Embed Size (px)
Citation preview

Original Article
Early fetal echocardiography: Experience of a tertiary diagnostic service
Ritu MOGRA,1,2,3 Rahmah SAAID,1 Greg KESBY,1,3 Janette HAYWARD,3
Jessica MALKOUN3 and Jon HYETT1,2
1Department of High Risk Obstetrics, RPA Women and Babies, Royal Prince Alfred Hospital, 2Discipline of Obstetrics, Gynaecology andNeonatology, Faculty of Medicine, University of Sydney, and 3Sydney Ultrasound for Women, Sydney, New South Wales, Australia
Background: There is a growing body of evidence that most of the major cardiac abnormalities can be diagnosed at 14–15 weeks of gestation. We present our experience of early fetal echocardiography.Materials and Methods: This is a retrospective cohort study of women referred for early fetal echocardiography at 13–16 weeks of gestation at Royal Prince Alfred Hospital and Sydney Ultrasound for Women between August 2011 andMarch 2014. Findings of early fetal echocardiography, details of subsequent ultrasound examinations and pregnancyoutcome were recorded.Results: Early fetal echocardiography was performed in 400 euploid fetuses at a mean gestational age of 15+2 weeks. 85%of women were referred for increased nuchal translucency. 383/400 (96%) women had both normal early and late fetalechocardiograms 15/400 (3.7%) were found to have a cardiac defect at early fetal echocardiography, including 14 majorand one minor abnormality. Two additional minor cardiac defects were diagnosed at later antenatal ultrasounds. One case,defined as being normal antenatally, was found to have a minor cardiac abnormality post-natally. Eight (57%) womenwhose fetus had a major cardiac defect chose to terminate the pregnancy. In the pregnancies that continued, the sensitivityand specificity for major cardiac defects was 100%, 95% CI (0.98–1.00).Conclusion: Early fetal echocardiography is feasible and highly sensitive and specific in experienced hands. The highspecificity facilitates early reassurance of those women assessed at increased risk for fetal cardiac malformations.
Key words: congenital heart disease, echocardiography, fetus, prenatal diagnosis, ultrasound.
Introduction
Congenital heart disease (CHD) is a significantcontributor to infant mortality and morbidity. Majorabnormalities that are potentially lethal or require surgicalrepair within the first year of life affect approximately 4per 1000 live births.1,2 This is similar to the prenatalprevalence of chromosomal abnormality, but thedevelopment of highly sensitive screening programs foraneuploidy means that CHD is effectively six times morecommon in the post-natal period.3,4 Antenatal screeningfor CHD has proven to be difficult. Policies defining ahigh-risk cohort based on maternal demographics are oflimited value as the majority (>90%) of affected infantshave no significant historical identifier.5,6 Routineanatomical assessment at the 20-week morphologyultrasound scan, imaging the four-chamber view and
outflow tracts, has had varying success7,8 with reliance onthis mid-trimester assessment also meaning thatabnormalities are identified relatively late in pregnancy,increasing the social, psychological and medical risksassociated with decisions around termination ofpregnancy.9
The ability to detect fetal cardiac malformations in the1st trimester is desirable but limited by fetal size and otherimaging considerations. Nevertheless, markers for cardiacabnormality can be ascertained at 11–13+6 weeks ofgestation, including increased nuchal translucency andchanges in the haemodynamic patterns of flow through thetricuspid valve and ductus venosus, which are known toidentify a group of women at increased risk for fetalcardiac malformations.10–12 Improvements in theresolution of 2D grey scale and colour Doppler ultrasoundimaging, and increasing confidence with regard to fetalechocardiography, mean that it is becoming easierto interrogate the fetal heart at earlier points ingestation.13,14 Many major cardiac defects can beeffectively diagnosed at an earlier stage of pregnancy, withhigh levels of sensitivity and specificity, allowing cliniciansto have confidence in managing these findings.15–21 Wereport our experience in offering an early fetalechocardiography service to women identified at increased
Correspondence: Dr Ritu Mogra, Staff Specialist in Obstetricand Gynaecological Ultrasound, RPA Women and Babies,Royal Prince Alfred Hospital, Missenden Road,Camperdown, NSW 2050, Australia. Email:[email protected]
Received 14 January 2015; accepted 18 June 2015.
552 © 2015 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
Australian and New Zealand Journal of Obstetrics and Gynaecology 2015; 55: 552–558 DOI: 10.1111/ajo.12379
Th e Australian and New Zealand Journal of Obstetrics and Gynaecology
risk for fetal cardiac malformation in Sydney, New SouthWales (NSW), Australia.
