Embed Size (px)
Citation preview
Document name:
Diarrhoea Policy
Document type:
Policy
What does this policy replace?
IPC policies which previously belonged to Care Services Direct have been harmonised with existing SWYPFT policies to reflect the needs of the whole organisation.
Staff group to whom it applies:
All staff within the Trust
Distribution:
The whole of the Trust
How to access:
Intranet
Issue date:
January 2015
Next review:
January 2018
Approved by:
Executive Management Team
Developed by:
Infection Prevention and Control Team
Director leads:
Director of Nursing, Clinical Governance and Safety acting as Director of Infection Prevention and Control
Contact for advice:
Infection Prevention and Control Team 01924 32 7063 / 32 7147 01226 43 3363 / 43 3364

2
Diarrhoea Policy Index Section
1. Introduction 3
2. Purpose and scope of this policy 3
3. Definitions 4
4. Duties 4 5. Principles 10 6. Equality Impact Assessment 10 7. Dissemination and implementation arrangements (including training) 10 8. Process for monitoring compliance and effectiveness 11 9. Review and revision arrangements (including archiving) 13 10. References 13 11. Associated documents 14 12. Appendices 15
12.1: clinical information
1. Management of an inpatient with diarrhoea 2. Care of affected individuals within the home environment 3. Side room escalation procedure 4. The Bristol Stool Form Scale 5. Inter-healthcare infection control transfer form 6. Diarrhoea / Clostridium difficile flow chart 12.2. Equality Impact Assessment 12.3. Checklist for the Review and Approval of Procedural Document 12.4. Version control sheet

3
Diarrhoea Policy 1. Introduction Diarrhoea is defined as an increase in stool liquidity usually accompanied by increased frequency of bowel motion. It can be a life threatening event and requires careful monitoring to prevent complications. Infectious diarrhoea may be caused by many different bacterial, viral and parasitic enteric agents. It may be accompanied by other symptoms, including fever, dehydration, electrolyte imbalance, and skin excoriation 1.1. Transmission The micro organisms that cause gastro intestinal infection are spread mainly from person to person following contact with faeces or cross infection. Viruses, particularly Noro-virus, are transmitted easily from person to person through aerosols and environmental contamination. 1.2. Diagnosis Diagnosis All diarrhoea stool samples from hospital patients aged >2 years, all community service users aged >65 years, and from community service users aged <65 years, wherever clinically indicated
will be tested for Clostridium difficile. All samples are sent for culture and sensitivity testing, which will identify other diarrhoeal pathogens including Campylobacter, Salmonella and other infections. During periods of increased incidence of diarrhoea in communal settings, tests for Norovirus may be requested by the Consultant Microbiologist or Consultant Communicable Disease Control (CCDC) Public Health Agency. 1.3 Identification of need To reduce organisational risk, the policies of Care Services Direct, which now forms the Barnsley BDU, needed to be harmonised with those of South West Yorkshire Partnership Foundation Trust (SWYPFT) to recognise service provision changes. This policy is intended to meet the needs of the organisation as a whole. 2. Purpose and Scope of the Policy The Trust has a legal requirement to comply with national external compliance standards, including the Health and Social Care Act (DH 2008): Code of Practice on the prevention and control of infection. This states that the policy should make provision for:
diagnostic criteria;
isolation of infected service users and cohort nursing;
environmental decontamination;
antibiotic prescribing policies; and
contraindication of anti-motility agents.

4
This policy outlines the strategic arrangements for the prevention and control of individuals suffering from infectious or potentially infectious diarrhoea. The Trust will have systems in place to remove or minimise the risk of infection and cross infection.
This policy cannot anticipate every situation therefore professional judgement should be used to identify when a risk assessment is needed to protect those who are vulnerable and / or at risk. The process will enable staff to identify the level of vulnerability and the risks posed to individuals. This policy applies to all Trust staff. It should be read and followed whenever advice regarding diarrhoea is required. 3. Definitions This document is a policy, which clearly specifies its’ purpose and scope. 4. Duties Infection prevention and control is everybody’s responsibility. South West Yorkshire Partnership NHS Foundation Trust has a duty and is committed to reducing the risk of infection. All Trust staff are responsible for demonstrating compliance with this policy. Instructions for managing affected individuals can be found in the appendices of the policy. The following specific duties apply: 4.1 Chief Executive The Chief Executive has overall accountability for reducing the risk of infection by ensuring that there are arrangements for the management of infectious or potentially infectious diarrhoea within the organisation. They will:
review and monitor trends of Clostridium difficile cases across the Trust.
challenge areas with high rates of infection
be responsible for ensuring that all Directors, the Executive Management Team, Business Delivery Units (BDUs) and all other staff understand and accept their responsibilities in relation to this policy.
be responsible for ensuring that infection prevention and control (IPC) is embedded at all levels of the organisation.
4.2 Trust Board Trust Board is responsible for signing off the approval, dissemination and implementation of this policy. They will:
ensure there are effective and adequately resourced arrangements for managing infectious or potentially infectious diarrhoea.
regularly review the progress of Clostridium difficile statistics.
receive outbreak reports and reports of serious untoward incidents.
review relevant infection prevention and control data.
receive and approve the annual IPC report and annual plan
monitor progress
review and monitor other relevant IPC data, including compliance with education and training.
5
4.3 Executive Management Team (EMT) The Executive Management Team is responsible for approving the contents of the policy. 4.4 Clinical Governance & Clinical Safety Committee The Clinical Governance & Clinical Safety Committee is responsible for the dissemination and implementation of this policy on behalf of Trust Board. They will review relevant infection prevention and control data. 4.5 Director of Infection Prevention and Control (DIPC) The DIPC will report directly to the Chief Executive and the board, and not through any other officer. They will:
oversee local implementation of the Diarrhoea policy, procedure and guidelines.
produce statistical information relating to infectious diarrhoea including Clostridium difficile infections and Norovirus outbreaks.
challenge inappropriate clinical hygiene practice as well as antibiotic prescribing decisions.
review relevant data including root cause analysis (RCA) and assist with mortality reviews
be an integral member of the organisation’s clinical governance and patient safety teams and structures.
assess the impact of all policies and plans on infection, and make recommendations for change.
be the lead director responsible for engaging relevant stakeholders in the development of the policy.
ensure appropriate arrangements are in place for managing any resource implications, including dissemination, implementation and training.
be responsible for ensuring the most current version of the policy is in use and obsolete versions have been withdrawn from circulation.
submit the infection prevention and control assurance framework objectives for the coming year to Trust Board for approval.
produce an annual report on the state of Health Care Associated Infection (HCAI) in the organisation, and release it publicly.
4.6 Director of Nursing The Director of Nursing will:
monitor and support the activities of the IP&CT
support the development of the Diarrhoea policy and its implementation
promote best practice related to IP&C within the organisation
ensure compliance with the Diarrhoea policy with all matters related to nursing and professions
ensure complaints related infectious or potentially infectious diarrhoea are monitored and trends identified.
4.7 Director of Estates and Facilities The Director of Estates and Facilities will:

