Embed Size (px)
Citation preview
Mirzapur City
Program Implementation Plan
National Urban Health Mission
Prepared by District Health Officials with support from Urban Health Initiative

Contents 1- District Profi le- ..................................................................................................................................... 7
1.1 LOCATION, BOUNDRIES, AREA AND POPULATION ............................................................. 7
1.2 HISTORY OF THE DISTRICT AS AN ADMINISTRATIVE UNIT- ............................................ 8
1.3 SUBDIVISIONS, TEHSILS AND POLICE STATIONS .............................................................. 8
1.4 Blocks Name – ................................................................................................................................. 8
1.5-Block Position in the District—........................................................................................................ 9
1.6 District Mirzapur at A Glance ( Comparison of 2001 and 2011)................................................ 9
2- SITUATION ANALYSIS OF URBAN AREA MIRZAPUR.............. 10
2.1- Nagar Palika Mirzapur (Mirzapur and Vindhyachal city) ......................................................... 10
2.2-Population, Literacy Rate & Sex Ratio – Mirzapur City ............................................................ 11
2.3-Demographic profile of Mirzapur City .......................................................................................... 11
2.4-Nagar Panchayat Kachhnwa- ....................................................................................................... 11
2.5- Nagar panchayat chunar ............................................................................................................. 12
2.6- Nagar panchayat Ahraura ............................................................................................................ 12
2.7- Urban area Selected Under NUHM Programme-..................................................................... 12
2.8-Urban Poor & Slums of Mirzapur City- ........................................................................................ 13
2.9 -Map and Listing of Slums in Mirzapur as Per DUDA-.............................................................. 14
2.10- List of Slums- ............................................................................................................................... 14
2.11- Muslim populated areas- ............................................................................................................ 15
2.12 -Urban Governance ...................................................................................................................... 16
2.13- Urban Governance and Service delivery institutions............................................................. 16
2.14-Access to Public Facilities........................................................................................................... 17
2.15- Housing ......................................................................................................................................... 17
2.16- Housing Characteristics ............................................................................................................. 17
2.17- Water Resources......................................................................................................................... 18
2.18 Water Supply Indicators ............................................................................................................. 18
2.19 Sewerage and Sanitation Facilities............................................................................................ 18
2.20- Sewage Management (Sewerage and Sanitation) ................................................................ 18
2.21 -Drainage ....................................................................................................................................... 18
2.22-Solid Waste Management ........................................................................................................... 19

District Programme Management Unit, NRHM, Mirzapur Page 3
2.23- Solid Waste Management Indicators ....................................................................................... 19
3- Health Infrastructure in Mirzapur City_...................................... 19
3.1-First and Second Tier Health Services........................................................................................ 19
3.2- Health Structure in Mirzapur ........................................................................................................ 20
3.3-Private Health Care providers ...................................................................................................... 20
3.4-.Health Scenario- ............................................................................................................................ 21
3.5- Amenities and Living Conditions ................................................................................................ 26
3.6- Maternal Health............................................................................................................................. 26
3.7- Child Health ................................................................................................................................... 27
3.8- General Health & Health Seeking Behaviour........................................................................... 28
4- Key Issues .................................................................................... 29
4.1-Strategies, Activities and Work plan ............................................................................................ 30
4.2-Listing and Mapping of Households in slums and Key Focus Areas ..................................... 30
4.3-Facility Survey for gaps in infrastructure, HR, equipment, drugs and consumables ........... 31
4.4- -Activity Plan under NUHM for the state and cities .................................................................. 34
4.5-Programme Management Arrangements ................................................................................... 37
4.6-City Level Indicators & Targets .................................................................................................... 39

District Programme Management Unit, NRHM, Mirzapur Page 4
PREAMBLE
National Urban Health Mission aims to improve the health status of urban population in general and the
poor and other disadvantaged sections in particular. This would be made possible by facilitating equitable
access to quality health care through a revamped primary public health care system, targeted outreach
services and involvement of the community and urban local bodies. Under the scheme, the government
proposes to strengthen and enhance the health care service delivery in urban areas with targeted focus
on urban poor and the disadvantaged.
Mirzapur with a population of 2,496,970 (Census: 2011), is one of the Sixteen districts in Uttar Pradesh
(UP). In 2006 the Ministry of Panchayati Raj named Mirzapur one of the country's 250 most backward
districts (out of a total of 640). It is one of the 34 districts in Uttar Pradesh currently receiving funds from
the Backward Regions Grant Fund Programme (BRGF).
The current sex ratio for the urban areas is 869 females per thousand males which is an area of grave
concern. The AHS-2010-11 reports that institutional deliveries are around 55.8 % in the city and the IMR
is 83 % (AHS 2011-12) with MMR at 308 (AHS 2011-12) which again is a matter of concern. Complete
immunization status of the district is around 45.0% (AHS 2010-11) and if we see the 3+ANC, it is as low
as 25.1% (AHS-10-11) at the district level. Unmet need for family planning services at the district level is
28.5 (AHS-10-11) and if we further examine the data, 10.9 % is for limiting and 17.7 % for spacing
methods.
The health indicators for Mirzapur show are way behind in so many aspects and the launch of National
Urban Health Mission, the efforts for improving the health parameters will complement towards
betterment of urban population and in particular to the urban poor, muslims & slum dwellers.
The NUHM planning for this financial year is based under consideration of direction given by Govt. UP
vide letter.no. 1533/52-3-2013-sa(30) dated 24 August 2013 point No 10 through which 20% of Muslim
community must be benefitted by all activities under NUHM Programme. It is also based on the data,
surveys and available information at city level and hoping that we will initiate the process very
systematically so that we can make the difference in improvement of quality life of urban people specially
by reaching the unreached areas.
District Programme Management Unit, NRHM deserves a very special mention for providing generous
technical support in preparation of City PIP.
Dr. Umesh Singh Yadav Anil Dhingra
Chief Medical Officer/Secretery District Magistrate/Chiarman District Health Society District Health Society
Mirzapur Mirzapur

District Programme Management Unit, NRHM, Mirzapur Page 5
ACKNOWLEDGEMENT
Considerable efforts have been made by the team in preparing this Project Implementation Plan for Mirzapur under the newly announced National Urban Health Mission. This has been possible through dedication, perseverance and hard work. This exercise of planning would not
have been complete without the help and support of the team.
We do not have hesitation in saying that this work would not have come up without the valuable support and continuous encouragement of Shri Anil Dhingra (IAS), District Magistrate, Mirzapur. His great confidence in team and spurred us into action.
My special gratitude goes to Dr. Umesh Yadav, Chief Medical Officer, Mirzapur, a dynamic and
enthusiastic professional. He has always been a source of great encouragement for us. The initiation and completion of this work has been possible due to his sincere and able guidance, expertise, precious opinion, keen attention, constructive suggestions and constant help. His
critical reading of all the parts of the work has helped shape the NUHM planning in its present form.
I express my gratefulness to Shri. Amit Kumar Ghosh, IAS, Mission Director, National Health Mission & Mr. Shashank Vikram, IFS, Additional Mission Director, NUHM for overarching support and building the thoughts in our mind.
I owe my sincere gratitude to Dr. M. R. Gautam (General Manager), Dr. Usha Gangwar, (Deputy
General Manager-NUHM) and HUP-PFI who have helped us immensely by providing relevant information and valuable suggestions. This planning work got accomplished with their valuable support and eagerness to help.
I am privileged to have such good city level team especially Shri Omkar Singh (DCPM), Shri.
Rupesh Mishra (DDAM) and Shri Kamlesh Kumar Maurya (HMIS Operator) who have supported and helped in contributing their great efforts towards planning and compilation of Data for this city level plan under the NUHM.
I would also like to appreciate the precious help and motivation which I received from
government line department - DUDA, ICDS, Nagar Palika Parishad, Education department, CMS & DTO.
Last but not the least; I would like to thanks all those people who were involved in the planning process directly or indirectly.
Anil Kumar Mishra Dr. D.K. Singh
DPM, NRHM, Add. CMO (RCH), Mirzapur Mirzapur

District Programme Management Unit, NRHM, Mirzapur Page 6
Acronyms ANM Auxiliary Nurse Midwife ASHA Accredited Social Health Activist AWC Aanganwari Center AWW Aanganwari Worker BSGY Bal Swasthya Guarantee Yojna BSUP Basic services for urban poor BSA Basic Shiksha Adhikari CDPO Child Development Project Officer DH District Hospital DHS District Health Society DUDA District Urban Development Authority ICDS Integrated Child Development Scheme IDSMT Integrated Development of Small & Medium Towns IDSP Integrated Diseases Surveillance Program IHL Individual House level IMR Infant Mortality Rate KFA Key Focus Area LHV Lady Health Visitor LT Lab Technician MAS Mahila Arogya Samiti MMR Maternal Mortality Ratio NHM National Health Mission NPP Nagar Palika Parishad NPSP National Polio Surveillance Program NRHM National Rural Health Mission NUHM National Urban Health Mission OD Open Drainage RSAP Remote Sensing Application Center UA Urban Agglomeration UCHC Urban Community Health Center UFWC Urban Family Welfare Center UHI Urban Health Initiative UHP Urban Health Post UPHC Urban Primary Health Center SAM Severely acute Malnourishment