Materials and Methods
This was a retrospective review of a cohort of pregnanciesthat had early fetal echocardiography performed at onetertiary obstetric hospital and one private practice incentral Sydney, NSW. The data represent a consecutivecohort of women seen between August 2011 and March2014. Early fetal echocardiography was performedbetween 13 and 16 weeks’ gestation. Pregnancies thatwere affected by chromosomal abnormality are excludedfrom this data set. Analysis was performed in accordancewith ethics approval granted by Sydney Local HealthDistrict.The early fetal echocardiography service accepted
referrals from multiple disciplines, including generalpractitioners, obstetricians, maternal–fetal medicinespecialists and clinical geneticists. Appointments werescheduled after and separate to screening for chromosomalabnormality (typically performed at 11–13+6 weeks’gestation). Women who had a high risk for aneuploidycalculated by combined first trimester screening wereoffered invasive testing (chorionic villus sampling), andthese results were normally available at the time ofechocardiographic assessment. All early fetalechocardiograms were performed by one sonologist (RM)who has received training and has a special interest in thisarea.Two-dimensional sonography and colour flow mapping
(E8, General Electric Company, Cincinnati, OH, USAwith RAB 4–8 Mhz transabdominal and 5–9 Mhztransvaginal probes) were used to assess abdominal situs,the four-chamber view, the right and left ventricularoutflow tracts, including crossover of the great arteries, thethree-vessel and tracheal views.22 Systemic and pulmonaryvenous drainage was also assessed. In most cases, all views
could be obtained using a transabdominal approach. Incases where these views were not satisfactory, transvaginalassessment was also performed (5% of total cases). Inaddition to the cardiac assessment, a systematic sequentialanatomical survey was performed. Women werecounselled about any abnormality and those that chose tocontinue the pregnancy had further detailedechocardiography at 20 weeks’ gestation and weremanaged by a multidisciplinary paediatric cardiologyservice through to delivery and infancy.Details describing the indication for referral were
prospectively recorded at the time of the examinationtogether with maternal demographic history and thefindings at each ultrasound examination. In circumstanceswhere an infant was born with a cardiac defect, details ofthe nature of the anomaly were obtained from post-natalechocardiogram and/or surgical records.
Results
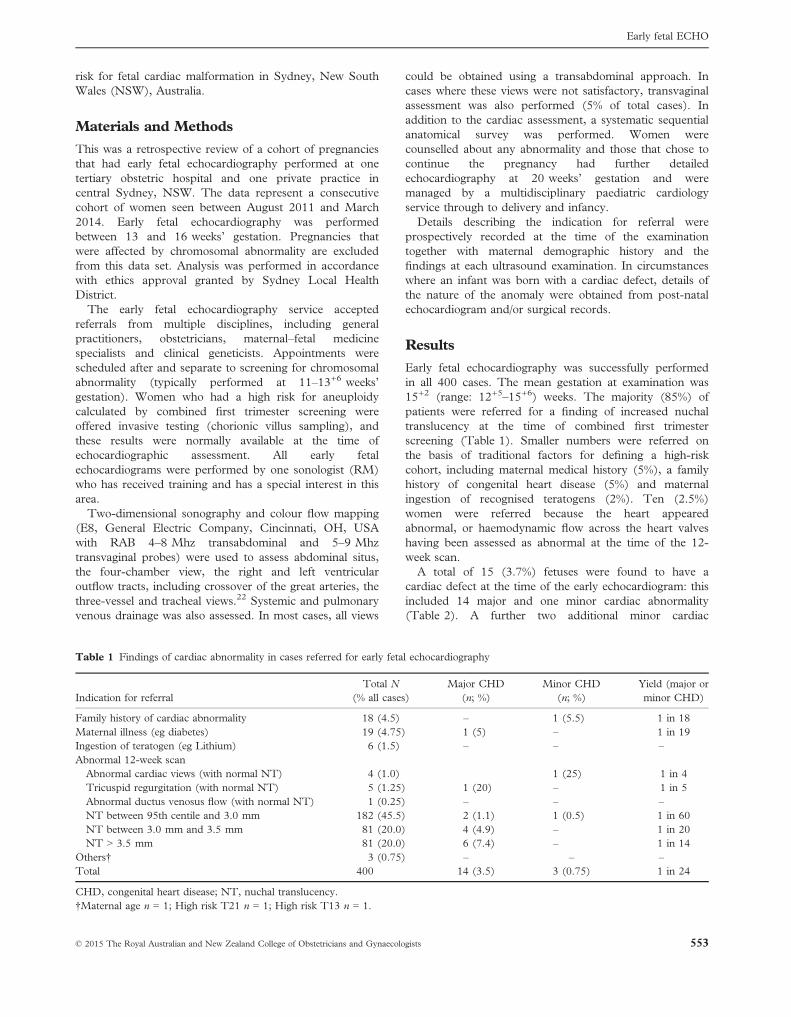
