Embed Size (px)
Citation preview

Effects of Long-Acting Insulin Analogues on Breast and Colon Cancer
Promotion
by
Eunhyoung Ko
A thesis submitted in conformity with the requirements
for the degree of Master of Science
Department of Physiology
University of Toronto
© Copyright by Eunhyoung Ko (2014)

ii
Effects of Long-Acting Insulin Analogues on Breast and Colon Cancer
Promotion
Eunhyoung Ko
Master of Science
Department of Physiology
University of Toronto
2014
Abstract
Insulin glargine, a long-acting insulin analogue, has been implicated in increased cancer risk by
epidemiological studies and has been reported to increase mitogenicity in in vitro studies.
However, studies in preclinical models confirming the tumor promoting effect of glargine are
lacking. Methylnitrosourea and azoxymethane treated female Sprague-Dawley rats were
randomly assigned to receive saline, neutral protamine Hagedorn (NPH, unmodified insulin),
glargine, or detemir (long-acting insulin analogues) for 6 weeks (30/group). Rats treated with
NPH had significantly higher mammary tumour multiplicity and a tendency to increased tumour
incidence. Mammary tumour burden tended to increase in all insulin-treated rats compared to
control. There was no effect of insulin on aberrant crypt foci, a precursor of colon cancer,
compared to control. These data suggest that glargine does not promote breast or colon cancer to
a greater extent than unmodified insulin. This is important information in the management of
patients with diabetes.

iii
Acknowledgments
I would first and foremost like to thank my supervisor, Dr. Adria Giacca, for all the
assistance that she has provided during this project. The tasks were not always easy, but with her
guidance and patience we were able to succeed. I could not have finished this research without
her and I am deeply grateful for the incredible opportunity- she provided me to develop both
academically and personally. I feel privileged to have such a considerate and caring supervisor.
Furthermore, I would like to thank all my colleagues in the Giacca lab including Simon
Chang, June Gua, Alex Ivovic, Sandra Peirera, Tejas Desai, Khajag Koulajian, Tiffany Yu,
Linda Qu, Stuart Wiber, and Yuri Crispim de Moraes. The project students, Linda and Stuart,
and a medical student, Yuri, assisted me on taking metabolic measurements and sacrificing rats.
Your advice and encouragement throughout my project truly made my experience enjoyable and
memorable. I would also like to thank Loretta Lam for all her technical assistance and guidance.
Another special thank you to Rudolf Furrer, who injected the rats with the carcinogens, taught
me the techniques of chemical carcinogenesis, and supported me from the very beginning with
words of wisdom and encouragement. I am also very grateful to my supervisory committee
members Dr. Young-In Kim and Dr. George Fantus for their suggestions and guidance
throughout my project. They continued to encourage me and support me on my project and
future career.
Finally, I would like to thank all my friends and family for all their support throughout
the years. Your continued encouragement and understanding helped make difficult times easier
to get through and good times all the more enjoyable. For that I am forever grateful.

iv
Table of Contents
Abstract................................................................................................... ...................................ii
Acknowledgements................................................................................................... ................iii
Table of Contents.................................................................................................. ....................iv
List of Abbreviations.......................................................................................... ......................vii
List of Tables.................................................................................................... .........................ix
List of Figures................................................................................................ .............................x
Chapter 1: Introduction.............................................................................. .................................1
1.1 Diabetes............................................................................................. ....................................1
1.2 Insulin Treatment............................................................................ ......................................2
1.2.1 Regular Human Insulin.............................................................................................2
1.2.2 Long-Acting Insulin Analogues................................................................................3
1.3 Insulin Receptor (IR), Insulin-like Growth Factor-1 Receptor (IGF-1R), and Hybrid
receptors............................................................................................ ..........................................5
1.4 Diabetes, Obesity, Insulin Resistance, Inflammation, and Cancer............ ...........................8
1.5 Insulin Therapy, Insulin-like growth factor (IGF)-1 and Cancer Risk:
Focusing on Breast and Colon Cancer.................................... .................................................10
1.5.1 Insulin, IGF-1, and Cancer......................................................................................10
1.5.1.1 Epidemiological studies............................................................................10
1.5.1.2 In Vitro studies.........................................................................................12
1.5.1.3 In Vivo studies...........................................................................................12
1.5.2 Insulin Analogues and Cancer.................................................................................13
1.5.2.1 B10Asp.....................................................................................................13
1.5.2.2 Long-Acting Insulin analogues.................................................................14
1.5.2.2.1 Epidemiological studies.............................................................14
1.5.2.2.2 In Vitro Studies..........................................................................17
1.5.2.2.3 In Vivo Studies...........................................................................18
1.6 Multistage Model of Chemically-Initiated Carcinogenesis....................... .........................20
1.6.1 Initiation..................................................................................................................20
1.6.2Promotion.................................................................................................................21
1.6.3 Malignant Conversion.............................................................................................21

v
1.6.4 Progression..............................................................................................................21
1.7 Breast and Colon Cancer Animal Models using Carcinogen................... ..........................21
1.7.1 Breast Cancer Model - Methylnitrosourea (MNU) ................................................21
1.7.2 Colon Cancer Model - Azoxymethane (AOM) ......................................................22
1.7.3 Aberrant Crypt Foci (ACF) ....................................................................................23
1.7.4 Dual-Organ Carcinogenesis Model.........................................................................23
1.8 Rationale and Significance..................................................................... ............................24
1.9 Hypothesis............................................................................................ ..............................24
Chapter 2: Materials and Methods................................................. ..........................................25
2.1 Procedure............................................................................... .............................................25
2.1.1 Experimental Animal Model and Sacrifice Procedures...............................25
2.1.1.1 Animals ....................................................................................................26
2.1.1.2 Carcinogen Preparation............................................................................26
2.1.1.3 Injections...................................................................................................27
2.1.1.3.1 Carcinogens...............................................................................27
2.1.1.3.2 Insulin........................................................................................27
2.1.1.4 Rat Monitoring..........................................................................................27
2.1.1.5 Sacrifice....................................................................................................28
2.2 Tumour Evaluation Methods................................................................. .............................28
2.2.1 Mammary Tumour Analysis....................................................................................28
2.2.2 Western Blots...........................................................................................................28
2.2.3 ACF Scoring............................................................................................................29
2.3 Calculations......................................................................................... ...............................29
2.3.1 Power Calculations..................................................................................................29
2.3.2 Statistical Analysis...................................................................................................30
Chapter 3: Results............ .........................................................................................................31
3.1 Metabolic Measurements..... ...............................................................................................31
3.1.1 Rat Weight...............................................................................................................31
3.1.2 Food Consumption...................................................................................................31
3.1.3 Blood Glucose Levels..............................................................................................32

vi
3.2 Mammary Tumour Analysis............................................ ...................................................35
3.2.1 Mammary Tumour Incidence, Multiplicity, Burden, Growth Rate.........................35
3.2.2 Histology..................................................................................................................38
3.2.3 Western Blot............................................................................................................38
3.3 Colon Cancer (ACF) Results................................................ ..............................................39
Chapter 4: Discussion...................................................................... .........................................40
4.1 Mammary Cancer..................................................................... ...........................................41
4.2 Colon Cancer......................................................................... ..............................................43
4.3 General Discussion and Future Direction.......................... .................................................44
References.......................................................................... .......................................................47
Appendix A.................................................................. .............................................................69

vii
List of Abbreviations
DMBA 7,12-Dimethylbenz(a)anthracene
ACF Aberrant Crypt Foci
ADA American Diabetes Association
ANOVA analysis of variance
AOM Azoxymethane
Bcl-2 B-cell CLL/lymphoma 2
BMI Body Mass Index
JNK c-Jun N-terminal Kinases
CI Confidence Interval
PIP2 Di-phosphorylated Phosphoinositide
EGF Epidermal Growth Factors
EPIC European Prospective Investigation into Cancer and Nutrition
F344 Fischer 344
FDA Food and Drug Administration
Grb-2 Growth Factor Receptor-bound Protein 2
HCT116 Human Colorectal Cancer Cell Line
HR Hazard ratio
HEAL Health, Eating, Activity, and Lifestyle
HFD High Fat Diet
HIF-1 Hypoxia-Inducible Factor-1
IKK IkB kinase
IKB Inhibitor of NF-kB
IR Insulin Receptor
IRS-1 Insulin Receptor Substrate-1
ITT Insulin Tolerance Test
IGF-1R Insulin-like Growth Factor-1 Receptor
IL-1 Interleukin-1
IL-6 Interleukin-6
i.p. intraperitoneal
i.v. intravenous
LID Liver-specific IGF-1 Deficient
mSos mammalian Son of Sevenless
MCF-7 Michigan Cancer Foundation-7 (Human breast cancer cell line)
MKR Skeletal Muscle-specific loss of IGF-1 Receptor
MNU Methylnitrosourea
MAPK Mitogen Activated Protein Kinases
MDF Mucin-Depleted Foci
NPH Neutral Protamine Hagedorn
PTEN Phosphatase and tensin homolog

viii
PBS Phosphate Buffered Solution
PI3K Phosphoinositide 3-kinase
PVDF Polyvinylidene Fluoride
RIA Radioimmuno Assay
RIPA Radioimmunoprecipitation Assay
RR Relative Risk
SEM Standard Error of Mean
s.c. subcutaneous
PIP3 Tri-phosphorylated Phosphoinositide
TNF-α Tumour Necrosis Factor-α
WHI Women's Health Initiative
WHO World Health Organization

ix
List of Tables
Table 1 Summary of epidemiological studies reporting the association between the use of
insulin glargine and all-cancer risks................................................................................. .........15
Table 2 Summary of epidemiological studies reporting the association between the use of
insulin glargine and breast cancer risk.......................................................................... ............16
Table 3 Diet Information............................................................................................ ...............26

x
List of Figures
Figure 1 Regular Insulin..............................................................................................................3
Figure 2 Insulin Glargine (Lantus) .......................................................................... ...................4
Figure 3 Insulin Detemir (levemir- 14C) and Insulin Degludec (16C) ................... ...................5
Figure 4 Schematic Overview of Insulin-IGF System............................................ ....................7
Figure 5 Post-receptor Signaling Pathways of Insulin Receptor (IR) and Insulin-like Growth
Factor-1 Receptor (IGF-1R)............................................................ ................... ........................8
Figure 6 Metabolite Formation of Insulin Glargine after Injection...........................................19
Figure 7 Multi-stage Chemical Carcinogenesis.................................................. ......................20
Figure 8 Overall Schematic Animal Protocol............................................. ..............................25
Figure 9 Weekly Average Body Weight.................................................... ...............................31
Figure 10 Weekly Average Food Consumption........................................................................32
Figure 11 Blood Glucose Before Insulin Injection....................................................................33
Figure 12 Blood Glucose at 4 hours Post-insulin Injection.......................................................33
Figure 13 Blood Glucose at 8 hours Post-insulin Injection.......................................................34
Figure 14 Glycated Hemoglobin Level........................................ .............................................34
Figure 15 Mammary Tumour Incidence....................................................................................35
Figure 16 Mammary Tumour Incidence over time................ ...................................................36
Figure 17 Mammary Tumour Multiplicity.......................... ......................................................36
Figure 18 Mammary Tumour Burden............................... ........................................................37
Figure 19 Mammary Tumour Growth rate/day.............. ...........................................................37
Figure 20 Histology of Mammary Tumours in each group.......................................................38
Figure 21 Preliminary Western blots.........................................................................................39
Figure 22 ACF Analysis............................................................................................................39

1
Chapter 1
Introduction
1.1 Diabetes
Diabetes Mellitus, a metabolic disorder mainly characterized by an elevated blood
glucose levels (hyperglycemia), is one of the most prominent disorders worldwide. The World
Health Organization (WHO) estimates 347 million people have diabetes around the globe
(Accessed on January 2013). In Canada alone, it is estimated that over 9 million people have
diabetes or pre-diabetes (Canadian Diabetes Association, Accessed on January 2013), which is
about a third of the Canadian population.
There are three main types of diabetes mellitus: Type 1, Type 2, and gestational
diabetes. Type 1 diabetes is caused by an autoimmune response toward β-cells, which secrete
insulin. In contrast, Type 2 diabetes is a consequence of lack of insulin sensitivity or insulin
resistance in insulin target organs, including muscle, liver, and adipose tissues. Compensatory
hyperinsulinemia (elevated level of insulin in blood) follows insulin resistance and eventually
results in dysglycemia due to β-cell exhaustion in predisposed individuals. Lastly, gestational
diabetes occurs in pregnant women when insulin action is impaired due to pregnancy related
factors such as human placental lactogen.
Type 2 diabetes accounts for about 90% of all diabetes cases. The well-known
symptoms and signs of diabetes include polyuria (frequent urination), polydipsia (frequent
thirst) and polyphagia (frequent hunger) but can also include fatigue, weight loss and blurred
vision. There are some risk factors that contribute to development of Type 1 and Type 2
diabetes. Main risk factors for Type 1 diabetes include race, family history, and certain viral
infections in childhood. For Type 2 diabetes, the core risk factors are: diet, race, family history,
age, Body Mass Index (BMI), and sedentary lifestyle. Diabetic patients are at risk of developing
complications such as retinopathy, nephropathy, and cardiovascular disease (1). Moreover,
multiple epidemiological studies have demonstrated that there is an association between
diabetes and risk for cancer, including breast and colorectal cancer (2-7). Currently, the
incidence of diabetes is increasing and no cure is available; however, the disease can be
managed by diet, exercise, and medications such as metformin, insulin secretagogues, or
exogenous insulin.

2
1.2 Insulin Treatment
1.2.1 Regular Human Insulin
The discovery of insulin by Banting and Best in the 1920s was a breakthrough in the
diabetes community. At first, insulin was extracted from bovine or porcine pancreas. With time,
biosynthetic human insulin became available by mass production using biotechnology (8)
(Figure 1). Even though insulin is not a cure for diabetes, the hormone has saved millions of
diabetic patients and bestowed a better quality of life; however, a difficulty in controlling blood
glucose still remains. Regular human insulin has relatively short-duration of action with
unstable absorption and therefore diabetic patients are required to receive injections multiple
times a day. Moreover, if not controlled carefully, the patients may be at risk of hypo- or
hyperglycemia. In order to prolong the action of the insulin, unmodified human insulin called
Neutral Protamine Hagedorn (NPH) was developed. By adding neutral protamine (an arginine
rich nuclear protein group), the absorption of insulin from the subcutaneous injection site is
retarded (9). Prolonged action-profile of NPH allowed diabetic patients to establish a bed time
basal insulin level but due to its peak release at 4-8 hours post-injection and an insufficient
duration, high risk of nocturnal hypoglycemia, and morning hyperglycemia were experienced
(9). In order to overcome these problems, long-acting insulin analogues were developed.

3
Figure 1: Proinsulin and Insulin Insulin is a peptide hormone that contains 51 amino acids. It
is composed of an A-chain and a B-chain, which are linked by disulphide bonds. Proinsulin,
which is the precursor molecule to insulin, is cleaved by prohormone convertases (at cleavage
sites) to produce a C-peptide and insulin. An additional removal of 4 amino acids (denoted by
red colors) by carboxypeptidase E reproduces a mature insulin. C-peptide and insulin molecules
are stored in granules to be released in response to stimuli, such as elevated blood glucose.
1.2.2 Long-Acting Insulin Analogues
Insulin analogues are modified insulin molecules at a primary structural level by
recombinant technology. They were developed to best mimic endogenous insulin secretion by
altering the pharmacokinetics. Some analogues, such as insulin aspart and lispro, are modified
so that the molecules are absorbed much faster than regular insulin and remain in circulation for
shorter duration. These analogues are suitable for administration prior to meal time. In contrast,
other analogues are modified to have a prolonged time-action profile. Long-acting insulin
analogues, such as insulin glargine (Lantus) and detemir (Levemir), are used to establish a
stable basal insulin level for diabetic patients. The long-acting insulin analogues greatly reduce
nocturnal hypoglycemia when compared to NPH and last for sufficient duration overnight.

