Embed Size (px)
DESCRIPTION
Tuberculosis New Guidelines
Citation preview
Anti TB Drugs
Evelyn B. Yumiaco M.D.Department of PharmacologySchool of MedicineAngeles University Foundation
Country PictureCountry Picture Population 2007 = 88 Million Global rank – 9th among HBCs Regional rank – 3rd among WPR
countries TB Incidence (New SS+)(New SS+) = 131/100,000 Case Detection Rate 2006 = 74% Cure Rate (New SS+)(New SS+) 2005 = 82% Success Rate (New SS+)(New SS+) 2005 = 90%
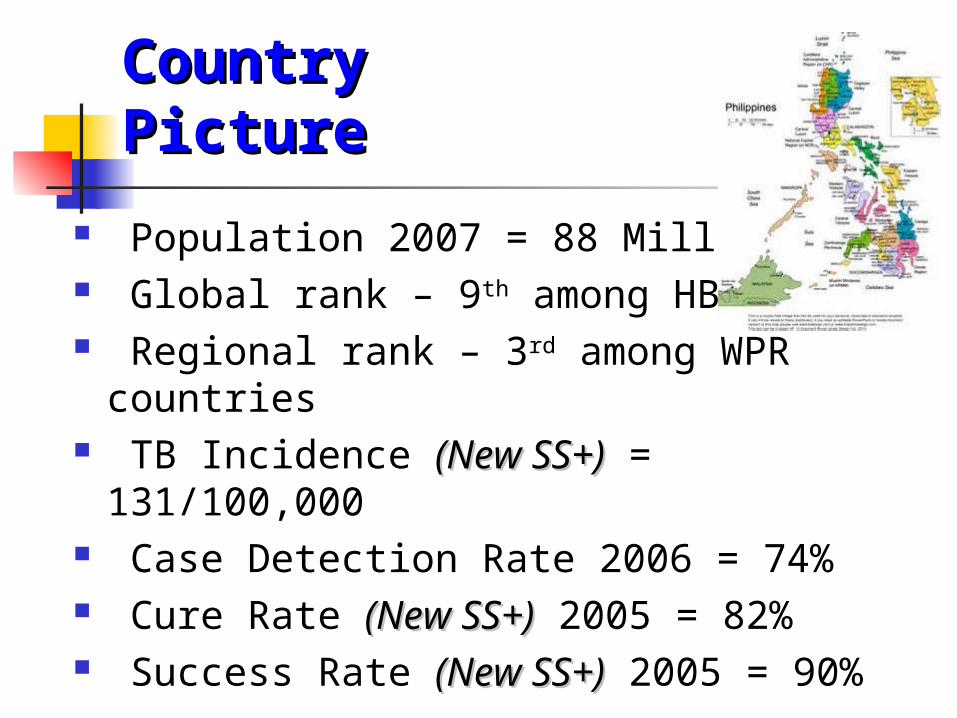
MORBIDITY 2009
1. ARI2. ALTI/PNEUMONIA3. BRONCHITIS/BRONCHIOLITIS4.HYPERTENSION5. ACUTE WATERY DIARRHEA6.INFLUENZA7. UTI8. TB (RESPIRATORY)9. INJURIES10. ACUTE FEBRILE ILLNESS
DEPARTMENT OF HEALTH
MORTALITY 2009
1. DISEASES OF THE HEART2. DISEASES OF THE VASCULAR SYSTEM3. MALIGNANT NEOPLASM4. PNEUMONIA5. ACCIDENTS6. TB (ALL FORMS)7. CHRONICLOWER RESPIRATORY DISEASES8. DIABETES9. NEPHRITIS/NEPHROTIC SYNDROME10. PERINATAL CONDITIONS
DEPARTMENT OF HEALTH
National TB Program Manual of Procedure (MOP)
HON. FRANCISCO T. DUQUE III, MD, MSc.
Secretary of Health Department of Health
December 2005
VISION, MISSION, AND GOAL OF THE NTP Vision: A country where TB is no
longer a public health problem Mission: Ensure that TB DOTS
services are available, accessible, and affordable to the communities in collaboration with the LGUs and other partners
Goal: To reduce prevalence and mortality from TB by half by the year 2015 (Millennium Development Goals)
D irectly
O bserved
T herapy
S hortcourse
A strategy!
DOTS Strategy: Elements
1. Political commitment to tuberculosis control
2. Facilities for the microscopic diagnosis of sputum smear–positive tuberculosis
3. An uninterrupted supply of good quality anti-tuberculosis drugs
4. Direct observation of therapy
5. Good record-keeping to facilitate assessment of the effectiveness of the control program
Direct Observation of Treatment
1. Who will undergo DOT? All smear (+) TB2. Who can be treatment partner?
Staff of the health center or clinic Member of the community such as the BHW,
local government official or former Tb patient. Member of the patient’s family (last priority)
3. Where to do DOT? in any accessible and convenient place (RHU, home, school)
4. How long is the DOT? whole treatment
CASE FINDING THE INDENTIFICATION AND
DIAGNOSIS OF TB CASES AMONG INDIVIDUALS WITH SUSPECTED SIGNS AND SYMPTOMS OF TB
DIRECT SPUTUM SAMPLE MICROSCOPY (DSSM) PRINCIPAL DIAGNOSTIC METHOD
CASE FINDING DIRECT SPUTUM
SAMPLE MICROSCOPY (DSSM) PROVIDES DEFITIVE
DIAGNOSIS PROCEDURE IS SIMPLE ECONOMICAL CAN BE AVAILABLE IN
REMOTE AREAS
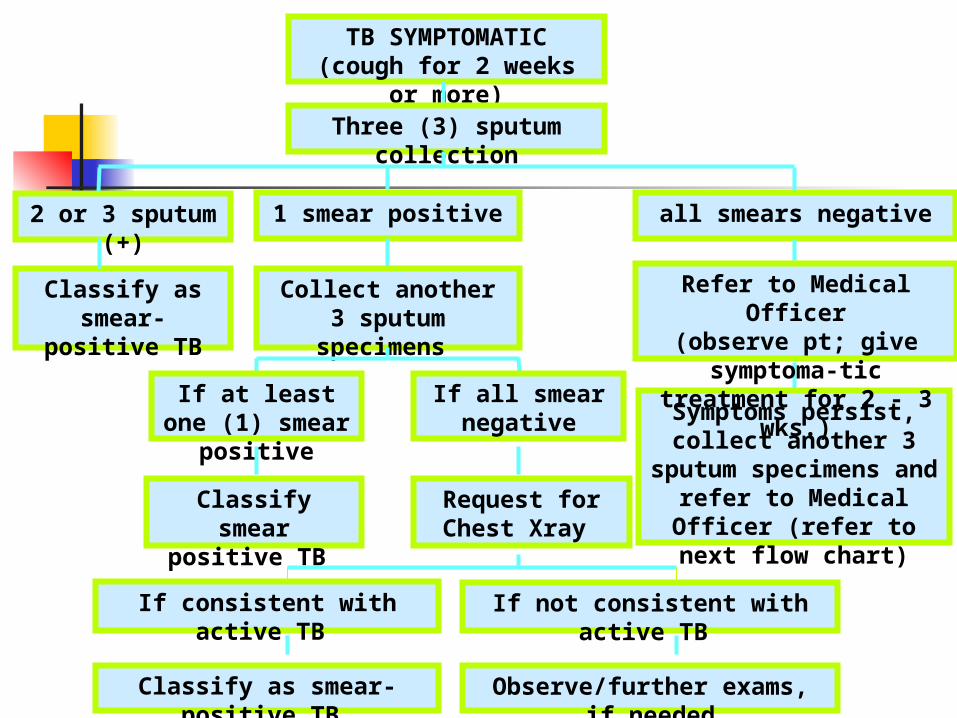
TB SYMPTOMATIC(cough for 2 weeks or more)
Three (3) sputum collection
2 or 3 sputum (+) 1 smear positive all smears negative
Classify as smear-positive TB
Collect another 3 sputum specimens
Symptoms persist, collect another 3 sputum
specimens and refer to Medical Officer (refer to
next flow chart)
If all smear negative
If at least one (1) smear positive
Refer to Medical Officer(observe pt; give symptoma-tic treatment for 2 - 3 wks.)