6
ensure that the environment is fit for purpose, cleaned and maintained to promote, best practice in the management of infectious or potentially infectious diarrhoea.
deliver the actions related to own sphere of responsibility.
ensure the cleanliness of the environment is monitored and reports are presented to the Infection Prevention and Control Trust Action Group (IPC TAG).
4.8 Director of Human Resources The Director of Human Resources will:
ensure systems are maintained to enable training attendance to be recorded and reported as a performance issue to Trust board, clinical and management teams as required.
4.9 Medical Directors The Medical Director will:
ensure that appropriate systems are in place to review reports and statistics
ensure clinical responsibility for the management of infectious or potentially infectious diarrhoea is clearly identified and delivered.
4.10 Infection Prevention and Control Trust Action Group (IPC TAG) The IPC TAG will review new legislation and guidance and ensure that its implications are fully understood within the Trust. It will:
commission a revision of the existing policy accordingly and oversee the dissemination
implementation of the revised policy. Commissioning and development of this policy may be undertaken in liaison with the Health and Safety TAG, Drugs and Therapeutics Committee, and the Estates TAG.
receive quarterly reports from the IPCT in order to monitor compliance with relevant IPC policies.
4.11 Infection Prevention and Control Team (IPCT) The IPCT will:
promptly report all positive results to relevant clinicians
provide specialist infection prevention and control advice to management, clinicians and practitioners.
advise on appropriate isolation measures for infected and symptomatic service users, correcting hazardous or ineffective procedures.
produce and monitor policies, procedures and guidance for the prevention and control of infectious or potentially infectious diarrhoea, monitoring numbers, identifying outbreaks or increases in numbers.
provide education to prevent and control infectious or potentially infectious diarrhoea to all relevant Trust staff.
produce an annual programme of infection prevention and control activities and an annual report to the IPC TAG.
provide advice on decontamination and control of infectious pathogens in the environment.
participate and initiate audit to prevent and control infectious or potentially infectious diarrhoea.