4
Insulin glargine, which is the first long-acting insulin analogue produced by recombinant
technology, has a glycine substitution for asparagine at A21 position and two arginine additions
on the C-terminal end of B chain of the insulin molecule (10) (Figure 2). These modifications
shift the isoelectric point of the insulin glargine molecules from pH 5.4 to pH 6.7 and thus,
glargine precipitates under the neutral condition of the subcutaneous tissue (11). Precipitated
glargine molecules are released slowly into the bloodstream, which protracts the duration of
action to about 20 hours without any prominent peak. Insulin detemir, another long-acting
insulin analogue, is modified using a different strategy. Amino acid threonine at B30 is
removed and a 14-carbon fatty acid chain is acylated on B29 lysine (Figure 3). These
modifications permit the molecules to bind albumin and to be released over a prolonged period
of time (12). Insulin detemir lasts about 18 hours. Lastly, insulin degludec, an ultra long-acting
insulin analogue, utilizes a similar approach as insulin detemir. It also has a deletion of B30
threonine and an addition of hexadecadionic (C16) fatty acid chain (13) (Figure 3). An
exceptionally prolonged duration of insulin degludec (up to 48 hours) results from formation of
multi-hexamer chains by the molecules in the subcutaneous tissue. While it is currently
approved by the European Union, Japan, and Mexico, the Food and Drug Administration (FDA)
rejected its approval in February 2013 due to a lack of cardiovascular outcome (Medscape
News; accessed on April 13, 2013).
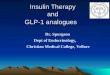
Figure 2: Insulin Glargine (Lantus) Insulin glargine has a substitution to glycine for
asparagine in position 21 on the A-chain. Also, it has additions of two arginine molecules at the
end of the B-chain.

5
Figure 3: Insulin Detemir (Levemir- 14C) and Insulin degludec (16C) Both insulin detemir
and degludec are missing threonine in position 30 on B-chain and have either a 14-C or 16-C
fatty acid chain attached onto lysine 29 on the B-chain respectively.
1.3 Insulin Receptor (IR), Insulin-like Growth Factor-1 Receptor (IGF-1R), and Hybrid
receptors
IR and IGF-1R are members of the receptor tyrosine kinase family that share 47-67%
amino acid homology (14). They are activated by their cognate ligands, insulin and IGFs
respectively, to "turn-on" the downstream signaling pathways. IGF-1R and IR resemble each
other structurally to an extent that their designated ligands can bind to each other's receptor with
low affinity (15) (Figure 4).
IRs can exist in two isoforms, IR-A and IR-B, depending on the presence or absence of
exon 11. IR-A, which lacks exon 11, is expressed ubiquitously in low levels but predominantly
in central nervous system. It is also highly expressed during fetal growth where it may be
activated by insulin (16). Thus, it mainly activates a mitogenic signaling pathway. In contrast,
IR-B retains exon 11 and is expressed dominantly in classical insulin targets: liver, muscle, and
adipose tissue (16). A metabolic signaling pathway is predominantly activated by IR-B when
bound to its ligand, insulin. While insulin can bind to IR-A, IGF-2 can also bind and activate
IR-A to mediate a mitogenic effect (15). Once IR is activated by insulin, it mainly activates the
PI3K/Akt pathway (Figure 5). Activated IR phosphorylates insulin receptor substrate (IRS),
which in turn activates phosphoinositide 3-kinase (PI3K). PI3K phosphorylates di-

6
phosphorylated phosphoinositide (PIP2) to tri-phosphorylated phosphoinositide (PIP3), which
then activates Akt or protein kinase B. The activation of Akt by PI3K is inhibited by
phosphatase and tensin homolog (PTEN) dephosphorylation of PIP3. Activated Akt is an
important mediator that acts on various cellular processes, including glucose metabolism,
cellular growth, and survival.
IGF-1R is well-documented to induce mitogenic signaling and thus, it has been
implicated in cancer development (17). Upon stimulation by its ligands, IGF-1 and 2, Shc
protein is phosphorylated by the beta-subunit of the receptor. Then a growth factor receptor-
bound protein 2 (Grb 2)-mammalian Son of Sevenless (mSos) complex is recruited. The
activated mSos loads GTP onto small G protein Ras, then the series of kinase activities occur
downstream to mediate cell proliferation (18). Both IGF-1R and IR share very similar
intracellular signaling pathways (19). Thus, it is a general consensus that IR and IGF-1R have
overlapping functions besides their own distinguishing functions.
Insulin can also act as a weak agonist for IGF-1R. While the mitogenic effect derived
from insulin (at a physiological concentration) by activation of IGF-1R is expected to be almost
negligible in normal tissues when compared to IGF-1, overexpression of IGF-1R displayed in
breast cancer cells (20) and colorectal polyps (21) may allow the mitogenic effect of insulin to
manifest in breast and colon cancer promotion, especially in hyperinsulinemic condition (19).
Moreover, many malignant cells also overexpress IR-A, which appears to mediate growth-
promoting effect over metabolic effect. Hyperactivation of IR-A by increased levels of insulin
may facilitate malignant cell growth and survival (19).
Intriguingly, due to highly homologous structure shared by IR and IGF-1R, half
receptors from each type can heterodimerize to form an IR/IGF-1R hybrid receptor. As IRs can
exist in two forms, IR-A and IR-B, the hybrid receptors can also exist in two isoforms, IR-
A/IGF-1R and IR-B/IGF-1R. A study by Pandini et al. evaluated the differences in signaling
and biological roles of two hybrid isoforms in engineered cells (22). The author reported an up-
regulation of IGF signaling system (mitogenic pathway) by IR-A/IGF-1R hybrid receptors by
binding to IGF-1 and IGF-2 with similar affinity and to insulin with slightly lower affinity
albeit in a physiological range. It is noteworthy that insulin, resembling IGF-1 and IGF-2,
activated IGF-1R downstream pathway through IR-A/IGF-1R hybrid receptors. In contrast, IR-
B/IGF-1R hybrid receptors bound to IGF-1 and IGF-2 with 6-fold lower affinity, and to insulin
with negligible binding affinity. Thus, cells containing predominantly the IR-A/IGF-1R hybrid

7
receptors are more effectively stimulated by both insulin and IGFs than cells mainly composed
of IR-B/IGF-1R hybrid receptors.
Figure 4: Schematic overview of insulin-IGF system Binding of ligands (one of insulin, IGF-
1, and IGF-2) to their designated receptor activates either metabolic or mitogenic effects. Thick
arrows represent strong affinity or signal, and thin arrows represent weak binding or signal. The
figure is modified from Pollak et al. (23) and the figure is not meant to be all-inclusive.

8
Figure 5: Post-receptor signaling pathways of insulin receptor (IR) and insulin-like
growth factor-1 receptor (IGF-1R) Both insulin and IGF-1 bind to IR and IGF-1R, while the
affinity is much higher toward their cognate receptor. Once corresponding ligand binds to the
receptor, a series of phosphorylation event occurs downstream. Phosphorylation through the
PI3K/Akt pathway results not only in metabolic effects, but also anti-apoptosis and protein
synthesis. The MAPK pathway results in mitogenesis (cell proliferation). IR (especially IR-A)
can also activate the MAPK pathway (Erk1/2). Thick arrows represent strong downstream
signaling pathways whereas thin arrows represent weaker signal. The figure is modified from
Tognon and Sorensen (24) and the figure is not meant to be all-inclusive.
1.4 Diabetes, Obesity, Insulin Resistance, Inflammation, and Cancer
Many epidemiological studies have shown associations between diabetes and increased
incidence of various types of cancers. Although prostate cancer risk seems to have a reduced
among diabetic patients (25), other major types of cancer risks including colorectal (26),
pancreatic (27) , breast (28), hepatic (29), and endometrial (4) are increased. Moreover, diabetes

9
has been associated with increased cancer mortality (30). In Canada, a slightly but significantly
increased relative risks (RR) of 1.1 to 1.2 were shown for breast (5;6) and colorectal (3) cancer
in diabetes patients. This increase may appear to be negligible, however due to the high
prevalence of diabetes and breast and colorectal cancer, diabetes is a risk factor in a sizeable
population of cancer patients. The type of diabetes that is associated with cancer is type 2,
whereas this association is not clear in type 1 (31).
Obesity has been historically known as a risk factor for both diabetes and cancer.
Additionally, a decreased cancer incidence and mortality rates were reported for obese patients
who underwent bariatric surgery (32-34).Obesity is also independently associated with cancer.
Solid epidemiological studies have linked overweight and obesity to certain types of cancer,
such as breast and colorectal (35-40). In fact, a large meta analysis based on 30 European
countries reported that 2.5% of new cancer cases in men and 4.1% of new cancer cases in
women (or over 70,000 in absolute terms) were attributable to excess BMI (BMI ≥ 25 kg/m2)
over 10 years (36). Among all the cancer types, endometrial (33,421) cancer was the largest
attributable new cancer, followed by post-menopausal breast (27,770) and colorectal (23,720)
cancer. With a generally accepted association between overweight/obesity and increased cancer
risks, a few mechanisms may explain how obesity increases cancer prevalence and cancer
deaths: inflammation and insulin resistance (41).
Obesity is associated with metabolic inflammation, which is characterized as low-
grade, chronic inflammatory state induced by excess nutrients (42). Although the initiating
mechanism of metabolic inflammation is unclear, one mechanism proposed is hypoxia. Due to
adipose tissue expansion, some cells distant from blood vessels become poorly oxygenated,
resulting in local hypoxia (43). This hypoxia condition activates hypoxia-inducible factor
(HIF)-1α to mediate infiltration of macrophages and monocytes into adipose tissue (44). It has
been shown that both macrophages and monocytes secrete cytokines such as tumour necrosis
factor (TNF)-α after their infiltration into the adipose tissue in obese individuals (45). TNF-α is
implicated in cell survival (46), growth, and differentiation (47;48); these effects are believed to
be through inhibiting the inhibitor of NF-kB (IkB). Inactivation of IkB activates NF-kB to
establish its anti-apoptotic effect, thus enhancing cancer cell survival (46). Furthermore, NF-kB
activation in cancer cells promotes cell cycling through c-Myc and cyclin D1 to increase
proliferation and growth (46;47). Thus, obesity-induced inflammation may facilitate
carcinogenesis.

10
Obesity is also highly associated with the development of insulin resistance, a
pathological condition that reduces insulin sensitivity in the body. An increased rate of lipolysis
due to expanded adipose tissues in obese conditions results in excess free fatty acids, which can
trigger the inflammatory pathways to impair insulin signaling (49). Additionally, an increased
secretion of pro-inflammatory cytokines, including interleukin (IL)-6, IL-1β, and TNF-α, by
adipose tissue can activate serine kinases such as IkB kinase (IKK) and c-Jun N-terminal
Kinases (JNK). These kinases phosphorylate serine residues of the IRS-1 to impair downstream
cascades (49) and thus induce insulin resistance. Inflammation is induced and a consequence of
insulin resistance, as cytokines impair insulin signaling and insulin has an anti-inflammatory
effect (50). Insulin resistance is a key pathogenic factor of type 2 diabetes and is associated
with augmented circulating insulin levels (51). This compensatory hyperinsulinemia exposes
tissues to elevated insulin and insulin signaling. Since insulin resistance mainly occurs in the
PI3K dependent metabolic effects of insulin in the target tissues (52), the MAPK dependent
proliferative effect remains intact. Various studies have reported a proliferative effect elicited
by elevated insulin levels. For example, insulin was found to promote proliferation by
shortening the G1 phase in the Michigan Cancer Foundation-7 (MCF-7) human breast cancer
cell line (53). These studies will be detailed in section 1.5.1.2.
1.5 Insulin Therapy, Insulin-like growth factor (IGF)-1 and Cancer Risk: Focusing on
Breast and Colon Cancer
1.5.1 Insulin, IGF-1, and Cancer
In addition to its well-known metabolic effect, insulin also increases cell growth as well
as proliferation of many cell types (54), the most common target being malignant cells (55;56).
The stimulation of proliferation by insulin differs from that of IGF-1. While insulin exhibits
mitogenic properties, IGF-1 is not a mutagen but may favor either spontaneous mutation or
dedifferentiation (57).
1.5.1.1 Epidemiological studies
The increased cancer risks such as breast and colorectal cancer in type 2 diabetic
patients can be independent of obesity (19;58). A number of epidemiological studies have
demonstrated a positive association between serum insulin and breast/colon cancer risks. For
example, the Women's Health Initiative (WHI) revealed that postmenopausal women with

11
higher levels of serum insulin were more prone to develop colorectal cancer (59). Moreover, an
increase in C-peptide levels was shown to be positively associated with higher breast and
colorectal cancer risk by a few studies, including the European Prospective Investigation into
Cancer and Nutrition (EPIC) (60;61). Furthermore, a meta-analysis in 2008 that included
prospective and case-control studies reported a 26% higher breast cancer risk (RR of 1.26; 95%
Confidence Interval (CI); 1.06-1.48) in patients with higher C-peptide levels (62). Health,
Eating, Activity, and Lifestyle (HEAL) study by the National Cancer Institute, which was a
prospective, multiethnic cohort study, reported a 35% increased breast cancer-specific deaths in
patients with a 1ng/ml increase in C-peptide levels (63) (range of C-peptide: 0.25 to 9.7 ng/ml).
Case-control as well as cohort studies also indicated a positive association between fasting
insulin levels and breast cancer incidence with a RR of 2 to 3 (64;65). C-peptide is also linked
with colorectal cancer risk. Studies displayed an association between elevated C-peptide levels
and increased colorectal cancer risk (60). Also, higher levels of C-peptide is reported to be a
predictive factor for higher colorectal neoplasia susceptibility according to a meta-analysis (66).
Not only is endogenous insulin associated with cancer risk, but exogenous insulin therapy has
been reported to be linked to cancer risk in type 2 diabetes by most studies (67-73) with a few
exceptions (57;74). Although one meta-analysis observed that insulin use is not significantly
associated with increased breast cancer risk , it was reported to be linked with increased
colorectal risk (75).
The association between hyperinsulinemia and cancer may be partly explained by IGF-1.
Insulin can increase IGF-1 production from the liver by up-regulating growth hormone receptor
and its downstream signaling (76). In addition to increased production of IGF-1, insulin
simultaneously diminishes the level of Insulin-like Growth Factor-Binding Proteins (IGFBPs),
which results in increased bioavailable IGF-1 (77;78). Higher levels of serum IGF-1 is
correlated with increased breast and colorectal cancer risks. A meta-analysis involving 96
studies found that higher circulating IGF-1 levels elevated cancer risks, including breast and
colorectal cancer (79). Moreover, another study reported that increased serum IGF-1 levels
were associated with higher risk of cancer mortality in older men (80). Thus, the association
between cancer risks and insulin levels in blood, whether it is direct or indirect, shows that
insulin may play a role in cancer development.

12
1.5.1.2 In Vitro studies
Both insulin and IGF-1 have been shown to stimulate proliferation and migration in
cancer cell lines including breast and colorectal cancer cells (81-84). In breast tumour tissues,
IR is overexpressed compared to normal breast tissue; this difference results in greater insulin
induced cell proliferation in comparison to normal tissue (85). Increased proliferation by insulin
was found to be mediated through IGF-1R and partly through IR (86) via both the MAPK and
PI3K/Akt signaling pathways (87). Similarly, IGF-1 induced increased proliferation in MCF-7
breast cancer cells by activating MAPK and PI3K/Akt pathways (88). These pathways were
activated by IGF-1 also in colorectal cancer cell lines (89;90). In both breast and colorectal
cancer cells, IGF-1 activates Src kinase that consequently transactivates other growth factor
receptors, such as epidermal growth factors (EGF) (81;91). Moreover, IGF-1 was found to
oppose chemotherapy-induced death of breast cancer cells by increasing proliferation and
inhibiting apoptosis (92). In addition to stimulation of proliferation and inhibition of apoptosis
of cancer cell lines, IGF-1R can induce assumption of some malignant in vitro characteristics
(such as anchorage-independent colony formation and loss of cell polarity) of non-cancerous
breast (82) and colorectal (81) cell lines. The potential of IR to induce these characteristics is
controversial (93;94).
1.5.1.3 In Vivo studies
In vivo data shows some heterogeneity in the link between insulin and cancer risk. A
study by Tran et al. demonstrated that exogenous insulin administrations promoted colon
tumour (tubular adenoma) formation in azoxymethane (AOM)-treated male Fischer 344 (F344)
rats (95). They injected rats with doses of insulin (porcine NPH) of 15U/kg 5 times per week for
17 weeks. The insulin levels achieved are pathophysiological, i.e. can be seen in very insulin
resistant rats. Another group did not find a significant increase in the number of aberrant crypt
foci (ACF) in AOM-treated female F344 rats by exogenous insulin injections (bovine NPH,
20U/kg 5 times/wk for 14 weeks), but the crypt multiplicity was significantly increased (96),
which indicates advanced dysplasia. A tumour promoting effect of insulin was also seen in
mammary tumours. A study by Heuson et al. reported that exogenous insulin injection (dosage
of 25U/kg Lente insulin (species not indicated but likely either bovine or porcine because the
study was carried out before the introduction of human insulin) 6 times per week for 6 weeks
significantly increased mammary tumour growth (in cm2) in 1,2 dimethylbenz(a)anthracene
(DMBA)-treated female Sprague-Dawley rats compared to control rats (55). Moreover, the