Classify smear positive TB
Request for Chest Xray
If consistent with active TB If not consistent with active TB
Observe/further exams, if neededClassify as smear-positive TB
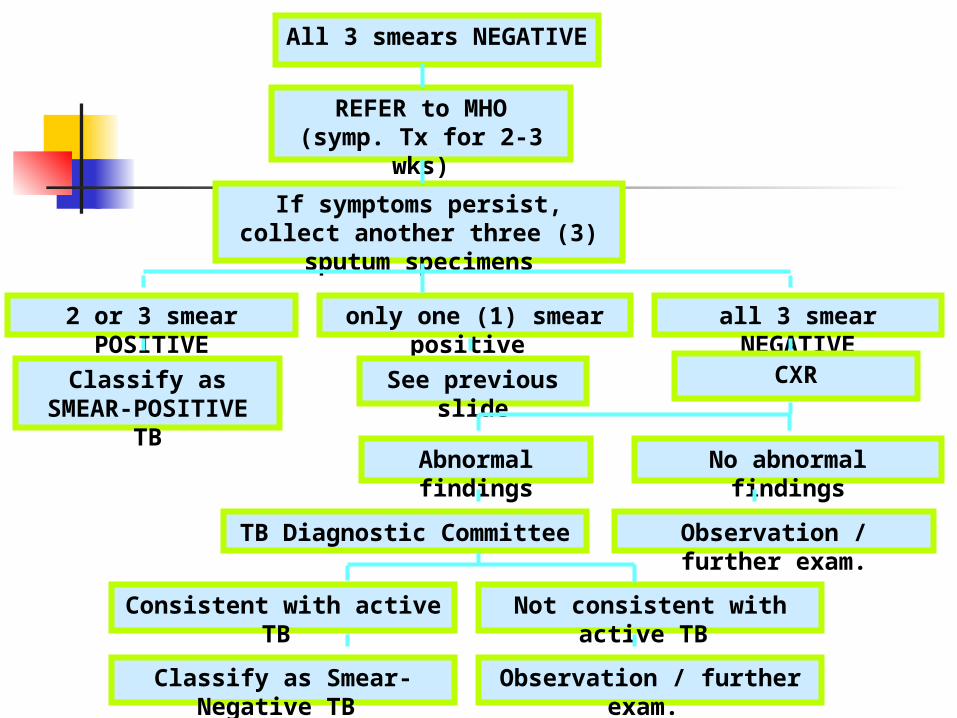
All 3 smears NEGATIVE
REFER to MHO(symp. Tx for 2-3 wks)
If symptoms persist, collect another three (3) sputum specimens
2 or 3 smear POSITIVE only one (1) smear positive all 3 smear NEGATIVE
Classify as SMEAR-POSITIVE TB
See previous slide CXR
Abnormal findings No abnormal findings
TB Diagnostic Committee Observation / further exam.
Consistent with active TB Not consistent with active TB
Classify as Smear-Negative TB Observation / further exam.
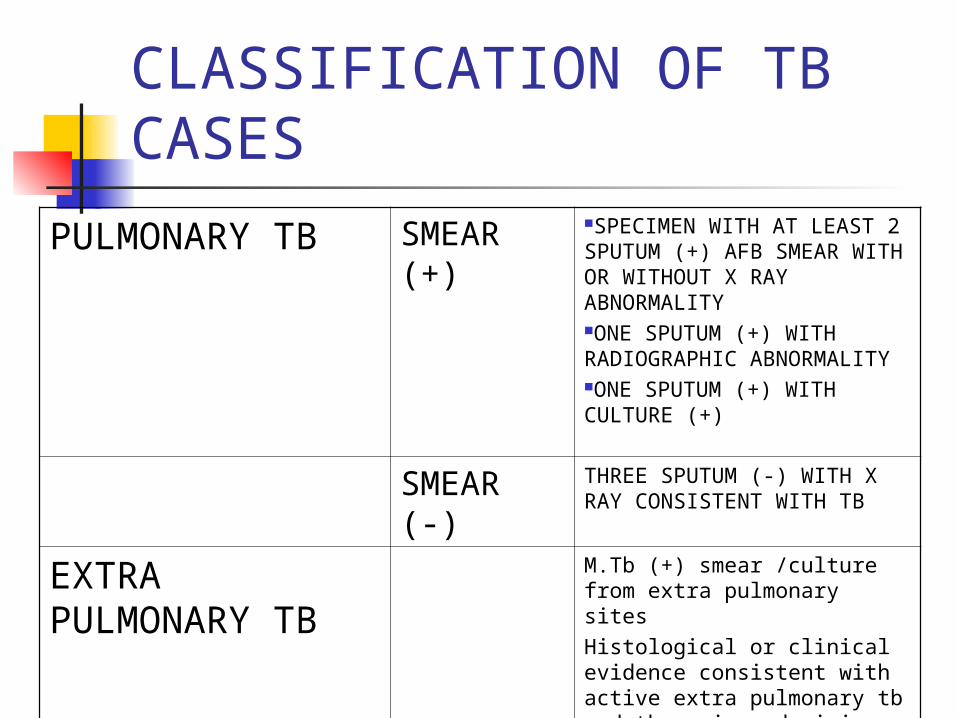
CLASSIFICATION OF TB CASES
PULMONARY TB SMEAR (+)
SPECIMEN WITH AT LEAST 2 SPUTUM (+) AFB SMEAR WITH OR WITHOUT X RAY ABNORMALITYONE SPUTUM (+) WITH RADIOGRAPHIC ABNORMALITYONE SPUTUM (+) WITH CULTURE (+)
SMEAR (-) THREE SPUTUM (-) WITH X RAY CONSISTENT WITH TB
EXTRA PULMONARY TB
