Embed Size (px)
Citation preview

Gut, 1980, 21, 1017-1023
Allergic proctitis, a clinical and immunopathologicalentityP C M ROSEKRANS,* C J L M MEIJER, A M VAN DER WAL, AND J LINDEMAN
From the Department of Gastroenterology and Pathology, University Medical Centre, Leiden,the Netherlands
SUMMARY Patients with isolated ulcerative proctitis form a heterogeneous group. Some maydevelop ulcerative colitis, others have a limited, benign disease. Twelve patients with isolated proctitiswith a mean course of seven years were studied. All patients had a typical clinical picture consistingof a mild and intermittent course of the disease with the presenting symptom of rectal blood loss. Atendoscopic examination the inflammatory process was limited to the rectal and distal sigmoidcolonic mucosa with a clear upper border beyond which the mucosa of the sigmoid colon was
normal. Histologically the mucosal biopsy specimens of the affected rectum resembled those ofulcerative colitis. However, in contrast with proctitis on the base of ulcerative colitis or Crohn'sdisease, immunoperoxidase staining revealed a markedly increased number of IgE containing cellsin the lamina propria of rectal mucosa biopsies. As an IgE-mediated immune mechanism was con-
sidered to play a role in this type of proctitis, eight of the 12 patients were treated with oral adminis-tration of disodium cromoglycate (DSCG). All patients were improved by the drug. The remainingfour patients with mild proctitis did not require treatment. We concluded that, in patients withisolated proctitis on clinical and immunopathological criteria, a group can be separated whichresponds to DSCG, a condition for which we suggest the name 'allergic proctitis'.
Isolated ulcerative proctitis can be defined as aninflammatory process of the rectal mucosa, withouta specific cause, indistinguishable in appearancefrom that seen in ulcerative colitis, but with a clearupper border beyond which the mucosa of the sig-moid colon is normal by endoscopical vision and onx-ray examinination.1-3 Ulcerative proctitis may be alimited, relatively benign disease with few complica-tions and a good prognosis.24 Some workers believethat diffuse ulcerative colitis and ulcerative proctitisare pathologically identical and consider proctitis avariant of ulcerative colitis.15 Other authors claimthat proctitis is not the same as ulcerative colitis,primarily on the basis of clinical criteria. Many ofthe alleged differences could be explained by theextent of involvement.6fi Rice-Oxley8 describedproctitis as early ulcerative colitis.
Thus, the difference between isolated proctitis andulcerative colitis appears to be the ultimate course
*Address for correspondence: P C M Rosekrans, Department ofGastroenterology Academisch Ziekenhuis Leiden. 2333 AA Leiden,the Netherlands.
Received for publication 8 July 1980
of the disease rather than the presence of definitedistinguishing features at the onset.
Systemic and local immunological abnormalitieshave been described in ulcerative colitis; however,data regarding the local immunological factors areconflicting.9-13 Immunological abnormalities havealso been reported in isolated ulcerative procti-tiS.14 15
Wright and Truelove16 have suggested a possiblepathogenetic role for milk in ulcerative colitis, asmilk antibodies were found in many patients.Intradermal tests, especially to casein, were fre-quently positive in patients with ulcerative colitis,but the results did not differ from those found inhealthy individuals.17
Large numbers of eosinophils have been reportedin the rectal mucosa of patients with ulcerativecolitis18 and proctitis19, suggesting an allergicphenomenon in these disorders. The beneficialeffect of disodium cromoglycate (DSCG) in patientswith proctitis20 21 and less clear-cut responses inpatients with definite ulcerative colitis22-24 suggeststhat different immunological mechanisms may beimplicated in these diseases.
1017
on Novem
ber 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.21.12.1017 on 1 Decem
ber 1980. Dow
nloaded from

Rosekrans, Meijer, van der Wal, and Lindeman
In the present study we have examined the laminapropria cellular infiltrate of patients with localisedulcerative proctitis and compared this with the proc-titis associated with ulcerative colitis and Crohn'sdisease. In contrast with patients with ulcerativecolitis and Crohn's disease, patients with localisedproctitis have an increased number of IgE containingcells in the rectal mucosa. We believe that thisgroup of patients, with typical clinical and immuno-pathological features, form a separate entity.