District Programme Management Unit, NRHM, Mirzapur Page 7
National Urban Health Mission- Programme Implementation Plan
Mirzapur 2013-14 1- District Profile-
According to the tradition , the name of this town,after which the district itself is named was
GIRZAPUR which in terms derives its name from the goddess Parvati (Girija) who
sacrificed hersel here in a vajna. Mirza, Vindhyavasini and Lakshmi are the other names of the
goddess whose temple exists at Vindhyachal. The present name of the district is derived
from goddess Lakshmi who emerged from the sea .
The word Mirza is formed from two words Mir meaning sea and ja meaning
outcome , with the dditional pur standing for town. It is also locally believed that the town
was founded by raja Nanner and was known as Girijapur,but later on it came to know as
Mirzapur .
The earliest mention of the town is found in the writings of Tieffenthaler, who drew up his
description of the country between 1760 and 1770. He mentioned it, under the name of
Mirzapur specially as a great mart. In the records of Jonathan Duncan, who was resident of
Varanasi, frequent mention is made of the place as Mirzapur.
1.1 LOCATION, BOUNDRIES, AREA AND POPULATION
The District of Mirzapur lies between the aralles of
23.52 & 25.32 North latitude and 82.7 and
83.33 East longitude. It forms a portion of the
Varanasi Division. On the north and north-east it is
bounded by the Varanasi district; on the south bounded
by district Sonbhadra. On the south west by the district of
Allahabad. The shape to the north and west is some what
irregular. In no direction, except for about 13 km. in the
north east where he Ganga separates the Tehsil of
Chunar from the district of Varanasi , has Mirzapur a natural frontier.
According to Central Statistical organisation the district of Mirzapur had an area of 4521
Sq.Km.
An official Census 2011 detail of Mirzapur, a district of Uttar Pradesh has been released by
Directorate of Census Operations in Uttar Pradesh. Enumeration of key persons was also done
by census officials in Mirzapur District of Uttar Pradesh.
In 2011, Mirzapur had population of 2,494,533 of which male and female were 1,312,822 and
1,181,711 respectively. There was change of 17.89 percent in the population compared to
population as per 2001. In the previous census of India 2001, Mirzapur District recorded
increase of 27.44 percent to its population compared to 1991.
The initial provisional data suggest a density of 561 in 2011 compared to 476 of 2001.

District Programme Management Unit, NRHM, Mirzapur Page 8
1.2 HISTORY OF THE DISTRICT AS AN ADMINISTRATIVE UNIT-
The District of Mirzapur, with the exception of the Villages namely Mowat, Merolatand,
Mahespur, Durjanipur, Mangarahi Deohat, Katra and Bamsaur received from Allahabad in 1861,
falls entirely within the tract of country once known as the province of Benaras. The sovereignty
of this was formally ceded to the East India Company in 1775 year the Nawab-vizir of Avadh;
but the tract itself was included in the zamindari of the raja of Benares and remained
in his actual possession until 1794, when Mahip Narayan Singh surrendered its control of the
Governor General of India by the agreement of 27th october of that year. It is not until
1830 that Mirzapur became a separate revenue jurisdiction of its own, because until that
year it had been included in Varanasi.
Mirzapur was then placed under a local collector of customs, the subdivisions
assigned to new collectorate being tappasChaurasi, Chhiyanve, Upraudh,Kon and
Sakteshgarh of pargana Kantit and other paragnas, Bhagwat Bhuili, Haveli, Chunar,uriat,
Sikhar,Agori, Barhar and Bijaigarh,Bhadohi,Kon and Majhwa were restored to Varanasi on the
protest of raja but were afterwards re-annexed to Mirzapur.At present Agori,Barharand
Bijaigarh are in Sonbhadra District however Bhadohi is in Sant Ravidas Nagar District.
There has been no change in the territorial limits of Mirzapur since 1833, revenue and judicial
administrations were made to coincide throughout the Benares province;but several when the
alternation have been made in the sub-divisional boundries since the tract came in to the
possession of the British.In 1801 every pargana and tappa, with a few exception had a
separate Tehsildar.
In 1804 it was resolved to abolish the office of Tehsildar in the Benares Province. In 1806,
tahsildars were established for tappas Chaurasi, Upraudh, Chhiyanvey Sakteshgarh and
Bhagwat at Chaurasi; and for pargnas Agori-Barhar and Bijaigarh (at present lies in onbhadra
District) at Kusancha.The first of the two tahsils created in 1809 corresponds to a great extent
with the present Mirzapur tahsil.Saketeshgarh and Bhagwat have been taken may from it and
kon and Majhwa added. To the tahsil which had its headquarters in 1809 at Kusancha, Singrauli
and Dudhi were added and the whole was for some time known as the Shahganj tahsil
(Now all these are in Sonbhadra District).
1.3 SUBDIVISIONS, TEHSILS AND POLICE STATIONS
At present the district Mirzapur has four tahsils, Namely Sadar (Mirzapur), Chunar, Marihan and
Lalganj for administrative point of view.
To reached the development at root level the Mirzapur district has 12 blocks and 15
thana which are as under-
1.4 Blocks Name –
Total no of blocks 12 distributed in 04 Tehsils A. Sadar Tehsil
1. Mirzapur (City), 2. Chhanbey,

District Programme Management Unit, NRHM, Mirzapur Page 9
3. Kon, B. Marihan Tehsil (on way to District Sonebhadra, UP) 1. Marihan, 2. Rajgarh 3. Pahari C. Lalganj Tehsil (on way to District Rewa in MP)
1. Lalganj. 2. Halia, D. Chunar Tehsil (on way to District Varanasi, UP)
1. Sikhar 2. Jamalpur 3. Narayanpur 4. Majhwan ,
1.5-Block Position in the District—
1.6 District Mirzapur at A Glance ( Comparison of 2001 and 2011)
Description 2011 2001
Area 4522 sq. kms
Geographical location Between 24.34 & 25.16 deg. North Latitude (AXANSH) and 82.05 & 83.11
deg East Longitude (DESHANTAR) Surroundings North: Sant Ravidas Nagar (Bhadohi)
West: Allahabad
East: Varanasi
South: Sonebhadra and Rewa District of Madhya Pradesh. Actual Population 2,496,970 2,116,042
Male 1,312,302 1,115,249
Female 1,184,668 1,000,793
Population Growth 18.00% 27.44%
Area Sq. Km 4,405 4,405
Density/km2 567 476
Proportion to Uttar Pradesh 1.25% 1.27%

District Programme Management Unit, NRHM, Mirzapur Page 10
Population
Sex Ratio (Per 1000) 903 897
Child Sex Ratio (0-6 Age) 902 929
Average Literacy 68.48 55.31
Male Literacy 78.97 69.59
Female Literacy 56.86 39.26
Total Child Population (0-6
Age)
410,621 425,405
Male Population (0-6 Age) 215,841 220,577
Female Population (0-6
Age)
194,780 204,828
Literates 1,428,683 935,101
Male Literates 865,837 622,631
Female Literates 562,846 312,470
Child Proportion (0-6 Age) 16.44% 20.10%
Boys Proportion (0-6 Age) 16.45% 19.78%
Girls Proportion (0-6 Age) 16.44% 20.47%
2- SITUATION ANALYSIS OF URBAN AREA MIRZAPUR
District Mirzapur has covered with Urban areas namely –
1- Nagar Palika Mirzapur
2- Nagar Panchayat Kachhnwa
3- Nagar panchay chunar
4- Nagar panchayat Ahraura
The Urban Population of Mirzapur District is 14 % in
comparison with Rural population as shown in Pie
diagramme.
The detailed demographic information is as follows-
Description Mirzapur District 2011 Mirzapur Urban 2011
Actual Population 2494533 58097 Male 1312822 30571
Female 1181711 27526 Population Decadal Growth rate 27.62 27.62
Density/km2 4522 sq. kms
Sex Ratio (Per 1000) 959
Child Sex Ratio (0-6 Age) 922 Average Literacy (%) 39.68 %
Male Literacy (%) 54.75 %
Female Literacy (%) 22.35 %
2.1- Nagar Palika Mirzapur (Mirzapur and Vindhyachal city)
Mirzapur and Vindhyachal city is governed by Municipal Corporation which comes under Mirzapur and
Vindhyachal Metropolitan Region. As per provisional reports of Census India, population of Mirzapur and
Vindhyachal in 2011 is 233,691; of which male and female are 125,003 and 108,688 respectively.

District Programme Management Unit, NRHM, Mirzapur Page 11
Although Mirzapur and Vindhyachal city has population of 233,691; its urban / metropolitan population is
245,817 of which 131,534 are males and 114,283 are females.
2.2-Population, Literacy Rate & Sex Ratio – Mirzapur City
Mirzapur and Vindhyachal City Total Male Female
Population 233,691 125,003 108,688
Literates 161,128 92,423 68,705
Children (0-6) 27,774 14,779 12,995
Average Literacy (%) 78.25 83.85 71.80
Sex ratio 869
Child Sexratio 879
2.3-Demographic profile of Mirzapur City
Total Population of city (in lakhs) 2.34 Source: Census 2011
Slum Population (in lakhs) 0.58 Source: DUDA
Slum Population as percentage of urban population 20.27
Number of Notified Slums 51 Source: DUDA
Number of slums not notified 0
No. of Slum Households 10334 Source: DUDA
No. of slums covered under slum improvement
programme (BSUP, IDSMT,etc.)
51
Number of slums where households have individual
water connections*
24
Number of slums connected to sewerage network* 3
Number of slums having a Primary school 175 Source: BSA Deptt.
No. of slums having AWC 51 Source: ICDS Mirzapur
No. of slums having primary health care facility 1 UHP
Total AWC in Urban Area 200
2.4-Nagar Panchayat Kachhnwa-
Kachhwa is a town and a nagar panchayat in Mirzapur district. It is located at 25.22°N 82.72°E. It has an
average elevation of 84 metres (275 feet). It is around 35 km. away from Mirzapur district H.Q.
As of 2011 India census Kachhwa had a population of 15,962. Males constitute 52.44% of the population
and females 47.56%. Kachhwa has an average literacy rate of 57%, lower than the national average of
59.5%: male literacy is 66%, and female literacy is 46%. In Kachhwa, 16% of the population is under 6
years of age.
Total Population of city (in lakhs) 0.16 Source: nagar panchay
Slum Population (in lakhs) 0.063 Source: DUDA
Slum Population as percentage of urban population 39.93
Number of Notified Slums 5 Source: DUDA
Number of slums not notified 0
No. of Slum Households 1103 Source: DUDA
No. of slums covered under slum improvement
programme (BSUP, IDSMT,etc.)
5