7
assist in the review of infectious or potentially infectious service users’ ongoing care and management.
support, advise and provide information to the service user and relatives as appropriate.
provide information to contractors, visitors and service users to prevent and control infection.
advise on appropriate microbiological tests.
ensure that Directors of BDUs are made aware of issues which occur within their care groups as they arise.
provide other timely reports to Trust Board, EMT, the Clinical Governance & Clinical Safety Committee, BDUs, Managers and any other relevant groups throughout the year. These will include lessons learnt, performance management and changes to policy and procedures.
lead by example and challenge poor practice 4.12 Business Delivery Units BDUs will:
work with the IP&CT to prevent and control infection.
ensure the prompt isolation and correct management of service users with infectious or potentially infectious diarrhoea in inpatient areas
ensure there is suitable and sufficient personal protective equipment to control and prevent the transmission of infectious or potentially infectious diarrhoea
ensure the provision of adequate equipment to facilitate the maintenance of hygiene and cleanliness
ensure that the environment and equipment is regularly decontaminated and monitored for cleanliness and is fit for purpose.
review the statistical information in relation to their area of practice, meeting national and local infection reduction targets.
ensure staff are aware and comply with policies, procedures and guidance related to the management and prevention of infectious or potentially infectious diarrhoea including attending appropriate education sessions.
be consulted in the development of the policy.
ensure that the policy is implemented within their areas.
ensure that business plans capture any resource implications identified to prevent the effective implementation of this policy.
4.13 Consultants Consultants will:
ensure that all policies and procedures related to the prevention and control of infection are implemented in their area.
ensure that service users with infectious or potentially infectious diarrhoea receive the appropriate clinical care and management.
ensure that junior medical staff are fully informed and adhere to current policies and procedures in relation to the prevention, control and management of infection.
adhere to the Trust’s antibiotic prescribing policy.
participate in audit programmes, reviewing outcomes and taking appropriate action.
8
review the statistical data related to infectious or potentially infectious diarrhoea, implementing the action plan and meeting national and local targets for reduction.
on discharge will ensure GP’s are advised that the service user has had infectious diarrhoea.
4.14 Medical staff: Medical staff will:
implement the infection prevention and control policies, procedures and guidelines of the trust
undertake infection prevention and control training as identified in the training needs analysis
deliver the IPC strategy related to their own area of responsibility
adhere to the Trust’s antibiotic prescribing policy. 4.15 General Managers / Practice Governance Coach General Managers / Practice Governance Coach have a key responsibility for the environment in which care is provided. They have a pivotal role in supporting the IPCT to ensure effective implementation of the Diarrhoea policy. They will:
ensure that standards for the prevention and control of infectious or potentially infectious diarrhoea are met.
ensure that the policy, procedures and guidance are integrated into clinical practice.
undertake monitoring, surveillance and audit to provide evidence of compliance with the policy.
ensure a safe clean environment by a process of monitoring and liaison with Facilities / Hotel Services / Domestic Department.
liaise and work closely with the IP&CT to prevent and control infectious or potentially infectious diarrhoea
review and distribute statistical data to areas of responsibility, working to meet national reduction targets.
ensure equipment is clean and fit for purpose as per decontamination policy
liaise with service users and relatives, providing information as required.
participate proactively in promoting infection prevention and control, acting as a role model
work closely with the IPC Team. 4.16 Unit / Department Managers Community staff/ Ward Sisters/ Ward Managers will:
seek advice as soon as possible from the IPCT with regard to any relevant issues related to this policy.
adhere to and ensure compliance with the policies, procedures and guidance relating to the prevention and control of infectious or potentially infectious diarrhoea, in the area.
ensure that all staff for whom they have line management responsibility are aware of, and comply with this policy.
ensure their area of responsibility provides a safe clean environment, and equipment that is clean and fit for purpose.

9
ensure effective communication with staff, domestics, service users and visitors, to control the transmission of infectious or potentially infectious diarrhoea.
ensure strict adherence to the correct clinical care and management of individuals with infectious or potentially infectious diarrhoea.
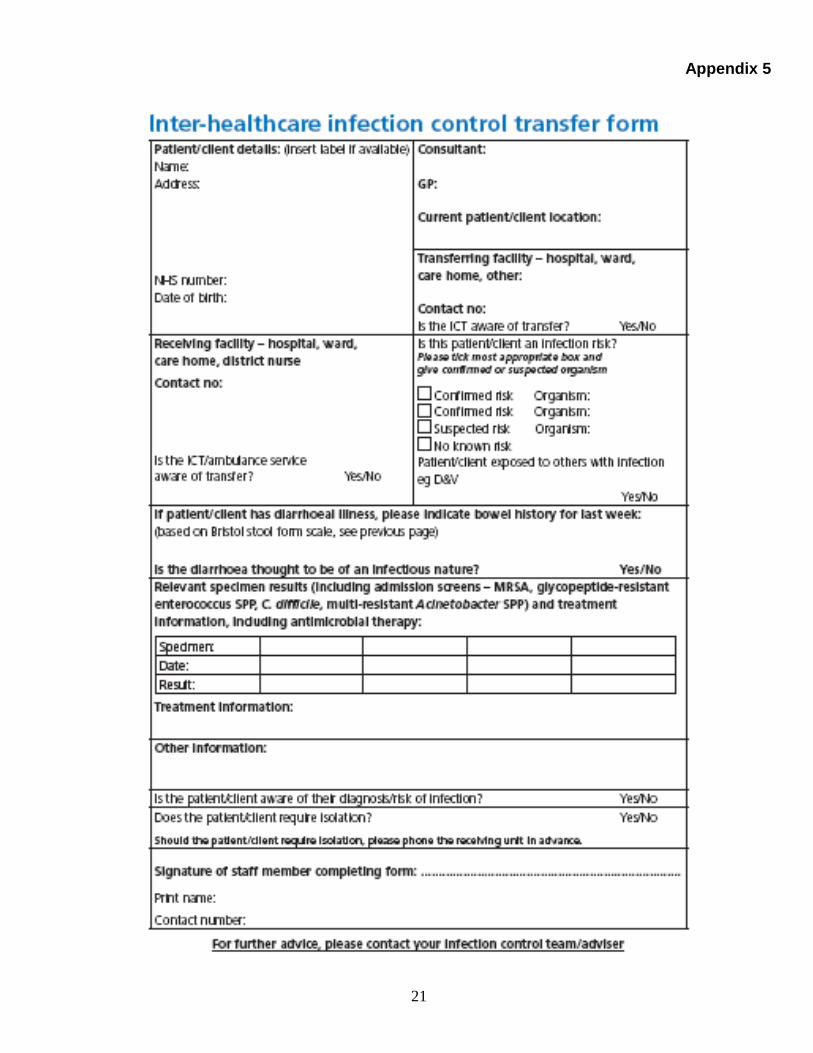
complete the inter-healthcare infection prevention and control transfer form (appendix 9) on all internal and external transfers/discharges where health care will be provided.
ensure records of mandatory IPC training are sent to the Learning & Development Centre for collation.
4.17 Link Practitioners Link Practitioners will:
actively promote compliance with this policy.
take part in promotional events where appropriate.
reinforce good practice by attending the Link Professionals meetings/updates.
lead by example. 4.18 Employees Infection prevention and control is everyone’s business. All employees are responsible for taking reasonable care of themselves, service users and any other people affected by their acts or omissions in accordance with Health and Safety at Work Act 1974. Employees have an individual responsibility to ensure they are working within legal and ethical boundaries. It is each member of staff’s responsibility to seek out guidance and help in implementing this policy where they have difficulty. If any member of staff is aware of difficulties in following the policy they must alert their line manager as soon as is practical. All employees must:
adhere to the policies, procedures and guidelines on the prevention and control of infectious or potentially infectious diarrhoea.
ensure the correct usage of PPE to prevent transmission of infection.
attend appropriate training as required.
complete the inter-healthcare infection prevention and control transfer form (appendix 9) on all internal and external transfers/discharges where health care will be provided.
report failure in protocol on the DATIX system
be aware of the risks to others as a consequence of non-compliance with this policy.
have responsibility for accessing and complying with this policy.
ensure equipment is clean and fit for purpose as per decontamination policy 4.19 Volunteers, Agency Staff, External Contractors and visitors/members of the public Visitors, agency staff and external contractors are expected to comply with reasonable instructions given by staff who are seeking to protect them from risk of infection by requesting compliance with the policy. 4.20 Occupational Health. Occupational Health will:
monitor staff health.
assist with the assessment of risk following an infection if required.

