Embed Size (px)
Citation preview
Enterprise | Interest
Nothing to declare
Joint Slide Seminar Pathology in Favour of Developing Countries & AORTIC/APOFDr. Maria Elena Laurenti, Dr. Kakule Musafiri Alphonse,
Dr. Fenocchio Daniela
CASE 8
Clinical History
77 years-old male
Firm, palpable mass of about 40 mm of greatest diameter, adherent to muscolaris fascia and subcutaneous tissue.
The overlying skin was retracted but not ulcerated.
Management
A FNAB was performed and digital selected images of microscopic representative
fields were sent through the Internet for diagnostic purpose to an Italian network
of pathologists within a program of collaboration between Anoalite Hospital of
Mungbere, Democratic Republic of Congo (AHM) and the Italian NGO “Associazione
Patologi Oltre Frontiera (APOF).
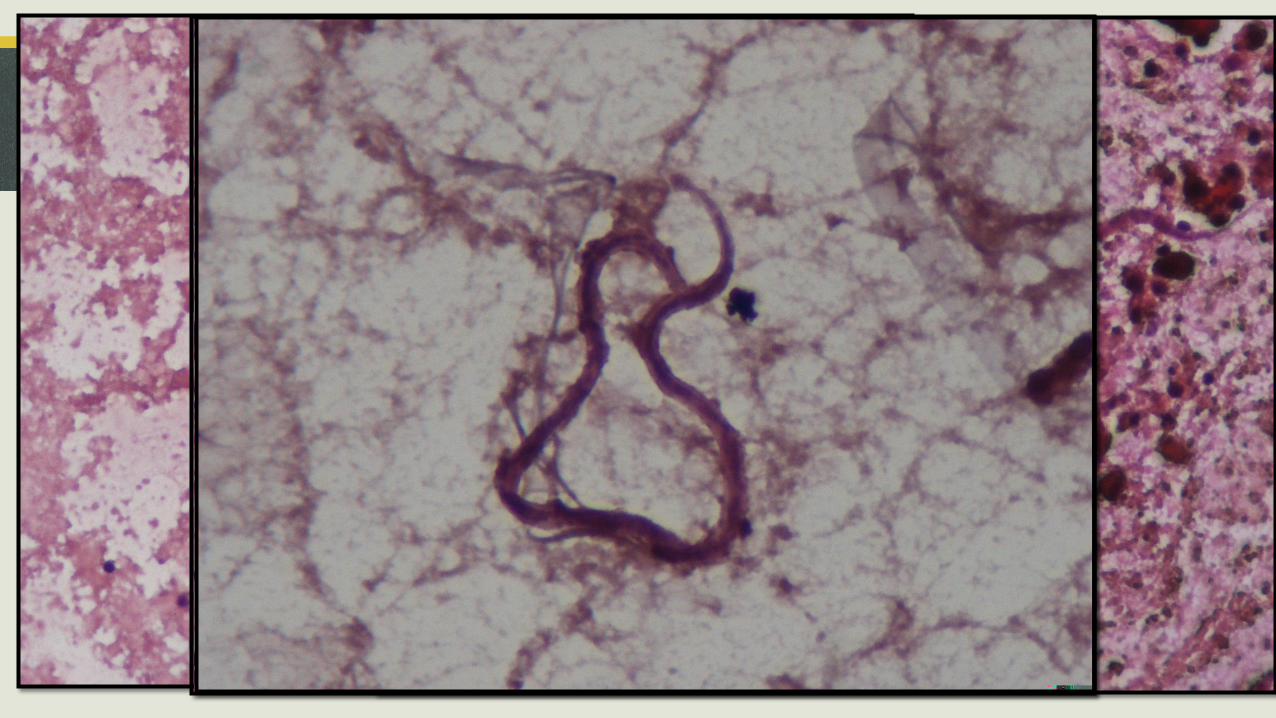
Cytology
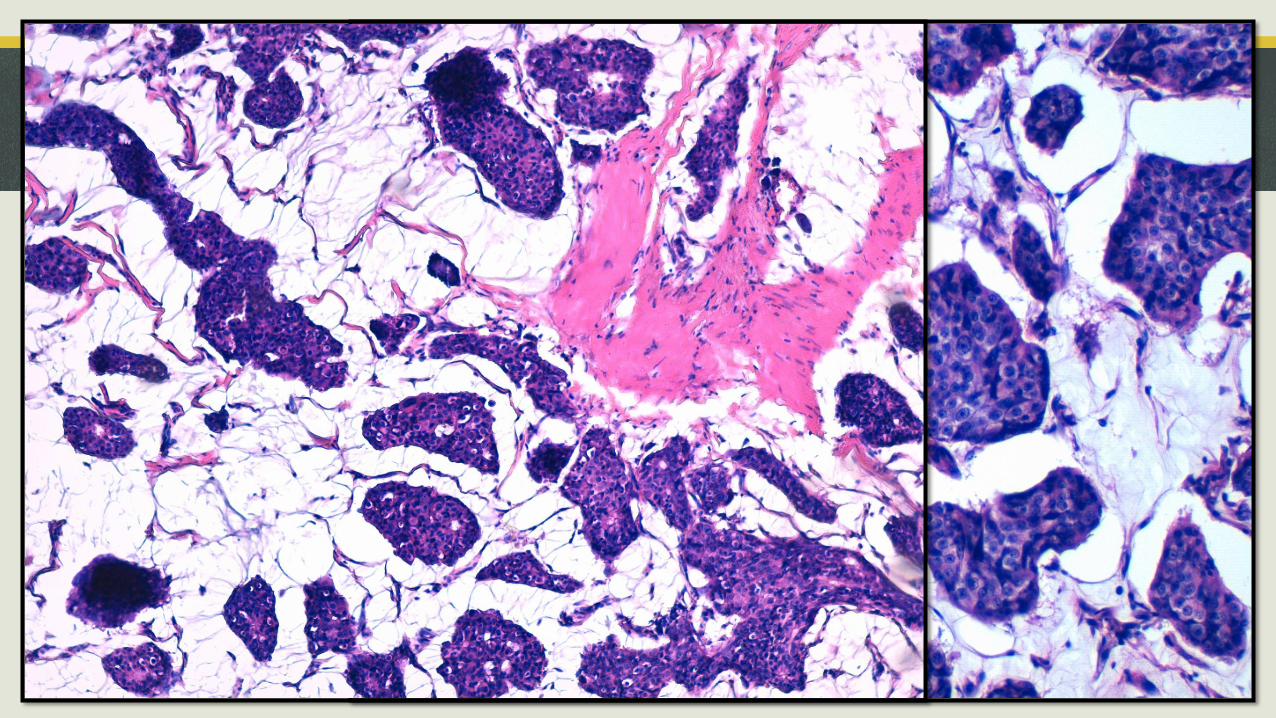
Histology
10X 20X
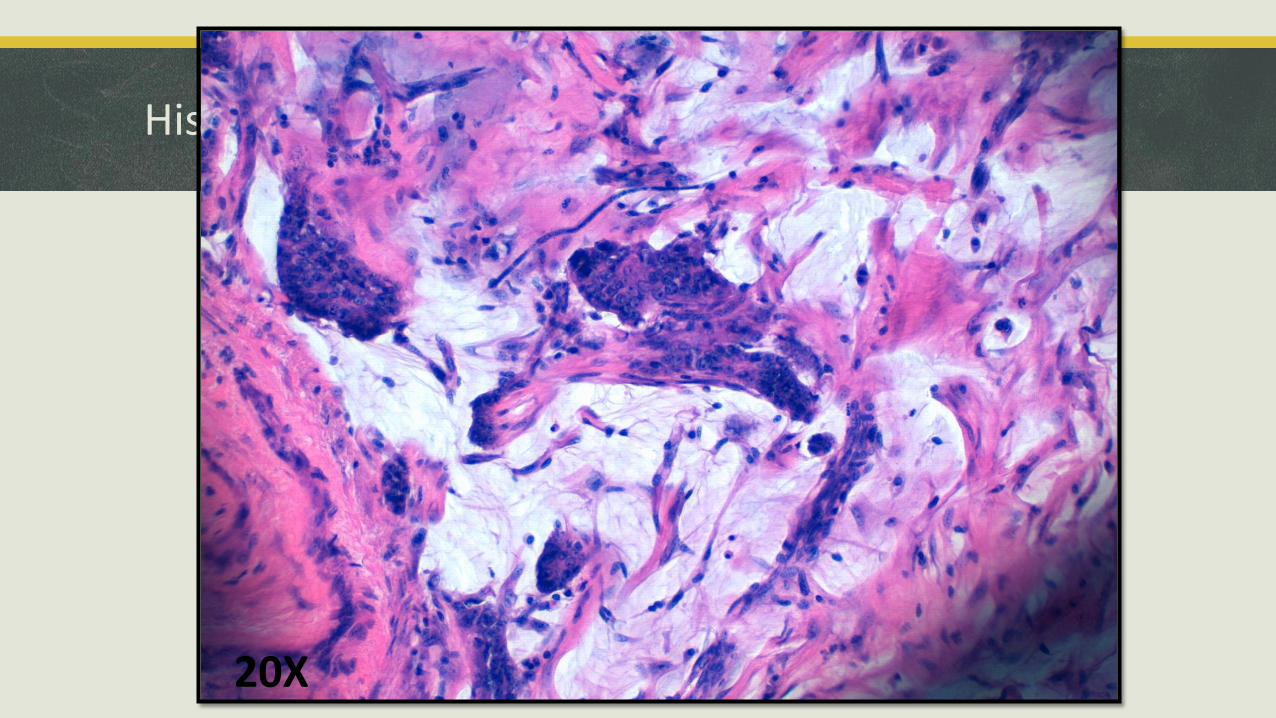
Histology
20X
MALE BREAST CARCINOMA: EPIDEMIOLOGY
Very rare
Have higher risk for second primary [breast, stomach and melanoma (Breast Cancer Res 2007)]
In U.S., males have 1% the rate of breast carcinoma of women; 1000 - 1500 new cases per year in U.S.
Mean age 60 years at diagnosis
Histology similar to women, mostly ductal and most ER+
MALE BREAST CARCINOMA: RISK FACTORS
Breast carcinoma in first degree relatives
BRCA2 > BRCA1 mutation carriers
Older age
Infertility
Obesity
