Embed Size (px)
Citation preview

FRR
Testing for thrombophilia: is it ever useful?
F.R. Rosendaal, Leiden
ISTH Educational Course on Thrombosis, Thrombophilia, Thrombolysis and DIC
Moscow, 17-19 September 2014

FRR
Thou art always figuring diseases in me, but thou art full of error: I am sound
(Shakespeare W. Measure for measure 1604; Act I, Scene II)

FRR
Tests through history
• the very first test....

Georgio Giulio Clovio
Book of Hours (1546)
Eve tests Adam
(test of faith/love)

Titian (1550)

Judgement of Paris
(test of beauty)

Roman augur
(test for going to war)

Rice water diarrhoea
(test for cholera)

FRR
Modern tests
• Test for clinical disease (e.g. ECG)• Test for early disease (e.g. Pap smear)• Test for risk of disease (e.g. blood pressure)• Test for fetal disease (e.g., amniocentesis)• Test for risk of fetal disease (e.g. carrier testing)• Test for past infection (e.g. Mantoux)• Test for state (e.g. pregnancy test)
• etc

FRR
Not always happy end
Sistine Chapel
Michelangelo (1512)

FRR
Not always a happy end
.. a thousand ships
(film: Troy, 2004)


FRR
Costs and benefits
• medical benefits (NNT, NNS)• medical costs (side effects)• psychosocial benefits (+ Qol)• psychosocial costs (-QoL)• economical benefits (+ €)• economical costs (- €)

FRR
Testing for thrombophilia
• Factor V Leiden worldwide most performed genetic test
• Often in combination with protein C, protein S, antithrombin, factor VIII, MTHFR 677T and homocysteine

FRR
How many tests are done?
• survey over 4 months via large diagnostic center• 2000 questionnaires to ordering physicians• response 63% (n=1132)
• extrapolation: 15 000 per year– EU: 500 000 per year– USA: 300 000 per year
Population 16 million(Coppens, J Throm Haemost 2007)

FRR
Indications for testing
• Internal Medicine, Vascular Medicine, Hematology, Pulmonology, Cardiology, Surgery, Obstetrics, General Practitioners
VT42%
arterial23%
obstetric17%
family16%
(Coppens J Throm Haemost 2007)
no changes in management in 24%

FRR
Indications for testing
• obstetric
• arterial disease
• venous thrombosis
• weak relation with pregnancy loss• no effective treatment
• weak relation with arterial disease• no specific treatment

FRR
If testing: for what?

FRR
Confirmed genetic risk factors patients (%) pop. (%) RR PAR (%)
AT/PC/PS deficiency 3 <1 >10 1
Factor V Leiden rs6025 19 3 7.9 17
PT 20210A rs1799963 6 2 2.8 3
FGG C10034T rs2066865 12 6 2.4 8
non-00 bloodgroup 71 57 1.8 31
FGB his95arg rs6003 19 14 1.5 7
FXIII leu34val (rec.) rs5985 96 94 1.4 27
PROC A2418G rs1799809 22 19 1.3 5
FGA Thr312Ala rs6050 29 26 1.2 5
FGB 455 G/A rs1800788 26 21 1.3 6
F11 rs2289252 48 41 1.3 13
F5 rs4524 79 73 1.3 19
GP6 rs1613662 84 82 1.2 11
SERPINC1 rs2227589 17 10 1.3 3

FRR
Testing for genetic variants
• To be discussed– deficiencies of protein C, S or antithrombin– factor V Leiden– prothrombin 20210A
• all others too weak effect

FRR
Testing for genetic variants
• Aim– prevent thrombosis (death)
• Method– screening– intensified treatment or removal risk factors
• Target– asymptomatic patients (prevent 1st event)– symptomatic patients (prevent recurrence)

FRR
Major distinction
• unselected individuals– patients, relatives, non-related
• selected patients (familial thrombophilia)– patients, relatives

FRR
Unselected individuals
• screening of asymptomatics– everybody– prior to risk situations (surgery, OCs)
• all• relatives of patients
• testing of symptomatics– prevention of recurrencies
• prolonged anticoagulant treatment• liberal short-term prophylaxis

FRR
Testing for genetic variants
• Aim– prevent thrombosis (death)
• Method– screening– intensified treatment or removal risk factors
• Target– asymptomatic patients (prevent 1st event)– symptomatic patients (prevent recurrence)