13
same author also reported mammary tumour growth dependence on insulin by showing
regression of existing mammary tumour in DMBA-induced female Sprague-Dawley rats by
treatment with alloxan (97) or streptozotocin (98), which destroys beta-cells in pancreas.
Additionally, streptozotocin-induced diabetes resulted in regression of MCF-7 orthografts, an
effect reversed by insulin treatment (99). On the other hand, other studies did not find the
promoting effect of hyperinsulinemia. For instance, when female MNU-treated Sprague-
Dawley rats were injected with insulin (same insulin type, dosage, and number of injections per
week as Tran et al.) for 25 weeks, no differences in mammary tumour incidence were observed
(100). There are also other studies that tested diabetic animal model. A study by Novosyadlyy
et al. used muscle creatine kinase promoter/human IGF-I receptor (MKR) mice, which are lean,
insulin resistant, and hyperglycemic, to assess the effect of insulin on breast cancer. The
hyperinsulinemic state in MKR mice (about three-fold higher insulin level than the wild-type
mice) caused hyperplasia in mammary gland and enhanced development of precancerous and
cancerous mammary gland lesion. Both normal and malignant breast tissues from MKR mice
exhibited augmented phosphorylation of IR and IGF-1R and a downstream biomarker, Akt
(101). Also, after inoculation with orthotopic mammary tumours in MKR mice, the tumour
growth was significantly greater than in inoculated wild-type mice. Expectedly, the use of
selective IR/IGF-1R inhibitor (BMS-536924) decreased the tumour growth (101).
As cell culture studies have shown, in vivo studies also confirmed the association
between IGFs and increased breast and colon cancer. Liver-specific IGF-1 deficient (LID) mice,
which exhibit only 25% of the serum IGF-1 level observed in wild-type, are protected from
genetic and carcinogen-induced mammary and colon cancer (102;103). Another study reported
that both male and female LID mice had significant 25% reduction in colon tumour size even
though tumour incidence and multiplicity were not (104). These findings suggest that IGF-1 is
an independent cancer promoter, which augments the growth of tumour.
1.5.2 Insulin Analogues and Cancer
1.5.2.1 B10Asp
While insulin analogues are preferred over regular human insulin owing to their
favorable kinetics, some of these new insulin analogues may exhibit an increased mitogenic
potential compared to regular insulin. This mitogenicity may have derived from either higher
IGF-1R binding affinity or slower dissociation-rate from IR or both. These characteristics were
observed with the first insulin analogue developed, B10Asp insulin (105). It is a rapid-acting

14
insulin analogue with an absorption rate twice as fast as human insulin. It had a substitution of
histidine on B10 position with aspartic acid. B10Asp not only exhibited a higher binding
affinity for IGF-1R, but it also phosphorylated IR and Akt to a greater extent and for more
prolonged time than regular insulin. It was demonstrated to induce spontaneous mammary
cancer in female Sprague-Dawley rats (105). Although its carcinogenic potential in rats
prevented it from becoming commercialized, the mitogenic potency of B10Asp raised concerns
about the carcinogenic potential of insulin analogues.
1.5.2.2 Long-Acting Insulin analogues
1.5.2.2.1 Epidemiological studies
In 2009, a strong concern about the safety of insulin glargine arose from a German study
that demonstrated a dose-dependent association between all cancer risk and the use of insulin
glargine among diabetic patients (70) (Table 1). However, it is noteworthy that the higher
overall cancer incidence among the patients using insulin glargine over human insulin was
found only after adjustments for insulin dose, whereas with the unadjusted data the opposite
finding was observed (70). Another study found three other European studies followed up to
address this issue (69;106;107). None of the three studies found an association between all-
cancer risk and the use of insulin glargine. While two studies reported an increased breast
cancer risk with the usage of glargine at least in subsets of patients (106;107), one study found
no association (69). The study by Jonasson et al. showed a breast cancer RR of 1.99 (95% CI
1.31–3.03) over 2 years (2006-2007) (107) but no increase in breast cancer risk was observed
with the use of insulin glargine in the follow-up study with the identical group in third year
(2008) (108). The study by Colhoun et al. showed increased breast cancer risk in a subset of
patients using insulin glargine alone (106) (Table 2). Echoing the Jonasson's and Colhoun's
data, another large population-based cohort study that included almost 20,000 patients reported
a significant positive association between the use of insulin glargine and breast cancer risk
([Hazard ratio (HR)] 1.58 -Hazard ratio is the ratio of the hazard in treatment group versus
control group. It differs from relative risk (RR) because HR is a cumulative risk of the entire
study with a defined endpoint while RR is an at one time point of the study (usually the end),
95% CI 1.22-2.05) (109).

15
Author Year Study type Patient
Number (N)
All-Cancer Risks (95%
Confidence Interval)
Hemkens
et al.
2009 Cohort study 127,031 HR= 1.19 (1.10-1.30) at 30U and
HR= 1.31 (1.20-1.42) at 50U
glargine vs human insulin
Mannucci
et al.
2010 Case-Control 1,340 OR= 1.33 (1.07-1.65) glargine
≥0.3U/kg/day vs human insulin
Currie et
al.
2009 Cohort study 62,809 HR= 1.24 (0.90-1.70, p=0.19)
glargine alone vs basal human
insulin alone
Gerstein
et al.
2012 Randomized
controlled
study
12,537 HR= 1.00 (0.88-1.13) glargine vs
other treatment
Chang et
al.
2010 Cohort study 59,443 HR= 0.86 (0.72-1.01) glargine vs
intermediate/long-acting human
insulin
Ljung et
al.
2011 Cohort study 114 838 HR= 1.10 (0.96-1.26) glargine
only vs other types of insulin
Blin et al. 2012 Cohort study 6,649 HR= 0.59 (0.28-1.25) glargine vs
human insulin
Fagot et
al.
2012
Cohort study 70,027 HR= 1.01 (0.71-1.45) glargine vs
other basal insulin
Table 1: Summary of epidemiological studies reporting the association between the use of
insulin glargine and all-cancer risks
However, this study observed a lower all cancer risk with the use of insulin glargine (HR 0.75,
95% CI 0.71-0.80). The association between insulin glargine and breast cancer risk was also
observed in a study by Suissa et al., where the authors found an increased breast cancer risk
with the usage of insulin glargine after 5 years (first 5 years: HR 0.9; 95% CI 0.7-1.3, after 5
years: HR 1.8; 95% CI 0.8-4.0), and a significant increase for the women who had insulin prior
to taking insulin glargine (HR 2.7; 95% CI 1.1-6.5) (110).

16
Author Year Study
type
Patient
Number (N)
Breast Cancer Risk (95%
Confidence Interval)
Colhoun et al. 2009 Cohort
study
36,254 HR= 3.39 (1.46-7.85) glargine only
vs non-glargine insulin alone
Jonasson et al. 2009 Cohort
study
114,841 RR= 1.97 (1.29-3.00) glargine only
vs other insulin
Suissa et al. 2011 Cohort
study
15,227 HR= 1.8 (0.8-4.0) glargine vs other
insulin after 5 years
HR= 2.7 (1.1-6.5) glargine vs other
insulin for women who had been
on insulin before switching to
glargine
Ruiter et al. 2012 Cohort
study
19,377 HR= 1.58 (1.22-2.05) glargine vs
human insulin
Habel et al. 2013 Cohort
study
128,175 HR= 1.3 (1.0-1.8) ever used
glargine vs NPH
Currie et al.
2009 Cohort
study
62,809 HR= 0.86 (0.42-1.75) glargine vs
other insulin
Chang et al. 2011 Cohort
study
59,443 HR= 0.62 (0.21-1.31) glargine vs
human insulin
Fagot et al. 2012 Cohort
study
70,027 HR= 0.97 (0.87-1.07) glargine vs
other basal insulin
Grimaldi-
Bensouda et
al.
2013 Case-
control
3,825 HR= 1.04 (0.76-1.44) glargine vs
other insulin
Sturmer et al. 2013 Cohort
study
52,453 HR= 1.12(0.95-1.32) initiating
glargine vs initiating NPH
Table 2: Summary of epidemiological studies reporting the association between the use of
insulin glargine and breast cancer risk.

17
Other studies with a shorter follow-up period also yielded a positive association between
glargine and breast cancer in subgroups (108;111;112). There are a few studies that reported no
association between insulin glargine use and breast cancer risk (69;113-116). Thus, results in
epidemiological studies for the effect of insulin glargine and breast cancer risk are still under
debate, and longer follow-up is required. As far as all-type cancer is concerned, the majority of
studies, except for one study (70;117), do not confirm the increased cancer risk by glargine
(69;71;118-120). For instance, a study by Blin et al. used the French National Healthcare
Insurance Database to report an all-type cancer HR of 0.59 (95% CI 0,28-1.25) among the type
2 diabetic patients (118). In fact, this study demonstrated a lower cancer risk with using insulin
glargine compared to regular insulin. There are two recent randomized control studies, which
also found no adverse carcinogenic effect of insulin glargine (119;120). However, it must be
noted that the cancer incidence was secondary endpoint in these studies.
1.5.2.2.2 In Vitro Studies
Numerous in vitro studies investigated the mitogenic effect of insulin glargine on
malignant cell lines, including breast (121) and colorectal cancer cells (89). Not only MCF-7
breast cancer cells treated with insulin glargine showed a maximum of 3.1-fold increased
proliferation compared to untreated cells, but also significantly higher proliferation than cells
treated with human insulin (121). The author stated that the higher proliferative effect by insulin
glargine in MCF-7 cells derived from a strong activation of IGF-1R and MAPK pathway.
Consistently, a greater binding affinity (6- to 8-fold higher) and a higher activation of IGF-1R
by insulin glargine compared to regular insulin or insulin detemir was reported by other studies
(11;122-124). A study reported that insulin glargine can induce a significantly higher
proliferative effect on MCF-7 cells at 1.5nM and 15nM concentration compared to regular
insulin, but no proliferation enhancing effect was observed on benign mammary cell line MCF-
10A (123). The mitogenicity pertaining to insulin analogues may be partly linked with the IGF-
1R:IR ratio of the cell, considering the ratio of 4:1 in MCF-7 cell line and 0.8:1 in MCF-10A
(125).
Despite having a higher binding affinity towards IGF-1R than human insulin, insulin
glargine has a faster dissociation rate from IR compared to regular insulin (122). It is thus
thought that the higher mitogenic potency of insulin glargine is derived from an increased
activation of IGF-1R signaling. However, it was reported that insulin analogues exhibiting
slower dissociation rate from IR have higher mitogenic potency versus regular insulin

18
(122;126), thus suggesting a possible attenuation of the mitogenic potency of insulin glargine
through IR. A study by Sciacca et al. compared mitogenic effects (cell proliferation and colony
formation) of regular insulin, long-acting insulin analogues, and IGF-1 using engineered cell
cultures that express only one of IR-A, IR-B, or IGF-1R to assess the contribution of each
receptor (127). They found that both long-acting insulin analogues, insulin glargine, and
detemir, induced a significantly higher Erk phosphorylation through IR-A receptor and IGF-1R
compared to regular insulin. The author also assessed cell proliferation induced by both long-
acting insulin analogues. Coinciding with the Erk phosphorylation data, both insulin glargine
and detemir induced a greater cell proliferation in IR-A, IR-B, and IGF-1R expressing cells
(127). In other study, the activation of IR and IGF-1R by insulin glargine was seen human
cancer cell lines. Insulin glargine at 50 ng/ml concentration induced phosphorylation of both IR
and IGF-1R HCT 116 cells, and showed a robust phosphorylation of Akt signaling pathways,
whereas Erk phosphorylation was comparable to regular insulin and IGF-1 (89). Insulin
glargine had significantly higher proliferative effect and anti-apoptotic activities. Increased
phosphorylation of Akt in MCF-7 cells is reported by Teng et al. when treating cells with
insulin glargine (128). They also found that anti-apoptotic B-cell CLL/lymphoma 2 (Bcl-2) in
up-regulated while Bax, a competitive antagonist of Bcl-2, is down-regulated. The author
concluded that insulin glargine can exert a growth-promoting effect on breast cancer cells by
enhanced anti-apoptotic signal activation through the Akt pathway.
1.5.2.2.3 In Vivo Studies
As mentioned above, B10Asp insulin analogue was found to promote spontaneous
mammary cancer in female Sprague-Dawley rats. Although both B10Asp insulin and insulin
glargine exhibit higher binding affinity for IGF-1R, insulin glargine does not promote
spontaneous mammary cancer in vivo. A study by Stammberger et al. reported that there was no
difference in mammary tumour incidence in both rats and mice when given a daily
subcutaneous injection with various doses of insulin glargine or human NPH (129). One other
study compared insulin glargine and NPH (Human, doses from 5 to 20 U/kg/day) for 18 weeks
on colonic mucosa cell proliferation and aberrant crypt foci formation in 1,2 dimethylhydrazine-
treated female db/db mice to see the effects of insulin glargine on colon cancer promotion (a
widely used mouse model of type 2 diabetes) (130). In this study, both NPH and insulin
glargine resulted in a higher colonic epithelial proliferation and aberrant crypt foci formation

19
versus saline control. However, insulin glargine did not induce increased colonic epithelial
proliferation or aberrant crypt foci formation when compared to NPH.
Figure 6: Metabolite formation of insulin glargine after injection Insulin undergoes
metabolism to form M1, missing two arginine molecules at the C-terminus, and M2, missing
two arginine molecules and a threonine at the C-terminus of B chain.
In vivo, it was also discovered that insulin glargine rapidly undergoes proteolytic
degradation to form two metabolites called M1 and M2 after its subcutaneous injection in rats,
dogs, and humans (11;131). It was reported that insulin glargine and M1/M2 are present in a
ratio of 50:50 in human serum (131) and in vitro experiment using the serum of patients under
glargine treatment had shown a 47% to 98% (mean of 72%) metabolism of insulin glargine into
M1 (132). M1 has been found to be the predominant form in the circulation (Figure 6). While
both M1 and M2 show similar binding affinity for IR as insulin glargine, they have weaker
binding affinity to and activation of IGF-1R, and mitogenicity that is comparable to regular
insulin (11). Intriguingly however, one pilot cross over randomized study reported that serum of
type 1 diabetic patients under insulin glargine treatment evoked higher proliferation in MCF-7
cells than the serum of patients under NPH treatment (133). This finding suggests that in vivo,
the concentration of glargine may be enough to induce proliferative effect at least in some

20
individuals that presumably metabolize glargine slowly. Most recently, an abstract presented at
the American Diabetes Association (ADA) 2013 reported that unlike IGF-1 treatment, there
was no increase in mammary tumour growth versus control using glargine treatment (12.5U/kg)
for 2 weeks in MKR mice grafted with two types of mouse mammary tumour cells (134).
1.6 Multistage Model of Chemically-Initiated Carcinogenesis
Multi-stage chemical carcinogenesis can be divided into four stages: tumour initiation,
tumour promotion, malignant transformation, and tumour progression (Figure 7).
Figure 7: Multi-stage chemical carcinogenesis DNA damage due to chemical exposure can
lead to activation of proto-oncogenes and/or inhibition of tumour-suppressor genes. The figure
is adapted from: Holland-Frei Cancer Medicine, 5th edition (2000)
1.6.1 Initiation
Tumour initiation involves irreversible damage to DNA. Tumour initiation by chemical
carcinogen is brought about from formation of adducts between the carcinogen and nucleotides
in DNA. The modification of DNA structure caused by carcinogen-DNA adducts can lead to
mutation during DNA synthesis. In general, a positive correlation is observed with the amount
of adducts detected and the number of tumours formed in an animal model (135). Carcinogen-
DNA adduct formation is believed to be necessary for tumour initiation and more specifically,
formation of a DNA adduct that results in mutation activating a proto-oncogene or inhibiting a