M.Tb (+) smear /culture from extra pulmonary sitesHistological or clinical evidence consistent with active extra pulmonary tb and there is a decision to treat
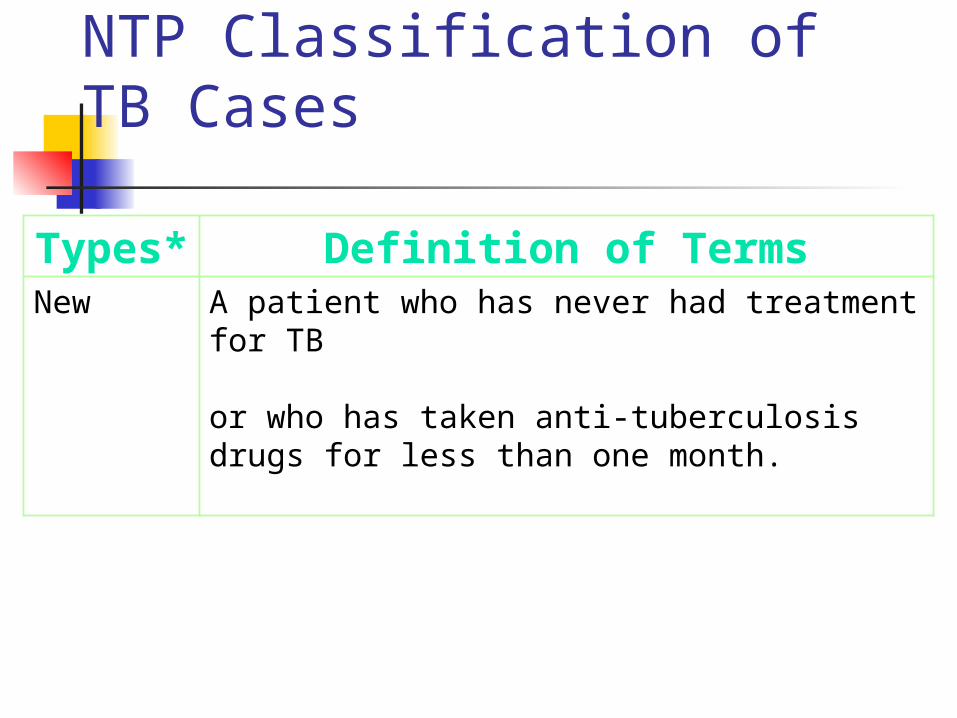
NTP Classification of TB Cases
Types* Definition of TermsNew A patient who has never had treatment for TB
or who has taken anti-tuberculosis drugs for less than one month.
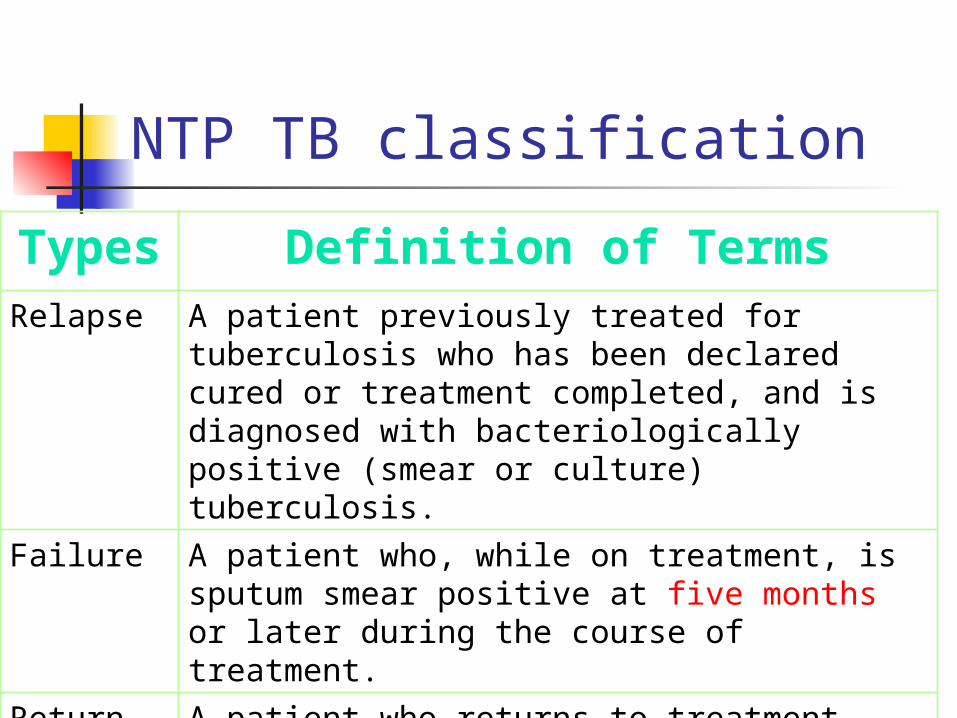
NTP TB classificationTypes Definition of Terms
Relapse A patient previously treated for tuberculosis who has been declared cured or treatment completed, and is diagnosed with bacteriologically positive (smear or culture) tuberculosis.
Failure A patient who, while on treatment, is sputum smear positive at five months or later during the course of treatment.
Return afterDefault (RAD)
A patient who returns to treatment with positive bacteriology (smear or culture), following interruption of treatment for two months or more.
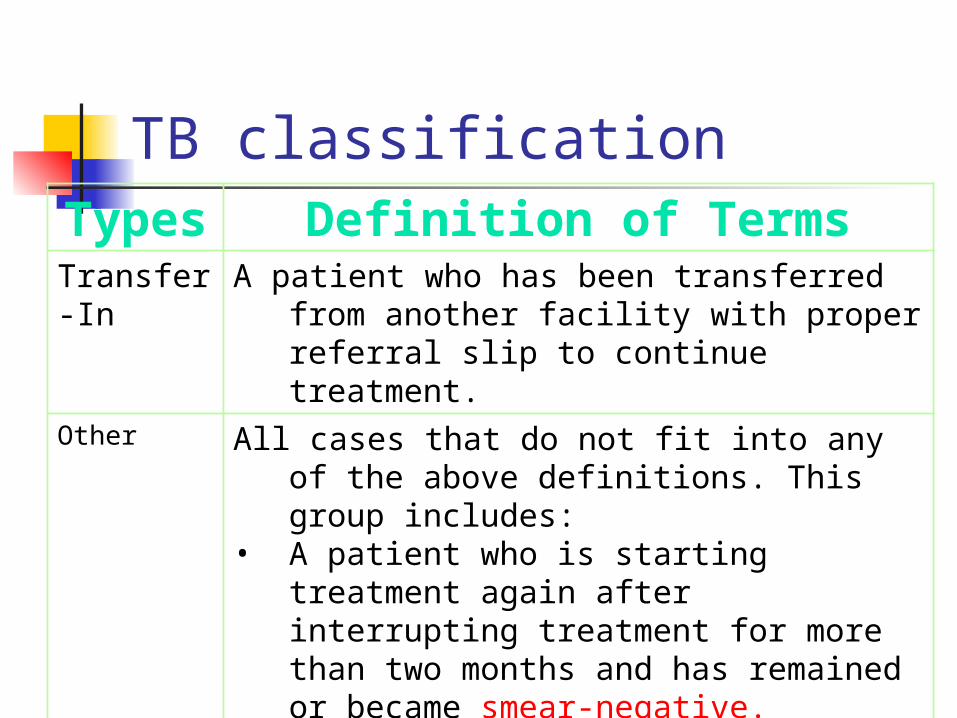
TB classificationTypes Definition of Terms
Transfer-In A patient who has been transferred from another facility with proper referral slip to continue treatment.