FRR
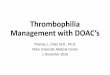
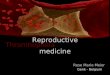
Gene-environment interaction
0
5
10
15
20
25
30
35
neither OC FVL both
(Vandenbroucke, Lancet 1994)
Absolute risks:
Neither 0.5 / 10 000OC 2.0 / 10 000FVL 4.0 / 10 000Both 14 / 10 000
What can be gained
- 10 / 10000 (VT)- 1 / 10000 (death)

FRR
How many to test to prevent one
Risk: 10/10 000
- 1000 with FVL should not take OCs to prevent one VT- 10000 with FVL should not take OCs to prevent one death
How to find 1000 women with factor V Leiden
- Population (5%) : test 20 000- Patients’ relatives
- Patients (20%): test 5 to find one with FVL- Relatives (25-50%): test 2-4 to find one
- to find 1000 women with FVL:- test 10 000 patients and >2000 relatives

FRR
Costs
• whether patients or asymptomatic women• we need to test > 10 000 individuals to prevent one VT• we need to test > 100 000 individuals to prevent one death
• cost per consultation and test: € 150,-
• cost to prevent one VT: 1.5 million euros• cost to prevent one death: 15 million euros

FRR
Screening asymptomatics
• risk reduction too low to render it cost-effective
• not rational
• this includes screening looking for relatives of patients

FRR
Testing for genetic variants
• Aim– prevent thrombosis
• Method– screening– intensified treatment or removal risk factors
• Target– asymptomatic patients (prevent 1st event)– symptomatic patients (prevent recurrence)

FRR
Testing thrombosis patients
• testing of unselected patients
• can only be useful if– patients with positive test have higher
recurrence risk than those without– there are ways to reduce this risk with a positive
risk-benefit ratio (side-effects)

FRR
Testing thrombosis patients
• testing of unselected patients
• can only be useful if– patients with positive test have higher
recurrence risk than those without– there are ways to reduce this risk with a positive
risk-benefit ratio (side-effects)

FRR
Leiden Thrombophilia Study
• 474 consecutive patients with DVT– exclusion: malignancy
• prospective follow-up• mean follow-up 7.3 yr (max 12 yr)• 90 recurrent thrombotic event• event rate 2.6 percent per year
(Christiansen, JAMA 2005)

FRR
No long-term effect thrombophilia
(Christiansen, JAMA 2005)
• abnormalities
PC, PS, AT
FVL, PT20210A
FVIII, FIX, FXI
homocysteine
• HR: 1.4 (CI95: 0.9-2.2)

FRR
Cambridge study
( Baglin, Lancet 2003)
• N=489
• 2 yr follow-up
• anticoagulant defects
PC, PS, AT
FVL, PT20210A
• HR 1.50 (CI95 0.8-2.8)

FRR
Recurrence risk by defect
RR CI95
factor V Leiden 1.2 0.7 - 1.9
prothrombin 20210A 0.7 0.3 - 2.0
PC/PS/AT deficiency 1.8 0.9 - 3.7
high FVIII 1.1 0.7 - 1.8
high FIX 0.9 0.5 - 1.7
high FXI 0.6 0.3 - 1.1
hyperhomocysteinemia 0.9 0.5 - 1.6
(Christiansen, JAMA 2005)

FRR
Conclusion
• Effect of laboratory abnormalities on recurrence small or absent
• Test result does not predict who is at increased risk

FRR
Testing thrombosis patients
• testing of unselected patients
• can only be useful if– patients with positive test have higher
recurrence risk than those without– there are ways to reduce this risk with a positive
risk-benefit ratio (side-effects)

FRR(Agnelli, N Engl J Med 2001)
Prolonged anticoagulation
• idiopathic VT
• N=267
• 3 vs 12 months
• catch-up
• no benefit

FRR
Conclusion
• Effect of laboratory abnormalities on recurrence probably small
• No clear strategy to reduce risk except life-long anticoagulation
– risk of severe hemorrhage 1-2 percent per year

FRR
Real predictors
Relative risk
sex
men vs women 3- to 4-fold
type of first event
idiopathic vs secondary 2- to 3-fold
(Baglin, Lancet 2003; Baglin, JTH 2004; Kyrle, NEJM 2004; Christiansen, JAMA 2005)

FRR
Unselected individuals
• screening asymptomatic individuals– risk reduction too low to render it cost-effective– not rational
• screening symptomatic patients– does not identify those at high risk of recurrence– does not open treatment options– not rational

