Embed Size (px)
Citation preview

1
Principles of Antimicrobial Therapy
NAFRIALDI

2
Principles of Antimicrobial Therapy
• Antimicrobial agents are the most commonly used and misused of all drugs
• The inevitable consequence emergence of antibiotic-resistant pathogens
• Reducing inappropriate AM use is thought to be the best way to control resistance.
• Over prescribing remains widespread. – patients demand,– time pressure on clinician, – diagnostic uncertainty

3
Susceptibility of Microorganism to AMA
• Successful AM therapy depends on concentration of AMA at the site of infection – must be sufficient to inhibit the growth of
microorganism – must remain below toxic level in this condition, microorganism is considered
susceptible to AMA
• If host defenses are intact and active, bacteriostatic agent may be sufficient.
• If host defenses are impaired, a bactericidal effect is required

4
Bacterial Resistance to AMA
• The emergence of bacterial resistance to AMA is a very serious development that threatens the end of antibiotic era
• Some steps to diminish AM resistance:– Choosing AM based on local pattern of susceptibility– Judicious use and proper attention to indwelling
catheter– Proper antiseptic technique– Appropriate use of prophylactic AB in surgery– Strict compliance to hand hygiene– Vaccination

5
Selection of AMA (1)
• Four options of AM therapy:– Empirical, experimental, definitive,
prophylaxis
• Empirical th/ is widely utilized, and is potential for abuse

6
CONSIDERATIONS IN SELECTING AMA
– Whether it is even indicated. – In cases of symptoms are present but are not life-
threatening, it is better to postpone the AM until the D/ is obvious. Example: FUO
– The Diagnosis may be masked if therapy is started and appropriate culture are not obtained.
– AM often may be used if disease is severe or if withholding of therapy will result in failure to manage a potentially serious life-threatening infection.

7
Selection of AMA (2)
• Optimal and judicious selection of AM requires– clinical judgment – detailed knowledge of pharmacological and
microbiological factors– knowledge of the most likely infecting microorganisms
and their susceptibility to AMA.
• The most practical method for immediate identification of bacteria is examination of the infected secretion or body fluids with gram stain.

8
Selection of AMA (3)• In many situations, identification of morphology
of the infecting organism is not adequate to arrive at specific bacteriological diagnosis Broad spectrum AM is then indicated, Culture of the presumed site of infection and blood, should be taken prior to the institution of drug therapy.
• For definitive therapy, once an organism has been isolated and results of susceptibility tests are known, the regimen should be changed to specific and narrow spectrum AMA

9
Pharmacokinetic Factor of AM Th/ (1)
• In vitro activity is only a guide as to whether an AM is likely to be effective for an infection.
• Successful th/ depends on achieving a drug concentration that is sufficient to inhibit or kill bacteria at the site of infection without harming the patient.
• The drug concentration at the infected site should be at least equal to the MIC for the infecting microorganism (it is advisable to achieve multiples of this concentration).

10
Pharmacokinetic Factor of AM Th/ (2)
• Three most important pharmacokinetic parameters for evaluating antibiotic efficacy:– Peak serum level (Cmax), – Trough level (Cmin), – Area Under the serum concentration time
Curve (AUC).
• While the PK parameters quantify the serum level time course, they do not describe the killing activity of an antibiotic.

11
PK/PD • Integrating the PK parameters with the MIC
gives three PK/PD parameters which quantify the activity of an antibiotic: – Peak / MIC ratio, – T > MIC, – 24h-AUC / MIC ratio.
For “concentration-dependent killing” the high Peak/MIC ratio is important
For “time-dependent killing” AM, the T above MIC and AUC24/MIC ratio is important

12
PK/PD Parameters

13

14
Pharmacokinetic factor of AM Th/ (2)
• Penetration of drugs into sites of infection almost always depends on passive diffusion. The rate of penetration is proportional to the concentration of free drug in the plasma or extracellular fluid.
• Drugs with high protein bound have limited penetration, and thus may have reduced activity because only the unbound fraction is free to interact with the target.
• Fluoroquinolones, isoniazid, cotrimoxazole, and rifampicin penetrate cell well and achieve concentration that inhibit or kill pathogens residing within cells.

15
Pharmacokinetic Factor of AM Th/ (3)
• Pharmacokinetic properties of AM determine their ability to eradicate bacteria at concentration attained during therapy.
• These properties are: – 1) Time above MIC (time-dependent AB)– 2) Peak / MIC ratio – 3) AUC24 / MIC ratio (AUIC).
2) and 3) for concentration-dependent killing

16
Concentration-dependent killing AM
• Aminoglycosides, metronidazole and fluoroquinolone exibits concentration-dependent activity.
• Their efficacy is correlated with Cmax/MIC and AUC24/MIC ratios.
• For example, an AUC24/MIC ratio of 30 to 50 (at least 10) is thought to predict optimal bacterial activity
• For this class of drug, administration of maximum dose for a shorter time would be optimal.

