Embed Size (px)
Citation preview
Insulin Analogues versus Pump Insulin Analogues versus Pump
Therapy in Type 2 Diabetes:Therapy in Type 2 Diabetes:
Benefits from Pump TherapyBenefits from Pump Therapy
Eric RENARD, MD, PhDEric RENARD, MD, PhD
Endocrinology Dept, Endocrinology Dept, LapeyronieLapeyronie HospitalHospital
Montpellier, FranceMontpellier, France
ee--renard@[email protected]
Type 2 Diabetes Burnout : What is the Type 2 Diabetes Burnout : What is the
Remedy and for Whom ? Remedy and for Whom ?
Needles ?Needles ?Or Pump ?Or Pump ?
What is the Current Experience of Glucose What is the Current Experience of Glucose
Control with Insulin Injections in Type 2 Control with Insulin Injections in Type 2
Diabetes ?Diabetes ?
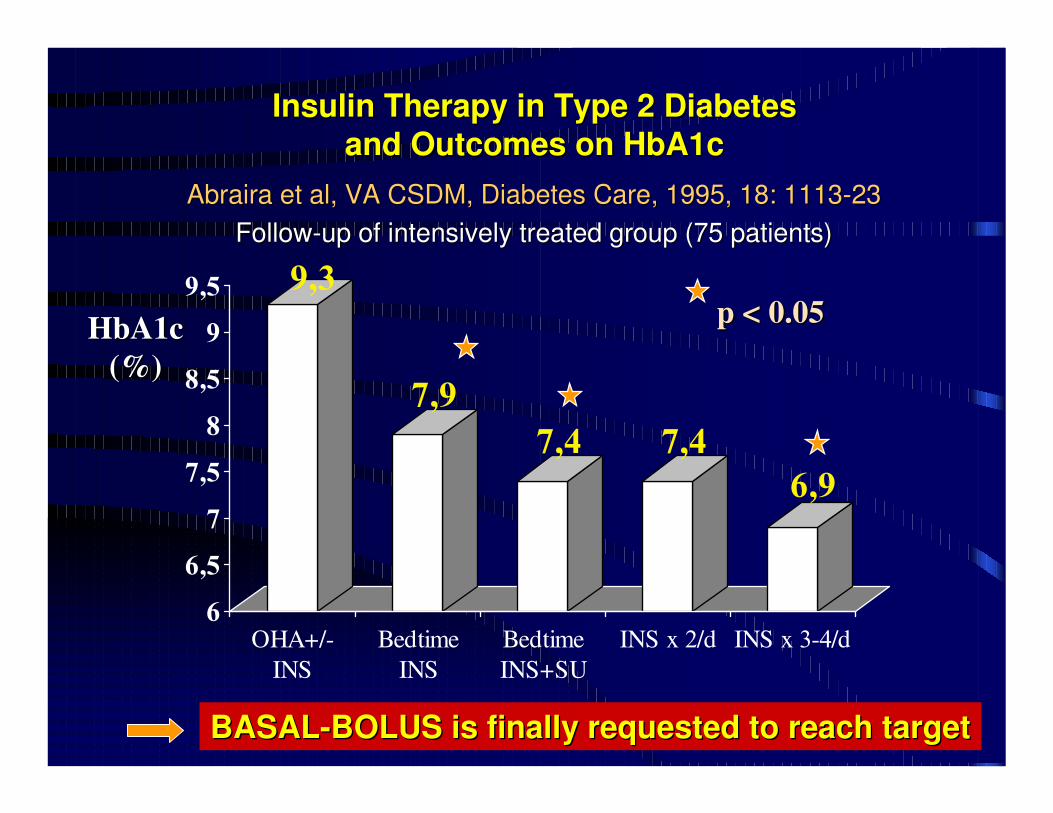
Insulin Therapy in Type 2 Diabetes Insulin Therapy in Type 2 Diabetes
and Outcomes on HbA1cand Outcomes on HbA1c
9,3
7,9
7,4 7,4
6,9
6
6,5
7
7,5
8
8,5
9
9,5
OHA+/-
INS
Bedtime
INS
Bedtime
INS+SU
INS x 2/d INS x 3-4/d
AbrairaAbraira et al, VA CSDM, Diabetes Care, 1995, 18: 1113et al, VA CSDM, Diabetes Care, 1995, 18: 1113--2323
FollowFollow--up of intensively treated group (75 patients)up of intensively treated group (75 patients)
p < 0.05p < 0.05HbA1c HbA1c
(%)(%)
BASALBASAL--BOLUS BOLUS isis finallyfinally requestedrequested to to reachreach targettarget
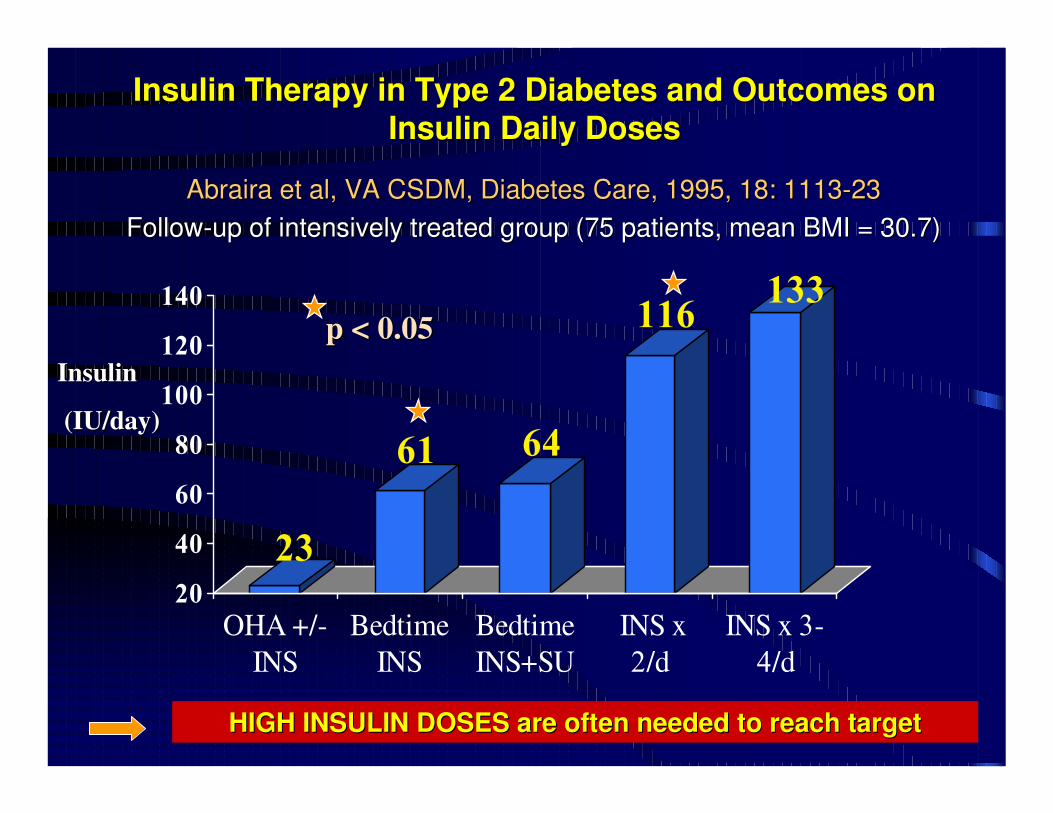
23
61 64
116133
20
40
60
80
100
120
140
OHA +/-
INS
Bedtime
INS
Bedtime
INS+SU
INS x
2/d
INS x 3-
4/d
p < 0.05p < 0.05
InsulinInsulin
(IU/day)(IU/day)
HIGH INSULIN DOSES are HIGH INSULIN DOSES are oftenoften neededneeded to to reachreach targettarget
Insulin Therapy in Type 2 Diabetes and Outcomes on Insulin Therapy in Type 2 Diabetes and Outcomes on