PATIENTSWe examined 12 patients with symptoms of proctitis(average age 47 years; range 28-71 years). The pre-senting symptom in all cases was rectal bleeding,usually mild in degree and intermittent in appear-ance. In contrast with patients with diffuse colonicinvolvement no patient had rectal haemorrhage ofsufficient severity to require blood replacement. Achange in bowel habits was noted by most of thepatients. Some had constipation, particularly ifstool frequency is not considered to include smalldischarges of blood and mucopurulent material.True diarrhoea was present in only three patientswith an average of not more than four stools a day.Two patients had abdominal cramps associatedwith tenesmus. The general health of all patients wasgood with absence of malaise, fever, or weight loss.At sigmoidoscopic examination these proctitispatients were selected from those with ulcerativecolitis by the sharp limitation of the inflammatoryprocess at, or just above the level of, the recto-sigmoid junction. The sigmoidoscopic appearanceis one of marked hyperaemia and oedema of therectal mucosa, with superficial ulcerations. Multiplepunctate haemorrhages may be visible and minormanipulation of the endoscope produces freshbleeding.Only one patient (no. 2) had a history of atopy.
She had hay fever, eczema, and allergic rhinitis.Two patients had a family history ofatopy (no. 8 hayfever, no. 9 flexural eczema).For all patients the course was one of intermittent
remission and exacerbation. The mean duration ofthe disease was seven years.At least two mucosal biopsies were obtained from
each patient. The first biopsy was taken from therectum, approximately 7 cm from the anal margin,the second from the distal sigmoid colon at approxi-mately 20 cm.
Eight of the 12 patients were treated with DSCGt,800 mg orally (200 mg qds, before meals and sleep-ing). The patients were instructed to open the cap-sule and to dissolve the DSCG powder in a glass ofwarm water. This was done to avoid the possibilitytObtained from Fisons Ltd., Pharmaceutical Division, England.
that DSCG might form aggregates with the gelatinin the upper gastrointestinal tract and not be welldispersed in the colon. The remaining four patients(nos. 5, 6, 11, and 12) with very mild proctitis or aspontaneous remission did not require treatment.Clinical data of the patients are summarised inTable 1.
All patients were treated with oral sulphasalazine.Three patients (nos. 1, 3, and 4) had topical corti-costeroid treatment.The immunohistochemical and morphometric
biopsy findings from the 12 proctitis patients werecompared with the rectal and colonic sigmoidbiopsy specimens obtained from three groups ofpatients:
Ulcerative colitis groupThere were 10 patients in this group with ulcerativecolitis (average age 37 years; range 27-63 years). Thediagnosis was based on clinical, radiological, endo-scopic, and histological findings.25 All patients in thisgroup had severely inflamed mucosae in the sigmoidcolon and rectum.
Crohn's disease groupTen patients with Crohn's disease of the colon(average age 34; range 21-49 years) were includedin this group. The history, radiological, endoscopic,and histological findings were typical of coloniclocalisation of Crohn's disease. In a number ofcases there were only minor signs of inflammation inthe distal colon because of the segmental nature ofCrohn's disease.
ControlgroupThe ten control patients in this group had nosign of colitis and colonoscopy was performed be-cause of a single polyp or the irritable bowel syn-drome (average age 35 years; range 19-64 years).
Methods
The sigmoidoscopic examinations were performedwith an Olympus fibre colonoscope (CFIB) and anOlympus fibre sigmoidoscope (TCF IS).