21
tumour-suppressor gene is considered to be a tumour initiating event. Proto-oncogenes are
genes involved in growth that, when mutated, can become oncogenes, i.e. cause uncontrolled
growth. Conversely, tumour-suppresor genes suppress growth of the cells and when inactivated,
can cause uncontrolled growth.
1.6.2 Promotion
Tumour promotion stage comprises a selective clonal expansion of initiated cells. Since
the accumulation of mutation is proportional to the rate of cell division, selective cellular
expansion of initiated cells produces cells with increased risk of further genetic changes
(because proliferating cells are more susceptible to mutations) and malignant conversion.
Tumour promoters, such as IGF-1 or insulin, are non-mutagenic and non-carcinogenic by
themselves. The contribution of cancer promoters to the process of carcinogenesis is the
expansion of initiated cell population, which will then be more susceptible to malignant
conversion. These agents are characterized by their ability to reduce tumour latency period of
initiated cells or to increase tumour number formed.
1.6.3 Malignant Conversion
With accumulation of genetic mutations in initiated cells, a fraction of these cells
undergo malignant conversion, which is the transformation of preneoplastic cells into ones that
express a malignant phenotype, defined based on genetic instability, uncontrolled growth, and
invasion.
1.6.4 Progression
Tumour progression refers to expression of malignant phenotype and more aggressive
characteristics in malignant cells with time. Metastasis may occur if the tumour cells exhibit an
ability to secrete proteases that permits penetration beyond their primary site. During tumour
progression, further genetic mutations can occur to activate proto-oncogenes or inhibit tumour-
suppressor genes.
1.7 Breast and Colon Cancer Animal Models using Carcinogen
1.7.1 Breast Cancer Model - Methylnitrosourea (MNU)
Methylnitrosourea (MNU) is a water-soluble alkylating agent that induces mammary
tumours in rats when injected subcutaneously and in contrast to 7,12-
Dimethylbenz(a)anthracene (DMBA - another widely used mammary carcinogen), metabolic
activation is not required (136). MNU decomposes spontaneously to result in methyl diazonium

22
ion, which is believed to be the ultimate carcinogen (137). Due to its direct carcinogenesis,
MNU is one of the widely used carcinogens for inducing mammary tumours. About 90% of the
rat mammary tumours induced by MNU are known to contain activating H-ras mutations
(members of the ras family are proto-oncogenes that increase cell proliferation), caused by
guanine to adenine transition (138). Rat mammary tumours induced by MNU are estrogen
receptor-positive and locally invasive, but metastasis is uncommon (139). Thus, MNU tumours
are good models for estrogen receptor positive tumours. However, they are not good models for
HER2/neu receptor positive and triple negative human mammary tumour. Also, ras mutations
are not commonly found in human mammary tumour (<10%) (140). A study by Isaacs et al.
investigated the mammary tumour incidence by subcutaneous (s.c.) injection of MNU (dosage
50mg/kg of body weight) in 50-days old Sprague-Dawley female rats (141). Among 20 rats
tested, 95% tumour carcinoma incidence, 3.9 average tumour number, and 68 day latency
period were observed. The same study also compared the efficacy between s.c. and intravenous
(i.v.) injections of MNU in Sprague-Dawley rats and found no significant difference between
the two modes of delivery. Thus, the author recommended the s.c. injection since it has the
advantage of being easier and faster to perform and allows a reproducible treatment of a large
quantity of animals by a minimal number of technicians.
1.7.2 Colon Cancer Model - Azoxymethane (AOM)
Azoxymethane (AOM) is an alkylating agent that is potent in inducing colon tumours
(mostly adenocarcinoma) in rats and mice. AOM is a derivative of 1,2-dimethylhydrazine,
which is as potent as AOM at inducing colon carcinogenesis. However, 1,2-dimethylhydrazine
undergoes a side reaction that consequently results in a highly toxic asymmetric hydrazine
derivative (142). Thus, although 1,2-dymethylhydrazine is cheaper and more readily available,
AOM is preferred for inducing colon tumours in animals. After administration, AOM is
metabolized by CYP2E1 into methylazoxymethanol, which is the active agent that causes DNA
mutation (143). AOM-initiated colon tumours often contain mutations in K-ras and B-catenin
similar to human colon tumours (144). However, unlike human tumours, Apc gene is seldom
mutated and p53 gene is never mutated. In addition, there is a low tendency for AOM-treated
rat colon tumour to metastasize (145). Azoxymethane is found to give rise to aberrant crypt foci
(ACF), colon preneoplastic lesions, as early as 3 weeks post-injection (146) and induce tumours
(adenoma and adenocarcinoma) after 36 weeks post-AOM injection in rats (147).

23
1.7.3 Aberrant Crypt Foci (ACF)
ACF are generally thought to be the precancerous lesions that may develop into colon
tumours (148-151). Studies found a positive association between the number of ACF and colon
tumour development. It was suggested that increasing number of crypts in ACF (increased ACF
multiplicity) displayed more advanced preneoplastic state (152). ACF are found in both humans
and rodents. A study by Pretlow et al. reported the presence of ACF in the colonic mucosa of
colon cancer patients (149). They observed a much higher number of ACF in the mucosa from
colon cancer patients compared to the colon from non-colon cancer patients. Despite the
acknowledgement of ACF as the preneoplastic lesions of colon tumours, ACF may not be a
reliable predictor of colon tumours. For example, a study of colon cancer prevention found a
significantly increased ACF multiplicity in AOM-treated male F344 rats while colon tumour
incidence and multiplicity were significantly decreased (153). This study also found that crypt
foci with absent or minimal mucous production called mucin-depleted foci (MDF) may be a
better predictor because the total number of MDF and crypt number/MDF significantly
decreased, showing a consistent result as with the colon tumour incidence. Moreover, MDF
were found to be more dysplastic than ACF when their histological dysplasia were graded
according to dysplasia parameters (such as number of mitosis, nuclear crowding, and increase in
nuclear:cytoplasmic ratio) at 7 and 15 weeks. MDF detection was also confirmed in human
colon cancer patients by two studies (154;155).
1.7.4 Dual-Organ Carcinogenesis Model
A study by Shivapurka et al. demonstrated a potential way to examine both mammary
and colon cancer in a single animal model, the female Sprague-Dawley rat (156). Three-week
old rats underwent acclimatization and quarantine for a week and were then provided with high
fat diet (HFD). The authors gave either a s.c. injection of MNU at a dosage of 50 mg/kg or an
injection of saline at the end of two weeks on HFD. For the following week 3 and 4, the rats
were given one s.c. injection of AOM at a dosage of 15 mg/kg or an injection of saline per
week. MNU and AOM showed a relative specificity for their respective organs. Rats injected
with MNU alone had only mammary tumours and rats injected with AOM alone had colon
tumours. At the end of the protocol (32 weeks), the author reported similar mammary tumour
incidence between MNU+AOM treated rats and rats treated with MNU alone (100% vs 95%).
The colon tumour incidence was also similar between rats treated with MNU+AOM and AOM

24
alone (70% vs 65%). The authors also used a short-term protocol (11 weeks), which resulted in
identical mammary tumour incidence in both MNU+AOM-treated rats and rats treated with
MNU (80% vs 80%). In this short-term protocol, only ACF but no colon tumours were detected.
The number of ACF formed was not significantly different as rats treated with MNU+AOM had
64.9±8.38 and rats treated with AOM had 63.6±7.52. This short-term protocol is the protocol
followed in this thesis.
1.8 Rationale
A large body of epidemiological studies and in vitro studies point to the potential
mitogenic actions of insulin glargine. However, the epidemiological studies only show
association, which may not be causal, and the in vitro studies cannot address the
pharmacokinetics, such as peak action by NPH and proteolytic metabolism of insulin glargine.
Currently, there is a paucity of preclinical animal studies that investigate the effect of insulin
glargine on breast and colon cancer promotion. Moreover, only a dearth of available data
regarding the effect of insulin detemir on cancer promotion under in vivo condition is available.
Thus, the current study investigates the effect of insulin glargine and detemir on breast and
colon cancer promotion in carcinogen-treated female Sprague-Dawley rats.
1.9 Hypothesis
Insulin glargine treatment will promote breast and colon cancer to a greater extent than
treatment with unmodified insulin (NPH) or other insulin analogues. To test this hypothesis, we
used a carcinogen-induced mammary and colon tumour model in rats.

25
CHAPTER 2
Materials and Methods
2.1 Procedure
2.1.1 Experimental animal model and sacrifice procedures
Figure 8: Overall Schematic Animal Protocol 120 female Sprague-Dawley rats, age of 3
weeks, were used. Following a week of acclimatization to the facility, a high fat diet (HFD) was
provided. After two weeks, one s.c. MNU injection (50mg/kg) was given and for the following
two weeks, one s.c. AOM injection (15mg/kg) was given per week. 4 days later, the dark cycle
was anticipated by 6 hours (12 hour light/dark cycle beginning at 7am to 12 hour light/dark
cycle beginning at 1am) (the reason for anticipating the dark cycle is explained in the text).
Then at age of 9 weeks, all rats were randomly allocated into four groups (Saline control, NPH,
glargine, or detemir) and injected subcutaneously with assigned treatments 5 times/week for 6
weeks. When the rats were 15 weeks old, they were sacrificed for further analysis. The
carcinogen injection protocol used was a well-established rapid dual-organ carcinogen model
protocol (156). The insulin injection protocol used was that of Tran et al. (95) and Lu et al (100).

26
2.1.1.1Animals
The rapid dual carcinogenesis model of Shivapurkar et al. (156) was used. A hundred
and twenty 3 week old female Sprague-Dawley rats weighing 50-60g were obtained from
Charles River Laboratory International Inc. They were exposed to a 12 h light/dark cycle and
caged in static cages in the animal facility (Department of Comparative Medicine, Medical
Science Building, University of Toronto). The temperature of the animal facility was 22oC and
60% humidity. After 1 week of acclimatization during which they were fed a regular pelleted
rodent chow, the diet was switched to the HFD used in Shivapurkar et al. (156). The HFD was
purchased from Dyets Inc. in Bethlehem, Pennsylvania, USA (Table 3). The purpose of the
HFD was to induce insulin resistance (157) and also increase the tumour incidence (156).
Table 3: Diet information The nutrient breakdown of the High Fat Diet (HFD) used in the
experiment. The table was taken from Shivapurkar et al. (156). The diet contains roughly 40%
fat by calorie.
2.1.1.2 Carcinogen Preparation
According to the protocol in Shivapurkar et al. (156) the mammary tumours were
induced by MNU (Sigma). MNU was dissolved in 0.9% NaCl saline (vehicle) at a

27
concentration of 10mg/ml. ACF were induced by AOM (Sigma). AOM was also diluted in
0.9% NaCl saline at a concentration of 10mg/ml.
2.1.1.3 Injections
2.1.1.3.1 Carcinogens
One s.c. injection of MNU at a dosage of 50mg/kg was given to 6 week old rats to
induce mammary tumours. For the following two weeks, one s.c. injection of AOM at a dosage
of 15mg/kg was given each week to induce ACF as per Shivapurkar et al. (156) (Figure 7).
These injections were performed by Rudolf Furrer, who is a senior technician as well as an
expert in animal cancer models.
2.1.1.3.2 Insulin
The insulin treatment was same as in Tran et al. (95) and Lu et al. (100). Three days
before insulin injection began, the light/dark cycle was anticipated by 6 hours (from 7am-
7pm(light) 7pm-7am(dark) to 1am-1pm(light) 1pm-1am(dark)). This was done in preparation
for insulin injections because we wished the rats, which eat in the dark, once injection to eat at
the peak of insulin effect in order to avoid hypoglycemia. S.c. insulin injections were given 5
times a week (from Monday to Friday) between 11am-noon for 6 weeks starting when the rats
were 9 weeks old. Rats were randomly allocated into four groups: control (saline), NPH, insulin
glargine, and detemir (N=30 rats/group) (Figure 7). NPH is an unmodified human insulin, and
insulin glargine and detemir are long-acting insulin analogues. Rats were injected
subcutaneously with the assigned treatments. They were injected with increasing dosage for the
first week as follows: 5U/kg first two days, 10U/kg next two days, and 15U/kg for the
remainder of the experiment, which according to blood glucose levels obtained at the peak of
insulin action (4-8 hours after injection) achieved a moderate degree of glucose lowering
(glucose level of 4-5mM). The insulin dosage was recalculated weekly according to the body
weight measurements.
2.1.1.4 Rat Monitoring
Metabolic measurements, including food consumption, weight, and blood glucose were
obtained twice a week (Monday and Thursday) before the injection of insulin. After insulin
injections commenced, blood glucose levels determined prior to every insulin injection (11am)
and 4-5 hours after the insulin injection (3-4pm). In a subgroup of rats, blood glucose was also
determined at 7pm (i.e. 8 hours after the insulin injections). Blood glucose was obtained by a
nick in the tail and glucose levels were measured by a glucose meter (The OneTouch Ultra 2

28
Meter). The glycated hemoglobin (HbA1c level of each rat was determined just before sacrifice
using the A1C NOW kit from Bayer.
2.1.1.5 Sacrifice
When the rats were 15 weeks old, they were sacrificed. As the rats had to be sacrificed
between 4-5 hours after the insulin injection, the assigned insulin injection was given to each rat
every 15 minutes beginning at 11am. The sacrifice began at 3pm. As mentioned, the HbA1c
level was measured prior to euthanasia for each rat. The rats were euthanized by ketamine
injection at a dosage of 1 ml/kg. The euthanized rats were palpated for any presence of
mammary tumours and the tumours were excised if there were any. Thus, we might have
missed small non-palpable tumours. The excised mammary tumours were cut in half. Each
mammary tumour was weighed and subsequently, one half of the tumour was fixed in formalin
for histological analysis and the other half was frozen in liquid nitrogen for Western Blot.
Following the mammary tumour excision, the colon was cut out from the anus to just before the
caecum. Then the colon was washed thoroughly with phosphate buffered solution (PBS). Any
fat and connective tissues that were attached to the colon were removed. The clean colon was
cut into three pieces and laid on a Petri dish paper and these pieces were cut open along the
longitudinal median axis and spread out flat. Then the paper was placed in a Petri dish to be
fixed in 10% formalin. The Petri dishes containing all the colon samples were stored in air-
sealed containers.
2.2 Tumour Evaluation Methods
2.2.1 Mammary Tumour Analysis
Mammary glands were palpated and mammary tumours were measured (length and
width) using a caliper twice a week. At sacrifice, the excised tumours were weighed. A few
(n=) mammary tumours in each group underwent histological analysis by a pathologist
Dr.R.Renlund) after hematoxylin & eosin staining performed by the pathology lab.
2.2.2. Western Blots
Frozen mammary tumours were collected as described in 2.1.1.5 and homogenized with
a homogenizer in radioimmunoprecipitation assay (RIPA) buffer containing protease inhibitor
cocktail (Roche Diagnostics, Laval, QC). The cell lysates were then spun at 12,000rpm for 10
minutes and the supernatant mixed with the dye was loaded onto 10% gel (Biorad, Hercules,
CA) and transferred onto polyvinylidene fluoride (PVDF) membrane using the Turbo Blotter
Transfer System (Biorad, Hercules, CA). The membrane was cut longitudinally along the 55

29
kDa protein ladder line to separately detect for Akt and Erk1/2. The membrane that contained
the protein size bigger than 55 kDa was probed with rabbit anti-phospho Akt (60 kDa) antibody
(Cell Signaling) at a 1:500 dilution and developed on a film after detection with anti-rabbit
secondary antibody (1:1000). Then the identical membrane was stripped and probed for Total
Akt with rabbit anti-Akt antibody (Cell Signaling) at a 1:1000 dilution, which was developed
again on a film. The other membrane that retained protein size smaller than 55kDa was used for
detection of Erk1/2 (42 and 44 kDa) by using rabbit anti-phospho Erk1/2 antibody (Cell
Signaling) at a 1:500 dilution and developed on a film after detection with anti-rabbit secondary
antibody (1:1000). The actin was also detected using the corresponding membrane with goat
anti-actin at a 1:1000 dilution and developed on a film after detection with anti-goat secondary
antibody (1:1000). The images were then quantified using Image J software.
2.2.3 ACF Scoring
Fixed colons were first washed with PBS and placed on microscope slides. Then each
colon was stained with 0.1% methylene blue solution (methylene blue powder was dissolved in
PBS and filtered to remove any debris) for 10 minutes. Each colon was washed again with PBS
and scored for ACF with a light microscope.
2.3 Calculations
2.3.1 Power calculations
Initially, a sample size calculation was done based on the following equation extracted
from a paper by Florey (158):
n= ((1.96 + 0.842)2(p
lq
l +p
2q
2))/True difference
2
where p1 and p
2 are the percentages of rats that had mammary tumour (tumour incidence) and q
1
and q2 are the percentages of rats that did not have any mammary tumour (100-p
1) in the NPH
and control groups respectively. The true difference is the percentage difference in mammary
tumour incidence between control and insulin-treated rats. We used the incidence value
obtained in pilot data (33.3% difference between control and NPH). The value 1.96 is a
multiplier when α = 5% or 0.05 and 0.842 is a multiplier when β = 20% or 0.2, giving a power
of 80%. With the power of 80%, we obtained a n=30/group.
Based on our pilot data that showed a significant difference in tumour multiplicity, we
also performed a power calculation for tumour multiplicity using the following equation (158):
n=2(1.96+0.842)2 s
2/d
2

30
where d is the difference between the groups and s is the standard deviation of the variable. the
value 1.96 is a multiplier when α = 5% or 0.05 and 0.842 is a multiplier when β = 20% or 0.2,
giving a power of 80%. With the power of 80%, we obtained a n=28/group. Thus, we used 30
rats per group for this study.
2.3.2 Statistical Analysis
Continuous data are presented as means +/- standard error (SEM). Statistics were done
with one way nonparametric analysis of variance (ANOVA) followed by Tukey's posthoc test
for continuous data, Fisher's exact test followed by Bonferroni's correction was used for
categorical data (incidence). Calculations were performed using statistical analysis software
(SAS) (Cary, NC).