Insulin Daily DosesInsulin Daily Doses
AbrairaAbraira et al, VA CSDM, Diabetes Care, 1995, 18: 1113et al, VA CSDM, Diabetes Care, 1995, 18: 1113--2323
FollowFollow--up of intensively treated group (75 patients, mean BMI = 30.7)up of intensively treated group (75 patients, mean BMI = 30.7)
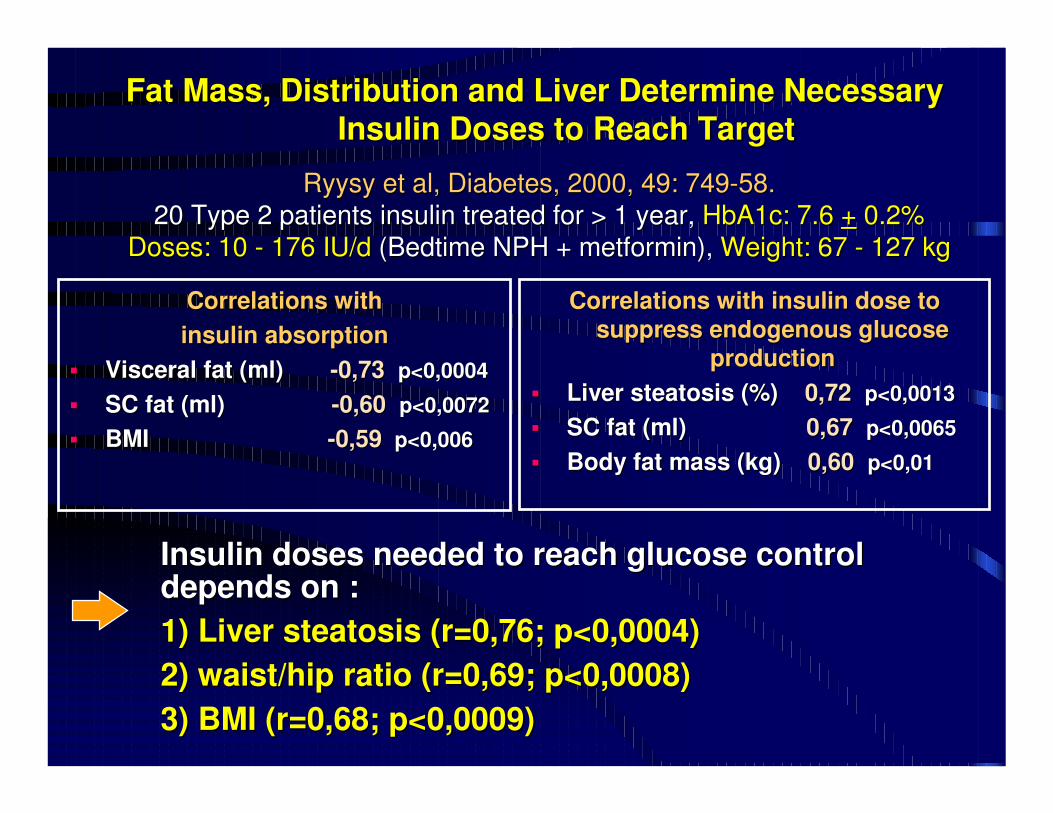
Fat Mass, Distribution and Liver Determine Necessary Fat Mass, Distribution and Liver Determine Necessary
Insulin Doses to Reach TargetInsulin Doses to Reach Target
Correlations with Correlations with
insulin absorption insulin absorption
�� Visceral fat (ml)Visceral fat (ml) --0,73 0,73 p<0,0004 p<0,0004
�� SC fat (ml) SC fat (ml) --0,60 0,60 p<0,0072p<0,0072
�� BMIBMI --0,59 0,59 p<0,006p<0,006
Correlations with insulin dose to Correlations with insulin dose to
suppress endogenous glucose suppress endogenous glucose
productionproduction
�� Liver Liver steatosissteatosis (%) (%) 0,72 0,72 p<0,0013p<0,0013
�� SC fat (ml) SC fat (ml) 0,67 0,67 p<0,0065p<0,0065
�� Body fat mass (kg) Body fat mass (kg) 0,60 0,60 p<0,01p<0,01
RyysyRyysy et al, Diabetes, 2000, 49: 749et al, Diabetes, 2000, 49: 749--58.58.
20 Type 2 patients insulin treated for > 1 year,20 Type 2 patients insulin treated for > 1 year, HbA1c: 7.6 HbA1c: 7.6 ++ 0.2%0.2%
Doses: 10 Doses: 10 -- 176 IU/d176 IU/d (Bedtime NPH + (Bedtime NPH + metforminmetformin), ), Weight: 67 Weight: 67 -- 127 kg127 kg
Insulin doses needed to reach glucose control Insulin doses needed to reach glucose control depends on : depends on :
1) Liver 1) Liver steatosissteatosis (r=0,76; p<0,0004)(r=0,76; p<0,0004)
2) waist/hip ratio (r=0,69; p<0,0008) 2) waist/hip ratio (r=0,69; p<0,0008)
3) BMI (r=0,68; p<0,0009)3) BMI (r=0,68; p<0,0009)