Other All cases that do not fit into any of the above definitions. This group includes:
• A patient who is starting treatment again after interrupting treatment for more than two months and has remained or became smear-negative.
• A sputum smear negative patient initially before starting treatment and became sputum smear-positive during the tx.
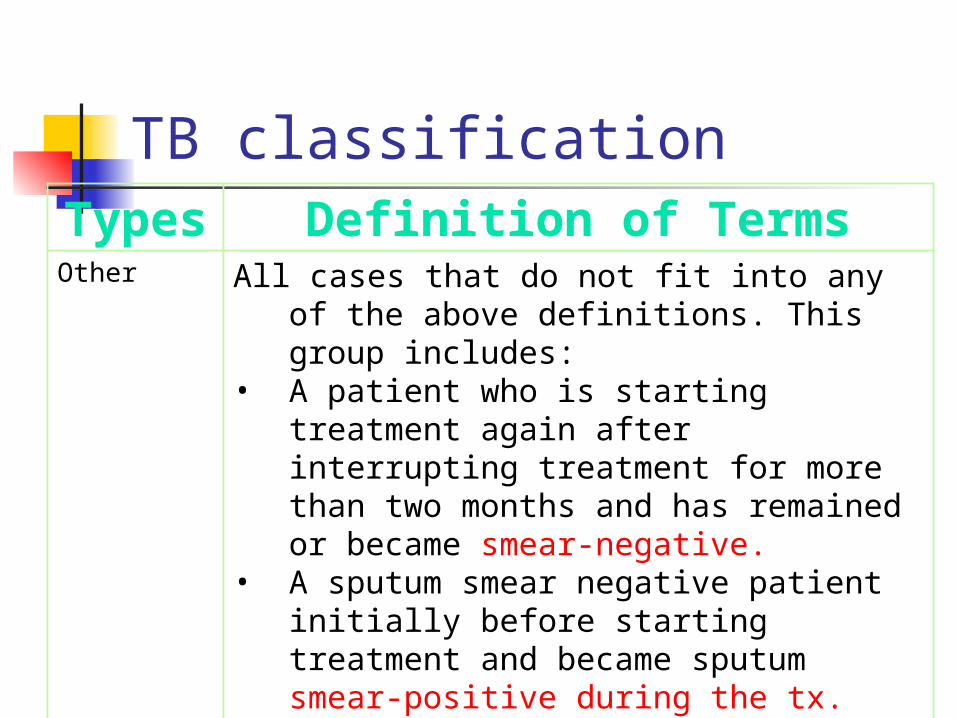
TB classificationTypes Definition of Terms
Other All cases that do not fit into any of the above definitions. This group includes:
• A patient who is starting treatment again after interrupting treatment for more than two months and has remained or became smear-negative.
• A sputum smear negative patient initially before starting treatment and became sputum smear-positive during the tx.
• Chronic case-remained sputum (+) at the end of treatment
NTP: Outcomes of Treatment Treatment Completed
a patient who has completed treatment but has not met the criteria for cure or failure
A sputum smear-positive patient who has completed treatment but without DSSM follow - up during the treatment, or with only one negative DSSM during the treatment, or without DSSM in the last month of treatment.
Sputum smear negative who has completed treatment
NTP: Outcomes of Treatment Cure
a sputum smear-positive patient who has completed treatment and is sputum smear negative in the last month of treatment and on at least one previous occasion in the continuation phase
NTP: Outcomes of Treatment Died
a patient who died for any reason during the course of treatment
Transfer out A patient who transferred to another
DOTS facility with proper referral slip for continuation of treatment and whose treatment outcome is not known
NTP: Outcomes of Treatment Defaulted - a patient who
interrupted treatment for two consecutive months or more
NTP: Outcomes of Treatment Failed
A patient who is sputum smear-positive at five months or later during the treatment
An initially sputum smear-negative patient before starting treatment who becomes smear-positive during the treatment. (Note: This case will be re-registered as Other with a new TB case number.)