31
Chapter 3
Results
All results refer to 30/group, unless otherwise specified.
3.1 Metabolic Measurements
3.1.1 Rat Weight
The weekly average weight of each group is plotted throughout the protocol. Although it
was expected that the weight of insulin-treated groups would be higher than that of the control,
the average weight between four groups showed no difference (Figure 9).
Figure 9: Weekly average body weight The body weight of each group did not differ among
groups. Data are presented as means +/- SEM.
3.1.2 Food Consumption
The weekly average food consumption of HFD (HFD consumption began at 4 weeks of age) of
each rat was measured and showed that all four groups consumed similar amount of diet. A
slight decrease in food consumption in all groups between 6-8weeks may be due to the stress
arisen from carcinogen injections (Figure 10). Also, it is possible that a transient peak at 5
week is due to the 'novelty' of the HFD.

32
Figure 10: Weekly average food consumption Food consumption did not differ among
groups. Data are presented as means +/- SEM.
3.1.3 Blood Glucose Levels
When measured at 11am (before the insulin treatment), the blood glucose levels of all
groups remained relatively constant throughout the experiment. However, soon after the
commencement of insulin injections in three groups (NPH, glargine, and detemir), we observed
that the insulin treated groups maintained slightly but significantly higher blood glucose levels
than the control group at 11am (Figure 11), consistent with a glucose rebound presumably due
to counter-regulation. While the blood glucose level of control group remained constant when
measured at 3pm (peak insulin release: 4 hours after the insulin treatment), the three insulin
treated groups (NPH, glargine, and detemir) showed significantly decreased blood glucose
levels at the same time (Figure 12). In a few rats (n in figure legend) blood glucose levels were
measured at 7pm (end of peak release: 8 hours after the insulin treatment) (Figure 13). Insulin
glargine and NPH groups had significantly lower blood glucose levels compared to control and
insulin detemir showed significant decrease during last week. To determine the average blood
glucose concentration over the protocol duration, HbA1C levels were measured at sacrifice
(Figure 14). As expected, all three insulin treated groups had significantly lower glycated
hemoglobin levels compared to the control.

33
Figure 11: Blood glucose before insulin injection Blood glucose measured at 11 am (Prior to
insulin injection) of each group. Data are presented as means +/- SEM.
Figure 12: Blood glucose at 4 hours post-insulin injection Blood glucose measurements 4
hours after insulin injections for each group. Data are presented as means +/- SEM . *P<0.05 vs.
control

34
Figure 13: Blood glucose at 8 hours post-insulin injection Blood glucose measurements 8
hours after insulin injections for each group. Control n=12, NPH n=10, Glargine n=11, and
Detemir n=8. Data are presented as means +/- SEM. *P<0.05 vs. control
Figure 14: Glycated hemoglobin level Glycated hemoglobin level taken at sacrifice for each
group. Data are presented as means +/- SEM. *P<0.05 vs. control

35
3.2 Mammary Tumour Analysis
3.2.1 Mammary Tumour Incidence, multiplicity, burden, growth rate
At sacrifice, the mammary tumour incidence of insulin glargine and detemir groups
showed a comparable result as control (57% and 63 vs. 60%). NPH displayed a tendency for an
increase in tumour incidence compared to the control (80% vs. 60%) (Figure 15). In a few rats
(n in figure) where we had data to show the cumulative incidence overtime and the mammary
tumour incidence overtime of all insulin treated groups tended to have shorter latency period
compared to control group (Figure 16). Insulin glargine and detemir showed a strong tendency
towards increased tumour multiplicity (average number of tumours per rat) vs. control (1.53 and
1.43 vs. 0.8), but the difference was not significant. NPH group had a significantly higher
tumour multiplicity versus control (1.77 vs. 0.8) (Figure 17). Finally, while the increase was not
significant, all insulin-treated groups tended to have higher tumour burden compared to control
(Figure 18). In a few rats (n in Figure), where we had longitudinal data on tumour growth, we
did not find significant differences among groups (Figure 19).
Figure 15: Mammary tumour incidence Mammary tumour incidence (% of tumour positive
of all rats) was determined at sacrifice and analyzed. n=30/group for all graphs unless specified

36
Figure 16: Mammary tumour incidence over time cumulative mammary tumour incidence in
rats following the 50mg/kg MNU injection. Insulin injection began when rats were 9 weeks old.
Figure 17: Mammary tumour multiplicity Tumour multiplicity (number of tumours/rat) of
each group. Value in non-tumour-bearing rats was counted as 0. Data are presented as means
+/- SEM P<0.05 vs. control.

37
Figure 18: Mammary tumour burden The total tumour weight is the additions of all tumour
weights per rat. Data are presented as means +/- SEM.
Figure 19: Increase in tumour area/day Overtime measurement of mammary tumour growth
rate/day. Data are presented as means +/- SEM

38
3.2.2 Histology
One representative tumour from each group underwent histological analysis. The
tumours exhibited abnormal architecture including reduced tubule formation, hyperchromia and
mitosis, and irregular size and shape of the nuclei, which are all indicators of carcinoma (Figure
20). A pathologist (Dr.Renlund) confirmed that these tumours were adenocarcinomas.
Figure 20: Histology of Mammary tumours in each group. H&E stained mammary tumours
of a representative tumour from NPH group at 40x magnification. Black and white arrows
denote mitotic figures and prominent nucleoli respectively.
3.2.3 Western Blot
Pilot Western blot results showed a tendency for greater p-Akt phosphorylation in the NPH
group (Figure 21).

39
p-Akt p-Erk1/2
Actin Actin
Figure 21: Preliminary Western blots results Expression levels of phospho-Akt and phospho
Erk1/2, which are markers of Akt and Erk activity respectively, were analyzed. As a loading
control, actin levels were also measured.
3.3 Colon Cancer Precursors (ACF) Results
ACF, the putative preneoplastic lesions, were scored and analyzed (Figure 22). The
average total number of ACF in each rat and the average number of crypts per ACF were
determined. All three insulin treated groups displayed no significant difference compared to
control group in the total number of ACF and the number of crypts per ACF.
Figure 22: ACF analysis a) Analysis of total ACF number per rat b) ACF multiplicity. Data
are presented as means +/- SEM

40
CHAPTER 4
Discussion
Since the insulin discovery in 1921, insulin-based therapies have played a vital role in
controlling the blood glucose levels of patients with diabetes. With recombinant technology,
insulin analogues have been developed for their favorable pharmacokinetics but the molecular
modifications of the original human insulin molecule sometimes resulted in unexpected changes
in its properties: an increased mitogenic effect. Ever since insulin glargine was reported to
potentially increase cancer risks, enormous efforts have been made to address its true potential
as a cancer-promoter, but much remains to be unveiled. Epidemiological studies showed that
breast cancer was predominantly linked with the use of insulin glargine (106;107;109;110). In
vitro studies showed an increased mitogenic potency of insulin glargine using the MCF-7 breast
cancer cell line (mainly used due to its greater sensitivity towards insulin than other cell lines
(159)), which supported the epidemiological findings (89;121;123;128). Although various cell
line studies also demonstrated higher proliferation in HCT-116 colorectal cancer cells when
treated with insulin glargine (89;127), the epidemiological studies of the link between insulin
glargine and colon cancer are mostly negative (71;107). With a limited number of preclinical
animal studies (only one abstract, sponsored by the glargine producer, reporting no effect of
insulin glargine on tumour growth of mouse mammary tumour orthografts unlike IGF-1 (134)),
acknowledging the carcinogenic potential of insulin glargine solely based on epidemiological
studies and in vitro studies is far-fetched. Thus, the current study investigated the mammary and
colon cancer-promoting potency of the long-acting insulin analogue, insulin glargine, compared
to the unmodified insulin NPH and saline control in carcinogen-treated female Sprague-Dawley
rats. We used a dual-organ carcinogen model to also study the effect of glargine on colon cancer
precursors because of the in vitro data, although based on the negative epidemiological data we
expected these colon precursor data to turn out mainly as a negative control. Another long-
acting insulin analogue, insulin detemir, although not generally associated with cancer, was also
included in our study because it had not been widely investigated.

41
4.1 Mammary Cancer
The NPH group displayed the highest mammary tumour incidence (80%) although the
results were not significant compared to control. While the differences in tumour burden were
not significant, tumour multiplicity was significantly higher in NPH compared to control (1.77
vs. 0.8, p<0.05). The glargine and detemir groups did not show greater tumour incidence,
multiplicity, and burden than the NPH group and in fact, in these groups, tumour multiplicity
was not significantly different from control. Tumour incidence and multiplicity are suggestive
of cancer initiation and promotion whereas tumour burden reflects tumour growth. Thus,
considering the general acceptance of insulin as a growth factor, a significant increase in tumour
multiplicity seen in our study suggests that insulin increases the susceptibility of cell mutation
perhaps because of its effect of proliferation (proliferating cells are more susceptible to
mutations) or allows mutated cells to survive because of decreased apoptosis. This effect of
NPH may be the result of its pharmacokinetics, which exhibits a prominent peak 4-8 hours after
the injection. During this peak, NPH may possibly cross a threshold (160) for cancer promotion,
while insulin analogues with relatively stable release may not or may less so. The insulin levels
will be determined. However, due to the different cross-reactivity of the analogues with the
radioimmuno assay, the results may not be totally reliable. Nevertheless, the blood glucose at
defined time points and overall glycated hemoglobin suggest that the effect on glucose
metabolism was the same in all insulin groups. In contrast to our results, there is one study that
did not find a promoting effect of insulin on mammary carcinogenesis in the female Sprague-
Dawley rat model (100). In this study, intraperitoneal (i.p.) injection of MNU at a 37.5mg/kg
dosage was given to rats. Over the duration of 26 weeks, no significant differences in mammary
tumour incidence, and number of tumours per tumour-bearing rat between NPH insulin treated
rats and control rats were observed. However, the diet used in this study differed from that of
the current study. The study used pelleted AIN-93M diet, which is a diet commonly used for
maintenance of the animal and composed of 10% fat by calorie. However, our study used HFD
that contained 40% fat by calorie. The differences in the diet may have resulted in different
metabolic conditions in the animals, such as insulin resistance, which may produce different
outcomes between two studies. As indicated in the introduction, insulin resistance is associated
with inflammation and oxidative stress, which may amplify the effect of insulin on cancer.
Indeed, most studies supported the link between all-type cancer and type 2 diabetic patients (67-
73), whose main characteristic is insulin resistance, whereas this link is not clear in type 1

42
diabetes (31). Preliminary Western blot results showed increased phospho-Akt content in the
tumour with NPH compared to control. Increased promotion of mammary cancer by NPH
insulin is consistent with the Western blot results because the proliferative effect of insulin on
mammary cancer is thought to be more dependent on the Akt signaling pathway (89). In terms
of tumour burden, our study did not find significance but a tendency for all insulin-treated
groups to show increased tumour burden compared to control. However, tumour growth did not
appear to be affected. A definite conclusion about tumour growth should not be extrapolated
solely based on this study because our study was a short-term experiment and the protocol was
not designed for assessing tumour growth. There is a study that used Sprague-Dawley rats fed
with DMBA to measure the mammary tumour growth promotion by insulin (55). This study
found almost 5-fold increase in tumour growth in rats injected daily with insulin (unmodified
insulin, Lente preparation). However, this study used a different carcinogen (20mg/kg DMBA
dissolved in sesame oil vs. 50mg/kg s.c. injection of MNU) and higher insulin dosage (25 U/kg
vs 15U/kg) than our study. The effects of insulin on mammary cancer are in accordance with
other in vivo studies that showed increased tumour growth of DMBA-treated Sprague-Dawley
rats (55;98) and human breast cancer cell (MCF-7) orthografts in nude mice (99) by exogenous
insulin treatment.
Insulin glargine displayed no significant promotion of mammary cancer compared to
control. These results imply that glargine does not promote mammary cancer more than
unmodified human insulin (NPH) and may even have less promoting effect. These results
contradicted our hypothesis that was based on various epidemiological and in vitro studies
(70;89;106;107;109;124;127;133). No increase in mammary cancer promotion in our study may
be due to rapid metabolism of insulin glargine after its s.c. injection into glargine metabolites,
M1 and M2 (predominantly M1), which exhibit comparable binding affinities towards IR and
IGF-1R as regular insulin (11). As a consequence, both M1 and M2 were found to have equal
mitogenic potential compared to human insulin in the same study. Therefore, insulin glargine
may behave like regular insulin in vivo. Differences in glargine metabolism between individuals
may account for the different results observed in epidemiological studies as a study showed
greater proliferation of MCF-7 cells when exposed to the serum of type 1 diabetic patients
under insulin glargine treatment compared to serum of NPH users (133). Although
quantification of insulin analogues in plasma is difficult, our preliminary data (collaboration
with Dr.Thevis in Germany) suggest that M1 and M2 are present in rat plasma of glargine-

43
treated rats. The absence of adverse effect of insulin glargine on mammary cancer is consistent
with the aforementioned ADA abstract, which showed no increased breast cancer growth in
glargine-treated mice compared to control (134).
For insulin detemir, our study showed no increase in mammary tumour incidence,
multiplicity, and burden compared with NPH. Although there are not many available studies, a
meta-analysis from the producing company of detemir showed no carcinogenic effect (161).
Detemir exhibited a much lower binding affinity to IGF-1R compared to insulin glargine (124)
and a lower binding affinity towards IRs compared to regular insulin (127). while in vitro
studies are contradictory (89;122;127). However, binding affinity studies are difficult with
detemir because of its affinity for albumin.
Although the difference in tumour multiplicity expressed as the number of tumours/rat
between long-acting insulin analogues (glargine or detemir) and control did not reach statistical
significance, when tumour multiplicity was expressed as number of tumours/tumour-bearing rat,
there was a significant difference between glargine and control, and the difference between
detemir and control almost reached significance (Appendix A). These findings suggest that all
insulins have the same effect. Because of this and because insulin itself has been amply shown
to promote cancer in epidemiological studies, we can combine the insulin treated groups. When
combined insulin therapy (NPH, glargine, and detemir) is compared with control, a significant
increase in mammary tumour multiplicity and burden, and tendency to shorten tumour latency
are observed (Appendix A). These observations suggest the importance of action of insulin on
cancer promotion. This action is likely exerted directly via the activation of IR as a study
reported that specific down-regulation of IR by short hairpin RNA (shRNA) in breast cancer
cell lines (T46D and LCC6) lead to reduced formation of in vitro colonies and reduced tumour
growth in vivo (162). The effect of unmodified insulin and insulin analogues on cancer
promotion via IR requires further research in IR knock-out model.
4.2 Colon Cancer
The current study did not show any significant differences in the total number of ACF
and crypt multiplicity per ACF between the groups. Insulin glargine displayed no adverse
effects on either ACF formation or crypt multiplicity when compared to saline control, NPH,
and insulin detemir. While insulin glargine displayed an increased proliferative effect on HCT
116 colorectal cancer cells compared to regular insulin (89), glargine did not increase ACF

44
number and multiplicity compared to unmodified insulin in the only available in vivo study
(130). The absence of a promoting effect of insulin glargine on ACF formation compared to
NPH observed in our study was in accordance with this study using AOM-treated female db/db
mice, which reported no significant differences in epithelial colonic proliferation and ACF
formation between insulin glargine and NPH. However, the latter study observed a significantly
higher epithelial colonic proliferation and ACF formation for both insulin- and glargine-treated
groups when compared to saline control after 18 week treatment. There are two studies that
reported an increased ACF multiplicity and colon tumour incidence in insulin-treated rats
(95;96). One study used AOM-treated female F344 rats injected with Ultralente bovine insulin
and reported a significantly higher ACF multiplicity versus saline control for 100 days (96).
The other study by Tran et al., demonstrated that NPH is a colon tumour promoter in AOM-
treated male F344 rats (95). The authors gave s.c. injection to the rats 5 times/week with NPH at
a same dosage of insulin as our study. The insulin treatment continued for 17 weeks and they
found a significant increase in colon tumour incidence with insulin vs. saline control (79% vs.
50%). The different results of the effect of insulin on colon cancer promotion in our study
compared to others may be due to different strains of rat, gender, and duration of treatment. The
male F344 rat is a better established as model of colorectal cancer than the female Sprague-
Dawley rat, although AOM-treated female Sprague-Dawley rats do develop colonic tumour
(156). Also, male rats are known to be more prone to develop colorectal cancer when induced
by a carcinogen (163-165). The reason may be the lower estrogen in male animals because
estrogen reduces synthesis and secretion of bile acids, which are believed to be carcinogenic to
colon epithelium (166-168).
Speculations of the effect of insulin analogues on colon tumour solely based on ACF
may lead to misinterpretations. Despite the acknowledgement of ACF as the preneoplastic
lesions of colon tumours, MDF may be better predictor of colon tumour incidence (153).
4.3 General Discussion, Limitations, and Future Directions
While there are only a few animal studies available on the effect of long-acting insulin
analogues on cancer promotion, our study investigated the effects of long-acting insulin
analogues specifically on mammary and colon cancer promotion compared to saline control and
NPH. Our study used the female Sprague-Dawley rat, a well-established animal model that has
been shown to be susceptible to both MNU and AOM (156). Moreover, this model was used for

