Embed Size (px)
Citation preview

Thrombophilia Thrombophilia
Dr Galila ZaherDr Galila Zaher
MRCPathMRCPath
Consultant Consultant HematologistHematologist

ThrombophiliaThrombophilia‘‘A disorder of the haemostatic mechanism A disorder of the haemostatic mechanism
with a predisposition towards thrombosis’with a predisposition towards thrombosis’
BUTBUT Many patients with defects remain Many patients with defects remain asymptomatic despite multiple challengesasymptomatic despite multiple challenges
ANDAND >50% patients with TED will have no >50% patients with TED will have no identifiable laboratory abnormalityidentifiable laboratory abnormality
ANDAND proven thrombophilic defect and a proven thrombophilic defect and a family history of TED are at greater risk of family history of TED are at greater risk of TED than individuals with no family history TED than individuals with no family history but a similar defectbut a similar defect

ThrombophiliaThrombophilia Patients with spontaneous venous Patients with spontaneous venous
thromboses, or of a severity that is out thromboses, or of a severity that is out of proportion to a recognised stimulusof proportion to a recognised stimulus

Venous Thromboembolic Venous Thromboembolic DiseaseDisease
Common , associated with considerable Common , associated with considerable morbidity and mortalitymorbidity and mortality
USA: USA:
1:1,000 pa clinically significant DVTs1:1,000 pa clinically significant DVTs
250,000 hospitalisations annually 250,000 hospitalisations annually due to VTEDdue to VTED

ComplicationsComplicationsRisk of recurrence: 2 years Risk of recurrence: 2 years 17.5%17.5%
5 years5 years 24.6%24.6%
Fatal PE: Fatal PE: 1:50,000 pa 1:50,000 pa
20-30% PM 20-30% PM
Commonest cause of death in Commonest cause of death in pregnancypregnancy
Post-phlebitic syndrome up to 20%Post-phlebitic syndrome up to 20%

Who to test?Who to test?
Thrombosis at an unusual siteThrombosis at an unusual site
Recurrent thrombosesRecurrent thromboses
Family history of thrombosisFamily history of thrombosis
Age less than 40Age less than 40
Recurrent miscarriagesRecurrent miscarriages

Inherited ThrombophiliaInherited Thrombophilia1965 AT mutation identified1965 AT mutation identified [Egeberg [Egeberg et et alal]]
1967 Dysfunctional fibrinogen1967 Dysfunctional fibrinogen [Egeberg [Egeberg et et alal]]
1981 Protein C1981 Protein C [Griffin [Griffin et et alal]]
1984 Protein S1984 Protein S [Comp [Comp et alet al]]]]
1993/4 APCr/FV L1993/4 APCr/FV L [Dalhback/Bertina [Dalhback/Bertina et et alal]]
1996 Prothrombin mutation 1996 Prothrombin mutation [Poort [Poort et et alal]]

Thrombophilia Thrombophilia PrevalencePrevalence
Risk factorRisk factor Subjects with Subjects with thrombosis (%)thrombosis (%)
General General population (%)population (%)
Relative Risk Relative Risk of Thrombosisof Thrombosis
AntithrombinAntithrombin 11 0.20.2 25-5025-50
Protein CProtein C 33 0.30.3 10-1510-15
Protein SProtein S 2-32-3 0.20.2 1111
Factor V Factor V LeidenLeiden HeteroHetero
20-5020-50 3-153-15 3-8/80 Homo3-8/80 Homo
Prothrombin 3' Prothrombin 3' UTR mutationUTR mutation
HeteroHetero
66 22 33

Other Inherited Risk Other Inherited Risk FactorsFactors
HyperhomocysteineaemiaHyperhomocysteineaemiaDysfibrinogenaemiasDysfibrinogenaemiasFactor VII Factor VII //Heparin Cofactor IIHeparin Cofactor IIFactor XII deficiencyFactor XII deficiencyDisordered fibrinolysisDisordered fibrinolysisElevated PAI-1Elevated PAI-1Plasminogen deficiencyPlasminogen deficiencyThrombin Activatable Fibrinolytic Inhibitor Thrombin Activatable Fibrinolytic Inhibitor
(TAFI)(TAFI)

Anti-phospholipid antibodiesAnti-phospholipid antibodies
Risk factorRisk factor Subjects with Subjects with VTE (%)VTE (%)
General General population (%)population (%)
RR of RR of ThrombosisThrombosis
Lupus Lupus anticoagulant anticoagulant
3-103-10 44 1111
Anti-cardiolipin Anti-cardiolipin antibodies antibodies
3-103-10 44 3.23.2
OCPOCP 2121 66 4.24.2
PregnancyPregnancy
6.26.2 2.32.3 2.82.8
Previous VTEDPrevious VTED 1414 22 88

AcquiredAcquired ObesityObesity Immobility (surgery/trauma)Immobility (surgery/trauma) OCP/HRTOCP/HRT Pregnancy/puerperiumPregnancy/puerperium HaemoglobinopathiesHaemoglobinopathies Myeloproliferative syndromesMyeloproliferative syndromes Hyperviscosity syndromesHyperviscosity syndromes Cardiac failureCardiac failure

AcquiredAcquiredChronic inflammatory disordersChronic inflammatory disorders
Klinefelter’s syndromeKlinefelter’s syndrome
Behçets syndromeBehçets syndrome
MalignancyMalignancy
Drug induced (e.g. HIT)Drug induced (e.g. HIT)
TTP/HUSTTP/HUS
Nephrotic syndromeNephrotic syndrome
Protein S deficiencyProtein S deficiency
Inflammatory bowel diseaseInflammatory bowel disease