Rectal and sigmoid colonic mucosal biopsyspecimens were fixed for three hours in a sublimateformaldehyde mixture.26 After fixation tissue sam-ples were embedded in paraplast and 4 ,um thicksections were cut perpendicular to the luminal sur-face and mounted on glass slides. Sections werestained with haematoxylin and eosin (HE) andperiodic acid Schiff (PAS) and specifically forIgA, IgG, IgM, IgD, and IgE heavy chains, using anindirect immunoperoxidase technique.
Rabbit antisera against IgA, IgG, and IgM heavy
1018
on Novem
ber 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.21.12.1017 on 1 Decem
ber 1980. Dow
nloaded from

Allergic proctitis, a clinical and immimnopathological entity
Table I Clinical and laboratory data ofpatients with histologically proven proctitis
X..X -.Z zz Z: Z rz .^n -ZCJS.. S~.
§L CP
Superficial NormalulcerationsSuperficial Normalulcerations
Superficial Constip.ulcerationsUlcerations Constip.Superficial NormalulcerationsSuperficial NormalulcerationsHyperemia DiarrhoeaoedemaHyperemia DiarrhoeaoedemaSuperficial Constip.ulcerationsSuperficial DiarrhoeaulcerationsHyperemia NormaloedemaOedema Normal
z
Lu~~b
~ 1 11C .-
_ a: ~ ': a wC~ S.bp , LuiS.i
4LU Cl -1.1
Intermittent 9.1
Intermittent 8.5
Intermittent 8.3
Intermittent 8.8Intermittent 7-2
Intermittent 8.4
Intermittent 8-2
Intermittent 9.4
Intermittent 9.0
Intermittent 8-3
Intermittent 8.4
Intermittent 7.5
17
10
3
816
12
7
5
13
190 31 12 53 -
50 34 9 30
50 16 7 21 -
180 35 9 82 +100 29 6 80 NT
180 12 8 49 - NT
160 14 12 51 - +
150 1 1 8 56 - +
50 26 1 2 20 - +
14 220 32 6
10 170 19 9
10 90 15 6
24 - +
72 - NT
192 - NT
ESR: erythrocyte sedimentation rate, Westergren's method. Eos: peripheral blood eosinophils, normal count: 40-400/mm2. Rectum and sigmoidIgE/mm: number of IgE containing cells per mm mucosal length. Serum IgE: healthy controls 95 % < 500 ng/ml. IgE anti-milk: RAST for specificIgE milk antibodies. Effect DSCG: + beneficial effect DSCG treatment: NT: no DSCG treatment.
chains were obtained from Dakopatts (Denmark)and rabbit antisera against lgD and IgE from theCentral Laboratory of the Netherlands Red CrossBlood Transfusion Service, Amsterdam. The speci-ficity of these antisera has been described before.27Horse-radish peroxidase labelled goat anti-rabbitIgG was obtained from Miles (Yedah, Israel).The method we used for morphometric study of
the stained sections of rectal and colonic biopsyspecimen was as follows:Images of the sections were projected with a
standard magnification of x 200 on graph paperand drawings were made. The morphometricanalysis of the drawings was done on a graphictablet (Tektronix) interfaced to a laboratory com-puter (PDP 11/10; Digital Equipment Corp.,Maynard, Mass., USA).The immunoglobulin containing cell number was
expressed per millimetre mucosal length.13Serum 1gE was estimated by a solid phase radio-
immunoassay and specific IgE milk antibodies by aradio-allergo-sorbent test (RC Aalberse, CentralLaboratory of the Netherlands Red Cross BloodTransfusion Service, Amsterdam).
Statistical analysis was performed using Student'st test.
Results
The histopathological findings in the patients withisolated proctitis were similar to those with ulcera-tive colitis. The infiltrate was mainly restricted tothe mucosa. In seven patients with isolated proctitisan increased number of eosinophils was noticed andin nine patients the number of mast cells was in-creased. The degree of inflammation in most ulcera-tive colitis patients was more pronounced than inisolated proctitis.
