Embed Size (px)
Citation preview

Instituto de Investigación Nutricional, Lima, Perú
Page 1 of 48
IMPROVING DIARRHOEA ESTIMATES
Claudio F. Lanata, M.D., M.P.H. Walter Mendoza, M.D.
Instituto de Investigación Nutricional A.P. 18-0191, Lima-18
PERU
Advisor: Robert E. Black, M.D., M.P.H.
Chairman Department of International Health School of Hygiene and Public Health
Johns Hopkins University, Baltimore, MD, USA.
Presented to:
Monitoring and Evaluation Team Child and Adolescent Health and Development
World Health Organization Geneva, Switzerland.
October 2002
Instituto de Investigación Nutricional, Lima, Perú
Page 2 of 48
1. INTRODUCTION Diarrhoeal diseases remain a leading cause of morbidity and mortality in the world, particularly in developing countries. WHO, UNICEF and other partners are interested in updating the previous reviews on total and cause-specific diarrhoea morbidity and mortality in the world, to best estimate the burden of diarrhoeal diseases for the world in the year 2000. In this study, we wanted to produce the following outcomes:
1. To produce a data base for each of the WHO regions and 14 sub-regions, in the period 1990-2000, for children under 5 years of age, on the proportion of diarrhoeal illness caused by each type of diarrhoeal pathogen, at the community and health facility level.
2. To apply these estimates to the current estimates of diarrhoea burden produced by the U. of Virginia team.
3. To compare the current burden with the last global burden of diseases exercise and discuss potential reasons for current trends.
4. To describe the methodology used, data availability and assumptions used in reaching these new estimates.
5. To provide recommendations on how these estimates could be improved, interpreted and used.
It is expected that this exercise will contribute to the discussion and assessment of the diarrhoea-attributable burden of disease and injury for the year 2000 done by WHO. We present in this report our final results, to help in its discussion and interpretation.
2. METHODOLOGY 2.1 Data Sources and Statistical Analysis A systematic literature review was been conducted in order to get both printed or web based articles from journals and other sources. Efforts have also been made to contact relevant clinicians and scientists to identify all other non-published studies and all relevant model inputs as well. Search algorithms and strategies has been developed for the literature review and printed literature has been retrieved from leading libraries in Public Health, whether by library loan or photocopying them. Keywords used to conduct the search included “diarrhea” (or “diarrhoea”), “diarrhea AND epidemiology”, “diarrhea AND etiology”, “diarrhea AND community”, and “diarrhea AND hospital”, for the period 1990-2002, inclusive (August). Copies of papers identified with cause-specific data on diarrheal diseases were reviewed.. Besides hand search was conducted from all available articles. The search engines to locate web based publications and/or references included the following: Freemedicalhournals: www.freemedicaljournals.com PubMed: www.ncbi.nlm.nih.gov/entrez/query.fcgi MedHunt: www.hon.ch/MedHunt Medexplorer: www.medexplorer.com Medscape: www.medscape.com Medical World Search: www.mwsearch.com 2.2 Inclusion and exclusion criteria
Instituto de Investigación Nutricional, Lima, Perú
Page 3 of 48
All identified published papers in the period 1990-20021 (June) were systematically reviewed, using the following criteria.
Inclusion criteria: a) Community studies
• < 1 week in frequency of home visits or telephone contacts. • > 1 year of surveillance • All types of diarrhoea or only dysenteric illness (Classified accordingly) • Stool cultures taken, even only for one enteropathogen. • Population under study < 5 yo.
b) Hospital or health facility-based Studies • > 1 year of surveillance • All diarrhoea cases studied or those selected by systematic sampling • Population under study < 5 yo
Exclusion Criteria:
• Outbreaks • Studies in day care centres or similar • Studies of special populations (nursing homes, etc) • Only on AIDS patients • Not definition of surveillance frequency or sampling scheme • Nosocomial infections
2.3 Data Base A data base on SPSS 11.0 was created including the above data, besides the following variables:
• Authors’ last name and initials • Journal reference • Year of publication • Year of study onset • Duration of follow-up (in months completed) • Type of study
o 1 = community based, o 2 = health services or hospital-based o 3 = day care centres (or similar) o 4 = Outbreaks o 5 = other types
• Description of type of study (written description) • Diarrhoea definition
o 1 = acceptable (3 or 4 liquid or semi liquid stools /24 h, or mother’s report) o 2 = not acceptable (others, excluding dysentery)
1 For most regions there was at least one available article, but for those which didn’t fulfill this condition we went further back to consider studies published before 1990 and after 1985. With this criterion AfroD and AfroE presented at least one study per setting, while other regions (EuroB and EuroC) didn’t have available information for community and/or outpatient studies.
Instituto de Investigación Nutricional, Lima, Perú
Page 4 of 48
• Dysenteric illness definition o 1 = acceptable (one or more bloody stools ) o 2 = unacceptable (only mucus mixed with stools, others) o 9 = Not provided, unknown.
• Description of definition of diarrhoea or dysentery (written description) • Paper selected for review?
o 1 = Yes o 2 = No
• Country • WHO Region (use codes, 1-14) • Number of subjects studied (or No. stool samples or No. of persons-year studied) • Age group • Male:Female ratio • Number of males/Number of females • Description of Cohort characteristics and age (descriptive information) • Description of surveillance frequency, recall period, selection, etc (descriptive
information) • Type of stool sample studied:
o 1 = fresh stools o 2 = rectal swabs o 3 = both
• Description of timing of stool sampling, transport media used, time period until plates were inoculated, etc. (descriptive information)
• Stool microbiologic methods appropriateness? (samples inoculated into transport media and into plates within 24 h of being passed, laboratory methods acceptable. See methods below)
o 1 = Yes o 2 = No o 9 = unable to classify, lack of information on paper.
• Number of coinfected samples/number of samples tested • Percentage of coinfection
Since frequently more than one enteropathogen is present causing diarrhoea, we considered mixed infections whenever the data were reported.
• Salmonella (excluding S. typhi, treating all other types of Salmonella as one) o % positive (0 means not isolated, 99 means not reported) o number of positive samples o number of stool samples tested o Describe the types of Salmonella isolated (descriptive information)
• Shigella (all types) o % positive, any type (0 means not isolated, 99 not reported) o % positive Shigella dysenteriae (0 means not isolated, 99 means not
reported) o number of positive samples o % positive Shigella flexneri (0 means not isolated, 99 means not reported) o number of positive samples o % positive Shigella boydii (0 means not isolated, 99 means not reported) o number of positive samples
Instituto de Investigación Nutricional, Lima, Perú
Page 5 of 48
o % positive Shigella sonei (0 means not isolated, 99 means not reported) o number of positive samples o number of stool samples tested for any Shigella o Describe the methods for Shigella identification (descriptive information)
• Campylobacter o % positive (0 means not isolated, 99 means not reported) o number of positive samples o number of stool samples tested o Describe the methods for Campylobacter isolation (descriptive
information) • Vibrios
o % positive, any type (0 means not isolated, 99 not reported) o % positive Vibrio cholerae O1 (0 means not isolated, 99 means not
reported) o number of positive samples o % positive Vibrio cholerae O139 (0 means not isolated, 99 means not
reported) o number of positive samples o number of stool samples tested for any Vibrio o Describe the methods for Vibrio identificartion (descriptive information)
• ETEC o % positive, any type (0 means not isolated, 99 not reported) o % positive ETEC ST only (0 means not isolated, 99 means not reported) o number of positive samples o % positive ETEC LT only (0 means not isolated, 99 means not reported) o number of positive samples o % positive ETEC ST/LT only (0 means not isolated, 99 means not
reported) o number of positive samples o number of stool samples tested for any ETEC o Describe the methods for ETEC identification (descriptive information)
• EPEC o % positive EPEC (0 means not isolated, 99 means not reported) o number of positive samples o number of stool samples tested for any EPEC o Describe the methods for EPEC identification (descriptive information)
• Rotavirus o % positive Rotavirus (0 means not isolated, 99 means not reported) o number of positive samples o number of stool samples tested for Rotavirus o Describe the methods for Rotavirus identification (descriptive information)
• Giardia lamblia o % positive Giardia (0 means not isolated, 99 means not reported) o number of positive samples o number of stool samples tested for Giardia o Describe the methods for Giardia identification (descriptive information)
• Cryptosporidium sp. o % positive Cryptosporidium (0 means not isolated, 99 means not reported) o number of positive samples o number of stool samples tested for Cryptosporidium
Instituto de Investigación Nutricional, Lima, Perú
Page 6 of 48
o Describe the methods for Cryptosporidium identification (descriptive information)
• Entamoeba hystolitica (for dysenteric illness only) o % positive E. hystolitica (0 means not isolated, 99 means not reported) o number of positive samples o number of stool samples tested for E. hystolitica in dysenteric cases o Describe the methods for E. hystolitica identification (descriptive
information) As a reference, the following laboratory methods (or acceptable variations that were discussed individually) were considered acceptable, although it was not used as an inclusion or exclusion criteria since not all papers provided detailed laboratory methods information.
• Salmonella/Shigella: SS, XLD, BSA,Hectoen, Selenite enrichment for salmonella. • Campylobacter: transport media with antibiotics (Skirrow´s supplement). Blood
agar (5% sheep blood) with Butzler supplement. Cultivated at 42C and with low oxigen tension or anaerobic chamber
• Vibrios: alkaline peptone water enrichment and subculture at 8 hs into TCBS agar • E coli: MacConkey agar, • ETEC: sondas DNA, cell cultures (Y1, cho cells), ileac loop, mouse model, • EPEC: Hep 2 cell cultures (diffuse, localized, auto aggregative). DNA probes for
EAF plasmid and other plasmids. • Rotavirus: ELISA. Electronic microscopy. • Giardia: MIF, SAF transport media, direct or zinc sulphate concentration. ELISA. • Crypto: MIF, SAF transport media. Modified Ziel Nielsen stain. • Entamoeba hystolitica: MIF, SAF transport media. Direct exam.
Data was entered into the data base for all articles reviewed up to the variable where the decision for inclusion or not into this review was taken. For papers not selected for the review, no further data was entered into the data base. 2.4 Data Analysis Papers selected for the review, satisfying all inclusion criteria and not having any exclusion criteria, were selected from the data base and grouped into two categories:
• Community-based studies • Health-facility studies (separately inpatients and outpatients)
For each of these groups, median percentages and 25% and 75% percentiles were calculated for each pathogen, for children 0-4 years of age. Those papers that provided narrower age groups were treated together with those that provided data for 0-4 yrs of age children.
2.5 Proposed Models
Based on the review of the data available, and after reviewing the natural history of diarrhoeal diseases, we considered a simple model to estimate the burden of diarrhoea, with the components described below. To construct it, we combined information obtained from the literature review, with demographic and health service utilization data available from other
Instituto de Investigación Nutricional, Lima, Perú
Page 7 of 48
sources, most importantly the Demographic and Health Surveys (DHS) conducted worldwide with support from USAID; the Multiple Indicator Cluster Survey (MICS) conducted by Unicef; and other surveys conducted by the CDC, World Bank, Ministries of Health and other national or regional studies provided they all are using the same operational definition. Else, if other regional estimations (incidence, proportion missing in a few regions, and under five mortality rate due to diarrhoea) were needed to complete our data they will be estimated. In doing so, the components and sources to obtain the needed information would be:
1. Number of diarrhoeal disease episodes in children <5 years of age: This is the burden of diarrhoeal episodes at global and regional level. The estimate will be obtained from literature review, applying the median estimate of the incidence rate of diarrhoea obtained from community-based cohort studies2 to the 2000 population of children <5 years of age for the world and for the regions. Whenever the information is missing at regional level it will be estimated modelling known risk factors;
2. Number of diarrhoeal episodes attributable to diarrhoea in children <5 years of age in community: The median proportion of each aetiology of diarrhoeal disease estimated from community-based cohort studies from the literature review for the world and WHO regions will be used and applied to the number of diarrhoeal episodes estimated above;
3. Number of diarrhoeal episodes attributable to enteropathogens seen in outpatient facilities in children <5 years of age: We estimated the number of diarrhoeal episodes seen in outpatient services globally and in each WHO region. Since this information may have important variations amongst countries, even within the same region, we propose to use DHS, MICS and other data to estimate this figure. We will use the proportion of children with diarrhoea in the last two weeks that were seen in health facilities. Though this estimate has seasonal variations, we will apply that percentage to the total number of diarrhoeal estimates obtained above to estimate the number of diarrhoeal episodes seen in health facilities or by private doctors globally and in each region. We then will apply the median proportion of each enterpathogen in diarrhoea cases seen in outpatient facilities globally and on the WHO region, based on our literature review, to estimate the number of specific diarrhoeal episodes seen in outpatient facilities in each level;
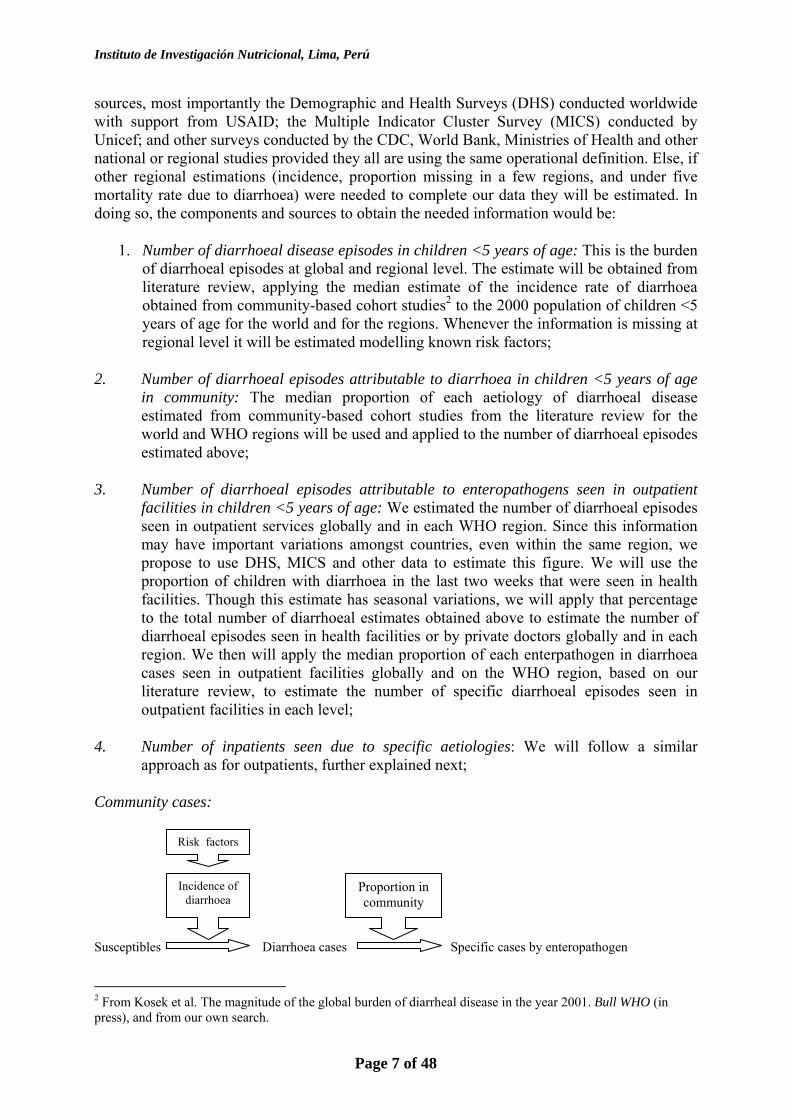
4. Number of inpatients seen due to specific aetiologies: We will follow a similar approach as for outpatients, further explained next;
Community cases: Susceptibles Diarrhoea cases Specific cases by enteropathogen 2 From Kosek et al. The magnitude of the global burden of diarrheal disease in the year 2001. Bull WHO (in press), and from our own search.
Incidence of diarrhoea
Proportion in community
Risk factors
Instituto de Investigación Nutricional, Lima, Perú
Page 8 of 48
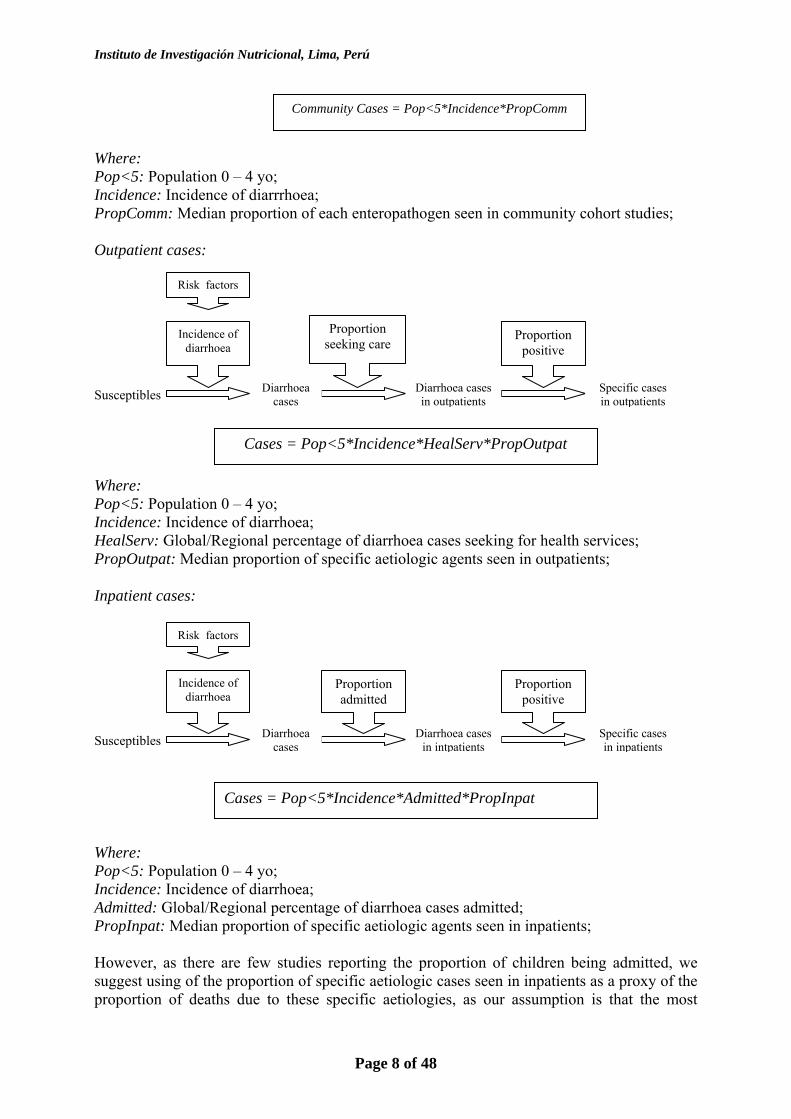
Where: Pop<5: Population 0 – 4 yo; Incidence: Incidence of diarrrhoea; PropComm: Median proportion of each enteropathogen seen in community cohort studies; Outpatient cases: Susceptibles
Where: Pop<5: Population 0 – 4 yo; Incidence: Incidence of diarrhoea; HealServ: Global/Regional percentage of diarrhoea cases seeking for health services; PropOutpat: Median proportion of specific aetiologic agents seen in outpatients; Inpatient cases: Susceptibles
Where: Pop<5: Population 0 – 4 yo; Incidence: Incidence of diarrhoea; Admitted: Global/Regional percentage of diarrhoea cases admitted; PropInpat: Median proportion of specific aetiologic agents seen in inpatients; However, as there are few studies reporting the proportion of children being admitted, we suggest using of the proportion of specific aetiologic cases seen in inpatients as a proxy of the proportion of deaths due to these specific aetiologies, as our assumption is that the most
Incidence of diarrhoea
Proportion seeking care
Diarrhoea cases in outpatients
Diarrhoea cases
Proportion positive
Specific cases in outpatients
Cases = Pop<5*Incidence*HealServ*PropOutpat
Community Cases = Pop<5*Incidence*PropComm
Risk factors
Incidence of diarrhoea
Proportion admitted
Diarrhoea cases in intpatients
Diarrhoea cases
Proportion positive
Specific cases in inpatients
Cases = Pop<5*Incidence*Admitted*PropInpat
Risk factors
Instituto de Investigación Nutricional, Lima, Perú
Page 9 of 48
severe cases get admitted. In so doing, in this report we will advance only to estimate the said proportion of specific aetiologies. This said specific proportion could be further used by us as a proxy of deaths by aetiology once the CHERG releases its new estimation of the annual number of deaths by diarrhoea in <5 yo. So, whilst the expected number of annual deaths to be estimated by the CHERG becomes available, our inpatient model becomes more simple: Susceptibles
According to the above formulae global figures can be readily estimated, but since in some regions some information is missing (incidence, specific proportions in any setting, service use), new estimations based on modelling known risk factors for enteropathogens causing diarrhoea might be calculated to fill the said gaps. 2.6 Population
Table 2. Estimated under five years old world population for year 2000
WHO Region population
AfroD 48,432,770 AfroE 57,195,691 AmroA 21,585,736 AmroB 44,814,382 AmroD 9,381,213 EmroB 16,421,557 EmroD 53,344,704 EuroA 21,535,945 EuroB 17,946,351 EuroC 12,475,780 SearoB 28,408,345 SearoD 140,336,521 WproA 8,070,921 WproB 124,981,979 Total 604,931,894
Source: WHO 3. Results 3.1 Global estimations
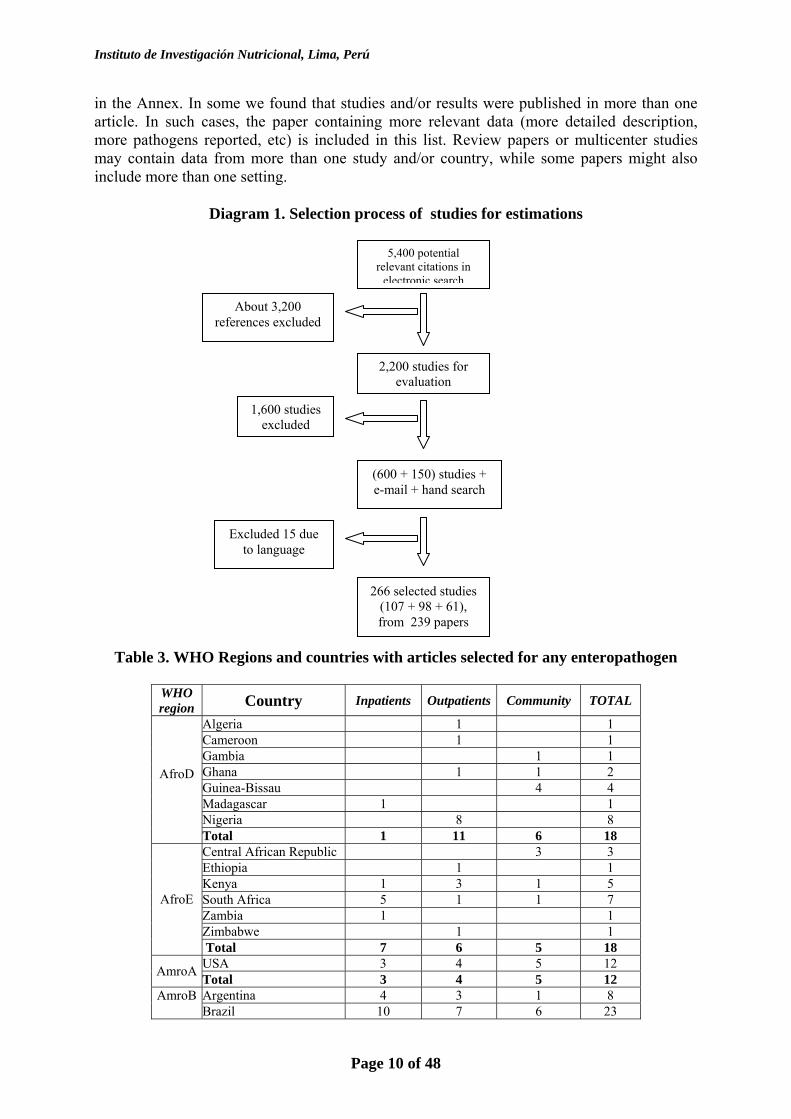
3.1.1 Articles selected
Search of the literature yielded 266 studies from 239 papers that met the inclusion criteria and none of the exclusion criteria, published in the period under study, with data on the proportion of diarrhoea due to any of the relevant enteropathogens. These articles represent at least one study in at least one of the three settings in 69 countries (36% of 191 countries), and are listed
Risk factors
Specific proportion positive hospitalized
Specific deaths by aetiolgy
Annual diarrhoea
deaths This Report
Instituto de Investigación Nutricional, Lima, Perú
Page 10 of 48
in the Annex. In some we found that studies and/or results were published in more than one article. In such cases, the paper containing more relevant data (more detailed description, more pathogens reported, etc) is included in this list. Review papers or multicenter studies may contain data from more than one study and/or country, while some papers might also include more than one setting.