Early fetal echocardiography was successfully performedin all 400 cases. The mean gestation at examination was15+2 (range: 12+5–15+6) weeks. The majority (85%) ofpatients were referred for a finding of increased nuchaltranslucency at the time of combined first trimesterscreening (Table 1). Smaller numbers were referred onthe basis of traditional factors for defining a high-riskcohort, including maternal medical history (5%), a familyhistory of congenital heart disease (5%) and maternalingestion of recognised teratogens (2%). Ten (2.5%)women were referred because the heart appearedabnormal, or haemodynamic flow across the heart valveshaving been assessed as abnormal at the time of the 12-week scan.A total of 15 (3.7%) fetuses were found to have a
cardiac defect at the time of the early echocardiogram: thisincluded 14 major and one minor cardiac abnormality(Table 2). A further two additional minor cardiac
Table 1 Findings of cardiac abnormality in cases referred for early fetal echocardiography
Indication for referralTotal N
(% all cases)Major CHD
(n; %)Minor CHD
(n; %)Yield (major orminor CHD)
Family history of cardiac abnormality 18 (4.5) – 1 (5.5) 1 in 18Maternal illness (eg diabetes) 19 (4.75) 1 (5) – 1 in 19Ingestion of teratogen (eg Lithium) 6 (1.5) – – –Abnormal 12-week scanAbnormal cardiac views (with normal NT) 4 (1.0) 1 (25) 1 in 4Tricuspid regurgitation (with normal NT) 5 (1.25) 1 (20) – 1 in 5Abnormal ductus venosus flow (with normal NT) 1 (0.25) – – –NT between 95th centile and 3.0 mm 182 (45.5) 2 (1.1) 1 (0.5) 1 in 60NT between 3.0 mm and 3.5 mm 81 (20.0) 4 (4.9) – 1 in 20NT > 3.5 mm 81 (20.0) 6 (7.4) – 1 in 14
Others† 3 (0.75) – – –Total 400 14 (3.5) 3 (0.75) 1 in 24
CHD, congenital heart disease; NT, nuchal translucency.†Maternal age n = 1; High risk T21 n = 1; High risk T13 n = 1.
© 2015 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists 553
Early fetal ECHO
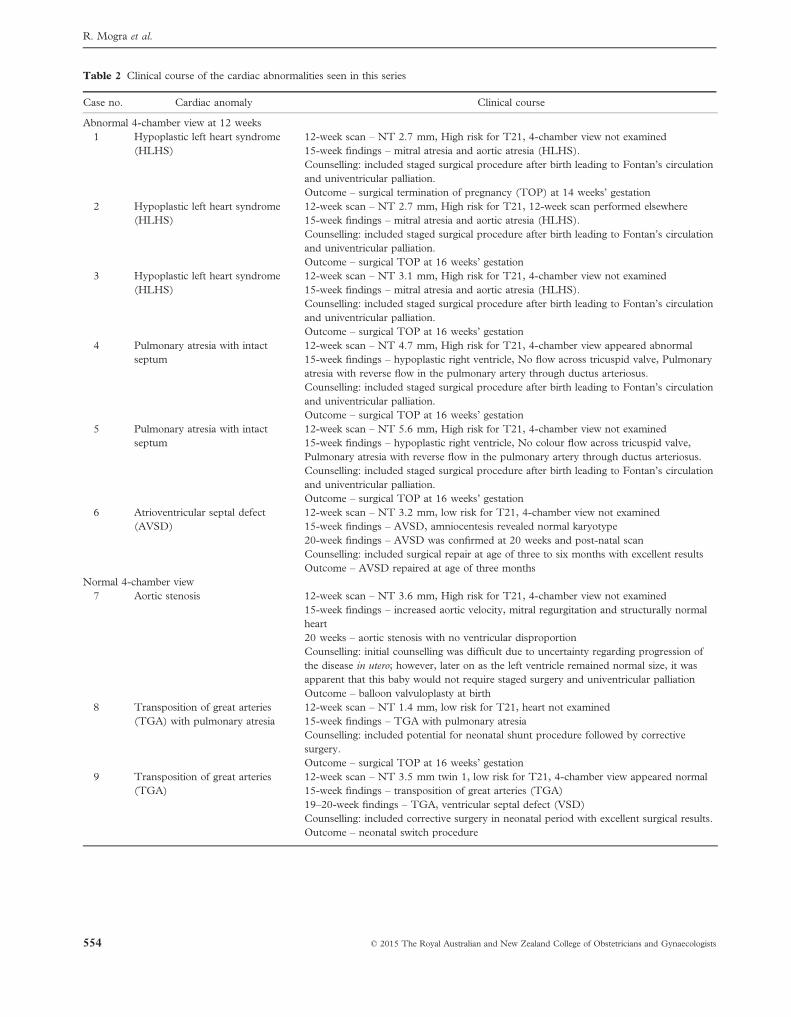
Table 2 Clinical course of the cardiac abnormalities seen in this series
Case no. Cardiac anomaly Clinical course
Abnormal 4-chamber view at 12 weeks1 Hypoplastic left heart syndrome
(HLHS)12-week scan – NT 2.7 mm, High risk for T21, 4-chamber view not examined15-week findings – mitral atresia and aortic atresia (HLHS).Counselling: included staged surgical procedure after birth leading to Fontan’s circulationand univentricular palliation.Outcome – surgical termination of pregnancy (TOP) at 14 weeks’ gestation
2 Hypoplastic left heart syndrome(HLHS)
12-week scan – NT 2.7 mm, High risk for T21, 12-week scan performed elsewhere15-week findings – mitral atresia and aortic atresia (HLHS).Counselling: included staged surgical procedure after birth leading to Fontan’s circulationand univentricular palliation.Outcome – surgical TOP at 16 weeks’ gestation
3 Hypoplastic left heart syndrome(HLHS)