45
assessing the effects of regular insulin on mammary cancer (100). We assessed mammary
cancer, which is generally thought to be influenced by insulin glargine the most, and colon
cancer precursors mainly as a negative control. Animal studies allow consideration of the
pharmacokinetics and biotransformation of insulin glargine into its metabolites, M1 and M2, in
serum. The metabolism of glargine is shared by both humans and rats so the results of this study
may be clinically relevant (131).
While there are strengths in this study, some limitations exist. First, it is possible that the
duration of insulin treatment, although enough to detect the action of insulin (97), was not long
enough to detect the differences between the types of insulin. Second, although the Sprague-
Dawley rat is a well-established and widely used model of mammary carcinogenesis, these rats
do not develop hyperglycemia despite being fed a HFD. Also, while a 40% HFD is known to
induce insulin resistance (157), we did not confirm the insulin resistant state. Even though there
are numerous methods available to measure insulin resistance, most of the accurate methods are
not feasible for this study. For example, hyperinsulinemic euglycemic glucose clamping, which
is known to be a gold-standard for measuring insulin resistance, requires vessel cannulation of
the rats for i.v. infusion of insulin and glucose and is therefore too invasive. However, we could
have performed an insulin tolerance test (ITT), which only requires one i.p. injection of insulin.
Alternatively, insulin signaling in target tissues could be assessed and we have collected liver
tissues to address this issue. Another limitation includes scoring ACF as a preneoplastic lesion
for colon cancer. As mentioned above, ACF have been criticized as a predictor of colon tumour
incidence or multiplicity. In order to better estimate colon cancer promotion in a short-term
protocol, MDF can be scored instead.
Although our study provided evidence that long-acting insulin analogues do not
adversely affect both mammary and colon cancer promotion, future studies must follow-up on
our results. Studying the cancer-promoting effects of the long-acting insulin analogues on
diabetic animal models, such as Zucker diabetic fatty (ZDF) rats or HFD fed streptozotocin-
treated rats, would better mimic the conditions of diabetic patients. Also, the dose of insulin
would be more relevant to the therapeutic doses. The streptozotocin-HFD model is perhaps
preferable to the ZDF model because in Zucker rats, from which the ZDF rats are derived,
MNU was found to induce benign cysts rather than carcinomas (169). Finally, when attempting
to translate the results obtained in animal models to humans, it should be mentioned that in vivo
studies in animals address the effect of insulin and insulin analogues on animal tumours when

46
in fact, comparison of binding affinity and receptor composition between human and rat tissues
and tumours have not been thoroughly investigated. The binding affinity of insulin analogues to
rat IR and IGF-1R may not be identical as to human IR and IGF-1R. Moreover, the expression
levels of these two receptors in rat mammary tumour have not been thoroughly characterized. A
possible method to overcome this issue is to engraft MCF-7 human breast cancer cell line in
immunodeficient mice. This study would allow an examination of human mammary cancer
response to insulin analogues in an in vivo setting. It would also allow to better study the effect
of mammary tumour growth. Furthermore, a long-term study with colon tumour incidence as an
endpoint could be performed to confirm the findings of ACF data. Even if MDF, which is
thought to be a better predictor of colon tumour incidence, are scored instead of ACF, it is
always preferable to validate the results with colon tumour endpoint. An experimental protocol
of 21 weeks should be sufficient to analyze the colon tumour incidence according to previous
studies (95). Another future study should assess the carcinogenic potential of insulin degludec,
which is the newest ultra long-acting insulin analogue. Since it was approved very recently in
Europe and is still not approved in Canada, we could not include it in our study. There are
currently no studies investigating the cancer risks involved in using insulin degludec and also,
there are no in vitro studies assessing its binding affinity for IGF-1R or IR to our knowledge.
Thus, investigating the binding affinity of insulin degludec on IR and IGF-1R and proliferation
on cell culture would be valuable although degludec structure is similar to detemir and
therefore, similar results may be expected. Within the present limitations, our study is the first
to compare unmodified insulin and insulin analogues to show that insulin glargine does not
have a greater carcinogenic effect than unmodified insulin in a breast cancer model. This is
important to know in the management of patients of diabetes since glargine is one of the most
widely used insulin analogues.

47
Reference List
1. Nathan,DM: Long-term complications of diabetes mellitus. N Engl J Med 328:1676-
1685, 1993
2. Coughlin,SS, Calle,EE, Teras,LR, Petrelli,J, Thun,MJ: Diabetes mellitus as a predictor
of cancer mortality in a large cohort of US adults. Am J Epidemiol 159:1160-1167,
2004
3. Johnson,JA, Bowker,SL, Richardson,K, Marra,CA: Time-varying incidence of cancer
after the onset of type 2 diabetes: evidence of potential detection bias. Diabetologia
54:2263-2271, 2011
4. Lambe,M, Wigertz,A, Garmo,H, Walldius,G, Jungner,I, Hammar,N: Impaired glucose
metabolism and diabetes and the risk of breast, endometrial, and ovarian cancer.
Cancer Causes Control 22:1163-1171, 2011
5. Lipscombe,LL, Goodwin,PJ, Zinman,B, McLaughlin,JR, Hux,JE: Increased
prevalence of prior breast cancer in women with newly diagnosed diabetes. Breast
Cancer Res Treat 98:303-309, 2006

48
6. Lipscombe,LL, Goodwin,PJ, Zinman,B, McLaughlin,JR, Hux,JE: Diabetes mellitus
and breast cancer: a retrospective population-based cohort study. Breast Cancer Res
Treat 98:349-356, 2006
7. Michels,G, Mohamed,GA, Weber,N, Chovolou,Y, Kampkotter,A, Watjen,W,
Proksch,P: Effects of methylated derivatives of Luteolin isolated from Cyperus
alopecuroides in rat H4IIE hepatoma cells*. Basic Clin Pharmacol Toxicol 98:168-
172, 2006
8. Galloway,JA, Hooper,SA, Spradlin,CT, Howey,DC, Frank,BH, Bowsher,RR,
Anderson,JH: Biosynthetic human proinsulin. Review of chemistry, in vitro and in
vivo receptor binding, animal and human pharmacology studies, and clinical trial
experience. Diabetes Care 15:666-692, 1992
9. BURNHAM,DK: Insulin and insulin mixtures; nph insulin. Calif Med 75:412-415,
1951
10. Smith,U, Gale,EA: Does diabetes therapy influence the risk of cancer? Diabetologia
52:1699-1708, 2009
11. Sommerfeld,MR, Muller,G, Tschank,G, Seipke,G, Habermann,P, Kurrle,R,
Tennagels,N: In vitro metabolic and mitogenic signaling of insulin glargine and its
metabolites. PLoS One 5:e9540, 2010

49
12. Havelund,S, Plum,A, Ribel,U, Jonassen,I, Volund,A, Markussen,J, Kurtzhals,P: The
mechanism of protraction of insulin detemir, a long-acting, acylated analog of human
insulin. Pharm Res 21:1498-1504, 2004
13. Tahrani,AA, Bailey,CJ, Barnett,AH: Insulin degludec: a new ultra-longacting insulin.
Lancet 379:1465-1467, 2012
14. Kim,JJ, Accili,D: Signalling through IGF-I and insulin receptors: where is the
specificity? Growth Horm IGF Res 12:84-90, 2002
15. Frasca,F, Pandini,G, Sciacca,L, Pezzino,V, Squatrito,S, Belfiore,A, Vigneri,R: The
role of insulin receptors and IGF-I receptors in cancer and other diseases. Arch Physiol
Biochem 114:23-37, 2008
16. Varewijck,AJ, Janssen,JA: Insulin and its analogues and their affinities for the IGF1
receptor. Endocr Relat Cancer 19:F63-F75, 2012
17. Pollak,M: Insulin and insulin-like growth factor signalling in neoplasia. Nat Rev
Cancer 8:915-928, 2008
18. LeRoith,D: Insulin-like growth factor I receptor signaling--overlapping or redundant
pathways? Endocrinology 141:1287-1288, 2000
19. Vigneri,P, Frasca,F, Sciacca,L, Pandini,G, Vigneri,R: Diabetes and cancer. Endocr
Relat Cancer 16:1103-1123, 2009

50
20. Paonessa,F, Foti,D, Costa,V, Chiefari,E, Brunetti,G, Leone,F, Luciano,F, Wu,F,
Lee,AS, Gulletta,E, Fusco,A, Brunetti,A: Activator protein-2 overexpression accounts
for increased insulin receptor expression in human breast cancer. Cancer Res 66:5085-
5093, 2006
21. Shan,HB, Zhang,R, Li,Y, Xu,GL, Luo,GY, Gao,XY, Yang,HL: Expression of IGF-1R
in colorectal polyps and its role in colorectal carcinogenesis. Technol Cancer Res
Treat 10:381-389, 2011
22. Pandini,G, Frasca,F, Mineo,R, Sciacca,L, Vigneri,R, Belfiore,A: Insulin/insulin-like
growth factor I hybrid receptors have different biological characteristics depending on
the insulin receptor isoform involved. J Biol Chem 277:39684-39695, 2002
23. Pollak,M: The insulin receptor/insulin-like growth factor receptor family as a
therapeutic target in oncology. Clin Cancer Res 18:40-50, 2012
24. Tognon,CE, Sorensen,PH: Targeting the insulin-like growth factor 1 receptor (IGF1R)
signaling pathway for cancer therapy. Expert Opin Ther Targets 16:33-48, 2012
25. Kasper,JS, Giovannucci,E: A meta-analysis of diabetes mellitus and the risk of
prostate cancer. Cancer Epidemiol Biomarkers Prev 15:2056-2062, 2006
26. Deng,L, Gui,Z, Zhao,L, Wang,J, Shen,L: Diabetes mellitus and the incidence of
colorectal cancer: an updated systematic review and meta-analysis. Dig Dis Sci
57:1576-1585, 2012

51
27. Ben,Q, Xu,M, Ning,X, Liu,J, Hong,S, Huang,W, Zhang,H, Li,Z: Diabetes mellitus and
risk of pancreatic cancer: A meta-analysis of cohort studies. Eur J Cancer 47:1928-
1937, 2011
28. Boyle,P, Boniol,M, Koechlin,A, Robertson,C, Valentini,F, Coppens,K, Fairley,LL,
Boniol,M, Zheng,T, Zhang,Y, Pasterk,M, Smans,M, Curado,MP, Mullie,P, Gandini,S,
Bota,M, Bolli,GB, Rosenstock,J, Autier,P: Diabetes and breast cancer risk: a meta-
analysis. Br J Cancer 107:1608-1617, 2012
29. Wang,C, Wang,X, Gong,G, Ben,Q, Qiu,W, Chen,Y, Li,G, Wang,L: Increased risk of
hepatocellular carcinoma in patients with diabetes mellitus: a systematic review and
meta-analysis of cohort studies. Int J Cancer 130:1639-1648, 2012
30. LeRoith,D, Novosyadlyy,R, Gallagher,EJ, Lann,D, Vijayakumar,A, Yakar,S: Obesity
and type 2 diabetes are associated with an increased risk of developing cancer and a
worse prognosis; epidemiological and mechanistic evidence. Exp Clin Endocrinol
Diabetes 116 Suppl 1:S4-S6, 2008
31. Giovannucci,E, Harlan,DM, Archer,MC, Bergenstal,RM, Gapstur,SM, Habel,LA,
Pollak,M, Regensteiner,JG, Yee,D: Diabetes and cancer: a consensus report. CA
Cancer J Clin 60:207-221, 2010
32. Adams,TD, Gress,RE, Smith,SC, Halverson,RC, Simper,SC, Rosamond,WD,
Lamonte,MJ, Stroup,AM, Hunt,SC: Long-term mortality after gastric bypass surgery.
N Engl J Med 357:753-761, 2007

52
33. Sjostrom,L, Narbro,K, Sjostrom,CD, Karason,K, Larsson,B, Wedel,H, Lystig,T,
Sullivan,M, Bouchard,C, Carlsson,B, Bengtsson,C, Dahlgren,S, Gummesson,A,
Jacobson,P, Karlsson,J, Lindroos,AK, Lonroth,H, Naslund,I, Olbers,T, Stenlof,K,
Torgerson,J, Agren,G, Carlsson,LM: Effects of bariatric surgery on mortality in
Swedish obese subjects. N Engl J Med 357:741-752, 2007
34. Sjostrom,L, Gummesson,A, Sjostrom,CD, Narbro,K, Peltonen,M, Wedel,H,
Bengtsson,C, Bouchard,C, Carlsson,B, Dahlgren,S, Jacobson,P, Karason,K,
Karlsson,J, Larsson,B, Lindroos,AK, Lonroth,H, Naslund,I, Olbers,T, Stenlof,K,
Torgerson,J, Carlsson,LM: Effects of bariatric surgery on cancer incidence in obese
patients in Sweden (Swedish Obese Subjects Study): a prospective, controlled
intervention trial. Lancet Oncol 10:653-662, 2009
35. Pan,SY, Johnson,KC, Ugnat,AM, Wen,SW, Mao,Y: Association of obesity and cancer
risk in Canada. Am J Epidemiol 159:259-268, 2004
36. Renehan,AG, Soerjomataram,I, Tyson,M, Egger,M, Zwahlen,M, Coebergh,JW,
Buchan,I: Incident cancer burden attributable to excess body mass index in 30
European countries. Int J Cancer 126:692-702, 2010
37. Renehan,AG, Tyson,M, Egger,M, Heller,RF, Zwahlen,M: Body-mass index and
incidence of cancer: a systematic review and meta-analysis of prospective
observational studies. Lancet 371:569-578, 2008

53
38. Kuriyama,S, Tsubono,Y, Hozawa,A, Shimazu,T, Suzuki,Y, Koizumi,Y, Suzuki,Y,
Ohmori,K, Nishino,Y, Tsuji,I: Obesity and risk of cancer in Japan. Int J Cancer
113:148-157, 2005
39. Calle,EE, Rodriguez,C, Walker-Thurmond,K, Thun,MJ: Overweight, obesity, and
mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med
348:1625-1638, 2003
40. Bergstrom,A, Pisani,P, Tenet,V, Wolk,A, Adami,HO: Overweight as an avoidable
cause of cancer in Europe. Int J Cancer 91:421-430, 2001
41. Louie,SM, Roberts,LS, Nomura,DK: Mechanisms linking obesity and cancer. Biochim
Biophys Acta 2013
42. Gregor,MF, Hotamisligil,GS: Inflammatory mechanisms in obesity. Annu Rev
Immunol 29:415-445, 2011
43. Neels,JG, Olefsky,JM: Inflamed fat: what starts the fire? J Clin Invest 116:33-35,
2006
44. van Kruijsdijk,RC, van der,WE, Visseren,FL: Obesity and cancer: the role of
dysfunctional adipose tissue. Cancer Epidemiol Biomarkers Prev 18:2569-2578, 2009

54
45. Weisberg,SP, McCann,D, Desai,M, Rosenbaum,M, Leibel,RL, Ferrante,AW, Jr.:
Obesity is associated with macrophage accumulation in adipose tissue. J Clin Invest
112:1796-1808, 2003
46. Liu,ZG, Hsu,H, Goeddel,DV, Karin,M: Dissection of TNF receptor 1 effector
functions: JNK activation is not linked to apoptosis while NF-kappaB activation
prevents cell death. Cell 87:565-576, 1996
47. Duyao,MP, Buckler,AJ, Sonenshein,GE: Interaction of an NF-kappa B-like factor
with a site upstream of the c-myc promoter. Proc Natl Acad Sci U S A 87:4727-4731,
1990
48. Guttridge,DC, Albanese,C, Reuther,JY, Pestell,RG, Baldwin,AS, Jr.: NF-kappaB
controls cell growth and differentiation through transcriptional regulation of cyclin
D1. Mol Cell Biol 19:5785-5799, 1999
49. McArdle,MA, Finucane,OM, Connaughton,RM, McMorrow,AM, Roche,HM:
Mechanisms of obesity-induced inflammation and insulin resistance: insights into the
emerging role of nutritional strategies. Front Endocrinol (Lausanne) 4:52, 2013
50. Dandona,P, Aljada,A, Bandyopadhyay,A: Inflammation: the link between insulin
resistance, obesity and diabetes. Trends Immunol 25:4-7, 2004
51. Samuel,VT, Petersen,KF, Shulman,GI: Lipid-induced insulin resistance: unravelling
the mechanism. Lancet 375:2267-2277, 2010