Diagram 1. Selection process of studies for estimations
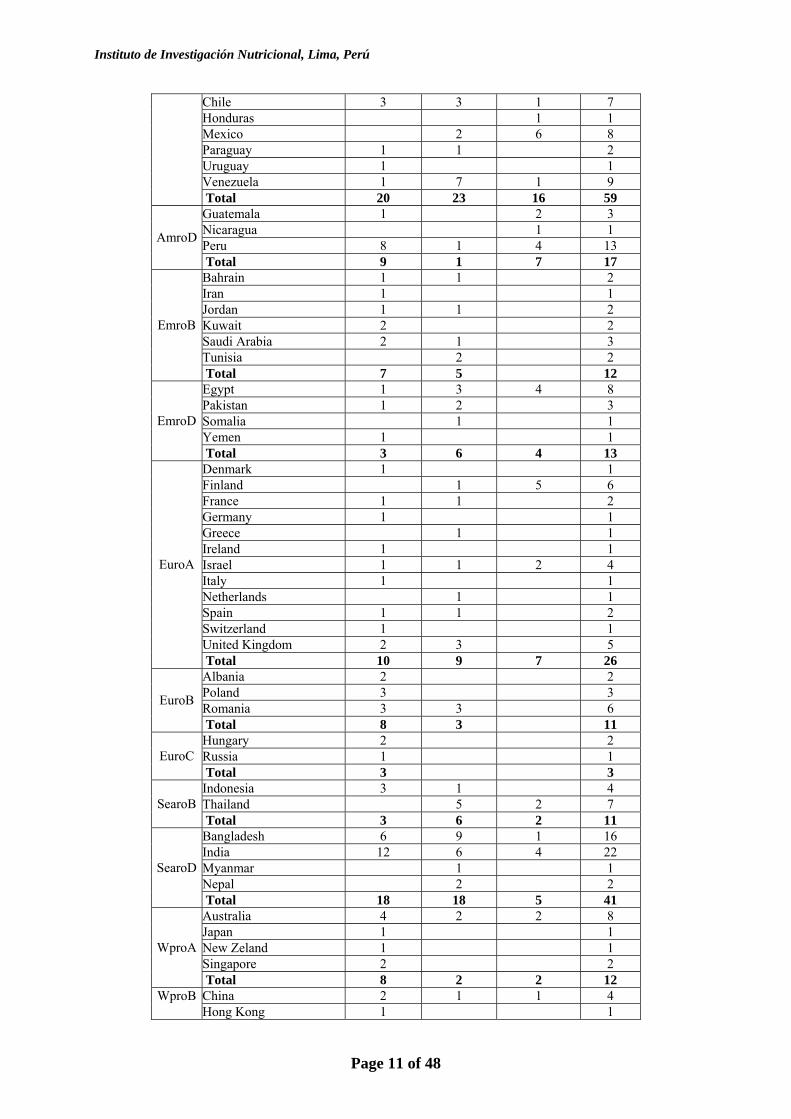
Table 3. WHO Regions and countries with articles selected for any enteropathogen
WHO region Country Inpatients Outpatients Community TOTAL
Algeria 1 1 Cameroon 1 1 Gambia 1 1 Ghana 1 1 2 Guinea-Bissau 4 4 Madagascar 1 1 Nigeria 8 8
AfroD Total 1 11 6 18
Central African Republic 3 3 Ethiopia 1 1 Kenya 1 3 1 5 South Africa 5 1 1 7 Zambia 1 1 Zimbabwe 1 1
AfroE
Total 7 6 5 18 USA 3 4 5 12 AmroA Total 3 4 5 12 Argentina 4 3 1 8 AmroB Brazil 10 7 6 23
5,400 potential relevant citations in
electronic search
About 3,200 references excluded
2,200 studies for evaluation
Excluded 15 due to language
(600 + 150) studies + e-mail + hand search
1,600 studies excluded
266 selected studies (107 + 98 + 61), from 239 papers
Instituto de Investigación Nutricional, Lima, Perú
Page 11 of 48
Chile 3 3 1 7 Honduras 1 1 Mexico 2 6 8 Paraguay 1 1 2 Uruguay 1 1 Venezuela 1 7 1 9 Total 20 23 16 59 Guatemala 1 2 3 Nicaragua 1 1 Peru 8 1 4 13 AmroD
Total 9 1 7 17 Bahrain 1 1 2 Iran 1 1 Jordan 1 1 2 Kuwait 2 2 Saudi Arabia 2 1 3 Tunisia 2 2
EmroB
Total 7 5 12 Egypt 1 3 4 8 Pakistan 1 2 3 Somalia 1 1 Yemen 1 1
EmroD
Total 3 6 4 13 Denmark 1 1 Finland 1 5 6 France 1 1 2 Germany 1 1 Greece 1 1 Ireland 1 1 Israel 1 1 2 4 Italy 1 1 Netherlands 1 1 Spain 1 1 2 Switzerland 1 1 United Kingdom 2 3 5
EuroA
Total 10 9 7 26 Albania 2 2 Poland 3 3 Romania 3 3 6 EuroB
Total 8 3 11 Hungary 2 2 Russia 1 1 EuroC Total 3 3 Indonesia 3 1 4 Thailand 5 2 7 SearoB Total 3 6 2 11 Bangladesh 6 9 1 16 India 12 6 4 22 Myanmar 1 1 Nepal 2 2
SearoD
Total 18 18 5 41 Australia 4 2 2 8 Japan 1 1 New Zeland 1 1 Singapore 2 2
WproA
Total 8 2 2 12 China 2 1 1 4 WproB Hong Kong 1 1
Instituto de Investigación Nutricional, Lima, Perú
Page 12 of 48
Korea 2 2 Lao PDR 1 1 Malaysia 1 1 Papua New Guinea 1 1 Vietnam 1 2 3 Total 7 4 2 13
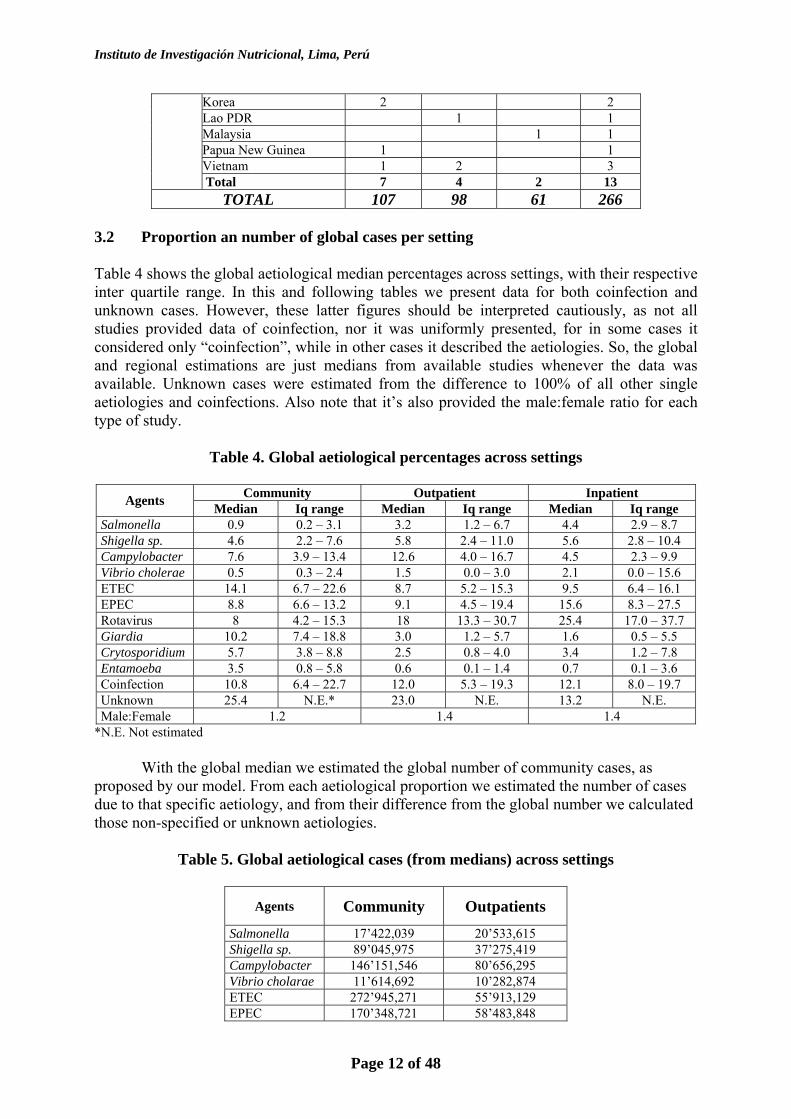
TOTAL 107 98 61 266 3.2 Proportion an number of global cases per setting Table 4 shows the global aetiological median percentages across settings, with their respective inter quartile range. In this and following tables we present data for both coinfection and unknown cases. However, these latter figures should be interpreted cautiously, as not all studies provided data of coinfection, nor it was uniformly presented, for in some cases it considered only “coinfection”, while in other cases it described the aetiologies. So, the global and regional estimations are just medians from available studies whenever the data was available. Unknown cases were estimated from the difference to 100% of all other single aetiologies and coinfections. Also note that it’s also provided the male:female ratio for each type of study.
Table 4. Global aetiological percentages across settings
Community Outpatient Inpatient Agents Median Iq range Median Iq range Median Iq range Salmonella 0.9 0.2 – 3.1 3.2 1.2 – 6.7 4.4 2.9 – 8.7 Shigella sp. 4.6 2.2 – 7.6 5.8 2.4 – 11.0 5.6 2.8 – 10.4 Campylobacter 7.6 3.9 – 13.4 12.6 4.0 – 16.7 4.5 2.3 – 9.9 Vibrio cholerae 0.5 0.3 – 2.4 1.5 0.0 – 3.0 2.1 0.0 – 15.6 ETEC 14.1 6.7 – 22.6 8.7 5.2 – 15.3 9.5 6.4 – 16.1 EPEC 8.8 6.6 – 13.2 9.1 4.5 – 19.4 15.6 8.3 – 27.5 Rotavirus 8 4.2 – 15.3 18 13.3 – 30.7 25.4 17.0 – 37.7 Giardia 10.2 7.4 – 18.8 3.0 1.2 – 5.7 1.6 0.5 – 5.5 Crytosporidium 5.7 3.8 – 8.8 2.5 0.8 – 4.0 3.4 1.2 – 7.8 Entamoeba 3.5 0.8 – 5.8 0.6 0.1 – 1.4 0.7 0.1 – 3.6 Coinfection 10.8 6.4 – 22.7 12.0 5.3 – 19.3 12.1 8.0 – 19.7 Unknown 25.4 N.E.* 23.0 N.E. 13.2 N.E. Male:Female 1.2 1.4 1.4
*N.E. Not estimated
With the global median we estimated the global number of community cases, as proposed by our model. From each aetiological proportion we estimated the number of cases due to that specific aetiology, and from their difference from the global number we calculated those non-specified or unknown aetiologies.
Table 5. Global aetiological cases (from medians) across settings
Agents Community Outpatients
Salmonella 17’422,039 20’533,615 Shigella sp. 89’045,975 37’275,419 Campylobacter 146’151,546 80’656,295 Vibrio cholarae 11’614,692 10’282,874 ETEC 272’945,271 55’913,129 EPEC 170’348,721 58’483,848
Instituto de Investigación Nutricional, Lima, Perú
Page 13 of 48
Rotavirus 154’862,565 115’682,336 Giardia 196’481,879 19’280,389 Crytosporidium 110’339,577 16’131,259 Entamoeba 67’752,372 3’856,078 Coinfection 208’096,572 76’800,217 Unknown 491’688,643 147’816,318
3.2.1 Number of diarrhoeal episodes at the community level by cause for the year 2000
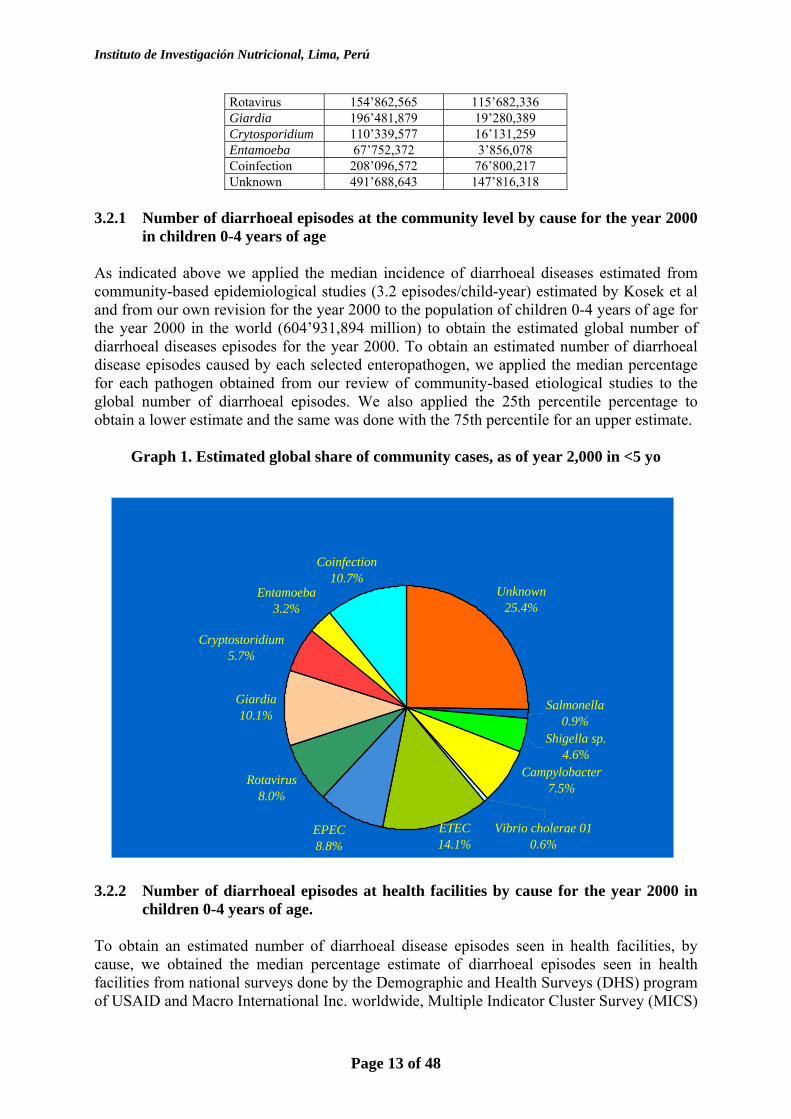
in children 0-4 years of age As indicated above we applied the median incidence of diarrhoeal diseases estimated from community-based epidemiological studies (3.2 episodes/child-year) estimated by Kosek et al and from our own revision for the year 2000 to the population of children 0-4 years of age for the year 2000 in the world (604’931,894 million) to obtain the estimated global number of diarrhoeal diseases episodes for the year 2000. To obtain an estimated number of diarrhoeal disease episodes caused by each selected enteropathogen, we applied the median percentage for each pathogen obtained from our review of community-based etiological studies to the global number of diarrhoeal episodes. We also applied the 25th percentile percentage to obtain a lower estimate and the same was done with the 75th percentile for an upper estimate.
Graph 1. Estimated global share of community cases, as of year 2,000 in <5 yo
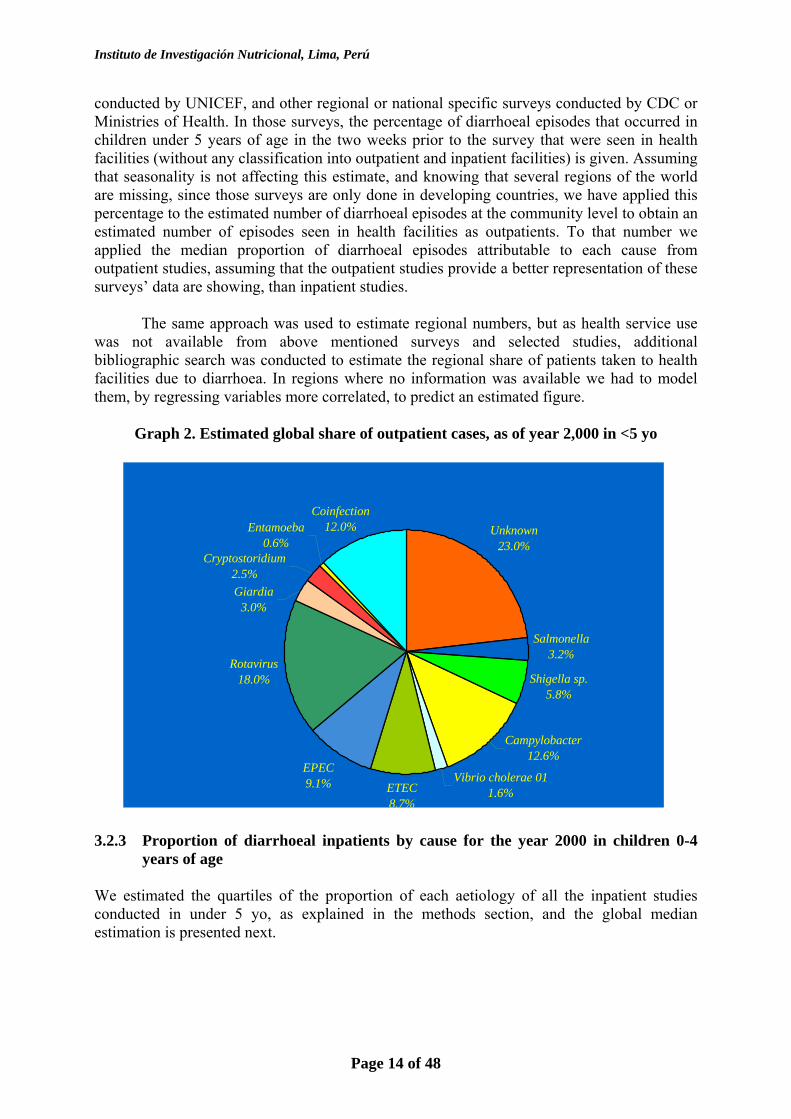
3.2.2 Number of diarrhoeal episodes at health facilities by cause for the year 2000 in
children 0-4 years of age. To obtain an estimated number of diarrhoeal disease episodes seen in health facilities, by cause, we obtained the median percentage estimate of diarrhoeal episodes seen in health facilities from national surveys done by the Demographic and Health Surveys (DHS) program of USAID and Macro International Inc. worldwide, Multiple Indicator Cluster Survey (MICS)
Unknown25.4%
EPEC8.8%
Rotavirus 8.0%
Giardia10.1%
ETEC14.1%
Vibrio cholerae 010.6%
Cryptostoridium5.7%
Campylobacter7.5%
Shigella sp. 4.6%
Salmonella0.9%
Entamoeba 3.2%
Coinfection10.7%
Instituto de Investigación Nutricional, Lima, Perú
Page 14 of 48
conducted by UNICEF, and other regional or national specific surveys conducted by CDC or Ministries of Health. In those surveys, the percentage of diarrhoeal episodes that occurred in children under 5 years of age in the two weeks prior to the survey that were seen in health facilities (without any classification into outpatient and inpatient facilities) is given. Assuming that seasonality is not affecting this estimate, and knowing that several regions of the world are missing, since those surveys are only done in developing countries, we have applied this percentage to the estimated number of diarrhoeal episodes at the community level to obtain an estimated number of episodes seen in health facilities as outpatients. To that number we applied the median proportion of diarrhoeal episodes attributable to each cause from outpatient studies, assuming that the outpatient studies provide a better representation of these surveys’ data are showing, than inpatient studies.