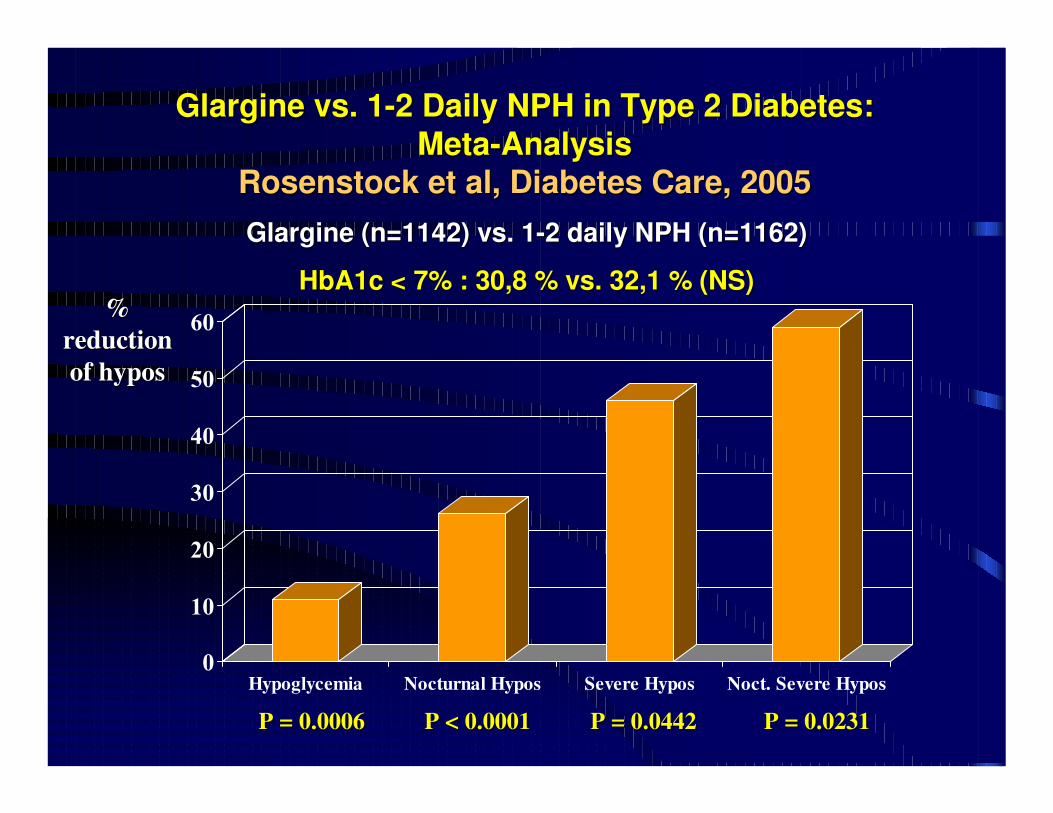
GlargineGlargine vs. 1vs. 1--2 Daily NPH in Type 2 Diabetes: 2 Daily NPH in Type 2 Diabetes:
MetaMeta--AnalysisAnalysis
RosenstockRosenstock et al, Diabetes Care, 2005et al, Diabetes Care, 2005
0
10
20
30
40
50
60
Hypoglycemia Nocturnal Hypos Severe Hypos Noct. Severe Hypos
GlargineGlargine (n=1142) vs. 1(n=1142) vs. 1--2 daily NPH (n=1162)2 daily NPH (n=1162)
HbA1c < 7% : 30,8 % vs. 32,1 % (NS)HbA1c < 7% : 30,8 % vs. 32,1 % (NS)% %
reduction reduction
of hyposof hypos
P = 0.0006P = 0.0006 P < 0.0001P < 0.0001 P = 0.0442P = 0.0442 P = 0.0231P = 0.0231
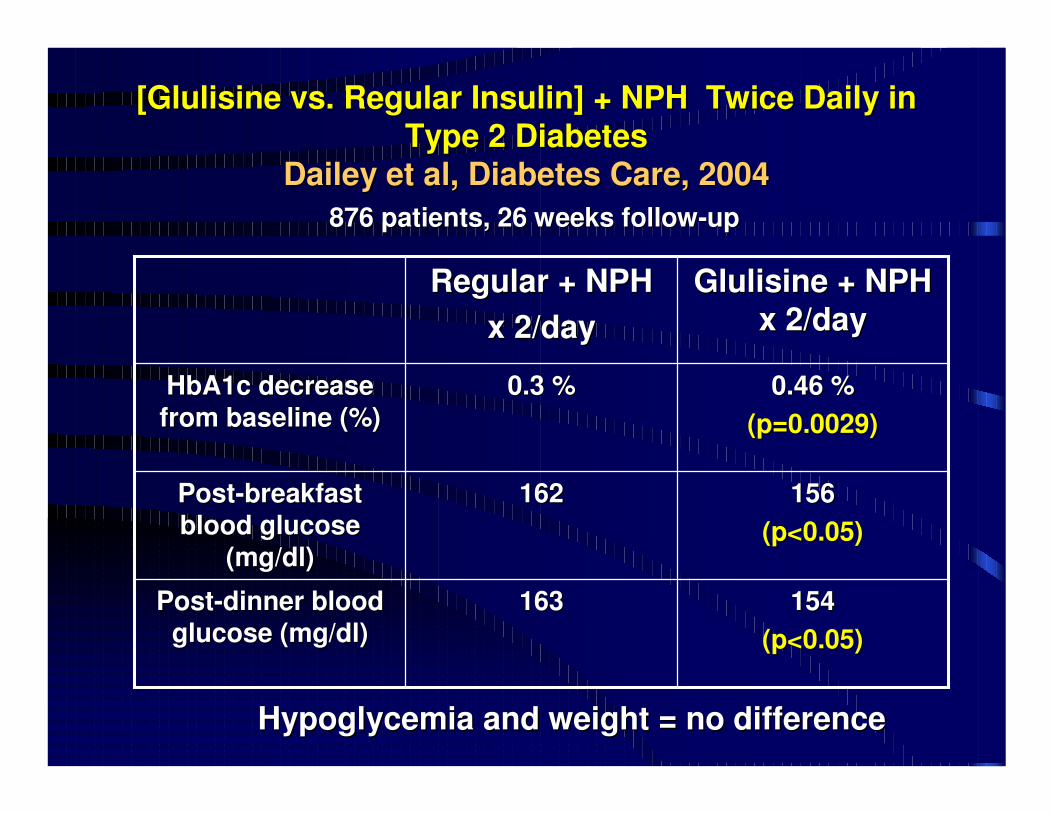
[[GlulisineGlulisine vs. Regular Insulin] + NPH Twice Daily in vs. Regular Insulin] + NPH Twice Daily in
Type 2 DiabetesType 2 Diabetes
Dailey et al, Diabetes Care, 2004Dailey et al, Diabetes Care, 2004
876 patients, 26 weeks follow876 patients, 26 weeks follow--upup
154154
(p<0.05)(p<0.05)
163163PostPost--dinner blood dinner blood
glucose (mg/dl)glucose (mg/dl)
156156
(p<0.05)(p<0.05)
162162PostPost--breakfast breakfast
blood glucose blood glucose
(mg/dl)(mg/dl)
0.46 %0.46 %
(p=0.0029)(p=0.0029)
0.3 %0.3 %HbA1c decrease HbA1c decrease
from baseline (%)from baseline (%)
GlulisineGlulisine + NPH + NPH
x 2/dayx 2/dayRegular + NPH Regular + NPH
x 2/dayx 2/day
Hypoglycemia and weight = no differenceHypoglycemia and weight = no difference
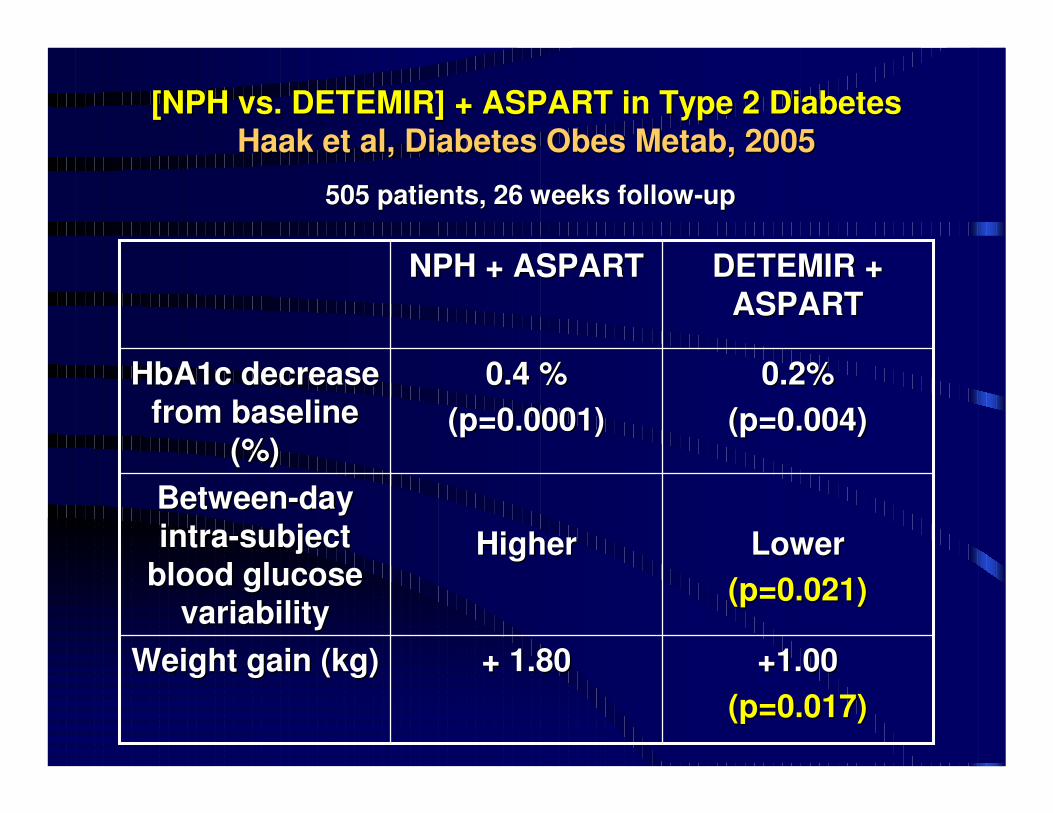
[NPH vs. DETEMIR] + ASPART in Type 2 Diabetes[NPH vs. DETEMIR] + ASPART in Type 2 Diabetes
HaakHaak et al, Diabetes et al, Diabetes ObesObes MetabMetab, 2005, 2005
505 patients, 26 weeks follow505 patients, 26 weeks follow--upup
+1.00+1.00
(p=0.017)(p=0.017)
+ 1.80+ 1.80Weight gain (kg)Weight gain (kg)