55
52. Cusi,K, Maezono,K, Osman,A, Pendergrass,M, Patti,ME, Pratipanawatr,T,
DeFronzo,RA, Kahn,CR, Mandarino,LJ: Insulin resistance differentially affects the PI
3-kinase- and MAP kinase-mediated signaling in human muscle. J Clin Invest
105:311-320, 2000
53. Gross,GE, Boldt,DH, Osborne,CK: Perturbation by insulin of human breast cancer cell
cycle kinetics. Cancer Res 44:3570-3575, 1984
54. Pollak,M: The insulin and insulin-like growth factor receptor family in neoplasia: an
update. Nat Rev Cancer 12:159-169, 2012
55. Heuson,JC, Legros,N, Heimann,R: Influence of insulin administration on growth of
the 7,12-dimethylbenz(a)anthracene-induced mammary carcinoma in intact,
oophorectomized, and hypophysectomized rats. Cancer Res 32:233-238, 1972
56. Osborne,CK, Bolan,G, Monaco,ME, Lippman,ME: Hormone responsive human breast
cancer in long-term tissue culture: effect of insulin. Proc Natl Acad Sci U S A
73:4536-4540, 1976
57. Mannucci,E: Insulin therapy and cancer in type 2 diabetes. ISRN Endocrinol
2012:240634, 2012
58. Sturmer,T, Buring,JE, Lee,IM, Gaziano,JM, Glynn,RJ: Metabolic abnormalities and
risk for colorectal cancer in the physicians' health study. Cancer Epidemiol
Biomarkers Prev 15:2391-2397, 2006

56
59. Gunter,MJ, Hoover,DR, Yu,H, Wassertheil-Smoller,S, Rohan,TE, Manson,JE,
Howard,BV, Wylie-Rosett,J, Anderson,GL, Ho,GY, Kaplan,RC, Li,J, Xue,X,
Harris,TG, Burk,RD, Strickler,HD: Insulin, insulin-like growth factor-I, endogenous
estradiol, and risk of colorectal cancer in postmenopausal women. Cancer Res 68:329-
337, 2008
60. Ma,J, Giovannucci,E, Pollak,M, Leavitt,A, Tao,Y, Gaziano,JM, Stampfer,MJ: A
prospective study of plasma C-peptide and colorectal cancer risk in men. J Natl
Cancer Inst 96:546-553, 2004
61. Jenab,M, Riboli,E, Cleveland,RJ, Norat,T, Rinaldi,S, Nieters,A, Biessy,C,
Tjonneland,A, Olsen,A, Overvad,K, Gronbaek,H, Clavel-Chapelon,F, Boutron-
Ruault,MC, Linseisen,J, Boeing,H, Pischon,T, Trichopoulos,D, Oikonomou,E,
Trichopoulou,A, Panico,S, Vineis,P, Berrino,F, Tumino,R, Masala,G, Peters,PH, van
Gils,CH, Bueno-de-Mesquita,HB, Ocke,MC, Lund,E, Mendez,MA, Tormo,MJ,
Barricarte,A, Martinez-Garcia,C, Dorronsoro,M, Quiros,JR, Hallmans,G, Palmqvist,R,
Berglund,G, Manjer,J, Key,T, Allen,NE, Bingham,S, Khaw,KT, Cust,A, Kaaks,R:
Serum C-peptide, IGFBP-1 and IGFBP-2 and risk of colon and rectal cancers in the
European Prospective Investigation into Cancer and Nutrition. Int J Cancer 121:368-
376, 2007
62. Pisani,P: Hyper-insulinaemia and cancer, meta-analyses of epidemiological studies.
Arch Physiol Biochem 114:63-70, 2008

57
63. Irwin,ML, Duggan,C, Wang,CY, Smith,AW, McTiernan,A, Baumgartner,RN,
Baumgartner,KB, Bernstein,L, Ballard-Barbash,R: Fasting C-peptide levels and death
resulting from all causes and breast cancer: the health, eating, activity, and lifestyle
study. J Clin Oncol 29:47-53, 2011
64. Gunter,MJ, Hoover,DR, Yu,H, Wassertheil-Smoller,S, Rohan,TE, Manson,JE, Li,J,
Ho,GY, Xue,X, Anderson,GL, Kaplan,RC, Harris,TG, Howard,BV, Wylie-Rosett,J,
Burk,RD, Strickler,HD: Insulin, insulin-like growth factor-I, and risk of breast cancer
in postmenopausal women. J Natl Cancer Inst 101:48-60, 2009
65. Kabat,GC, Kim,M, Caan,BJ, Chlebowski,RT, Gunter,MJ, Ho,GY, Rodriguez,BL,
Shikany,JM, Strickler,HD, Vitolins,MZ, Rohan,TE: Repeated measures of serum
glucose and insulin in relation to postmenopausal breast cancer. Int J Cancer
125:2704-2710, 2009
66. Chen,L, Li,L, Wang,Y, Li,P, Luo,L, Yang,B, Wang,H, Chen,M: Circulating C-peptide
level is a predictive factor for colorectal neoplasia: evidence from the meta-analysis of
prospective studies. Cancer Causes Control 2013
67. Baur,DM, Klotsche,J, Hamnvik,OP, Sievers,C, Pieper,L, Wittchen,HU, Stalla,GK,
Schmid,RM, Kales,SN, Mantzoros,CS: Type 2 diabetes mellitus and medications for
type 2 diabetes mellitus are associated with risk for and mortality from cancer in a
German primary care cohort. Metabolism 60:1363-1371, 2011

58
68. Bowker,SL, Majumdar,SR, Veugelers,P, Johnson,JA: Increased cancer-related
mortality for patients with type 2 diabetes who use sulfonylureas or insulin. Diabetes
Care 29:254-258, 2006
69. Currie,CJ, Poole,CD, Gale,EA: The influence of glucose-lowering therapies on cancer
risk in type 2 diabetes. Diabetologia 52:1766-1777, 2009
70. Hemkens,LG, Grouven,U, Bender,R, Gunster,C, Gutschmidt,S, Selke,GW,
Sawicki,PT: Risk of malignancies in patients with diabetes treated with human insulin
or insulin analogues: a cohort study. Diabetologia 52:1732-1744, 2009
71. van Staa,TP, Patel,D, Gallagher,AM, de Bruin,ML: Glucose-lowering agents and the
patterns of risk for cancer: a study with the General Practice Research Database and
secondary care data. Diabetologia 55:654-665, 2012
72. Bowker,SL, Yasui,Y, Veugelers,P, Johnson,JA: Glucose-lowering agents and cancer
mortality rates in type 2 diabetes: assessing effects of time-varying exposure.
Diabetologia 53:1631-1637, 2010
73. Carstensen,B, Witte,DR, Friis,S: Cancer occurrence in Danish diabetic patients:
duration and insulin effects. Diabetologia 55:948-958, 2012
74. Yang,X, Ko,GT, So,WY, Ma,RC, Yu,LW, Kong,AP, Zhao,H, Chow,CC, Tong,PC,
Chan,JC: Associations of hyperglycemia and insulin usage with the risk of cancer in
type 2 diabetes: the Hong Kong diabetes registry. Diabetes 59:1254-1260, 2010

59
75. Janghorbani,M, Dehghani,M, Salehi-Marzijarani,M: Systematic review and meta-
analysis of insulin therapy and risk of cancer. Horm Cancer 3:137-146, 2012
76. Baxter,RC, Bryson,JM, Turtle,JR: Somatogenic receptors of rat liver: regulation by
insulin. Endocrinology 107:1176-1181, 1980
77. Cordain,L, Eades,MR, Eades,MD: Hyperinsulinemic diseases of civilization: more
than just Syndrome X. Comp Biochem Physiol A Mol Integr Physiol 136:95-112, 2003
78. Kaaks,R, Lukanova,A: Energy balance and cancer: the role of insulin and insulin-like
growth factor-I. Proc Nutr Soc 60:91-106, 2001
79. Chen,W, Wang,S, Tian,T, Bai,J, Hu,Z, Xu,Y, Dong,J, Chen,F, Wang,X, Shen,H:
Phenotypes and genotypes of insulin-like growth factor 1, IGF-binding protein-3 and
cancer risk: evidence from 96 studies. Eur J Hum Genet 17:1668-1675, 2009
80. Major,JM, Laughlin,GA, Kritz-Silverstein,D, Wingard,DL, Barrett-Connor,E: Insulin-
like growth factor-I and cancer mortality in older men. J Clin Endocrinol Metab
95:1054-1059, 2010
81. Sekharam,M, Nasir,A, Kaiser,HE, Coppola,D: Insulin-like growth factor 1 receptor
activates c-SRC and modifies transformation and motility of colon cancer in vitro.
Anticancer Res 23:1517-1524, 2003

60
82. Litzenburger,BC, Kim,HJ, Kuiatse,I, Carboni,JM, Attar,RM, Gottardis,MM,
Fairchild,CR, Lee,AV: BMS-536924 reverses IGF-IR-induced transformation of
mammary epithelial cells and causes growth inhibition and polarization of MCF7
cells. Clin Cancer Res 15:226-237, 2009
83. Fox,EM, Miller,TW, Balko,JM, Kuba,MG, Sanchez,V, Smith,RA, Liu,S, Gonzalez-
Angulo,AM, Mills,GB, Ye,F, Shyr,Y, Manning,HC, Buck,E, Arteaga,CL: A kinome-
wide screen identifies the insulin/IGF-I receptor pathway as a mechanism of escape
from hormone dependence in breast cancer. Cancer Res 71:6773-6784, 2011
84. Masur,K, Vetter,C, Hinz,A, Tomas,N, Henrich,H, Niggemann,B, Zanker,KS:
Diabetogenic glucose and insulin concentrations modulate transcriptome and protein
levels involved in tumour cell migration, adhesion and proliferation. Br J Cancer
104:345-352, 2011
85. Frittitta,L, Vigneri,R, Papa,V, Goldfine,ID, Grasso,G, Trischitta,V: Structural and
functional studies of insulin receptors in human breast cancer. Breast Cancer Res
Treat 25:73-82, 1993
86. Milazzo,G, Giorgino,F, Damante,G, Sung,C, Stampfer,MR, Vigneri,R, Goldfine,ID,
Belfiore,A: Insulin receptor expression and function in human breast cancer cell lines.
Cancer Res 52:3924-3930, 1992
87. Gliozzo,B, Sung,CK, Scalia,P, Papa,V, Frasca,F, Sciacca,L, Giorgino,F, Milazzo,G,
Goldfine,ID, Vigneri,R, Pezzino,V: Insulin-stimulated cell growth in insulin receptor

61
substrate-1-deficient ZR-75-1 cells is mediated by a phosphatidylinositol-3-kinase-
independent pathway. J Cell Biochem 70:268-280, 1998
88. Zhang,Y, Moerkens,M, Ramaiahgari,S, de,BH, Price,L, Meerman,J, van de,WB:
Elevated insulin-like growth factor 1 receptor signaling induces antiestrogen resistance
through the MAPK/ERK and PI3K/Akt signaling routes. Breast Cancer Res 13:R52,
2011
89. Weinstein,D, Simon,M, Yehezkel,E, Laron,Z, Werner,H: Insulin analogues display
IGF-I-like mitogenic and anti-apoptotic activities in cultured cancer cells. Diabetes
Metab Res Rev 25:41-49, 2009
90. Ebi,H, Corcoran,RB, Singh,A, Chen,Z, Song,Y, Lifshits,E, Ryan,DP, Meyerhardt,JA,
Benes,C, Settleman,J, Wong,KK, Cantley,LC, Engelman,JA: Receptor tyrosine
kinases exert dominant control over PI3K signaling in human KRAS mutant colorectal
cancers. J Clin Invest 121:4311-4321, 2011
91. Jin,Q, Esteva,FJ: Cross-talk between the ErbB/HER family and the type I insulin-like
growth factor receptor signaling pathway in breast cancer. J Mammary Gland Biol
Neoplasia 13:485-498, 2008
92. Gooch,JL, Van Den Berg,CL, Yee,D: Insulin-like growth factor (IGF)-I rescues breast
cancer cells from chemotherapy-induced cell death--proliferative and anti-apoptotic
effects. Breast Cancer Res Treat 56:1-10, 1999

62
93. Rubini,M, Hongo,A, D'Ambrosio,C, Baserga,R: The IGF-I receptor in mitogenesis
and transformation of mouse embryo cells: role of receptor number. Exp Cell Res
230:284-292, 1997
94. Giorgino,F, Belfiore,A, Milazzo,G, Costantino,A, Maddux,B, Whittaker,J,
Goldfine,ID, Vigneri,R: Overexpression of insulin receptors in fibroblast and ovary
cells induces a ligand-mediated transformed phenotype. Mol Endocrinol 5:452-459,
1991
95. Tran,TT, Medline,A, Bruce,WR: Insulin promotion of colon tumors in rats. Cancer
Epidemiol Biomarkers Prev 5:1013-1015, 1996
96. Corpet,DE, Jacquinet,C, Peiffer,G, Tache,S: Insulin injections promote the growth of
aberrant crypt foci in the colon of rats. Nutr Cancer 27:316-320, 1997
97. Heuson,JC, Legros,N: Influence of insulin deprivation on growth of the 7,12-
dimethylbenz(a)anthracene-induced mammary carcinoma in rats subjected to alloxan
diabetes and food restriction. Cancer Res 32:226-232, 1972
98. Cohen,ND, Hilf,R: Influence of insulin on growth and metabolism of 7,12-
dimethylbenz(alpha)anthracene-induced mammary tumors. Cancer Res 34:3245-3252,
1974

63
99. Shafie,SM, Grantham,FH: Role of hormones in the growth and regression of human
breast cancer cells (MCF-7) transplanted into athymic nude mice. J Natl Cancer Inst
67:51-56, 1981
100. Lu,S, Lee,WM, Archer,MC: Insulin does not promote rat mammary carcinogenesis.
Carcinogenesis 19:699-702, 1998
101. Novosyadlyy,R, Lann,DE, Vijayakumar,A, Rowzee,A, Lazzarino,DA, Fierz,Y,
Carboni,JM, Gottardis,MM, Pennisi,PA, Molinolo,AA, Kurshan,N, Mejia,W,
Santopietro,S, Yakar,S, Wood,TL, LeRoith,D: Insulin-mediated acceleration of breast
cancer development and progression in a nonobese model of type 2 diabetes. Cancer
Res 70:741-751, 2010
102. Wu,Y, Yakar,S, Zhao,L, Hennighausen,L, LeRoith,D: Circulating insulin-like growth
factor-I levels regulate colon cancer growth and metastasis. Cancer Res 62:1030-1035,
2002
103. Wu,Y, Cui,K, Miyoshi,K, Hennighausen,L, Green,JE, Setser,J, LeRoith,D, Yakar,S:
Reduced circulating insulin-like growth factor I levels delay the onset of chemically
and genetically induced mammary tumors. Cancer Res 63:4384-4388, 2003
104. Ealey,KN, Xuan,W, Lu,S, Archer,MC: Colon carcinogenesis in liver-specific IGF-I-
deficient (LID) mice. Int J Cancer 122:472-476, 2008

64
105. Dideriksen,LH, Jorgensen,LN, Dreijer,K: Carcinogenic effect on female rats after 12
months administration of insulin analogue B10 asp. Diabetes 41: 1992
106. Colhoun,HM: Use of insulin glargine and cancer incidence in Scotland: a study from
the Scottish Diabetes Research Network Epidemiology Group. Diabetologia 52:1755-
1765, 2009
107. Jonasson,JM, Ljung,R, Talback,M, Haglund,B, Gudbjornsdottir,S, Steineck,G: Insulin
glargine use and short-term incidence of malignancies-a population-based follow-up
study in Sweden. Diabetologia 52:1745-1754, 2009
108. Ljung,R, Talback,M, Haglund,B, Jonasson,JM, Gudbjornsdottir,S, Steineck,G: Insulin
glargine use and short-term incidence of malignancies - a three-year population-based
observation. Acta Oncol 50:685-693, 2011
109. Ruiter,R, Visser,LE, van Herk-Sukel,MP, Coebergh,JW, Haak,HR, Geelhoed-
Duijvestijn,PH, Straus,SM, Herings,RM, Stricker,BH: Risk of cancer in patients on
insulin glargine and other insulin analogues in comparison with those on human
insulin: results from a large population-based follow-up study. Diabetologia 55:51-62,
2012
110. Suissa,S, Azoulay,L, Dell'Aniello,S, Evans,M, Vora,J, Pollak,M: Long-term effects of
insulin glargine on the risk of breast cancer. Diabetologia 54:2254-2262, 2011