Ionizing radiation
Klinefelter's syndrome (50X risk)
Estrogen treatment for prostate carcinoma or cirrhosis
MALE BREAST CARCINOMA: CLINICAL AND PATHOLOGICAL FEATURES
Nipple discharge in men is strongly suggestive
Often presents at high stage since minimal breast substance
Axillary nodes involved in 50% at presentation
Same pathological classification as for women, same prognostic and predictive factors.
Luminal A and B subtypes are most common
FILARIASIS: AT A GLANCE
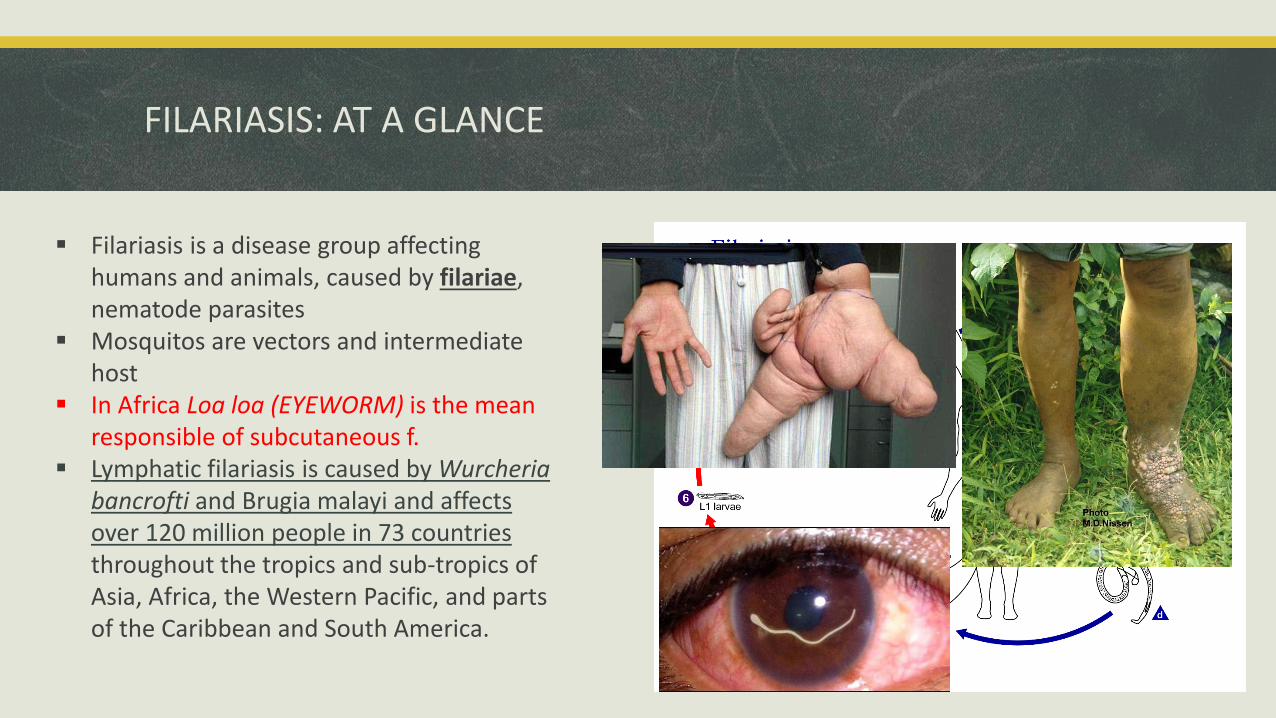
Filariasis is a disease group affecting humans and animals, caused by filariae, nematode parasites
Mosquitos are vectors and intermediate host
In Africa Loa loa (EYEWORM) is the mean responsible of subcutaneous f.