LowerLower
(p=0.021)(p=0.021)
HigherHigher
BetweenBetween--day day
intraintra--subject subject
blood glucose blood glucose
variabilityvariability
0.2%0.2%
(p=0.004)(p=0.004)
0.4 %0.4 %
(p=0.0001)(p=0.0001)
HbA1c decrease HbA1c decrease
from baseline from baseline
(%)(%)
DETEMIR + DETEMIR +
ASPARTASPARTNPH + ASPARTNPH + ASPART
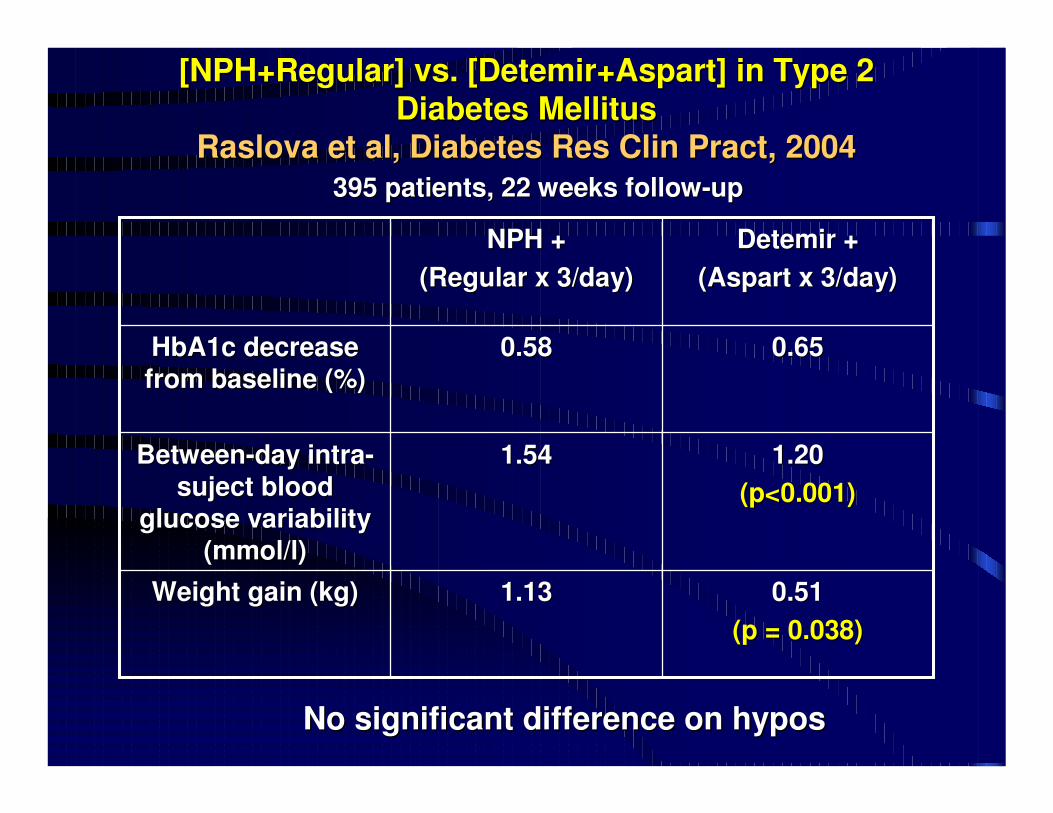
[[NPH+RegularNPH+Regular] vs. [] vs. [Detemir+AspartDetemir+Aspart] in Type 2 ] in Type 2
Diabetes MellitusDiabetes Mellitus
RaslovaRaslova et al, Diabetes et al, Diabetes ResRes ClinClin PractPract, 2004, 2004
395 patients, 22 weeks follow395 patients, 22 weeks follow--upup
0.510.51
(p = 0.038)(p = 0.038)
1.131.13Weight gain (kg)Weight gain (kg)
1.201.20
(p<0.001)(p<0.001)
1.541.54BetweenBetween--day intraday intra--
sujectsuject blood blood
glucose variability glucose variability
((mmol/lmmol/l))
0.650.650.580.58HbA1c decrease HbA1c decrease
from baseline (%)from baseline (%)
DetemirDetemir + +
((AspartAspart x 3/day)x 3/day)
NPH + NPH +
(Regular x 3/day)(Regular x 3/day)
No significant difference on hyposNo significant difference on hypos
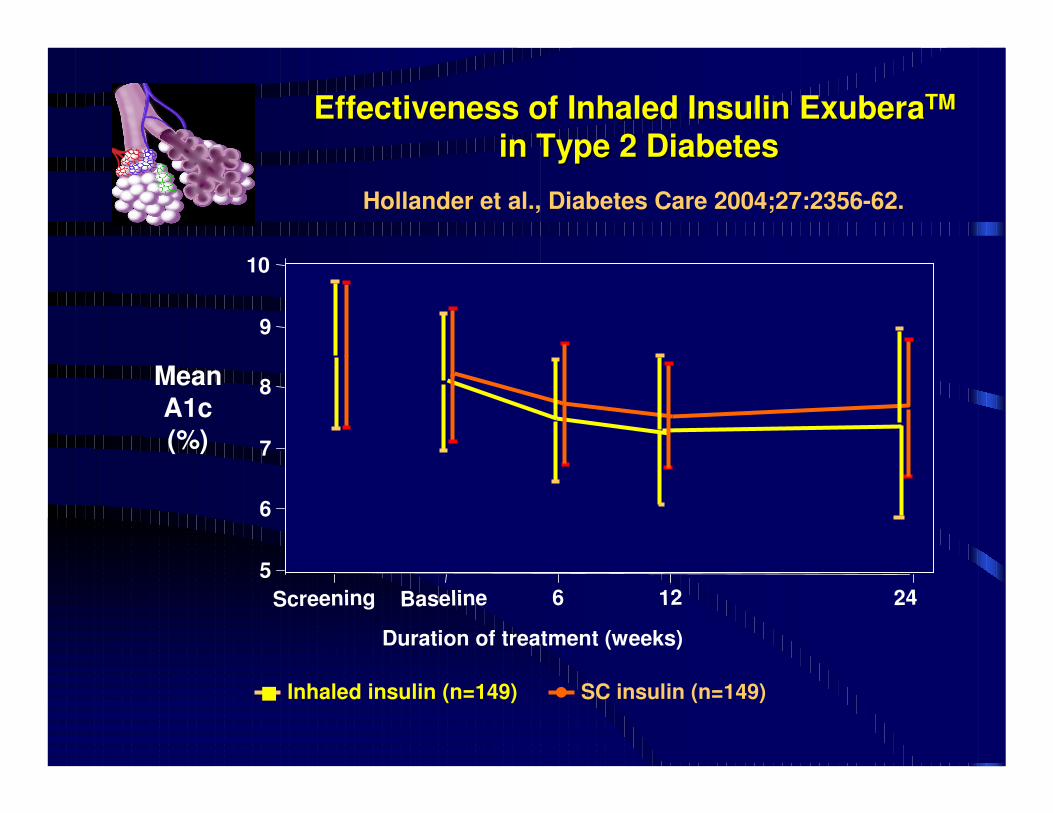
Screening Baseline 6 12 24
SC insulin (n=149)Inhaled insulin (n=149)
55
6
7
8
9
10
��
Duration of treatment (weeks)
MeanA1c(%)
Hollander et al., Diabetes Care 2004;27:2356-62.
Effectiveness of Inhaled Insulin Effectiveness of Inhaled Insulin ExuberaExuberaTMTM
in Type 2 Diabetesin Type 2 Diabetes
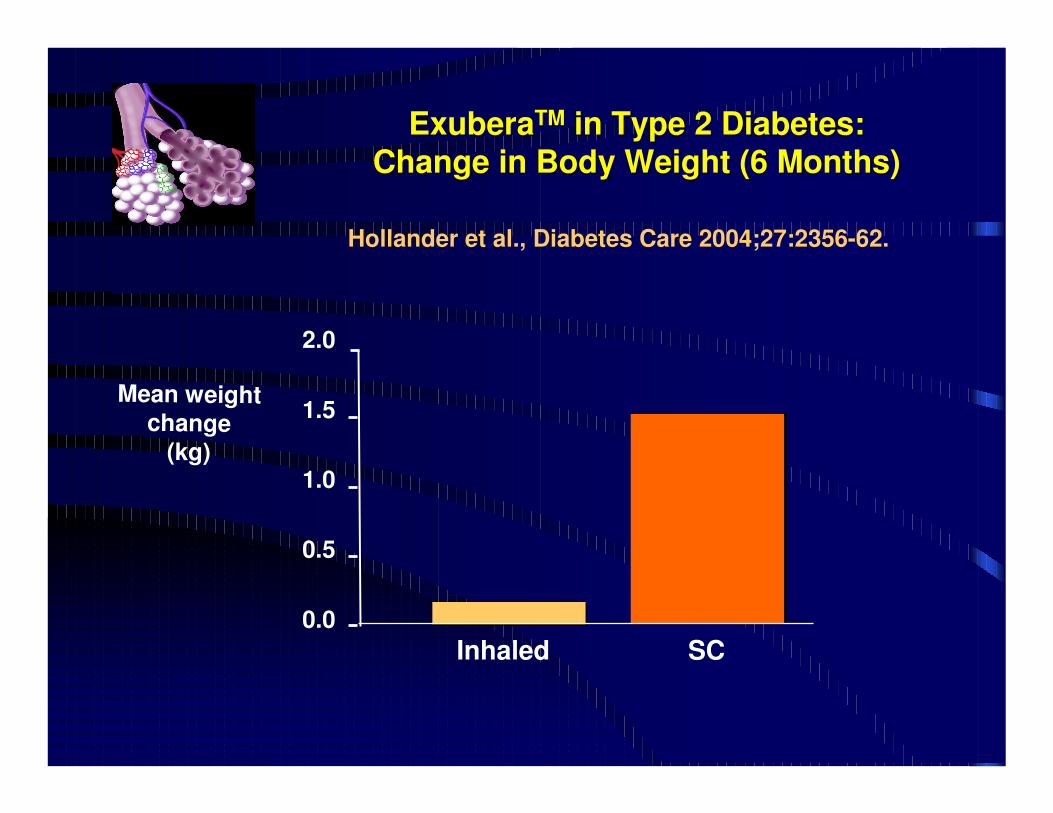
Inhaled SC
Mean weightchange
(kg)
0.0
0.5
1.0
1.5
2.0
ExuberaExuberaTMTM in Type 2 Diabetes:in Type 2 Diabetes:
Change in Body Weight (6 Months)Change in Body Weight (6 Months)
Hollander et al., Diabetes Care 2004;27:2356-62.