12-week scan – NT 3.1 mm, High risk for T21, 4-chamber view not examined15-week findings – mitral atresia and aortic atresia (HLHS).Counselling: included staged surgical procedure after birth leading to Fontan’s circulationand univentricular palliation.Outcome – surgical TOP at 16 weeks’ gestation
4 Pulmonary atresia with intactseptum
12-week scan – NT 4.7 mm, High risk for T21, 4-chamber view appeared abnormal15-week findings – hypoplastic right ventricle, No flow across tricuspid valve, Pulmonaryatresia with reverse flow in the pulmonary artery through ductus arteriosus.Counselling: included staged surgical procedure after birth leading to Fontan’s circulationand univentricular palliation.Outcome – surgical TOP at 16 weeks’ gestation
5 Pulmonary atresia with intactseptum
12-week scan – NT 5.6 mm, High risk for T21, 4-chamber view not examined15-week findings – hypoplastic right ventricle, No colour flow across tricuspid valve,Pulmonary atresia with reverse flow in the pulmonary artery through ductus arteriosus.Counselling: included staged surgical procedure after birth leading to Fontan’s circulationand univentricular palliation.Outcome – surgical TOP at 16 weeks’ gestation
6 Atrioventricular septal defect(AVSD)
12-week scan – NT 3.2 mm, low risk for T21, 4-chamber view not examined15-week findings – AVSD, amniocentesis revealed normal karyotype20-week findings – AVSD was confirmed at 20 weeks and post-natal scanCounselling: included surgical repair at age of three to six months with excellent resultsOutcome – AVSD repaired at age of three months
Normal 4-chamber view7 Aortic stenosis 12-week scan – NT 3.6 mm, High risk for T21, 4-chamber view not examined
15-week findings – increased aortic velocity, mitral regurgitation and structurally normalheart20 weeks – aortic stenosis with no ventricular disproportionCounselling: initial counselling was difficult due to uncertainty regarding progression ofthe disease in utero; however, later on as the left ventricle remained normal size, it wasapparent that this baby would not require staged surgery and univentricular palliationOutcome – balloon valvuloplasty at birth
8 Transposition of great arteries(TGA) with pulmonary atresia
12-week scan – NT 1.4 mm, low risk for T21, heart not examined15-week findings – TGA with pulmonary atresiaCounselling: included potential for neonatal shunt procedure followed by correctivesurgery.Outcome – surgical TOP at 16 weeks’ gestation
9 Transposition of great arteries(TGA)
12-week scan – NT 3.5 mm twin 1, low risk for T21, 4-chamber view appeared normal15-week findings – transposition of great arteries (TGA)19–20-week findings – TGA, ventricular septal defect (VSD)Counselling: included corrective surgery in neonatal period with excellent surgical results.Outcome – neonatal switch procedure