District Programme Management Unit, NRHM, Mirzapur Page 12
2.5- Nagar panchayat chunar
Chunar located in Mirzapur District of Uttar Pradesh state, India, is an ancient town. The railway tracks
passing through Chunar railway station leads to major destinations of India, including Howrah, Delhi,
Tatanagar and Varanasi. National Highway number 7 also passes through Chunar. It is connected to
Varanasi, the ancient and pilgrimage city also well known as Kashi or Benaras, by roads and rails.
Chunar is well known for its pottery work especially clay toys.
As of 2011 India census Chunar had a population of 40024. Males constitute 53% of the population and
females 47%. Chunar has an average literacy rate of 57%, lower than the national average of 59.5%:
male literacy is 66% and, female literacy is 47%. In Chunar, 16% of the population is under 6 years of
age.
Total Population of city (in lakhs) 0.400 Source: Census 2011
Slum Population (in lakhs) 0.099 Source: Census 2011
Slum Population as percentage of urban population 24.77
Number of Notified Slums 15 Source: DUDA
Number of slums not notified 0
No. of Slum Households 1531 Source: Census 2011
No. of slums covered under slum improvement
programme (BSUP, IDSMT,etc.)
15
2.6- Nagar panchayat Ahraura
Ahraura is a city and a municipal board in Mirzapur district in the Indian state of Uttar Pradesh. Aharaura
has many famous places from the point of view holyness as there is a temple situated in rocky mountain
and there is stone letter which is by Emperor Ashok.
As of 2011 India census Ahraura had a population of 27308. Males constitute 52% of the population and
females 48%. Ahraura has an average literacy rate of 52%, lower than the national average of 59.5%;
with 63% of the males and 37% of females literate. 18% of the population is under 6 years of age.
Total Population of city 234871 Source: Census 2011
Slum Population 98000 Source: Census 2011
Slum Population as percentage of urban population 24 %
Number of Notified Slums 7 Source: DUDA
Number of slums not notified 0
No. of Slum Households 1549 Source: Census 2011
No. of slums covered under slum improvement
programme (BSUP, IDSMT,etc.)
7
2.7- Urban area Selected Under NUHM Programme-
NUHM will cover the state capitals, district headquarters and all cities and towns having a population
more than 50,000 (as per census 2011) in a phased manner. Since the fund available for 2013-14 is
modest, the state/UT will need to prioritise cities/towns that are more vulnerable in terms of larger
proportion of slums and inadequate provision for primary healthcare services.

District Programme Management Unit, NRHM, Mirzapur Page 13
Hence in District Mirzapur only City Mirzapur cum Vindhyachal will cover under NUHM
Programme as it has a total population of 2.34 Lacks, which exceed min population of 0.50 lacks.
2.8-Urban Poor & Slums of Mirzapur City-
The UP Slum Areas (Improvement and Clearance) Act, 1962, considers an area a slum if the
majority of buildings in the area are dilapidated, are over-crowded, have faulty arrangement of
buildings or streets, narrow streets, lack ventilation, light or sanitation facilities, and are
detrimental to safety, health or morals of the inhabitants in that area, or otherwise in any respect
unfit for human habitation. It mentions factors such as repairs, stability, extent of dampness,
availability of natural light and air, water supply; arrangement of drainage and sanitation facilities
as considerations. Based on the definition, estimates of slum population vary, so much so that
the Census 2001 originally did not report any slums and then later revised its findings. DUDA
follows the definition as stated in the UP Slum Areas (Improvement & Clearance) Act 1962;
SUDA/UNCHS do not follow this definition but define poverty in terms of vulnerability as does
Oxfam.
DUDA’s estimation of slum population is a conservative increase over the Census estimation.
that There are 51 poor settlements in the city that can be categorized as slums - authorized and
unauthorized (map overleaf). This classification is on the basis of tenure. An authorized slum is
one where there is security of tenure with the cluster being either an outcome of a government
resettlement programme or being located on private/own land. Unauthorized settlements are
those that have emerged on available vacant plots, mainly railway land or on encroached areas.
Slum clusters on the riverbanks or on drains are classified as unauthorized. The most recent
information on slums available in Mirzapur is from DUDA Mirzapur and this plan has mainly
used this information, partly on the advice of SUDA. Other sources of information have been
cited mainly to point out the range in the available data that will impact the earmarking of
resources for this group. Approximately 58000 people are living in slums with few basic civic
amenities.
Table 5: Selected indicators of slum conditions in Mirzapur
Characteristic Percentage of people/families Water Supply Facilities 42.68%
Individual tap 38.84% Community tap 6.06%
Others Sanitation 47.12%
Individual toilet facility 20.98%
Community toilet facility 28.30% Others
Employment 9.78% Employed 7.97%
Unemployed 81.91% Self employed 41.68%

District Programme Management Unit, NRHM, Mirzapur Page 14
2.9 -Map and Listing of Slums in Mirzapur as Per DUDA-
2.10- List of Slums-
S. No. Name of Slums Population
1 Angarh Mahabir 936
2 B.D. Pokhara 974
3 Bagh Knjangir 1061
4 Barundha 911
5 Barho Imilia 762
6 Basahi 2037
7 Bathua 924
8 Bhatwa ki Pokhari 3533
9 Bisundarpur 1362
10 Chandradeepa 1918
11 Chota Mirzapur 1337
12 Chhoti Basti 746
13 Chorba Nala 172

District Programme Management Unit, NRHM, Mirzapur Page 15
14 Danghar 1557
15 Devpurva 2280
16 Dumrauli 552
17 Gaibee Ghat 798
18 Ganeshganj 1799
19 Ghurahoo Patti 1080
20 Gosain Talab 952
21 Imarti Talab 452
22 Imlaha 1269
23 Jalalpur 824
24 Jamunaiya 602
25 Jayarangiri Bagh 1286
26 Jogiyabari 371
27 Kajrahwa 885
28 kantit 426
29 Katwaroo ka Pura 775
30 Mahuaria 546
31 Mallahi Tola 608
32 Natwa 1173
33 Neebi 784
34 Ojhala 340
35 Prasab ka pura 707
36 Pakka Pokhara 1956
37 Packi Saraiya 1567
38 Purani Dasmi 843
39 Ramaipatti 2648
40 Rambagh 1627
41 Ranibagh 817
42 Ratanganj 555
43 Rukhad Ghat 827
44 Sabri 2082
45 Sakhaura 690
46 Mahant Shivala 768
47 Shivpura 567
48 Shukalha 759
49 Tarkapur 4078
50 Tedwa 700
51 Vindhyachal 874
The rapidly growing urban population poses great challenge to the efforts of the state
government towards improving the health of the urban poor.
2.11- Muslim populated areas-
As per Govt of UP guideline 20% Muslim Population must be cover in all developmental program
through which maximum Muslim community benefitted.

District Programme Management Unit, NRHM, Mirzapur Page 16
In city mirzapur following Major Muslim Slums and General pocket are present-
Sl No Muslim Locality Sl No Muslim Locality
1 BASAHI 9 Imarti Road 2 Bhatwa ki Pokhari 10 Hayat Nagar 3 Natwa 11 Rani Bagh 4 Sabari 12 Kaji Talab 5 Tarka Pur 13 Gosai Talab
6 Immabara 14 Gaurian 7 Ram Bagh 15 Pakki Sarai 8 Ghore Shahid 16 Gajia Tola
2.12 -Urban Governance
There are multiple agencies responsible for urban governance and provision and management
of infrastructure and services. While, the Mirzapur Nagar Panchayat (MNP), MIrzapur Jal Kal
Sansthan (MJKS), Mirzapur Development Authority (MDA) and UP Jal Nigam (UPJN) are the
key urban service providers, other agencies include the Housing Board, Central and State Public
Works Departments (CPWD and PWD), Transport Department, Industries Department and the
Department of Environment. There is significant overlap of roles and responsibilities and
fragmentation in service provision and management of infrastructure, which makes it difficult to
hold institutions accountable and to coordinate.
2.13- Urban Governance and Service delivery institutions
City Level
Mirzapur Nagar Panchayat
(MNP)
Local level governance; Primary Collection of Solid Waste; Maintenance of
Storm Water Drains; Maintenance of municipal roads; Allotment of Trade
Licenses under the Prevention of Food Adulteration Act; O&M of internal
sewers and community toilets; Street lighting; O&M of water supply and
sewerage assets; Collection of water tariff
MIrzapur Development
Authority (MDA)
Preparation of Master Plans for land use; Development of new areas as
well as provision of housing and necessary infrastructure
District Urban Development
Authority (DUDA)
Implementing agency for plans prepared by DUDA.
Responsible for the field work relating to community development –
focusing on the development of slum communities, construction of
community toilets, assistance in construction of individual household
latrines, awareness generation etc.
State Level
UP Jal Nigam (UPJN)
Water supply and sewerage including design of water supply and
sewerage networks. In the last two decades ‘pollution control of rivers’ has
become one of their primary focus areas
UP Awas Vikas Parishad
(UPAVP)
Nodal agency for housing in the state. Involved in planning, designing,
construction and development of almost all types of urban development
projects in the state. Autonomous body generating its own resources
through loans from financial institutions
UP State Transport
Corporation (UPSTC)
Provides intra-city and state wide public transport; maintenance of buses,
bus stands