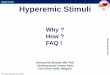
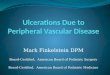
Similarly, the number of IgA, IgG, and IgMcontaining cells per mm mucosa length resembled thefindings in ulcerative colitis. The number of IgGcontaining cells correlated with the degree of activityof the disease. Sometimes a slight increase in thenumber of IgM containing cells was found (Fig. 1).
In the group of patients with isolated proctitis wecompared the immunohistochemical findings in therectal biopsy specimens taken at 7 cm from the analmargin with the findings in the biopsies taken moreproximally from the distal sigmoid colon. Thenumbers of IgA, IgG, and IgM containing cells permm mucosal length did not differ significantly inthe two biopsy specimens. The number of IgE con-taining cells per mm mucosal length in the rectal
C -o
S.C
x,,
1 57 F
2 33 F Hay fever.
rhinitis,eczema
Family
Family
16
8
11
74
5
7
1 1
3
2
8
3
45
6
7
8
9
10
11
12
42
50
32
28
45
42
70
40
59
71
F
M
F
F
F
M
M
F
FF
20
15
15
810
20
15
15
25
10
20
20
1019
on Novem
ber 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.21.12.1017 on 1 Decem
ber 1980. Dow
nloaded from

Rosekrans, Meijer, van der Wal, and Lindeman
vAllergic proctitis Ulcerative colitis
(n=12 ) ( n=10
Fig. 1 Statistical analysis showed no significantdifference between the number of immunoglobulincontaining cells (IgA, IgG and IgM) in rectal mucosa ofpatients with ulcerative colitis and allergic proctitis.
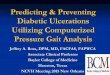
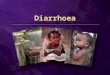
mucosa biopsy specimens was much higher than inthe sigmoid colonic biopsy specimens, where theactivity of inflammation was less (Fig. 2).We compared the number of IgE containing cells
in the rectal and sigmoid colonic mucosa obtainedfrom the isolated proctitis patients with the results ofimmunohistochemical study in the three controlgroups (ulcerative colitis patients, patients withCrohn's disease of the colon, and patients withoutcolitis). The number of IgE containing cells in thecontrol groups was significantly lower than in theproctitis group for both rectal and sigmoid colonicbiopsy specimens (p <0-001, Fig. 2).
Eight of the 12 proctitis patients were treated withoral DSCG in a dose of 800 mg daily for at least sixweeks. All patients responded to DSCG. Dis-appearance or diminution of the daily blood loss wasthe most striking effect. The frequency of bowelmotions changed only in two patients with diar-rhoea (nos 7 and 8). There was no significant changein the haemoglobin, white cell count, or ESRduring treatment.
All patients who used topical corticosteroids(nos. 1, 3, and 4) were able to stop this treatment.Two patients (nos. 1 and 2) had a relapse of the
proctitis two and four months after discontinuingDSCG therapy. After discontinuing therapy patient
30
25
20
15-
10
5-
T
1,;1'ill 1
Rectum
Sigmoid
1 SD
Fig. 2 Patients with allergic proctitis showed astatistically significant increased number ofIgEcontaining cells in rectal and sigmoid colonic mucosacompared with controls and patients with ulcerativecolitis and Crohn's disease (rectum: P< 0.0001,sigmoid: P< OO0O1).
no. 1 needed a dose of 1600 mg DSCG daily toachieve remission.Four patients were examined endoscopically at
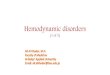
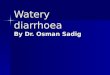
least six weeks after starting DSCG treatment. In allthese patients the endoscopic appearance was con-siderably improved, the ulcers had disappeared, andthe rectal mucosa was normal or mild hyperaemiaand oedema was seen in the distal part of the rectum(nos. 1, 2, 4, and 7). On histological examination ofthe mucosal biopsy specimens the acute inflamma-tory changes had disappeared (Fig. 3) The numberof IgE containing cells per mm mucosal length didnot differ significantly before and after DSCG treat-ment (Table 2) and showed no change withclinical response.
