Embed Size (px)
DESCRIPTION
A brief summary of the current state of e-prescribing in the pharmaceutical industry and recommendations for assessing this trend via primary marketing research.
Citation preview

Eric JohnSenior Vice PresidentOffice: 610-234-2083
Cell: [email protected]
E-Prescribing Assessment CapabilitiesMarch 2012

SMG Proprietary Information
Table of Contents
• What is E-Prescribing?
• Why E-Prescribing is Important
• Key E-Prescribing Issues to Assess
• E-Prescribing Assessment – Qualitative Approach
• Discussion Guide Flow
• Potential Output from E-Prescribing Study
• Team Biographies
2
2

SMG Proprietary Information
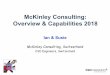
What is E-Prescribing?E-Prescribing reduces manual paperwork and the potential for medical errors, while increasing adherence in the prescription process
3
Patient sees physician and receives an Rx.
Physician/NP/PA uses laptop, PDA, or smartphone to generate patient’s prescription and electronically submits to patient’s pharmacy.E-Rx system at practice can provide:• Medicine description• Formulary status• Co-pay information
Pharmacy receives E-Rx and fills after confirming eligibility/coverage. Patient picks up prescription at pharmacy when it is ready.
Patient Physician/NP/PA Pharmacy
A recent Surescripts® study showed a 10 percent increase
in patient adherence (i.e., new prescriptions that were
picked up by the patient) among E-prescribing physicians vs. non-E-
prescribing physicians.
3

SMG Proprietary Information
Why E-Prescribing is ImportantE-Prescribing has already made significant in-roads into key components of the pharmaceutical industry
4
Prescriptions
• 326 million Rxs were electronic in 2010; this was roughly 8% of all prescriptions in the US.
Prescribers
• 291,000 physicians had E-Prescribed by end of 2011; this was 52% of all office-based prescribers.
Pharmacies
• 94% of community pharmacies able to E-Prescribe by end of 2011.
4

SMG Proprietary Information
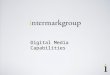
Why E-Prescribing is ImportantE-prescribing changes the way in which pharmaceuticals are distributed
5
Traditional Non-E-Rx Process
New E-Rx
Process
Rx
Adjudication of Rx
Rx
Adjudication of RxVia E-Rx System Reference
Fewer than 100 PBMs Coordinating Benefit Informationin the US
More than 1,000Software Companies Coordinating Benefit Info. by Installing E-Rx Systems
E-Rx Paradigm
Shift
5
Vs.

SMG Proprietary Information
Why E-Prescribing is ImportantThe E-Rx user interface will become the most frequent exposure to your brand with profound implications on how your product is used
6
• Alphabetization on drop-down menus could aid or harm the frequency of exposure to your brand’s name.
• Instant patient record access confirms how long a patient has been on a medication and can trigger a reassessment of treatment options and goals.
6

SMG Proprietary Information
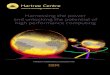
Why E-Prescribing is ImportantDue to penalty exemptions, 2011 may have represented an E-Rx lull; threat of a definite -1.5% Part B penalty in 2013 may re-accelerate E-Prescribing by end of this year
7
1 Many physicians applied for 2011 E-Rx exemption to avoid 2012 1% penalty.2 Incentives recorded in one calendar year are applied in the following calendar year. A physician needs to
submit 10 E-Rxs by June 30, 2012 to receive the 0.5% Part B rebate and avoid a -1.5% Part B penalty in 2013.
E-Prescribing Statistics Compared with Medicare Part B Incentives/Penalties
7
2009 2010 2011 2012 2013
Medicare Part B Incentive 2% 2% 1% 1% 0.5%
Medicare Part B Penalty1,2 0% 0% 0% -1% -1.5%
Increase in E-Rx Physicians from Previous Year
82,000 78,000 57,000 ? ?
Increase in E-Rxs from Previous Year
123 million 135 millionData To Be Released
Soon? ?