554 © 2015 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
R. Mogra et al.
abnormalities (small ventricular septal defects that havenot required surgical repair) were identified on follow-upultrasound at 19 weeks’ gestation. A total of 12/14(85.7%) of the major cardiac defects had increased nuchaltranslucency at the time of the routine 11–13+6-week scan:six had a NT between the 95th centile and 3.5 mm(which equates to the 99th centile) and six had a NT>3.5 mm. The two remaining major defects weresuspected for differing reasons: a maternal history of type1 diabetes and the finding of tricuspid regurgitation at the12-week scan.A total of 180/400 cases had a high adjusted risk for
aneuploidy through combined first trimester screening. In
the high-risk group, 165 had an invasive test, six hadNIPT, and nine declined any further investigation. Allpregnancies that resulted in termination were karyotyped.In the liveborn cohort, no abnormal phenotypic featuressuggestive of chromosomal abnormalities were identified.A total of seven of the 14 (50%) women who had a
fetus affected by a major cardiac defect chose to terminatethe pregnancy <16 weeks’ gestation, and another had atermination of pregnancy after a second echocardiographicassessment at 20 weeks’ gestation. Ultrasound-basedcardiac findings were checked by a second experiencedsonologist prior to termination of pregnancy in all cases.Four women had fetal hypoplastic left heart, and two fetal
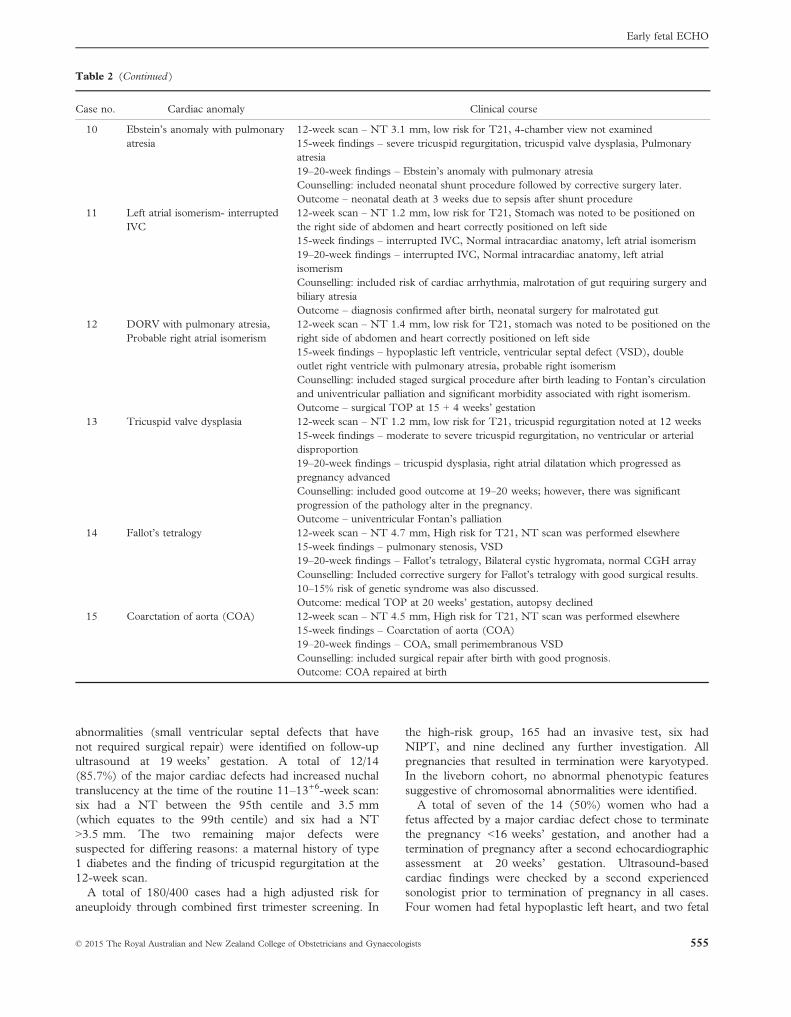
Table 2 (Continued )
Case no. Cardiac anomaly Clinical course
10 Ebstein’s anomaly with pulmonaryatresia
12-week scan – NT 3.1 mm, low risk for T21, 4-chamber view not examined15-week findings – severe tricuspid regurgitation, tricuspid valve dysplasia, Pulmonaryatresia19–20-week findings – Ebstein’s anomaly with pulmonary atresiaCounselling: included neonatal shunt procedure followed by corrective surgery later.Outcome – neonatal death at 3 weeks due to sepsis after shunt procedure
11 Left atrial isomerism- interruptedIVC
12-week scan – NT 1.2 mm, low risk for T21, Stomach was noted to be positioned onthe right side of abdomen and heart correctly positioned on left side15-week findings – interrupted IVC, Normal intracardiac anatomy, left atrial isomerism19–20-week findings – interrupted IVC, Normal intracardiac anatomy, left atrialisomerismCounselling: included risk of cardiac arrhythmia, malrotation of gut requiring surgery andbiliary atresiaOutcome – diagnosis confirmed after birth, neonatal surgery for malrotated gut
12 DORV with pulmonary atresia,Probable right atrial isomerism
12-week scan – NT 1.4 mm, low risk for T21, stomach was noted to be positioned on theright side of abdomen and heart correctly positioned on left side15-week findings – hypoplastic left ventricle, ventricular septal defect (VSD), doubleoutlet right ventricle with pulmonary atresia, probable right isomerismCounselling: included staged surgical procedure after birth leading to Fontan’s circulationand univentricular palliation and significant morbidity associated with right isomerism.Outcome – surgical TOP at 15 + 4 weeks’ gestation
13 Tricuspid valve dysplasia 12-week scan – NT 1.2 mm, low risk for T21, tricuspid regurgitation noted at 12 weeks15-week findings – moderate to severe tricuspid regurgitation, no ventricular or arterialdisproportion19–20-week findings – tricuspid dysplasia, right atrial dilatation which progressed aspregnancy advancedCounselling: included good outcome at 19–20 weeks; however, there was significantprogression of the pathology alter in the pregnancy.Outcome – univentricular Fontan’s palliation
14 Fallot’s tetralogy 12-week scan – NT 4.7 mm, High risk for T21, NT scan was performed elsewhere15-week findings – pulmonary stenosis, VSD19–20-week findings – Fallot’s tetralogy, Bilateral cystic hygromata, normal CGH arrayCounselling: Included corrective surgery for Fallot’s tetralogy with good surgical results.10–15% risk of genetic syndrome was also discussed.Outcome: medical TOP at 20 weeks’ gestation, autopsy declined
15 Coarctation of aorta (COA) 12-week scan – NT 4.5 mm, High risk for T21, NT scan was performed elsewhere15-week findings – Coarctation of aorta (COA)19–20-week findings – COA, small perimembranous VSDCounselling: included surgical repair after birth with good prognosis.Outcome: COA repaired at birth
© 2015 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists 555