Thrombophilia and Thrombophilia and Laboratory TestingLaboratory Testing
Diagnostic accuracyDiagnostic accuracyClinical value of the testsClinical value of the testsInterpretation of resultsInterpretation of results
Tests frequently requested (and Tests frequently requested (and interpreted) by individuals who are not interpreted) by individuals who are not specialists in this areaspecialists in this areaLaboratories frequently have no clinical Laboratories frequently have no clinical information relating to the patientinformation relating to the patient

Genetic TestingGenetic Testing
Reliable and reasonably robustReliable and reasonably robust
NNational ational EExternal xternal QQuality uality AAssurance ssurance SSchemes chemes (NEQAS)(NEQAS)
Some incorrectly identified samplesSome incorrectly identified samples
APCr low: APCr low: Factor V Leiden mutation confirms Factor V Leiden mutation confirms
APCr normal: No further testingAPCr normal: No further testing
Risk of VTED modestRisk of VTED modest
Do we seek informed consent for genetic testing?Do we seek informed consent for genetic testing?

Phenotypic Testing Phenotypic Testing AccuracyAccuracy
Enormous variability in results:Enormous variability in results:NEQAS/ECAT data supports thisNEQAS/ECAT data supports this
Oral anticoagulants : Protein C/SOral anticoagulants : Protein C/SInappropriate to base a diagnosis on Inappropriate to base a diagnosis on a single result but how many a single result but how many times ?times ?Incorrect information to patients Incorrect information to patients may be falsely reassuring or result may be falsely reassuring or result in inappropriate treatmentin inappropriate treatment

Antithrombin deficiencyAntithrombin deficiency
24 patients with genotypically proven 24 patients with genotypically proven AT deficiencyAT deficiency
Heparin co-factor assayHeparin co-factor assay
IIa substrate:Correctly identified all mutationsIIa substrate:Correctly identified all mutations
Xa substrate:Correctly diagnosed only 50% casesXa substrate:Correctly diagnosed only 50% cases
NEQAS thrombophilia Survey March 2000NEQAS thrombophilia Survey March 2000Functional AT assays showed significant differences Functional AT assays showed significant differences
depending upon substratedepending upon substrate

Laboratory TestsLaboratory Tests
Heterozygotes
Normal relatives
15% heterozygous PC deficient patients had normal PC activity and 5% normal relatives had low PC activity

Immediate Management Immediate Management
No evidence that anticoagulation is less efficient No evidence that anticoagulation is less efficient with prothrombotic abnormalitieswith prothrombotic abnormalitiesAntithrombin deficiency : Heparin resistance is Antithrombin deficiency : Heparin resistance is rare type I :can be efficiently anticoagulated , rare type I :can be efficiently anticoagulated , antithrombin concentrates is not usually antithrombin concentrates is not usually indicatedindicatedPC and PS deficiency:Warfarin induced skin PC and PS deficiency:Warfarin induced skin necrosis is rarenecrosis is rareScreening prior to initiating OAC therapy Screening prior to initiating OAC therapy inappropriateinappropriateLA,severe FXII deficiency&elevated Factor VIII LA,severe FXII deficiency&elevated Factor VIII levels difficult monitoring UFHlevels difficult monitoring UFH

Intensity Or Duration Of Intensity Or Duration Of Anticoagulation Anticoagulation
No randomised prospective studies:Current No randomised prospective studies:Current data/experience standard oral anticoagulant protocols data/experience standard oral anticoagulant protocols
No evidence that more intensive regimes or extended No evidence that more intensive regimes or extended periods of anticoagulation are required periods of anticoagulation are required
BUT - APL/multiple inherited abnormalities including BUT - APL/multiple inherited abnormalities including may be exceptionsmay be exceptions
Risk of recurrence may be increased and extended Risk of recurrence may be increased and extended periods of treatment may be requiredperiods of treatment may be required
OACs:OACs: Mortality 0.3-0.4% Mortality 0.3-0.4%
Major bleed 2-3%Major bleed 2-3%

Aggressive Aggressive Thromboprophylaxis?Thromboprophylaxis?
RR increased but the absolute risk is RR increased but the absolute risk is smallsmall
Thromboprophylaxis :Thromboprophylaxis :
Asymptomatic :No indication Asymptomatic :No indication
At-risk individuals & high risk periods: At-risk individuals & high risk periods: should be given should be given
‘‘Economy Class syndrome’ 90% have Economy Class syndrome’ 90% have >2 risk factors for thrombosis>2 risk factors for thrombosis

Prothrombotic Abnormality & Prothrombotic Abnormality & OCPOCP
Thrombosis in women with inherited Thrombosis in women with inherited prothrombotic & OCP is increasedprothrombotic & OCP is increasedFamily studies may be of value in Family studies may be of value in establishing the risk of thrombosis if a establishing the risk of thrombosis if a genetic risk factor has been identifiedgenetic risk factor has been identifiedPOP or progestagen-containing IUDs no POP or progestagen-containing IUDs no increased risk of VTEDincreased risk of VTEDFactor V Leiden + OCPFactor V Leiden + OCP
RR VTED RR VTED 35/50-fold increase35/50-fold increase

Prothrombotic Abnormality & Prothrombotic Abnormality & OCPOCP
Avoid Avoid In women with history of TED In women with history of TED 1st-degree relative with TED1st-degree relative with TED in women with multiple genetic defectsin women with multiple genetic defects
Asymptomatic women with identified Asymptomatic women with identified genetic risk factors - not absolute genetic risk factors - not absolute contraindication OCPcontraindication OCP

