Embed Size (px)
Citation preview
Finance, Information and Cluster Reporting
Paul StefanoskiDirector of ResourcesBlack Country Partnership Trust Kevin GittinsPbR Finance LeadSouth Staffordshire and Shropshire Healthcare NHS FT
November 2013
1
Mental Health Payment by Results Guidance for 2013/14
The three most important documents are:
•MH Payment by Results Guidance for 2013/14•MH Clustering Tool Booklet 2013/14
(Includes the Cluster Decision Tree chart)•MH Cluster Tool Allocation Algorithm
(Based on Health of the Nation Outcome Scales) (HoNOS)
2
Mental Health Payments by Results Guidance for 2013/14
•Comprehensive guidance can be found on the following website:https://www.gov.uk/government/publications/mental-health-payment-by-results-arrangements-for-2013-14
3
MH Payment by Results (PbR) 2013/14
“PbR is the term given to a payment system based on a standard price or tariff using an agreed contracting currency”
• National Mental Health Contract currency is Care Clusters• Recognise the relationship between Needs, Price and Outcome• Interventions to be based on NICE guidance and Best Practice• Block contracts with an income guarantee to be maintained• Indicative Cluster Review Periods to be used in contracts• Difficulties of having a Single Price for all Commissioners• Unable to have a National Tariff for 2013/14• Develop Payment System linked to Quality Outcomes Measures.• Develop Business Rules for a future Payment System• Improvements to the National Cluster Reference Costs for 2012/13 which will be used to help determine a National Tariff
4
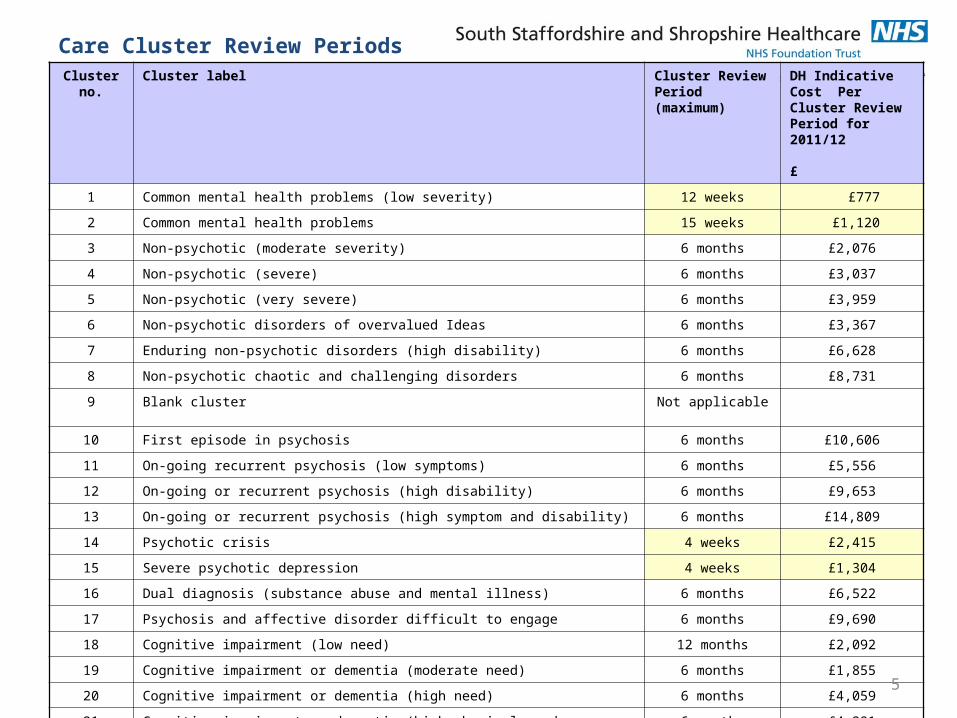
Cluster no.