17
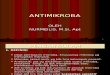
Pharmacokinetic/Pharmacodynamic (PK/PD) Parameters
MIC
Time
CONC.
Cmax
Area Under the Curve
Time above-MIC
• Time-dependent killing Time above MIC required: > 40%
• Concentration-dependent killing Cmax/MIC required > 10 x

18
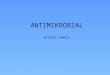
Relationship between time above MIC and bacterial eradication for -lactams
40
60 100
20
80Time above MIC (%)
Bact
eri
al era
dic
ati
on
(%)
20
40
60
80
100
(Craig,2002)

19
Time-dependent killing AM
• Type II antibiotics (beta-lactams, clindamycin, erythromcyin, and linezolid) demonstrate the complete opposite properties. The ideal dosing regimen for these antibiotics maximizes the duration of exposure. The T>MIC is the parameter that best correlates with efficacy. For beta-lactams and erythromycin, maximum killing is seen when the time above MIC is at least 70% of the dosing interval.

20
Penetration of AMs into CSF
• The integrity of BBB is diminished during active bacterial infection; tight junctions in cerebral capillaries open, leading to a marked increase in the penetration of even polar drugs.
• As the infection is eradicated, and the inflammatory reaction subsides, penetration return to normal. Since this may occur while viable microorganisms persist in the CSF, drug dosage should not be reduced as the patient improves.

21
Penetration of AMs into CSF
• Meninges normal; good penetration: – 3rd cephalosporins (exclude ceftriaxone),
chloramphenicol, ethambutol, isoniazid, metronidazole, rifampicin, sulphonamide, trimetoprim.
• Meninges inflamed; good penetration:– penicillins, ceftriaxone, cefuroxime,
cefotaxime, tetracycline, fluconazole.
• Meninges inflamed; poor penetration: – 1st and 2nd cephalopsporins, aminoglycosides,
macrolides, vancomycin.

22
Role of Host Factors in AMT (1)
• The functional state of host defense mechanisms is a critical determinant of therapeutic effectiveness of AMAs. Both humoral and celular immunity are important
• In the immunocompetent host, halting the multiplication of microorganisms with a bacteriostatic agent is sufficient to cure the infection
• In immunocompromized host, a bactericidal agent is required (bacterial endocarditis, bacterial meningitis, infections in neutropenic patients, HIV/AIDS, uncontrolled DM, malnutrition, …)

23
Role of Host Factors in AMT (2)
• Local factors affect the AM activity. – Pus, can bind drugs or inhibit drug action. Low
pH in infected sites and anaerobic condition can reduce AM activity, particularly aminoglycosides.
– Foreign body markedly reduces the likelihood of successful AM therapy.
– Prosthetic materials promotes a bacterial biofilm that impairs phagocytosis. Within the biofilm , bacterial density is high and bacterial growth is slow.
favor bacterial persistence frequent relapses

24
Combined AMAs
INDICATIONS:• Severe infection in which the cause is unknown.
Prolong use should be avoided, because toxicity, superinfection, and selection of multiple drug resistant may result.
• Polymicrobial infection• To have synergistic effect in specific infection
(endocarditis, Ps aeruginosa infection, H influenza infection).
• To prevent the emergence of resistant microorganism (in TBC, H pylori infection)

25
Disadvantage of Combinations of AMAs
• Increase risk of toxicity
• Selection of multiple-drug resistant microorganisms
• Eradication of normal host flora with subsequent superinfection.
• Increase cost to patients
• Possibility of antagonistic effect.

26
Prophylaxis of Infection with AM
• Chemoprophylaxis is used to protect patients from invasion by specific microorganisms to which they are exposed. But it remains controversial in numerous situations.
• If a single, effective, and non toxic drug is used to prevent infection by a specific microorganism or to eradicate an early infection, the prophylaxis is successful.
• If the aim of prophylaxis is to prevent colonization or infection by any or all microorganisms present in the environment of a patient, then prophylaxis often fail.

27
Successful Examples of Chemoprophylaxis
• Rifampicin used to prevent meningococcal meningitis
• Prevention of gonorrhoea or syphilis after contact with with an infected person
• Intermittent use of cotrimoxazole to prevent recurrent UTI caused by E coli.
• AM prophylaxis to prevent infections in transplantation or chemotherapy

28
Successful Examples of Chemoprophylaxis
• Primary or secondary infection in AIDS patients whose CD4 counts are less than 200
• Patients with valvular or other structural lesion of heart who are undergoing dental surgery
• Prophylactic antibiotic in surgical procedure.