The same approach was used to estimate regional numbers, but as health service use was not available from above mentioned surveys and selected studies, additional bibliographic search was conducted to estimate the regional share of patients taken to health facilities due to diarrhoea. In regions where no information was available we had to model them, by regressing variables more correlated, to predict an estimated figure.
Graph 2. Estimated global share of outpatient cases, as of year 2,000 in <5 yo
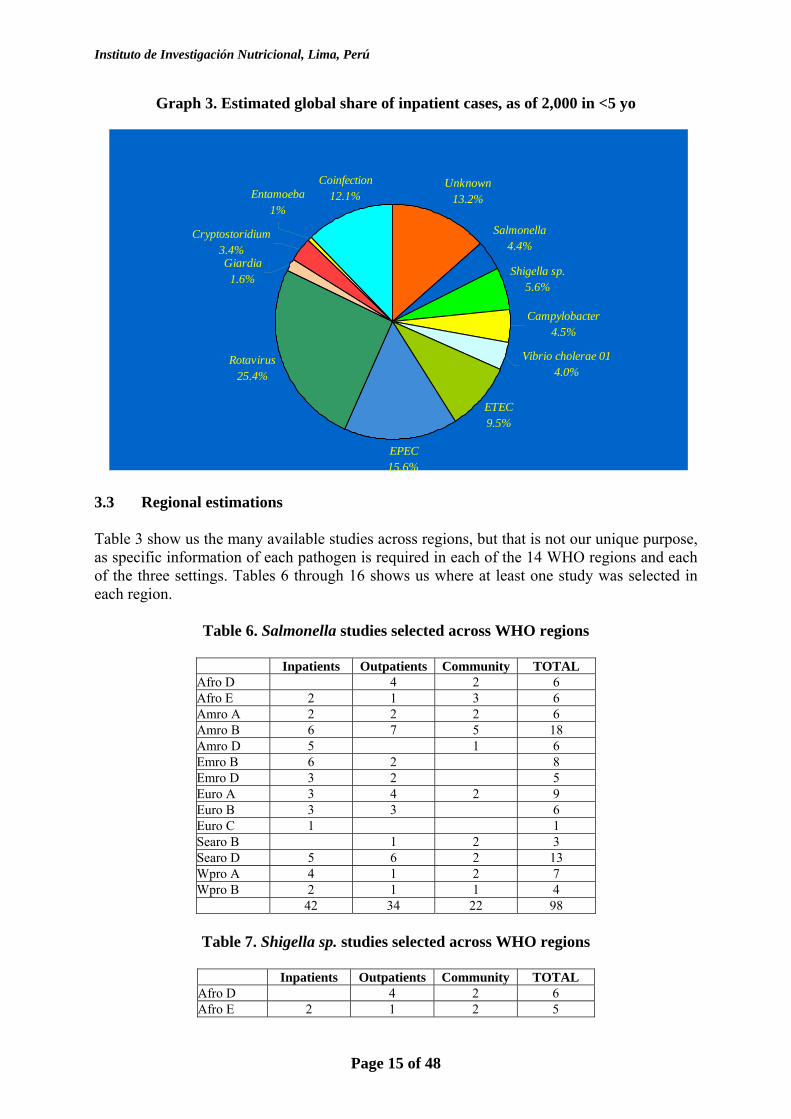
3.2.3 Proportion of diarrhoeal inpatients by cause for the year 2000 in children 0-4
years of age We estimated the quartiles of the proportion of each aetiology of all the inpatient studies conducted in under 5 yo, as explained in the methods section, and the global median estimation is presented next.
Unknown23.0%
Salmonella3.2%
Shigella sp. 5.8%
Campylobacter12.6%
Vibrio cholerae 011.6%ETEC
8.7%
EPEC9.1%
Rotavirus 18.0%
Coinfection12.0%Entamoeba
0.6%Cryptostoridium
2.5%Giardia
3.0%
Instituto de Investigación Nutricional, Lima, Perú
Page 15 of 48
Graph 3. Estimated global share of inpatient cases, as of 2,000 in <5 yo
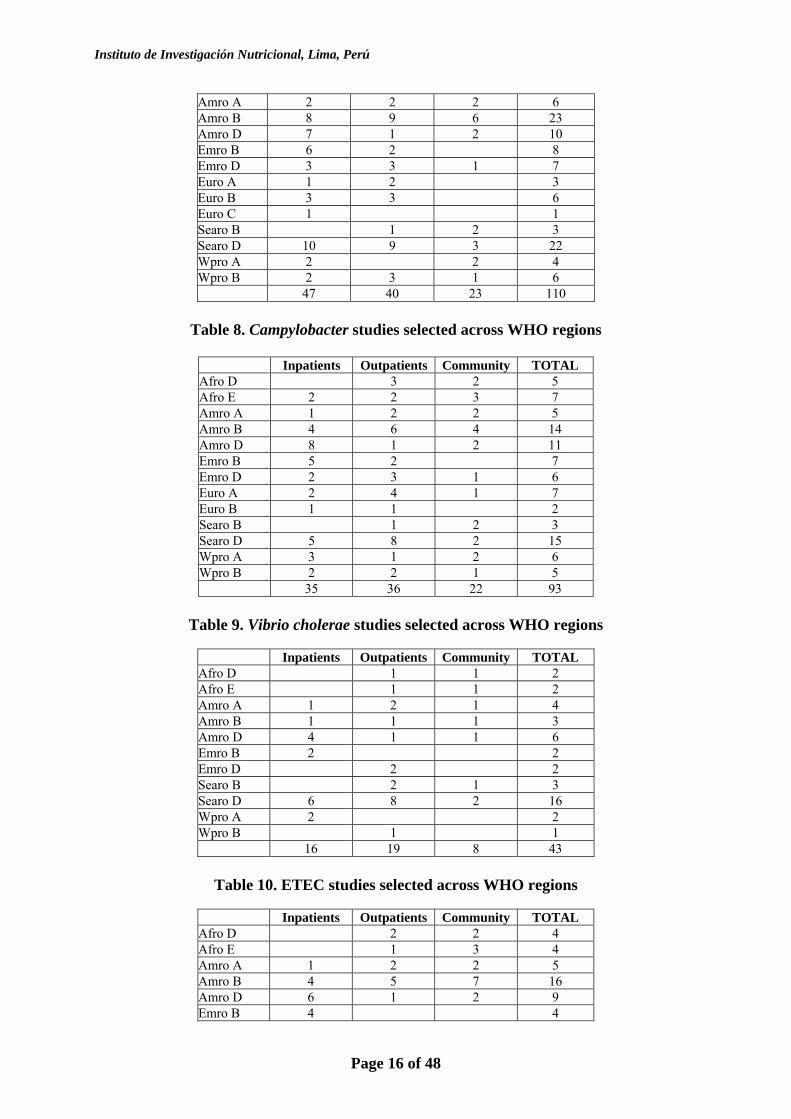
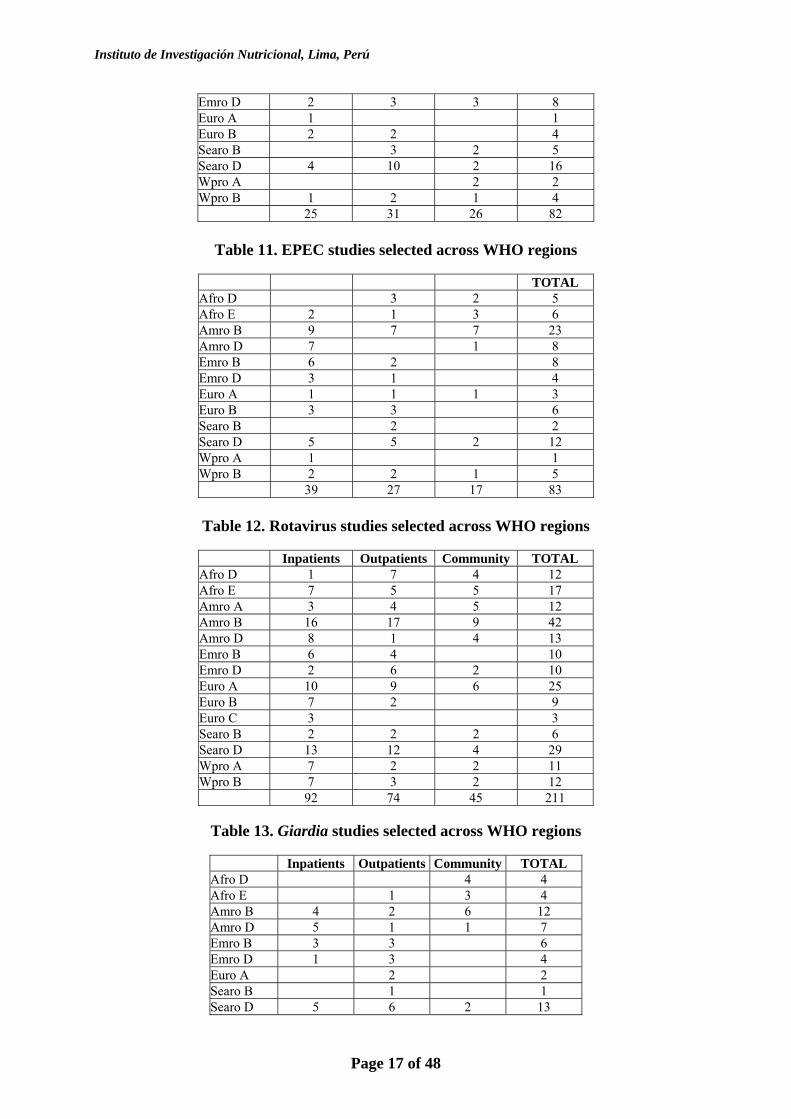
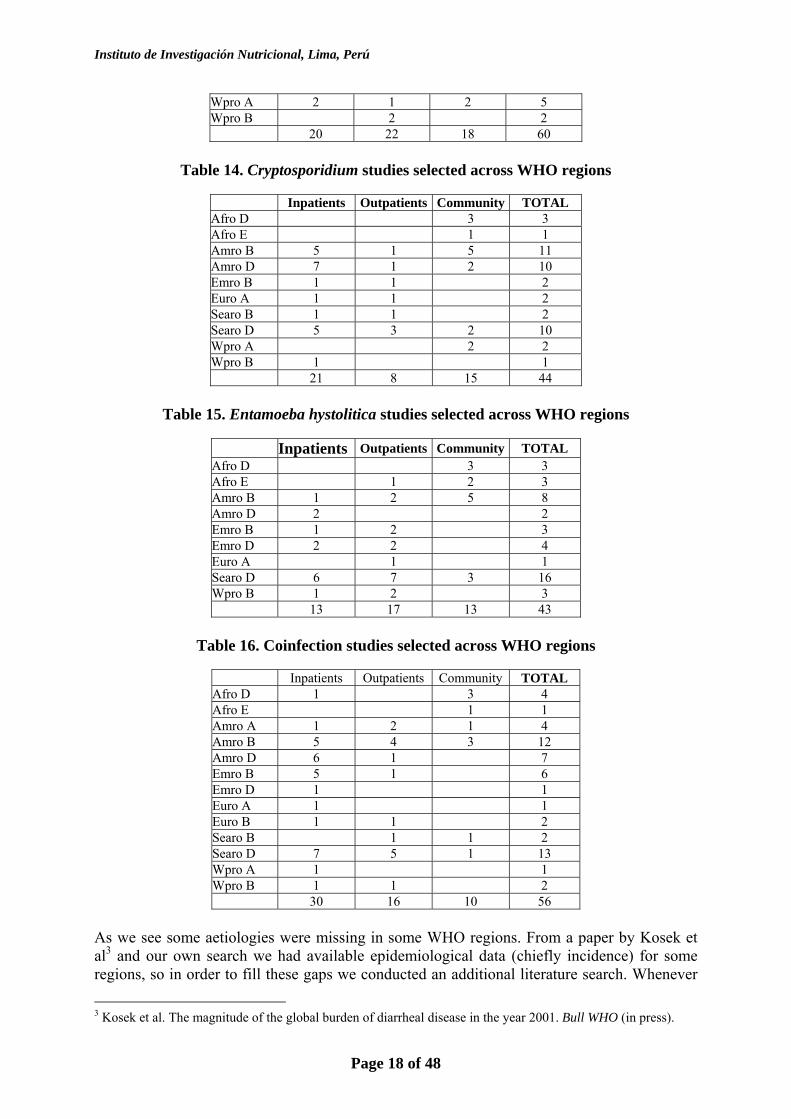
3.3 Regional estimations Table 3 show us the many available studies across regions, but that is not our unique purpose, as specific information of each pathogen is required in each of the 14 WHO regions and each of the three settings. Tables 6 through 16 shows us where at least one study was selected in each region.
Table 6. Salmonella studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 4 2 6 Afro E 2 1 3 6 Amro A 2 2 2 6 Amro B 6 7 5 18 Amro D 5 1 6 Emro B 6 2 8 Emro D 3 2 5 Euro A 3 4 2 9 Euro B 3 3 6 Euro C 1 1 Searo B 1 2 3 Searo D 5 6 2 13 Wpro A 4 1 2 7 Wpro B 2 1 1 4 42 34 22 98
Table 7. Shigella sp. studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 4 2 6 Afro E 2 1 2 5
Unknown13.2%
Salmonella4.4%
Shigella sp. 5.6%
Campylobacter4.5%
Vibrio cholerae 014.0%
ETEC9.5%
EPEC15.6%
Rotavirus 25.4%
Coinfection12.1%
Giardia1.6%
Entamoeba 1%
Cryptostoridium3.4%
Instituto de Investigación Nutricional, Lima, Perú
Page 16 of 48
Amro A 2 2 2 6 Amro B 8 9 6 23 Amro D 7 1 2 10 Emro B 6 2 8 Emro D 3 3 1 7 Euro A 1 2 3 Euro B 3 3 6 Euro C 1 1 Searo B 1 2 3 Searo D 10 9 3 22 Wpro A 2 2 4 Wpro B 2 3 1 6 47 40 23 110
Table 8. Campylobacter studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 3 2 5 Afro E 2 2 3 7 Amro A 1 2 2 5 Amro B 4 6 4 14 Amro D 8 1 2 11 Emro B 5 2 7 Emro D 2 3 1 6 Euro A 2 4 1 7 Euro B 1 1 2 Searo B 1 2 3 Searo D 5 8 2 15 Wpro A 3 1 2 6 Wpro B 2 2 1 5 35 36 22 93
Table 9. Vibrio cholerae studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 1 1 2 Afro E 1 1 2 Amro A 1 2 1 4 Amro B 1 1 1 3 Amro D 4 1 1 6 Emro B 2 2 Emro D 2 2 Searo B 2 1 3 Searo D 6 8 2 16 Wpro A 2 2 Wpro B 1 1 16 19 8 43
Table 10. ETEC studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 2 2 4 Afro E 1 3 4 Amro A 1 2 2 5 Amro B 4 5 7 16 Amro D 6 1 2 9 Emro B 4 4
Instituto de Investigación Nutricional, Lima, Perú
Page 17 of 48
Emro D 2 3 3 8 Euro A 1 1 Euro B 2 2 4 Searo B 3 2 5 Searo D 4 10 2 16 Wpro A 2 2 Wpro B 1 2 1 4 25 31 26 82
Table 11. EPEC studies selected across WHO regions
TOTAL Afro D 3 2 5 Afro E 2 1 3 6 Amro B 9 7 7 23 Amro D 7 1 8 Emro B 6 2 8 Emro D 3 1 4 Euro A 1 1 1 3 Euro B 3 3 6 Searo B 2 2 Searo D 5 5 2 12 Wpro A 1 1 Wpro B 2 2 1 5 39 27 17 83
Table 12. Rotavirus studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 1 7 4 12 Afro E 7 5 5 17 Amro A 3 4 5 12 Amro B 16 17 9 42 Amro D 8 1 4 13 Emro B 6 4 10 Emro D 2 6 2 10 Euro A 10 9 6 25 Euro B 7 2 9 Euro C 3 3 Searo B 2 2 2 6 Searo D 13 12 4 29 Wpro A 7 2 2 11 Wpro B 7 3 2 12 92 74 45 211
Table 13. Giardia studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 4 4 Afro E 1 3 4 Amro B 4 2 6 12 Amro D 5 1 1 7 Emro B 3 3 6 Emro D 1 3 4 Euro A 2 2 Searo B 1 1 Searo D 5 6 2 13
Instituto de Investigación Nutricional, Lima, Perú
Page 18 of 48
Wpro A 2 1 2 5 Wpro B 2 2 20 22 18 60
Table 14. Cryptosporidium studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 3 3 Afro E 1 1 Amro B 5 1 5 11 Amro D 7 1 2 10 Emro B 1 1 2 Euro A 1 1 2 Searo B 1 1 2 Searo D 5 3 2 10 Wpro A 2 2 Wpro B 1 1 21 8 15 44
Table 15. Entamoeba hystolitica studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 3 3 Afro E 1 2 3 Amro B 1 2 5 8 Amro D 2 2 Emro B 1 2 3 Emro D 2 2 4 Euro A 1 1 Searo D 6 7 3 16 Wpro B 1 2 3 13 17 13 43
Table 16. Coinfection studies selected across WHO regions
Inpatients Outpatients Community TOTAL Afro D 1 3 4 Afro E 1 1 Amro A 1 2 1 4 Amro B 5 4 3 12 Amro D 6 1 7 Emro B 5 1 6 Emro D 1 1 Euro A 1 1 Euro B 1 1 2 Searo B 1 1 2 Searo D 7 5 1 13 Wpro A 1 1 Wpro B 1 1 2 30 16 10 56
As we see some aetiologies were missing in some WHO regions. From a paper by Kosek et al3 and our own search we had available epidemiological data (chiefly incidence) for some regions, so in order to fill these gaps we conducted an additional literature search. Whenever
3 Kosek et al. The magnitude of the global burden of diarrheal disease in the year 2001. Bull WHO (in press).
Instituto de Investigación Nutricional, Lima, Perú
Page 19 of 48
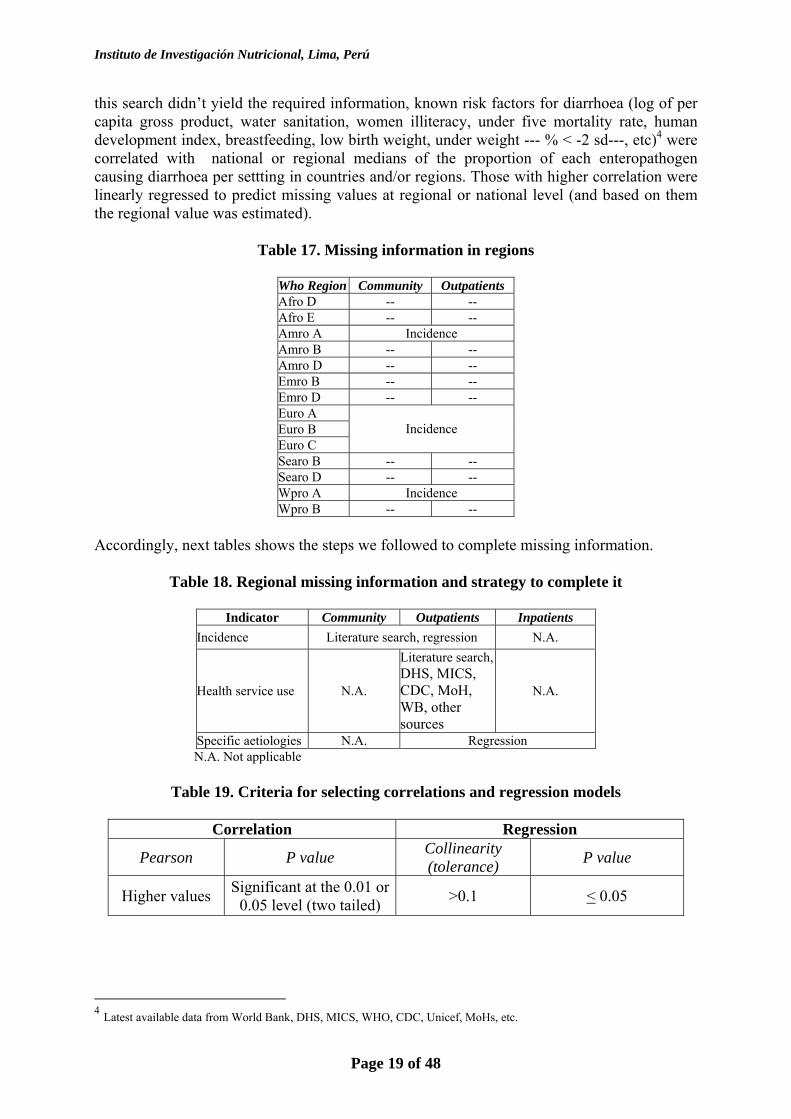
this search didn’t yield the required information, known risk factors for diarrhoea (log of per capita gross product, water sanitation, women illiteracy, under five mortality rate, human development index, breastfeeding, low birth weight, under weight --- % < -2 sd---, etc)4 were correlated with national or regional medians of the proportion of each enteropathogen causing diarrhoea per settting in countries and/or regions. Those with higher correlation were linearly regressed to predict missing values at regional or national level (and based on them the regional value was estimated).
Table 17. Missing information in regions
Who Region Community Outpatients Afro D -- -- Afro E -- -- Amro A Incidence Amro B -- -- Amro D -- -- Emro B -- -- Emro D -- -- Euro A Euro B Euro C
Incidence
Searo B -- -- Searo D -- -- Wpro A Incidence Wpro B -- --
Accordingly, next tables shows the steps we followed to complete missing information.
Table 18. Regional missing information and strategy to complete it
Indicator Community Outpatients Inpatients Incidence Literature search, regression N.A.
Health service use N.A.
Literature search, DHS, MICS, CDC, MoH, WB, other sources
N.A.