Lymphatic filariasis is caused by Wurcheriabancrofti and Brugia malayi and affects over 120 million people in 73 countries throughout the tropics and sub-tropics of Asia, Africa, the Western Pacific, and parts of the Caribbean and South America.
FILARIASIS IN FNAC: LITERATURE
Tropical Parasitology. 2012;2(1):61-63. doi:10.4103/2229-5070.97244
Diagn Cytopathol. 2012 Apr;40(4):292-6. doi: 10.1002/dc.21557. Epub 2010 Nov 22Journal of Cytology. 2017;34(1):43-45. doi:10.4103/0970-9371.197617
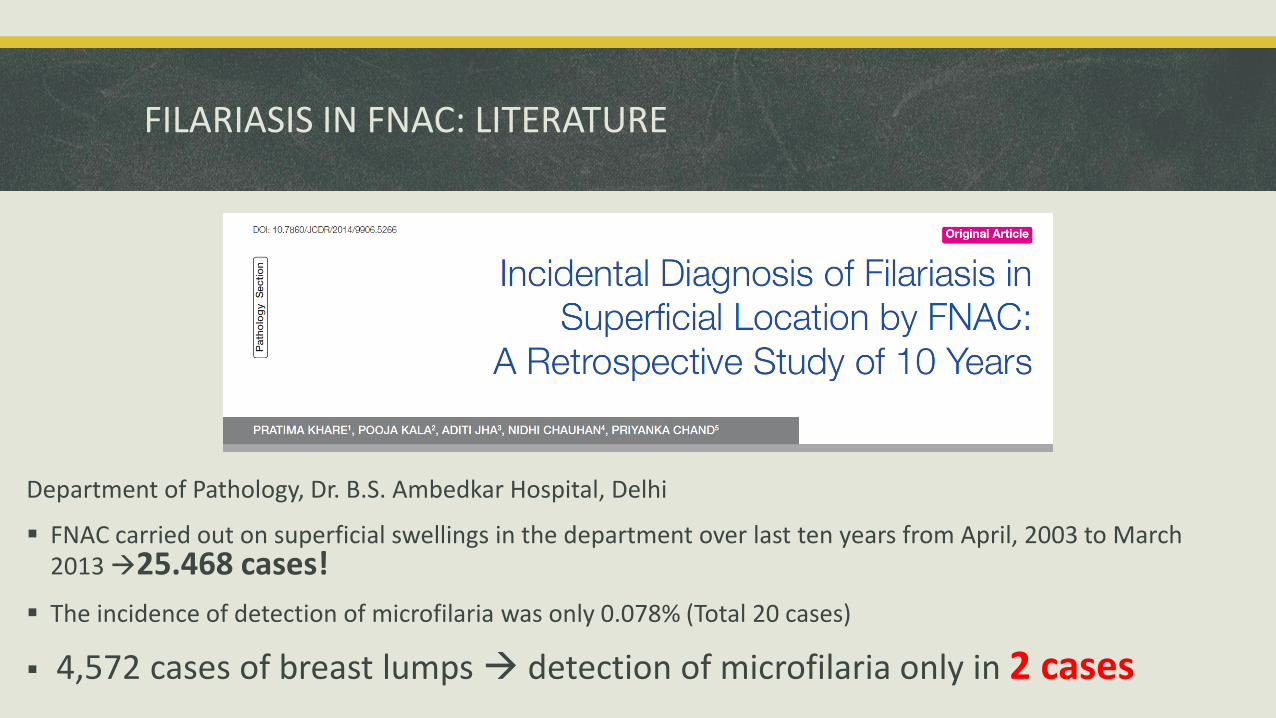
Department of Pathology, Dr. B.S. Ambedkar Hospital, Delhi
FNAC carried out on superficial swellings in the department over last ten years from April, 2003 to March 2013 25.468 cases!