SMG Proprietary Information
Key E-Prescribing Issues to AssessIntegrate Current E-Rx Patterns with Opportunities
8
• Specialty? Age? Size of practice?
• Demographics of patients? Medicare population?
• Existence and use of electronic medical records (EMR) in practice?
• Provider of E-Rx system?
Available information in system:
• Formulary status? By health plan?
• Co-pays? Substitution options?
• Ability to override system defaults?
• Level of interest in bonuses/rebates from payers?
• Current revenues from bonuses/rebates from payers?
Sales Force Opportunities
• Facilitate physician interaction with pharmacy?
• Support physician interaction with system?
E-Rx Topics for
Research
Profile of High vs. Low
E-Rx’ers?
Degree of E-Rx Impact on Your
Product(s)?
Impact of Medicare/Payer
Incentives on Your Product’s
E-Rxs?
Opportunity for Your Brand in E-Prescribing?
8

SMG Proprietary Information
Qualitative In-Person Individual Depth Interviews Or Quantitative Web Surveys
Recruitment Criteria for Interview/Survey:
Currently employ an E-Prescribing system which sends prescriptions electronically to retail pharmacies.
Mix of E-Prescribing utilization levels.
Agree to conduct one or more “mock E-Rx” as part of the interview/survey process.
Meet standard screening criteria.
Interview/Survey Detail:
• SciMedica Group MR&C will conduct in-person interviews/web surveys.
‒ Each interview will last roughly 45-60 minutes.
‒ Each web survey lasts 30-60 minutes
‒ Respondents will go through one or more mock E-Rxs as part of the in-person interview or web survey.
Interviews by Target Segment:PCPs
SpecialistsNurses
PharmacistsIT/Office Managers
9
9

SMG Proprietary Information
Discussion Guide Flow
Capture E-Rxing adoption process• Entities and roles in decision process?
• Impact of changes in reimbursement/legislation?
Demonstration
Feedback
Capture current level of use of E-Rxing system• Comfort level and satisfaction with E-Rxing?
• How does the process work?
• Changed Rxing habits?
E-Rxing demonstration for a hypothetical patient using client-specific products• Step-by-step review of how to prescribe a client product in
the system.
Capture feedback on future utilization and opportunities• How might their use of E-Rxing change over the next year?
• Opportunities for manufacturers?
Adoption Process
Level of Use
10
10

SMG Proprietary Information
Sample E-Prescribing OutputSpecific Results for Your Product(s)
11
• Reported Formulary Status• Reported Co-pays• Availability of Substitutions• Existence of System Override• Variations by Health Plan
• Links to EMR Availability• Size of Practice• Medicare Population• Key Attitudes• Technology Skills
Summary for Your Product(s)
• Contracting Initiatives• Sales Force Initiatives• Marketing Initiatives
Key Opportunities Identified
Profile of E-Rx Levels forYour Product(s)
11

SMG Proprietary Information
Ted Felix President – SciMedica Group MR&C
Ted leads the Marketing Research and Consulting business unit at SciMedica Group with a successful track record of providing consultative marketing research and strategic planning services to the pharmaceutical and allied healthcare industries. He employs more than 20 years of experience in healthcare marketing research consulting to help clients answer their key strategic, business questions.
Prior to joining SciMedica Group Marketing Research and Consulting, Ted served over 10 years as a senior executive at one of the largest U.S.-based marketing Research and Consulting firms. Drawing on his extensive experience in pharmaceutical sales, field operations, and marketing research consultation, Ted has led strategy development workshops with global brand teams for a number of products across several therapeutic areas. He also served as a member of the faculty of a Marketing Seminar Series.
Ted is an active member of Pharmaceutical Marketing Research Group (PMRG), Council of American Survey Research Organizations (CASRO), and Pharmaceutical Business Intelligence Research Group (PBIRG). Ted co-presented the PMRG workshop, “Appraising Competitive Factors in a Changing Environment” at the 2006 PMRG national conference. He is also an active member of the PMRG Marketing Committee.
Ted holds a B.A. in Marketing and Business Management from Temple University.
12

SMG Proprietary Information
Eric G. John, MSSenior Vice President – SciMedica Group MR&C
Eric G. John has 18 years of healthcare industry analysis experience including 13 years experience in directing primary market research from both the client and supplier side in the pharmaceutical industry. His career includes management positions in marketing research management at Novo Nordisk Inc., Scott-Levin (now part of SDI Health), TVG, and The Mattson Jack Group. Mr. John recently published an article on e-prescribing in the August 2011 issue of Medical Marketing & Media magazine.
Mr. John’s areas of methodological expertise include post-launch market research (ATUs and Message Assessment studies) and prescription driver/in-licensing/opportunity assessments (trade-off studies). His treatment area experience includes research for products treating cardiovascular, endocrine, immunologic, neurological, ophthalmic, respiratory, and women’s health conditions. Mr. John has also developed and delivered seminars to train the pharmaceutical industry on the design and execution of marketing research studies for input into new product evaluations or as part of post-launch assessment.
He has an M.S. in Business Administration from Temple University and a B.A. in Economics from the University of Scranton.
13