Prothrombotic Abnormality & Prothrombotic Abnormality & HRTHRT
HRT increases risk of TED ~3-foldHRT increases risk of TED ~3-fold
Risk highest in the initial 12 ms of treatmentRisk highest in the initial 12 ms of treatment
Synergy between HRT and thrombophiliaSynergy between HRT and thrombophilia
Use with caution in women with a PMH of TEDUse with caution in women with a PMH of TED
EVTET studyEVTET study HRT:HRT: 10.7% incidence of 10.7% incidence of VTEDVTED
Placebo:Placebo:2.3%2.3%
Asymptomatic women with identified genetic Asymptomatic women with identified genetic risk factors - not an absolute contraindication to risk factors - not an absolute contraindication to HRTHRT

Thromboprophylaxis In Thromboprophylaxis In PregnancyPregnancy
Risk of VTED increased in pregnancyRisk of VTED increased in pregnancy Genetic risk factorGenetic risk factor Multiple pregnancyMultiple pregnancyAdvanced maternal ageAdvanced maternal ageProlonged bed-restProlonged bed-restPrevious thrombotic history Previous thrombotic history Recurrent miscarriagesRecurrent miscarriages
Routine thromboprophylaxis is not Routine thromboprophylaxis is not indicated in all women with indicated in all women with thrombophiliathrombophilia

Thrombophilia & Arterial Thrombophilia & Arterial DiseaseDisease
No good evidence No good evidence
Anti-phospholipid syndromeAnti-phospholipid syndrome
HyperhomocysteineaemiaHyperhomocysteineaemia
Factor V Leiden/Prothrombin mutation - Factor V Leiden/Prothrombin mutation - Possible synergistic interaction with Possible synergistic interaction with other risk factorsother risk factors

SummarySummary
Increasing enthusiasm for thrombophilia Increasing enthusiasm for thrombophilia testingtestingConcerns about accuracy and interpretation Concerns about accuracy and interpretation Lack of evidence-based data to aid Lack of evidence-based data to aid managementmanagementAre we providing patients and clinicians with Are we providing patients and clinicians with inaccurate information that leads to false inaccurate information that leads to false reassurance or alternatively creates panic and reassurance or alternatively creates panic and results in inappropriate treatment?results in inappropriate treatment?

Genetic defect NO TEDGenetic defect NO TED
TED 50% No lab abnormalityTED 50% No lab abnormality
Lab abnormality +FH >lab with NO Lab abnormality +FH >lab with NO FHFH

Other Inherited Risk Other Inherited Risk FactorsFactors
Histidine rich glycoproteinHistidine rich glycoprotein
Elevated FVIII/FX/FXIElevated FVIII/FX/FXI
Thrombomodulin mutationsThrombomodulin mutations
EPCR mutationsEPCR mutations
Tissue Factor Pathway Inhibitor (TFPI) Tissue Factor Pathway Inhibitor (TFPI)
Factor V CambridgeFactor V Cambridge
Factor XIII (Val234Leu)Factor XIII (Val234Leu)
Platelet glycoprotein receptor polymorphismsPlatelet glycoprotein receptor polymorphisms

ThrombophiliaThrombophilia
Thrombosis is a multi-factorial diseaseThrombosis is a multi-factorial disease
Multiple genetic risk factors increase the Multiple genetic risk factors increase the risk of TEDrisk of TED
In the majority: screen for only the In the majority: screen for only the ‘common’ inherited/acquired ‘common’ inherited/acquired prothrombotic abnormalities prothrombotic abnormalities
50% of patients with TED have no 50% of patients with TED have no evidence of prothrombotic evidence of prothrombotic abnormalitiesabnormalities

Management of Management of thrombophiliathrombophilia
Dr Galila Zaher Dr Galila Zaher
MRCPathMRCPath
Consultant Consultant Hematologist Hematologist

BLOOD CLOTTINGBLOOD CLOTTING
Blood clotting interactionsBlood clotting interactions
Plasma protein clotting factorsPlasma protein clotting factors
Vascular endotheliumVascular endothelium Platelets

HemostasisSubendothelial matrixSubendothelial matrix
PlateletsPlatelets
Hemostatic plugHemostatic plug
FibrinFibrin
Endothelial cellEndothelial cell
RBCRBCWBCWBC
WBCWBC
HemostasisSubendothelial matrixSubendothelial matrix
PlateletsPlatelets
Hemostatic plugHemostatic plug
FibrinFibrin
Endothelial cellEndothelial cell
RBCRBCWBCWBC
WBCWBC

COAGULOPATHIESCOAGULOPATHIES
Bleeding Bleeding Thrombosis Thrombosis
Clotting factors Natural Clotting factors Natural anticoagulantanticoagulant
plateletsplatelets

Clot formationClot formation
Platelet Platelet activation activation Primary Primary hemostasishemostasis
No &countNo &count (immediate)(immediate)
Fibrin generationFibrin generation plasma clotting plasma clotting Secondary Secondary
hemostasishemostasisfactorsfactors (delayed) (delayed)

Adhesion
GpIIb/IIIa
Platelet Activation
GpIIb/IIIaGpIIb/IIIa Aggregation
ADP
Adrenaline Platelet GpIb
Exposed Collagen
Endothelium
vWF
COLLAGEN
GpIIb/IIIaGpIIb/IIIa AggregationGpIIb/IIIaGpIIb/IIIa Aggregation
AdhesionAdhesion
ADP
Adrenaline
THROMBINTHROMBIN

Clotting factor productionClotting factor production
Liver: source of plasma clotting factors Liver: source of plasma clotting factors except VWF except VWF
Factor VIII: produced by liver & Factor VIII: produced by liver & endotheliumendothelium
VWF: endothelial cells & megakaryocytesVWF: endothelial cells & megakaryocytes
Vitamin K dependent clotting factors are: Vitamin K dependent clotting factors are: II, VII, IX, XII, VII, IX, X