10
advise managers and employees on the management of infection sustained at work. 4.21. Consultation and Communication with Stakeholders The organisation recognises that policies need to be developed in consultation and communication with a range of stakeholders. The DIPC is responsible for ensuring relevant stakeholders have been consulted during the development of the policy. The following list identifies some of the individuals or groups who have been consulted in the development of this policy. This is not an exhaustive list.
Stakeholder Level of involvement
Executive Management Team Approval
Director of Infection Prevention and Control Initiation, lead, development, receipt, circulation
Infection prevention and control trust action group ( IPCTAG) Health and safety TAG (H&S TAG) Drugs and therapeutics committee
Commissioning, development, consultation, dissemination, implementation, monitoring
Infection Prevention and Control Team Development, consultation, dissemination, implementation, training, audit
Specialist advisors Development, consultation, dissemination, implementation
Business Delivery Units Consultation, dissemination, implementation, monitoring
Managers, Professional groups and leaders, unit managers, link practitioners, service users and carers
Development, consultation, dissemination, implementation
5. Principles The organisation must fulfil its obligation in reducing healthcare associated infections. The organisation must fulfil its obligations for the Health and Social Care Act, Care Quality Commission Standards, NHS Litigation Authority Risk Management Standards and any other corporate accreditation processes.
For the purpose of this policy the assurance framework takes the form of the Annual Infection Prevention and Control Report and Annual Programme.
6. Equality Impact Assessment The Trust aims to ensure its policies and procedures promote equality both as a provider of services and as an employer. Please see appendix 2 for equality impact assessments.
7. Dissemination and implementation arrangements (including training)
7.1 Dissemination This policy is available in read only format via the document store on the Trust intranet. Staff are informed of any changes to the policy via the weekly staff communication on the Trust intranet and a communication from the IPCT via the home
11
page of the Intranet and other media forms.
7.2 Implementation Support to assist implementation of this policy is available from the IPCT. Additional downloadable information is also available on the infection prevention and control pages on the intranet. 7.3 Training IPC training is mandatory for all staff. This will be as advised by the annual training needs analysis (TNA) identified by the Learning and Development Lead. BDUs and Service managers are responsible for ensuring that all their staff attend mandatory IPC training sessions. The IPCT will offer training in a number of formats e.g. face to face, e-learning, DVD, to accommodate the diversity of the service. 8. Process for monitoring compliance and effectiveness Regular audit of processes and procedures will take place and be reported via the IPCT, IPC TAG and other appropriate internal and external Governance Committees. Any incidents will be reported by the DATIX system. Any outbreaks and untoward incidents will also be reported through the IPC TAG and other appropriate Governance Committees. The Annual Infection Prevention and Control Programme is monitored and a quarterly written report is produced to demonstrate compliance. This quarterly report is scrutinised at the IPC TAG where achievements and exceptions are discussed. Progressive action then planning takes place if required. This report is then in turn processed through the internal and external governance arrangements within the organisation. 8.1 Monitoring Compliance Arrangements are in place for ensuring and monitoring compliance with this policy, and these are reported up through the organisation and evidenced through the following legislation and guidance. 8.1.1 External Standard requirements: This policy meets the minimum requirements in the NHSLA Risk Management Standards 2012/13: Standard 4: Safe environment, criteria 1.4.6 / 1.4.7 DH (2008) The Health and Social Care Act: Code of Practice on the prevention and control of infections and related guidance. DH (2010) Essential Standards for Quality and Safety: Outcome 8 Safeguarding and Safety (regulation 12): cleanliness and infection control. DH (2006) Essential Steps to Safe, Clean Care.
12
DH(2004) Towards Cleaner Hospitals and Lower Rates of Infection. DH (2003) Winning Ways, Working Together to Reduce Health Care Associated Infection in England. Report from the Chief Medical Officer. EPIC 3 (2104) National Evidence-based Guidelines for Preventing HCAI in NHS Hospitals in England Health and Safety at Work Act 1974. NICE (2012) Prevention of Healthcare Associated Infection in Primary and Community Care. 8.1.2 Key performance indicators The IPC TAG has developed the following key indicators to enable adequate performance management of Clostridium difficile practice within the organisation and to ensure continuous quality improvement of the KPI scores:
reductions in the number of untoward incidents associated with infection
reductions in the number of clearly defined outbreaks of infection
number of infection control audits undertaken
environmental audit scores
meeting trajectories for HCAI as set locally and nationally
These KPIs are monitored and reported to the IPC TAG on a quarterly basis and a report is included in the infection prevention and control annual report and programme for the coming year. 8.2 Effectiveness The IPC TAG will commission annual audits by the Clinical Governance Support Team / data analyst (CGST / data analyst) of the infection prevention and control practice of all staff on behalf of the DIPC. These reports and action plans will form the basis of the infection prevention and control assurance framework objectives for the coming year. They are also responsible for facilitating the monitoring and auditing the hand hygiene technique of staff on an annual basis. The audit results will be provided to the IPCT for action plans to be generated if required and to CGST / data analyst for an audit report which will be included in the IPC annual report.
This audit will also be supported by action plans generated from regular monitoring and kitchen inspections carried out by the Facilities Department and by the Service user Led Assessment Care Environment Team inspections (PLACE) as part of the Care Quality commission (CQC) Essential Standards annual health check requirements. 9. Review and revision arrangements (including archiving)
9.1 Process for reviewing the policy The review date for this policy will be Dec 2016 and two yearly thereafter unless otherwise indicated by an identified need for change.