Current Experience of Glucose Control with Current Experience of Glucose Control with
Insulin Injections in Type 2 DiabetesInsulin Injections in Type 2 Diabetes
�� Evolution of insulin therapy toward Evolution of insulin therapy toward basalbasal--bolusbolus is is needed to reach target.needed to reach target.
�� High insulin dosesHigh insulin doses are commonly requested, are commonly requested, according to according to fat distribution and liver fat distribution and liver steatosissteatosis..
�� Insulin analoguesInsulin analogues decrease occurrence of hypos, decrease occurrence of hypos, improve glucose stability, may reduce weight improve glucose stability, may reduce weight gain but gain but often fail in further lowering of HbA1coften fail in further lowering of HbA1c..
�� Expected benefit of Expected benefit of inhaled insulininhaled insulin looks looks minor, minor, except for the acceptance of insulin and except for the acceptance of insulin and perhaps perhaps for weight controlfor weight control..
What Can We Expect from Insulin Pumps in What Can We Expect from Insulin Pumps in
Type 2 Diabetes ?Type 2 Diabetes ?
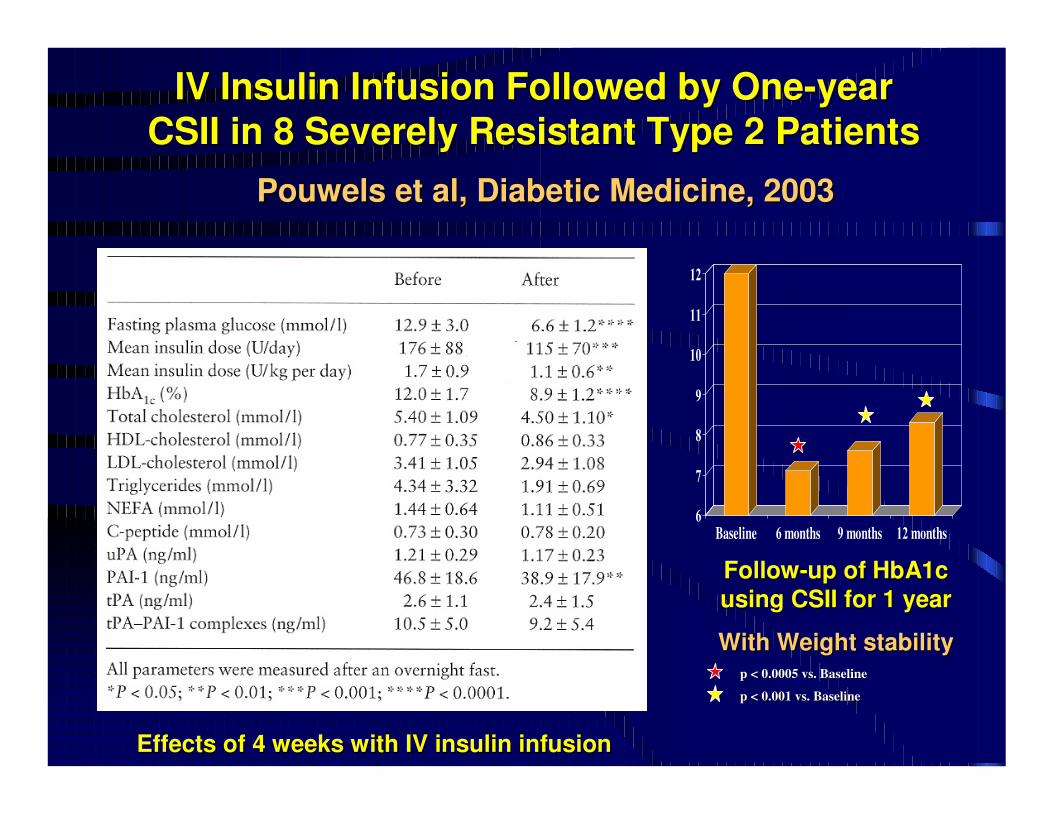
IV Insulin Infusion Followed by OneIV Insulin Infusion Followed by One--year year
CSII in 8 Severely Resistant Type 2 PatientsCSII in 8 Severely Resistant Type 2 Patients
PouwelsPouwels et al, Diabetic Medicine, 2003et al, Diabetic Medicine, 2003
6
7
8
9
10
11
12
Baseline 6 months 9 months 12 months
FollowFollow--up of HbA1c up of HbA1c
using CSII for 1 yearusing CSII for 1 year
With Weight stabilityWith Weight stabilityp < 0.0005 vs. Baselinep < 0.0005 vs. Baseline
p < 0.001 vs. Baselinep < 0.001 vs. Baseline
Effects of 4 weeks with IV insulin infusionEffects of 4 weeks with IV insulin infusion
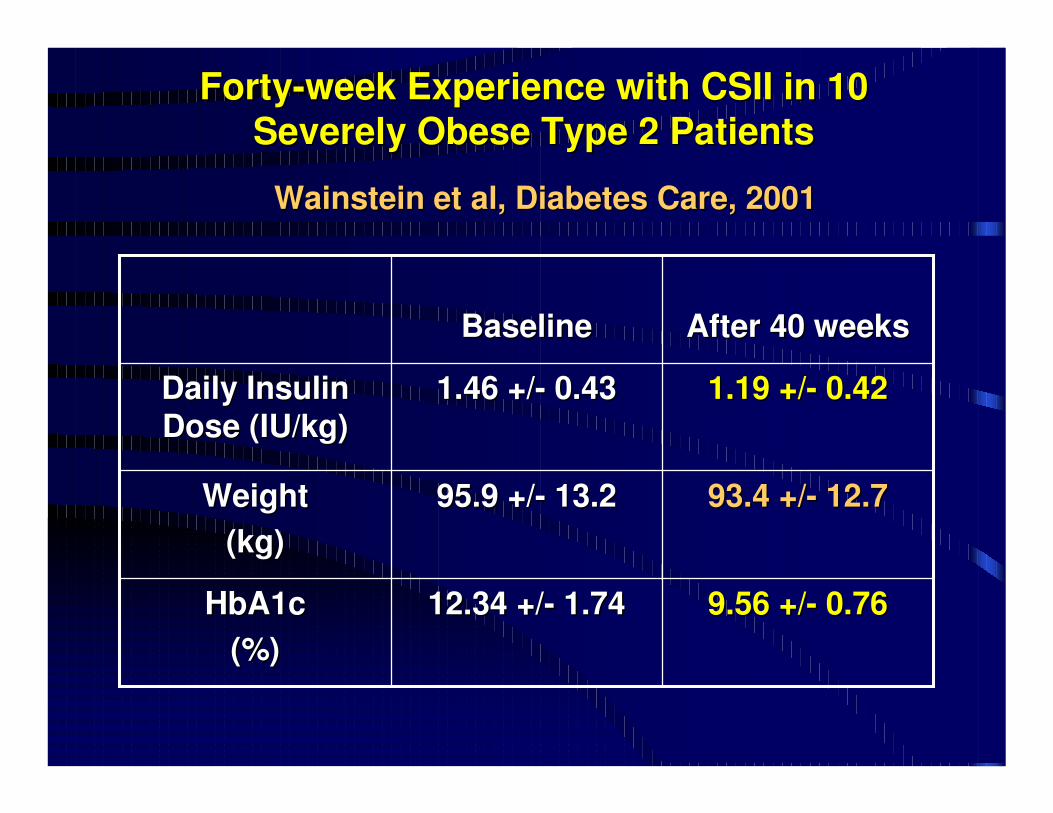
FortyForty--week Experience with CSII in 10 week Experience with CSII in 10
Severely Obese Type 2 PatientsSeverely Obese Type 2 Patients
WainsteinWainstein et al, Diabetes Care, 2001et al, Diabetes Care, 2001
9.56 +/9.56 +/-- 0.760.7612.34 +/12.34 +/-- 1.741.74HbA1cHbA1c
(%)(%)
93.4 +/93.4 +/-- 12.712.795.9 +/95.9 +/-- 13.213.2Weight Weight
(kg)(kg)
1.19 +/1.19 +/-- 0.420.421.46 +/1.46 +/-- 0.430.43Daily Insulin Daily Insulin
Dose (IU/kg)Dose (IU/kg)
After 40 weeksAfter 40 weeksBaselineBaseline
Does it mean
that insulin
pump is only
good for me ?
No Sir, we
shall perform
randomized
studies now !