Early fetal ECHO

hypoplastic right heart; these women had been advisedthat the baby would require staged operations leading toFontan’s circulation and univentricular palliation. Onefetus had transposition of the great arteries withpulmonary atresia that would have required a neonatalshunt procedure and corrective surgery later; the motherelected to interrupt the pregnancy at an early stage. Onewoman asked to terminate the pregnancy at 20 weeks’gestation; the fetus had Fallot’s tetralogy, and the decisionto end the pregnancy was based on the presence of otherextracardiac abnormalities. Seven women had a surgicaltermination <16 completed weeks’ gestation, and the fetalheart was not available for examination. One woman had amedical termination at 20 weeks’ gestation but declinedautopsy.The outcomes of the six pregnancies that had a major
defect and three pregnancies with minor anomalies thatcontinued to term were confirmed post-natally (Table 2).Additional minor cardiac findings (ventricular septaldefect) were identified in two of the cases with a majorone that had previously been defined as having coarctationof the aorta, the other with transposition of the greatarteries. No major cardiac anomalies were reported in theremaining cohort of 383 women who had a normal earlyfetal echocardiography and a normal scan at 20 weeks,although one infant, affected by Noonan syndrome, wasfound to have pulmonary stenosis at six months of age –this is being managed expectantly.The sensitivity for major cardiac defects for the
pregnancies which continued was 100%, 95% CI (0.74–1.00) and specificity was 100%, 95% CI (0.98–1.00).
Discussion
Early fetal echocardiography provides a valuableopportunity to examine fetal cardiac anatomy in womendeemed to have a fetus at high risk of having an affectedpregnancy. A total of 3.7% of fetuses referred forassessment at this early gestation had a cardiacabnormality, approximately a tenfold increase on theprevalence seen in a background population. Thesensitivity and specificity in detecting major defects wasvery high (100%) as was the negative predictive value – sowomen deemed to be high risk after their 12-week scancould also benefit from early echocardiographicreassurance. Minor defects were harder to identify at thisearly gestation. Although the sample size is small (onlyfour fetuses had an isolated minor cardiac defect), onlyone of these anomalies was detected at 14–15 weeks’gestation, whilst two were identified at 19 weeks and onewas not defined until six months of age.There are no recognised national or international
guidelines describing indications for referral for early fetalechocardiography. Indications typically vary according toresources that are available. We have establishedindications for referral based on assessment of maternalhistory, indirect signs of cardiac function (nuchaltranslucency, ductus venosus and tricuspid valve
haemodynamics) and the appearance of the fetal heart atthe time of the 12-week scan. Increased nuchaltranslucency is recognised as being associated withstructural cardiac defects, although the sensitivity of thistool in screening for cardiac abnormalities has variedsignificantly in different studies.10,23 However, this markeris routinely assessed in all 11–13+6-week scans, and thiswas the commonest indication for referral in our cohort.We chose to define the 95th centile as the point where arisk of a cardiac defect was increased – and an early fetalechocardiogram should be offered. Using this cut-offallowed detection of twice as many major cardiac defects –although it also led to three times as many scans beingperformed when compared to a static 3.5 mm cut-off.The other indirect signs of a cardiac defect that can bedemonstrated at 11–13+6 weeks are reversed flow in the Awave of the ductus venosus and reversed flow across thetricuspid valve. These features are not commonly assessedas part of combined first trimester screening in Australia,reflected in the relatively low number of fetuses referredfor early fetal echocardiography on the basis of thesefindings in our series. This may also explain the apparentlow prevalence of these markers in the group of majorcardiac defects that were reviewed.Fetal heart activity is routinely documented at 11–