District Programme Management Unit, NRHM, Mirzapur Page 17
Public Works Department
(PWD)
Construction of main roads and transport infrastructure including
construction and maintenance of Government houses and Institutions
State Tourism Department
(STC)
Promotion of tourism
Archaeological Survey of
India (ASI)
Maintenance of heritage areas and monuments
UP Pollution Control Board
(UPPCB)
Pollution control and monitoring especially river water quality and
regulating industries
Town and Country Planning
Department (TCPD)
Preparation of Town Plans including infrastructure for the state (rural and
urban)
Office of Commissioner
Vindhayachal Division
Coordination of activities of various institutions
2.14-Access to Public Facilities
Infrastructure development has not been commensurate with the growth of the city and there are
problems confronting the city in terms of access and coverage in key infrastructure sectors –
water supply, sewerage, housing, drainage, and transport. Overall service levels are inadequate
and the situation is worse for the urban poor.
2.15- Housing
Mirzapur has witnessed a radial growth – greater along the Kacchawa Road Majhawa Block,
Bisundarpur and Kantit City Block and Chunar Bajar Narayanpur Block in recent years, The
latter has not been factored into the Master Plan – the formal basis for Government panning.
Estimates of infrastructure requirements and population projections are therefore likely to be
conservative.
The position of the City as the only large urban centre amidst a number of small towns in the
surrounding districts makes it an attractive destination for job seekers and people in need of
education and health facilities. One of the features of the city’s growth has been an increase in
the number of slums but disagreements about the definition of slums and about data hamper
efforts to address service delivery challenges in these areas.
2.16- Housing Characteristics
INDICATOR %
Households living in a Pucca House (%) 88.7
Households living in a Owned House (%) 97.9
Households treating water to make it safer for drinking (%) 1.9
Households having access to toilet facility (%) 84.6
Households sharing toilet facility (%) 27.1
Households having access to electricity (%) 90.1
Households using Electricity (%) 86.1
Households using Firewood/Crop Residues/Cow Dung Cake (%) 42.9
Households using LPG/PNG (%) 54.1
Households having a separate Kitchen (%) 60.6
Households having Computer/laptop with or without Internet Connectivity (%) 10.1
Households having Telephone/Mobile (%) 77.1

District Programme Management Unit, NRHM, Mirzapur Page 18
2.17- Water Resources
Aside from water resource issues such as pollution of the River GANGA and the declining
quality of groundwater, Mirzapur carries a burden of old infrastructure and the absence of
metering makes it difficult to estimate costs and leakages. Information about assets in physical
and functional terms is also inadequate. Overlapping institutional roles make it difficult to hold
the institutions clearly accountable.
2.18 Water Supply Indicators
Water Supply Indicators
Coverage of water supply
connections (100%)
Per capita supply of water
(1351pcd)
Extent of metering of
water connection
(100%)
Continuity of
water supply (24
Hours)
63 158 0 5
2.19 Sewerage and Sanitation Facilities
Mirzapur has seen no major investment in sewage infrastructure after the proposals in the 1948
Sewage Master Plan. Taking into consideration the service latrines, latrines discharging into
nallas, existing public toilets and open defecation about 40% of the population do not have
access to adequate sanitation. Informal sewers connecting a few households and discharging
into nearby open drains are also seen. The existing main network therefore is for the most part
not able to handle additional load leading to the sullage being discharged directly into the River
GANGA In many places the sewers have been choked by the disposal of solid waste in them as
well as encroachment in sections. This does not allow complete cleaning of the network and
aggravates the problem of discharge.
The lack of current data and information on assets severely impacts planning. While in the newly
developed and developing areas, networks are being provided by developers, coordination with
the state planning process is tenous.
2.20- Sewage Management (Sewerage and Sanitation)
Sewage Management (Sewerage and Sanitation)
Coverage of toilets (100%) Coverage of sewage network
service (100%)
Adequacy of sewage treatment
capacity (100%)
68 57 100
2.21 -Drainage
While in general, the City is good drained, there are local pockets of water logging especially in
areas where the carrying capacity of the drains has been reduced either due to encroachment or
blockage. Such flooding has been observed in Tarka pur ,Kajrahwaha Pokhra and Ghurahu Patti
almost each year during rains. In the newly developed areas, while the developer is responsible
for the provision of internal surface water drainage, the linking of these drains to the larger local
drains and nallahs is neglected, causing waterlogging problems at some places. Maintenance of

District Programme Management Unit, NRHM, Mirzapur Page 19
drains is ‘reactive’ with the common practice to desilt the drains and dump the sludge near the
edge of the drains to dry out before lifting. In practice, sludge either gets blown away or ends up
in open drains.
Table 10: Storm Water Drainage IndicatorsStorm Water Drainage Indicators
Coverage of storm water drainage network (100%) Incidence of water logging/flooding (0%)
74 583
2.22-Solid Waste Management
The present solid waste management system is not synchronized. There are some pockets
where door-to-door collection has been introduced largely on the initiative of the local residents;
there is no system of collection, transportation and disposal nullifies efforts at the household
level. The numbers of existing waste depots are inadequate for the quantum of waste generated
and are also located far from the city, which encourages indiscriminate dumping. Behavioural
patterns pose health risks and therefore pose health risks for those working in this sector as well
as residents living around waste depots. The indiscriminate dumping results in garbage finding
its way back into sewers and contributing to their choking.
2.23- Solid Waste Management Indicators
Solid Waste Management Indicators
Household level coverage of solid waste management services (100%)
Extent of segregation of municipal solid waste (100%)
Extent of municipal solid waste recovered (80%)
41 53 4
3- Health Infrastructure in Mirzapur City_
Unlike in the rural areas, where the health department has a wide network of primary health care
facilities providing reproductive and child health services, the urban slums lack basic health
infrastructure and outreach services. Thus, they are often bypassed even by national
programmes providing immunization, safe motherhood and family planning services. The sparse
health coverage provided by health facilities like urban family welfare centers, health posts, and
maternity homes in cities is used more for emergencies and curative services. Often these
facilities are far from their service area, poorly staffed, with inadequate space and supply of
medicines and equipment. Urban local bodies like municipal corporations and nagar panchayats
are also expected to provide health care, but resource scarcity restricts them to only providing
sanitation services. NGOs and private trusts are also few and far between.
3.1-First and Second Tier Health Services
The Government of Uttar Pradesh has committed itself to make provisions for health care
services to its population. Though the efforts have been rural centric some efforts have also
been made to improve the delivery of primary health care services to the population living in
urban areas. It has established D Type health centers and dispensaries for providing family

District Programme Management Unit, NRHM, Mirzapur Page 20
welfare services and OPD facilities. The Urban Local bodies and Department of Health and
Family Welfare are the two main stakeholders for managing these services. In urban areas of
UP, first tier health services are available through D-type health centers, the family welfare
centre, health post and PP centers. Second tier health services are provided in urban areas
through District Male and Female or Combined Hospitals.
3.2- Health Structure in Mirzapur
Sl.
No.
Name & Type of
Facility (DH,
Maternity Home,
CHC, other ref.
hospital UFWC,
UHP,
PHC,Dispensary
etc.)
Managing
Authority
(Municipal
Council,
State Health
Department,
facilities
functioning
on PPP
basis)
Location of
Health
Facility
Population
Covered
by the
Facility
Services
Provided
Human
Resources
available
(List Type
and
Number of
HR
available
i.e. ANM,
LT, SN,
MOs,
Specialists
etc.
No. and
Type of
Equipment
Available
(X-ray
machine,
USG,
autoclave
etc.)
1. PPP NA Rambag,
Mirzapur
100000 RI, ANC,
PNC, NSV
MOs- 1
ANM- 2
NO
2. FWC NA Rambag
Mirzapur
RI, ANC,
PNC, NSV
ANM - 2 NO
3. Urban Helth
Post
NA Tarkapur
Mirzapur.
5078 RI, ANC,
PNC, NSV
MOs – 1
SN – 1
ANM – 1
Other Staff - 1
NO
The data given in the table above reveals inadequacy of primary health care services. The first
tier health facilities were planned for a population of 50000 but as a result of rapid population
growth they are currently serving a population of more than 75000. The situation gets
compounded due to lack of adequate infrastructure, equipments and medicines. The staff mainly
Doctors and ANM is also inadequate. The high population- staff ratio results in poor service
coverage with some areas being entirely unserved. From the above assessment it becomes
evident to consider the poor health indicators for deciding the norms of staff population ratio.
Uttar Pradesh has eight medical colleges and one post-graduate institute which offer tertiary and
superspecialty health services.
3.3-Private Health Care providers
A large network of private providers exists along with a large number of public sector providers.
The total number of private sector doctors is estimated at 500 (Registered and unregistered all
inclusive). The Dai’s (TBAs) are estimated at 450 (Trained and untrained) Commercial outlets
including medical shops, pharmacies etc. number about 150. Unlike the distribution of public
sector providers, the highest concentration of the private providers is in the western region. The

District Programme Management Unit, NRHM, Mirzapur Page 21
distribution of health providers understandably has strong bearing on the health care in U.P.
Regions with lower concentration of medical providers (in proportion to population) have lower
maternal and child health care coefficient and higher unmet need for family planning services.
3.4-.Health Scenario-
Based on the results of AHS the health scenario of Mirzapur city (proxy by the urban part of the
district) is presented as below. The detailed tables are given in the annexure.
Indicator %
Marrige below legal age (%)
Among females (below 18 Years) 16.7
Among males (below 21 Years) 27.8
CMW age ( 20-24 Years) married before age 18 years 51.2
CMM age ( 20-24 Years) married before age 21 years 52.9
Mean Age at Marriage
Male 22.7
Female 20.2
Morbidity and Health issues
Number of disable persons (1000,000 population)
Person 1607
Male 1692
Female 1519
Number of Injured Persons by type of Treatment received (Per 100,000 Population)
Severe
Person 155
Male 181
Female 127
Major
Person 278
Male 363
Female 190
Minor
Person 1453
Male 2054
Female 823
Persons Suffering from any kind of Acute Illness
(Per 100,000 Population)
Diarrhoea/Dysentery
Person 989
Male 1269
Female 696
Acute Respiratory Infection (ARI)
Person 309
Male 363