65
111. Lind,M, Fahlen,M, Eliasson,B, Oden,A: The relationship between the exposure time
of insulin glargine and risk of breast and prostate cancer: an observational study of the
time-dependent effects of antidiabetic treatments in patients with diabetes. Prim Care
Diabetes 6:53-59, 2012
112. Morden,NE, Liu,SK, Smith,J, Mackenzie,TA, Skinner,J, Korc,M: Further exploration
of the relationship between insulin glargine and incident cancer: a retrospective cohort
study of older Medicare patients. Diabetes Care 34:1965-1971, 2011
113. Chang,CH, Toh,S, Lin,JW, Chen,ST, Kuo,CW, Chuang,LM, Lai,MS: Cancer risk
associated with insulin glargine among adult type 2 diabetes patients--a nationwide
cohort study. PLoS One 6:e21368, 2011
114. Fagot,JP, Blotiere,PO, Ricordeau,P, Weill,A, Alla,F, Allemand,H: Does insulin
glargine increase the risk of cancer compared with other basal insulins?: A French
nationwide cohort study based on national administrative databases. Diabetes Care
36:294-301, 2013
115. Grimaldi-Bensouda,L, Cameron,D, Marty,M, Barnett,AH, Penault-Llorca,F, Pollak,M,
Charbonnel,B, Riddle,M, Mignot,L, Boivin,JF, Khachatryan,A, Rossignol,M,
Benichou,J, Alperovitch,A, Abenhaim,L: Risk of breast cancer by individual insulin
use - an international multicenter study. Diabetes Care 2013
116. Sturmer,T, Marquis,MA, Zhou,H, Meigs,JB, Lim,S, Blonde,L, Macdonald,E, Wang,R,
Lavange,LM, Pate,V, Buse,JB: Cancer Incidence Among Those Initiating Insulin

66
Therapy With Glargine Versus Human NPH Insulin. Diabetes Care 36:3517-3525,
2013
117. Mannucci,E, Monami,M, Balzi,D, Cresci,B, Pala,L, Melani,C, Lamanna,C, Bracali,I,
Bigiarini,M, Barchielli,A, Marchionni,N, Rotella,CM: Doses of insulin and its
analogues and cancer occurrence in insulin-treated type 2 diabetic patients. Diabetes
Care 33:1997-2003, 2010
118. Blin,P, Lassalle,R, Dureau-Pournin,C, Ambrosino,B, Bernard,MA, Abouelfath,A,
Gin,H, Le,JC, Pariente,A, Droz,C, Moore,N: Insulin glargine and risk of cancer: a
cohort study in the French National Healthcare Insurance Database. Diabetologia
55:644-653, 2012
119. Gerstein,HC, Bosch,J, Dagenais,GR, Diaz,R, Jung,H, Maggioni,AP, Pogue,J,
Probstfield,J, Ramachandran,A, Riddle,MC, Ryden,LE, Yusuf,S: Basal insulin and
cardiovascular and other outcomes in dysglycemia. N Engl J Med 367:319-328, 2012
120. Rosenstock,J, Fonseca,V, McGill,JB, Riddle,M, Halle,JP, Hramiak,I, Johnston,P,
Davis,M: Similar progression of diabetic retinopathy with insulin glargine and neutral
protamine Hagedorn (NPH) insulin in patients with type 2 diabetes: a long-term,
randomised, open-label study. Diabetologia 52:1778-1788, 2009
121. Shukla,A, Grisouard,J, Ehemann,V, Hermani,A, Enzmann,H, Mayer,D: Analysis of
signaling pathways related to cell proliferation stimulated by insulin analogs in human
mammary epithelial cell lines. Endocr Relat Cancer 16:429-441, 2009

67
122. Kurtzhals,P, Schaffer,L, Sorensen,A, Kristensen,C, Jonassen,I, Schmid,C, Trub,T:
Correlations of receptor binding and metabolic and mitogenic potencies of insulin
analogs designed for clinical use. Diabetes 49:999-1005, 2000
123. Mayer,D, Shukla,A, Enzmann,H: Proliferative effects of insulin analogues on
mammary epithelial cells. Arch Physiol Biochem 114:38-44, 2008
124. Varewijck,AJ, Goudzwaard,JA, Brugts,MP, Lamberts,SW, Hofland,LJ, Janssen,JA:
Insulin glargine is more potent in activating the human IGF-I receptor than human
insulin and insulin detemir. Growth Horm IGF Res 20:427-431, 2010
125. Mussig,K, Staiger,H, Kantartzis,K, Fritsche,A, Kanz,L, Haring,HU: Type 2 diabetes
mellitus and risk of malignancy: is there a strategy to identify a subphenotype of
patients with increased susceptibility to endogenous and exogenous hyperinsulinism?
Diabet Med 28:276-286, 2011
126. Hansen,BF, Danielsen,GM, Drejer,K, Sorensen,AR, Wiberg,FC, Klein,HH,
Lundemose,AG: Sustained signalling from the insulin receptor after stimulation with
insulin analogues exhibiting increased mitogenic potency. Biochem J 315 ( Pt 1):271-
279, 1996
127. Sciacca,L, Cassarino,MF, Genua,M, Pandini,G, Le,MR, Squatrito,S, Vigneri,R:
Insulin analogues differently activate insulin receptor isoforms and post-receptor
signalling. Diabetologia 53:1743-1753, 2010

68
128. Teng,JA, Hou,RL, Li,DL, Yang,RP, Qin,J: Glargine promotes proliferation of breast
adenocarcinoma cell line MCF-7 via AKT activation. Horm Metab Res 43:519-523,
2011
129. Stammberger,I, Bube,A, Durchfeld-Meyer,B, Donaubauer,H, Troschau,G: Evaluation
of the carcinogenic potential of insulin glargine (LANTUS) in rats and mice. Int J
Toxicol 21:171-179, 2002
130. Nagel,JM, Staffa,J, Renner-Muller,I, Horst,D, Vogeser,M, Langkamp,M, Hoeflich,A,
Goke,B, Kolligs,FT, Mantzoros,CS: Insulin glargine and NPH insulin increase to a
similar degree epithelial cell proliferation and aberrant crypt foci formation in colons
of diabetic mice. Horm Cancer 1:320-330, 2010
131. Kuerzel,GU, Shukla,U, Scholtz,HE, Pretorius,SG, Wessels,DH, Venter,C,
Potgieter,MA, Lang,AM, Koose,T, Bernhardt,E: Biotransformation of insulin glargine
after subcutaneous injection in healthy subjects. Curr Med Res Opin 19:34-40, 2003
132. Agin,A, Jeandidier,N, Gasser,F, Grucker,D, Sapin,R: Glargine blood
biotransformation: in vitro appraisal with human insulin immunoassay. Diabetes
Metab 33:205-212, 2007
133. Mayer,D, Chantelau,E: Treatment with insulin glargine (Lantus) increases the
proliferative potency of the serum of patients with type-1 diabetes: a pilot study on
MCF-7 breast cancer cells. Arch Physiol Biochem 116:73-78, 2010

69
134. Gallagher EJ, Tobin-Hess A, Blank J, Buffin N, Polin A, Tennagels N, Werner U,
LeRoith D: Insulin glargine does not increase bresat cancer growth in an animal model
(Abstract). American Diabetes Association, 2013
135. Weston A, Harris CC: Chemical Carcinogenesis. In Halland-Frei Cancer Medicine
5th edition. Bast RC, Kufe DW, Pollock RE, Weichselbaum RR, Eds. Hamilton(ON),
BC Decker, 2000,
136. Perse,M, Cerar,A, Injac,R, Strukelj,B: N-methylnitrosourea induced breast cancer in
rat, the histopathology of the resulting tumours and its drawbacks as a model. Pathol
Oncol Res 15:115-121, 2009
137. King,MM, McCay,PB, Kosanke,SD: Comparison of the effect of butylated
hydroxytoluene on N-nitrosomethylurea and 7,12-dimethylbenz[a]-anthracene-
induced mammary tumors. Cancer Lett 14:219-226, 1981
138. Zarbl,H, Sukumar,S, Arthur,AV, Martin-Zanca,D, Barbacid,M: Direct mutagenesis of
Ha-ras-1 oncogenes by N-nitroso-N-methylurea during initiation of mammary
carcinogenesis in rats. Nature 315:382-385, 1985
139. Russo,J, Russo,IH: Atlas and histologic classification of tumors of the rat mammary
gland. J Mammary Gland Biol Neoplasia 5:187-200, 2000
140. Pylayeva-Gupta,Y, Grabocka,E, Bar-Sagi,D: RAS oncogenes: weaving a tumorigenic
web. Nat Rev Cancer 11:761-774, 2011

70
141. Thompson,HJ, Meeker,LD: Induction of mammary gland carcinomas by the
subcutaneous injection of 1-methyl-1-nitrosourea. Cancer Res 43:1628-1629, 1983
142. Weisburger,JH: Colon carcinogens: their metabolism and mode of action. Cancer
28:60-70, 1971
143. Gonzalez,FJ: The 2006 Bernard B. Brodie Award Lecture. Cyp2e1. Drug Metab
Dispos 35:1-8, 2007
144. Shivapurkar,N, Tang,Z, Ferreira,A, Nasim,S, Garett,C, Alabaster,O: Sequential
analysis of K-ras mutations in aberrant crypt foci and colonic tumors induced by
azoxymethane in Fischer-344 rats on high-risk diet. Carcinogenesis 15:775-778, 1994
145. Corpet,DE, Pierre,F: Point: From animal models to prevention of colon cancer.
Systematic review of chemoprevention in min mice and choice of the model system.
Cancer Epidemiol Biomarkers Prev 12:391-400, 2003
146. Pereira,MA, Barnes,LH, Rassman,VL, Kelloff,GV, Steele,VE: Use of azoxymethane-
induced foci of aberrant crypts in rat colon to identify potential cancer
chemopreventive agents. Carcinogenesis 15:1049-1054, 1994
147. Kumar,SP, Roy,SJ, Tokumo,K, Reddy,BS: Effect of different levels of calorie
restriction on azoxymethane-induced colon carcinogenesis in male F344 rats. Cancer
Res 50:5761-5766, 1990

71
148. Pretlow,TP, O'Riordan,MA, Somich,GA, Amini,SB, Pretlow,TG: Aberrant crypts
correlate with tumor incidence in F344 rats treated with azoxymethane and phytate.
Carcinogenesis 13:1509-1512, 1992
149. Pretlow,TP, Barrow,BJ, Ashton,WS, O'Riordan,MA, Pretlow,TG, Jurcisek,JA,
Stellato,TA: Aberrant crypts: putative preneoplastic foci in human colonic mucosa.
Cancer Res 51:1564-1567, 1991
150. McLellan,EA, Bird,RP: Aberrant crypts: potential preneoplastic lesions in the murine
colon. Cancer Res 48:6187-6192, 1988
151. McLellan,EA, Bird,RP: Specificity study to evaluate induction of aberrant crypts in
murine colons. Cancer Res 48:6183-6186, 1988
152. Bird,RP: Role of aberrant crypt foci in understanding the pathogenesis of colon
cancer. Cancer Lett 93:55-71, 1995
153. Caderni,G, Femia,AP, Giannini,A, Favuzza,A, Luceri,C, Salvadori,M, Dolara,P:
Identification of mucin-depleted foci in the unsectioned colon of azoxymethane-
treated rats: correlation with carcinogenesis. Cancer Res 63:2388-2392, 2003
154. Femia,AP, Giannini,A, Fazi,M, Tarquini,E, Salvadori,M, Roncucci,L, Tonelli,F,
Dolara,P, Caderni,G: Identification of mucin depleted foci in the human colon. Cancer
Prev Res (Phila) 1:562-567, 2008

72
155. Sakai,E, Morioka,T, Yamada,E, Ohkubo,H, Higurashi,T, Hosono,K, Endo,H,
Takahashi,H, Takamatsu,R, Cui,C, Shiozawa,M, Akaike,M, Samura,H, Nishimaki,T,
Nakajima,A, Yoshimi,N: Identification of preneoplastic lesions as mucin-depleted foci
in patients with sporadic colorectal cancer. Cancer Sci 103:144-149, 2012
156. Shivapurkar,N, Tang,ZC, Frost,A, Alabaster,O: A rapid dual organ rat carcinogenesis
bioassay for evaluating the chemoprevention of breast and colon cancer. Cancer Lett
100:169-179, 1996
157. Dobbins,RL, Szczepaniak,LS, Myhill,J, Tamura,Y, Uchino,H, Giacca,A, McGarry,JD:
The composition of dietary fat directly influences glucose-stimulated insulin secretion
in rats. Diabetes 51:1825-1833, 2002
158. Florey,CD: Sample size for beginners. BMJ 306:1181-1184, 1993
159. Dricu,A, Kanter,L, Wang,M, Nilsson,G, Hjertman,M, Wejde,J, Larsson,O: Expression
of the insulin-like growth factor 1 receptor (IGF-1R) in breast cancer cells: evidence
for a regulatory role of dolichyl phosphate in the transition from an intracellular to an
extracellular IGF-1 pathway. Glycobiology 9:571-579, 1999
160. Goodwin,PJ, Ennis,M, Pritchard,KI, Trudeau,ME, Koo,J, Madarnas,Y, Hartwick,W,
Hoffman,B, Hood,N: Fasting insulin and outcome in early-stage breast cancer: results
of a prospective cohort study. J Clin Oncol 20:42-51, 2002

73
161. Dejgaard,A, Lynggaard,H, Rastam,J, Krogsgaard,TM: No evidence of increased risk
of malignancies in patients with diabetes treated with insulin detemir: a meta-analysis.
Diabetologia 52:2507-2512, 2009
162. Zhang,H, Fagan,DH, Zeng,X, Freeman,KT, Sachdev,D, Yee,D: Inhibition of cancer
cell proliferation and metastasis by insulin receptor downregulation. Oncogene
29:2517-2527, 2010
163. Ochiai,M, Watanabe,M, Kushida,H, Wakabayashi,K, Sugimura,T, Nagao,M: DNA
adduct formation, cell proliferation and aberrant crypt focus formation induced by
PhIP in male and female rat colon with relevance to carcinogenesis. Carcinogenesis
17:95-98, 1996
164. Odagiri,E, Jibiki,K, Kato,Y, Nakamura,S, Oda,S, Demura,R, Demura,H: Steroid
receptors in dimethylhydrazine-induced colon carcinogenesis. Cancer 56:2627-2634,
1985
165. Gershbein,LL: Action of estrogen and adrenocorticoids on adenocarcinoma induction
by 1,2-dimethylhydrazine in male rats. Res Commun Chem Pathol Pharmacol 81:117-
120, 1993
166. Narisawa,T, Magadia,NE, Weisburger,JH, Wynder,EL: Promoting effect of bile acids
on colon carcinogenesis after intrarectal instillation of N-methyl-N'-nitro-N-
nitrosoguanidine in rats. J Natl Cancer Inst 53:1093-1097, 1974

74
167. McMichael,AJ, Potter,JD: Host factors in carcinogenesis: certain bile-acid metabolic
profiles that selectively increase the risk of proximal colon cancer. J Natl Cancer Inst
75:185-191, 1985
168. McMichael,AJ, Potter,JD: Reproduction, endogenous and exogenous sex hormones,
and colon cancer: a review and hypothesis. J Natl Cancer Inst 65:1201-1207, 1980
169. Lee,WM, Lu,S, Medline,A, Archer,MC: Susceptibility of lean and obese Zucker rats
to tumorigenesis induced by N-methyl-N-nitrosourea. Cancer Lett 162:155-160, 2001

75
Appendix A
Figure 1: Mammary Tumour burden among tumour-bearing rats was compared between control
(n=18), NPH (n=24), glargine (n=17), and detemir (n=19) treated groups.* p<0.05
Figure 2: Tumour incidence overtime was compared between the control group (n=12) and a
combined group of insulins (n=29). *p <0.05

76
Figure 3: Mammary Tumour multiplicity among tumour-bearing rats was compared between
the control group (n=30) and a combined group of insulins (n=90) .* p<0.05
Figure 4: Mammary Tumour burden among tumour-bearing rats was compared between the
control group (n=30) and a combined group of insulin (n=90). *p<0.01