13
9.2 Version Control This policy has been updated from its previous format and is version 2. 9.3 Archiving The Integrated Governance Manager will be responsible for maintaining a corporate record of this policy and notifying the Lead Director when the policy is due for review. 10. References Department of Health (2010) Clostridium difficile: How To Deal With the Problem Department of Health. The Health and Social Care Act (2008): Code of Practice on the prevention and control of infections and related guidance. London. DH 2008 http://www.dh.gov.uk Essential Standards of Quality and Safety Outcome 8 Safeguarding and Safety (DH 2010) (regulation 12): cleanliness and infection control. Health and Safety at Work Act (1974) HMS) NHS Estates (2002): Infection Control in the Built Environment: Design and Planning. Health Facilities Note (HFN) 30. Available from: http://195.92.246.148/knowledge_network/documents/publications/designguidance/ic.pdf NICE (2012) Prevention of Healthcare Associated Infection in Primary and Community Care. Royal College of Nursing (2013) The Management of Diarrhoea in Adults 11. Associated documents This document should be read in conjunction with the following SWYPFT documents:
Infection Prevention and Control policies
Local Antibiotic Prescribing Policy
Clostridium difficile policy
Barrier Nursing procedure
Confidentiality policy
Health and Safety policy
Legionella (Control of and Water Safety) policy
COSHH guidance
Incident Reporting and Management (including Serious Untoward Incidents) policy
Occupational Health and Wellbeing policy
Human Resources policy
Mandatory training policy
Whistle blowing policy