COAGULATION PATHWAYSCOAGULATION PATHWAYS
Intrinsic & extrinsic pathways Intrinsic & extrinsic pathways ““conclude” in the common pathwayconclude” in the common pathway
Intrinsic pathway clotting factorsIntrinsic pathway clotting factors
Extrinsic pathway clotting factorsExtrinsic pathway clotting factors
Common pathway clotting factorsCommon pathway clotting factors

Intrinsic pathway XII ---> XIIa
XI---------XIa
IX --------> IXa + VIII APC PC +PSCa +PL
X----------------------> Xa [Common pathway]
V+Ca+PL
Prothrombin -------------> thrombin AT
vfibrinogen--------------> fibrin
Extrinsic pathwayVII + TF ----->VIIa/TF

Activation of fibrinolysis
plasminogenplasminogen
thrombin
plasmin
damaged cellsdamaged cells
t-PAPAI
cross-linked fibrinfibrinogen
FDP(X,Y,D,E)
X-FDP(D-Dimer, cross-linked oligomers, DD/E ...)
antiplasmin
extrinsic pathway extrinsic pathway
inflammation
traumamental/physical stress

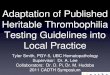
Generation Of Fibrin and D-DimerGeneration Of Fibrin and D-Dimer
DE
D
E
DDEE
F XIIIa
fibrin
fibrin polymer DDE
DE
D
E
DDE
cross-linkedfibrin (clot)
fibrinogenE
DDE
thrombinFpA, FpB
D-dimer cross-linkage
ED
ED
ED
ED
E
DE
DE
E
DDE
E
D
E
D
E
EDD
E

D-Dimer
D-Dimer is a synonym for a variety of cross-linked fibrin degradation products.
Indicative for dissolution of an existing thrombus.
Evidence of a previous thrombotic event

Clinical Application Of D-Clinical Application Of D-
DimerDimer Exclusion of deep vein thrombosis
(DVT)
Exclusion of pulmonary embolism (PE)
Supports diagnosis and monitoring of
DIC

Incidence Of Venous Thromboembolism
Annual frequency per 100,000 : Deep vein thrombosis 160
Symptomatic, non-fatal PE 20
Fatal, autopsy-detected PE 50 250,000 hospitalisations annually due to VTED
Int Angiol 1997

ComplicationsComplications Risk of recurrence: 2 years Risk of recurrence: 2 years 17.5%17.5% 5 years5 years 24.6%24.6% Fatal PE: Fatal PE: 1:50,000 pa 1:50,000 pa
20-30% PM 20-30% PM Commonest cause of death in pregnancyCommonest cause of death in pregnancy Post-phlebitic syndrome Post-phlebitic syndrome
3 years after DVT 3 years after DVT 35- 69% 35- 69% 5-10 years after DVT 49-100% 5-10 years after DVT 49-100%
Venous ulcersVenous ulcers

Mortality From Pulmonary Embolism
About 1/10 hospital deaths is due to PE
PE is still the leading cause of maternal mortality

Diagnosis Of DVT
Compression ultrasound (CUS) Sensitivity ~97%; Specificity ~94%Problems: Calf vein thrombosis
sensitivity Previous thrombosis
specificity Combine with D-Dimer and PTP

Clinical Prediction Rule Entire leg tenderness along deep
veins collateral superficial veins
Entire leg swellingCalf swelling >3 cm differenceDilated superficial veins
Pitting edema

Clinical Prediction RuleClinical Prediction Rule
Recent bed ridden >3 days Recent bed ridden >3 days
Major surgery within last 3 ms.Major surgery within last 3 ms. Active cancer within last 6 mo. Active cancer within last 6 mo.
PlasterPlaster Paralysis Paralysis Presence of alternative Diagnosis Presence of alternative Diagnosis
-2 -2

Diagnostic Strategies for First Attackproximal Deep Venous Thrombosis
High probability Moderate-Low probability (>3) (1-2)
(0)
Doppler US D-Dimers
Abnormal Normal Normal High Doppler US
Venography Normal Abnormal
Normal Abnormal Save to withhold treatment
Treat with heparin

Diagnostic Strategies for First AttackDistal Deep Venous Thrombosis
High probability Moderate-Low probability (>3) (1-2) (0)
Doppler US D-Dimers
Abnormal Normal High Normal Doppler US
Repeat in W or venography Normal abnormal
Abnormal Normal
Save to withhold treatment withhold treatment
Treat with heparin

Acute VTEAcute VTE
The usual management consists of The usual management consists of UFH or LMWH followed by warfarin.UFH or LMWH followed by warfarin.
Heparin is continued for at least 5 Heparin is continued for at least 5 days or untill INR is in the days or untill INR is in the therapeutic range.therapeutic range.
Warfarin can be started within the Warfarin can be started within the first 24h.first 24h.

Heparin
Mechanism of action :augments anti-thrombin action AT:T 1:1 Heparin AT:T 1:1000
T ½ : 90mDose :loading: 80U/Kg IV :maintenance :18U/Kg/hRoute of administration: IV/SCDuration :3-5d DVT 7-10d PE

Heparin
Monitoring :APTT:1.5-2.5 X control 4-6 hReversal :stop heparin protamine sulphate :1U
neutralize 100 IU heparin No FFPSide effects: Bleeding osteoporosis HIT

Heparin
Contraindications :congenital bleeding disorders HIT
Recent eye or CNS operation

LMWH
Dose :brand dependent Mechanism of action :anti-X > anti-II Route of administration :IV or S/C Monitoring : not indicated Indication for monitoring : pregnancy ,morbid
obesity , sever renal or liver derangement Duration :3-5 d DVT 7-10 d PE Reversal :stop heparin protamine sulphate :un-predictable
response

LMWH
Contra-indications :PMH :HIT CNS eye
operations Inherited bleeding
disordersSide effect : less HIT , bleeding &
osteoporosis.