District Programme Management Unit, NRHM, Mirzapur Page 22
Female 253
Fever (All Types)
Person 5966
Male 6344
Female 5570
Any type of Acute Illness
Person 9645
Male 10695
Female 8544
Taking treatment from Any Source (%)
Person 95.5
Male 95.6
Female 95.6
Taking treatment from Government Source (%)
Person 3.0
Male 3.0
Female 3.1
Having Any kind of Symptoms of Chronic Illness
(Per 100,000 Population)
Person 8161
Male 7855
Female 8481
sought Medical Care (%)
Person 88.6
Male 89.2
Female 88.1
Diagnosed for (Per 100,000 Population)
Any kind of Chronic Illness
Person 1020
Male 846
Female 1203
Diabetes
Person 464
Male 725
Female 190
Hypertension
Person 1020
Male 846
Female 1203
Tuberculosis (TB)
Person 213
Male 181
Female 253
Asthma/Chronic Respiratory Disease
Person 711

District Programme Management Unit, NRHM, Mirzapur Page 23
Male 906
Female 506
Arthritis
Person 989
Male 785
Female 1203
Getting Regular Treatment (%)
Person 66.5
Male 71.6
Female 61.8
Getting Regular Treatment from Government Source (%)
Person 16.4
Male 17.0
Female 15.8
FERTILITY
Total Fertility Rate (TFR) 3.0
Women aged 20-24 reporting birth of order 2 & above (%) 33.3
birth of order 3 & above (%) 34.8
Women with two children wanting no more children (%) 71.3
Median age at first live birth of Women aged 15-49 years 22.7
Median age at first live birth of Women aged 25-49 years 22.3
Women age 15-19 who were already mothers or pregnant at the time of the survey
(%)
47.4
Mean number of children ever born to aged 15-49 3.0
Mean number of children surviving to Women aged 15-49 2.7
Mean number of children ever born to Women aged 45-49 4.1
Live Births taking place after an interval of 36 months (%) 43.5
ABORTION to EMW 15-49 Years (%)
Pregnancy resulting in abortion 6.7
Women who received any ANC before abortion 20.0
Married Women who went for Ultrasound before abortion 30.0
Average Month of pregnancy at the time of abortion 3.3
Abortion performed by skilled health personnel (%) 90.0
Abortion taking place in Institution (%) 70.0
Currently Married Pregnant Women aged 15-49 registered for ANC (%)
Current Usage
Any method (%) 51.0
Any modern method (%) 39.2
Female sterilization (%) 23.9
Male sterilization (%) 1.1
Copper-T/IUD (%) 4.5

District Programme Management Unit, NRHM, Mirzapur Page 24
Pills (%) 1.2
Condom/Nirodh (%) 8.4
Emergency Contraceptive Pills (%) .0.
Any traditional method (%) 11.8
Periodic abstinence (%) 4.5
Withdrawal (%) 1.8
LAM (%) 1.1
UNMET NEED FOR FAMILY PLANNING
Unmet need for Spacing (%) 11.4
Unmet need for Limiting (%) 11.2
Total Unmet need (%) 22.6
Maternal Health Care
ANTE NATAL CARE
Mothers who received any antenatal check-up (%) 86.7
Mothers who had antenatal check-up in first trimester (%) 55.0
Mothers who received 3 or more antenatal care (%) 40.0
Mothers who received at least one tetanus toxoid (TT) injection (%) 85.8
Mothers who consumed IFA for 100 days or more (%) 5.8
Mothers who had Full Antenatal Check-up (%) 5.8
Mothers who received ANC from Govt. Source (%) 56.7
Mothers whose Blood Pressure (BP) taken (%) 40.8
Mothers whose Blood taken for Hb (%) 26.7
Mothers who underwent Ultrasound (%) 29.2
DELIVERY CARE
Institutional Delivery (%) 55.8
Delivery at Government Institution (%) 25.0
Delivery at Private Institution (%) 30.8
Delivery at Home(%) 44.2
Delivery at home conducted by skilled health personnel (%) 25.5
Safe delivery *(%) 64.2
Caesarean out of total delivery taken place in Government Institutions (%) 13.3
Caesarean out of total delivery taken place in Private Institutions (%) 43.2
Less than 24 hrs. stay in institution after delivery (%) 38.8
Mothers who received Post-natal Check-up within 48 hrs. of delivery (%) 95.0
Mothers who received Post-natal Check-up within 1 week of delivery (%) 95.0
Mothers who did not receive any post-natal Check-up (%) 5.0
New borns who were checked up within 24 hrs. of birth (%) 90.0
JANANI SURAKSHA YOJANA (JSY)
Mothers who availed financial assistance for delivery under JSY (%) 25.3

District Programme Management Unit, NRHM, Mirzapur Page 25
Mothers who availed financial assistance for institutional delivery under JSY (%) 41.8
Mothers who availed financial assistance for government institutional delivery
under JSY(%)
93.3
IMMUNIZATION (%)
No of Children age 12-23 months 83.3
Children aged 12-23 months who have received BCG 83.3
Children aged 12-23 months who have received 3 doses of Polio vaccine 63.3
Children aged 12-23 months who have received 3 doses of DPT vaccine 63.3
Children aged 12-23 months who have received Measles vaccine 63.3
Children aged 12-23 months Fully Immunized 56.7
Children who have received Polio dose at birth 83.3
Children who did not receive any vaccination 13.3
Children Vitamin A dose during last six months 33.7
Children (aged 6 months) who received IFA tablets/syrup during last 3 months (%) 12.8
Children whose birth weight was taken (%) 63.0
Children with birth weight less than 2.5 Kg. (%) 11.3
CHILDHOOD DISEASES
Children suffering from Diarrhoea (%) 10.2
Children suffering from Diarrhoea
who received HAF/ORS/ORT (%)
84.6
Children suffering from Acute Respiratory Infection (%) 5.5
Children suffering from Acute Respiratory Infection who sought treatment (%) 100.0
Children suffering from Fever (%) 32.3
Children suffering from Fever who sought treatment (%) 100.0
Child Feeding practices and nutritional staus of children (%)
Children under 3 years breastfed within one hour of birth 40.7
Children (aged 6-35 months) exclusively breastfed for at least six months (%) 9.9
Water 84.9
Animal/Formula Milk 82.6
Semi-Solid mashed food 16.3
Solid (Adult) Food 9.3
Vegetables/Fruits 15.1
Average month of receiving foods other than other than breast milk for children
under 3 years
Water 2.3
Animal/Formula Milk 2.85.8
Semi-Solid mashed food 7.9
Solid (Adult) Food 6.2
Vegetables/Fruits
BIRTH REGISTRATION 59.8

District Programme Management Unit, NRHM, Mirzapur Page 26
Birth registered (%) 22.0
Children whose birth was registered and received birth certificate (%)
AWARENESS ON HIV/AIDS
Women who are aware of HIV/AIDS (%) 90.4
Women who are aware of RTI/STI (%) 98.00
Women who are aware of HAF/ORS/ORT (%) 99.6
Women who are aware of danger signs of ARI/Pneumonia (%) 97.3
3.5- Amenities and Living Conditions
About 97.9% households were living in their own houses. About 11% were still living in Kutcha
or Semi Pucca houses. Though almost all households had access to improved sources of
drinking water, but 1.9% only were treating water to make it safer.
Whereas 27.1% were sharing toilets, still about 15% were defecating in open. About 87% had
access to electricity. Though 54% were using LPG for cooking, 15% were still using fire
wood/dung cakes/ crop residues for cooking. As high as 90% had telephones/ mobiles and
10.1% even had computers.
3.6- Maternal Health
Fertility
The Total Fertility Rate for Mirzapur city was
estimated at 3.15 which is broadly equals mean
number of children ever born to women age 15-49
years. The births of order 3 and above were reported
by 34.8% only and women with 2 children and
wanting no more child was as high as 71.3%. Further
as high as 44% of births had interval of 36 months or
more. The girls marrying below the legal age of 18
years were only 2.3%. 53% reported using any family
planning method. The most common methods of
family planning were female sterilization - 17% and
condoms as 20%. The use of IUD was just 2.6% and
pills 4%. The traditional method was reported as
being used by 9%. The total unmet need for family
planning was 31%, 14.6% for spacing and 16.6% for limiting.
Ante Natal Care
Though mothers receiving any ante natal check up were 87%, only 40% had full ANC. Around
57% of pregnant women received ANC from Government sources. Of various components of
ANC, at least one TT received by 85.8%, BP taken 41%, blood examination for Hb 28%,
underwent ultrasound 29.2%. Though 40% pregnant women received 3 or more ANCs, those
who consumed IFA for 100 days or more was only 5.8%.