Specific aetiologies N.A. Regression N.A. Not applicable
Table 19. Criteria for selecting correlations and regression models
Correlation Regression
Pearson P value Collinearity (tolerance) P value
Higher values Significant at the 0.01 or 0.05 level (two tailed) >0.1 < 0.05
4 Latest available data from World Bank, DHS, MICS, WHO, CDC, Unicef, MoHs, etc.
Instituto de Investigación Nutricional, Lima, Perú
Page 20 of 48
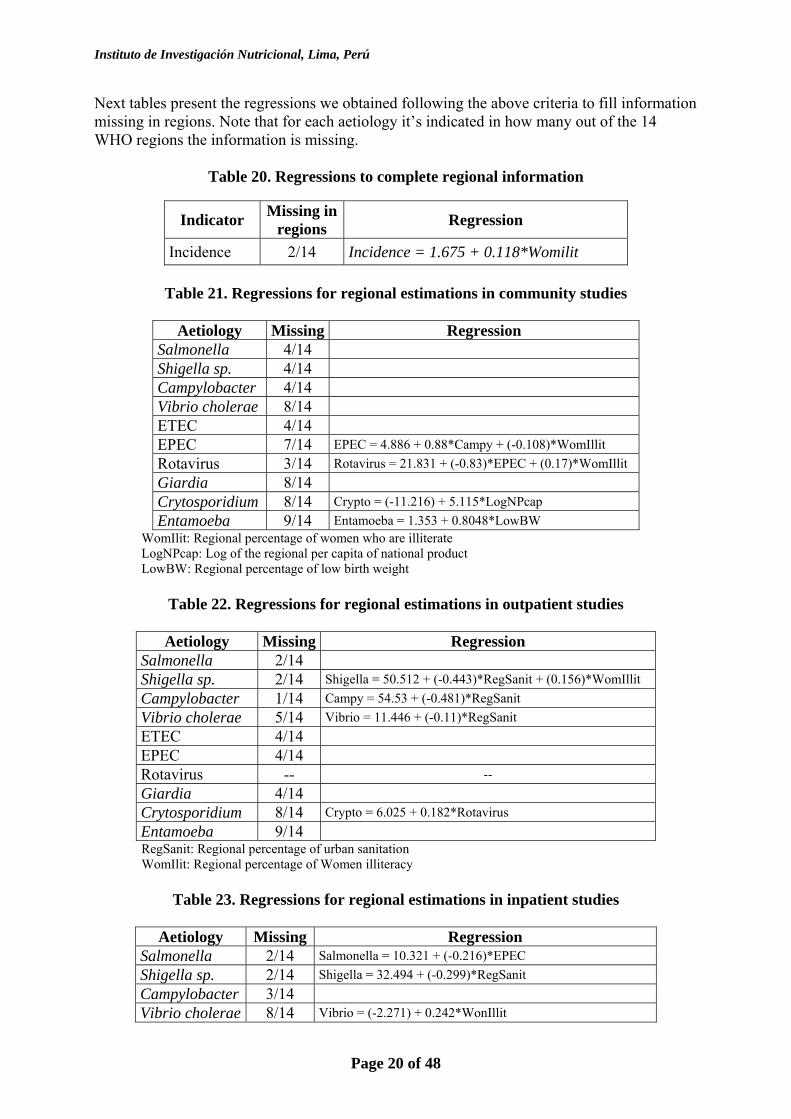
Next tables present the regressions we obtained following the above criteria to fill information missing in regions. Note that for each aetiology it’s indicated in how many out of the 14 WHO regions the information is missing.
Table 20. Regressions to complete regional information
Indicator Missing in regions Regression
Incidence 2/14 Incidence = 1.675 + 0.118*Womilit
Table 21. Regressions for regional estimations in community studies
Aetiology Missing Regression Salmonella 4/14 Shigella sp. 4/14 Campylobacter 4/14 Vibrio cholerae 8/14 ETEC 4/14 EPEC 7/14 EPEC = 4.886 + 0.88*Campy + (-0.108)*WomIllit Rotavirus 3/14 Rotavirus = 21.831 + (-0.83)*EPEC + (0.17)*WomIllit Giardia 8/14 Crytosporidium 8/14 Crypto = (-11.216) + 5.115*LogNPcap Entamoeba 9/14 Entamoeba = 1.353 + 0.8048*LowBW
WomIlit: Regional percentage of women who are illiterate LogNPcap: Log of the regional per capita of national product LowBW: Regional percentage of low birth weight
Table 22. Regressions for regional estimations in outpatient studies
Aetiology Missing Regression
Salmonella 2/14 Shigella sp. 2/14 Shigella = 50.512 + (-0.443)*RegSanit + (0.156)*WomIllit Campylobacter 1/14 Campy = 54.53 + (-0.481)*RegSanit Vibrio cholerae 5/14 Vibrio = 11.446 + (-0.11)*RegSanit ETEC 4/14 EPEC 4/14 Rotavirus -- -- Giardia 4/14 Crytosporidium 8/14 Crypto = 6.025 + 0.182*Rotavirus Entamoeba 9/14
RegSanit: Regional percentage of urban sanitation WomIlit: Regional percentage of Women illiteracy
Table 23. Regressions for regional estimations in inpatient studies
Aetiology Missing Regression Salmonella 2/14 Salmonella = 10.321 + (-0.216)*EPEC Shigella sp. 2/14 Shigella = 32.494 + (-0.299)*RegSanit Campylobacter 3/14 Vibrio cholerae 8/14 Vibrio = (-2.271) + 0.242*WonIllit
Instituto de Investigación Nutricional, Lima, Perú
Page 21 of 48
ETEC 5/14 ETEC = 6.049 + 0.362*BreastFed + (-0.557)*LowBW EPEC 4/14 EPEC = 19.088 + 0.886*LowBW + (-0.55)*Rotavirus Rotavirus -- -- Giardia 7/14 Crytosporidium 7/14 Entamoeba 8/14 Entamoeba = (-28.746) + 10.389*LogNPcap RegSanit: Regional percentage of urban sanitation
WomIlit: Regional percentage of Women illiteracy BreastFed: Regional percentage of children exclusively breast fed in first 6 months
LowBW: Regional percentage of low birth weight LogNPcap: Log of the regional per capita of national product
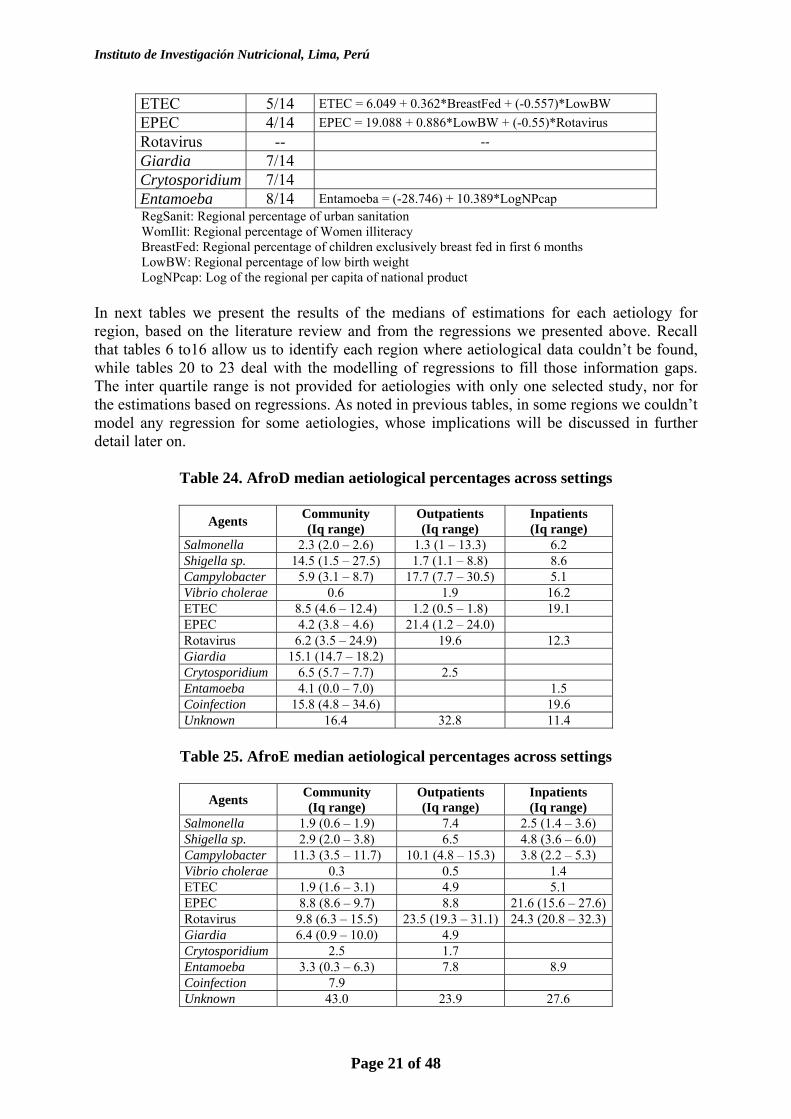
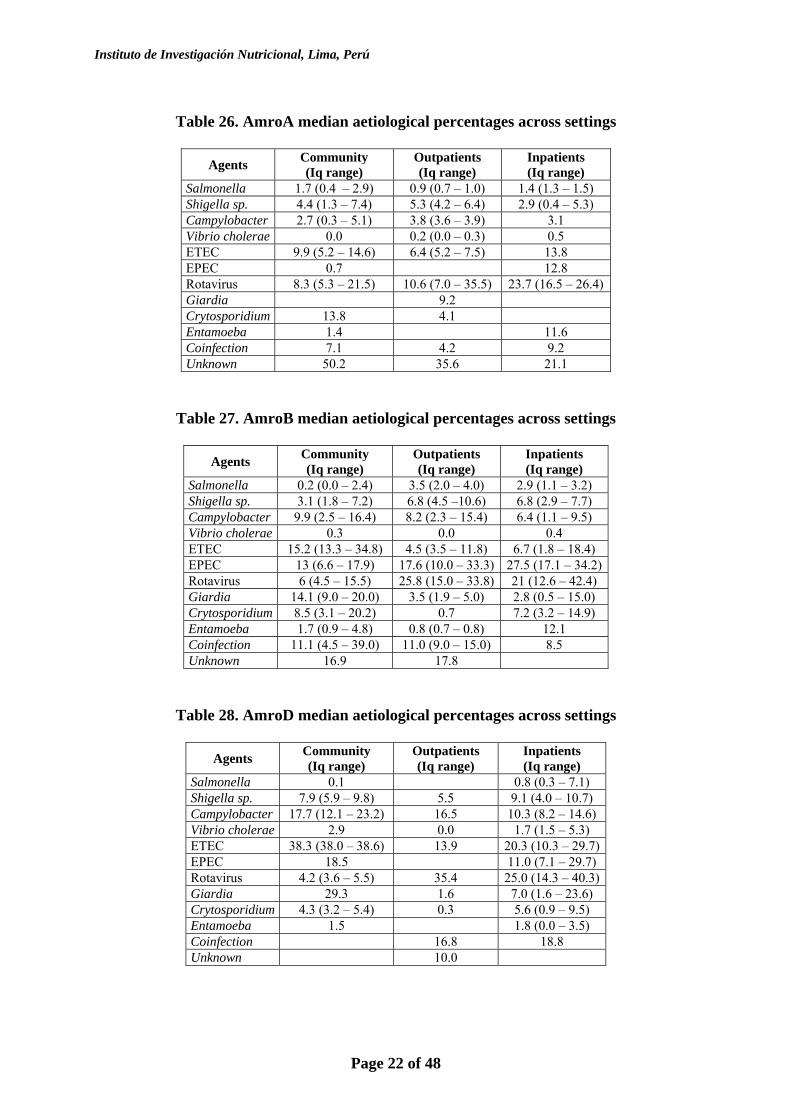
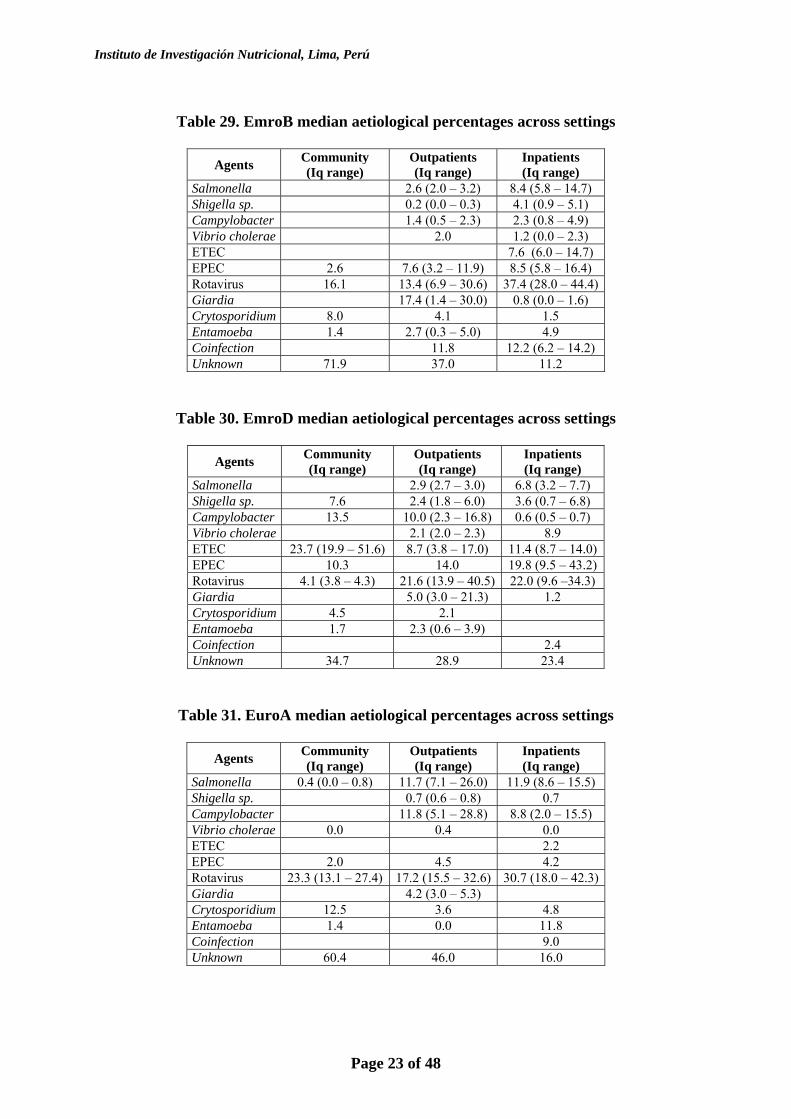
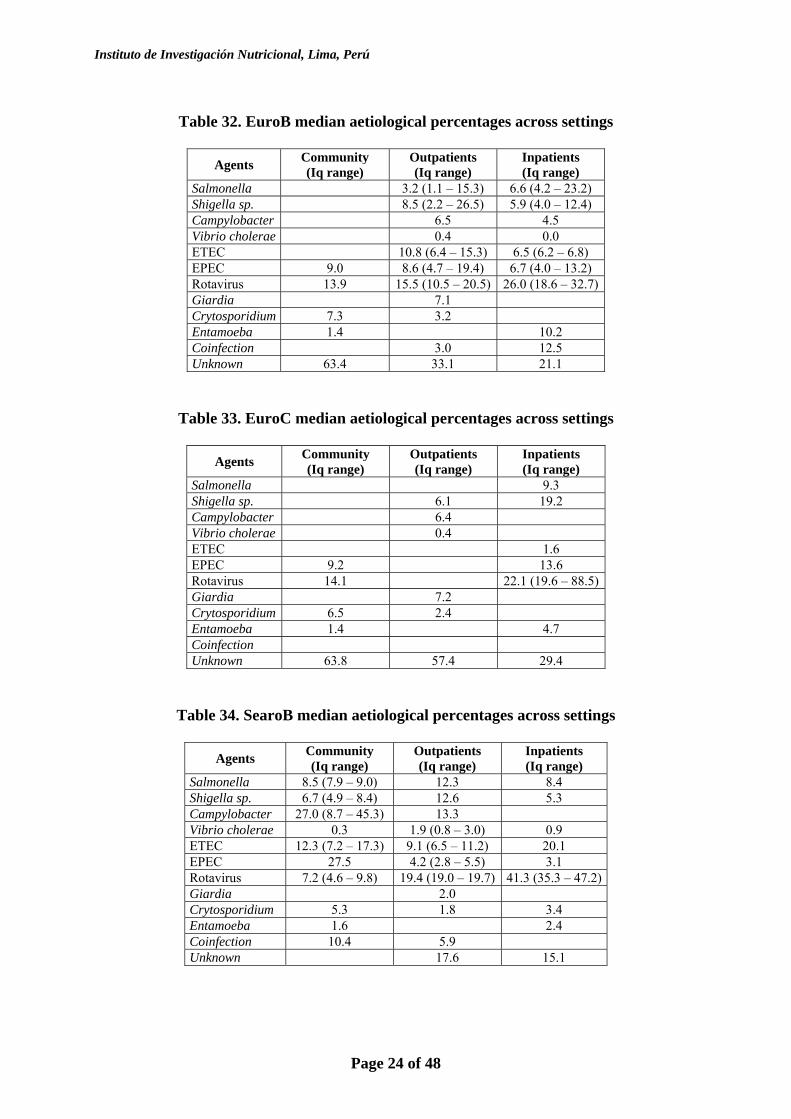
In next tables we present the results of the medians of estimations for each aetiology for region, based on the literature review and from the regressions we presented above. Recall that tables 6 to16 allow us to identify each region where aetiological data couldn’t be found, while tables 20 to 23 deal with the modelling of regressions to fill those information gaps. The inter quartile range is not provided for aetiologies with only one selected study, nor for the estimations based on regressions. As noted in previous tables, in some regions we couldn’t model any regression for some aetiologies, whose implications will be discussed in further detail later on.