Warfarin
Mechanism of action : Vit K antagonist Vit K :gamma carboxylation as a post
translation modification Pro-coagulant :X,IX,VII&II(1972) Natural anticoagulant PC &PST1/2 PC is shorter than FVII temporary
hyper-coagulable stateDose :5 mg P.ORoute of administration: P.O

WarfarinMonitoring :INR INR: (PT patient/PT control )ISI
Desired target INR:2.5 INR 3.5 : mechanical heart valve ,
recurrent VTE despite proper anti-caogulation ,+/- APL
Side effect : bleeding 1/100/y ICH 2.5/1000/y Warfarin induced skin
necrosisContra-indications: pregnancy (first &last
trimester),Inhetited bleeding disorders ,acute stage HIT

ThrombophiliaThrombophilia‘‘A disorder of the haemostatic mechanism A disorder of the haemostatic mechanism
with a predisposition towards thrombosis’with a predisposition towards thrombosis’
BUTBUT Many patients with defects remain Many patients with defects remain asymptomatic despite multiple challengesasymptomatic despite multiple challenges
ANDAND >50% patients with TED will have no >50% patients with TED will have no identifiable laboratory abnormalityidentifiable laboratory abnormality
ANDAND proven thrombophilic defect and a proven thrombophilic defect and a family history of TED are at greater risk of family history of TED are at greater risk of TED than individuals with no family history TED than individuals with no family history but a similar defectbut a similar defect

ThrombophiliaThrombophilia
Thrombosis is a multi-factorial diseaseThrombosis is a multi-factorial diseaseMultiple genetic risk factors increase the risk Multiple genetic risk factors increase the risk of TEDof TEDIn the majority: screen for only the ‘common’ In the majority: screen for only the ‘common’ inherited/acquired prothrombotic inherited/acquired prothrombotic abnormalities Patients with spontaneous abnormalities Patients with spontaneous venous thromboses, or of a severity that is out venous thromboses, or of a severity that is out of proportion to a recognised stimulusof proportion to a recognised stimulus
50% of patients with TED have no evidence of 50% of patients with TED have no evidence of prothrombotic abnormalitiesprothrombotic abnormalities

ThrombophiliaThrombophiliaDefinition : abnormal tendency towards excessive Definition : abnormal tendency towards excessive thrombosis .thrombosis .
Indications :Indications : VTE below 35-40 YVTE below 35-40 Y Unprovoked VTEUnprovoked VTE VTE at unusual sites VTE at unusual sites Life threatening VTELife threatening VTE Recurrent fetal lose syndromeRecurrent fetal lose syndrome Recurrent first trimester abortions Recurrent first trimester abortions Investigating SLE patientsInvestigating SLE patients
Recurrent thrombosesRecurrent thrombosesFamily history of thrombosisFamily history of thrombosis

Whom to test?Whom to test? Thrombosis at an unusual siteThrombosis at an unusual site Unprovoked VTEUnprovoked VTE Life threatening VTELife threatening VTE Age less than 40Age less than 40 Recurrent thrombosesRecurrent thromboses Family history of thrombosisFamily history of thrombosis Recurrent miscarriagesRecurrent miscarriagesVTE below 35Y VTE below 35Y Recurrent fetal lose syndromeRecurrent fetal lose syndrome Recurrent first trimester abortions Recurrent first trimester abortions Investigating SLE patientsInvestigating SLE patients

Inherited ThrombophiliaInherited Thrombophilia1965 AT mutation identified1965 AT mutation identified [Egeberg [Egeberg et et alal]]
1967 Dysfunctional fibrinogen1967 Dysfunctional fibrinogen [Egeberg [Egeberg et et alal]]
1981 Protein C1981 Protein C [Griffin [Griffin et et alal]]
1984 Protein S1984 Protein S [Comp [Comp et alet al]]]]
1993/4 APCr/FV L1993/4 APCr/FV L [Dalhback/Bertina [Dalhback/Bertina et et alal]]
1996 Prothrombin mutation 1996 Prothrombin mutation [Poort [Poort et et alal]]

Thrombophilia Thrombophilia PrevalencePrevalence
Risk factorRisk factor Subjects with Subjects with thrombosis (%)thrombosis (%)
General General population (%)population (%)
Relative Risk Relative Risk of Thrombosisof Thrombosis
AntithrombinAntithrombin 11 0.20.2 25-5025-50
Protein CProtein C 33 0.30.3 10-1510-15
Protein SProtein S 2-32-3 0.20.2 1111
Factor V Factor V LeidenLeiden HeteroHetero
20-5020-50 3-153-15 3-8/80 Homo3-8/80 Homo
Prothrombin 3' Prothrombin 3' UTR mutationUTR mutation
HeteroHetero
66 22 33

Other Inherited Risk Other Inherited Risk FactorsFactors
HyperhomocysteineaemiaHyperhomocysteineaemia
DysfibrinogenaemiasDysfibrinogenaemias
Factor VII Factor VII //Heparin Cofactor IIHeparin Cofactor II
Factor XII deficiencyFactor XII deficiency
Disordered fibrinolysisDisordered fibrinolysis
Elevated PAI-1Elevated PAI-1
Plasminogen deficiencyPlasminogen deficiency
Thrombin Activatable Fibrinolytic Inhibitor Thrombin Activatable Fibrinolytic Inhibitor (TAFI)(TAFI)

AcquiredAcquired ObesityObesity Immobility (surgery/trauma)Immobility (surgery/trauma) OCP/HRTOCP/HRT Pregnancy/puerperiumPregnancy/puerperium HaemoglobinopathiesHaemoglobinopathies Myeloproliferative syndromesMyeloproliferative syndromes Hyperviscosity syndromesHyperviscosity syndromes Cardiac failureCardiac failure