District Programme Management Unit, NRHM, Mirzapur Page 27
Delivery Care
About 56% of deliveries in Mirzapur were conducted in institutions, of which 25% were in
Government institutions and 43% in private institutions. The home deliveries were only 44% of
which 59% were conducted by skilled health personnel. Caesarian cases were as high as
43.2%, about two-third being conducted in private institutions.
It is important to note that because of high demand on beds for insti tutional deliveries, in about
39% of the cases the stay in the hospital after delivery was less than 24 hours. About 95.0%
mothers received post natal care and new born were also checked.
Importantly, 23.3% of mothers availed financial assistance for deliveries under JSY and 93.3% of mothers availed financial assistance for government institutional delivery.
3.7- Child Health
Child Immunization
About 63.3% of children were fully immunized. Those who received Vitamin A dose were33 %.
Birth Weight
In 63.0% cases birth weight of the child was taken and based on that 11.3% of children were low
birth weight (<2.5Kg). About 74% of births were registered and 68% had birth certificates.
Childhood Diseases
Children with diarrhea, Acute Respiratory Infection and fever were reported as 10%, 5.5% and
32.3% respectively. Those suffering from fever who sought treatment were 94%.
Brest Feeding
Only 10% of children were exclusively breast feed.
Infant & Child Mortality
The IMR was 83 per 1000 live births. The Neo Natal Mortality Rate was high at 60 and Post Neo
Natal at 23. Under 5 Child Mortality Rate was 111.
District Programme Management Unit, NRHM, Mirzapur Page 28
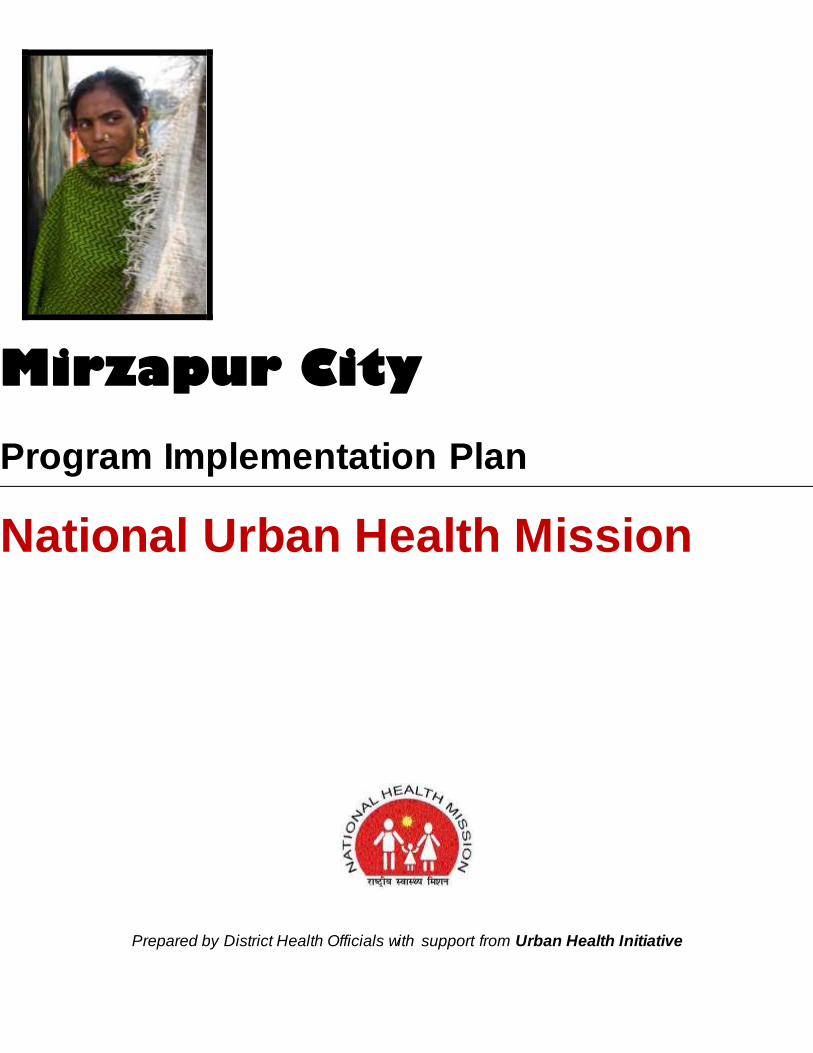
3.8- General Health & Health Seeking Behaviour
Morbidity
As per the AHS 2010-11, the morbidity rate for acute illness in Mirzapur was estimated at 3.6% it
being higher for females (3.7%) as compared to males (3.4%) as to the specific acute illnesses
the prevalence of fever was estimated at 2.5% (higher for females 2.7% compared to males
2.4%). The prevalence of Diarrhea/ dysentery was estimated at 0.4% for Acute Respiratory
Infection as 0.2%. It is observed that for acute illnesses 99% in Mirzapur took treatment of which
15% from government sources.
The symptoms related to chronic illnesses were reported by 4% in Mirzapur, it being significantly
higher for females (4.5%) as compared to males (3.6%). Of these about 94% were reported as
diagnosed. As to specific chronic illnesses Hypertension was reported by 1.6% and Diabetes by
1%. The prevalence for Hypertension lifestyle disease was higher among females as compared
to males. The problem of Arthritis and Asthma was reported by 0.5% and 0.2% respectively. The
problem of arthritis was much higher among females as compared to males. Tuberculosis was
reported more by males as compared to females, the prevalence being 0.16% in males. For
chronic illnesses 71% reported taking regular treatment of which 27% was from Government
Sources.
Injuries
Little less than 0.9% of the population had injuries due to accidents of which 20% were severe
where individual had to be kept in ICU and another 20% major requiring hospitalization.
Table 12: Disease/Cause of Morbidity Data : Mirzapur
Sl. Name of Disease/ Cause of Morbidity (e.g. COPD,
Trauma, Cardiovascular Disease etc.)
Number of cases
admitted in 2012 Source of Data
1 Injuries and Trauma 1895 IDSP
2 Self inflicted injuries/suicide 00
3 Cardiovascular Disease 1834 IDSP
4 Cancer (Breast cancer) 00
5 Cancer (cervical cancer) 00
6 Cancer (other types) 00
7 Mental health and depression 08 IDSP
8 Chronic Obstructive Pulmonary Disease (COPD) 2604 IDSP
9 Malaria 107 IDSP
10 Dengue 00
11 Infectious fever (like H1N1, avian influenza, etc.) 00
12 TB 478 TB Hospital
13 MDR TB 00
14 Diarrhea and gastroenteritis 11318 IDSP
15 Jaundice/Hepatitis 17 IDSP
16 Skin diseases 00
17 Severely Acute Malnourishment (SAM) 00

District Programme Management Unit, NRHM, Mirzapur Page 29
18 Iron deficiency disorder 42 IDSP
19 Others 00
(Source: IDSP, TB Hospital)
The above table reflects the health/ morbidity profile of the Mirzapur city. As there are three
sources of data, the city planning team has approached all three sources for getting most
authenticated as well as updated data. So, data from IDSP, TB clinic and District hospital were
taken and mentioned in the above table.
4- Key Issues
The Eleventh Plan had suggested Governance reforms in public health system, such as
Performance linked incentives and Devolution of powers and functions to local health care
institutions and making them responsible for the health of the people living in a defined
geographical area. NRHM’s strategy of decentralization, PRI involvement, integration of vertical
programmes, inter-pectoral convergence and Health Systems Strengthening has been partially
achieved. Despite efforts, lack of capacity and inadequate flexibility in programmes forestall
effective local level Planning and execution based on local disease priorities.
In order to ensure that plans and pronouncements do not remain on paper, NUHM UP would
strive for system of accountability that shall be built at all levels, reporting on service delivery
and system, district health societies reporting to state, facility managers reporting on health
outcomes of those seeking care, and territorial health managers reporting on health outcomes in
their area. Accountability shall be matched with authority and delegation; the NUHM shall frame
model accountability guidelines, which will suggest a framework for accountability to the local
community, requirement for documentation of unit cost of care, transparency in operations and
sharing of information with all stakeholders. The state will incorporate the core principles of The
National Health Mission of Universal Coverage, Achieving Quality Standards, Continuum of
Care and Decentralized Planning.
Following would be the issues for the cities to address: City Health Planning, Public Private
Partnership, Convergence, Capacity Building, Migration, Communitization, Strengthen Data,
Monitoring and Supervision, Health Insurance, Information Dissemination and Focus on NCDs/
Life-Style Diseases.
After considering the available data, city scenario and analysis, the City planning team has
identified issues at both service delivery & demand generation level. Following are the details of
issues which would be addressed through NUHM at the city level:
Need of community volunteers (ASHAs) for taking up the community mobilization activities
Need of Mahila Arogya Samiti (MAS- a group of 10-12 women) for wider spread of
information/ rights and entitlements
Strengthening of ANC, PNC & identification of high risk pregnancies at community level
Home based care of neonates at community level.
Promotion of institutional deliveries
Health education for all, especially for adolescent group
Complete immunization of pregnant women & children
Needs to strengthen the existing health care facilities by recruiting human resources

District Programme Management Unit, NRHM, Mirzapur Page 30
Need assessment of community in health scenario
Need a better convergence with other programs and wider determinants
Need of training & capacity building of human resources
Need of Strengthened program management structure at district level
Need of intensive baseline survey to start the community processes and identifying local
needs
Involvement of local bodies in decision making and managing the program locally
Gap analysis of HR & recruitment
Promotion of family planning methods through basket of choice approach & counselling
because unmet need for family planning is high in Mirzapur
Management of communicable & non- communicable diseases
Strengthening AYUSH
Constitution of BSGY team for urban areas.
Identification & management of SAM children
4.1-Strategies, Activities and Work plan
The key overarching strategies under NUHM for 2013-14 include data based planning,
strengthening of management and monitoring systems at the state and district level, improving
the primary health care delivery system and community outreach through ASHAs, MAS and
Urban Health and Nutrition Days(UHNDs).
The key activities at the district level will include convergence with key urban stakeholders,
sensitization of ULBs on their role in urban health, strengthening UPHCs for provision of primary
health care to urban poor, community outreach through selection, training and support to ASHAs
and MAS, conducting UHNDs and outreach camps to get services closer to the community and
reach complete coverage of slum and vulnerable populations.
With the aim to improve the health parameters of urban population in the city, structures and
strategies as recommended for the NUHM in its framework will be adopted and operationalized
rapidly over the years.
4.2-Listing and Mapping of Households in slums and Key Focus Areas
Listing and mapping of households will provide accurate numbers for population their family size
and composition residing in slums. Currently, estimates of population residing in slums are
available from District Urban Development Agency (DUDA) and National Polio Surveillance
Project as the immunization micro plans (under NPSP) provide updated estimates of slum and
vulnerable populations and are expected to be fairly complete. The current plan for covering
slums is based on the currently available data of urban population of each city.
Once the ASHA are deployed they will list all households and fill the Slum Health Index
Registers (SHIR) including the number and details of family members in each household. This
data will be compiled for city and will provide the population composition of slums and key focus
areas. This will also help the urban ASHA know her community better and build a rapport with
the families that will go a long way in helping her advocate for better health behaviours and link