FRR
Selected individuals

FRR
Familial thrombosis
It is probably more than coincidence when six or more members of the same family each develop from one to five thromboembolic conditions and when most of them eventually die of such conditions (Wright, 1952)
TE TE
TE TE TE
TETE
† †
† †
†
TE: thromboembolism
†: fatal thromboembolism

FRR
Selected individuals
Age at first thrombosis:• consecutive patients with 1st VT (N=378)
– protein C deficiency 47 yr– no defect found 43 yr
• familial thrombophilia (24 families, N=229)– protein C deficiency 35 yr– no defect found 33 yr
(Lensen, Blood 1997)

FRR
EPCOT study
• 9 centres in Europe • all their patients with clear familial thrombophilia• prospective follow-up (1995-2001)• 1626 patients (probands and relatives)• AT/PC/PS deficiency or FVL
(Leiden, Barcelona, Glasgow, Sheffield, Frankfurt, Vienna, Malmö, Bologna, Paris)

FRR
EPCOT: asymptomatic people
• incidence of venous thrombosis (no AC)– 0.8 % per year (CI95 0.5-1.2%)
• majority of events spontaneous• risk not greater than that of anticoagulation
• testing will not affect management
(Vossen, J Thromb Haemost 2005)

FRR
EPCOT: symptomatic patients
• patients with one prior event• divided in those +/- long-term anticoagulation
• incidence of venous thrombosis– long term AC: 1.1 % per year – no AC: 5.3 % per year
• gradient of risk over type of thrombophilia– AT-def: 10.5%/yr (2.7 on AC), FVL: 3.8%/yr (0.0 on AC)
• incidence of major hemorrhage: 0.6%/yr
(Vossen, Arterioscler Thromb Vasc Biol 2005)

FRR
Familial thrombophilia
• asymptomatic people (relatives)– no obvious advantage of screening– no obvious management choices
• symptomatic patients– suggestive of benefit of long-term
anticoagulation (esp. AT-deficiency) – no randomised studies

FRR
Testing for genetic variants
• screening in unselected individuals or patients with thrombosis not indicated
• Screening symptomatic individuals in highly penetrant familial thrombophilia may be indicated – only antithrombin deficiency– no studies that prove positive benefit-risk-ratio

FRR
Testing in selected patients
• Symptomatic patients with familial thrombophilia: very small group

FRR
Experimental evidence
• case-cohort study of patients with recurrent VT
• idea: compare patients with recurrence to those without
• if testing prevents recurrence, more tests in the latter
• 197 patients with recurrent VT during follow-up• 324 patients without recurrence
(Coppens, J Throm Haemost 2008)

FRR
No benefit
% tested OR for recurrent VT (tested vs not-
tested)Recurrent VT (cases)
No recurrent VT (controls)
all 35 30 1.2 (0.8-1.8)
women 41 35 1.4 (0.7-2.9)
First VT with OC use
60 32 3.4 (1.3-8.6)
Positive family history for VT
47 39 1.5 (0.7-3.1)
(Coppens, J Throm Haemost 2008)

FRR
Psychological impact
(Cohn, J Throm Haemost 2008)

FRR
Impact of testing – my e-mails
“I personally have a chronically elevated factor VIII activity (186%, 242%, and 192%), an elevated Factor XI activity (212%), as well as being heterozygous for MTHFR A1298C. …… After researching the literature and finding a sparcity of information reguarding my problem, I believe the only hope for finding advice and guidance in my care is to personally ask the experts leading the research in the field of hypercoagulability. Please attempt to share your wisdom and advice with me.”

FRR
More consultations
“I recently discovered I am heterozygous for Factor II G20210A and Factor V Leiden. I have never had a DVT. …..
I would like to get the best estimate I can of my risk, and how to monitor and reduce it. ……
My daughter was on birth control because she had an ovarian cyst. She has tested positive for Factor II and has stopped birth control—need she do so? Should I have my son tested?...
From the genomics service, the reported risk of a first DVT based on my Factor II and V results is 57% over the next 14 years, ie until I turn 74, and the likelihood increases sharply thereafter with a lifetime estimated risk of 90%. ”

FRR
Conclusion
• our knowledge of genetics has not positively affected clinical care
• testing seems mainly psychotherapeutic• studies in patients inconclusive• studies in physicians not performed

FRR
Conclusion: we test too much!
• Seems natural ‘to want to know’• Wanting to know not always a good idea
(film: Troy, 2004)