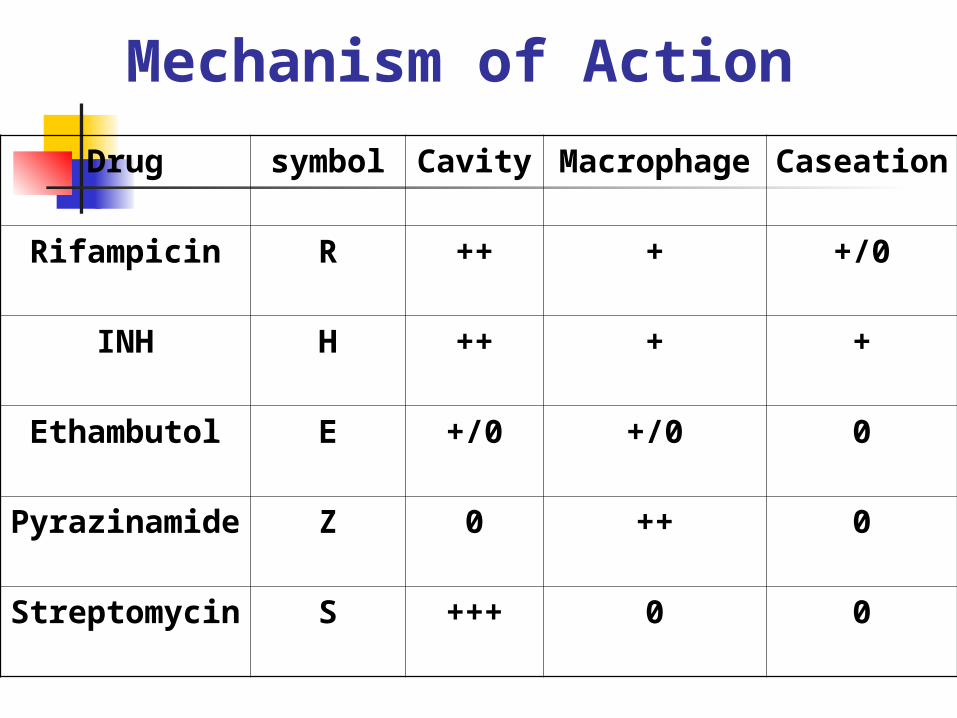
Drug symbol Cavity Macrophage Caseation
Rifampicin R ++ + +/0
INH H ++ + +
Ethambutol E +/0 +/0 0
Pyrazinamide Z 0 ++ 0
Streptomycin S +++ 0 0
Mechanism of Action
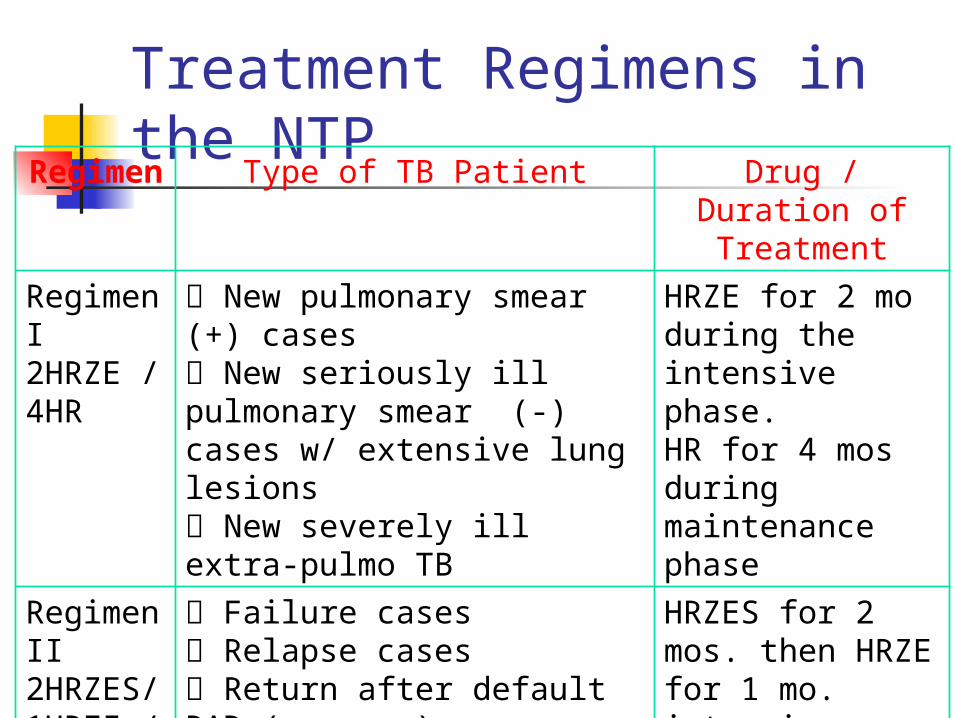
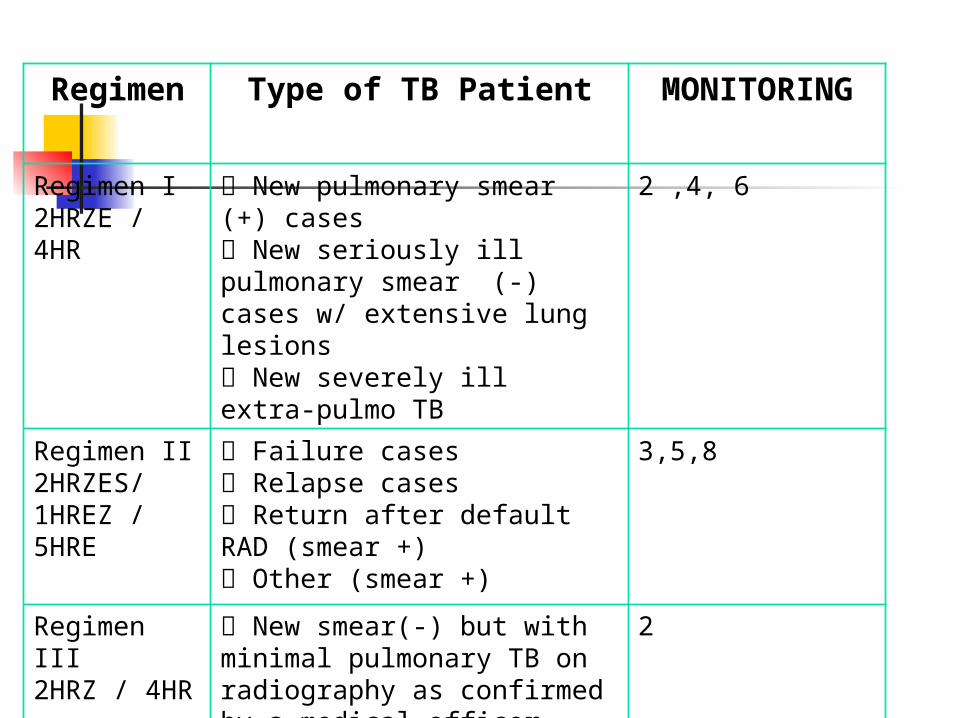
Treatment Regimens in the NTP
Regimen Type of TB Patient Drug / Duration of Treatment
Regimen I 2HRZE / 4HR
New pulmonary smear (+) cases New seriously ill pulmonary smear (-) cases w/ extensive lung lesions New severely ill extra-pulmo TB
HRZE for 2 mo during the intensive phase.HR for 4 mos during maintenance phase
Regimen II2HRZES/1HREZ / 5HRE
Failure cases Relapse cases Return after default RAD (smear +) Other (smear +)
HRZES for 2 mos. then HRZE for 1 mo. intensive phase.HRE for 5 mos as maintenance phase
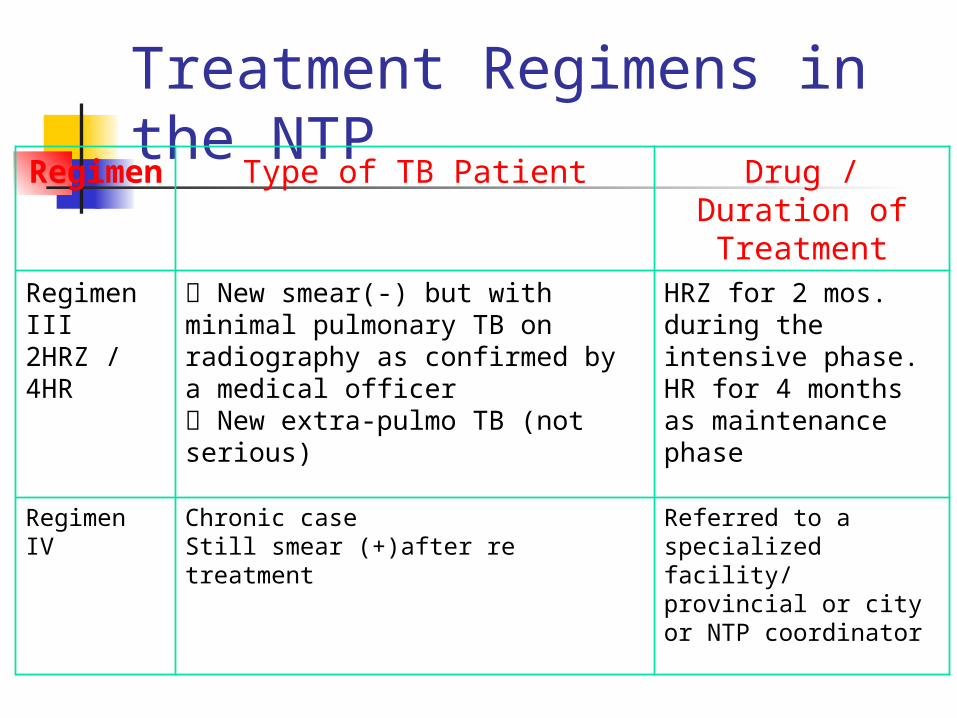
Treatment Regimens in the NTP
Regimen Type of TB Patient Drug / Duration of Treatment
Regimen III2HRZ / 4HR