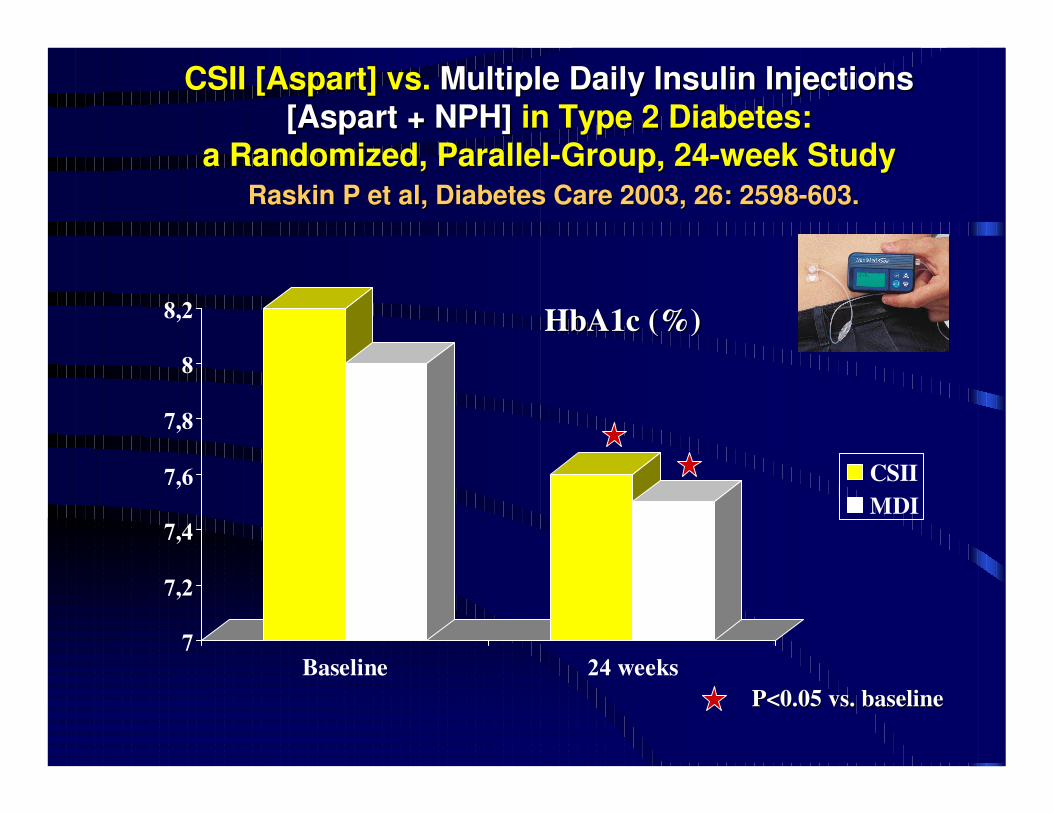
CSII [CSII [AspartAspart] vs. ] vs. Multiple Multiple DailyDaily InsulinInsulin InjectionsInjections
[[AspartAspart + NPH]+ NPH] in Type 2 in Type 2 DiabetesDiabetes: :
a a RandomizedRandomized, , ParallelParallel--GroupGroup, 24, 24--week week StudyStudy
RaskinRaskin P et P et alal, , DiabetesDiabetes Care 2003, 26: 2598Care 2003, 26: 2598--603.603.
7
7,2
7,4
7,6
7,8
8
8,2
Baseline 24 weeks
CSII
MDI
P<0.05 vs. P<0.05 vs. baselinebaseline
HbA1c (%)HbA1c (%)
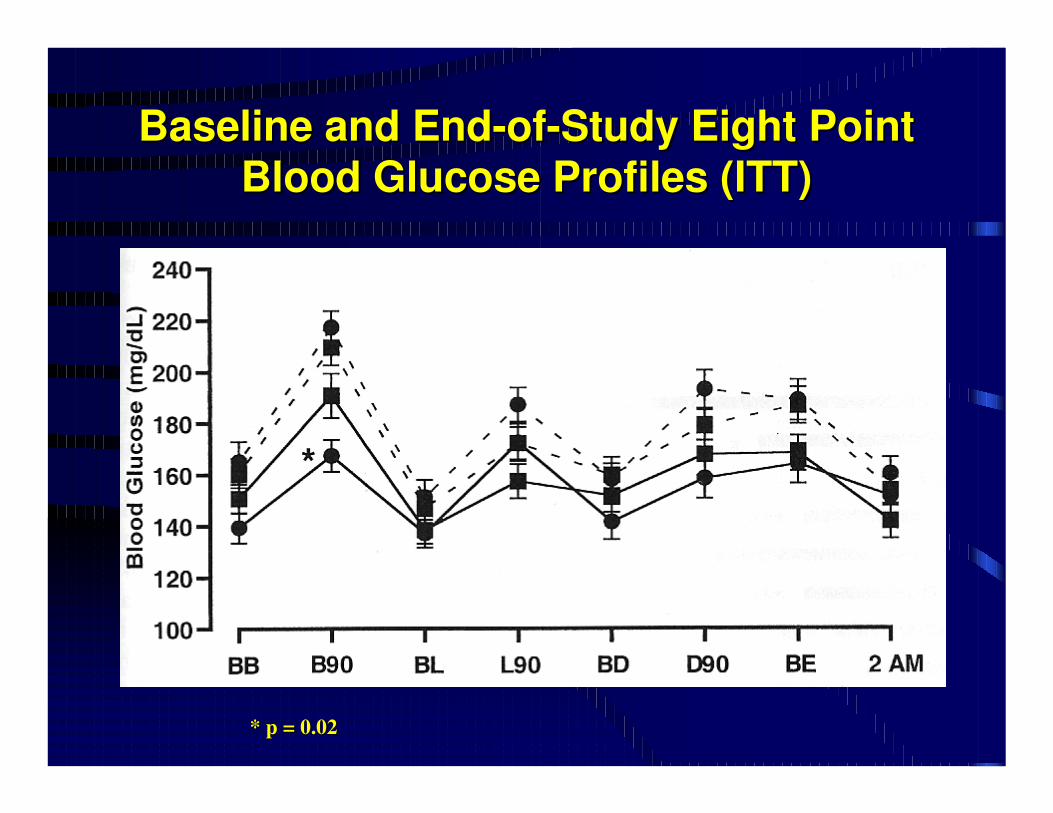
Baseline and EndBaseline and End--ofof--Study Eight Point Study Eight Point
Blood Glucose Profiles (ITT)Blood Glucose Profiles (ITT)
* p = 0.02* p = 0.02
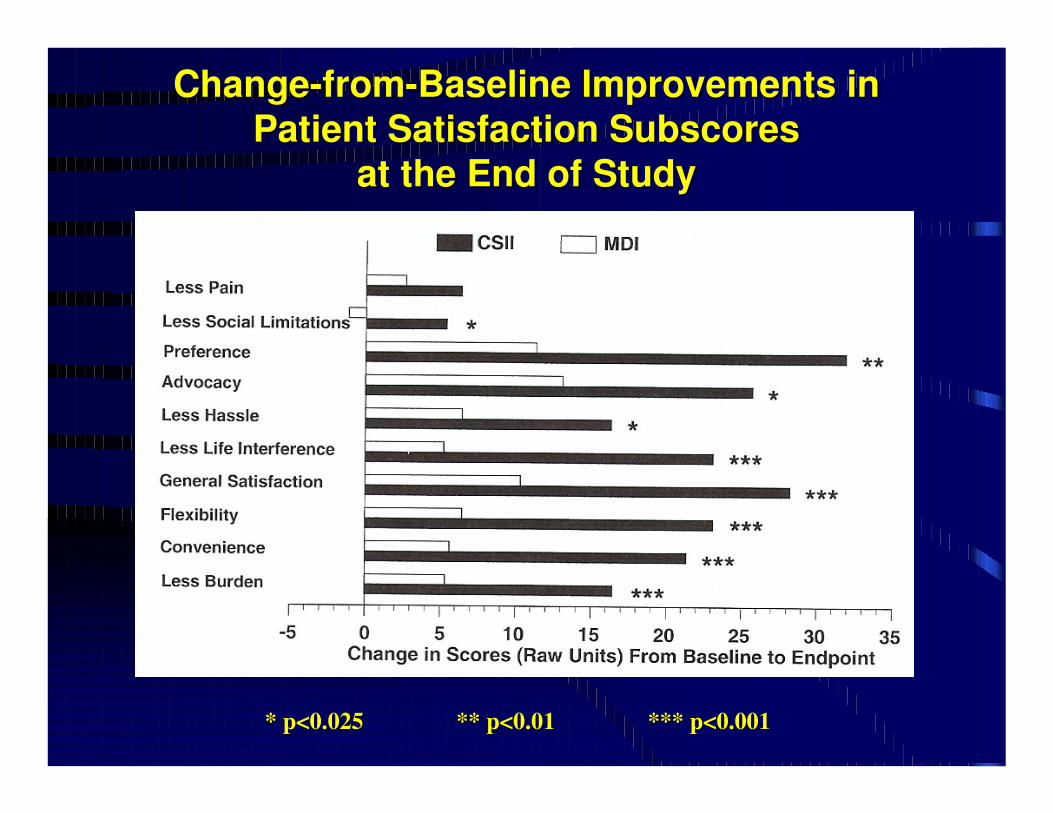
ChangeChange--fromfrom--Baseline Improvements in Baseline Improvements in
Patient Satisfaction Patient Satisfaction SubscoresSubscores
at the End of Studyat the End of Study
* p<0.025* p<0.025 ** p<0.01** p<0.01 *** p<0.001*** p<0.001
For sure,
they will
never try
to
randomize
me…
Don’t be
so
negative,
it may
happen !