AcquiredAcquiredChronic inflammatory disordersChronic inflammatory disorders
Klinefelter’s syndromeKlinefelter’s syndrome
Behçets syndromeBehçets syndrome
MalignancyMalignancy
Drug induced (e.g. HIT)Drug induced (e.g. HIT)
TTP/HUSTTP/HUS
Nephrotic syndromeNephrotic syndrome
Protein S deficiencyProtein S deficiency
Inflammatory bowel diseaseInflammatory bowel disease

Anti-phospholipid antibodiesAnti-phospholipid antibodies
Risk factorRisk factor Subjects with Subjects with VTE (%)VTE (%)
General General population (%)population (%)
RR of RR of ThrombosisThrombosis
Lupus Lupus anticoagulant anticoagulant
3-103-10 44 1111
Anti-cardiolipin Anti-cardiolipin antibodies antibodies
3-103-10 44 3.23.2
OCPOCP 2121 66 4.24.2
PregnancyPregnancy
6.26.2 2.32.3 2.82.8
Previous VTEDPrevious VTED 1414 22 88

Thrombophilia and Thrombophilia and Laboratory TestingLaboratory Testing
Diagnostic accuracyDiagnostic accuracy
Clinical value of the testsClinical value of the tests
Interpretation of resultsInterpretation of results
Tests frequently requested (and Tests frequently requested (and interpreted) by individuals who are not interpreted) by individuals who are not specialists in this areaspecialists in this area
Laboratories frequently have no clinical Laboratories frequently have no clinical information relating to the patientinformation relating to the patient

Thrombophilia screen
PC level : Functional assay PS level : Functional assayAT level : Functional assay APCR ratio :functional assay correlates
with genetic study: FVL Prothrombin gene mutationMTHFRAPS: LA: functional assay Anti-cardilipin antibodies

Genetic TestingGenetic Testing
Reliable and reasonably robustReliable and reasonably robust
NNational ational EExternal xternal QQuality uality AAssurance ssurance SSchemes chemes (NEQAS)(NEQAS)
Some incorrectly identified samplesSome incorrectly identified samples
APCr low: APCr low: Factor V Leiden mutation confirms Factor V Leiden mutation confirms
APCr normal: No further testingAPCr normal: No further testing
Risk of VTED modestRisk of VTED modest
Do we seek informed consent for genetic Do we seek informed consent for genetic testing?testing?

Phenotypic Testing Phenotypic Testing AccuracyAccuracy
Enormous variability in results:Enormous variability in results:NEQAS/ECAT data supports thisNEQAS/ECAT data supports this
Oral anticoagulants : Protein C/SOral anticoagulants : Protein C/SInappropriate to base a diagnosis on Inappropriate to base a diagnosis on a single result but how many a single result but how many times ?times ?Incorrect information to patients Incorrect information to patients may be falsely reassuring or result may be falsely reassuring or result in inappropriate treatmentin inappropriate treatment

Antithrombin deficiencyAntithrombin deficiency
24 patients with genotypically proven 24 patients with genotypically proven AT deficiencyAT deficiency
Heparin co-factor assayHeparin co-factor assay
IIa substrate:Correctly identified all mutationsIIa substrate:Correctly identified all mutations
Xa substrate:Correctly diagnosed only 50% Xa substrate:Correctly diagnosed only 50% casescases
NEQAS thrombophilia Survey March 2000NEQAS thrombophilia Survey March 2000Functional AT assays showed significant Functional AT assays showed significant
differences depending upon substratedifferences depending upon substrate

Laboratory TestsLaboratory Tests
Heterozygotes
Normal relatives
15% heterozygous PC deficient patients had normal PC activity and 5% normal relatives had low PC activity

Timing Of Thrombophilia
Avoid acute presentation: consumption of the natural anticoagulant Heparin & warfarin therapy interfere with
the assayBest time after D/C of warfarin therapy by
2-4 WAny abnormal results should be repeated
4-6W apart before labeling patient as thrombophilia

Interpretation
Life threatening episode40-50% of selected patients with
VTE have normal results despite extensive testing
APS & AT are highly thrombogenic & associated with high recurrence rate.
Double heterozygosity :high incidence of VTE

Immediate ManagementImmediate Management
No evidence that anticoagulation is less efficient No evidence that anticoagulation is less efficient with prothrombotic abnormalitieswith prothrombotic abnormalitiesAntithrombin deficiency : Heparin resistance is Antithrombin deficiency : Heparin resistance is rare type I :can be efficiently anticoagulated , rare type I :can be efficiently anticoagulated , antithrombin concentrates is not usually antithrombin concentrates is not usually indicatedindicatedPC and PS deficiency:Warfarin induced skin PC and PS deficiency:Warfarin induced skin necrosis is rarenecrosis is rareScreening prior to initiating OAC therapy Screening prior to initiating OAC therapy inappropriateinappropriateLA,severe FXII deficiency&elevated Factor VIII LA,severe FXII deficiency&elevated Factor VIII levels difficult monitoring UFHlevels difficult monitoring UFH

Intensity Or Duration Of Intensity Or Duration Of AnticoagulationAnticoagulation
No randomised prospective studies:Current No randomised prospective studies:Current data/experience standard oral anticoagulant protocols data/experience standard oral anticoagulant protocols
No evidence that more intensive regimes or extended No evidence that more intensive regimes or extended periods of anticoagulation are required periods of anticoagulation are required
BUT - APL/multiple inherited abnormalities including BUT - APL/multiple inherited abnormalities including may be exceptionsmay be exceptions
Risk of recurrence may be increased and extended Risk of recurrence may be increased and extended periods of treatment may be requiredperiods of treatment may be required
OACs:OACs: Mortality 0.3-0.4% Mortality 0.3-0.4%
Major bleed 2-3%Major bleed 2-3%