New smear(-) but with minimal pulmonary TB on radiography as confirmed by a medical officer New extra-pulmo TB (not serious)
HRZ for 2 mos. during the intensive phase.HR for 4 months as maintenance phase
Regimen IV Chronic case Still smear (+)after re treatment
Referred to a specialized facility/ provincial or city or NTP coordinator
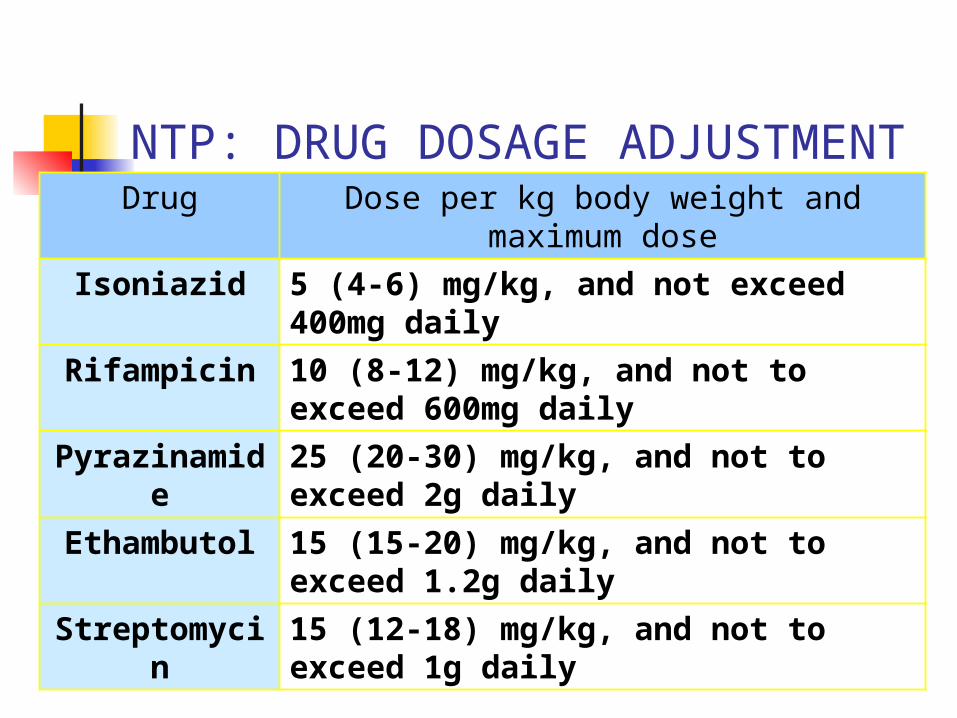
NTP: DRUG DOSAGE ADJUSTMENT
Drug Dose per kg body weight and maximum dose
Isoniazid 5 (4-6) mg/kg, and not exceed 400mg daily
Rifampicin 10 (8-12) mg/kg, and not to exceed 600mg daily
Pyrazinamide
25 (20-30) mg/kg, and not to exceed 2g daily
Ethambutol 15 (15-20) mg/kg, and not to exceed 1.2g daily
Streptomycin
15 (12-18) mg/kg, and not to exceed 1g daily
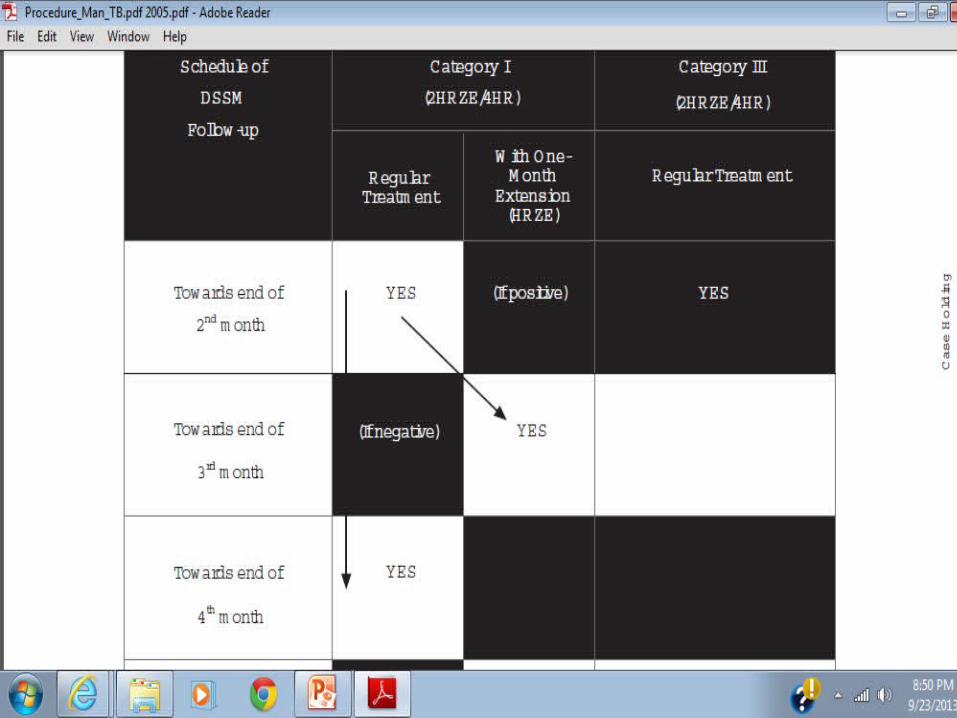
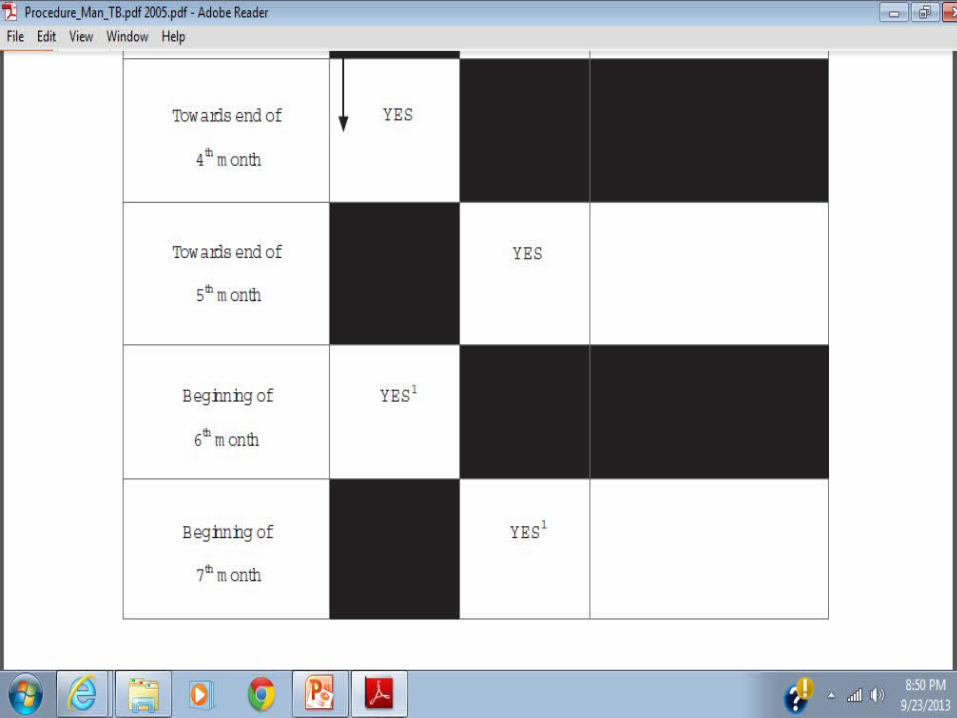
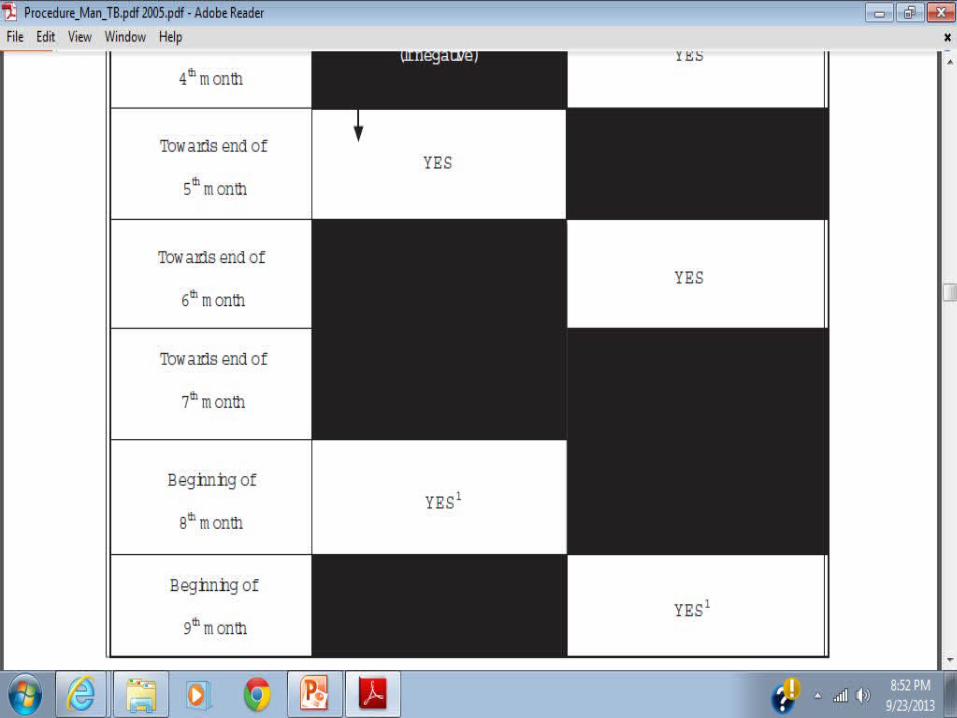
Regimen Type of TB Patient MONITORING
Regimen I 2HRZE / 4HR