Table 24. AfroD median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 2.3 (2.0 – 2.6) 1.3 (1 – 13.3) 6.2 Shigella sp. 14.5 (1.5 – 27.5) 1.7 (1.1 – 8.8) 8.6 Campylobacter 5.9 (3.1 – 8.7) 17.7 (7.7 – 30.5) 5.1 Vibrio cholerae 0.6 1.9 16.2 ETEC 8.5 (4.6 – 12.4) 1.2 (0.5 – 1.8) 19.1 EPEC 4.2 (3.8 – 4.6) 21.4 (1.2 – 24.0) Rotavirus 6.2 (3.5 – 24.9) 19.6 12.3 Giardia 15.1 (14.7 – 18.2) Crytosporidium 6.5 (5.7 – 7.7) 2.5 Entamoeba 4.1 (0.0 – 7.0) 1.5 Coinfection 15.8 (4.8 – 34.6) 19.6 Unknown 16.4 32.8 11.4
Table 25. AfroE median aetiological percentages across settings
Agents Community
(Iq range) Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 1.9 (0.6 – 1.9) 7.4 2.5 (1.4 – 3.6) Shigella sp. 2.9 (2.0 – 3.8) 6.5 4.8 (3.6 – 6.0) Campylobacter 11.3 (3.5 – 11.7) 10.1 (4.8 – 15.3) 3.8 (2.2 – 5.3) Vibrio cholerae 0.3 0.5 1.4 ETEC 1.9 (1.6 – 3.1) 4.9 5.1 EPEC 8.8 (8.6 – 9.7) 8.8 21.6 (15.6 – 27.6) Rotavirus 9.8 (6.3 – 15.5) 23.5 (19.3 – 31.1) 24.3 (20.8 – 32.3) Giardia 6.4 (0.9 – 10.0) 4.9 Crytosporidium 2.5 1.7 Entamoeba 3.3 (0.3 – 6.3) 7.8 8.9 Coinfection 7.9 Unknown 43.0 23.9 27.6
Instituto de Investigación Nutricional, Lima, Perú
Page 22 of 48
Table 26. AmroA median aetiological percentages across settings
Agents Community
(Iq range) Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 1.7 (0.4 – 2.9) 0.9 (0.7 – 1.0) 1.4 (1.3 – 1.5) Shigella sp. 4.4 (1.3 – 7.4) 5.3 (4.2 – 6.4) 2.9 (0.4 – 5.3) Campylobacter 2.7 (0.3 – 5.1) 3.8 (3.6 – 3.9) 3.1 Vibrio cholerae 0.0 0.2 (0.0 – 0.3) 0.5 ETEC 9.9 (5.2 – 14.6) 6.4 (5.2 – 7.5) 13.8 EPEC 0.7 12.8 Rotavirus 8.3 (5.3 – 21.5) 10.6 (7.0 – 35.5) 23.7 (16.5 – 26.4) Giardia 9.2 Crytosporidium 13.8 4.1 Entamoeba 1.4 11.6 Coinfection 7.1 4.2 9.2 Unknown 50.2 35.6 21.1
Table 27. AmroB median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 0.2 (0.0 – 2.4) 3.5 (2.0 – 4.0) 2.9 (1.1 – 3.2) Shigella sp. 3.1 (1.8 – 7.2) 6.8 (4.5 –10.6) 6.8 (2.9 – 7.7) Campylobacter 9.9 (2.5 – 16.4) 8.2 (2.3 – 15.4) 6.4 (1.1 – 9.5) Vibrio cholerae 0.3 0.0 0.4 ETEC 15.2 (13.3 – 34.8) 4.5 (3.5 – 11.8) 6.7 (1.8 – 18.4) EPEC 13 (6.6 – 17.9) 17.6 (10.0 – 33.3) 27.5 (17.1 – 34.2) Rotavirus 6 (4.5 – 15.5) 25.8 (15.0 – 33.8) 21 (12.6 – 42.4) Giardia 14.1 (9.0 – 20.0) 3.5 (1.9 – 5.0) 2.8 (0.5 – 15.0) Crytosporidium 8.5 (3.1 – 20.2) 0.7 7.2 (3.2 – 14.9) Entamoeba 1.7 (0.9 – 4.8) 0.8 (0.7 – 0.8) 12.1 Coinfection 11.1 (4.5 – 39.0) 11.0 (9.0 – 15.0) 8.5 Unknown 16.9 17.8
Table 28. AmroD median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 0.1 0.8 (0.3 – 7.1) Shigella sp. 7.9 (5.9 – 9.8) 5.5 9.1 (4.0 – 10.7) Campylobacter 17.7 (12.1 – 23.2) 16.5 10.3 (8.2 – 14.6) Vibrio cholerae 2.9 0.0 1.7 (1.5 – 5.3) ETEC 38.3 (38.0 – 38.6) 13.9 20.3 (10.3 – 29.7) EPEC 18.5 11.0 (7.1 – 29.7) Rotavirus 4.2 (3.6 – 5.5) 35.4 25.0 (14.3 – 40.3) Giardia 29.3 1.6 7.0 (1.6 – 23.6) Crytosporidium 4.3 (3.2 – 5.4) 0.3 5.6 (0.9 – 9.5) Entamoeba 1.5 1.8 (0.0 – 3.5) Coinfection 16.8 18.8 Unknown 10.0
Instituto de Investigación Nutricional, Lima, Perú
Page 23 of 48
Table 29. EmroB median aetiological percentages across settings
Agents Community
(Iq range) Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 2.6 (2.0 – 3.2) 8.4 (5.8 – 14.7) Shigella sp. 0.2 (0.0 – 0.3) 4.1 (0.9 – 5.1) Campylobacter 1.4 (0.5 – 2.3) 2.3 (0.8 – 4.9) Vibrio cholerae 2.0 1.2 (0.0 – 2.3) ETEC 7.6 (6.0 – 14.7) EPEC 2.6 7.6 (3.2 – 11.9) 8.5 (5.8 – 16.4) Rotavirus 16.1 13.4 (6.9 – 30.6) 37.4 (28.0 – 44.4) Giardia 17.4 (1.4 – 30.0) 0.8 (0.0 – 1.6) Crytosporidium 8.0 4.1 1.5 Entamoeba 1.4 2.7 (0.3 – 5.0) 4.9 Coinfection 11.8 12.2 (6.2 – 14.2) Unknown 71.9 37.0 11.2
Table 30. EmroD median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 2.9 (2.7 – 3.0) 6.8 (3.2 – 7.7) Shigella sp. 7.6 2.4 (1.8 – 6.0) 3.6 (0.7 – 6.8) Campylobacter 13.5 10.0 (2.3 – 16.8) 0.6 (0.5 – 0.7) Vibrio cholerae 2.1 (2.0 – 2.3) 8.9 ETEC 23.7 (19.9 – 51.6) 8.7 (3.8 – 17.0) 11.4 (8.7 – 14.0) EPEC 10.3 14.0 19.8 (9.5 – 43.2) Rotavirus 4.1 (3.8 – 4.3) 21.6 (13.9 – 40.5) 22.0 (9.6 –34.3) Giardia 5.0 (3.0 – 21.3) 1.2 Crytosporidium 4.5 2.1 Entamoeba 1.7 2.3 (0.6 – 3.9) Coinfection 2.4 Unknown 34.7 28.9 23.4
Table 31. EuroA median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 0.4 (0.0 – 0.8) 11.7 (7.1 – 26.0) 11.9 (8.6 – 15.5) Shigella sp. 0.7 (0.6 – 0.8) 0.7 Campylobacter 11.8 (5.1 – 28.8) 8.8 (2.0 – 15.5) Vibrio cholerae 0.0 0.4 0.0 ETEC 2.2 EPEC 2.0 4.5 4.2 Rotavirus 23.3 (13.1 – 27.4) 17.2 (15.5 – 32.6) 30.7 (18.0 – 42.3) Giardia 4.2 (3.0 – 5.3) Crytosporidium 12.5 3.6 4.8 Entamoeba 1.4 0.0 11.8 Coinfection 9.0 Unknown 60.4 46.0 16.0
Instituto de Investigación Nutricional, Lima, Perú
Page 24 of 48
Table 32. EuroB median aetiological percentages across settings
Agents Community
(Iq range) Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 3.2 (1.1 – 15.3) 6.6 (4.2 – 23.2) Shigella sp. 8.5 (2.2 – 26.5) 5.9 (4.0 – 12.4) Campylobacter 6.5 4.5 Vibrio cholerae 0.4 0.0 ETEC 10.8 (6.4 – 15.3) 6.5 (6.2 – 6.8) EPEC 9.0 8.6 (4.7 – 19.4) 6.7 (4.0 – 13.2) Rotavirus 13.9 15.5 (10.5 – 20.5) 26.0 (18.6 – 32.7) Giardia 7.1 Crytosporidium 7.3 3.2 Entamoeba 1.4 10.2 Coinfection 3.0 12.5 Unknown 63.4 33.1 21.1
Table 33. EuroC median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 9.3 Shigella sp. 6.1 19.2 Campylobacter 6.4 Vibrio cholerae 0.4 ETEC 1.6 EPEC 9.2 13.6 Rotavirus 14.1 22.1 (19.6 – 88.5) Giardia 7.2 Crytosporidium 6.5 2.4 Entamoeba 1.4 4.7 Coinfection Unknown 63.8 57.4 29.4
Table 34. SearoB median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 8.5 (7.9 – 9.0) 12.3 8.4 Shigella sp. 6.7 (4.9 – 8.4) 12.6 5.3 Campylobacter 27.0 (8.7 – 45.3) 13.3 Vibrio cholerae 0.3 1.9 (0.8 – 3.0) 0.9 ETEC 12.3 (7.2 – 17.3) 9.1 (6.5 – 11.2) 20.1 EPEC 27.5 4.2 (2.8 – 5.5) 3.1 Rotavirus 7.2 (4.6 – 9.8) 19.4 (19.0 – 19.7) 41.3 (35.3 – 47.2) Giardia 2.0 Crytosporidium 5.3 1.8 3.4 Entamoeba 1.6 2.4 Coinfection 10.4 5.9 Unknown 17.6 15.1
Instituto de Investigación Nutricional, Lima, Perú
Page 25 of 48
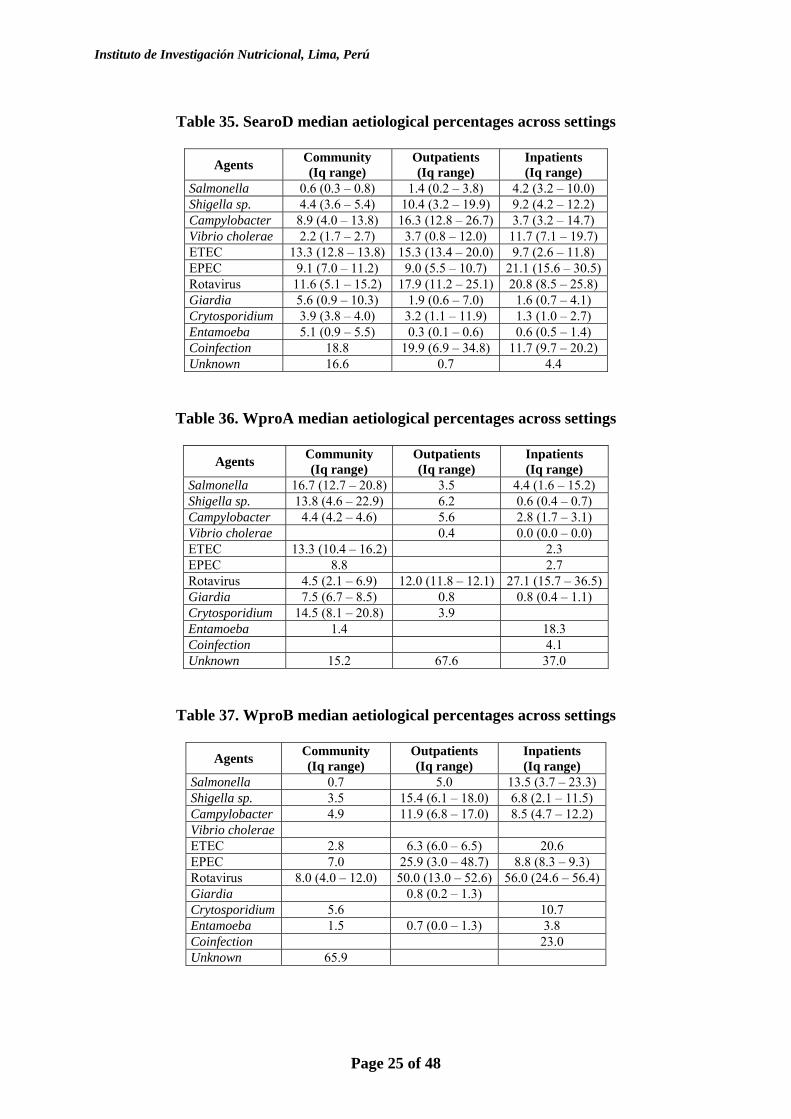
Table 35. SearoD median aetiological percentages across settings
Agents Community
(Iq range) Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 0.6 (0.3 – 0.8) 1.4 (0.2 – 3.8) 4.2 (3.2 – 10.0) Shigella sp. 4.4 (3.6 – 5.4) 10.4 (3.2 – 19.9) 9.2 (4.2 – 12.2) Campylobacter 8.9 (4.0 – 13.8) 16.3 (12.8 – 26.7) 3.7 (3.2 – 14.7) Vibrio cholerae 2.2 (1.7 – 2.7) 3.7 (0.8 – 12.0) 11.7 (7.1 – 19.7) ETEC 13.3 (12.8 – 13.8) 15.3 (13.4 – 20.0) 9.7 (2.6 – 11.8) EPEC 9.1 (7.0 – 11.2) 9.0 (5.5 – 10.7) 21.1 (15.6 – 30.5) Rotavirus 11.6 (5.1 – 15.2) 17.9 (11.2 – 25.1) 20.8 (8.5 – 25.8) Giardia 5.6 (0.9 – 10.3) 1.9 (0.6 – 7.0) 1.6 (0.7 – 4.1) Crytosporidium 3.9 (3.8 – 4.0) 3.2 (1.1 – 11.9) 1.3 (1.0 – 2.7) Entamoeba 5.1 (0.9 – 5.5) 0.3 (0.1 – 0.6) 0.6 (0.5 – 1.4) Coinfection 18.8 19.9 (6.9 – 34.8) 11.7 (9.7 – 20.2) Unknown 16.6 0.7 4.4
Table 36. WproA median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 16.7 (12.7 – 20.8) 3.5 4.4 (1.6 – 15.2) Shigella sp. 13.8 (4.6 – 22.9) 6.2 0.6 (0.4 – 0.7) Campylobacter 4.4 (4.2 – 4.6) 5.6 2.8 (1.7 – 3.1) Vibrio cholerae 0.4 0.0 (0.0 – 0.0) ETEC 13.3 (10.4 – 16.2) 2.3 EPEC 8.8 2.7 Rotavirus 4.5 (2.1 – 6.9) 12.0 (11.8 – 12.1) 27.1 (15.7 – 36.5) Giardia 7.5 (6.7 – 8.5) 0.8 0.8 (0.4 – 1.1) Crytosporidium 14.5 (8.1 – 20.8) 3.9 Entamoeba 1.4 18.3 Coinfection 4.1 Unknown 15.2 67.6 37.0
Table 37. WproB median aetiological percentages across settings
Agents Community (Iq range)
Outpatients (Iq range)
Inpatients (Iq range)
Salmonella 0.7 5.0 13.5 (3.7 – 23.3) Shigella sp. 3.5 15.4 (6.1 – 18.0) 6.8 (2.1 – 11.5) Campylobacter 4.9 11.9 (6.8 – 17.0) 8.5 (4.7 – 12.2) Vibrio cholerae ETEC 2.8 6.3 (6.0 – 6.5) 20.6 EPEC 7.0 25.9 (3.0 – 48.7) 8.8 (8.3 – 9.3) Rotavirus 8.0 (4.0 – 12.0) 50.0 (13.0 – 52.6) 56.0 (24.6 – 56.4) Giardia 0.8 (0.2 – 1.3) Crytosporidium 5.6 10.7 Entamoeba 1.5 0.7 (0.0 – 1.3) 3.8 Coinfection 23.0 Unknown 65.9
Instituto de Investigación Nutricional, Lima, Perú
Page 26 of 48
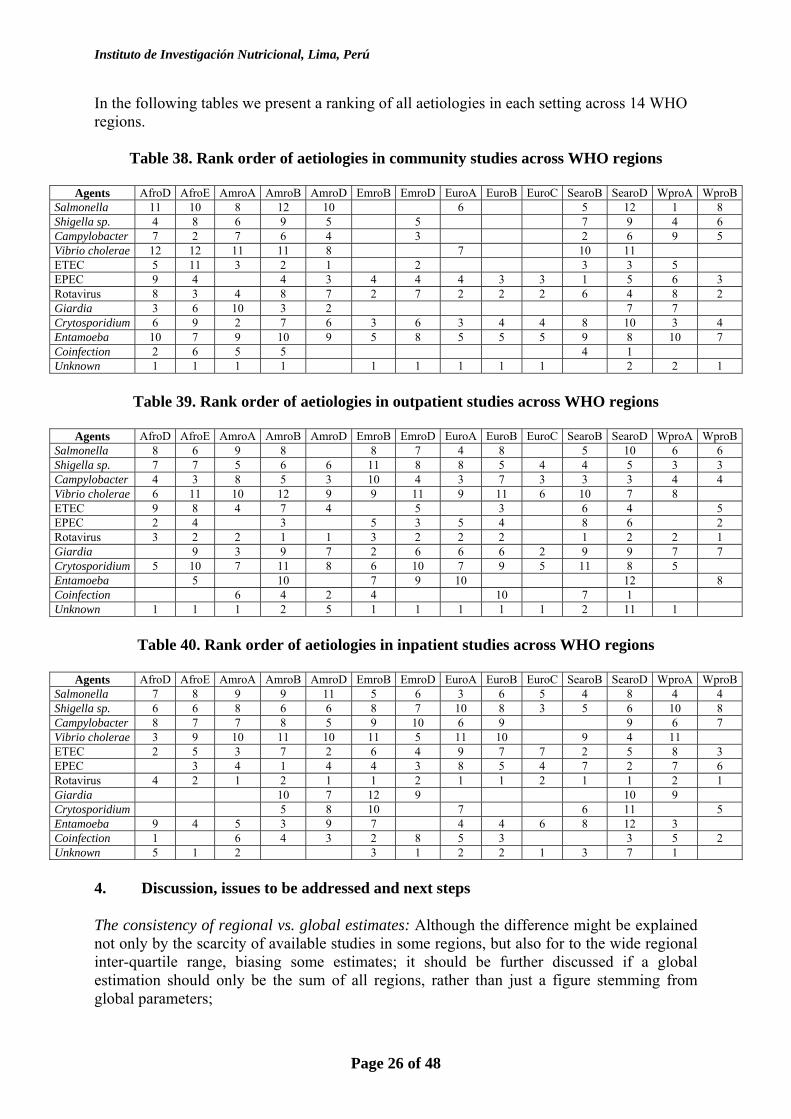
In the following tables we present a ranking of all aetiologies in each setting across 14 WHO regions.
Table 38. Rank order of aetiologies in community studies across WHO regions
Agents AfroD AfroE AmroA AmroB AmroD EmroB EmroD EuroA EuroB EuroC SearoB SearoD WproA WproBSalmonella 11 10 8 12 10 6 5 12 1 8 Shigella sp. 4 8 6 9 5 5 7 9 4 6 Campylobacter 7 2 7 6 4 3 2 6 9 5 Vibrio cholerae 12 12 11 11 8 7 10 11 ETEC 5 11 3 2 1 2 3 3 5 EPEC 9 4 4 3 4 4 4 3 3 1 5 6 3 Rotavirus 8 3 4 8 7 2 7 2 2 2 6 4 8 2 Giardia 3 6 10 3 2 7 7 Crytosporidium 6 9 2 7 6 3 6 3 4 4 8 10 3 4 Entamoeba 10 7 9 10 9 5 8 5 5 5 9 8 10 7 Coinfection 2 6 5 5 4 1 Unknown 1 1 1 1 1 1 1 1 1 2 2 1
Table 39. Rank order of aetiologies in outpatient studies across WHO regions
Agents AfroD AfroE AmroA AmroB AmroD EmroB EmroD EuroA EuroB EuroC SearoB SearoD WproA WproB
Salmonella 8 6 9 8 8 7 4 8 5 10 6 6 Shigella sp. 7 7 5 6 6 11 8 8 5 4 4 5 3 3 Campylobacter 4 3 8 5 3 10 4 3 7 3 3 3 4 4 Vibrio cholerae 6 11 10 12 9 9 11 9 11 6 10 7 8 ETEC 9 8 4 7 4 5 3 6 4 5 EPEC 2 4 3 5 3 5 4 8 6 2 Rotavirus 3 2 2 1 1 3 2 2 2 1 2 2 1 Giardia 9 3 9 7 2 6 6 6 2 9 9 7 7 Crytosporidium 5 10 7 11 8 6 10 7 9 5 11 8 5 Entamoeba 5 10 7 9 10 12 8 Coinfection 6 4 2 4 10 7 1 Unknown 1 1 1 2 5 1 1 1 1 1 2 11 1
Table 40. Rank order of aetiologies in inpatient studies across WHO regions
Agents AfroD AfroE AmroA AmroB AmroD EmroB EmroD EuroA EuroB EuroC SearoB SearoD WproA WproB
Salmonella 7 8 9 9 11 5 6 3 6 5 4 8 4 4 Shigella sp. 6 6 8 6 6 8 7 10 8 3 5 6 10 8 Campylobacter 8 7 7 8 5 9 10 6 9 9 6 7 Vibrio cholerae 3 9 10 11 10 11 5 11 10 9 4 11 ETEC 2 5 3 7 2 6 4 9 7 7 2 5 8 3 EPEC 3 4 1 4 4 3 8 5 4 7 2 7 6 Rotavirus 4 2 1 2 1 1 2 1 1 2 1 1 2 1 Giardia 10 7 12 9 10 9 Crytosporidium 5 8 10 7 6 11 5 Entamoeba 9 4 5 3 9 7 4 4 6 8 12 3 Coinfection 1 6 4 3 2 8 5 3 3 5 2 Unknown 5 1 2 3 1 2 2 1 3 7 1
4. Discussion, issues to be addressed and next steps
The consistency of regional vs. global estimates: Although the difference might be explained not only by the scarcity of available studies in some regions, but also for to the wide regional inter-quartile range, biasing some estimates; it should be further discussed if a global estimation should only be the sum of all regions, rather than just a figure stemming from global parameters;
Instituto de Investigación Nutricional, Lima, Perú
Page 27 of 48
On the aetiological agents considered: The fact that not only some regions are missing information on specific aetiological share causing diarrhoea in any of the three settings, but, also that there’s is still lack of evidence that some of the aetiologies we considered are proven causes of diarrhoea, may lead us to reconsider to continue including some of them;
On the availability of studies: Some regions/countries may be over-represented, somehow biasing the regional estimations, as not all regions/countries are epidemiologically homogenous. It might be worth discussing the convenience of considering at least two regions, as not them all are epidemiologicaly different;
Age groups under study: As any age grouping younger <5 yo was considered to be 0 – 4 yo, this might have biased some regional studies, not only because their scarcity, but also due to their epidemiology, which is not the same through these ages;
Misrepresentation of countries: Selected sites of study may not represent the country where it was conducted. Most likely investigators selected a particular area because diarrhoea was perceived to be a problem there. Besides, we didn’t distinguish rural from urban areas; The sensitivity and specificity of microbiological methods: We included only diagnoses done based on standard tests and procedures for each enteropathogen, whose different sensitivities and specificities were not considered in our estimations; Mixed infections: Each positive case was reported as present if counted as a single diarrhoeal episode and if alone. Not all studies provided this information, nor in all cases where coinfection is described this information is not uniformly presented;
On the estimates of diarrhoeal episodes seen in health facilities by cause: These figures should be taken cautiously, since empirical evidence suggests that the use of DHS, MICS and other estimates might be overestimated; No time trends considered: Though most studies haven’t been conducted in the last few years, we are assuming that the results of the studies remain steady; On the follow-up: Not all studies have a follow-up multiple of 12 months, which may introduce seasonality bias; No source of information of diarrhoeal deaths due to Rotavirus: Our assumption that the proportion of diarrhoeal episodes from inpatient studies, as being the most severe, may represent the proportion of diarrhoeal causes in children who died may be wrong; No nosocomial infections considered: Most of inpatient studies don’t present these data, but those that do, report some of them (e.g. rotavirus) as having an important epidemiological role with impact on costs and length of hospitalizations, so it’s worth discussing the convenience of its inclusion in further burden of diarrhoea estimations. This is one of the first efforts to estimate the burden of diarrhoeal diseases by aetiology at a global and regional level, and by categories of illness (diarrhoeal episodes seen at the community and in health facilities as well as diarrhoeal deaths). Several limitations exist in this study that limits its conclusions:
Instituto de Investigación Nutricional, Lima, Perú
Page 28 of 48
1. The intention by WHO to use this information to produce country-specific estimates by aetiology may not be valid, given all the problems identified in this review.
Even though all these limitations exist, important conclusions could be taken from our results. These are some:
• This is the first attempt to produce global and regional estimates of cause-specific burden of diarrhoeal diseases.
• The estimates obtained have produced similar ranking of enteropathogens as the most
important causes of diarrhoeal cases in the community or diarrhoeal deaths than previous estimates. It reinforce the current knowledge that rotavirus, ETEC and EPEC represent the most important causes of severe diarrhoea worldwide, which should be given priority for vaccine development.
We have looked for previous studies to compare our results with previous burden estimates. There are only estimates produced for some pathogens, like rotavirus and Shigella, but not for all enteropathogens. Our results are similar with those previous attempts, suggesting that although the overall diarrhoea mortality is being reduced significantly since the 1980s, the burden of disease for these pathogens have not changed significantly, which is unlikely. There is a need to develop better methods and to conduct better studies to facilitate more precise burden estimates. ANNEX 1 PUBLICATIONS IN THE PERIOD 1990 – 2001 SELECTED FOR THIS REVIEW 1. Abu-Elyazeed R, Wierzba TF, Mourad AS, Persuki LF, Kay BA, Rao M, Churilla
AM, Bourgeois AL, Mortagy AK, Kamal SM, Savarino SJ, Campbell JR, Murphy JR, Naficy A, Clemens JD. Epidemiology of Enterotoxigenic Escherichia coli Diarrhea in a Pediatric Cohort in a Periurban Area of Lower Egypt. J Infect Dis 1999;179:382-389.