14
12. Appendices As listed on the following pages
15
Appendix 1 Management of an inpatient with diarrhoea
Loose Stool:
Check and record normal bowel habit
Record date of onset of symptoms in service user’s record
Suspect that diarrhoea may be infective when there is no clear alternative cause
Check for any underlying conditions
Review medications to ensure diarrhoea not caused by overuse of aperients, or those which may cause diarrhoea or constipation
Exclude constipation with overflow – check bowel history
If infective diarrhoea is then suspected, obtain and send a faeces sample to the laboratories, ensuring the clinical details are completed
Stool must be loose enough to take the shape of the container when a faeces sample is obtained (Bristol Stool type 5-7)
Isolate Service user All service users must be isolated unless it is impracticable and unsafe to do so. A risk assessment must be completed in this case and appropriate systems utilised to minimise the risk of cross infection. This must be documented in the care plan.
Any service user with diarrhoea should be isolated and barrier nursed in a side room, unless clearly non infectious, following the second episode of diarrhoea. If the isolation room does not have its own toilet facilities, the service user should be given a designated toilet close to the room. If this is not possible a commode should be designated for that service user, this should not be stored in the service user’s room. This must be documented in the service users notes as a risk assessment.
Ensure barrier nursing notice is placed on the outside of the side room door.
It is the symptoms of diarrhoea that determines when the service user should be isolated not the presence of a diagnosis.
Barrier nursing should be discontinued once the service user has been asymptomatic for 48 hours and passed a normal stool (for that service user)
No side room
Commence barrier nursing immediately in existing bed space
Notify the senior nurse who will inform the site manager if a side room cannot be found within 1hour. The duty manager will escalate if the issue cannot be resolved
Notify IP&CT
Follow side room escalation procedure (Appendix 3)
Who to inform
IP&CT
16
The Service user - explain the need for isolation and importance of hand hygiene particularly before eating
The Medical Team – to review service user/medication and risk assess for infectious cause. Discuss any antibiotic therapy with the Consultant Microbiologist
Domestic Services – to ensure cleaning of the room/toilet facilities with Chlor-clean (1000ppm chlorine )
Relatives/carer – ensure that they are aware of strict hand washing with soap and water before and after visiting.
Continence Specialist Nurse if applicable
Supply information leaflets to service users / relatives Stool
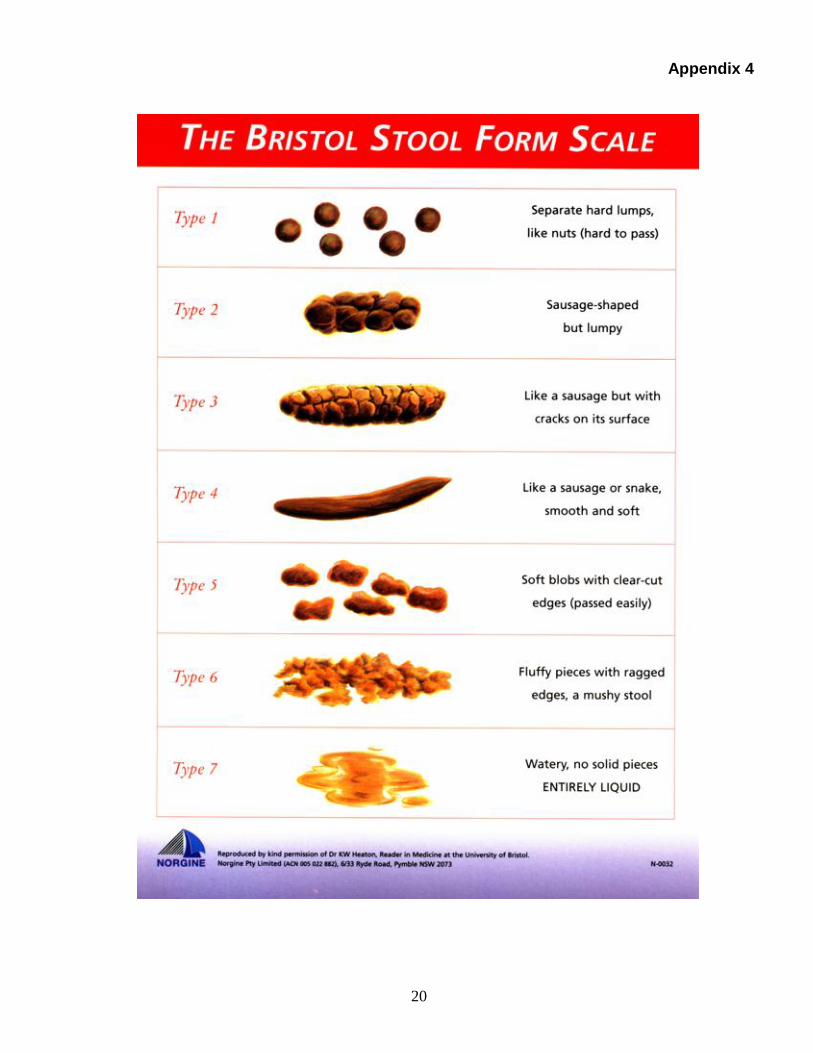
Commence stool chart utilising (Appendix 4) Bristol Stool Chart noting frequency and type of stool. Monitor completion. Continue for duration of symptoms
Hydration
Maintain daily fluid balance record, ensuring adequate hydration and monitoring of urea and electrolytes if required
Alert Medical Team for any indication of dehydration Nutrition
Ensure Nutritional Risk score assessment completed
Follow guideline regarding referral to dietician
Give supplements as indicated if required Tissue Viability
Ensure Norton or Waterlow risk assessment updated
Monitor for excoriation of skin
Use appropriate barrier cream as necessary
Involve Tissue Viability Nurse for advice if indicated Results
Check stool sample results
If an infectious agent is identified, follow specific guidance for that agent
If no infectious agent is identified and the symptoms persist, send another faeces sample if advised by Microbiology Consultant
Request medical review/referral to Gastroenterology if required
Re-risk assess likelihood of infectious cause with clinical team and re- evaluate need for isolation, seek Infection Prevention and Control advice

17
Hand hygiene and PPE
Ensure strict hand washing. Alcohol hand gel should be used to compliment rather than replace hand washing as this is not effective for some faecal organisms
Ensure gloves and aprons are readily available and worn as appropriate and disposed of appropriate
Service user movement
Service users who are symptomatic or are recovering from diarrhoea should not attend the therapeutic kitchen to participate in any food preparation activity until they have been clear of symptoms for 48 hours and passed a normal stool
Service users transferred to other health care settings should be discussed with the Infection Prevention and Control Team – complete inter healthcare transfer form
If service users need to attend other areas for diagnostic testing etc, please seek advice from the Infection Prevention and Control Team
Cleaning
Enhance environmental cleaning using Chlor- clean daily
Terminal cleaning of the room and equipment on discharge with Chlor-clean/Hydrogen Peroxide Vapour on advice from the Infection Prevention and Control Team
Ensure any equipment is cleaned after use by the service user
Ensure commodes are cleaned with Chlor-clean after every use Waste/Linen
Waste must be safely disposed of into the infected waste stream
Place linen into alginate bag inside the service users room once secure, place into a red linen bag outside the room, on no account must linen be left in the service users room.
Equipment
Equipment must be kept to a minimum within the isolation room
All equipment should be cleaned following use and removal from isolation room
Outbreak
Refer to trust Infectious Outbreak Guidelines