New pulmonary smear (+) cases New seriously ill pulmonary smear (-) cases w/ extensive lung lesions New severely ill extra-pulmo TB
2 ,4, 6
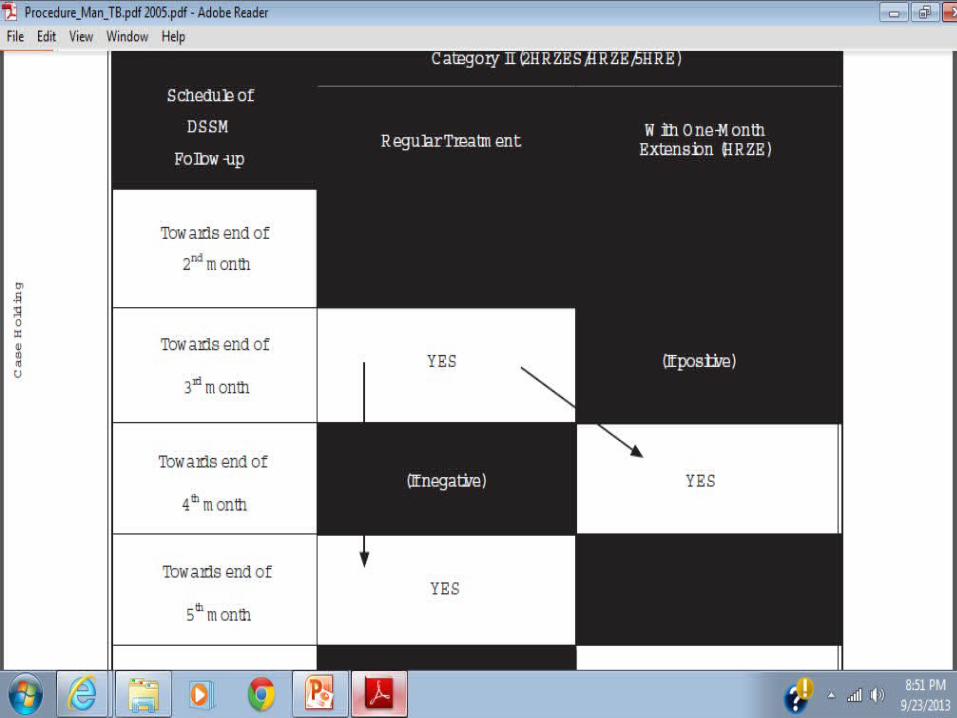
Regimen II2HRZES/1HREZ / 5HRE
Failure cases Relapse cases Return after default RAD (smear +) Other (smear +)
3,5,8
Regimen III2HRZ / 4HR
New smear(-) but with minimal pulmonary TB on radiography as confirmed by a medical officer New extra-pulmo TB (not serious)
2
Private Public Mix DOTSSTRATEGY ADOPTED BY THE NTP1. INCREASE CASE DETECTION2. SYNCHRONIZE DIAGNOSIS AND
TREATMENT IN THE PRIVATE AND PUBLIC SECTOR
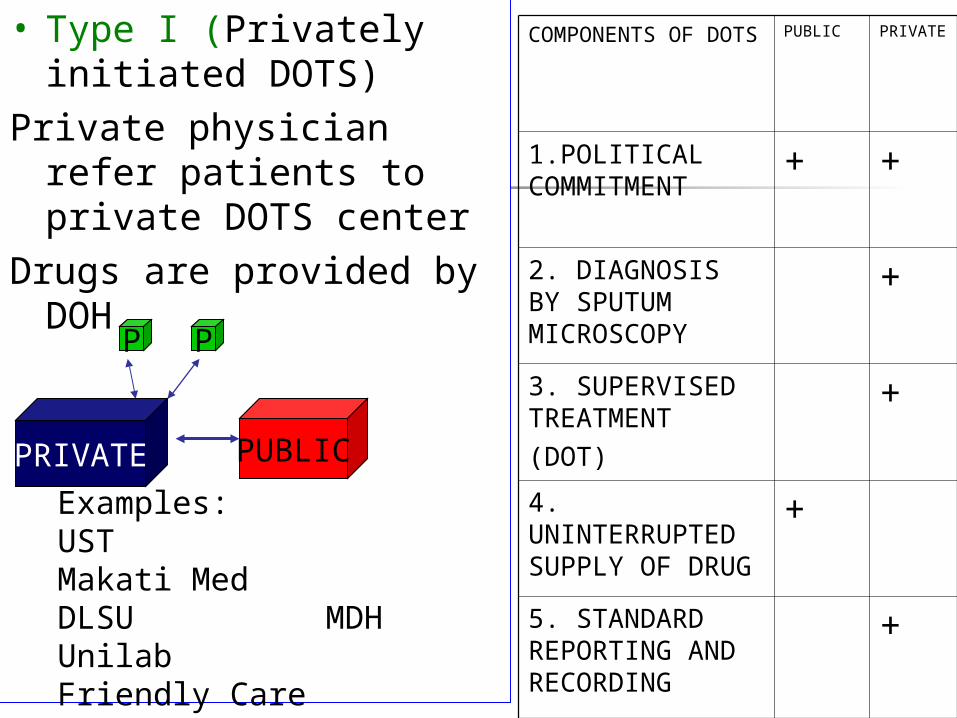
• Type I (Privately initiated DOTS)
Private physician refer patients to private DOTS center
Drugs are provided by DOH
PUBLIC
P
PRIVATE
P
Examples:UST Makati MedDLSU MDHUnilab Friendly CareAUFMC UERM
COMPONENTS OF DOTS
PUBLIC PRIVATE
1.POLITICAL COMMITMENT + +
2. DIAGNOSIS BY SPUTUM MICROSCOPY
+
3. SUPERVISED TREATMENT(DOT)