2. Agnew DG, Lima AAM, Newman RD, Wuhib T, Moore RD, Guerrant RL, Sears C.
Cryptosporidiosis in Northeastern Brazilian Children: Association with Increased Diarrhea Morbidity. J Infect Dis 1998;177:754-760.
3. Ahmed MU, Alam MM, Chowdhury NS, Haque MM, Shadid N, Kobayashi N,
Taniguchi K, Urasawa T, Urasawa S. Analysis of Human Rotavirus G Serotype in Bangladesh by Enzime-Linked Immunosorbent Assay and Polimerase Chain Reaction. J Diarrhoeal Dis Res 1999;17(1):22-27.
4. Akhter J, Sikotra S, Qadri SM Myint SH. Comparison of Paediatric Viral
Gastroenteritis at Large Medical Centres in Saudi Arabia and the United Kingdom. J Diarrhoeal Dis Res 1994;12(4):257-260.
Instituto de Investigación Nutricional, Lima, Perú
Page 29 of 48
5. Akinyemi KO, Oyefolu AO, Opere B, Otunba-Payne VA, Oworu AO. Escherichia coli in patients with acute gastroenteritis in Lagos, Nigeria. East Afr Med J 1998; 75(9):512-515.
6. Alam NH, Faruque ASG, Dewan N, Sarker SA, Fuchs GJ. Characteristics of Children
Hospitalized with Severe Dehydration and Persistent Diarrhoea in Bangladesh. J Health Popul Nutr 2001;19(1):18-24.
7. Albert MJ, Faruque ASG, Faruque SM, Sack RB, Mahalanabis D. Case-Control Study
of Enteropathogens Associated with Childhood Diarrhea in Dhaka, Bangladesh. J Clin Microbiol 1999;37(11):3458-3464.
8. Al-Bwardy MAA, Ramia S, Al-Frayh AR, Chagla AH, Al-Omair AA, El-Hazmi
MAF, Lambourne A, Bahakim H, Salman H. Bacterial, parasitic and viral enteropathogens associated with diarrhoea in Saudi children. Ann Trop Paediatr 1988;8:26-30.
9. de Andrade JAB, de Oliveira JOT, Fagundes Neto U. Letalidade em crianças
hospitalizadas com diarréia aguda – fatores associados ao óbito. Rev Ass Med Brasil 1999;45(2):121-127.
10. Ardern-Holmes SL, Lennon D, Pinnock R, Nicholson R, Graham D, Teele D,
Schousboe M, Gillies M, Hollis B, Clarkin A-M, Lindeman J, Stewart J. Trends in hospitalization and mortality from rotavirus disease in New Zeland infants. Pediatr Infect Dis J 1999;18(7):614-619.
11. Arista S, Giovannelli L, Pistoia D, Cascio A, Parea M, Gerna G. Electropherotypes,
subgroups and serotypes of human Rotavirus strains causing gastroenteritis in infants and young children in Palermo, Italy, from 1985 to 1989. Res Virol 1990;141:435-448.
12. Armah GE, Mingle JAA, Dodoo AK, Anyanful A, Antwi R, Commey J, Nkrumah FK.
Seasonality of rotavirus infections in Ghana. Ann Trop Paediatr 1994;14:223-230. 13. Audu R, Omilabu SA, de Beer M, Peenze I, Steele AD. Diversity of Human Rotavirus
VP6, VP7, and VP4 in Lagos State, Nigeria. J Health Popul Nutr 2002;20(1):59-64. 14. Banajeh SM, Ba-oum NHS, Al-Sanabani RMN. Bacterial Aetiology and Anti-
Microbial Resistance of Childhood Diarrhoea in Yemen. J Trop Ped 2001;47:301-303. 15. Baqui AH, Sack RB, Black RE, Haider K, Hossain A, Alim ARM, Yunus M,
Chowdhury HR, Siddique AK. Enteropathogens Associated with Acute and Persistent Diarrhea in Bangladeshi Children <5 Years of Age. J Infect Dis 1992;166:792-796.
16. Baqui AH, Yunus MD, Zaman K, Mitra AK, Hossain KMB. Surveillance of patients
attending a rural diarrhoea treatment centre in Bangladesh. Trop Geogr Med 1991;43(1-2):17-22.
17. Barnes G, Uren E, Stevens KB, Bishop RF. Etiology of Acute Gastroenteritis in
Hospitalized Children in Melbourne, Australia, from April 1980 to March 1993. J Clin Microbiol 1998;36(1):133-138.
Instituto de Investigación Nutricional, Lima, Perú
Page 30 of 48
18. Bates PR, Bailey AS, Wood DJ, Morris DJ, Couriel JM. Comparative Epidemiology
of Rotavirus, Subgroup F (Types 40 and 41) Adenovirus, and Astrovirus Gastroenteritis in Children. J Med Virol 1993;39:224-228.
19. Bereciartu A, Bok K, Gómez J. Identification of viral agents causing gastroenteritis
among children in Buenos Aires, Argentina. J Clin Virol 2002 (in press). 20. Bern C, Unicomb L, Gentsch JR, Banul N, Yunus M, Sack RB, Glass RI. Rotavirus
Diarrhea in Bangladeshi Children: Correlation of Disease Severity with Serotypes. J Clin Microbiol 1992;30(12):3234-3238.
21. Berner R, Schumacher RF, Hameister S, Foster J. Occurrence and impact of
community-acquired and nosocomial rotavirus infections – a hospital-based study over 10 y. Acta Pædiatr Suppl 1999;426:48-52.
22. Bernstein DI, Glass RI, Rodgers G, Davidson BL, Sack DA. Evaluation of Rhesus
Rotavirus Monovalent and Tetravalen Reassortant Vaccines in US Children. JAMA 1995;273(15):1191-1196.
23. Bernstein DI, Sander DS, Smith VE, Schiff GM, Ward RL. Protection from Rotavirus
Reinfection: 2-Year Prospective Study. J Infect Dis 1991;164:277-283. 24. Bingnan F, Unicomb L, Rahim Z, Banu NN, Podder G, Clemens J, van Loon FPL,
Rao MR, Malek A, Tzipori S. Rotavirus-Associated Diarrhea in Rural Bangladesh: Two-Year Study of Incidence and Serotype Distribution. J Clin Microbiol 1991;29(7):1359-1363.
25. Biswas R, Lyon DJ, Nelson EAS, Lau D, Lewindon PJ. Aetiology of acute diarrhea in
hospitalized children in Hong Kong. Trop Med Intern Health 1996;1(5):679-683. 26. Bittencourt JAF, Arbo E, Malysz AS, Oravec R, Dias C. Seasonal and Age
Distribution of Rotavirus Infection in Porto Alegre – Brazil. Braz J Infect Dis 2000;4(6):279-283.
27. Blake P, Ramos S, MacDonald KL, Rassi V, Tardelli TA, Ivey C, Bean NH, Trabulsi
LR. Pathogen-Specific Risk Factors and Protective Factors for Acute Diarrheal Disease in Urban Brazilian Infants. J Infect Dis 1993;167:627-32.
28. Boccatto E, Alves dos Santos S, Oliveira NA, Ramos de Andrade D, Roque F, Mitio
R. Evaluation of a rapid screening assay for bacterial identification (DOT-ELISA) in fecal samples from children. Rev Inst Med Trop S Paulo 1997;39(1):21-27.
29. Bok K, Castagnaro N, Borsa A, Nates S, Espul C, Fay O, Fabri A, Grinstein S, Miceli
I, Matson DO, Gómez JA. Surveillance for Rotavirus in Argentina. J Med Virol 2001;65:190-198.
30. Bon F, Fascia P, Dauvergne M, Tenembaum D, Planson H, Petion AM, Pothier P,
Kohli E. Prevalence of Group A Rotavirus, Human Calcivirus, Astrovirus, and Adenovirus Type 40 and 41 Infections among Children with Acute Gastroenteritis in Dijon, France. J Clin Microbiol 1999;37(9):3055-3058.
Instituto de Investigación Nutricional, Lima, Perú
Page 31 of 48
31. Broor S, Husain M, Chatterjee B, Chakraborty A, Seth P. Temporal Variation in the
Distribution of Rotavirus Electropherotypes in Dehli, India. J Diarrhoeal Dis Res. 1993;11(1):14-18.
32. Brown KH, Pérez F, Gastañaduy AS. Clinical Trial of Modified Whole Milk, Lactose-
Hydrolized Whole Milk, or Cereal-Milk Mixtures for the Dietary Management of Acute Childhood Diarrhea. J Pediatr Gastroenterol Nutr 1991;12(3):340-350.
33. Brüssow H, Benitez O, Uribe F, Sidoti J, Rosa K, Cravioto A. Rotavirus-Inhibitory
Activity in Serial Milk Samples from Mexican Women during Their First Year of Life. J Clin Microbiol 1993;31(3):593-597.
34. Cama R, Parashar UD, Taylor D, Hickey T, Figueroa D, Ortega YR, Romero S, Perez
J, Sterling C, Gentsch J, Gilman RH, Glass RI. Enteropathogens and Other Factors Associated with Severe Disease in Children with Acute Watery Diarrhea in Lima, Peru. J Infect Dis 1999;179:1139-44.
35. Casalino M, Yusuf MW, Nicoletti M, Bazzicalupo P, Coppo A, Colonna B, Cappelli
C, Bianchini C, Falbo V, Ahmed HJ, Omar KH, Maxamuud KB, Maimone F. A two-year study of enteric infections associated with diarrhoeal diseases in children in urban Somalia. Trans Royal Soc Trop Med Hyg 1988;82:637-641.
36. Cassel-Beraud AM, Michel P, Garbarg-Chenon A. Epidemiological Study of Infantile
Rotavirus Diarrhoea in Tananarive (Madagascar). J Diarrhoeal Dis Res 1993;11(3):82-87.
37. Chan PKS, Tam JS, Nelson EAS, Fung KSC, Adeyemi-Doro FAB, Fok TF, Cheng
AF. Rotavirus infection in Hong Kong: epidemiology and estimates of disease burden. Epidemiol Infect 1998;120:321-325.
38. Chandra RK. Effect of Lactobacillus on the incidence an severity of acute diarrhoea in
infants. A prospective placebo-controlled double-blind study. Nutr Res 2002;22:65-69. 39. Checkley W, Gilman RH, Epstein LD, Suárez M, Díaz JF, Cabrera L, Black RE,
Sterling CR. Asymptomatic and Symptomatic Cryptosporidiosis: Their Acute Effect on Weight Gain in Peruvian Children. Am J Epidemiol 1997;145(2):156-163.
40. Cheng-Rong Y, Zong-Da M, Xin W, Yu-Lan L, Yu-Xian Z, Qin-Po Z. Diarrhoea
surveillance in children aged under 5 years in a rural area of Hebei Province, China. J Diarrhoeal Dis Res 1990;8(4):155-159.
41. Chunge RN, Wamola IA, Kinoti SN, Muttunga J, Mutanda LN, Nagelkerke N,
Muthami L, Muniu E, Simwa JM, Karumba PN, Kabiru P. Mixed infections in childhood diarrhoea: results of a community study in Kiambu District, Kenya. East Afr Med J 1989;66(11):715-723.
42. Coluchi N, Mundorf V, Manzur J, Vasquez C, Escobar M, Weber E, Mármol P, Rácz
ML. Detection, Subgroup Specificity, and Genotype Diversity of Rotavirus Strains in Children with Acute Diarrhea in Paraguay. J Clin Microbiol 2002;40(5):1709-1714.
Instituto de Investigación Nutricional, Lima, Perú
Page 32 of 48
43. Constantiniu S, Buzdugan I, Cismaru M, Iosub C Ambăruş A. The Incidence of
Campylobacter jejuni/coli in Infants Acute Diarrhoeal Disease. Arch Roum Path Exp Microbiol 1987;46(2):105-110.
44. Cravioto A, Reyes RE, Trujillo F, Uribe F, Navarro A, De la Roca JM, Hernández JM,
Pérez G, Vásquez V. Risk of diarrhea during the first year of life associated with initial and subsequent colonization by specific enteropathogens. Am J Epidemiol 1990;131(5):886-904.
45. Cravioto A, Tello A, Navarrio A, Ruiz J, Villafán H, Uribe F, Eslava C. Association
of Escherichia coli HEp-2 adherence patterns with type and duration of diarrhoea. Lancet 1991;337:262-264.
46. Cruz JR, Cáceres P, Cano F, Flores J, Bartlett A, Torún B. Adenovirus Types 40 and
41 and Rotavirus Associated with Diarrhea in Children from Guatemala. J Clin Microbiol 1990;28(8):1780-1784.
47. Cruz JR, Cano F, Bartlett AV, Méndez H. Infection, diarrhea and dysentery caused by
Shigella species and Campylobacter jejuni among Guatemalan rural children. Pediatr Infect Dis J 1994;13(3):216-223.
48. Dagan R, Bar-David Y, Sarov B, Katz M, Kassis I, Greenberg D, Glass RI, Margolis
CZ, Sarov I. Rotavirus diarrhea in Jewish and Bedouin children in the Negev region of Israel: epidemiology, clinical aspects and possi ble role of malnutrition in severity of illness. Pediatr Infect Dis J 1990;9(5):314-321.
49. Dalsgaard A, Forslund A, Bodhidatta L, Serichantalergs O, Pitarangsi C, Pang L,
Shimada T, Echeverria P. A high proportion of Vibrio cholearae strains isolated from children with diarrhoea in Bangkok, Thailand are multiple antibiotic resistant and belong to heterogeneous non-O1, non-O139 O-serotypes. Epidemiol Infect 1999;122:217-226.
50. David E, Andronescu D, Şerban D, Jebeleanu L, Cocean S, N M, Marta L. Etiologia
bolii diareice acute la copii spitalizaţi şi din ambulator. Bacteriol Virusol Parazitol Epidemiol 1996;41(1-2):37-41.
51. Dennehy PH, Nelson SM, Spangenberger S, Noel JS, Monroe SS, Glass RI. A
Prospective Case-Control Study of the Role of Astrovirus in Acute Diarrhea among Hospitalized Young Children. J Infect Dis 2001;184:10-15.
52. Desai HS, Banker DD. Rotavirus infection among children in Bombay. Indian J Med
Sci 1993;47(2):27-33. 53. Diamanti E, Superti F, Marziano ML, Giovannangeli S, Tafaj F, Xhelili L, Gani D,
Donelli G. An Epidemiological Study on Viral Infantile Diarrhoea in Tirana. Microbiologica 1996;19:9-14.
54. Djuretic T, Ramsay M, Gay N, Wall P, Ryan M, Fleming D. An estimate of the
proportion of diarrhoeal disease episodes seen by general practitioners attribuitable to
Instituto de Investigación Nutricional, Lima, Perú
Page 33 of 48
rotavirus in children under 5 y of age in England and Wales. Acta Pædiatr Suppl 1999;246:38-41.
55. Domingues LAS, Vaz MGS, Moreno M, Câmara FP. Molecular Epidemiology of
Group A Rotavirus Causing Acute Diarrhea in Infants and Young Children Hospitalized in Rio de Janeiro, Brazil, 1995-1996. Braz J Infect Dis 2000;4(3):119-125.
56. Dutta P, Lahiri M, Sen D, Pal SC. Prospective hospital based study on persistent
diarrhoea. Gut 1991;32(7):787-790. 57. Dutta P, Mitra U, Manna B, Niyogi SK, Roy K, Mondal C, Bhattacharya SK. Double-
blind, randomised controlled clinical trial of hypo-osmolar oral rehydration salt solution in dehydrating acute diarrhoea in severely malnourished (marasmatic) children. Arch Dis Child 2001;84:237-240.
58. Dutta SR, Khalfan SA, Baig BH, Philipose L, Fulayfil R. Epidemiology of Rotavirus
Diarrhoea in Children under Five Years in Bahrain. Int J Epidemiol 1990;19(3):722-727.
59. Echeverria P, Orskov F, Orskov I, Knutton S, Scheutz F, Brown JE, Lexomboon U.
Attaching and Effacing Enteropahogenic Escherichia coli as a cause of Infantile Diarrhea in Bangkok. J Infect Dis 1991:164:550-554.
60. Echeverria P, Taylor DN, Lexsomboon U, Bhaibulaya M, Blacklow NR, Tamura K,
Sakazaki R. Case-Control Study of Endemic Diarrheal Disease in Thai Children. J Infect Dis 1989;159(3):543-548.
61. El Assouli SM, Mohammed KA, Banjar ZM. Human rotavirus genomic RNA
electrophoresis in Jeddah, Saudi Arabia from 1988 to 1992. Ann Trop Paediatr 1995;15:45-53.
62. El-Mougi M, Amer A, El-Abhar A, Hughes J, El-Shafie A. Epidemiological and
Clinical Features of Rotavirus Associated Infantile Diarrhoea in Cairo, Egypt. J Trop Pediatr 1989;35:230-233.
63. Enriquez FJ, Avila CR, Santos JI, Tanaka-Kido J, Vallejo O, Sterling C.
Cryptosporidium Infections in Mexican Children: Clinical, Nutritional, Enteropathogenic, and Diagnostic Evaluations. Am J Trop Med Hyg 1997;56(3):254-257.
64. Essers B, Burnens AP, Lanfrachini FM, Somaruga SGE, von Vigier RO, Schaad GE,
Aebi C, Bianchetti MG. Acute Community-Acquired Diarrhea Requiring Hospital Admission in Swiss Children. Clin Infect Dis 2000;30:192-196.
65. Fagundes-Neto U, Gandolfi SL, Scaletsky I. Acute Diarrhea due to Enteropathogenic
Escherichia coli: Epidemiological and Clinical Features in Brasilia, Brasil. Int J Infect Dis 1996;1(2):65-69.
Instituto de Investigación Nutricional, Lima, Perú
Page 34 of 48
66. Fang GD, Lima AAM, Martins CV, Nataro JP, Guerrant RL. Etiology and Epidemiology of Persistent Diarrhea in Northeastern Brazil: a Hospital-Based, Prospective, Case-Control Study. J Pediatr Gastroenterol Nutr 1995;21:137-144.
67. Fang Z-Y, Yang H, Zhang J, Li Y-F, Hou A-C, Ma L, Sun L-W, Wang C-X. Child
rotavirus in association with acute gastroenteritis in two Chinese sentinel hospitals. Ped Int 2000; 42:401-405.
68. Faruque ASG, Mahalanabis D, Islam A, Hoque SS, Hasnat A. Common diarrhea
pathogens and the risk of dehydration in young children with acute watery diarrhea: a case-control study. Am J Trop Med Hyg 1993;49(1):93-100.
69. Faruque ASG, Teka T, Fuch GJ. Shigellosis in children: a clinico-epidemiological
comparison between Shigella dysenteriae type I and Shigella flexneri. Ann Trop Paediatr 1998;18:197-201.
70. Fauveau V, Yunus M, Zaman K, Chakraborty J, Sarder AM. Diarrhoea Mortality in
Rural Bangladeshi Children. J Trop Pediatr 1991;37:31-36. 71. Ferreccio C, Prado V, Ojeda A, Cayyazo M, Abrego P, Guers L et al. Epidemiologic
patterns of acute diarrhea and endemic Shigella infections in children in a poor periurban setting in Santiago, Chile. Am J Epidemiol 1991; 134(6):614-627.
72. Figueroa-Quintanilla D, Salazar-Lindo E, Sack RB, León-Barúa R, Sarabia-Arce S,
Campos-Sánchez M, Eyzaguirre-Maccan E. A controlled trial of bismuth and subsalicylate in infants with acute watery diarrheal disease. NEJM 1993;328(23):1653-1658.
73. Fisher TK. Incidence of hospitalizations due to rotavirus gastroenteritis in Denmark.
Acta Pædiatr 2001;90:1073-1075. 74. Fisher TK, Steinsland H, Mølbak K, Ca R, Gentsch JR, Valentiner-Branth P, Aaby P,
Sommerfelt H. Genotype Profiles of Rotavirus Strains from Children in a Suburban Community in Guinea-Bissau, Western Africa. J Clin Microbiol 2000;38(1):264-267.
75. Flores A, Araque M, Vizcaya L. Multiple Shigella Species Isolated From Pediatric
Patients With Acute Diarrheal Disease. Am J Med Sci 1998;316(6):379-384. 76. Fraser D, Bilenko N, Deckelbaum RJ, Dagan R, El-On J, Naggan L. Giardia lamblia
Carriage in Israeli Bedouin Infants: Risk Factors and Consequences. Clin Infect Dis 2000; 30:419-424.
77. Gaggero A, O’Ryan M, Noel JS, Glass RI, Monroe SS, Mamani N, Prado V,
Avendaño LF. Prevalence of Astrovirus Infection among Chilean Children with Acute Gastroenteritis. J Clin Microbiol 1998;36(12):3691-3693.
78. Gedlu E, Aseffa A. Campylobacter enteritis among children in north-west Ethiopia: a
1-year prospective study. Ann Trop Paediatr 1996;16:207-212.
Instituto de Investigación Nutricional, Lima, Perú
Page 35 of 48
79. Georges-Courbot MC, Beraud-Cassel AM, Gouandjika I, Georges AJ. Prospective Study fo Enteric Campylobacter infections in Children from Birth to 6 Months in the Central African Republic. J Clin Microbiol 1987;25(5):836-839.
80. Georges-Coubot MC, Cassel-Beraud AM, Gouandjika I, Monges J, Georges AJ. A
cohort study of enteric campylobacter infection in children from birth to two years in Bangui (Central African Republic). Trans Royal Soc Trop Med Hyg 1990;84:122-125.
81. Georges-Courbot MC, Monges J, Beraud-Cassel, Gouandjika I, Georges AJ.
Prospective longitudinal study of rotavirus infections in children from birth to two years of age in Central Africa. Ann Inst Pasteur/Virol 1988;139:421-428.