13+6 weeks, and if this is carried out using an axial sectionof the chest, the sonographer can demonstrate the four-chamber view in 90% of cases, which has a high yield forabnormality.24,25 Assessment of flow across the tricuspidvalve can also be carried out in the 4-chamber view oncethe sonographer has identified the right heart chambers,improving recognition of cardiac anatomy at11–13+6 weeks. Colour Doppler is also valuable indemonstrating the outflow tracts. Although few fetuseswere referred on the basis of ‘an abnormal four-chamberview’, these cases have a high yield for abnormality andsonographers should be encouraged to develop these skills.Increased NT is a strong indicator for cardiac
abnormality. In this cohort, an NT 95th centile to 3 mmhad a prevalence of cardiac abnormality of 1.1%; a 3.6-fold increase from the background population. Thisincreased to a prevalence of 4.9% with NT 3.0–3.5 mmand 7.4% with NT >3.5 mm. These rates are very similarto those reported previously.26–28 Each cut-off impacts onthe specificity and positive predictive value of screeningand needs to be tailored to suit local service availability.First trimester echocardiography for the detection of
major cardiac malformations has been shown to be highlysensitive and specific in experienced hands. Sensitivity andspecificity of major cardiac defects (for the pregnancieswhich continued) in our study was 100%, which is notdifferent from other studies performed by experiencedoperators in first trimester. Accuracy of first trimesterdetection of major cardiac abnormalities was demonstratedin a systematic review of studies where verification waspossible either by post-natal echocardiography or by post-mortem; specificity reached nearly 100% in pooledanalysis.29 Three recent studies evaluated diagnostic
556 © 2015 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
R. Mogra et al.

accuracy of early fetal echocardiography by post-natalfollow-up and have demonstrated that most major cardiacabnormalities were correctly diagnosed in the firsttrimester with few false positives.19–21 It is encouraging tosee that all false positives were minor defects for whichintervention in the pregnancy would not have beenconsidered at earlier stage. The high sensitivity andspecificity of early fetal echocardiography, including thehigh negative predictive value, demonstrates the value ofextending the skill sets of fetal medicine specialists andpaediatric cardiologists to provide this service.The limitations of this study include that the prenatal
sonographic findings were not confirmed through aprocess of autopsy in 57% of the pregnancies where thepregnancy was interrupted. These data reflect a referredpopulation, so we are unable to comment on theprevalence of cardiac disease in a wider population –although there are other series that have reported theprevalence and detection rates of cardiac defects inrelation to first trimester markers.In conclusion, we have demonstrated that early fetal
echocardiography is feasible and is highly sensitive,specific and accurate in the diagnosis of major cardiacabnormality in experienced hands. Detailed fetalechocardiography at 14–16 weeks’ gestation also providesearly reassurance when cardiac anatomy is normal.
References1 Campbell M. Incidence of cardiac malformations at birth and
later, and neonatal mortality. Br Heart J 1973; 35: 189–200.2 Hoffmann JIE, Christianson R. Congenital heart disease in a
cohort 19,502 births with long-term follow up. Am J Cardiol1978; 42: 641–647.
3 Van der Linde D, Konings EE, Slager MA. Birth prevalenceof congenital heart disease worldwide: a systematic review andmeta-analysis. J Am Coll Cardiol 2011; 58: 2241–2247.
4 Morris JK, Alberman E. Trends in Down’s syndrome livebirths and antenatal diagnoses in England and Wales from1989 to 2008: analysis of data from the National DownSyndrome Cytogenetic Register. BMJ 2009; 339: b3794.
5 Wilson NJ, Allen BC, Clarkson PM et al. One-year audit of areferral fetal echocardiography service. N Z Med J 1994; 107:258–260.
6 Maher JE, Colvin EV, Samdarshi TE et al. Fetalechocardiography in gravidas with historic risk factors forcongenital heart disease. Am J Perinatol 1994; 11: 334–336.
7 Tegnander E, Eik-Nes SH. The examiner’s ultrasoundexperience has a significant impact on the detection rate ofcongenital heart defects at the second-trimester fetalexamination. Ultrasound Obstet Gynecol 2006; 28: 8–14.
8 Ogge G, Gaglioti P, Maccanti S et al. Prenatal screening forcongenital heart disease with four-chamber and outflow-tractviews: a multicenter study. Ultrasound Obstet Gynecol 2006; 28:779–784.