District Programme Management Unit, NRHM, Mirzapur Page 31
communities to health facilities under the NUHM. It is expected that once the household
mapping is completed in cities, the number of ASHAs will be reviewed and adjusted upwards or
downwards and the geographical boundaries of the coverage area for each ASHA would be
realigned. This is due to the reason that the actual population may be higher or lower than the
original estimate used for planning.
4.3-Facility Survey for gaps in infrastructure, HR, equipment, drugs and consumables
Facility survey will be carried out in the public facilities to assess the gaps in infrastructure,
human resource, equipment, drugs and consumables availability as against expected patient
load. Further planning, particularly for UCHCs, will be based on these gaps. This work will be
outsourced to a research agency. Development Partners like Health of the Urban Poor project
will technically support this effort.
Baseline Survey
The state envisions monitoring progress in health indicators in urban areas and among urban
poor over the period of implementation of NUHM. This proposed Baseline survey will generate
data on the health and related indicators which will be reviewed during the course of
implementation of the program to assess the impact of implementation and necessary course
corrections can accordingly be made and use of resources can be optimised.
Training and Capacity Building
ULB, Medical and Paramedical staff, Urban ASHAs and MAS will be trained. The trainings will
have to be followed by periodic refresher trainings to keep these frontline health workers
motivated. NUHM will engage with development organisations to develop the training modules
and facilitate the trainings.
Monitoring & Evaluation
The M&E systems would also capture qualitative data to understand the complexities in health
interventions, undertake periodic process documentation and self evaluation cross learning
among the Planning Units to be made more systematic.
The Monitoring and Evaluation framework would be based on triangulation of information. The
three components would be Community Based Monitoring, HMIS for reporting and feedback and
external evaluations.
Strengthening of health facilities
Urban - Primary Health Centre (U-PHC) –
During the first year of implementation of the program, the existing 1 urban health posts situated
at Tarka Pur Slum area will be attempted to be strengthened. Towards this, the UHPs existing

District Programme Management Unit, NRHM, Mirzapur Page 32
in rented accommodations will be shifted to adequately larger premises which would help in
rendering the mandated services.
There is a total population 2.34 lack out which 51 Slums as well as 16 Major Muslim
Pockets in City Mirzapur.As per NUHM guideline it will cover the state capitals, district
headquarters and all cities and towns having a population more than 50,000 (as per census
2011) in a phased manner. In the Year 2013-14 a Total No of 4 urban PHC’s will established at
Mirzapur City preferably in following places where maximum Muslim community and Slums are
Located-
Sl NO UPHC No Proposed Location
1 UPHC 1 Bhatwa ki Pokari 2 UPHC 2 Sabri
3 UPHC 3 Pakka Pokhra 4 UPHC 4 Natwa
A provision of Rs. 10,000/- per month per UPHC is being proposed for immediate service
provision capacity enhancement, but over the period of time the said rented accommodations
will be shifted to owned premises for sustained services. Accommodations belonging to other
stakeholder government line departments will be explored and then adopted after entering into
necessary agreements/ arrangements with the said department.
Targeted intervention for urban poor –
The process of listing of households in the KFAs, mapping of KFAs and health facilities and
baseline survey of the KFA households will help determine the scope and extent of services
required for targeting of the urban poor. A deliberate effort will be made to identify the vulnerable
poor on the basis of their residence status, occupational status and social status, besides other
micro-level indicators, which will further help focusing the health care services to the most
deserving.
Mahila Arogya Samiti (MAS)-
MAS will act as community based peer education group in slums, involved in community
mobilization, monitoring and referral with focus on preventive and promotive care, facilitating
access to identified facilities and management of grants received. Existing community based
institutions could be utilized for this purpose. City planning team is proposing formation of only
one MAS under each ASHA in the first year and the identification of the remaining planned MAS
will be undertaken in the subsequent years.
ASHA-
For reaching out to the households ASHAs (frontline community worker) would serve as an
effective and demand–generating link between the health facility and the urban slum population.

District Programme Management Unit, NRHM, Mirzapur Page 33
Each link worker/ASHA would have a well-defined service area of about 1000-2,500
beneficiaries/ between 200-500 households based on spatial consideration.
Outreach services –
Outreach services will be provided to the slum areas and KFAs through ANMs who would be
responsible for providing preventive and promotive healthcare services at the household level
through regular visits and outreach sessions. Each ANM will organize a minimum of one routine
outreach session in her area every month.
Special outreach sessions (for slum and vulnerable population) will be organized once in a week
in partnership with other health professionals (doctors/ pharmacist/ technicians/ nurses –
government or private). It will include screening and follow-up, basic lab investigations (using
portable /disposable kits), drug dispensing, and counselling. The outreach sessions (both routine
and special outreach) could be organized at designated locations mentioned in the aforesaid
paras in coordination with ASHA and MAS members
Innovations –
An urban specific IEC strategy covering urban contexts would be developed, field tested and
then applied to cover RCH. The IEC plans should especially focus on interpersonal or group
communication which would include a description of expected behaviour change in different
community segments. For effective tracking of its implementation, benchmarks and milestones
would be developed.
School Health Services
School health program under NUHM has been an important component to provide not only the
preventive and curative services to children but also to ensure their contribution in overall health
development of the urban communities. It is envisaged that the active involvement of children in
the program will enable them to be a change agent for themselves as well as communities by
taking home good knowledge and practices in terms of preventive health care activities. It is
planned that children will be engaged through innovative and creative actions to make the
learning entertaining and educational.
Objective: To evolve innovative ways to involve children in preventive health care activities to
make them a change agent for them and their families.
Innovation: An activity called SEEKH (Systematic Effort to Ensure Knowledge on Health) will be
implemented in each urban government school for active involvement of children based on two
way education and learning package.
Process: To ensure the participation of each and every children in proposed activity, the
following process and flow is planned and will be implemented:

District Programme Management Unit, NRHM, Mirzapur Page 34
A small booklet on primary health information will be developed (or leveraged from SALONI
program) for school going children.
The school health team will distribute the booklet to students during their visit to schools and
children will have to read the booklet in 45 minutes (we can call it SWASTHYA CLASS).
The reading will be followed by filling up a small questionnaire in 15 minutes
All the students participating in the activity will receive a batch with tagline “Member-Baal
Swasthya Sena”.
The three top scorer children will be rewarded as “Nayak-Baal Swasthya Sena” and will be
known as class monitor till the next round
These three will be responsible to ensure that all students are aware about mentioned good
health practices
They will also follow up with students that they are talking these points at their households and
practicing good practices (such as Hand wash, Personal hygiene etc)
PPP & CSR –
For Mirzapur city a few innovative interventions have been planned. Interventions performed
under Public Private Partnership (PPP) arrangements and Corporate Social Responsibiltoy
(CSR) will be undertaken with the intent to evolve successful models for health care delivery to
the urban poor.
Convergence –
Intra-sectoral convergence is envisaged to be established through integrated planning for
implementation of various health programmes like RCH, RNTCP, NVBDCP, NPCB, National
Mental Health Programme, National Programme for Health Care of the Elderly, etc. at the city
level. Inter-sectoral convergence with Departments of Urban Development, Housing and Urban
Poverty Alleviation, Women & Child Development, School Education, Minority Affairs, Labour
will be established through city level Urban Health Committees headed by the Municipal
Commissioner/ Deputy Commissioner/ District Collector.
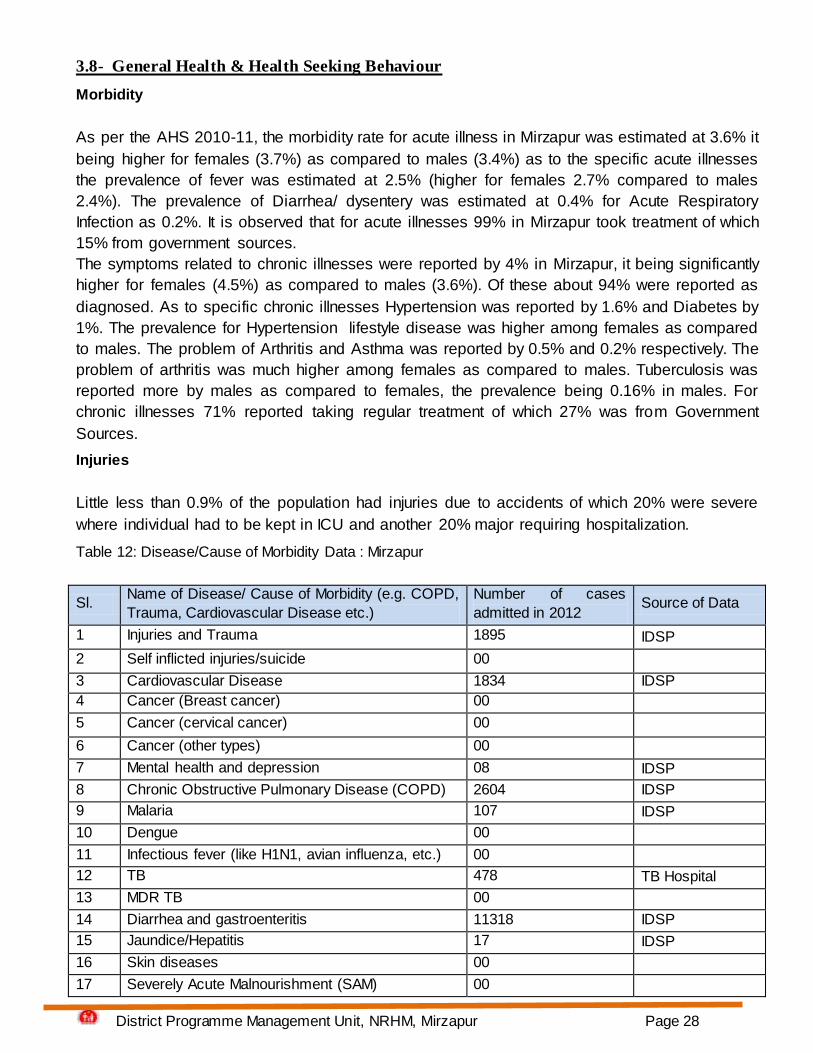
4.4- -Activity Plan under NUHM for the state and cities
Act.
No. Activity
Responsibility Months : October'13 - March'14 Remark
s
State
level
City
level Oct.
Nov.
Dec
Jan
Feb
Mar
1
Establishment of Platform for
Convergence at state level
Circular
to be
isued
from
state
level to