Aggressive Aggressive Thromboprophylaxis?Thromboprophylaxis?
RR increased but the absolute risk RR increased but the absolute risk is smallis smallThromboprophylaxis :Thromboprophylaxis :Asymptomatic :No indication Asymptomatic :No indication At-risk individuals & high risk At-risk individuals & high risk periods: should be given periods: should be given ‘‘Economy Class syndrome’ 90% Economy Class syndrome’ 90% have >2 risk factors for thrombosishave >2 risk factors for thrombosis

Prothrombotic Abnormality & Prothrombotic Abnormality & OCPOCP
Thrombosis in women with inherited Thrombosis in women with inherited prothrombotic & OCP is increasedprothrombotic & OCP is increasedFamily studies may be of value in Family studies may be of value in establishing the risk of thrombosis if a establishing the risk of thrombosis if a genetic risk factor has been identifiedgenetic risk factor has been identifiedPOP or progestagen-containing IUDs no POP or progestagen-containing IUDs no increased risk of VTEDincreased risk of VTEDFactor V Leiden + OCPFactor V Leiden + OCP
RR VTED RR VTED 35/50-fold increase35/50-fold increase

Prothrombotic Abnormality & Prothrombotic Abnormality & OCPOCP
Avoid Avoid In women with history of TED In women with history of TED 1st-degree relative with TED1st-degree relative with TED in women with multiple genetic in women with multiple genetic
defectsdefects
Asymptomatic women with identified Asymptomatic women with identified genetic risk factors - not absolute genetic risk factors - not absolute contraindication OCPcontraindication OCP

Prothrombotic Abnormality & Prothrombotic Abnormality & HRTHRT
HRT increases risk of TED ~3-foldHRT increases risk of TED ~3-fold
Risk highest in the initial 12 ms of treatmentRisk highest in the initial 12 ms of treatment
Synergy between HRT and thrombophiliaSynergy between HRT and thrombophilia
Use with caution in women with a PMH of TEDUse with caution in women with a PMH of TED
EVTET studyEVTET study HRT:HRT: 10.7% incidence of 10.7% incidence of VTEDVTED
Placebo:Placebo:2.3%2.3%
Asymptomatic women with identified genetic Asymptomatic women with identified genetic risk factors - not an absolute contraindication to risk factors - not an absolute contraindication to HRTHRT

Thromboprophylaxis In Thromboprophylaxis In PregnancyPregnancy
Risk of VTED increased in pregnancyRisk of VTED increased in pregnancy Genetic risk factorGenetic risk factor
Multiple pregnancyMultiple pregnancy
Advanced maternal ageAdvanced maternal age
Prolonged bed-restProlonged bed-rest
Previous thrombotic history Previous thrombotic history
Recurrent miscarriagesRecurrent miscarriages
Routine thromboprophylaxis is not Routine thromboprophylaxis is not indicated in all women with thrombophiliaindicated in all women with thrombophilia

Thrombophilia & Arterial Thrombophilia & Arterial DiseaseDisease
No good evidence No good evidence
Anti-phospholipid syndromeAnti-phospholipid syndrome
HyperhomocysteineaemiaHyperhomocysteineaemia
Factor V Leiden/Prothrombin mutation - Factor V Leiden/Prothrombin mutation - Possible synergistic interaction with Possible synergistic interaction with other risk factorsother risk factors

SummarySummary
Increasing enthusiasm for thrombophilia Increasing enthusiasm for thrombophilia testingtestingConcerns about accuracy and interpretation Concerns about accuracy and interpretation Lack of evidence-based data to aid Lack of evidence-based data to aid managementmanagementAre we providing patients and clinicians with Are we providing patients and clinicians with inaccurate information that leads to false inaccurate information that leads to false reassurance or alternatively creates panic and reassurance or alternatively creates panic and results in inappropriate treatment?results in inappropriate treatment?

Genetic defect NO TEDGenetic defect NO TED
TED 50% No lab abnormalityTED 50% No lab abnormality
Lab abnormality +FH >lab with NO Lab abnormality +FH >lab with NO FHFH

Other Inherited Risk Other Inherited Risk FactorsFactors
Histidine rich glycoproteinHistidine rich glycoprotein
Elevated FVIII/FX/FXIElevated FVIII/FX/FXI
Thrombomodulin mutationsThrombomodulin mutations
EPCR mutationsEPCR mutations
Tissue Factor Pathway Inhibitor (TFPI) Tissue Factor Pathway Inhibitor (TFPI)
Factor V CambridgeFactor V Cambridge
Factor XIII (Val234Leu)Factor XIII (Val234Leu)
Platelet glycoprotein receptor Platelet glycoprotein receptor polymorphismspolymorphisms

Diagnosis Of DVT/PE
Development and validation of structured clinical assessment for estimating pre-test probability (PTP)
Advances in availability of sensitive and rapid turnaround assays for D-Dimer
Integration of the two above advances into a diagnostic, safe algorithm for non-invasive objective testing, reducing the need for invasive procedures

Pre-test probability (PTP) for PEPre-test probability (PTP) for PE
according to Wells 1997according to Wells 1997
scoreclinical symptoms / signs of DVT 3.0active cancer treated within last 6 months 1.0heart rate > 100/min 1.5immobilization / surgery in last 4 weeks 1.5previous history of DVT or PE 1.5hemoptysis 1.0no alternative diagnosis (more) likely than PE 3.0
>6 = high PTP; 2-6 = moderate PTP; <1.5 = low PTP >6 = high PTP; 2-6 = moderate PTP; <1.5 = low PTP __ __

Strategy in diagnosis of PEStrategy in diagnosis of PE
low pre-test probability (PTP) and negative D-Dimer, VQ scan negative or non-diagnostic
PE excluded
high PTP and diagnostic VQ scanPE confirmed
in any other case further testing by CUS and /or angiography
SD Chunial, JS Ginsberg Throm Res 2000

Anti-thrombin deficiencyAnti-thrombin deficiency Resistant to heparin.Resistant to heparin. Heparin lower AT level by 30%.Heparin lower AT level by 30%. AT conc is safe & effective.AT conc is safe & effective. Recommended:Recommended:1.1. Difficult to achieve adequate Difficult to achieve adequate
anticoagulation .anticoagulation .2.2. Recurrent thrombosis despite adequate Recurrent thrombosis despite adequate
anticoagulation.anticoagulation.3.3. Thromboprphylaxis when anticoagulation is Thromboprphylaxis when anticoagulation is
contraindicated.contraindicated.