Values for the serum IgE varied between 20
___j
;
1020
on Novem
ber 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.21.12.1017 on 1 Decem
ber 1980. Dow
nloaded from

Allergic proctitis, a clinical and immunopathological entity
.s*.! ..:. ... _....
Fig. 3 (a) Four IgE containing cells in quiescent part of rectal mucosa in patient no. 7 with allergic proctitis. IgEperoxidase staining, x 120. (b) High power view of (a). Two IgE containing cells. IgE peroxidase staining, x 600.
and 192 ng/ml (95 % of healthy controls < 500ng/ml). The RAST test for specific lgE milk anti-bodies was negative in all patients.
Discussion
The results of this study show that in the patientswith isolated proctitis a group can be separated on
clinical criteria (intermittent, benign course, limita-tion of inflammatory extent) and immunopathologi-
cal findings (high numbers of IgE containing cells inrectal mucosa), a condition for which we suggest thename of 'allergic proctitis'.
In contrast with ulcerative colitis the course of thedisease limited to the rectum is more benign;there are fewer complications, the absence of extra-colonic manifestations is quite remarkable, spon-taneous remissions are much more likely to occur,and the health of the patient is generally maintained.
Allergic proctitis is characterised by persistent or
Table 2 Endoscopic appearance of rectal mucosa and IgE containing cells per nmn mucosal length in rectal biopsyspecimens before and after six weeks DSCG treatment.
Patient no. Before DSCG After DSCG
Endoscopic Rectum (IgE/mm) Endoscopic Rectuim (IgE/mm)appearance appearance
1 Superficial ulceration 31 Hyperaemia, oedema 222 Superficial ulceration 34 Normal 204 Ulcerations 35 Hyperaemia, oedema 327 Hyperaemia, oedema 14 Normal 17
1021
,k*..;Ell,'
on Novem
ber 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.21.12.1017 on 1 Decem
ber 1980. Dow
nloaded from

1022 Rosekrans, Meijer, van der Wal, and Lindeman
recurrent bloody mucous discharges. The stools areoften formed, but occasionally loose, and sometimesassociated with rectal tenesmus and urgency. Thesigmoidoscopic picture is identical with that seen inulcerative colitis, but the difference is in the sharplimitation of the inflammatory process to the level ofthe distal part of the sigmoid or below. In a meanfollow-up period of more than seven years, none ofthe 12 patients we studied has developed a moreextensive colitis.
Early reports claimed already that a food allergyfactor was operative in ulcerative colitis28 29 andadditional clinical observation led to a therapeutictrial of a milk-free diet.30 A subsequent relationshipwas found between high haemagglutinating anti-bodies to milk protein and relapses of ulcerativecolitis.31 There has been no further support for therole of milk allergy in ulcerative colitis. No differ-ence has been found between patients with ulcera-tive colitis and controls with respect to milk anti-bodies'7 and IgE specific antibodies to milk pro-tein.32 Similarly, we were unable to demonstrateIgE specific antibodies to milk protein in ourpatients.Only one patient had a personal history, while two
patients had a family history of atopy. This incidenceof atopic disorders is not as high as found by pre-vious studies.3233We found large numbers of IgE containing cells
in the rectal mucosa in patients with isolated procti-tis, whereas normal rectal mucosa contains only afew of these cells. This confirms the findings ofHeatley et al.'4 In ulcerative colitis, however,contrary to the results of O'Donoghue and Kumar,34we did not find increased numbers of IgE containingcells in rectal and colonic mucosal biopsy specimens.
Eight of the patients were treated with oralDSCG in a dose of 800 mg daily. In all patients thistreatment was effective. Heatley et al.20 were firstto report this treatment in patients with proctitis.They used a dose of 700 mg DSCG daily, partlygiven by enema and partly orally. Fourteen of the26 patients responded to DSCG treatment, butthere were no significant changes in rectal biopsyfindings.DSCG has also been investigated in ulcerative
colitis. Mani et al.21 treated 12 patients for sixmonths with 2 g of oral DSCG per day. Thesepatients showed an improvement clinically, sig-moidoscopically, and on rectal biopsy. However,subsequent studies were less promising.22-24
Different pathogenetic mechanisms may accountfor the variable results of DSCG treatment in in-flammatory bowel disease. As there is no directevidence that IgE mediated hypersensitivity isinvolved in the pathogenesis of ulcerative colitis, it
is conceivable that DSCG is not effective in thisdisorder.