The incidence of detection of microfilaria was only 0.078% (Total 20 cases)
4,572 cases of breast lumps detection of microfilaria only in 2 cases
FILARIASIS IN FNAC: LITERATURE
FILARIASIS OUT OF NODES
In most of the reported cases microfilaria have been detected in skin, soft tissue swelling, breast, epididymis, thyroid gland nodule, salivary gland, cervicovaginalsmears, ovarian cysts, effusion fluids, urine, bronchial, laryngeal and pharyngeal brushings.
AND IN NEOPLASMS?!
Larva may be present in the vasculature and aspiration may lead to the rupture of vessel and release of microfilaria into the aspirate from neoplasm.
Sparse reports are available about microfilariae in neoplasms, the real incidence is not established since there is no systematic review of the literature at the moment
FILARIASIS OUT OF NODES: BREAST
Microfilaria enter the lymphatic vessels of mammary gland (upper outerquadrant mostly) and develop into adult worms, disrupting lymphatic drainage
Intact adult worms produce minimal tissue reaction but can cause obstructionleading to lymphedema (peau d'orange skin: mimics malignancy)
Degenerating / dying worms provoke an inflammatory reaction forming a mass with eosinophilic and granulomatous inflammation
Secondary lymphangitis and fibrosis may result
Some of the inflammation is in response to antigens of the endosymbiotic bacteria Wolbachia, which the filarial worms contain!
TAKE HOME MESSAGE
Filariasis is ENDEMIC in many Countries of tropical and sub-tropical areas
Patiens often do not show clear symptoms/do not refer any previous infection
It is possible to find these worms in FNAC/FNAB an cytology smears done for many different purpuse (e.g. oncologic diagnosis, pap test) and it is important to recognize them in order to set the proper therapy
Bibliography
Varghese R, Raghuveer CV, Pai MR, Bansal R. Microfilariae in cytologic smears: A report of six cases. Acta Cytol. 1996;40:299–301. Yenkeshwar PN, Kumbhalkar DT, Bobhate SK. Microfilariae in fine needle aspirates: A report of 22 cases. Indian J Pathol Microbiol. 2006;49:365–9 Kolte SS, Satarkar RN, Mane PM. Microfilaria concomitant with metastatic deposits of adenocarcinoma in lymphnode fine needle aspiration cytology: A chance finding. J Cytol. 2010;27:78–80 Gupta S, Sodhani P, Jain S, Kumar N. Microfilariae in association with neoplastic lesions: Report of five cases. Cytopathology. 2001;12:120–6 Gupta K, Sehgal A, Puri MM, Sidhwa HK. Microfilariae in association with other diseases. A report of six cases. Acta Cytol. 2002;46:776–8 Ahluwalia C, Choudhary M, Bajaj P. Incidental detection of microfilariae in aspirates from Ewing's sarcoma of bone. Diagn Cytopathol. 2003;29:31–2 Thakur M, Lhamo Y. Breast filariasis. Journal of Surgical Case Reports. 2014;2014(1):rjt128