18
Care of Affected Individuals in the Home Environment 1. There should be no restriction on the discharge or transfer of service users who have had
infectious diarrhoea. If symptoms remain, the individual must have been deemed as medically fit by the doctor in charge of their care.
Once someone has recovered clinically they are not a risk to others even if they continue to carry an infection in their stool for a period provided they observe the normal personal hygiene precautions of hand washing after using the toilet. A service user with a formed stool and who is continent is not considered to present a risk for environmental contamination or cross infection. A history of diarrhoeal infection is not a contradiction to a service user returning to a care home/nursing home/ home setting.
2. In order to reduce the risk of transmission, individuals should be advised and encouraged to
decontaminate hands with soap and water, especially after using the toilet and before eating. It is recognised that for some service users this may be complex to achieve and as such individual circumstances would need to be assessed and documented. Alcohol hand rub is NOT effective against some bowel infections. Also keep surfaces in bathrooms, kitchens and other areas clean, cleaning on a regular basis with household detergent/disinfectant. It is also advisable that individuals keep a towel for their own use whilst the diarrhoea is still present.
3. Any soiled linen/clothes should be washed as a separate load to other items on the hottest
wash that will not damage the clothes; ideally at a temperature of 60 degrees. 4. Crockery and cutlery may be processed through the dishwasher or washed as normal.
Disposables are not required. 5. It is important that the individual drinks plenty of water to prevent dehydration 6. Frequent assessment of the affected individual should take place, ensuring adequate hydration
is maintained. 7. Visitors to the individual should also ensure strict hand hygiene is maintained, it is not
necessary for visitors to wear gloves and aprons unless delivering direct service user care. Repeat faeces samples are not required unless symptoms re occur, or advised by the IP&CT
Appendix 2

19
Appendix 3
Side-Room Escalation procedure Stage 1 Nurse in Charge not able to isolate service user Stage 2 Nurse in Charge contact IP&CT for advice and discuss. Action advised by IP&CT. Nurse in
Charge initiate advice. Stage 3 Nurse in Charge unable to initiate isolation of service user. Nurse in Charge to contact
Ward Manager. Stage 4 Ward Manager investigates isolation options as per Nurse in Charge and IP&CT advice. Stage 5 Ward Manager unable to initiate isolation of service user the service manager is informed
within 1hr. If the service manager unavailable contact the Operational Manager and Director of Infection Prevention and Control (DIPC)
Stage 6 Service manager or other director makes decision within 1 hour. Decision communicated to
Ward Manager, Nurse in Charge and IP&CT Stage 7 Decision and process documented by Nurse in Charge by the end of shift, copy to the
IP&CT. A datix report is also to be completed by the Duty Manager if the service user is not isolated.
The process and decision must be documented in the service user’s notes.
NB: The following information must be available before contacting the Infection Prevention and Control Team (IP&CT) for advice on matters relating to the isolation of service users:
Risk assessment of service user isolation requirements based on the Isolation Policy.
Up to date position of side rooms at the specific site (to include service users on MRSA eradication therapy, service users with multi-resistant strains of MRSA or other organisms, MRSA screens, infectious or potentially infectious symptomatic service users including date of last episode of vomiting or diarrhoea, up to date available laboratory results.)
Up to date overall position of isolation facilities with the specific site concerned (availability of side rooms, cohort facility beds)
Out of Hours:
The bleep holder is to assess the risk of cross infection and if urgent isolation is required. If required follow escalation procedure through on call directors
20
Appendix 4
21
Appendix 5

22
Diarrhoea / Clostridium Difficile Flowchart
PATIENT HAS
DIARRHOEA
1. Isolate the patient
2. Start Bristol stool chart
3. Start fluid balance chart
4. Send sample to lab after 2nd episode of unexplained
diarrhoea
5. Observe faecal oral precautions – place sign on door
6. Maintain hydration
7. Monitor U&E’s and inflammatory markers
8. Review patient’s condition and stop non essential treatment
and review e.g. PPI’s and antibiotics
9. Ensure gloves and aprons are used and readily available
10. Wash hands with soap and water. Alcohol gel ineffective for
C. diff and Norovirus
Prior to sending sample, please check:
Patient’s clinical / bowel history, i.e. patient on aperients / patient has overflow
Is the patient on antibiotics?
If suspected infectious diarrhoea – inform Infection Prevention & Control Team
Severe symptoms or strong
suspicion of Clostridium Difficile
infection i.e. odour, been on
antibiotic, previously positive for C
Difficile
Await stool results
Inform Infection Prevention and
control Team and start C. difficile
treatment if patient symptomatic.
Review when results are
available
Faeces sample positive for:
• Salmonella
• Shigella
• Campylobacter
1. Isolate the patient until 48
hours clear, passed a normal
stool and can maintain own
hygiene
2. Maintain hydration
3. Observe faecal oral
precautions
4. No repeat samples unless
requested by the infection
prevention & control team
C DIFF TOXIN
POSITIVE AND
HAS
DIARRHOEA
1. Isolate the patient until asymptomatic for 48 hours and a normal
stool has been passed
2. Commence C Diff care pathway
3. Start Bristol stool chart
4. Start fluid balance chart
5. Observe faecal oral precautions – place sign on door
6. Maintain hydration
7. Monitor U&E’s
8. In severe cases involve specialist (Gastroenterologist and
surgeons) for assessment for colectomy surgeons
9. Ensure gloves and aprons are used and readily available
10. Wash hands with soap and water, alcohol gel is ineffective
11. Review patient’s condition and stop non essential treatment and
review eg PPI’s and antibiotics
Do not send repeat samples on C Diff positive patients unless requested to do so
by Infection Prevention & Control team. Further samples may be sent if other
infection is suspected – contact Infection Prevention & Control Team –
433364/433363
1. Start treatment
2. If this is a relapse after a
course of treatment discuss
with microbiology
3. Stop all unnecessary
antibiotics
4. Stop PPI’s if appropriate
5. Stop aperients
6. Review medical history for
any changes
Infection Prevention and Control
Team to review patient regularly.
At day 7, monitor whether patient
still has diarrhoea
Contact Consultant
Microbiologist for advice
Does the patient still have diarrhoea?
Continue treatment until 14
day course completed
Yes No
Yes
No
Appendix 6