… and
for now,
don’t
move !!
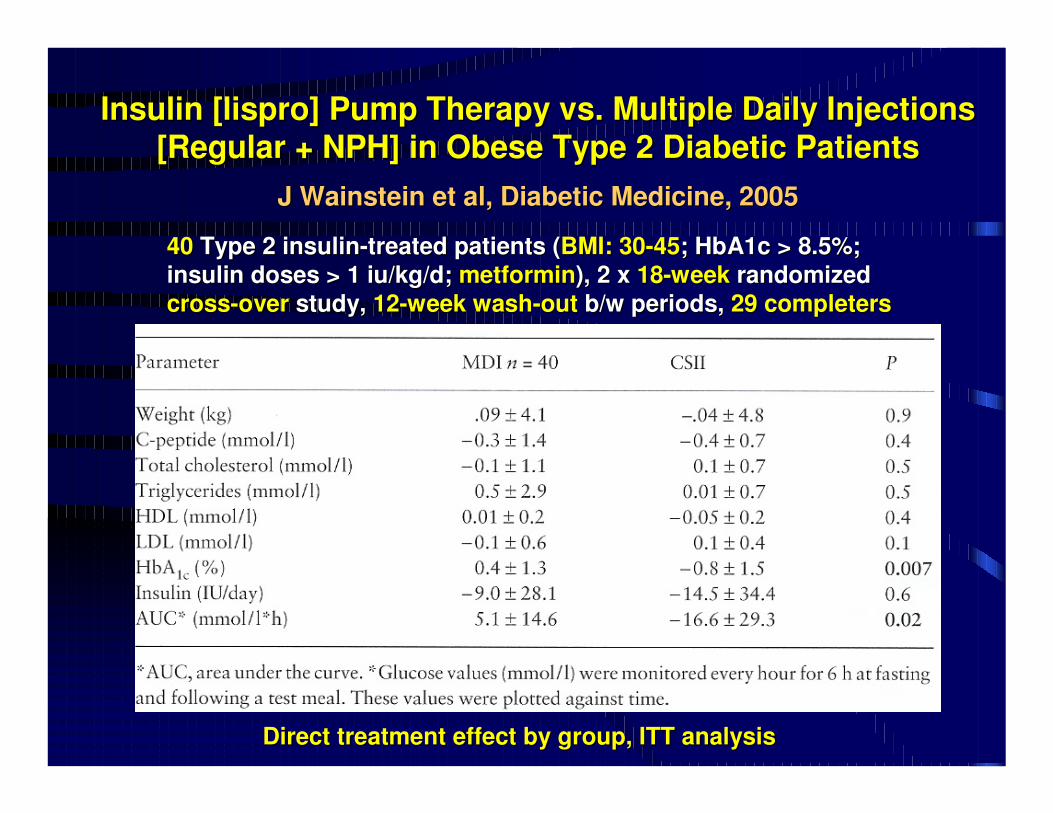
Insulin [Insulin [lisprolispro] Pump Therapy vs. Multiple Daily Injections ] Pump Therapy vs. Multiple Daily Injections
[Regular + NPH] in Obese Type 2 Diabetic Patients[Regular + NPH] in Obese Type 2 Diabetic Patients
J J WainsteinWainstein et al, Diabetic Medicine, 2005et al, Diabetic Medicine, 2005
4040 Type 2 insulinType 2 insulin--treated patients (treated patients (BMI: 30BMI: 30--4545; HbA1c > 8.5%; ; HbA1c > 8.5%;
insulin doses > 1 insulin doses > 1 iu/kg/diu/kg/d; ; metforminmetformin), 2 x ), 2 x 1818--weekweek randomized randomized
crosscross--overover study, study, 1212--week washweek wash--outout b/w periods, b/w periods, 29 completers29 completers
Direct treatment effect by group, ITT analysisDirect treatment effect by group, ITT analysis
Take your hands Take your hands
away of my pump !!!away of my pump !!!
The Results of this Study The Results of this Study FavourFavour Pump Therapy for Pump Therapy for
hardhard--toto--control Type 2 Obese Patientscontrol Type 2 Obese Patients
Gee ! ThatGee ! That’’s s
fun. Can I be fun. Can I be
randomized, randomized,
too ?too ?
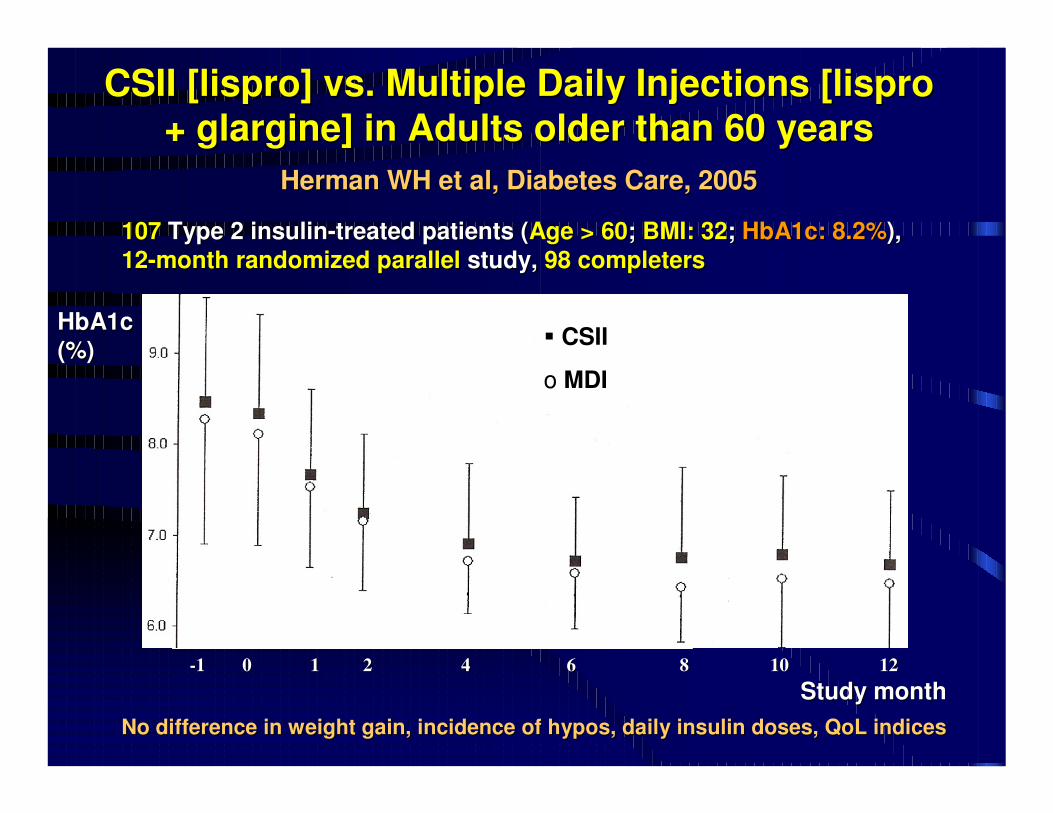
CSII [CSII [lisprolispro] vs. Multiple Daily Injections [] vs. Multiple Daily Injections [lisprolispro
+ + glargineglargine] in Adults older than 60 years] in Adults older than 60 years
Herman WH et al, Diabetes Care, 2005Herman WH et al, Diabetes Care, 2005
107107 Type 2 insulinType 2 insulin--treated patients (treated patients (Age > 60Age > 60; ; BMI: 32BMI: 32; ; HbA1c: 8.2%HbA1c: 8.2%), ),
1212--month randomizedmonth randomized parallelparallel study, study, 98 completers98 completers
--11 00 11 22 44 66 88 1010 1212
HbA1c HbA1c
(%)(%)
Study monthStudy month
�� CSII CSII
oo MDIMDI
No difference in weight gain, incidence of hypos, daily insulin No difference in weight gain, incidence of hypos, daily insulin doses, doses, QoLQoL indicesindices

OK for oldies, but what
about us, playing rugby ?