+
4. UNINTERRUPTED SUPPLY OF DRUG
+
5. STANDARD REPORTING AND RECORDING
+
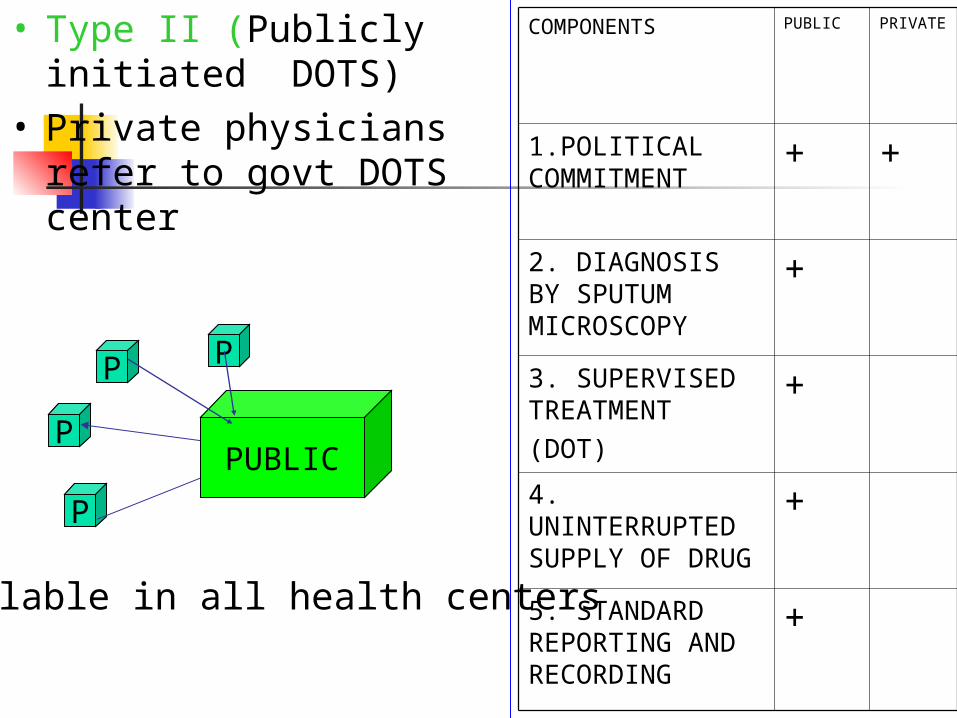
COMPONENTS PUBLIC PRIVATE
1.POLITICAL COMMITMENT + +
2. DIAGNOSIS BY SPUTUM MICROSCOPY
+
3. SUPERVISED TREATMENT(DOT)
+
4. UNINTERRUPTED SUPPLY OF DRUG
+
5. STANDARD REPORTING AND RECORDING
+
• Type II (Publicly initiated DOTS)
• Private physicians refer to govt DOTS center
P
P
PP
PUBLIC
Available in all health centers









![Update on TB-IRIS Meintjes - TB IRIS (27 Nov, 13h30).pdf · Update on TB-IRIS Graeme Meintjes ... new pleural effusion. ... SA HIV conference_TBIRIS_27Nov2012.ppt [Compatibility Mode]](https://img.pdfslide.us/doc/110x75/5ac1ad627f8b9ae45b8da39e/update-on-tb-meintjes-tb-iris-27-nov-13h30pdfupdate-on-tb-iris-graeme-meintjes.jpg)
![TB Activist Toolkit - TB Basics [Facilitators Notes]](https://img.pdfslide.us/doc/110x75/568c366e1a28ab02359801e7/tb-activist-toolkit-tb-basics-facilitators-notes.jpg)