82. Ghosh AR, Koley H, De D, Paul M, Nair GB, Sen D. Enterotoxigenic Escherichia coli
associated diarrhoea among infants aged less than six months in Calcutta, India. Eur J Epidemiol 1996;12:81-84.
83. Ghosh AR, Nair GB, Dutta P, Pal SC, Sen D. Acute diarrhoeal diseases in infants aged
below six months in hospital in Calcutta, India. Trans Royal Soc Trop Med Hyg 1991;85:796-798.
84. Ghosh AR, Nair GB, Naik TN, Paul M, Pal SC, Sen D. Entero-adherent Escherichia
coli is an important diarrhoeagenic agent in infants aged below 6 months in Calcutta, India. J Med Microbiol 1992;36:264-268.
85. Ghosh AR, Sehgal SC. Shigella infections among children in Andaman – an
archipelago of tropical islands in Bay of Bengal. Epidemiol Infect 1998;121:43-48. 86. Giordano MO, Ferreyra LJ, Isa MB, Martinez LC, Yudowski SI, Nates SV. The
epidemiology of acute viral gastroenteritis in hospitalized children in Cordoba City, Argentina: an insight of disease burden. Rev Inst Med Trop S Paulo 2001;43(4):193-197.
87. Gomes TAT, Rassi V, MacDonald KL, Silva SRT, Trabulsi LR, Vieira MAN, Guth
BEC, Candeias JAN, Ivey C, Toledo MRF, Blake. Enteropathogens Associated with Acute Diarrheal Disease in Urban Infants in São Paulo, Brazil. J Infect Dis 1991,164:331-337.
88. Gomwalk NE, Gosham LT, Umoh UJ. Rotavirus Gastroenteritis in Pediatric
Diarrhoea in Jos, Nigeria. J Trop Pediatr 1990;36:52-55. 89. Gomwalk NE, Umoh UJ, Gosham LT, Ahmad AA. Influence of Climatic Factors on
Rotavirus Infection among Children with Acute Gastroenteritis in Zaria, Northern Nigeria. J Trop Pediatr 1993;39:293-297.
90. Gonzáles FS, Sordo ME, Rowestein G, Sabbag L, Roussos A, De Petre E, Garello M,
Medei A, Bok K, Grinstein S, Gómez JA. Diarrea por Rotavirus. Impacto en un Hospital de Niños de Buenos Aires. Medicina (Buenos Aires) 1999;59:321-326.
Instituto de Investigación Nutricional, Lima, Perú
Page 36 of 48
91. González R, Díaz C, Marino M, Cloralt R, Pequeneze M, Pérez-Schael I. Age-specific prevalence of Escherichia coli with localized and aggregative adherence in Venezuelan infants with acute diarrhea. J Clin Microbiol 1997;35(3):1103-1107.
92. Gościniak G, Sobieszcańska B, Grzybek-Hryncewicz K. Rotawirusy w biegunkach u
dzieci hospitalizowanych w Klinikach Wroclavia (Rotavirus diarrhea in children hospitalized in Wrocalw clinics). Przegl Lek 1990;47(10):682-685.
93. Gracey M, Sullivan H, Burke V, Wymer V, Mogyorosy R, Gunzbung S, Iverson S.
Intestinal pathogens and parasites in Australian Aboriginal children from birth to two years of age. Trans Roy Soc Trop Med Hyg 1992;86:222-223.
94. Greenberg BL; Sack RB, Salazar-Lindo E, Budge E, Gutierrez M, Campos M,
Visberg A, León-Barúa R, Yi A, Maurutia D, Gómez M, Lindo I, Jauregui E. Measles-Associated Diarrhea in Hospitalized Children in Lima, Peru: Pathogenic Agents and Impact on Growth. J Infect Dis 1991;163:495-502.
95. Griffiths FH, Steele AD, Alexander JJ. The molecular epidemiology of rotavirus-
associated gastro-enteritis in the Transkei, Southern Africa. Ann Trop Paediatr 1992;12:259-264.
96. Grimwood K, Carzino R, Barnes GL, Bishop RF. Patients with enteric adenovirus
gastroenteritis admitted to an Australian pediatric teaching hospital from 1981 to 1992. J Clin Microbiol 1995(1) 33:131-136.
97. Gueddana N, Saffen S, Ben Aissa R, Khemiri F, Chaker A, Arouji A, Hammami A,
Lamine-Jomni S. Etude étiologique des gastroentéritis aguës de l’enfant en Tunisie. Arch Fr Pediatr 1988;45:207-211.
98. Guerrero ML, Noel JS, Mitchell DK, Calva JJ, Morrow AL, Martinez J, Rosales G,
Velásquez FR, Monroe SS, Glass RI, Pickering LK, Ruiz-Palacios GM. A prospective study of astrovirus diarrhea of infancy in Mexico City. Pediatr Infect Dis J 1998;17(8):723-727.
99. Gunzburg S, Gracey M, Burke V, Chang B. Epidemiology and microbiology of
diarrhoea in young Aboriginal children in the Kimberly region of Western Australia. Epidemiol Infect 1992;108:67-76.
100. Gupta DN, Sircar BK, Sengupta PG, Ghosh S, Banu MK, Mondal SK, Saha DR, De
SP, Sikdar SN, Manna B, Dutta S, Saha NC. Epidemiological and clinical profiles of acute invasive diarrhoea with special reference to mucoid episodes: a rural community-based longitudinal study. Trans Royal Soc Trop Med Hyg 1996;90:544-547.
101. Gusmão RHP, Mascarenhas JDA, Gabbay Y, Lins-Lainson Z, Ramos FLP, Monteiro
T, Valente SA, Fagundes-Neto U, Linhares AC. Rotavirus Sugroups, G Serotypes, and Electrophoretypes in Cases of Nosocomial Infantile Diarrhoea in Belém, Brazil. J Trop Ped 1999;45:81-86.
Instituto de Investigación Nutricional, Lima, Perú
Page 37 of 48
102. Haq JA, Rahman KM. Campylobacter jejuni as a cause of acute diarrhoea in children: a study at an urban hospital in Bangladesh. J Trop Med Hyg 1991;94:50-54.
103. Herrmann JE, Taylor DN, Echeverria P, Blacklow NR. Astroviruses as a cause of
gastroenteritis in children. NEJM 1991;324(25):1757-1760. 104. Hoque SS, Faruque ASG, Mahalanabis D, Hasnat A. Infectious Agents Causing Acute
Watery Diarrhoea in Infants and Young Children in Bangladesh and their Public Health Implications. J Trop Ped 1994;40:351-354.
105. Hossain MA, Albert MJ, Hasan KZ. Epidemiology of shigellosis in Teknaf, a coastal
area of Bangladesh: a 10-year survey. Epidemiol Infect 1990;105:41-49. 106. Howard P, Alexander ND, Atkinson A Clegg AO, Gerega G, Javati A, Kajoi M,
Lupiwa S, Lupiwa T, Mens M, Saleu G, Sanders RC, West B, Alpers MP. Bacterial, Viral and Parasitic Aetiology of Paediatric Diarrhoea in the Highlands of Papua New Guinea. J Trop Pediatr 2000;46:10-14.
107. Huilan S, Zhen LG, Mathan MM, Mathew, Olarte J, Espejo R, Maung K, Ghafoor
MA, Khan MA, Sami Z, Suton RG. Etiology of acute diarrhea among children in devoloping countries: a multicdngtre study in five countries. Bull WHO 1991;69(5):549-555.
108. Husain M, Seth P, Dar L, Broor S. Classification of rotavirus into G and P types with
specimens from children with acute diarrhea in New Delhi, India. J Clin Microbiol 1996;34(6):1592-1594.
109. Isenbarger DW, Bodhidatta L, Hoge C, Nirdnoy W, Pitarangsi C, Umpawasiri,
Echeverria P. Prospective study of the incidence of diarrheal disease and Helicobacter pylori infection among children in an orphanage in Thailand. Am J Trop Med Hyg 1998;59(5):796-800.
110. Isenbarger DW, Hien BT, Ha HT, Ha TT, Bohidatta L, Pang LW, Cam PD.
Prospective study of the incidence of diarrhoea and prevalence of bacterial pathogens in a cohort of Vietnamese children along the Red River. Epidemiol Infect 200;127:229-236.
111. Jain V, Das BK, Bhan MK, Glass RI, Gentsch JR, The Indian Strain Surveillance
Collaborating Laboratories. J Clin Microbiol 2001;39(10):3524-3529. 112. Joensuu J, Koskenniemi E, Pang X-L, Vesikari T. Randomised placebo-controlled
trial of rhesus-human reassortant rotavirus vaccine for prevention of severe rotavirus gastroenteritis. Lancet 1997;350:1205-1209.
113. Kaminsky RG. Parasitism and diarrhoea in children from two rural communities and
marginal barrio in Honduras. Trans R Soc Trop Med Hyg 1991;85(1):70-73. 114. Katouli M, Jaafari A, Farhoudi-Moghaddamam AA, Ketabi GR. Aetiological studies
of diarrhoeal in infants and young children in Iran. J Trop Med Hyg 1990;93:22-27.
Instituto de Investigación Nutricional, Lima, Perú
Page 38 of 48
115. Katsumata T, Hosea D, Wasito EB, Kohno S, Hara K, Soeparto, Rahnu IH. Cryptosporidiosis in Indonesia: A Hospital-Based Study and a Community-Based Survey. Am J Trop Med Hyg 1998;59(4):628-632.
116. Kelkar SD, Ayachit VL. Circulation of Group A Rotavirus Subgroups and Serotypes
in Pune, India, 1990-1997. J Health Popul Nutr 2000;18:163-170. 117. Kelkar SD, Purohit SD, Simha KV. Prevalence of rotavirus diarrhoea among
hospitalized children in Pune, India. Indian J Med Res 1999;109:131-135. 118. Kim K-H, Suh I-S, Kim JM, Kim CW, Cho Y-J. Etiology of Childhood Diarrhea in
Korea. J Clin Microbiol 1989;27(6):1192-1196. 119. Kim K-H, Yang J-M, Joo S-I, Cho Y-G, Glass R, Cho Y-J. Importance of Rotavirus
and Adenovirus Types 40 and 41 in Acute Gastroenteritis in Korean Children. J Clin Microbiol 1990;28(10):2279-2284.
120. Koulla-Shiro S, Loe C, Ekoe T. Prevalence of Campylobacter enteritis in children
from Yaounde (Cameroon). Cent Afr J Med 1995;4(3):91-94. 121. Lanata CF, Black RE, Flores J, Lazo F, Butrón B, Linares A, Huapaya A, Ventura G,
Gil A, Kapikian AZ. Immunogenicity, safety and protective efficacy of one dose of the rhesus rotavirus vaccine and serotype 1 and 2 human-rhesus rotavirus reassortants in children from Lima, Peru. Vaccine 1996;14(3):237-243.
122. Lanata CF, Black RE, Maúrtua D, Gil A, Gabilondo A, Yi A, Miranda E, Gilman RH,
León-Barúa R, Sack RB. Etiologic agents in acute vs. persistent diarrhea in children under three years of age in peru-urban Lima, Peru. Acta Pædiatr Suppl 1992;381:32-38.
123. Lanata CF, Midthun K, Black RE, Butron B, Huapaya A, Penny ME, Ventura G, Gil
A, Jett-Goheen M, Davidson BL. Safety, Immunogenicity, and Protective Efficacy of One and Three Doses of the Tetravalent Rhesus Rotavirus Vaccine in Infants in Lima, Peru. J Infect Dis 1996;174:268-275.
124. Lim YS, Ngan CCL, Tay L. Enteropathogenic Escherichia coli as a cause of diarrhoea
among children in Singapore. J Trop Med Hyg 1992;95:339-342. 125. Lima AAM, Moore SR, Barboza Jr MS, Soares AM, Schleupner MA, Newman RD,
Sears CL, Nataro JP, Fedorko DP, Wuhib T, Schorling JB, Guerrant RL. Persistent Diarrhea Signals a Critical Period of Increased Diarrhea Burdens and Nutritional Shortfalls: A Prospective Cohort Study among Children in Northern Brazil. J Infect Dis 2000;181:1643-1651.
126. Loening WEK, Coovadia YM, van den Ende J. Aetiological factors of infantile
diarrhoea: a community-based study. Ann Trop Paediatr 1989;9:248-255. 127. Lynch M, O'Halloran, Whyte D, Fanning S, Cryan B, Glass RI. Rotavirus in Ireland:
national estimates of disease burden, 1997-1998. Pediatr Infect Dis, 2001;20(7):693-698.
Instituto de Investigación Nutricional, Lima, Perú
Page 39 of 48
128. Madore HP, Christy C, Pichichero M, Long C, Pincus P, Vosefsky D, Kapikian AZ,
Dolin R, Elmwood, Panorama and Westfall Pediatric Groups. Field Trial of Rhesus Rotavirus or Human-Rhesus Rotavirus Reassortant Vaccine of VP7 Serotype 3 or 1 Specificity in Infants. J Infect Dis 1992;166:235-243.
129. Mahalanabis D, Alam AN, Rahman N, Hasnat A. Prognostic Indicators and Risk
Factors for Increased Duration of Acuter Diarrhoea and for Persistent Diarrhoea in Children. Int J Epidemiol 1991;20(4):1064-1072.
130. Maldonado Y, Cantwell M, Old M, Hill D, Sanchez ML, Logan L, Millan-Velasco F,
Valdespino JL, Sepúlveda J, Matsui S. Population-Based Prevalence of Symptomatic and Asymptomatic Astrovirus Infection in Rural Mayan Infants. J Infect Dis 1998;178:334-339.
131. Maltezou HC, Zafiropoulou A, Mavrikou M, Bozavoutoglou E, Liapi G, Foustoukou
M, Kafetzis. Acute Diarrhea in Children Treated in an Outpatient Setting in Athens, Greece. J Infect 2001;43:122-127.
132. Mathew M, Mathan M, Mani K, George R, Jebakumar K, Dharamsi R, Kirubajaran,
Pereira S, Mathan VI. The relationship of microbial pathogens to acute infectious diarrhoea of childhood. J Trop Med Hyg 1991;94:253-260.
133. McIver CJ, Hansman G, White P, Doultree JC, Catton M, Rawlinson WD. Diagnosis
of enteric pathogens in children with gastroenteritis. Pathology 2001;33:353-358. 134. McIver CJ, Palombo Doultree JC, Mustafa H, Marshall JA, Rawlinson. Detection of
astrovirus gastroenteritis in children. J Virol Methods 2000;84:99-105. 135. Mégraud F, Boudraa G, Bessaoud K, Bensid S, Dabis F, Soltana R, Touhami M.
Incidence of campylobacter infection in infants in western Algeria and the possible protective role of breast feeding. Epidemiol Infect 1990;105:73-78.
136. Mnisi YN, Williams MM; Steele AD. Subgroup and serotype epidemiology of human rotaviruses recovered at Ga-Rankuwa, Southern Africa. Cent Afr J Med 1992;38(6):221-225.
137. Mølbak K, Wested N, Højlying N, Scheutz F, Gottschau A, Aaby P, da Silva APJ. The
Etiology of Early Childhood Diarrhea: A community Study from Guinea-Bissau. J Infect Dis 1994;169:581-587.
138. Mølbak K, Højlying N, Ingholt L, Da Silva APJ, Søren J, Aaby P. An epidemic
outbreak of cryptosporidiosis: a prospective community study from Guinea Bissau. Pediatr Infect Dis J 1990;9(8):566-570.
139. Moulin F, Marc E, Lorrot M, Coquery S, Sauvé-Martin H, Ravilly S, Lebon P,
Raymond J, Brunet F, Gendrel D. Hospitalisations pour gastroentérites aiguës communautaires à rotavirus: une enquête de quatre ans. Arch Pédiatr 2002;9:255-261.
Instituto de Investigación Nutricional, Lima, Perú
Page 40 of 48
140. Mpabalwani M, Oshitani H, Kasolo F, Mizuta K, Luo N, Matsubayashi N, Bhat G, Suzuki H, Numazaki. Rotavirus gastro-enteritis in hospitalized children with acute diarrhea in Zambia. Ann Trop Paediatr 1995;15:39-43.
141. Mrukowicz JZ, Krobicka B, Duplaga M, Kowolska-Duplaga K, Domañski J,
Szajewska, Kantecki M, Iwañczak F, Pytrus T. Epidemiology and impact of rotavirus diarrhoea in Poland. Acta Pædiatr Suppl 1999;426:53-60.
142. Mrukowicz JZ, Thompson J, Reed GW, Tollefson SJ, Kobayashi M, Araki K, Wright
PF. Epidemiology of rotavirus in infants and protection against symptomatic illness afforded by primary infection and vaccination. Vaccine 1999;17:745-753.
143. Mubashar M, Khan A, Iqbal J, Ghafoor A, Burney M. Aetiological Agents of
Diarrhoeal Diseases in Hospitalized Children in Rawalpindi, Pakistan. J Diarrhoeal Dis Res 1988;6(3 & 4):228-231.
144. Mutanda LN, Gemert W, Kangethe SK, Juma R. Seasonal Pattern of Some Causatives
Agents of Childhood Diarrhoea in Nairobi. East Afr Med J 1986;63(6):373-381. 145. Mutanda LN, Kangethe SK, Juma R, Lichenga EO, Gathecha C. Aetiology of
diarrhoea in malnourished children at Kenyatta National Hospital. East Afr Med J 1985;62(12):835-842.
146. Naficy AB, Rao MR, Holmes JL, Abu-Elyazeed R, Savarino SJ, Wierzba TF, Frenck
RW, Monroe SS, Glass RI, Clemens JD. Astrovirus Diarrhea in Egyptian Children. J Infect Dis 2000;182:185-190.
147. Naficy AB, Abu-Elyazeed R, Holmes JL, Rao MR, Savarino SJ, Kim Y, Wierzba TF,
Peruski L, Lee YJ, Gentsch JR, Glass RI, Clemens JD. Epidemiology of Rotavirus Diarrhea in Egyptian Children and Implications for Disease Control. Am J Epidemiol 1999;150(7):770-777.
148. Nakano T, Binka FN, Afari EA, Agbodaze D, Aryeetey ME, Mingle JAA, Kamiya H,
Sakurai M. Survey of enteropathogenic agents in children with and without diarrhoea in Ghana. J Trop Med Hyg 1990;93:408-412.
149. Nakata S, Gatheru Z, Ukae S, Adachi N, Kobayashi N, Honma S, Muli J, Nyangao J,
Kiplagat E, Tukei PM, Chiba S. Epidemiological Study of the G Serotype Distribution of Group A Rotavirus in Kenya From 1991 to 1994. J Med Virol 1999;58:296-303.
150. Nath G, Shukla BN, Reddy DCS, Sanyal SC. A Community Study on the Aetiology of
Childhood Diarrhoea with Special Reference to Campylobacter jejuni in a Semiurban Slum of Varanasi, India. J Diarrhoeal Dis Res 1993;11(3):165-168.
151. Newman RD, Moore SR, Lima AAM, Nataro JP, Guerrant RL. A longitudinal study
of Giardia lamblia infection in nort-east Brazilian children. Trop Med Int Health 2001;6(8):624-634.
Instituto de Investigación Nutricional, Lima, Perú
Page 41 of 48
152. Newman R, Sears CL, Moore SR, Nataro JP, Wuhib T, Agnew DA, Guerrant RL, Lima AA. Longitudinal Study of Cryptosporidium Infection in Children in Northeastern Brazil. J Infect Dis 1999;180:167-175.
153. Nguyen VM, Nuguyen VT, Huynh PL, Dang DT, Nguyen THT, Pan VT, Nguyen TL,
Le TL, Ivanoff B, Gentsch JR, Glass RI. The Epidemiology and Disease Burden of Rotavirus in Vietnam: Sentinel Surveillance at 6 Hospitals. J Infect Dis 2001;183:1707-1712.
154. Nimri LF, Hijazi S. Rotavirus-associated Diarrhoea in Children in a Refugee Camp in
Jordan. J Diarrhoeal Dis Res 1996;14(1):1-4. 155. Nirdoy W, Serichantalergs O, Cravioto A, LeBron C, Wolf M, Hoge CW,
Svennerholm A-M, Taylor DN, Echeverria P. Distribution of Colonization Factor Antigens among Enterotoxigenic Escherichia coli Strains Isolated from Patients with Diarrhea in Nepal, Indonesia, Peru, and Thailand. J Clin Microbiol 1997;35(2):527-530.
156. Nishio O, Matsui K, Phuong Lan DT, Ushijima H, Isomura S. Rotavirus infection
among infants with diarrhea in Vietnam. Pediatr Int 2000;42:422-424. 157. Nishio O, Matsui K, Oka T, Ushiima H, Mubina A, Dure-Samin A, Isomura S.
Rotavirus infection among infants with diarrhea in Pakistan. Pediatr Int 2000;42:425-427.
158. O’Ryan ML, Mamani N, Avendaño LF, Cohen J, Peña A, Villarroel J, Chavez A,
Valdivieso F, Matson DO. Molecular epidemiology of human rotaviruses in Santiago, Chile. Pediatr Infect Dis J 1997;16(3):305-311.
159. O’Ryan M, Pérez-Schael I, Mamani N, Peña A, Salinas B, González G, González F,
Matson DO, Gómez J. Rotavirus-associated medical visits and hospitalizations in South America: a prospective study at three large sentinel hospitals. Pediatr Infect Dis J, 2001;20:685-693.
160. Obi CL, Coker AO, Epoke J, Ndip RN. Enteric Bacterial Pathogens in Stools of
Residents of Urban and Rural Regions in Nigeria: A Comparison of Patients with and without Diarrhoea and Controls without Diarrhoea. J Diarrhoeal Dis Res 1997;15(4):241-247.
161. Okeke IN, Lamikanra A, Steinrück H, Kaper JK. Characterization of Escherichia coli
Strains from Cases of Childhood Diarrhea in Provincial Southwestern Nigeria. J Clin Microbiol 2000; 38(1):7-12.
162. Oliva CAG, Scaletsky I, de Morais MB, Fagundes Neto U. Diarréia aguda grave
associada à Escherichia coli enteropatogénica clássica (EPEC): características clínicas e pedas fecais em lactentes hospitalizados. Rev Ass Med Brasil 1997;43(4):283-289.