District Programme Management Unit, NRHM, Mirzapur Page 35
Act.
No. Activity
Responsibility Months : October'13 - March'14 Remark
s
State
level
City
level Oct.
Nov.
Dec
Jan
Feb
Mar
all their
district
level
nodal
officers
2
Preparation & Finalization of
Guidelines for City Coord.
Committee/ City Program
Management Committee
These
will be
one time
activities
and will
apply
across
the state
3 Preparation & Finalization of
Guidelines for Urban ASHAs
4 Preparation & Finalization of
Guidelines for Mahila Arogya Samiti
5 Preparation & Finalization of
Guidelines for UHND
6
Preparation & Finalization of
Guidelines for Outreach sessions/
School Health Programs
7
Preparation & Finalization of Job
Descriptions for all district level
NUHM positions
8 Preparation & Finalization of
Guidelines for PPP
9 Induction of state level staff for
Urban Health Cell
10 Induction of city level staff for Urban
Health program
11
Meeting of DHS for establishment
of City Program Management
Committee (UH)
12 Sensitization of new probable
members on NUHM
13 Identification of NGOs for their role
under NUHM
14
Establishment & orientation of City
Program Management Committee
(UH)
15
Identification of groups, collectives
formed under various govt.
programs (like NHG under SJSRY,
self help groups etc.) for MAS

District Programme Management Unit, NRHM, Mirzapur Page 36
Act.
No. Activity
Responsibility Months : October'13 - March'14 Remark
s
State
level
City
level Oct.
Nov.
Dec
Jan
Feb
Mar
16
Organize meetings with women in
slums where no groups could be
identified
17 Formation and restructuring of
groups as per MAS guidelines
18 Orientation of MAS members
18 Selection of ASHAs
18a - Selection of local NGOs for
ASHA selection facilitation
18b - Listing of local community
members as facilitators by NGOs
18c - Listing of probable ASHA
candidates and finalize selection
19 Convergence meeting with govt.
Stakeholders
20 Mapping & listing exercise (for
health facilities and slums)
20a
- Mapping of all urban health
facilities (public & pvt.) for services
To
continue
in 2014-
15
20b
- Mapping of slums (listed and
unlisted)
To
continue
in 2014-
15
20c
- Houselisting of slums/ poor
settlements
To
continue
in 2014-
15
21 Planning for strengthening of health
facilites/ services
- Health Facility Assessment (of
public facilities including listing of
public facility wise infra & HR
requirement)
To
continue
in 2014-
15
22 Baseline survey of urban poor/
District Programme Management Unit, NRHM, Mirzapur Page 37
Act.
No. Activity
Responsibility Months : October'13 - March'14 Remark
s
State
level
City
level Oct.
Nov.
Dec
Jan
Feb
Mar
slums (KFAs)
(to determine vulnerability,
morbidity pattern & health status)
23 Meetings of RKS for all the public
health facilites under NUHM
24
Identification of alternate/ suitable
locations for UPHCs under various
urban devp. Programs
To
continue
in 2014-
15
25 Strengthening of public health
facilities
- Selection, training and
deployment of HR in pub. health
facilities
To
continue
in 2014-
15
26 IEC activities
27 Outreach camps & UHNDs (from
existing UHPs)
28
Empanelment of Private Health
Facilities for health care
provisioning
To
continue
in 2014-
15
29 Involvement of CSR activities
4.5-Programme Management Arrangements
Districts Heath Society will be the implementing authority for NUHM under the leadership of the
District Magistrate. District Program Management Units have been further strengthened to
provide appropriate managerial and operational support for the implementation of the NUHM
program at the district level.
After extensive deliberations the state plans to designate the District Health Society under the
chairmanship of the District Magistrate as the implementing authority for NUHM

District Programme Management Unit, NRHM, Mirzapur Page 38
Fund flow mechanisms have been set up and separate accounts will be opened at in the district
for receiving the NUHM funds.
Urban Health will be included as a key agenda item for review by the District Health Society with
participation of city level urban stakeholders.
An Additional / Deputy CMO has been designated as the nodal officer for NUHM at the district
level. The District Program Management Unit will co-opt implementation of NUHM program in
the district and the District Program Manager will be overall responsible for the implementation
of NUHM. To support this the following additional staff and funds are proposed for strengthening
the District Program Management Units for implementing NUHM:
Urban Health Coordinator, Accountant and Data Entry Operators according to the following norms:
District total Urban population Additional Staff Proposed
1lakh to 10lakhs
1 Urban Health Coordinator,
1 Accountant
1 Data Entry Operator
District Programme Manager will be nodal for all NUHM activities so extra incentive and budget
for 1 laptop to each DPM has been proposed for DPM for undertaking NUHM activities.
A onetime expense for computers, printer and furniture for the above staff has been budgeted
along with the recurring operations expenses.
Onetime expenses have been budgeted for up-gradation of the office of Additional/ Deputy CMO
and District Programme management Unit.
The City Program Management Committee will function as an Apex Body for management of the
City
Health Plan, which will lead to delivery of Maternal, Newborn, Child Health and Nutrition
(MNCHN) and water, sanitation and hygiene (WASH) services to the urban poor and will work
towards the following objectives:
Establish a forum for convergence of city level stakeholders for the delivery of MNCHN and
WASH services to the urban poor.
Serve as the nodal body for the planning and monitoring of MNCHN and WASH service delivery
to the urban poor.
Provide a forum for exploring, reviewing and approving PPP initiatives and innovations to
address the gaps in MNCHN and WASH service delivery to the urban poor.
The structure proposed for the City Coordination Committee :
Chairperson - DM/ Municipal Commissioner
Convener - CMO
Members – Health - ACMO-Urban
Member- NRHM - DPM, NRHM
Member – ICDS - CDPO
Member – Nagar Nigam - Sum Improvement Officer
Member – Water & Sanitation- Sup. En. / Ex.En. JalKal Vibhag, Nagar Nigam
Member DUDA & UD - Project Officer

District Programme Management Unit, NRHM, Mirzapur Page 39
Members – School Education - BSA & DIOS
Members – Dev. Partners - Partners working in urban health sector ( HUP)
Coordinator - Lead Dev. Partner
Review Meetings at UPHC and City Level
Nature of Meeting Periodicity Meeting
Venue
Participants
Mahila Aarogya Samiti
Meeting
Once a month for
each MAS
Slum ANM, HV, Community Organizer,
Social Mobilization officer
Review meeting with Link
workers and MAS
representatives
Once a month UPHC All ANMs, PHN, LMO, Community
Organizer, Social Mobilization officer
Meeting of UPHC
Coordination Committee
Once a month UPHC LMO, PHN/Community Organizer,
Social Mobilization officer,
representative from 2nd tier facility,
and reps. From other departments
Meeting with CMO & UH
Program Coordinator
Once a month CMO
Office
CMO, Program Coord., Asst.
Program Coordinator, LMO/ PHN/
Community Organizer, Social
Mobilization officer
City Task Force Meeting Once in two
months
DM’s
office
CMO, Program Coord. UH, Various
departments’ reps. , private partners,
NGOs
4.6-City Level Indicators & Targets
Indicators Baseline (as
applicable)
Number
Proposed
(2013-14)
Community Processes
1. Number of Mahila Arogya Samiti (MAS) formed * 0 60
2. Number of MAS members trained * 0 600

District Programme Management Unit, NRHM, Mirzapur Page 40
3. Number of Accredited Social Health Activists (ASHAs) selected
and trained * 0 30
Health Systems
4. Number of ANMs recruited * 0 18
5. No. of Special Outreach health camps organized in the slum/HFAs
* 0 8
6. No. of UHNDs organized in the slums and vulnerable areas * 0 58
7. Number of UPHCs made operational * 0 4
8. Number of UCHCs made operational * 0 00
9. No. of RKS created at UPHC and UCHC * 0 4
10. OPD attendance in the UPHCs 0 3000
11. No. of deliveries conducted in public health facilities 0 500
RCH Services
12. ANC early registration in first trimester 1500
13. Number of women who had ANC check-up in their first trimester of
pregnancy 1500
14. TT (2nd dose) coverage among pregnant women 1500
15. No. of children fully immunised (through public health facilities) 00
16. No. of Severely Acute Malnourished (SAM) children identified and
referred for treatment 00
Communicable Diseases
District Programme Management Unit, NRHM, Mirzapur Page 41
17. No. of malaria cases detected through blood examination 00
18. No. of TB cases identified through chest symptomatic 00
19. No. of suspected TB cases referred for sputum examination 00
20. No. of MDR-TB cases put under DOTS-plus 00
Non Communicable Diseases
21. No. of Diabetes cases screened in the city 00
22. No. of Cancer cases screened in the city 00
23. No. of Hypertension cases screened in the city 00