNicole I Wolf (Amsterdam) and Marjo S van der Knaap (Amsterdam)
Neurologyreg 202094458 doi101212WNL0000000000009070
With interest we read the report by Patel et al1 concerning a patient with Jacobsen syndromedue to an 11q23ndash11q24 deletion and MRI evidence for leukodystrophy with improvement ata follow-up substantiated by FLAIR images The authors claimed that these abnormalitiesrepresent hypomyelination Hypomyelination is defined as a significant and permanent myelindeficit2 Its MRI appearance is characterized by a diffusely hyperintense T2 white matter (WM)signal which is less high than the signal in other leukodystrophies23 and certainly less high thanthe WM signal in the patient discussed here1 who has strongly T2-hyperintense WM signalabnormalities
The chromosomal deletion encompasses HEPACAM Heterozygous and biallelic mutations inthis gene cause megalencephalic leukodystrophy with subcortical cysts (MLC) a vacuolatingleukodystrophy with macrocephaly In dominantHEPACAMmutations the leukodystrophyimproves over time4 In Jacobsen syndromeHEPACAM haploinsufficiency was earlier assumedto cause leukodystrophy5
Why did the authors classify their case as hypomyelination Many neurologists still categorizeleukodystrophies in hypomyelinating and demyelinating disorders3 Perhaps the MRI im-provement not compatible with a demyelinating (progressive) disorder prompted them tolabel this leukodystrophy hypomyelination This case nicely illustrated that not all leukodys-trophies are progressive and that there are more leukodystrophy categories beyond hypo-myelination and demyelination3
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
2 Pouwels PJ Vanderver A Bernard G et al Hypomyelinating leukodystrophies translational research progress and prospects AnnNeurol 2014765ndash19
3 van der KnaapMS Schiffmann RMochel F Wolf NI Diagnosis prognosis and treatment of the leukodystrophies Lancet Neurol 201918962ndash972
4 van der KnaapMS Boor I Estevez R Megalencephalic leukoencephalopathy with subcortical cysts chronic white matter oedema due toa defect in brain ion and water homoeostasis Lancet Neurol 201211973ndash985
5 Yamamoto T Shimada S Shimojima K et al Leukoencephalopathy associated with 11q24 deletion involving the gene encoding hepaticand glial cell adhesion molecule in two patients Eur J Med Genet 201558492ndash496
Copyright copy 2020 American Academy of Neurology
Author response Teaching NeuroImages A rare case of Jacobsensyndrome with global diffuse hypomyelination of brainHimadri Patel (Hershey PA) Ashutosh Kumar (Hershey PA) Gerald Raymond (Hershey PA)
and Gayatra Mainali (Hershey PA)
Neurologyreg 202094458ndash459 doi101212WNL0000000000009069
We thank Drs Wolfe and Van der Knaap for their insightful comment on our TeachingNeuroImages study1 and clarification of their precise definition of hypomyelinatingdisorders We agree that HEPACAM loss of function may account for some of the issuein imaging in Jacobsen syndrome but it does not appear to be the entire explanationgiven the lack of macrocephaly or cysts in most patients reported Regarding the hypo-myelination classification this was derived from the original radiology report interpreted
458 Neurology | Volume 94 Number 10 | March 10 2020 NeurologyorgN
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited
by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited

by the neuroradiologist as a global diffuse hypomyelination with mild diffuse brain atrophyFurther longitudinal studies would certainly be of interest
1 Patel H Kumar A Raymond G Mainali G Teaching NeuroImages a rare case of Jacobsen syndrome with global diffuse hypo-myelination of brain Neurology 201992e1665ndashe1666
Copyright copy 2020 American Academy of Neurology
CORRECTIONS
Clinical and neural responses to cognitive behavioral therapy forfunctional tremorNeurologyreg 202094459 doi101212WNL0000000000008714
In the article ldquoClinical and neural responses to cognitive behavioral therapy for functional tremorrdquoby Espay et al1 the full authorrsquos name should have appeared throughout as W Curt LaFrance JrThe authors regret the error
Reference1 Espay AJ Ries S Maloney T et al Clinical and neural responses to cognitive behavioral therapy for functional tremor Neurology 2019
93e1787ndashe1798
Clinical risk factors in SUDEPAnationwide population-based case-control studyNeurologyreg 202094459 doi101212WNL0000000000009154
In the article ldquoClinical risk factors in SUDEP A nationwide population-based case-controlstudyrdquo by Sveinsson et al1 the bottom box in figure 1 should read ldquon = 255rdquo and the fifth boxdown on the right should read ldquoControlsrdquo The editorial staff regret the errors
Reference1 Sveinsson O Andersson T Mattsson P Carlsson S Tomson T Clinical risk factors in SUDEP a nationwide population-based case-
control study Neurology 202094e419ndashe429
Genetic determinants of disease severity in the myotonic dystrophytype 1 OPTIMISTIC cohortNeurologyreg 202094459 doi101212WNL0000000000008715
In the article ldquoGenetic determinants of disease severity in the myotonic dystrophy type 1OPTIMISTIC cohortrdquo by Cumming et al1 the study funding section should have read ldquoStudyfunded by European Unionrsquos Seventh Framework Programme (FP72007ndash2013) under grantagreement number 305697 (the OPTIMISTIC project) the Wellcome Centre for Mito-chondrial Research (ref 203105Z16Z)) and donations to the DGM group from theMyotonic Dystrophy Support Group The funders had no role in the study design datacollection analysis interpretation of data writing the report or decisions regarding when tosubmit publicationsrdquo The authors regret the error
Reference1 Cumming SA Jimenez-Moreno C Okkersen K et al Genetic determinants of disease severity in the myotonic dystrophy type 1
OPTIMISTIC cohort Neurology 201993e995ndashe1009
NeurologyorgN Neurology | Volume 94 Number 10 | March 10 2020 459
Author disclosures are available upon request (journalneurologyorg)
Copyright copy 2020 American Academy of Neurology Unauthorized reproduction of this article is prohibited