Cluster label Cluster Review Period (maximum)
DH Indicative Cost Per Cluster Review Period for 2011/12 £
1 Common mental health problems (low severity) 12 weeks £777
2 Common mental health problems 15 weeks £1,120
3 Non-psychotic (moderate severity) 6 months £2,076
4 Non-psychotic (severe) 6 months £3,037
5 Non-psychotic (very severe) 6 months £3,959
6 Non-psychotic disorders of overvalued Ideas 6 months £3,367
7 Enduring non-psychotic disorders (high disability) 6 months £6,628
8 Non-psychotic chaotic and challenging disorders 6 months £8,731
9 Blank cluster Not applicable
10 First episode in psychosis 6 months £10,606
11 On-going recurrent psychosis (low symptoms) 6 months £5,556
12 On-going or recurrent psychosis (high disability) 6 months £9,653
13 On-going or recurrent psychosis (high symptom and disability) 6 months £14,809
14 Psychotic crisis 4 weeks £2,415
15 Severe psychotic depression 4 weeks £1,304
16 Dual diagnosis (substance abuse and mental illness) 6 months £6,522
17 Psychosis and affective disorder difficult to engage 6 months £9,690
18 Cognitive impairment (low need) 12 months £2,092
19 Cognitive impairment or dementia (moderate need) 6 months £1,855
20 Cognitive impairment or dementia (high need) 6 months £4,059
21 Cognitive impairment or dementia (high physical need or engagement) 6 months £4,291
Care Cluster Review Periods
5
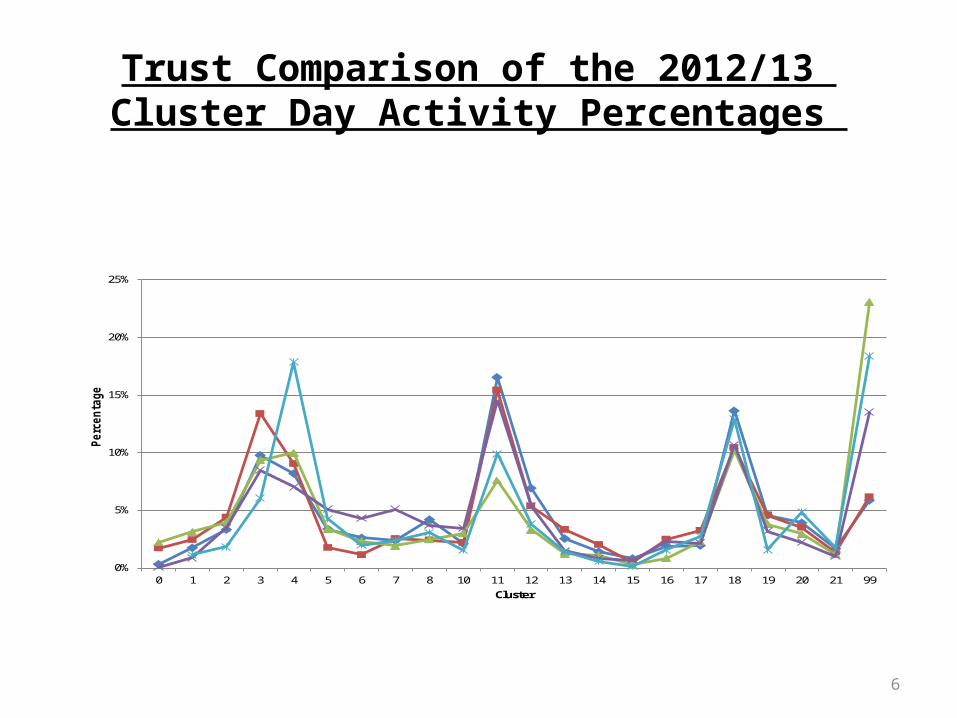
Trust Comparison of the 2012/13 Cluster Day Activity Percentages
6
0%
5%
10%
15%
20%
25%
0 1 2 3 4 5 6 7 8 10 11 12 13 14 15 16 17 18 19 20 21 99
Pe
rce
nta
ge
Cluster
Cluster & PbR Challenges
• Mental Health Trusts are on a journey and working together • Full Clinical Engagement is essential to success• Access to prompt and reliable Clinical information• Clinicians must be involved with developments and be able to drive change• Ensure 100% of Service Users are allocated to Care Cluster• Improve Data Quality and accuracy of Cluster information • Cluster Reviews should be an integral part of Clinical Practice and be linked to CPA Reviews and completed at the same time• Develop Care Pathways, Interventions and Quality Outcome measures for all Clusters using NICE guidance and Best Practice
7
Cluster Reporting Information to Commissioners
• The Trust has been working with it’s main Clinical Commissioning Groups (CCGs) and Commissioning Support Unit (CSU) to improve the accuracy and range of Cluster Reports available to improve the understanding of Clusters, Quality Outcomes and Data Quality Indicators.
8
The Trust provides the following Cluster Reports and Quality Metrics graphs to Commissioners: • Distribution of Cluster Days across all Clusters• Distribution of Service Users Caseload across Clusters• Distribution of Completed Cluster Review Periods across all Clusters • Distribution of Initial Assessments across all Clusters• Average Cluster Days within the Cluster Review Periods across all Clusters
9
Reporting Cluster Information to Commissioners