163. Pang X-L, Honma S, Nakata S, Vesikari T. Human Calciviruses in Acute
Gastroenteritis of Young Children in the Community. J Infect Dis 2000;181(Suppl. 2):S288-S294.
Instituto de Investigación Nutricional, Lima, Perú
Page 42 of 48
164. Paniagua M, Espinoza F, Ringman M, Reizenstein E, Svennerholm A-M, Hallander
H. Analyis of Incidence of Infection with Enterotoxigenic Escherichia coli in a Prospective Cohort Study of Infant Diarrhea in Nicaragua. J Clin Microbiol 1997; 35(6):1404-1410.
165. Parashar UD, Holman RC, Clarke MJ, Breese JS, Glass RI. Hospitalizations
Associated with Rotavirus Diarrhea in the United States, 1993 through 1995: Surveillance Based on the New ICD-9-CM Rotavirus-Specific Diagnostic Code. J Infect Dis 1998;177:13-17.
166. Patwari AK, Srinivasan A, Diwan N, Aneja S, Anand VK, Peshin S. Rotavirus as an
Aetiological Organism in Acute Watery Diarrhoea in Delhi Children: Reappraisal of Clinical and Epidemiological Characteristics. J Trop Pediatrics 1994;40:214-218.
167. Pazzaglia G, Bourgeois AL, Araby I, Mikhail I, Podgore JK, Mourad A, Riad S,
Gaffar T, Ramadan AM. Campylobacter-associated Diarrhoea in Egyptian Infants: Epidemiology and Clinical Manifestations of Disease and High Frequency of Concomitant Infections. J Diarrhoeal Dis Res 1993;11(1):6-13.
168. Pazzaglia G, Sack RB, Salazar E, Yi A, Chea E, León-Barúa R, Guerrero CE,
Palomino J. High Frequency of Coinfecting Enteropathogens in Aeromonas Associated Diarrhea of Hospitalized Peruvian Infants. J Clin Microbiol 1991;29(2):1151-1156.
169. Pennap G, Pager CT, Peenze I, de Beer MC, Kwaga JKP, Ogalla WN, Umoh JU,
Steele AD. Epidemiology of Astrovirus Infection in Zaria, Nigeria. J Trop Pediatr 2002;48:98-101.
170. Pennap G, Peenze I, de Beer M, Pager CT, Kwaga JKP, Ogalla WN, Umoh JU, Steele
D. VP6 Subgroup and VP7 Serotype of Human Rotavirus in Zaria, Northern Nigeria. J Trop Ped 2000;46:344-347.
171. Penny ME, Paredes P, Brown KH, Laughan Smith H. Lack of a role of the duodenal
microflora in pathogenesis of paersistent diarrhea-related malabsorption in Peruvian children. Pediatr Infect Dis J 1990;9(7):479-487.
172. Perch M, Sodemann Jakobsen MS, Vallentiner-Branth P, Steinland H, Fisher TK,
Duarte LD, Aaby P, Mølbak K. Seven years’ experience with Cryptosporidium parvum in Guinea-Bissau, West Africa. Ann Trop Paediatr 2001:21:313-318.
173. Pereira HG, Linhares AC, Candeias JAN, Glass RI. National Laboratory Surveillance
of Viral Agents of Gastroenteritis in Brazil. Bull PAHO 1993;27(3):224-233. 174. Pérez ME, Glass R, Alvarez G, Pericchi LR, González R, Kapikian AZ, Pérez-Schael
I. Rhesus rotavirus-based quadrivalent vaccine is efficacious despite age, socioeconomic conditions and seasonality in Venezuela. Vaccine 2001;19:976-981.
175. Pérez-Schael I, García D, Gonzáles M, Gonzáles R, Daoud N, Pérez M, Cunto W,
Kapikian AZ, Flores J. Prospective Study of Diarrheal Diseases in Venezuelan
Instituto de Investigación Nutricional, Lima, Perú
Page 43 of 48
Children to Evaluate the Efficacy of Rhesus Rotavirus Vaccine. J Med Virol 1990;30:219-229.
176. Pérez-Schael I, González R, Fernández R, Alfonzo E, Inaty D, Boher Y, Sarmiento L.
Epidemiological Features of Rotavirus Infections in Caracas, Venezuela: Implications for Rotavirus Immunization Programs. J Med Virol 1999;59:520-526.
177. Pérez-Schael I, Guntiñas MJ, Pérez M, Pagone V, Rojas AM, Gonzáles R, Cunto W,
Hoshino Y, Kapikian AZ. Efficacy of the Rhesus rotavirus-based quadrivalent vaccine in infants and young children in Venezuela. NEJM 1997;337(17):1181-1187.
178. Peruski Jr LF, Kay BA, El-Yazeed RA, El-Etr SH, Cravioto A, Wierzba TF, Rao M,
El-Ghorab N, Shaheen H, Khalil SB, Kamal K, Wasfy MO, Svennerholm AM, Clemens JD, Savarino SJ. Phenotypic Diversity of Enterotoxigenic Escherichia coli Strains from a Community-Based Study of Pediatric Diarrhea in Periurban Egypt. J Clin Microbiol 1999;37(9):2974-2978.
179. Phetsouvanh R, Midorikawa Y, Nakamura S. The Seasonal Variation in the Micro bial
Agents Implicated in the Etiology of Diarrheal Diseases Among Children in Lao People’s Democratic Republic. Southeast Asian J Trop Med Public Health 1999;30(2):319-323.
180. Punyaratabandhu P, Vathanophas K, Varavithya W, Sangchai R, Athipanyakom S,
Echeverria P, Wasi C. Childhood diarrhoea in a low-income urban community in Bangkok: incidence, clinical features, and child caretaker's behaviours. J Diarrhoeal Dis Res 1991;9(3):244-249.
181. Purohit SG, Kelkar SD,Simha VK. Time Series Analysis of Patients with Rotavirus
Diarrhoea in Pune, India. J Diarrhoeal Dis Res 1998;16(2):74-83. 182. Qadri F, Das SK, Faruque ASG, Fuchs GJ, Albert MJ, Sack RB, Svennerholm A-M.
Prevalence of Toxin Types and Colonization Factors in Enterotoxigenic Escherichia coli Isolated during a 2-Year Period from Diarrheal Patients in Bangladesh. J Clin Microbiol 2000;38(1):27-31.
183. Qiao H, Nillson M, Abreu ER, Hedlund KO, Johansen K, Zaori G, Svensson L. Viral
Diarrhea in children in Beijing, China. J Med Virol 1999; 57:390-396. 184. Radwan SF, Gabr MK, El-Maraghi S, El-Saifi AF. Serotyping of Group A Rotavirus
in Egyptian Neonates and Infant Less than 1 Year Old with Acute Diarrhea. J Clin Microbiol 1997;35(11):2996-2998.
185. Regua Mangia AH, Bravo BLR, Leal MC, Lobo Leite MEL. Epidemiological Survey
of the Enteropathogenic Escherichi coli Isolated from Children with Diarrhoea. J Trop Pediatr 1990;36:176-178.
186. Regua Mangia AH, Duarte AN, Duarte R, Silva LA, Bravo VLR, Leal MC. Aetiology
of Acute Diarrhoea in Hospitalized Children in Rio de Janeiro City, Brazil. J Trop Ped 1993;39:365-367.
Instituto de Investigación Nutricional, Lima, Perú
Page 44 of 48
187. Rodríguez J, Peñalver MD, Curros MV, Pavón P, Alonso C, Fraga JM. Rotavirus: Estudio clínico y epidemiológico en niños hospitalizados menores de dos años. An Esp Pediatr 1996;45(5):499-504.
188. Rowland SGJ, Lloy-Evans N, Williams K, Rowland MGM. The etiology of diarrhoea
studied in the community in young urban Gambian children. J Diarrhoeal Dis Res 1985;3(1):7-13.
189. Ruuska T, Vesikari T. A Prospective Study of Acute Diarrhoea in Finnish Children
from birth to 2 ½ Years of Age. Acta Pædiatr Scand 1991;80:500-507. 190. Ryan MJ, Ramsay M, Brown D, Gay NJ, Farrington CP, Wall PG. Hospital
Admissions Attribuitable to Rotavirus Infection in England and Wales. J Infect Dis 1996;174 (Suppl 1):S12-S18.
191. Rytlewska M, Bako W, Ratajczak, Marek A, Gwizdek A, Czarnecka-Rudnik D,
Świątkowska H, Tyl J, Korzon M. Epidemiological and clinical characteristics of rotaviral diarrhoea in children from Gdańsk, Gdynia and Sopot. Med Sci Monit 2000;6(1):117-122.
192. Sack RB, Santosham M, Reid R, Black R, Croll J, Yolken R, Aurelian L, Wolff M,
Chan E, Garret S, Froehlich J. Diarrhoeal Diseases in the White Mountain Apaches: Clinical Studies. J Diarrhoeal Dis Res 1995;13(1):12-17.
193. Saha MR, Saha D, Dutta P, Mitra U, Bhattacharya SK. Isolation of Salmonella
enterica Serotypes from Children with Diarrhoea in Calcutta, India. J Health Popul Nutr 2001;19(4):301-305.
194. Saidi SM, Iijima Y, Sang WK, Mwangudza AK, Oundo JO, Taga K, Aihara M,
Nagayama K, Yamamoto H, Waiyaki PG, Honda T. Epidemiological Study on Infectious Diarrheal Diseases in Children in a Coastal Rural Area of Kenya. Microbiol Immunol 1997;41(10):773-778.
195. Sakamoto T, Negishi H, Wang Q-H, Ahihara S, Kim B, Nishimura S, Kaneshi K,
Nakaya S, Ueda Y, Sugita K, Motohori T, Nishimura T, Ushijima H. Molecular Epidemiology of Astrovirus in Japan from 1995 to 1998 by Reverse Transcription-Polymerase Chain Reaction With Serotype-Specific Primers (1 to 8). J Med Virol 2000;61:326-331.
196. Salazar-Lindo E, Salazar M, Alvarez JO. Association of diarrhea and low retinol in
Peruvian children. Am J Clin Nutr 1993;58:110-113. 197. Santosham M, Letson GW, Wolff M, Reid R, Gahagan S, Adams R, Callahan C, Sack
RB, Kapikian AZ. A Field Study of the Safety and Efficacy of two Candidate Rotavirus Vaccine in a Native American Population. J Infect Dis 1991;163:483-487.
198. Santosham M, Moulton LH, Reid R, Croll J, Weatherholt R, Ward R, Forro J, Zito E,
Mack M, Brenneman G, Davidson BL. Efficacy and safety of high-dose rhesus-human reassortant rotavirus vaccine in Native American populations. J Pediatr 1997;131(4):632-638.
Instituto de Investigación Nutricional, Lima, Perú
Page 45 of 48
199. Santosham M, Sack RB, Reid R, Black R, Croll J, Yolken R, Aurelian L, Wolff M,
Chan E, Garret S, Froehlich J. Diarrhoeal Diseases in the White Mountain Apaches: Epidemiological Studies. J Diarrhoeal Dis Res 1995;13(1):18-28.
200. Sarabia-Arce S, Salazar-Lindo E, Gilman GH, Naranjo J, Miranda E. Case-control
study of Cryptosopridium parvum infection in Peruvian children hospitalized for diarrhea: possible association with malnutrition and nosocomial infection. Pediatr Infect Dis J 1990;9(9):627-631.
201. Scaletsky ICA, Pedrozo MZ, Oliva CAG, Carvalho RLB, Morais MB, Fagundes-Neto
U. A Localized Adherence-Like Pattern as a Second Pattern of Adherence of Classic Entheropathogenic Escherichia coli to HEp-2 Cells That Is Associated with Infantile Diarrhea. Infect Immun 1999;67(7):3410-3415.
202. Schorling JB, Wanke CA, Schorling SK, McAuliffe JF, De Souza MA, Guerrant R. A
prospective study of persistent diarrhea among children in an urban Brazilian slum. Am J Epidemiol 1990;132(1):144-156.
203. Sebata T, Steele D. Atypical Rotavirus Identified from Young Children with
Diarrhoea in South Africa. J Health Popul Nutr 2001;19(3):199-203. 204. Şerban D, Jebeleanu L, Andronescu D, Petrescu V, David E, Ivanof A, Miu N, Lizeta
M. Variaţia anuală şi sezonnieră a bacteriilor şi rotavirusurilor implicate în etiologia bolii diareice la copil. Bacteriol Virusol Parazitol Epidemiol 1992; 37(1-2): 58-66.
205. Sethi D, Cumberland P, Hudson MJ, Rodrigues LC, Wheeler JG, Roberts JA,
Tompkins DS, Cowden JM, Roderick PJ. A study of infectious intestinal disease in England: risk factors associated with group A rotavirus in children. Epidemiol Infect 2001;126:63-70.
206. Sethi SK, Khuffash FA. Bacterial and viral causes of diarrhoea in children in Kuwait.
J Diarrhoeal Dis Res 1989;7(3 & 4):85-88. 207. Sethi SK. Khuffash FA, Al-Nakib W. Microbial etiology of acute gastroenteritis in
hospitalized children in Kuwait. Pediatr Infect Dis J 1989;8(9):593-597. 208. Sharif M, Deb M, Singh R, Singh K. Cryptosporidium Infection in Children with
Diarrhoea of Acute Onset. J Trop Pediatr 2002;48:187-188. 209. Shornikova A-V, Isolauri E, Burkanova L, Lukovnikova S, Vesikari T. A trial in the
Karelian Republic of oral rehydration and Lactobacillus GG for treatment of acute diarrhoea. Acta Pædiatr 1997;86:460-465.
210. Shukry S, Zaki AM, DuPont HL, Shoukry I, El Tagi M, Hamed Z. Detection of
Enteropathogens in Fatal and Potentially Fatal Diarrhea in Cairo, Egypt. J Clin Microbiol 1986;24(6):959-962.
211. Silva MAR, Naveca FG, de Carvalho IP. Epidemiological Aspects of Rotavirus
Infections in Minas Gerais, Brazil. Braz J Infect Dis 2000;5(4):215-222.
Instituto de Investigación Nutricional, Lima, Perú
Page 46 of 48
212. Simhon A, Abed Y, Schoub B, Lasch EE, Morag A. Rotavirus Infection and Rotavirus
Serum Antibody in a Cohort of Children from Gaza Observed from Birth to the Age on One Year. Int J Epidemiol 1990;19(1):160-163.
213. Steele AD, Basetse HR, Blacklow NR, Herrmann JE. Astrovirus infection in South
Africa: a pilot study. Ann Trop Paediatr 1998;18:315-319. 214. Steele AD, Geyer A, Alexander JJ, Crewe-Brown HH, Fripp PJ. Enteropathogens
isolated from children with gastro-enteritis at Ga-Rankuwa Hospital, South Africa. Ann Trop Paediatr 1988;8:262-267.
215. Stewien K, Mós E, Yanaguita RM, Jerez JA, Durigon EL, Hársi CM, Tanaka H,
Moraes RM, Silva LA, Santos MAA, Candeias MG et. Viral, Bacteria and Parasitic Pathogens Associated wsith Severe Diarrhoea in the City of Sao Paulo, Brazil. J Diarrhoeal Dis Res 1993;11(3):148-152.
216. Subekti D, Lesmana M, Tjaniadi P, Safari N, Frazier E, Simanjuntak C, Komalarini S,
Taslim J, Campbell JR, Oyofo BA. Incidence of Nolwalk-like viruses, rotavirus and adenovirus infection in patients with acute gastroenteritis in Jakarta, Indonesia. FEMS Immunol Med Microbiol 2002 (in press)
217. Subekti D, Oyofo BA, Tjaniadi P, Corwin AL, Larasati W, Putri M, Simanjuntak C,
Punjabi NH, Taslim J, Setiawan B, Djelantik AAGS, Sriwati L, Sumardiati A, Putra E, Campbell JR, Lesmana M. Shigella spp. Surveillance in Indonesia: the Emergencie or Reemergence of S. dysenteriae. Emerg Infect Dis 2001;7(1):137-139.
218. Superti F, Diamanti E, Giovannangeli S, Dobi V, Xhelili L, Donelli G.
Electropherotypes of Rotavirus Strains Causing Gastroenteritis in Infants and Young Children in Tirana, Albania, from 1988 to 1991. Acta Virol 1995;39:257-261.
219. Szücz G, Új M, Mihály I, Deák J. Burden of human rotavirus-associated
hospitalizations in three geographic regions of Hungary. Acta Pædiatr Suppl 1999;426:61-65.
220. Szücz G, Matson DO, Új M, Kukán E, Mihály I, Jelenik Z, Estes K. Group A
rotavirus G type prevalence in two regions of Hungary. Arch Virol 1995;140:1693-1703.
221. Takala AK, Koskenniemi E, Joensuu J, Mäkelä M, Vesikari T. Economic Evaluation
of Rotavirus Vaccinations in Finland: Randomized, Double-Blind, Placebo-Controlled Trial of Tetravalent Rhesus Rotavirus Vaccine. Clin Infect Dis 1998;27:272-282.
222. Tiemessen CT, Wegerhoff FO, Erasmus MJ, Kidd AH. Infection by Enteric
Adenovirus, Rotaviruses, and Other Agents in a Rural African Environment. J Med Virol 1989;28:176-182.
223. Torres ME, Pírez MC, Schelotto F, Varela G, Parodi G, Allende F, Falconí E,
Dell’Acqua L, Gaione P, Méndez MV, Ferrari AM, Montano A, Zanetta E, Acuña
Instituto de Investigación Nutricional, Lima, Perú
Page 47 of 48
AM, Chiparelli H, Ingold E. Etiology of Children’s diarrhea in Montevideo, Uruguay: Associated Pathogens and Unusual Isolates. J Clin Microbiol 2001;39(6):2134-2139.
224. Trabelsi A, Peenze I, Pager C, Jeddi M, Steele D. Distribution of Rotavirus VP7
Serotypes and VP4 Genotypes Circulating in Soussa, Tunisia, from 1995 to 1999: Emergence of Natural Human Reassortants. J Clin Microbiol 2000;38(9):3415-3419.
225. Tswana SA, Jorgensen PH, Halliwell RW, Kapaata R, Moyo SR. The incidence of
Rotavirus Infection in children from two selected study areas in Zimbabwe. Cent Afr J Med 1990;36(10):241-246.
226. Unicomb LE, Kilgore PE, Faruque ASG, Hamadani JD, Fuchs GJ, Albert J, Glass RI.
Anticipating rotavirus vaccines: hospital-based surveillance for rotavirus diarrhea and estimates of disease burden in Bangladesh. Pediatr Infect Dis J 1997;16:947-951.
227. Urrestarazu MI, Liprandi F, Perez de Suárez E, Gonzáles R, Pérez-Schael I.
Características etiológicas, clínicas y sociodemográficas de la diarrea aguda en Venezuela. Rev Panam Sal Pub 1999;6(3):149-156.
228. Velásquez FR, Calva JJ, Guerrero ML, Mass D, Glass RI, Pickering LK, Ruiz-
Palacios GM. Cohort study of rotavirus serotyped patterns in symptomatic and asymptomatic infections in Mexican children. Pediatr Infect Dis J 1993;12:54-61.
229. Vesikari T, Rautanen T, Varis T, Beards GM, Kapikian AZ. Rhesus Rotavirus
Candidate Vaccine. Clinical Trial in Children Vaccinated Between 2 and 5 Months of Age. Am J Dis Child 1990;144:285-289.
230. Vesikari T, Ruuska T, Green KY, Flores J, Kapikian AZ. Protective efficacy against
serotype 1 rotavirus diarrhea by live oral rhesus-human reassortant rotavirus vaccines with human rotavirus VP7 serotype 1 or 2 specificity. Pediatr Infect Dis J 1992;11:535-542.
231. Viboud GI, Jouve MJ, Binsztein N, Vergara M, Rivas M, Quiroga M, Svennerholm
AM. Prospective Cohort Study of Enterotoxigenic Escherichia coli Infections in Argentinean Children. J Clin Microbiol 1999;37(9):2829-2833.
232. Vijayan V, Quak SH, Wong HB. Incidence, clinical features and epidemiology of
rotavirus gastro-enteritis in hospitalized children. Ann Trop Paediatr 1990;10:179-183.
233. Visser LE, Cano Portero R, Gay NJ, Martínez Navarro JF. Impact of rotavirus disease
in Spain: an estimate of hospital admissions due to rotavirus. Acta Pædiatr Suppl 1999;426:72-76.
234. Wanke CA, Schorling JB, Barret LJ, De Souza MA, Guerrant RL. Potential role of
adherence traits of Escherichia coli in persistent diarrhea in an urban Brazilian slum. Pediatr Infect Dis J 1991;10(10):746-751.
Instituto de Investigación Nutricional, Lima, Perú
Page 48 of 48
235. de Wit MAS, Koopmans MPG, Kortbeek LM, van Leeuwen NJ, Vinjé J, van Duynhoven THP. Etiology of Gastroenteritis in Sentinel General Practices in The Netherlands. Clin Infect Dis 2001;33:280-287.
236. de Wit MAS, Koopmans MPG, Kortbeek LM, Wannet WJB, Vinjé J, van Leusden,
Baertelds AIM, van Duynhoven THP. Sensor, a Population-based Cohort Study on Gastroenteritis in the Neetherlands: Incidence and Etiology. Am J Epidemiol 2001;154(7):666-674.
237. Yachha SK, Singh V, Kanwar SS, Mehta S. Epidemiology, subgroups and serotypes
of rotavirus diarrhea in north Indian communities. Indian Pediatr 1994;31:27-33. 238. Yap KL, Yasmin AM, Wong YH, Ooi YE, Tan SC, Jegathesan M et al. A one year
community-based study on the incidence of diarrhoea and rotavirus infection in urban and suburban Malaysian children. Med J Malaysia 1992;47(4):303-308.
239. Yousseff M, Shurman A, Bougnoux M-E, Rawashdeh M, Bretagne S, Strockbine N. Bacterial, viral and parasitic enteric pathogens associated with acute diarrhea in hospitalized children from northern Jordan. FEMS Immunol Med Microbiol 2000;28:257-263.