23
12.2. Equality Impact Assessment tool To be completed and attached to any policy document when submitted to the Executive Management Team for consideration and approval.
Equality Impact Assessment Questions:
Evidence based Answers & Actions:
1
Name of the policy that you are Equality Impact Assessing
Diarrhoea Policy
2
Describe the overall aim of your policy and context? Who will benefit from this policy?
The Trust will have in place systems which remove or minimise the risk of infection, including infectious diarrhoea This policy outlines the procedure for the management of infectious or potentially infectious within SWYPFT. The overall aim of the policy is to provide staff with clear and practical evidence based information on all aspects of infectious or potentially infectious diarrhoea that they can translate into their working practice within the context of the requirements of the H&S Act(2008), NHSLARMS (DH, 2010), NSF’s National Targets, Care Quality Commission and any other corporate accreditation processes. All staff
3 4
Who is the overall lead for this assessment? Who else was involved in conducting this assessment?
Director of Nursing, Compliance and Innovation (designated Director of Infection Prevention and Control) The Infection Prevention and Control Team
5
Have you involved and consulted service users, carers, and staff in developing this policy? What did you find out and how have you used this information?
The Executive Management Team and staff teams were consulted during the original development of the Policy It was identified that staff required clear and unambiguous information that was easily accessible. This was taken into account when developing the policies.
24
6 7
What equality data have you used to inform this equality impact assessment? What does this data say?
n/a
8
Taking into account the information gathered. Does this policy affect one group less or more favourably than another on the basis of:
Where negative impact has been identified please explain what action you will take to remove or mitigate this impact. If no action is to be taken please explain your reasoning.
YES NO This policy will affect everyone, however with no discrimination. This policy is applicable to everyone.
Race NO
Disability NO
Gender NO
Age NO
Sexual Orientation NO
Religion or Belief NO
Transgender NO
Carers NO
9
What monitoring arrangements are you implementing or already have in place to ensure that this policy:
promotes equality of opportunity who share the above protected characteristics
eliminates discrimination, harassment and bullying for people who share the above protected characteristics
promotes good relations between different equality groups,
This policy aims to standardise the approach to policy development, approval and dissemination and should ensure adoption of Equality Impact Assessments throughout the organisation.

25
10
Have you developed an Action Plan arising from this assessment?
None required
11
Who will approve this assessment and when will you publish this assessment.
Executive Management Team When revised policy is approved by Trust Board
12 Once approved, please forward a copy of this assessment to the Equality & Inclusion Team: [email protected]
If you have identified a potential discriminatory impact of this policy, please refer it to the Director of Corporate Development or Head of Involvement and Inclusion together with any suggestions as to the action required to avoid/reduce this impact. For advice in respect of answering the above questions, please contact the Director of Corporate Development or Head of Involvement and Inclusion.
26
12.3. Checklist for the Review and Approval of Procedural Document To be completed and attached to any policy document when submitted to EMT for consideration and approval.
Title of document being reviewed: Yes/No/ Unsure
Comments
1. Title
Is the title clear and unambiguous? YES
Is it clear whether the document is a guideline, policy, protocol or standard?
YES
Is it clear in the introduction whether this document replaces or supersedes a previous document?
YES
2. Rationale
Are reasons for development of the document stated?
YES
3. Development Process
Is the method described in brief? YES
Are people involved in the development identified?
YES
Do you feel a reasonable attempt has been made to ensure relevant expertise has been used?
YES
Is there evidence of consultation with stakeholders and users?
EMT
4. Content
Is the objective of the document clear? YES
Is the target population clear and unambiguous?
YES
Are the intended outcomes described? YES
Are the statements clear and unambiguous?
YES
5. Evidence Base
Is the type of evidence to support the document identified explicitly?
YES
Are key references cited? YES

27
Title of document being reviewed: Yes/No/ Unsure
Comments
Are the references cited in full? YES
Are supporting documents referenced? YES
6. Approval
Does the document identify which committee/group will approve it?
YES
If appropriate have the joint Human Resources/staff side committee (or equivalent) approved the document?
N/A
7. Dissemination and Implementation
Is there an outline/plan to identify how this will be done?
YES
Does the plan include the necessary training/support to ensure compliance?
N/A
8. Document Control
Does the document identify where it will be held?
YES
Have archiving arrangements for superseded documents been addressed?
YES
9. Process to Monitor Compliance and Effectiveness
Are there measurable standards or KPIs to support the monitoring of compliance with and effectiveness of the document?
YES
Is there a plan to review or audit compliance with the document?
YES
10 Review Date
Is the review date identified? YES
Is the frequency of review identified? If so is it acceptable?
YES
11 Overall Responsibility for the Document
Is it clear who will be responsible implementation and review document?
YES

28
12.4. Version control sheet This sheet should provide a history of previous versions of the policy and changes made
Version Date Author Status Comment / changes
1 August 2008
Director of Nursing, Clinical Governance and Safety (designated Director of Infection Prevention and Control)
Final Final version approved by Trust Board