Don’t look for
my pump, it’s
internal !
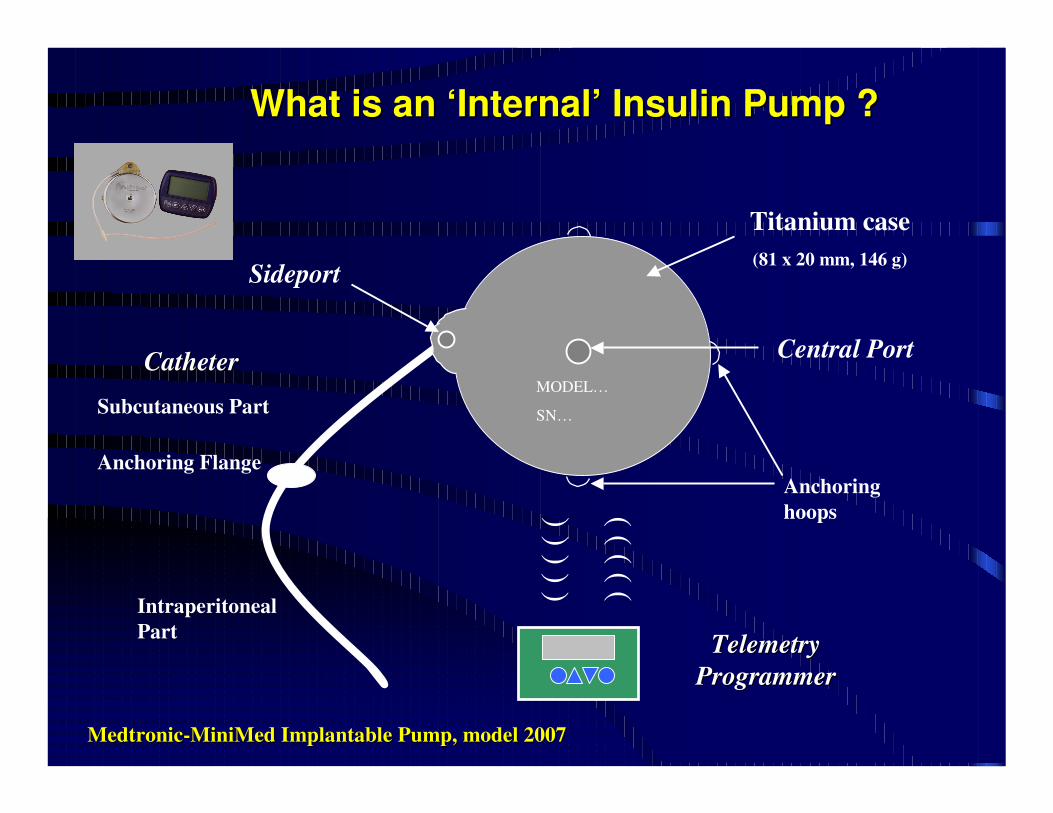
What is an ‘Internal’ Insulin Pump ? What is an ‘Internal’ Insulin Pump ?
CathCatheterter
Telemetry Telemetry
ProgrammerProgrammer
Central Port
Sideport
MODEL…
SN…Subcutaneous Part
Anchoring Flange
Intraperitoneal
Part
Anchoring
hoops
) )
) )
)) ) ) ) )
Titanium case
(81 x 20 mm, 146 g)
MedtronicMedtronic--MiniMedMiniMed Implantable Pump, model 2007Implantable Pump, model 2007
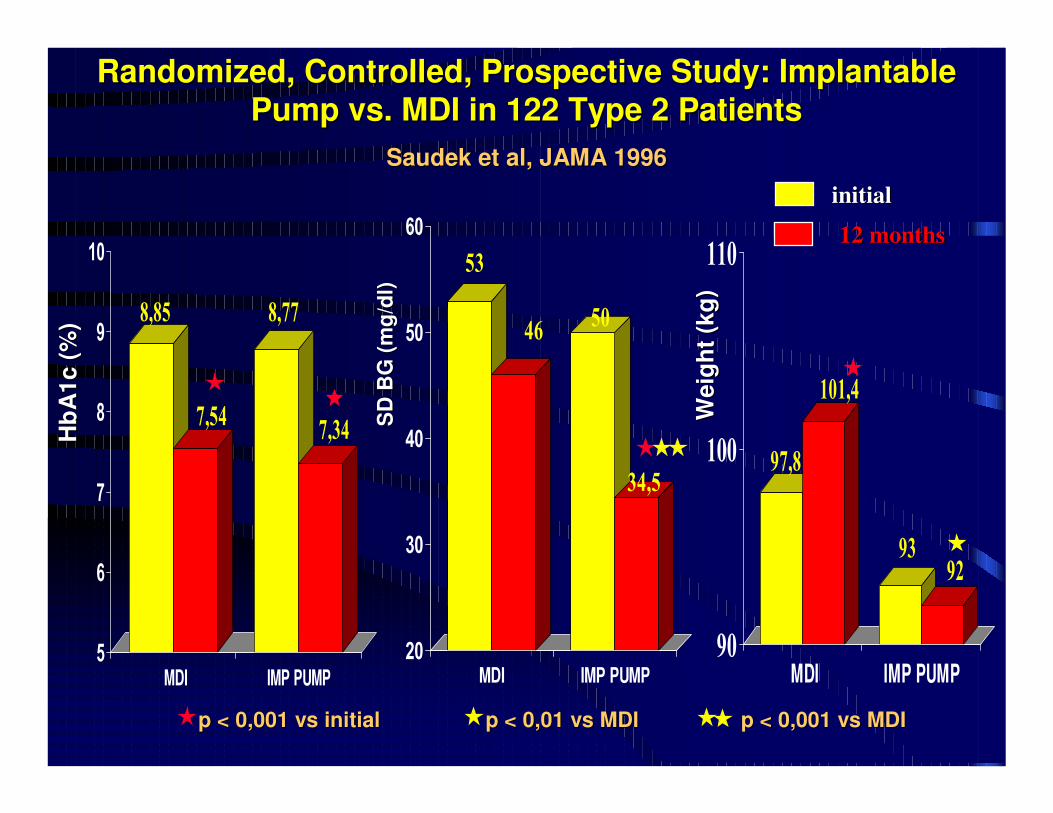
RandomizedRandomized, , ControlledControlled, Prospective , Prospective StudyStudy: Implantable : Implantable
PumpPump vs. MDI in 122 Type 2 Patientsvs. MDI in 122 Type 2 Patients
SaudekSaudek et et alal, JAMA 1996, JAMA 1996
8,85
7,54
8,77
7,34
5
6
7
8
9
10
MDI IMP PUMP
97,8
101,4
9392
90
100
110
MDI IMP PUMP
53
4650
34,5
20
30
40
50
60
MDI IMP PUMP
p < 0,001 vs initialp < 0,001 vs initial
SD
BG
(m
g/d
l)S
D B
G (
mg
/dl)
initialinitial
12 12 monthsmonths
p < 0,01 vs MDIp < 0,01 vs MDI p < 0,001 vs MDIp < 0,001 vs MDIW
eig
ht
(kg
)W
eig
ht
(kg
)
Hb
A1
c (
%)
Hb
A1
c (
%)
What Can We Expect from Insulin Pumps in What Can We Expect from Insulin Pumps in
Type 2 Diabetes ?Type 2 Diabetes ?
�� Insulin pumps are usable Insulin pumps are usable at any ageat any age with with at least at least similar effectivenesssimilar effectiveness, , no further weight gainno further weight gain, , no no more acute eventsmore acute events when compared with MDI when compared with MDI using analogues or not.using analogues or not.
�� They They may provide better satisfactionmay provide better satisfaction because of because of increased flexibility of use and avoidance of increased flexibility of use and avoidance of injections, injections, as they do in type 1as they do in type 1 diabetic patients.diabetic patients.
�� They may help in They may help in more efficientmore efficient glucose control glucose control in in severely resistant, obeseseverely resistant, obese patients.patients.
�� Further studies are needed to Further studies are needed to assess costassess cost--effectiveness and effectiveness and ––benefitbenefit..
Insulin Pump Therapy in Type 2 DiabetesInsulin Pump Therapy in Type 2 Diabetes
Yes, when glucose control with MDI looks as an
‘impossible mission’.
No, there is no reason for
any ‘diktat’ against pump in these patients.
We will probably have to think more of using pumps in the
future: younger patients, QoLissues, glucose sensors…
BeBe WelcomeWelcome in Montpellier to in Montpellier to KnowKnow More More
about about TheThe Future Future ofof DiabetesDiabetes TherapyTherapy !!
1st EuropeanDiabetes
Technology andTransplantation
Meeting