9 Rauch ER, Smulian JC, De Prince K et al. Pregnancyinterruption after second trimester diagnosis of fetal structuralanomalies: the New Jersey Fetal Abnormalities Registry. Am JObstet Gynecol 2005; 193: 1492–1497.
10 Hyett JA, Perdu M, Sharland GK et al. Increased nuchaltranslucency at 10–14 weeks of gestation as a marker formajor cardiac defects. Ultrasound Obstet Gynecol 1997; 10:242–246.
11 Chelemen T, Syngelaki A, Maiz N et al. Contribution ofductus venosus Doppler in first trimester screening for majorcardiac defects. Fetal Diagn Ther 2011; 29: 127–134.
12 Pereira S, Ganapathy R, Syngelaki A et al. Contribution offetal tricuspid regurgitation in first trimester screening formajor cardiac defects. Obstet Gynecol 2011; 117: 1384–1391.
13 Sairam S, Carvalho JS. Early fetal echocardiography andanomaly scan in fetuses with increased nuchal translucency.Early Hum Dev 2012; 88: 269–272.
14 Comas Gabriel C, Galindo A, Mart�ınez JM et al. Earlyprenatal diagnosis of major cardiac anomalies in a high-riskpopulation. Prenat Diagn 2002; 22: 586–593.
15 Huggon IC, Ghi T, Cook AC et al. Fetal cardiacabnormalities identified prior to 14 weeks’ gestation.Ultrasound Obstet Gynecol 2002; 20: 22–29.
16 Simpson JM, Jones A, Callaghan N et al. Accuracy andlimitations of transabdominal fetal echocardiography at 12-15 weeks of gestation in a population at high risk for congenitalheart disease. BJOG 2000; 107: 1492–1497.
17 Zosmer N, Souter VL, Chan CS et al. Early diagnosis ofmajor cardiac defects in chromosomally normal fetuses withincreased nuchal translucency. Br J Obstet Gynaecol 1999;106: 829–833.
18 Rustico MA, Benettoni A, D’Ottavio G et al. Early screeningfor fetal cardiac anomalies by transvaginal echocardiographyin an unselected population: the role of operator experience.Ultrasound Obstet Gynecol 2000; 16: 614–619.
19 Vita Zidere MD, Bellsham-Revell H, Nicola Persico MD et al.A comparison of the echocardiographic findings in fetuses lessthan 15 weeks’ gestation with later cardiac evaluation.Ultrasound Obstet Gynecol 2013; 42: 679–686.
20 Mirza FG, Bauer ST, Williams IA et al. Early fetalechocardiography: ready for prime time? Am J Perinatol 2012;29: 313–318.
21 Volpe P, De Robertis V, Campobasso G et al. Diagnosis ofcongenital heart disease by early and second-trimester fetalechocardiography. J Ultrasound Med 2012; 31: 563–568.
22 Carvalho JS, Allan LD, Chaoui R et al. International Societyof Ultrasound in Obstetrics and Gynecology. Ultrasound ObstetGynecol 2013; 41: 348–359.
23 Westin M, Saltvedt S, Bergman G et al. Is measurement ofnuchal translucency thickness a useful screening tool for heartdefects? A study of 16,383 fetuses. Ultrasound Obstet Gynecol2006; 27: 632–639.
24 Haak MC, Twisk JWR, Van Vugt JMG et al. How successfulis fetal echocardiographic examination in the first trimester ofpregnancy? Ultrasound Obstet Gynecol 2002; 20: 9–13.
25 Gembruch U, Shi C, Smrcek JM et al. Biometry of the fetalheart between 10 and 17 weeks’ gestation. Fetal Diagn Ther2000; 15: 20–31.
26 Mogra R, Alabbad N, Hyett J. Increased nuchal translucencyand congenital heart disease. Early Hum Dev 2012; 88: 261–267.
27 Atzei A, Gajewska K, Huggon IC et al. Relationship betweennuchal translucency thickness and prevalence of major cardiac
© 2015 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists 557
Early fetal ECHO

defects in fetuses with normal karyotype. Ultrasound ObstetGynecol 2005; 26: 154–157.
28 Clur SA, Mathijssen IB, Pajkrt E et al. Structural heart defectsassociated with an increased nuchal translucency: 9 yearsexperience in a referral centre. Prenat Diagn 2008; 28: 347–354.
29 Rasiah SV, Publicover M, Ewer AK et al. A systematic reviewof the accuracy of first-trimester ultrasound examination fordetecting major congenital heart disease. Ultrasound ObstetGynecol 2006; 28: 110–116.
558 © 2015 The Royal Australian and New Zealand College of Obstetricians and Gynaecologists
R. Mogra et al.