Heatley et al.14 found that patients with an in-creased number of IgE containing cells with anexcess of eosinophils in the rectal mucosa showedclinical improvement on DSCG. This suggests that ahypersensitivity reaction, mediated by IgE, isimportant in the pathogenesis of allergic proctitis.It is of interest that DSCG treatment does notaffect the number of IgE containing cells in themucosa of the rectum and the sigmoid colon. Thisis in keeping with the mode of action of DSCG,which inhibits the release of chemical mediatorssuch as histamine and does not influence IgE anti-body formation.35The pathogenesis of this disease is still unknown.
One explanation might be that antigens present inthe faeces are responsible for the inflammatoryprocess in the bowel wall at the site of maximumfaecal stasis, the rectum.
We gratefully acknowledge help from many peoplewho made it possible to conduct the study: Dr CCornelisse and Mrs A van der Zon for morpho-metric analysis, Dr J Hermans for statistical analysis,Mrs M van der Zee-Berkhout for administrativehelp, Fisons Limited, Pharmaceutical Division, forsupplying the disodium cromoglycate and Dr R CAalberse, Department of Immunochemistry of theCentral Laboratory of the Netherlands Red CrossBlood Transfusion Service, Amsterdam, for theanalysis of serum IgE and specific lgE milk anti-bodies.
References
'Lennard-Jones JE, Cooper GW, Newell AC, WilsonCWE, Avery Jones F. Observations on idiopathicproctitis. Gut 1962; 3: 201-6.2Nugent FW, Veidenheimer MC, Zuberi S, GarabedianMM, Parikh NK. Clinical course of ulcerative procto-sigmoiditis. Dig Dis 1970; 15: 321-6.3Powell-Tuck J, Ritchie JK, Lennard-Jones JE. Theprognosis of idiopathic proctitis. Scand J Gastroenterol1977; 12: 727-32.
4Folley JH. Ulcerative proctitis. N Engl J Med 1970;282: 1362-4.5Lockhart Mummery P. The varieties of colitis and theirdiagnosis by sigmoidoscopic examination. Br Med J1911;2: 1685-6.
6iBrooke BN. What is ulcerative colitis? Lancet 1953;1: 1220-5.7Goligher JC. What is ulcerative colitis? Lancet (letter)1953; 2: 38.8Rice-Oxley JM. What is ulcerative colitis? Lancet(letter) 1953; 2: 38.
on Novem
ber 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.21.12.1017 on 1 Decem
ber 1980. Dow
nloaded from

Allergic proctitis, a clinical and immunopathological entity 1023
9Crabbe PA, Heremens JF. The distribution of immuno-globulin containing cells along the human gastro-intestinal tract. Gastroenterology 1966; 51: 305-16.
'0Gelzayd EA, Kraft SC, Fitch FW, Kirsner JB. Distri-bution of immunoglobulins in human mucosa. 1IUlcerative colitis and abnormal mucosal controlsubjects. Gastroenterology 1968; 54: 341-7.
"Soltoft J, Binder V, Gudmand-Hoyer E. Intestinalimmunoglobulins in ulcerative colitis. Scand J Gastro-enterol 1973; 8: 293-300.
'2Baklien K, Brandtzaeg P. Immunohistochemicalcharacterization of local immunoglobulin formation inCrohn's disease of the ileum. Scand J Gastroenterol1976; 11: 447-57.
13Rosekrans PCM, Meijer CJLM, van der Wal AM,Cornelisse CJ, Lindeman J. Immunoglobulin-containingcells in inflammatory bowel disease. Gut 1980; 21: 941-7.