29
Effective and Judicious Use of Surgical Antibiotic Prophylaxis
• AMA must be present at wound site at the time of its closure. The drug must be given iv within 1 hour before incision and another one dose intra operatively for prolong procedure.
• The AMA must be active against the most likely contaminating microorganisms

30
Effective and Judicious Use of Surgical Antibiotic Prophylaxis
• The continued use of AMA after surgical procedure is unwarranted and potentially harmful.
• Use beyond 24 hour is unnecessary• Prophylaxis is justified in dirty and contaminated
procedure• In clean surgery, AMA should not be used
routinely

31
Superinfection• Definition: appearance of bacteriological and
clinical evidence of new infection during the AM therapy
• Therapeutic doses of AMA alter the normal microbial population of intestinal, respiratory, and urinary tracts; as a result, some develop superinfection,
• Microorganism responsible for the new infection can be drug-resistant strain of enterobacteriaceae, Pseudomonas, and Candida.
• The broader the AM spectrum, and the longer the period of AM treatment, the greater is the possibility of superinfection produced by a typical drug-resistant microorganism.

32
Misuses of AMAs (1)
• Treatment of viral infections• Therapy of FUO which can mask an underlying
infection, delay the diagnosis, prevent identification of the infectious pathogen by rendering culture negative.
• Improper dosage, wrong frequency, excessive or subtherapeutic dose.
• Inappropriate reliance on chemotherapy alone. Drainage, debridement, and removal of foreign body are important.

33
Misuses of AMAs (2)
• AM for hospitalized patients is too often given in the absence of supporting microbiological data.
• Selection and application of drug therapy unmatched with bacterial culture and Gram stains
• Frequent use of drug combinations or drugs with broader spectra as a cover for diagnostic imprecision.
• Routine dosage rather than individualized on the basis of clinical situation, microbiological information, and the pharmacological consideration.

34
New Strategies for Antimicrobial Use:
Mutant Prevention Concentration• When 1010 microorganisms are applied to agar
plates containing drug, two point of reduction in viable bacterial cell are seen.
• The first reduction occurred with the MIC drug concentration where the fraction of cfu recovered substantially declined.
• This is followed by a plateau whereby cells containing first-step resistant mutation are present and readily isolated from drug containing plate.

35
First-step mutants
MPC
MIC
Method :
Agar dilution as for MIC but
apply 1010 cells rather than 105
1
10-8
Fra
ctio
n of
col
ony
- fo
rmin
g un
its
reco
vere
d
Log Concentration (Fluoroquinolone)
0
Mutant Prevention Concentration

36
Mutant Prevention Concentration
• If drug concentration is increased, this plateau is decreased whereby the fgrowth of the firs-step resistant mutation is inhibited.
• The drug concentration required to inhibit the growth of this first-step resistant mutant is termed as: “mutant prevention concentration”.

37
Potential
Clearance
Healty immunne system
Time
Immune Threshold Breached
20 000 in 1 billion
Immunocompromised state
Prior Infection
Prior antibotic exposure
Acute infections/failed therapy
200 in 1 billion
MIC
2 in 1 billion

38
New Strategies for Antimicrobial Use
• MIC90: minimum concentration that inhibit 90% of 105 cfu/ml (NCCLS standardized susceptibility testing)
• MPC90: the drug concentration that would require an organism to possess two concurrent mutation for growth in the presence of drug.
• It may also be defined as the MIC of the most first-step resistant cell present in a bacterial population
• Measurement of MPC only apply to those organism deemed to be susceptible to the antimicrobial compound by NCCLS standardized susceptibility testing

39
New Strategies for Antimicrobial Use:Mutant Selection Window
• Another concept related to MPC is the mutant selection window (MSW).
• MSW is defined as the antimicrobial drug concentration lies between the MIC and MPC drug concentration.
• The MSW is, in essence, the “danger zone” for the drug accelerated selection of resistant subpopulation.
• When AM concentration < MIC, neither susceptible nor those that contain first-step resistant mutant will be inhibited, therefore, no selective amplification.

40

41
New Strategies for Antimicrobial Use
• When the drug concentration is > MPC value, both susceptible and first-step resistant cells are inhibited and selective amplification of resistant cells does not occur.
• When drug concentration fall within the MSW, susceptible cells are inhibited as drug concentration exceed the MIC, but first step mutant are not inhibited as the drug concentration is below the MPC.
• The net result of drug concentration falling within the MSW is the selective amplification of resistant population if present in the bacterial population.

42
New Strategies for Antimicrobial Use
• Recent thought seems to suggest that the best way to treat an infectious disease requiring therapy is to kill the pathogens and kill them quickly.
• To do this, one may need to consider the use of more potent agents, higher dosages, with proper dosing frequencies to keep the drug level higher and where possible for shorter duration of therapy.

43
Past vs New Strategies
• Past strategies– That narrow-spectrum agents be used.– That agents be used at the minimum doses
possible based on clinical trial data.– That antibiotic be used for unnecessarily long
period of treatment
• Net Results– Emergence of antimicrobial resistance

44
Past vs New Strategies
• Future strategies– Using more potent (not necessarily broader spectrum)
antimicrobial agent – Using more appropriate (perhaps higher) doses and
more appropriate (more frequent) dosing interval – Using antimicrobial for appropriate (possibly shorter)
duration.
• Net Results– Delaying, reducing or reversing the trends toward
higher antimicrobial resistance rates

45