Anti-thrombin deficiencyAnti-thrombin deficiency AT conc: pooled normal human plasma.AT conc: pooled normal human plasma.
recombinant AT .recombinant AT . Dose : 50 units /Kg .Dose : 50 units /Kg . Plasma monitoring : plasma level >80%.Plasma monitoring : plasma level >80%. Repeat 60% of the initial dose 24h.Repeat 60% of the initial dose 24h. The biological t1/2 2-4 days.The biological t1/2 2-4 days.

Protein C deficiencyProtein C deficiency
Warfarin induced skin necrosis ”rare”.Warfarin induced skin necrosis ”rare”. Warfarin reduce PC by 50%.Warfarin reduce PC by 50%. Routine measurement of plasma PC Routine measurement of plasma PC
before starting OAC is not recommended.before starting OAC is not recommended. Known cases of PC deficiency should Known cases of PC deficiency should
receive OAC under heparin &increased receive OAC under heparin &increased gradually.gradually.
PC conc or FFP can provide protection PC conc or FFP can provide protection against recurrent skin necrosis until a against recurrent skin necrosis until a stable level of anticoagulation is achieved. stable level of anticoagulation is achieved.

Long term therapy to Long term therapy to prevent recurrenceprevent recurrence
Recurrence in the first year is 27%.”Kearon” Recurrence in the first year is 27%.”Kearon” 3m Vs extended anticoagulation favours 3m Vs extended anticoagulation favours extended extended
The lowest recurrence found after 6-12 m of The lowest recurrence found after 6-12 m of initial therapy .initial therapy .
Long term warfarin is highly effective in Long term warfarin is highly effective in preventing recurrence as compared with 6 m preventing recurrence as compared with 6 m therapy(2.6Vs21%) this benefit is partially therapy(2.6Vs21%) this benefit is partially counterbalanced by a trend towered an counterbalanced by a trend towered an increased incidence of major bleeding (8 increased incidence of major bleeding (8 %Vs3% )&no difference in mortality .%Vs3% )&no difference in mortality .

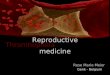
The cumulative incidence of The cumulative incidence of recurrence after of cessation OACrecurrence after of cessation OAC
0
5
10
15
20
25
30
First year 5 years 8 years
Recurrace
“Prandoni”.

Risk of recurrenceRisk of recurrence FVL &PG mutation heterozygosity :conflicting FVL &PG mutation heterozygosity :conflicting
reports.reports. Number of major bleeding would exceed the Number of major bleeding would exceed the
number of clinically PE that would be number of clinically PE that would be preventedprevented
Combined heterozygosity for FVL Combined heterozygosity for FVL &PG20210 :the recurrence rate is significantly &PG20210 :the recurrence rate is significantly high .high .
important risk factors : homozygous FVL, APS important risk factors : homozygous FVL, APS & cancer.& cancer.
PC&PS deficiency Low frequency to draw firm PC&PS deficiency Low frequency to draw firm conclusion.conclusion.

The decision to continue The decision to continue anticoagulation anticoagulation
Risk of recurrence.Risk of recurrence. Risk of major bleeding .Risk of major bleeding . Patient compliance &preference.Patient compliance &preference. Life expectancy.Life expectancy. Quality of life. Quality of life.

Recommendations .Recommendations . Indefinite anticoagulation at target INR 2-3 is Indefinite anticoagulation at target INR 2-3 is
recommended only in the following high risk recommended only in the following high risk patients:patients:
Two or more spontaneous thrombosis.Two or more spontaneous thrombosis. One spontaneous thrombosis in case of AT One spontaneous thrombosis in case of AT
deficiency or APS.deficiency or APS. One spontaneous life threatening thrombosis (near One spontaneous life threatening thrombosis (near
fatal PE ,cerebral, mesenteric ,or portal vein fatal PE ,cerebral, mesenteric ,or portal vein thrombosis).thrombosis).
One spontaneous thrombosis at an unusual site One spontaneous thrombosis at an unusual site (mesenteric ,cerebral).(mesenteric ,cerebral).
One Spontaneous thrombosis in the presence of One Spontaneous thrombosis in the presence of more than a single genetic defect. more than a single genetic defect.

Future approachesFuture approaches
Extended low intensity warfarin at INR Extended low intensity warfarin at INR 1.5-2.1.5-2.
The PREVENT study :low intensity The PREVENT study :low intensity warfarin reduce the rate of recurrence by warfarin reduce the rate of recurrence by more than 60% compared with placebo more than 60% compared with placebo without an increased in major bleeding.without an increased in major bleeding.
Ximelagatran :was compared to placebo Ximelagatran :was compared to placebo &was shwoen to be highly effective in &was shwoen to be highly effective in preventing recurrent VTE. preventing recurrent VTE.

surgerysurgery
Inherited thrombophilia& surgery :Inherited thrombophilia& surgery : Are high risk group .Are high risk group . Prophylactic perioperative anti-Prophylactic perioperative anti-
coagulation &LMWH.coagulation &LMWH.