14Heatley RV, Calcraft BJ, Fifield R, Rhodes J, White-head RH, Newcombe RG. Immunoglobulin E in rectalmucosa of patients with proctitis. Lancet 1975; 2:1010-2.
'5Das KM, Erber WF, Rubinstein A. Immunohisto-chemical changes in morphologically involved anduninvolved mucosa of patients with idiopathic proc-titis. J Clin Invest 1977; 59: 379-85.
'6Wright R, Truelove SC. A controlled therapeutic trialof various diets in ulcerative colitis. Br Med J 1965;2: 138-41.
17Jewell DP, Truelove SC. Circulating antibodies to cow'smilk proteins in ulcerative colitis. Gut 1972; 13: 796-801.
18Wright R, Truelove SC. Circulating and tissue eosino-phils in ulcerative colitis. Am JDig Dis 1966; 2: 831-46.
'9Heatley RV, James PD. Eosinophils in rectal mucosa.Gut 1978; 20: 787-91.
20Heatley RV, Calcraft BJ, Rhodes J, Owen E, Evans BK.Disodium cromoglycate in the treatment of chronicproctitis. Gut 1975; 16: 559-63.
21Mani V, Green FHY, Lloyd G, Fox H. Treatment ofulcerative colitis with oral disodium cromoglycate.Lancet 1976; 1: 439-41.
2Dronfield MW, Langman MJS. Controlled comparison
of sodium cromoglycate and sulphasalazine in themaintenance of remission in ulcerative colitis. Gut 1977;18: A973.
23Gould SR, Buckell NA, Day DW, Edwards AM,Lennard-Jones JE. Controlled trial of disodiumcromoglycate in chronic persistent colitis. Gut 1978;19: A444.
24Willoughby CP, Heyworth MF, Piris J, Truelove SC.Comparison of D.S.C.G. and sulphasalazine asmaintenance therapy for ulcerative colitis. Lancet 1979;1: 119-22.
25Morson BC, Dawson IMP. Gastrointestinal pathology,Oxford: Blackwell Scientific Publications; 512-74.
26Bosman FT, Lindeman J, Kuiper G, van der Wal A,Kreuning J. The influence of fixation on immuno-peroxidase staining of plasma cells in paraffin sectionsof intestinal biopsy specimens. Histochemistry 1977;53: 57-62.
27Rosekrans PCM, Meijer CJLM, Cornelisse CJ, vd WalAM, Lindeman J. Use of morphometry and immuno-histochemistry of small intestinal biopsy specimens inthe diagnosis of food allergy. J Clin Pathol 1980; 33:125-30.
28Andressen AFR. Ulcerative colitis. An allergic phe-nomenon. Am J Dig Dis 1941; 9: 91-8.
29Rowe AH. Chronic ulcerative colitis-allergy in itsetiology. Ann Intern Med 1942; 17: 83-100.
30Truelove SC. Ulcerative colitis provoked by milk.Br Med J 1961; 1: 154-60.
31Wright R, Truelove SC. Circulating antibodies todietary proteins in ulcerative colitis. Br Med J 1965;2:142-44.
32Jewell DP, Truelove SC. Reaginic hypersensitivity inulcerative colitis. Gut 1972; 13: 903-6.
33Mee AS, Brown D, Jewell DP. Atopy in inflammatorybowel disease. Scand J Gastroenterol 1979; 14: 743-6.
340'Donoghue DP, Kumar P. Rectal IgE cells in in-flammatory bowel disease. Gut 1979; 20: 149-53.
35Cox JG. Disodium cromoglycate. Mode of action andits possible relevance to the clinical use of the drug.Br J Dis Chest 1971; 65: 189-204.
on Novem
ber 4, 2020 by guest. Protected by copyright.
http://gut.bmj.com
/G
ut: first published as 10.1136/gut.21.12.1017 on 1 Decem
ber 1980. Dow
nloaded from